
A Call for a Reform of the Influenza Immunization Program in Mexico: Epidemiologic and Economic Evidence for Decision Making

Abstract
:1. Introduction
2. Materials and Methods
2.1. Epidemiological Analysis
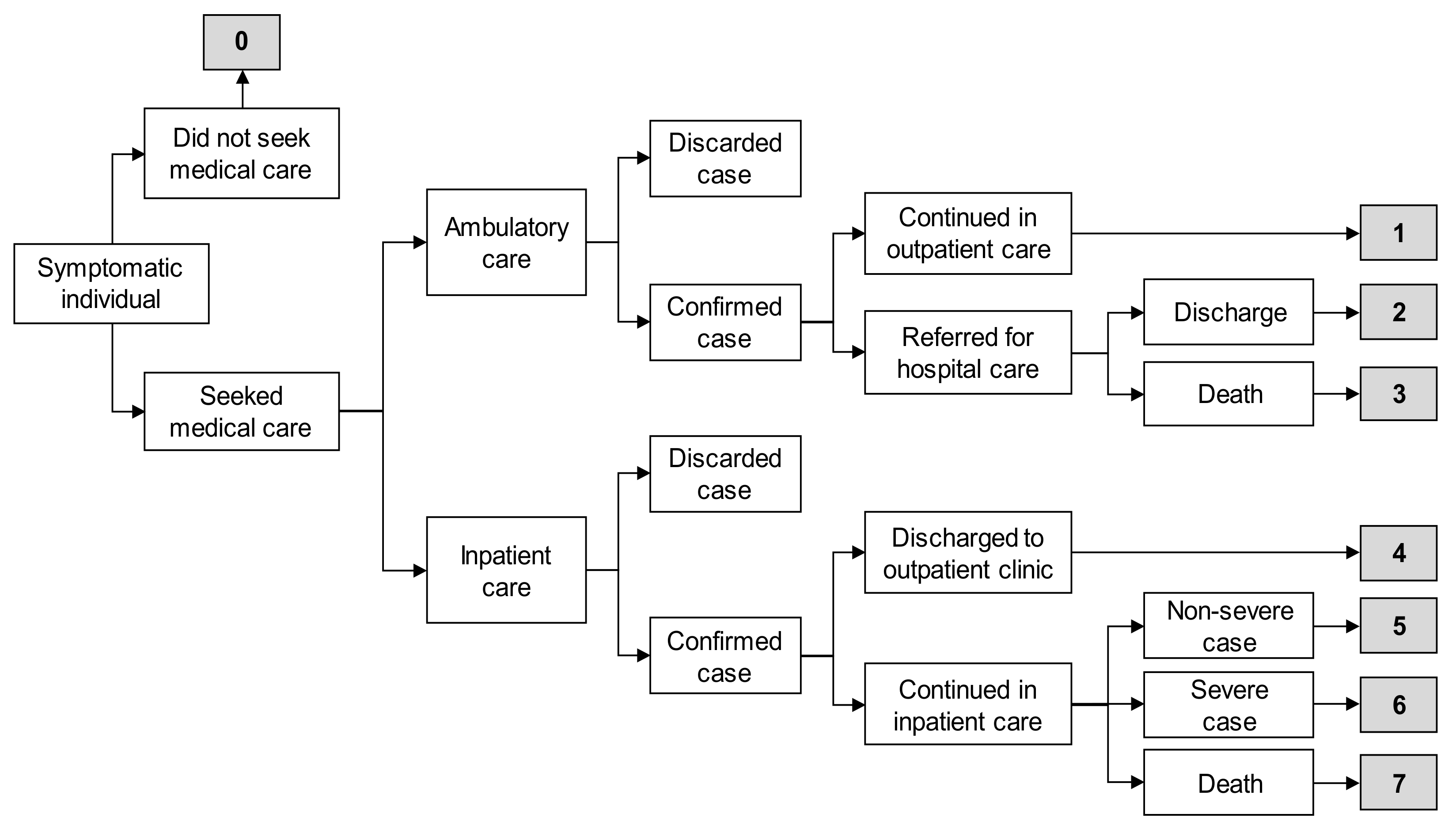
2.2. Economic Analysis
3. Results
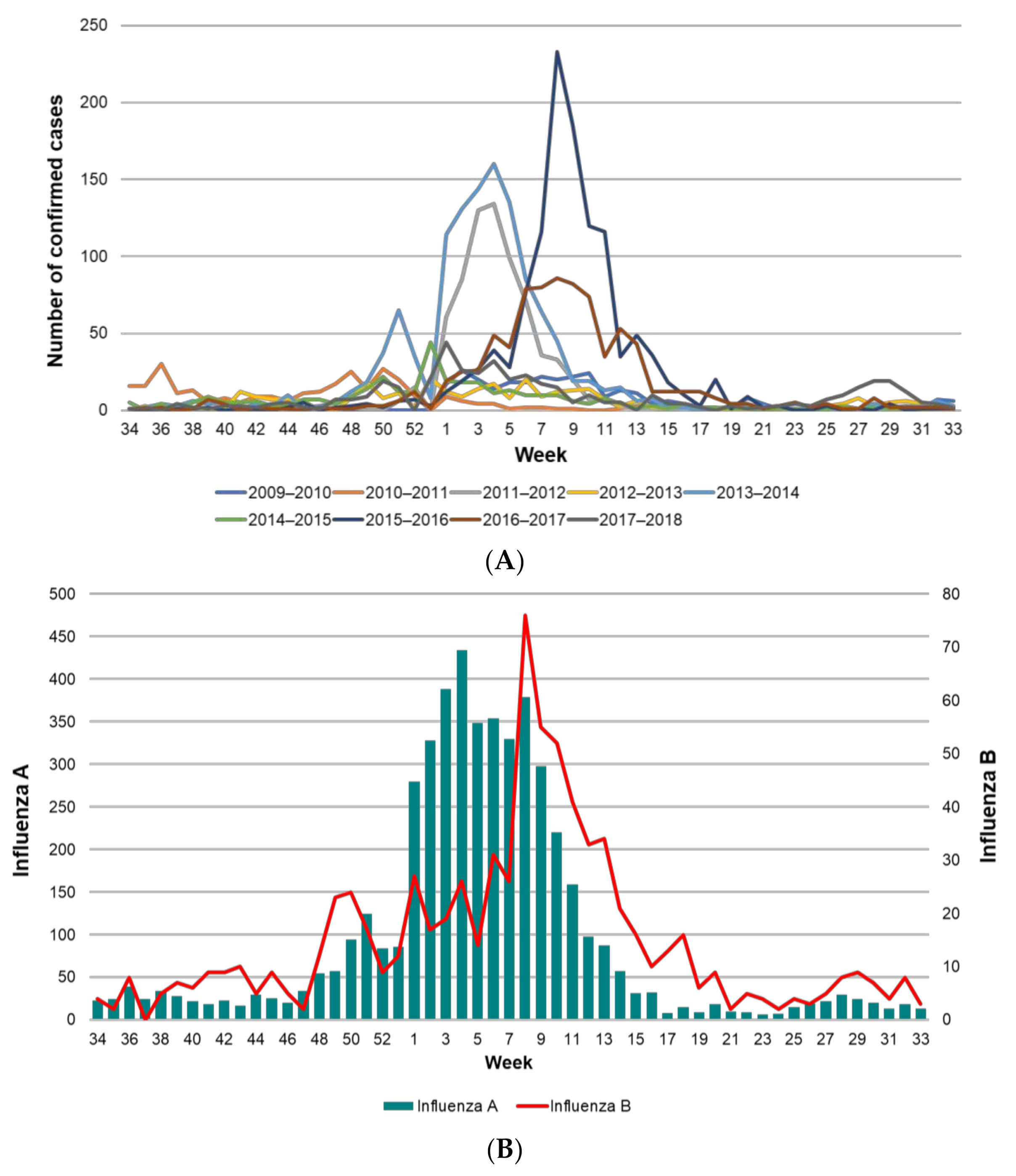
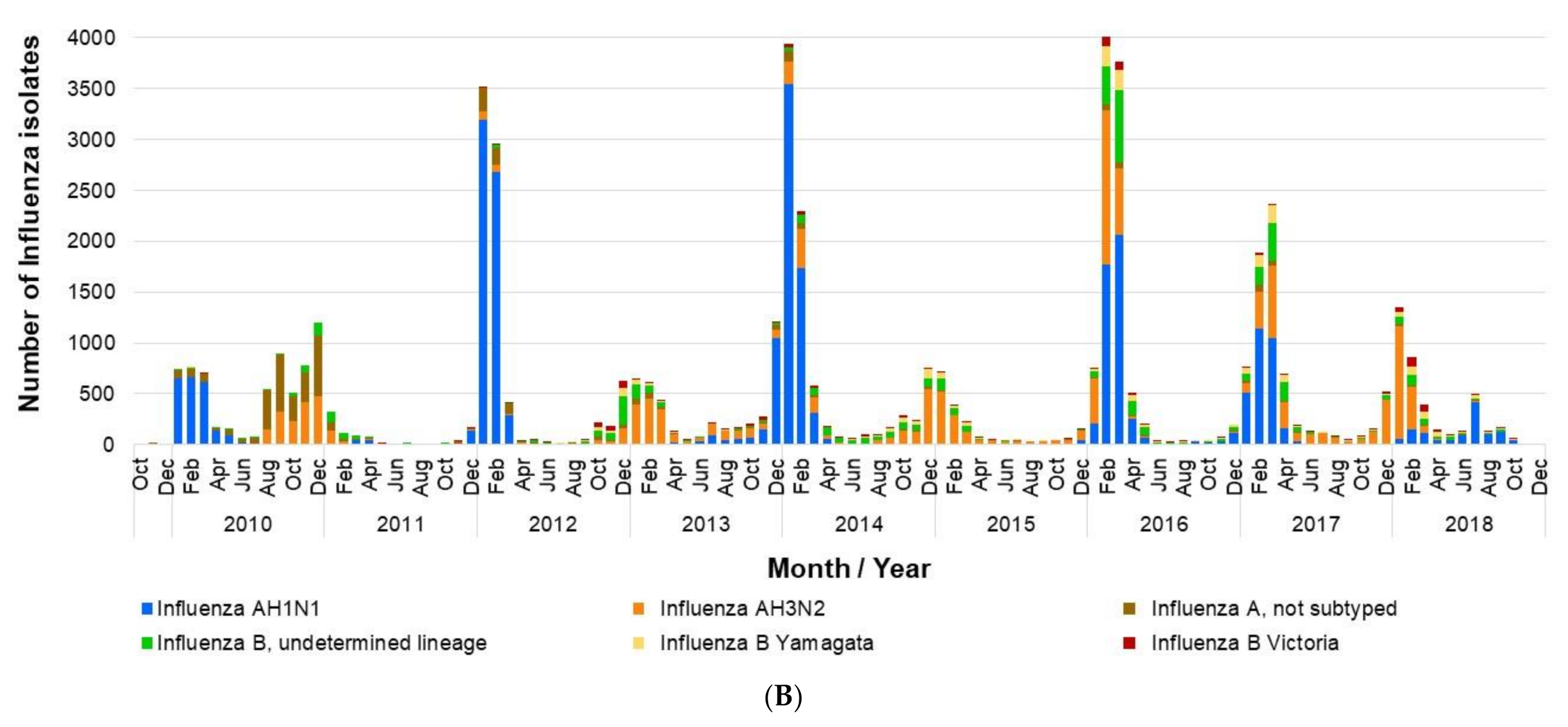
3.1. Influenza Burden of Disease
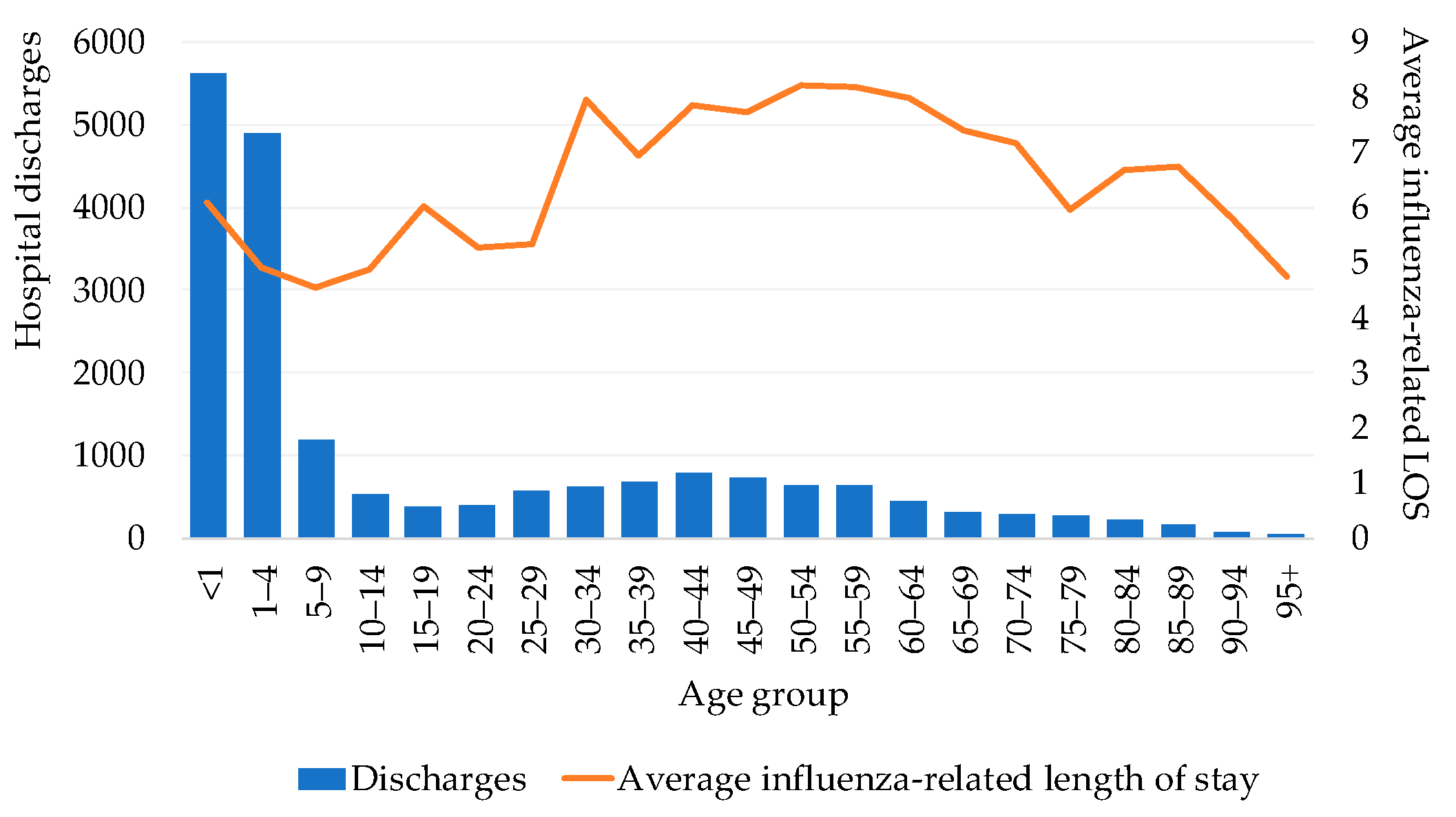
3.2. Hospital Discharges and Length of Stay
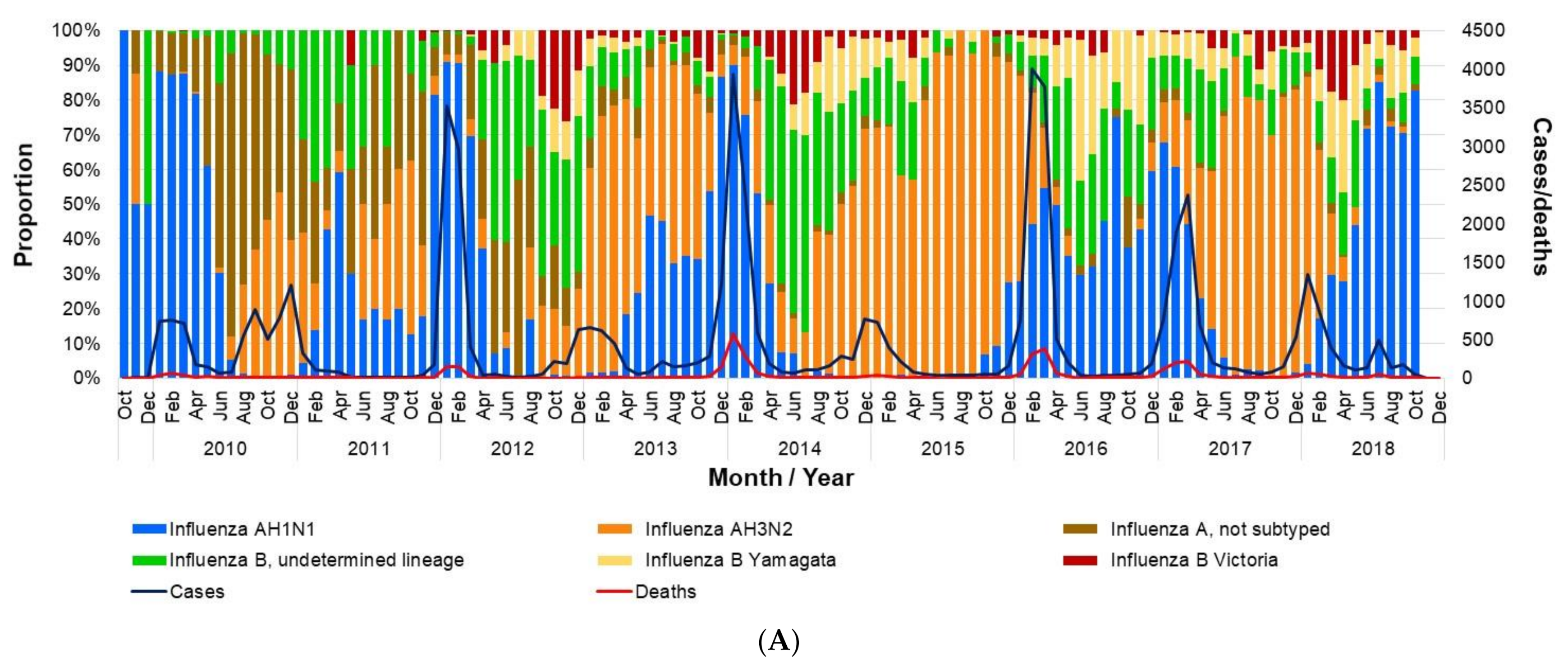
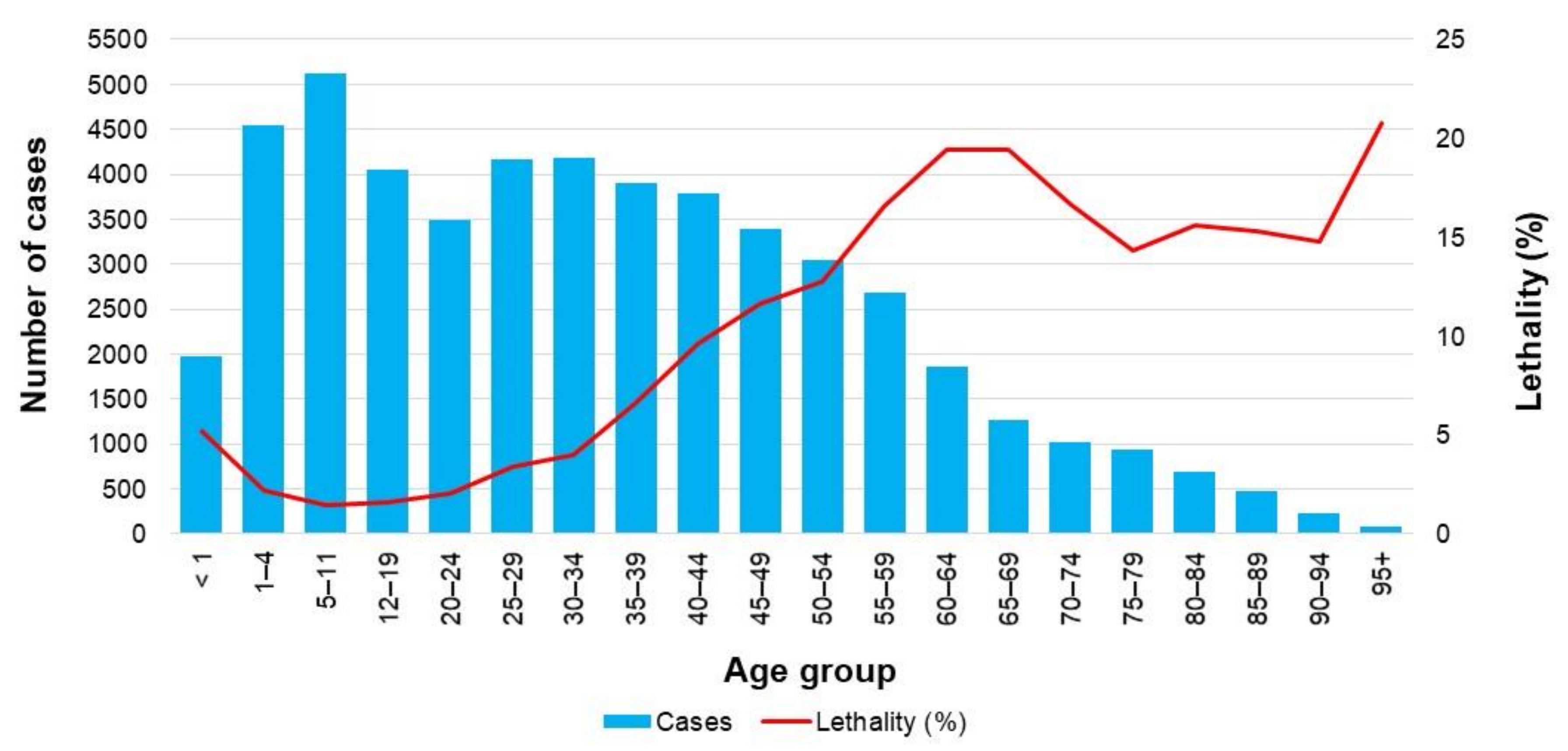
3.3. Deaths and Lethality
3.4. Risk Factors in Influenza Cases and Deaths
3.5. Economic Analysis
4. Discussion
4.1. Major Findings
4.2. Implications and Recommendations for the Health System
4.2.1. Reinforcing the Coverage of Current Policies
4.2.2. Universal Vaccination to Groups Currently Not Covered
4.2.3. Reinforcing Evidence-Based Decision Making
4.3. Limitations
4.4. Relevance of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Molinari, N.A.; Ortega-Sanchez, I.R.; Messonnier, M.L.; Thompson, W.W.; Wortley, P.M.; Weintraub, E.; Bridges, C.B. The annual impact of seasonal influenza in the US: Measuring burden of disease and costs. Vaccine 2007, 25, 5086–5096. [Google Scholar] [CrossRef] [PubMed]
- Savy, V.; Ciapponi, A.; Bardach, A.; Glujovsky, D.; Aruj, P.; Mazzoni, A.; Gibbons, L.; Ortega-Barria, E.; Colindres, R.E. Burden of influenza in Latin America and the Caribbean: A systematic review and meta-analysis. Influenza Other Respir. Viruses 2013, 7, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 21 October 2020).
- Ehreth, J. The global value of vaccination. Vaccine 2003, 21, 596–600. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Available online: http://www.cdc.gov/h1n1flu/highrisk.htm (accessed on 21 October 2020).
- Yang, K.C.; Hung, H.F.; Chen, M.K.; Chen, S.L.; Fann, J.C.; Chiu, S.Y.; Yen, A.M.F.; Huang, K.C.; Chen, H.H.; Wang, S.T.; et al. Cost-effectiveness analysis of universal influenza vaccination: Application of the susceptible-infectious-complication-recovery model. Int. J. Infect. Dis. 2018, 73, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Leidner, A.J.; Murthy, N.; Chesson, H.W.; Biggerstaff, M.; Stoecker, C.; Harris, A.M.; Acosta, A.; Dooling, K.; Bridges, C.B. Cost-effectiveness of adult vaccinations: A systematic review. Vaccine 2019, 37, 226–234. [Google Scholar] [CrossRef]
- Secretaría de Salud [Ministry of Health]. Available online: https://www.gob.mx/salud/articulos/esquema-de-vacunacion (accessed on 21 October 2020). (In Spanish)
- Romero-Martínez, M.; Shamah-Levy, T.; Vielma-Orozco, E.; Heredia-Hernández, O.; Mojica-Cuevas, J.; Cuevas-Nasu, L.; Rivera-Dommarco, J.; Grupo de trabajo Ensanut 2018–19. Encuesta nacional de salud y nutrición 2019–19: Metodología y perspectivas [National health and nutrition survey 2018–19: Methodology and perspectives]. Salud Publica Mex. 2019, 61, 917–923. (In Spanish) [Google Scholar] [CrossRef]
- Mereckiene, J.; Cotter, S.; Nicoll, A.; Lopalco, P.; Noori, T.; Weber, J.; D’Ancona, F.; Levy-Bruhl, D.; Dematte, L.; Giambi, C.; et al. Seasonal influenza immunization in Europe. Overview of recommendations and vaccination coverage for 3 seasons: Pre-pandemic (2008/09), pandemic (2009/10) and post-pandemic (2010/11). Eurosurveillance 2014, 19, 20780. [Google Scholar] [CrossRef] [Green Version]
- Grohskopf, L.A.; Alyanak, E.; Broder, K.R.; Walter, E.B.; Fry, A.M.; Fernigan, D.B. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices–United States, 2019-20 influenza season. MMWR Recomm. Rep. 2019, 68, 121. [Google Scholar] [CrossRef] [Green Version]
- Nichol, K.L. Cost-effectiveness and socio-economic aspects of childhood influenza vaccination. Vaccine 2011, 29, 7554–7558. [Google Scholar] [CrossRef]
- Baguelin, M. Assessing optimal target populations for influenza vaccination programmes: An evidence synthesis and modelling study. PLoS Med. 2013, e1001527. [Google Scholar] [CrossRef]
- Skowronski, D.M.; Leir, S.; De Serres, G.; Murti, M.; Dickinson, J.A.; Winter, A.L.; Olsha, R.; Croxen, M.A.; Drews, S.J.; Charest, H.; et al. Children under 10 years of age were more affected by the 2018/19 influenza A(H1N1)pdm09 epidemic in Canada: Possible cohort effect following the 2009 influenza pandemic. Eurosurveillance 2019, 24, 15. [Google Scholar] [CrossRef]
- Mertz, D.; Kim, T.H.; Johnstone, J.; Lam, P.P.; Science, M.; Kuster, S.P.; Fadel, S.A.; Tran, D.; Fernandez, E.; Bhatnagar, N.; et al. Populations at risk for severe or complicated influenza illness: Systematic review and meta-analysis. BMJ 2013, 347, f5061. [Google Scholar] [CrossRef] [Green Version]
- Petrie, J.G.; Ohmit, S.E.; Cowling, B.J.; Johnson, E.; Cross, R.T.; Malosh, R.E.; Thompson, M.G.; Monto, A.S. Influenza transmission in a cohort of households with children: 2010-2011. PLoS ONE 2013, 8, e75339. [Google Scholar] [CrossRef] [Green Version]
- Weidemann, F.; Remschmidt, C.; Buda, S.; Buchholz, U.; Ultsch, B.; Wichmann, O. Is the impact of childhood influenza vaccination less than expected: A transmission modelling study. BMC Infect. Dis. 2017, 17, 258. [Google Scholar] [CrossRef] [Green Version]
- Pannaraj, P.S.; Want, H.L.; Rivas, H.; Wiryawan, H.; Smit, M.; Green, N.; Aldrovandi, G.M.; El Amin, A.N.; Mascola, L. School-located influenza vaccination decreases laboratory-confirmed influenza and improves school attendance. Clin. Infect. Dis. 2014, 59, 325–332. [Google Scholar] [CrossRef] [Green Version]
- Cowling, B.J.; Chan, K.H.; Feng, S.; Chan, E.L.Y.; Lo, J.Y.C.; Peiris, J.S.M.; Chiu, S.S. The effectiveness of influenza vaccination in preventing hospitalizations in children in Hong Kong, 2009–2013. Vaccine 2014, 32, 5278–5284. [Google Scholar] [CrossRef] [Green Version]
- O’Halloran, A.C.; Lu, P.J.; Williams, W.W.; Bridges, C.B.; Singleton, J.A. Influenza vaccination coverage among people with high-risk conditions in the US. Am. J. Prev. Med. 2016, 50, e15–e26. [Google Scholar] [CrossRef] [Green Version]
- Falcón-Lezama, J.A.; Saucedo-Martínez, R.; Betancourt-Cravioto, M.; Alfaro-Cortes, M.M.; Bahena-González, R.I.; Tapia-Conyer, R. Influenza in the school-aged population in Mexico: Burden of disease and cost-effectiveness of vaccination in children. BMC Infect. Dis. 2020, 20, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Betancourt-Cravioto, M.; Falcón-Lezama, J.A.; Saucedo-Martínez, R.; Alfaro-Cortes, M.M.; Bahena-González, R.I.; Tapia-Conyer, R. Public health and economic benefits of influenza vaccination of the population aged 50 to 59 years without risk factors for influenza complications in Mexico. Vaccines 2021, 9, 188. [Google Scholar] [CrossRef]
- Sistema de Vigilancia Epidemiológica de Influenza SISVEFLU [Influenza Epidemiological Surveillance System SISVEFLU]. Available online: https://www.gob.mx/salud/iner/documentos/formato-sisveflu (accessed on 30 October 2020). (In Spanish).
- Secretaría de Salud–SEED [Ministry of Health–SEED]. Available online: http://www.dgis.salud.gob.mx/contenidos/basesdedatos/std_defunciones_gobmx.html (accessed on 21 October 2020). (In Spanish)
- Secretaría de Salud–SAEH [Ministry of Health–SAEH]. Available online: www.dgis.salud.gob.mx/contenidos/basesdedatos/da_egresoshosp_gobmx.html (accessed on 21 October 2020). (In Spanish)
- Consejo Nacional de Población–CONAPO [National Population Council–CONAPO]. Available online: https://datos.gob.mx/busca/dataset/proyecciones-de-la-poblacion-de-mexico-y-de-las-entidades-federativas-2016-2050 (accessed on 21 October 2020). (In Spanish)
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/flu/about/burden/index.html (accessed on 21 October 2020).
- Dirección General de Epidemiología [General Directorate of Epidemiology]. Available online: https://epidemiologia.salud.gob.mx/gobmx/salud/documentos/manuales/12_Manual_VE_Influenza.pdf (accessed on 30 October 2020). (In Spanish).
- World Health Organization. Available online: https://icd.who.int/browse10/2016/en (accessed on 21 October 2020).
- Ryder, H.F.; McDonough, C.; Tosteson, A.N.A.; Lurie, J.D. Decision analysis and cost-effectiveness analysis. Semin. Spine Surg. 2009, 21, 216–222. [Google Scholar] [CrossRef] [Green Version]
- Secretaría de Salud [Ministry of Health]. Available online: https://ensanut.insp.mx/encuestas/ensanut2018/descargas.php (accessed on 21 October 2020). (In Spanish)
- Secretaría de salud [Ministry of Health]. Available online: http://www.dgis.salud.gob.mx/contenidos/basesdedatos/std_nacimientos_gobmx.html (accessed on 21 October 2020). (In Spanish)
- Institute for Health Metrics and Evaluation (IHME). Available online: http://www.healthdata.org/policy-report/findings-global-burden-disease-study-2017 (accessed on 21 October 2020).
- Secretaría de Hacienda y Crédito Público [Ministry of Finance and Public Credit]. Available online: ppef.hacienda.gob.mx/work/models/PPEF2020/paquete/egresos/Proyecto_Decreto.pdf (accessed on 30 October 2020). (In Spanish)
- WHO Guide to Cost-effectiveness Analysis. Available online: https://www.who.int/choice/publications/p_2003_generalised_cea.pdf (accessed on 11 November 2020).
- Centro Nacional de Excelencia Tecnológica en Salud (CENETEC), Secretaría de Salud [National Center for Technological Excellence in Health (CENETEC), Ministry of Health]. Available online: http://www.cenetec.salud.gob.mx/descargas/gpc/CatalogoMaestro/384_SS_09_influenza_estacional/EyR_SS_384_09.pdf (accessed on 21 October 2020). (In Spanish)
- Campos-Nonato, I.; Hernandez-Barrera, L.; Pedroza-Tobias, A.; Medina, C.; Barquera, S. Hypertension in Mexican adults: Prevalence, diagnosis and type of treatment. Ensanut MC 2016. Salud Publica Mex. 2018, 60, 233–243. [Google Scholar] [CrossRef] [Green Version]
- Basto-Abreu, A.; Barrientos-Gutierrez, T.; Rojas-Martinez, R.; Aguilar-Salinas, C.A.; Lopez-Olmedo, N.; De la Cruz-Gongora, V.; Rivera-Dommarco, J.; Shamah-Levy, T.; Romero-Martinez, M.; Barquera, S.; et al. Prevalence of diabetes and poor glycemic control in Mexico: Results from Ensanut 2016. Salud Publica Mex. 2020, 62, 50–59. [Google Scholar] [CrossRef]
- Nowak, G.J.; Cacciatore, M.A.; Len-Ríos, M.E. Understanding and increasing influenza vaccination acceptance: Insights from a 2016 national survey of US adults. Int. J. Environ. Res. Public Health 2018, 15, 711. [Google Scholar] [CrossRef] [Green Version]
- Nowak, G.J.; Sheedy, K.; Bursey, K.; Smith, T.M.; Basket, M. Promoting influenza vaccination: Insights from a qualitative meta-analysis of 14 years of influenza-related communications research by U.S. Centers for Disease Control and Prevention (CDC). Vaccine 2015, 33, 2741–2756. [Google Scholar] [CrossRef]
- Organización Panamericana de la Salud [Pan American Health Organization]. Available online: https://iris.paho.org/bitstream/handle/10665.2/49179/9789275316320_spa.pdf?sequence=1&isAllowed=y (accessed on 21 October 2020). (In Spanish).
- Danovaro, M.C. Immunization Registries in Latin America and the Caribbean. Pan American Health Organization; World Health Organization. Available online: https://www.who.int/immunization/research/forums_and_initiatives/01_Danovaro_GVIRF14_Concept_Outline_Landscape.pdf?ua=1 (accessed on 13 January 2021).
- Danovaro-Holliday, M.C.; Contreras, M.P.; Pinto, D.; Molina-Aguilera, I.B.; Miranda, D.; García, O.; Velandia-Gonzalez, M. Assessing electronic immunization registries: The Pan American Health Organization experience. Rev. Panam. Salud Publica 2019, 43, e28. [Google Scholar] [CrossRef]
- Tapia-Conyer, R.; Betancourt-Cravioto, M.; Saucedo-Martínez, R.; Motta-Murguía, L.; Gallardo-Rincón, H. Strengthening vaccination policies in Latin America: An evidence-based approach. Vaccine 2013, 31, 3826–3833. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease or Risk Factor | Age Group (Years) | Source of Information for the Estimation of Prevalence |
|---|---|---|
| Diabetes | 20–59 | ENSANUT 2018; self-report of previous medical diagnosis with the following question: 3.1 Has any doctor told you that you are diabetic (or have high blood glucose)? |
| Uncontrolled hypertension | 20–59 | ENSANUT 2018; self-report of previous medical diagnosis with the following question: 4.1 Has any doctor told you that you have hypertension? Determination of uncontrolled hypertension based on blood pressure measurement during the survey under these criteria: systolic blood pressure ≥ 140 mmHg and diastolic blood pressure ≥ 90 mmHg. |
| Morbid obesity | 20–59 | ENSANUT 2018; Body Mass Index (BMI) estimated from weight and height measurements. Morbid obesity is considered as BMI ≥40 kg/m2. |
| Chronic renal failure | 20–59 | ENSANUT 2018; self-report of previous medical diagnosis with the following question: 6.1 Has any doctor ever told you that you have some kind of kidney disease, like kidney failure? |
| Asthma | 5–59 | Global Burden of Disease 2017; prevalence of asthma cases was obtained in 2017. |
| Pregnancy | 15–49 | SINAC 2017; total number of live births in 2017 was considered (latest year of available data) as proxy for pregnancy during the period of interest. |
| Age Group (Years) | Diabetes | Uncontrolled Hypertension | Morbid Obesity | Chronic Renal Failure | Asthma | Pregnancy |
|---|---|---|---|---|---|---|
| 5–9 | ND | ND | ND | ND | 6.5 | ND |
| 10–14 | ND | ND | ND | ND | 4.5 | ND |
| 15–19 | ND | ND | ND | ND | 4.5 | 397,395 |
| 20–24 | 0.4 | 1.1 | 3.35 | 0.3 | 4.1 | 604,429 |
| 25–29 | 0.7 | 0.8 | 4.90 | 0.4 | 2.6 | 514,830 |
| 30–34 | 2.0 | 1.8 | 4.94 | 0.3 | 2.2 | 342,685 |
| 35–39 | 4.4 | 2.7 | 6.30 | 1.1 | 2.3 | 163,567 |
| 40–44 | 7.3 | 5.4 | 6.10 | 0.5 | 2.3 | 38,175 |
| 45–49 | 10.1 | 8.0 | 4.83 | 0.7 | 2.2 | 3419 |
| 50–54 | 16.9 | 12.0 | 6.96 | 0.7 | 2.2 | ND |
| 55–59 | 19.4 | 12.8 | 6.40 | 1.4 | 2.3 | ND |
| Total | 6.7 | 5.1 | 5.3 | 1.0 | 3.2 | 2,064,500 |
| Scenario | No Medical Care | Outpatient Only | Hospitalization: Referred from Outpatient Clinic | Hospitalization: Admitted through ER | ||||
|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| Health Outcome | Not Demanding Medical Care | Outpatient Only | Hospitalization | Outpatient | Hospitalization | |||
| Discharge | Death | Non- Severe | Severe | Death | ||||
| Clinical Diagnosis | ||||||||
| Outpatient consultations 1 | 1 | 1 | 1 | |||||
| ER consultations 1 | 1 | 1 | 1 | 1 | ||||
| PCR 1 | 0.1 | 0.1 | 0.1 | 1 | 1 | 1 | 1 | |
| Direct costs | ||||||||
| Outpatient consultations 1 | 1 | |||||||
| Specialist consultations 1 | 2 | 3 | 1 | 2 | 3 | 4 | ||
| Amantadine 2 | 1 | |||||||
| Oseltamivir 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Paracetamol 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Bacteriologic culture 2 | 1 | 1 | 1 | 1 | 1 | |||
| Ceftriaxone 2 | 1 | 1 | 1 | 1 | 1 | |||
| Hospitalization days | 1 | 8.3 | 2 | 8.3 | 12.45 | 8.3 | ||
| Indirect costs | ||||||||
| Medical disability days | 3 | 8 | 5 | 15 | 26 | |||
| Years of life lost 3 | X | X | ||||||
| Unit Cost | 2009–2010 | 2010–2011 | 2011–2012 | 2012–2013 | 2013–2014 | 2014–2015 | 2015–2016 | 2016–2017 | 2017–2018 |
|---|---|---|---|---|---|---|---|---|---|
| Outpatient consultations | 331.74 | 323.79 | 332.10 | 345.34 | 356.53 | 367.07 | 384.25 | 416.33 | 443.64 |
| Specialist consultations | 528.72 | 512.30 | 524.01 | 544.56 | 561.67 | 578.31 | 606.14 | 657.76 | 701.45 |
| ER consultations | 362.78 | 363.93 | 375.38 | 389.29 | 403.43 | 414.65 | 429.28 | 459.08 | 484.20 |
| Hospitalization days | 3147.49 | 3040.89 | 3112.41 | 3240.17 | 3340.33 | 3441.46 | 3618.09 | 3939.79 | 4214.67 |
| Amantadine | 32.95 | 34.07 | 35.47 | 36.82 | 38.30 | 39.34 | 40.45 | 42.90 | 45.00 |
| Oseltamivir | 81.18 | 83.94 | 87.40 | 90.72 | 94.37 | 96.94 | 99.67 | 105.69 | 110.87 |
| Paracetamol | 2.82 | 2.86 | 2.96 | 3.06 | 3.18 | 3.26 | 3.35 | 3.56 | 3.73 |
| Ceftriaxone | 8.37 | 8.61 | 8.95 | 9.30 | 9.66 | 9.93 | 10.22 | 10.86 | 11.40 |
| PCR | 1576.29 | 1641.95 | 1712.28 | 1776.73 | 1849.83 | 1899.51 | 1948.37 | 2059.96 | 2155.92 |
| Bacteriologic culture | 147.42 | 152.44 | 158.71 | 164.75 | 171.37 | 176.03 | 181.00 | 191.94 | 201.34 |
| Disease or Risk Factor | Age Group (Years) | Source of Information for Estimation of Immunization Coverage |
|---|---|---|
| Diabetes | 20–59 | ENSANUT 2018; vaccine application self-report in the 2018–2019 season or vaccine application registered in the immunization card between September 2018 and date of survey |
| Uncontrolled hypertension | 20–59 | ENSANUT 2018; vaccine application self-report in the 2018–2019 season or vaccine application registered in the immunization card between September 2018 and date of survey |
| Morbid obesity | 20–59 | ENSANUT 2018; vaccine application self-report in the 2018–2019 season or vaccine application registered in the immunization card between September 2018 and date of survey |
| Chronic renal failure | 20–59 | ENSANUT 2018; vaccine application self-report in the 2018–2019 season or vaccine application registered in the immunization card between September 2018 and date of survey |
| Pregnancy | 15–49 | ENSANUT 2018; vaccine application self-report in the 2018–2019 season or vaccine application registered in the immunization card between September 2018 and date of survey |
| Asthma | 5–59 | ENSANUT 2018; vaccine application self-report in the 2018–2019 season or vaccine application registered in the immunization card between September 2018 and date of survey. As the survey does not include information on asthma, national prevalence was considered for this purpose |
| Age Group (Years) | Diabetes | Uncontrolled Hypertension | Morbid Obesity | Chronic Renal Failure | Asthma | Pregnancy |
|---|---|---|---|---|---|---|
| 5–9 | ND | ND | ND | ND | 26.83 | ND |
| 10–14 | ND | ND | ND | ND | 26.83 | ND |
| 15–19 | ND | ND | ND | ND | 26.83 | 14.6 |
| 20–24 | 34.8 | 22.2 | 19.4 | 19.3 | 26.83 | 14.6 |
| 25–29 | 35.7 | 26.2 | 47.6 | 35.6 | 28.66 | 10.6 |
| 30–34 | 35.2 | 33.8 | 30.8 | 34.7 | 27.00 | 9.3 |
| 35–39 | 33.6 | 35.2 | 23.8 | 26.7 | 28.35 | 7.2 |
| 40–44 | 33.5 | 29.2 | 38.2 | 35.2 | 25.45 | 9.4 |
| 45–49 | 36.0 | 40.3 | 23.7 | 39.0 | 27.40 | 6.6 |
| 50–54 | 33.3 | 27.2 | 25.1 | 28.6 | 27.25 | ND |
| 55–59 | 38.6 | 33.0 | 35.9 | 49.5 | 28.44 | ND |
| Total | 35.3 | 32.1 | 30.7 | 34.9 | 27.4 | 9.1 |
| Risk Factor | Diabetes | Uncontrolled Hypertension | Morbid Obesity | Chronic renal Failure | Asthma | Pregnancy |
|---|---|---|---|---|---|---|
| Current estimated vaccination coverage (%) 1 | 35.3 | 32.1 | 30.7 | 34.9 | 27.4 | 9.1 |
| Prevented influenza cases | 82,590 | 65,146 | 65,362 | 7142 | 70,839 | 50,781 |
| Prevented deaths | 12.8 | 10.4 | 19.4 | 5.1 | 1.7 | 1.1 |
| Associated events | ||||||
| Healthcare visits | 92,887 | 73,787 | 75,201 | 7615 | 79,636 | 54,521 |
| ER admissions | 32,096 | 22,696 | 19,474 | 2886 | 22,539 | 20,759 |
| Hospitalization | 32,210 | 22,791 | 19,549 | 2891 | 22,571 | 20,955 |
| Age Group (Years) | Total Population 2018–2019 | Estimated Prevalence | Population with Risk Factor | Incidence of Influenza (per 100,000) | Estimated Cases of Influenza | Estimated Cases of Influenza with Current Vaccination Coverage | Estimated Cases of Influenza with 75% Vaccination Coverage | Differential of Estimated Cases of Influenza Averted |
|---|---|---|---|---|---|---|---|---|
| 20–24 | 10,803,051 | 0.4 | 43,212 | 7050.5 | 3047 | 2509 | 1904 | 605 |
| 25–29 | 10,174,627 | 0.7 | 71,222 | 7050.5 | 5022 | 4135 | 3138 | 997 |
| 30–34 | 9,367,670 | 2 | 187,353 | 7050.5 | 13,209 | 10,878 | 8256 | 2622 |
| 35–39 | 8,848,819 | 4.4 | 389,348 | 7050.5 | 27,451 | 22,606 | 17,157 | 5449 |
| 40–44 | 8,391,604 | 7.3 | 612,587 | 7050.5 | 43,191 | 35,567 | 26,994 | 8573 |
| 45–49 | 7,678,041 | 10.1 | 775,482 | 7050.5 | 54,675 | 45,025 | 34,172 | 10,853 |
| 50–54 | 6,617,806 | 16.9 | 1,118,409 | 12,382.1 | 138,483 | 114,041 | 86,552 | 27,489 |
| 55–59 | 5,453,295 | 19.4 | 1,057,939 | 12,382.1 | 130,995 | 107,875 | 81,872 | 26,003 |
| Total | 67,334,913 | 4,255,554 | 416,073 | 342,636 | 260,046 | 82,590 |
| Age Group (Years) | Total Population 2018–2019 | Estimated Prevalence | Population with Risk Factor | Incidence of Influenza (per 100,000) | Estimated Cases of Influenza | Estimated Cases of Influenza with Current Vaccination Coverage | Estimated Cases of Influenza with 75% Vaccination Coverage | Differential of Estimated Cases of Influenza Averted |
|---|---|---|---|---|---|---|---|---|
| 20–24 | 10,803,051 | 1.1 | 121,913 | 7050.5 | 8595 | 7216 | 5372 | 1844 |
| 25–29 | 10,174,627 | 0.8 | 84,695 | 7050.5 | 5971 | 5013 | 3732 | 1281 |
| 30–34 | 9,367,670 | 1.8 | 170,517 | 7050.5 | 12,022 | 10,093 | 7514 | 2579 |
| 35–39 | 8,848,819 | 2.7 | 240,861 | 7050.5 | 16,982 | 14,256 | 10,614 | 3643 |
| 40–44 | 8,391,604 | 5.4 | 450,734 | 7050.5 | 31,779 | 26,679 | 19,862 | 6817 |
| 45–49 | 7,678,041 | 8.0 | 613,430 | 7050.5 | 43,250 | 36,308 | 27,031 | 9277 |
| 50–54 | 6,617,806 | 12.0 | 796,414 | 12,382.1 | 98,613 | 82,786 | 61,633 | 21,152 |
| 55–59 | 5,453,295 | 12.8 | 698,582 | 12,382.1 | 86,499 | 72,616 | 54,062 | 18,554 |
| Total | 67,334,913 | 3,177,147 | 303,713 | 254,967 | 189,820 | 65,146 |
| Age Group (Years) | Total Population 2018–2019 | Estimated Prevalence | Population with Risk Factor | Incidence of Influenza (per 100,000) | Estimated Cases of Influenza | Estimated Cases of Influenza with Current Vaccination Coverage | Estimated cases of Influenza with 75% Vaccination Coverage | Differential of Estimated Cases of Influenza Averted |
|---|---|---|---|---|---|---|---|---|
| 20–24 | 10,803,051 | 3.3 | 361,875 | 7050.5 | 25,514 | 21,598 | 15,946 | 5651 |
| 25–29 | 10,174,627 | 4.9 | 498,108 | 7050.5 | 35,119 | 29,728 | 21,949 | 7779 |
| 30–34 | 9,367,670 | 4.9 | 462,805 | 7050.5 | 32,630 | 27,621 | 20,394 | 7228 |
| 35–39 | 8,848,819 | 6.3 | 557,588 | 7050.5 | 39,313 | 33,278 | 24,571 | 8708 |
| 40–44 | 8,391,604 | 6.1 | 511,642 | 7050.5 | 36,073 | 30,536 | 22,546 | 7990 |
| 45–49 | 7,678,041 | 4.8 | 370,726 | 7050.5 | 26,138 | 22,126 | 16,336 | 5790 |
| 50–54 | 6,617,806 | 7.0 | 460,768 | 12,382.1 | 57,053 | 48,295 | 35,658 | 12,637 |
| 55–59 | 5,453,295 | 6.4 | 349,276 | 12,382.1 | 43,248 | 36,609 | 27,030 | 9579 |
| Total | 67,334,912 | - | 3,572,788 | - | 295,088 | 249,792 | 184,430 | 65,362 |
| Age Group (Years) | Total Population 2018–2019 | Estimated Prevalence | Population with Risk Factor | Incidence of Influenza (per 100,000) | Estimated Cases of Influenza | Estimated Cases of Influenza with Current Vaccination Coverage | Estimated Cases of Influenza with 75% Vaccination Coverage | Differential of Estimated Cases of Influenza Averted |
|---|---|---|---|---|---|---|---|---|
| 20–24 | 10,803,051 | 0.3 | 27,008 | 7050.5 | 1904 | 1572 | 1190 | 382 |
| 25–29 | 10,174,627 | 0.4 | 40,699 | 7050.5 | 2869 | 2369 | 1793 | 575 |
| 30–34 | 9,367,670 | 0.3 | 30,913 | 7050.5 | 2180 | 1799 | 1362 | 437 |
| 35–39 | 8,848,819 | 1.1 | 93,797 | 7050.5 | 6613 | 5459 | 4133 | 1326 |
| 40–44 | 8,391,604 | 0.5 | 41,119 | 7050.5 | 2899 | 2393 | 1812 | 581 |
| 45–49 | 7,678,041 | 0.7 | 54,514 | 7050.5 | 3844 | 3173 | 2402 | 771 |
| 50–54 | 6,617,806 | 0.7 | 48,972 | 12,382.1 | 6064 | 5006 | 3790 | 1216 |
| 55–59 | 5,453,295 | 1.4 | 74,710 | 12,382.1 | 9251 | 7636 | 5782 | 1855 |
| Total | 67,334,913 | 411,732 | 35,624 | 29,407 | 22,264 | 7143 |
| Age Group (Years) | Total Population 2018–2019 | Estimated Prevalence | Population with Risk Factor | Incidence of Influenza (per 100,000) | Estimated Cases of Influenza | Estimated Cases of Influenza with Current Vaccination Coverage | Estimated Cases of Influenza with 75% Vaccination Coverage | Differential of Estimated Cases of Influenza Averted |
|---|---|---|---|---|---|---|---|---|
| 5–9 | 11,045,962 | 6.5 | 718,259 | 9602.7 | 68,972 | 59,523 | 43,108 | 16,415 |
| 10–14 | 11,131,856 | 4.5 | 500,934 | 9602.7 | 48,103 | 41,513 | 30,065 | 11,449 |
| 15–19 | 11,048,379 | 4.5 | 497,177 | 8581.8 | 42,667 | 36,822 | 26,667 | 10,155 |
| 20–24 | 10,803,051 | 4.1 | 437,842 | 7050.5 | 30,870 | 26,641 | 19,294 | 7347 |
| 25–29 | 10,174,627 | 2.6 | 266,005 | 7050.5 | 18,755 | 16,185 | 11,722 | 4464 |
| 30–34 | 9,367,670 | 2.2 | 207,886 | 7050.5 | 14,657 | 12,649 | 9161 | 3488 |
| 35–39 | 8,848,819 | 2.3 | 201,870 | 7050.5 | 14,233 | 12,283 | 8896 | 3387 |
| 40–44 | 8,391,604 | 2.3 | 190,837 | 7050.5 | 13,455 | 11,612 | 8409 | 3202 |
| 45–49 | 7,678,041 | 2.2 | 168,602 | 7050.5 | 11,887 | 10,259 | 7430 | 2829 |
| 50–54 | 6,617,806 | 2.2 | 147,531 | 12,382.1 | 18,267 | 15,765 | 11,417 | 4348 |
| 55–59 | 5,453,295 | 2.3 | 127,417 | 12,382.1 | 15,777 | 13,616 | 9861 | 3755 |
| Total | 100,561,110 | 3,464,359 | 297,644 | 256,867 | 186,027 | 70,839 |
| Age Group (Years) | Total Population 2018–2019 | Estimated Prevalence | Population with Risk Factor | Incidence of Influenza (per 100,000) | Estimated Cases of Influenza | Estimated Cases of Influenza with Current Vaccination Coverage | Estimated cases of Influenza with 75% Vaccination Coverage | Differential of Estimated Cases of Influenza Averted |
|---|---|---|---|---|---|---|---|---|
| 15–19 | 11,048,379 | – | 361,192 | 8581.8 | 30,997 | 29,587 | 19,373 | 10,213 |
| 20–24 | 10,803,051 | – | 611,532 | 7050.5 | 43,116 | 41,154 | 26,948 | 14,207 |
| 25–29 | 10,174,627 | – | 542,570 | 7050.5 | 38,254 | 36,513 | 23,909 | 12,605 |
| 30–34 | 9,367,670 | – | 363,084 | 7050.5 | 25,599 | 24,435 | 16,000 | 8435 |
| 35–39 | 8,848,819 | – | 180,244 | 7050.5 | 12,708 | 12,130 | 7943 | 4187 |
| 40–44 | 8,391,604 | – | 45,105 | 7050.5 | 3180 | 3035 | 1988 | 1048 |
| 45–49 | 7,678,041 | – | 3682 | 7050.5 | 260 | 248 | 162 | 86 |
| Total | 66,312,191 | – | 2,107,409 | – | 154,114 | 147,102 | 96,321 | 50,781 |
| Costs | Diabetes | Uncontrolled Hypertension | Morbid Obesity | Chronic Renal Failure | Asthma | Pregnancy |
|---|---|---|---|---|---|---|
| Direct costs | ||||||
| Diagnosis | −4.10 | −2.95 | −2.60 | −0.36 | −1.75 | −2.97 |
| Healthcare visits | −3.79 | −2.87 | −2.75 | −0.32 | −1.76 | −2.98 |
| Medications | −0.41 | −0.32 | −0.32 | −0.04 | −0.20 | −0.35 |
| Hospitalizations | −33.06 | −23.06 | −19.85 | −2.66 | −13.01 | −22.08 |
| Vaccination | 5.52 | 4.45 | 5.17 | 0.54 | 3.53 | 5.39 |
| Direct costs subtotal | −35.84 | −24.75 | −20.35 | −2.84 | −13.19 | −22.99 |
| Indirect costs | ||||||
| Sick leave | −7.47 | −5.44 | −4.98 | −0.60 | −3.15 | −5.35 |
| Premature death | −1.14 | −0.93 | −1.85 | −0.46 | −0.09 | −0.16 |
| Indirect costs subtotal | −8.61 | −6.37 | −6.83 | −1.06 | −3.24 | −5.51 |
| Total costs | −44.45 | −31.12 | −27.18 | −3.90 | −16.43 | −28.5 |
| 5–11 Years | 50–59 Years | Total | |
|---|---|---|---|
| Preventions | |||
| Influenza cases | 671,461 | 199,500 | 870,961 |
| Deaths | 15 | 12 | 27 |
| Events associated with preventable cases | |||
| Healthcare visits | 262,812 | 120,798 | 383,610 |
| ER admission | 154,143 | 33,024 | 187,167 |
| Hospitalization | 97,637 | 33,091 | 130,728 |
| Net costs | |||
| Direct costs | |||
| Diagnosis | −13.27 | −4.37 | −17.64 |
| Healthcare visits | −14.58 | −4.48 | −19.06 |
| Medications | −2.59 | −0.77 | −3.36 |
| Hospitalizations | −93.51 | −41.66 | −135.17 |
| Vaccination | 27.42 | 10.53 | 37.95 |
| Direct costs subtotal | −96.53 | −40.75 | −137.28 |
| Indirect costs | |||
| Sick leave | −14.43 | −8.07 | −22.50 |
| Premature death | −1.03 | −0.99 | −2.02 |
| Indirect costs subtotal | −15.46 | −9.06 | −24.52 |
| Total costs | −111.99 | −49.81 | −161.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tapia-Conyer, R.; Betancourt-Cravioto, M.; Montoya, A.; Falcón-Lezama, J.A.; Alfaro-Cortes, M.M.; Saucedo-Martínez, R. A Call for a Reform of the Influenza Immunization Program in Mexico: Epidemiologic and Economic Evidence for Decision Making. Vaccines 2021, 9, 286. https://doi.org/10.3390/vaccines9030286
Tapia-Conyer R, Betancourt-Cravioto M, Montoya A, Falcón-Lezama JA, Alfaro-Cortes MM, Saucedo-Martínez R. A Call for a Reform of the Influenza Immunization Program in Mexico: Epidemiologic and Economic Evidence for Decision Making. Vaccines. 2021; 9(3):286. https://doi.org/10.3390/vaccines9030286
Chicago/Turabian StyleTapia-Conyer, Roberto, Miguel Betancourt-Cravioto, Alejandra Montoya, Jorge Abelardo Falcón-Lezama, Myrna María Alfaro-Cortes, and Rodrigo Saucedo-Martínez. 2021. "A Call for a Reform of the Influenza Immunization Program in Mexico: Epidemiologic and Economic Evidence for Decision Making" Vaccines 9, no. 3: 286. https://doi.org/10.3390/vaccines9030286