An Acquaintance with An Aging Society


1
Organization for Co-Creation Research and Social Contributions, Nagoya Institute of Technology, Gokiso-chou, Showa-ku, Nagoya, Aichi 466-8555, Japan
2
Liaison Office, Innovation Center for Clinical Research, National Center for Geriatrics and Gerontology, Morioka-chou 7-430, Obu, Aichi 474-8511, Japan
Soc. Sci. 2019, 8(4), 110; https://doi.org/10.3390/socsci8040110
Submission received: 31 January 2019
/
Revised: 3 March 2019
/
Accepted: 29 March 2019
/
Published: 3 April 2019
Abstract
:Low birth rates and higher life expectancy have been ravaging Japanese society. This article summarizes some of the latest medical knowledge and assistive activities, with a nod toward one nonprofit organization’s efforts to deliver better home healthcare to the elderly through housing and technologies, in the world’s first super-aging society. The response to the transforming society requires a combination of familiar customs and new technologies that create a favorable environment for mobility and continuous learning that are key to elderly health. As other countries will face similar issues, further international interdisciplinary knowledge-building will be necessary to face the challenges of super-aging societies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Japan’s Super-Aging Society
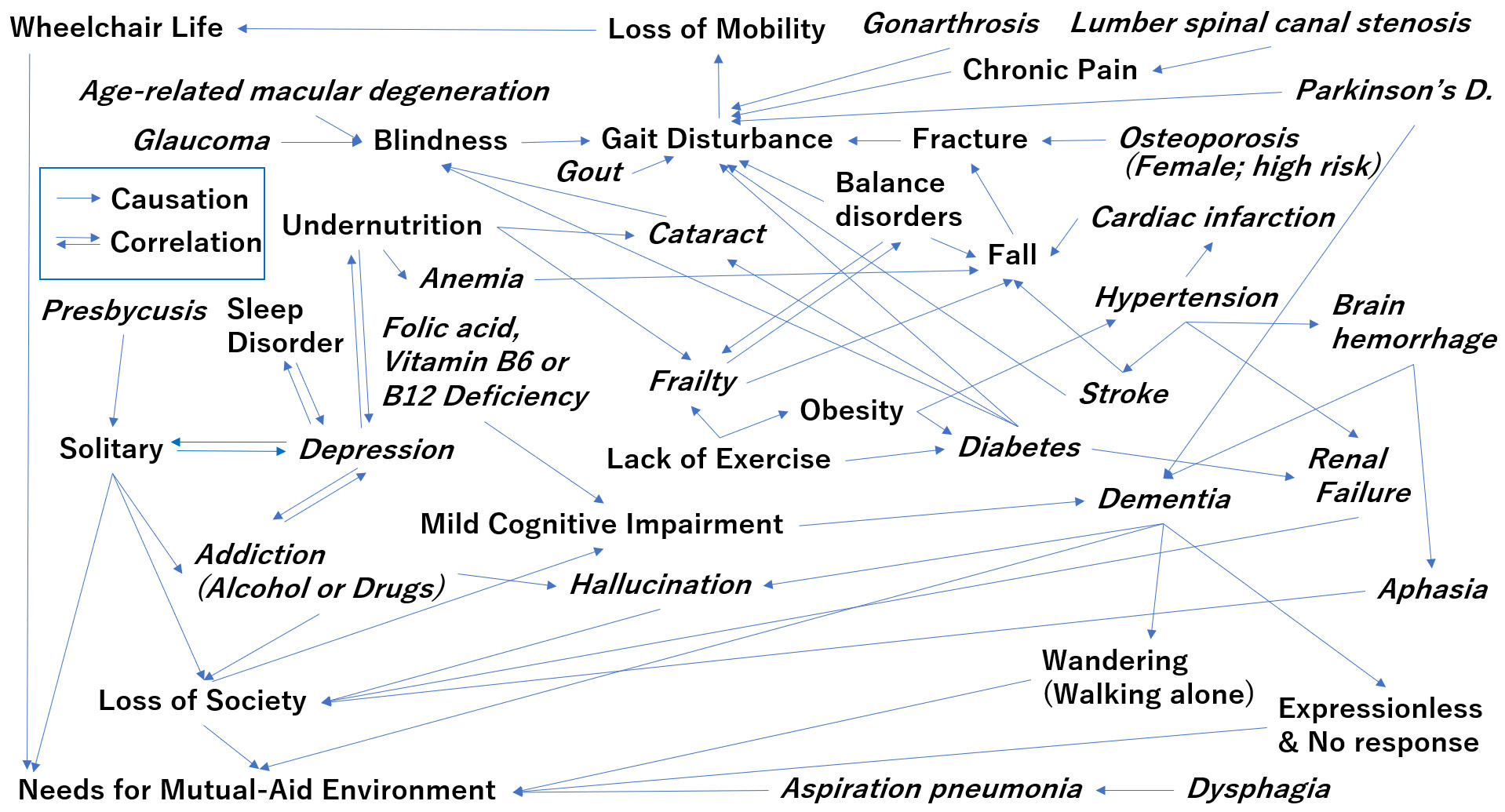
According to an announcement from the Statistics Bureau of Japan (SBJ) on 30 November 2018, Japan’s total population decreased by a record 0.21 percent to 126.44 million (provisional estimates) as of 1 October 2018; meanwhile, the population of those aged 65 years and above surpassed the 35 million mark for the first time—an increase of 468,000 (1.34%) over the previous year (Ministry of Internal Affairs and Communications Statistics Bureau, Japan 2018). According to the United Nations, Japan was already the oldest country in the world, as shown in Figure 1, which lists those countries in the world with the highest life expectancy ten years before and after 2015 (United Nations, Department of Economic and Social Affairs, Population Division 2017). Low birth rates and higher life expectancy resulted in Japan becoming a super-aging society, and its population started declining in 2017.
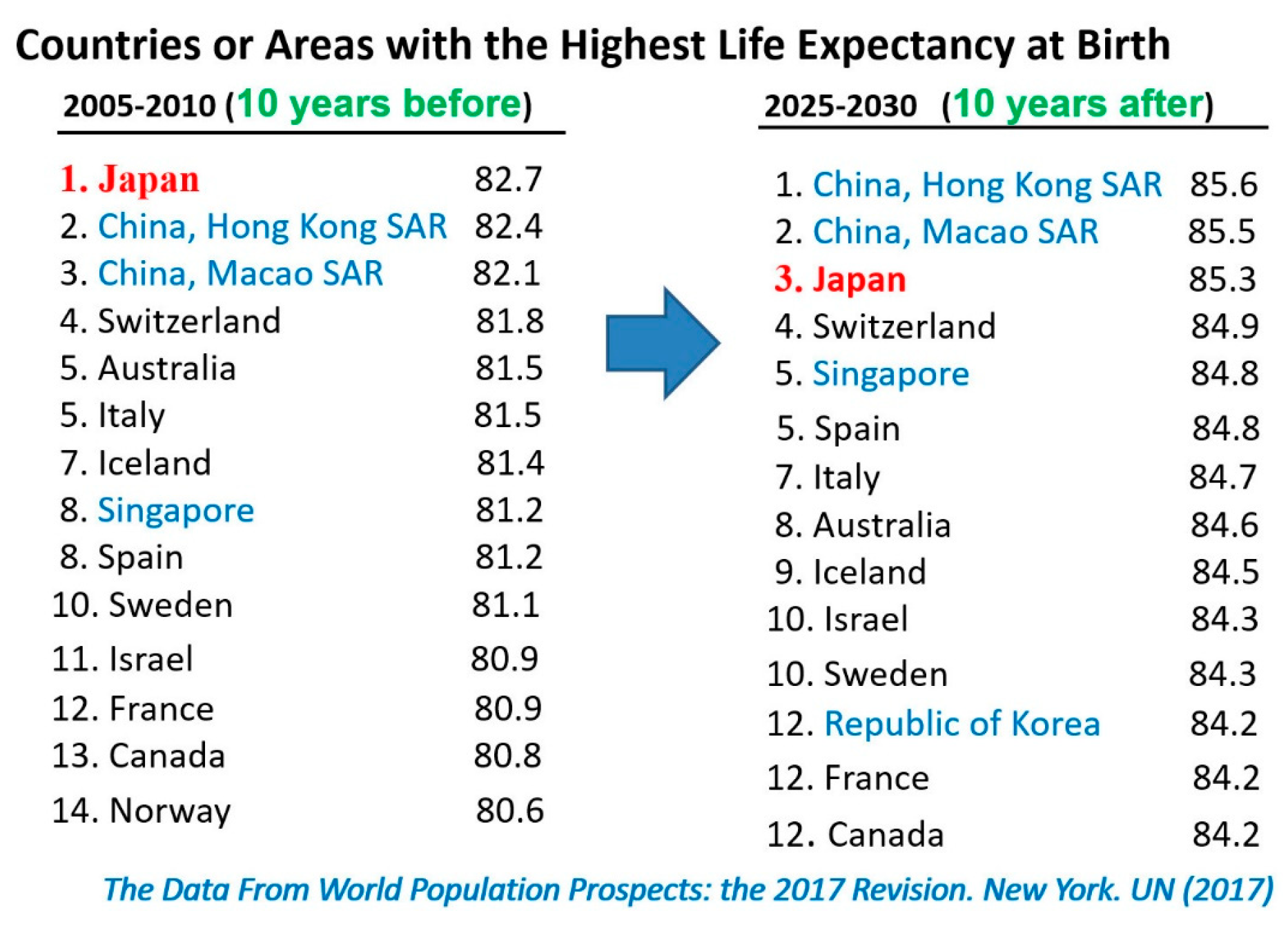
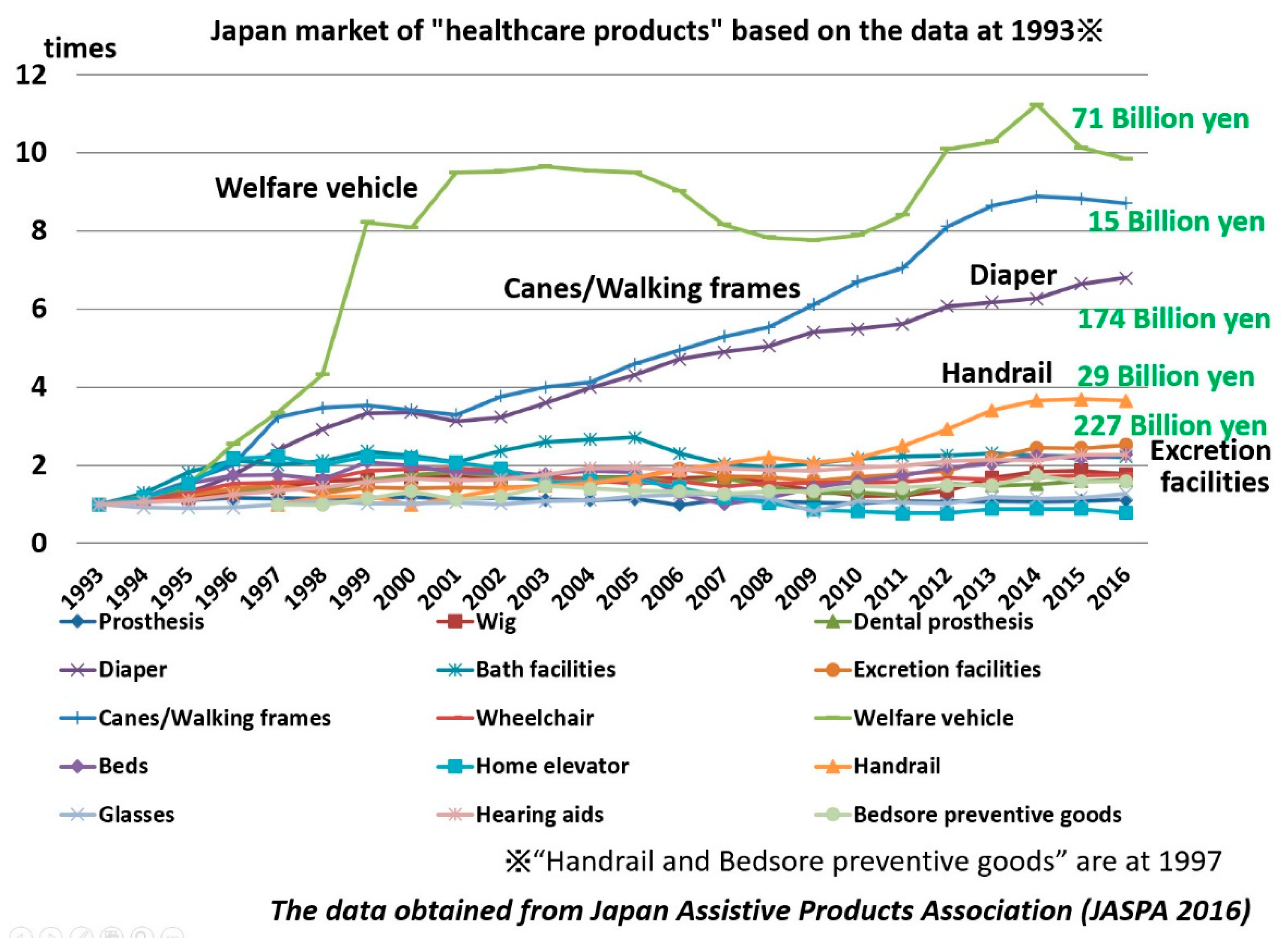
Figure 2 shows developing markets stimulated by Japan’s aging society, using data obtained from a 2016 report from the Japan Assistive Products Association, which took over this duty from Japan’s Ministry of Health, Labour and Welfare in 2003. While the market for products that assist the mobility of the elderly has surged since 1993—welfare vehicles, canes and walking frames, diapers, and handrails—the market for all other welfare products has grown 2.5-fold since 1993. Across Japan today, it is common to see people walking with their canes, often dressed in colorful clothes for high visibility.
The super-aging society is transforming Japan. Local governments, following policies based on “The Basic Law on Measures for the Aging Society” (Law No. 129, 1995), identify three components with towns: administrative organs, companies, and citizens (Cabinet Office 1995). Although companies have long been developing healthcare products for the elderly, as shown in Figure 2, the cry for more innovation in and access to such products and other forms of aid went largely unheeded until the sizable profit potential became clear.
2. Sawayaka-Aichi: Mutual-Aid Activities 24 Hours and 365 Days
In 1994, one nonprofit organization (NPO), Sawayaka-Aichi, began to carry out “mutual-aid activities in 24 h of 365 days” for the elderly, disabled, and families facing age-related challenges. Sawayaka-Aichi has developed its services to provide assistance all day, every day for those in need. Sawayaka-Aichi’s president, Satomi Kawakami, has earned an award for her efforts, honored as “Social Entrepreneur of the Year in Japan 2010” by the Institute for Strategic Leadership (ISL) Center for Social Innovation and the Schwab Foundation for Social Entrepreneurship. Today, Sawayaka-Aichi provides many services (see Figure 3), with about 350 helpers supporting 850 elderly and disabled people, and families facing problems, regardless of age and gender.
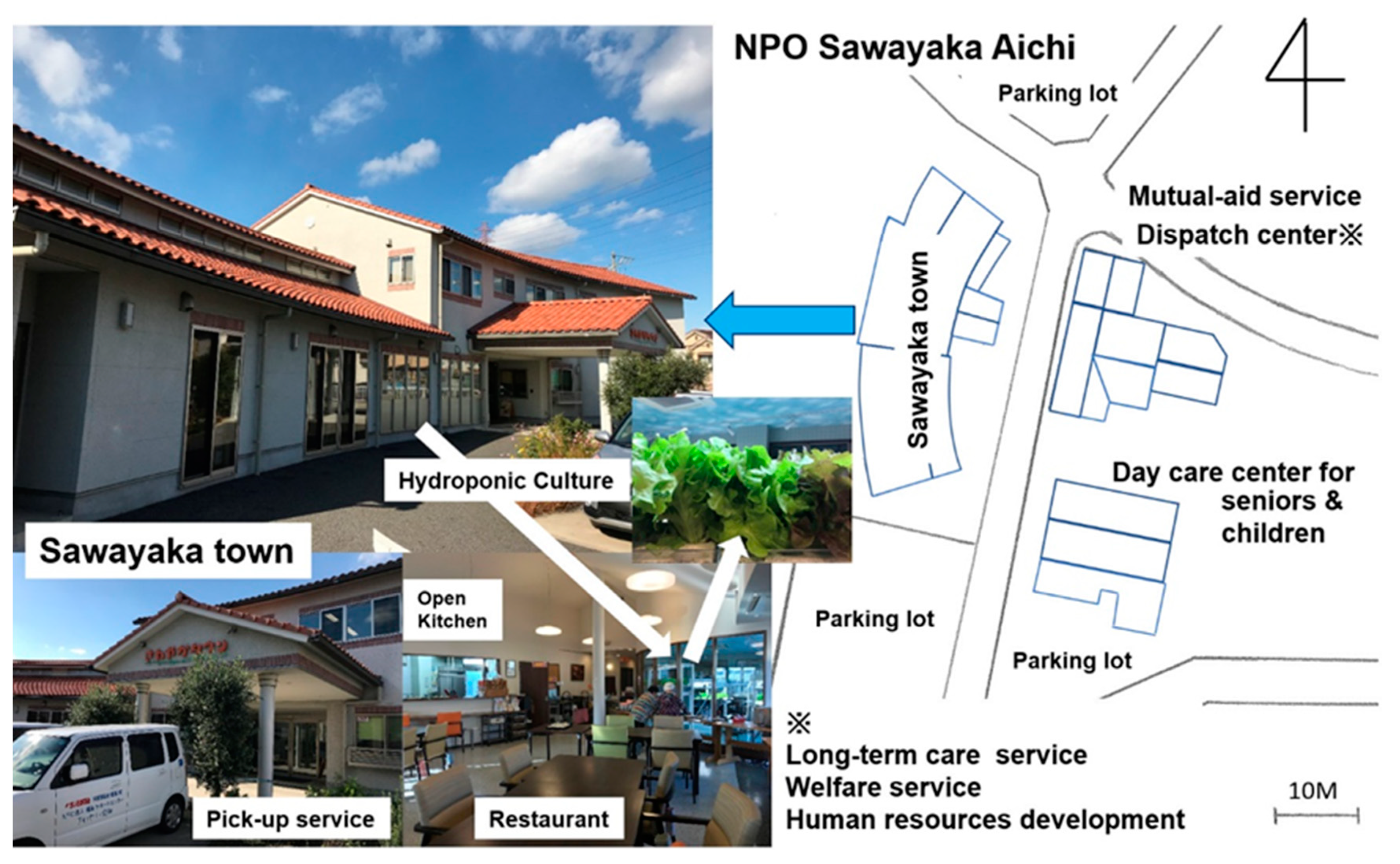
Sawayaka-Aichi means Fresh Aichi, and Aichi is the local prefecture name. Basically, the organization is committed to supporting most people’s desire to remain living at home. Their services include disabled welfare services, nursing in-home care services (including preventive care), nursing care insurance services (e.g., day care, in-home nursing care support), and an independent service of training courses for improved nursing skills. In addition to its “mutual-aid activities in 24 h of 365 days,” Sawayaka Town can also provide meals, health, and leisure activities (see Figure 4).
As Ms. Kawakami explains, Sawayaka-Aichi’s 24/7 “mutual aid” involves both the organization’s dedicated helpers and other users of the services. Anyone can be trained to assist, so there are some people—even those in their 80s—who are both elderly or disabled users and helpers. Helpers want to do “mutual-aid activities” in their local area, and the surrounding dwellers love the organization because it gives them a sense of community and the security of knowing that they can call for assistance at any time, as well as provide assistance to others. Helpers travel to the dwellers’ homes and assist with tasks and services such as spending time with someone who lives alone, taking someone shopping, stepping in to help family and others when someone is hospitalized, watering a garden, cleaning, and so on. On some occasions, helpers also respond to midnight calls to care for children when their parents are suffering from the flu. Sawayaka-Aichi recommends triangular relationships over bidirectional relationships to spread and strengthen the assistance network: thus, Resident A might be a helper for Resident B, Resident A might have the help of Resident C at another time, and Resident B might help Resident C with something else.
Key to the operations of Sawayaka-Aichi is the welfare complex, Sawayaka Town, with an age- and disability-friendly environment created to provide prevention, rehabilitation, and care for geriatric diseases (see Figure 4). Although much of the assistance takes place in users’ homes, having this welfare-oriented campus means that families can leave a parent with dementia or mobility issues at Sawayaka Town, where they will be accompanied by at least one helper at all times. The fan-shape of the building provides a change of view while the users enjoy walking indoors at “Sawayaka Town.” Additionally, the fan-shaped structure helps those with weakening visual acuity, early symptoms of glaucoma (which affects peripheral vision first), and slight cerebral infarction, making it easier for helpers to spot the symptoms than at the person’s home or in a straight hallway.
One woman said that she enjoyed having one last lunch with her late father in Sawayaka Town. To avoid dysphagia, heat-processed vegetables are frequently served instead of fresh vegetables in general facilities for the elderly. However, Sawayaka Town has hydroponic cultivation facilities for growing leaf lettuce varieties with very short fibers that are easier for the elderly to eat, and its restaurant has a fresh leaf lettuce buffet. Sawayaka-Aichi is committed to supporting people’s preference for living at home, but its campus offers complementary services such as restaurant services, bath services, and leisure services to maintain the precious aspects of daily life for dwellers to keep them as happy, healthy, and independent as possible. Ms. Kawakami recognizes that activities now handled almost exclusively by staff and helpers at Sawayaka Town will be substantially enhanced by technology and the Internet of Things (IoT), as robots and robotic assistance can provide additional support to the aging society’s worsening manpower shortage.
3. Architecture as Part of the Culture
“What of modern man’s scale of values?” asked Alvar Aalto, a well-known Finnish architect, in a 1927 article of the newspaper Turun Sanomat (Mizusawa et al. 2018). This question still echoes in the aging societies our countries face, with our growing need for age-friendly environments. The function of buildings has always been to allow people to live comfortably and safely. However, there has never been a strong element of the kinds of assistive support or accommodations necessary in aging societies.
Frank Lloyd Wright, one of America’s most famous architects, said that Chinese philosopher Laotze had expressed the truth of achievement in architecture when Laotze had declared “the reality of the building does not consist in the roof and walls but in the space within to be lived in” (Wright 1957; Laotze 2008). Wright added to Laotze’s wise words that modern machine masters were ruling man’s fate in his manufactured goods as well as in his architecture and arts (Wright 1957).
Le Corbusier, a famous Swiss-French architect who studied human proportions and the logic of machines, made extensive use of the “basic box” and concentrated on inventive ways to arrange interior spaces (Taylor et al. 1991). He believed that architecture must foster ecological stewardship by nurturing the individual, the community, and the earth for the future (Taylor 2009). Buildings connect everyone—citizens, medical professionals, patients, parents, children—to the surrounding environments and affect them. In other words, architecture that is designed for human beings within their environments, often using state-of-the-art materials and technologies, is the best medium to show the shapes of nature, life, and the arts of the times.
Japanese architect Tadao Andō was fascinated by Le Corbusier’s architecture in his youth, and he later declared “Architecture continues to be an integral part of culture, which is the driving force of human history” and “If buildings are to be created for those imperfect beings full of contradictions, then ideas born of flesh and blood, ideas that are at times violent and tenacious, at other times so subtle and sympathetic as to seem irrational, are surely also necessary” (Andō 2010).
In 1955, Alvar Aalto set down the principle that the equilibrium of our surroundings—our towns, villages, traffic arteries, nature, and all the other elements that make up the setting in which we live our lives—is a real sign of culture. Throughout his career, Aalto was an advocate of developing local hubs in rural areas to prevent centralization and migration to the cities (Mizusawa et al. 2018). Over the past 60 years, his principle, to which has been added the element of today’s aging society, has become even more important; it is especially critical to examine how the super-aging society has begun to paralyze the urban functions necessary for high population concentrations (e.g., transit systems, public rights-of-way).
On the Shikoku Island in Japan lies Miyoshi City, Tokushima, a merger of one village in the lower river area and five hamlets in the mountain area during the Heisei period (c. 1989–2018 AD), which saw the large-scale consolidation of many municipalities in Japan in the early 21st century. Seiichi Kurokawa, the mayor of Miyoshi City, declared that his city was not a barely viable community but a nearly extinct one; he told me on 28 July 2016, that his city was doing everything it could to survive. Miyoshi City presents “real experience” tourism, welcoming some 300,000 or more tourists (see Figure 5) each year. Tourism creates employment for the few young residents of the riverside hotels and requisition private houses in the mountain area as accommodations called “sky lodgings.” Hotel receptions hold dances like village festivals with ghosts, as the transient population greatly outnumbers the permanent residents; one hamlet has more scarecrows than full-time residents. However, the mostly young tourists visit so that they can view the archetypal images of old Japan that the country wishes to preserve.
Nowadays, we desire new ideas. In the super-aging society of Japan, an important new idea is to design buildings and environments for the elderly, as they are now the largest part of the society.
4. Japanese Innovations in Modern History
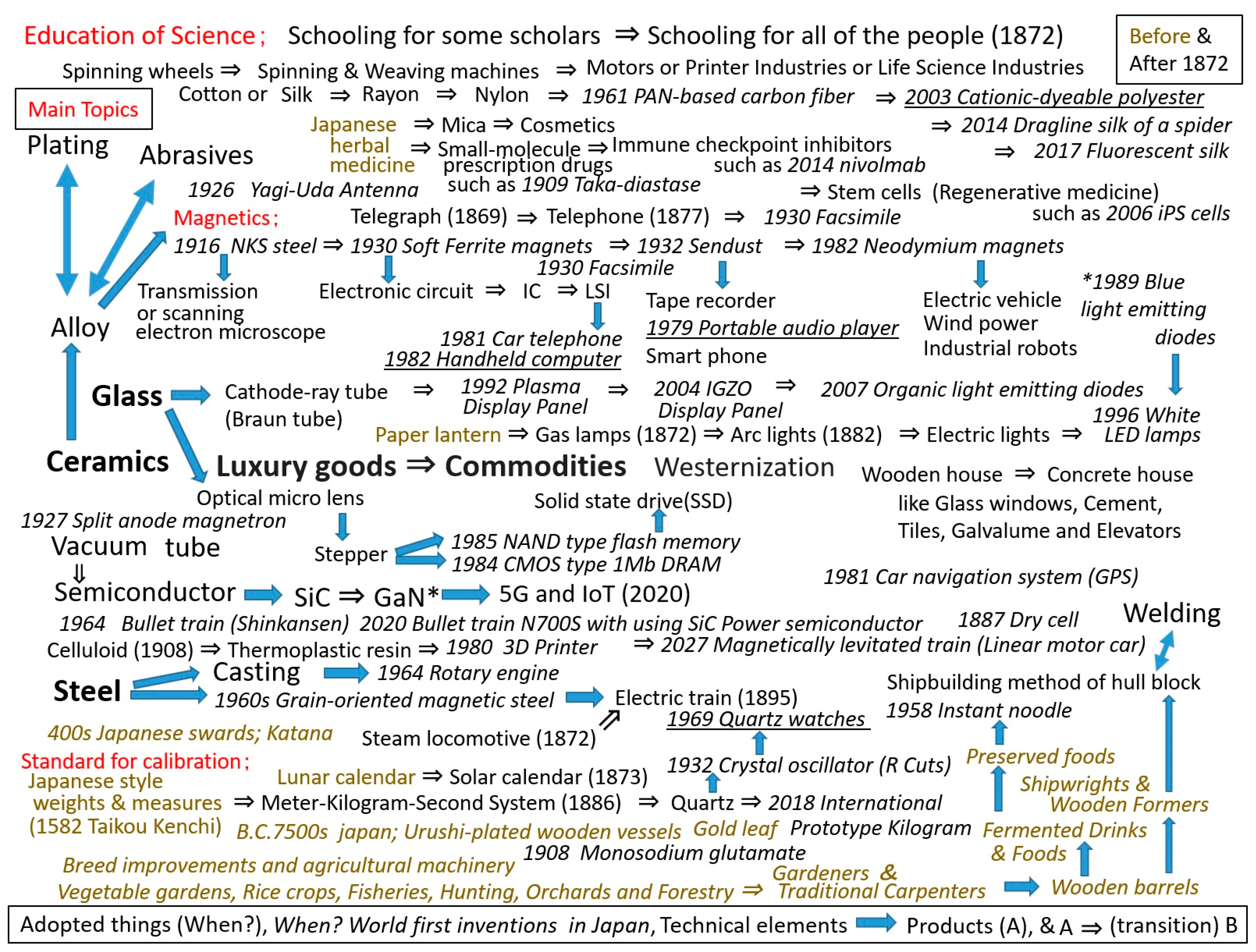
Japan ceased its national isolationist policies and opened up in 1854. Since then, Japan has actively adopted many of the customs of Western civilization and left behind its feudal system, changing Japanese society dramatically. Since 1872, all Japanese people have been able to receive an education in science, and many inventions have emerged during the past 150 years (see Figure 6) (Katō 2007; Shimonaka 1964; Iwata 1993; Tanabe 1975). Because Japan is poor in some natural resources, it has long relied on imports of petroleum and natural gas. After the 2011 Japan earthquake and tsunami, Japan started to pay greater attention to renewable energy. One unicorn company (unicorns are private companies valued at US$1 billion or more) called Euglena delivered Japan’s first bioliquid and diesel fuel production demonstration at a plant completed in 2018, and it declared itself part of “green oil Japan,” the aim to make Japan a biofuel-developed country (Euglena Co., Ltd. 2018). The company built its edible, outdoor, mass-culture technology based on the microalgae midorimushi (scientific name: euglena) in 2005. Using midorimushi and forming an alliance with trading, oil, airline, and other companies, Euglena will begin delivering next-generation biodiesel fuel in 2019 and bioliquid jet fuel in 2020. Such innovation is necessary in an aging society, and this is just one way in which Japan has embraced the Sustainable Development Goals (SDGs) promoted by the United Nations (United Nations, Department of Public Information 2015).
The underlined innovations in Figure 6, all handheld or wearable products, have become increasingly attractive for supporting the activities of daily living (ADL) for the elderly, especially given the growing expectations for IoT and robots as real partners of human beings. Most Japanese under 60 are familiar with robots from the many animated cartoons of their childhoods. Another unicorn company has been providing a wearable device that assists physically challenged wearers to move and enables them to exert greater motor energy than normal, like an energy-assisting exoskeleton. Originally conceived in 2009 as a device to ease the heavy work involved in nursing care support, the device has been expanded since 2015 to provide exercise-assistive medical devices for patients who suffer from spinal cord injuries, traumatic brain injuries, cerebrovascular diseases, diseases of the brain, and neuromuscular system disorders (Nordrum 2019). In 2015, one venture company developed and provided a walk-assist robot to support ankle dorsiflexion to stretch the gastrocnemius muscle in the back part of the lower leg, inducing reflex muscle contraction of the knee and hip joints to produce smooth forward steps (Tanaka et al. 2017; Zhuang et al. 2019). A nonpowered gait-assist suit based on passive walking has also been on the market (in Japan only) since 2015 (Sano 2017).
Japan has endured two World Wars and disasters such as tsunamis, volcanic eruptions, super typhoons, and earthquakes. Today, its total population is more than 3.5 times what it was 150 years ago. Japan had been supporting its overpopulation with food and energy earned by the hard work of importing raw materials, adding value with cheap labor and mass production or inventive value, and selling its products abroad. In this way, Japan has become an economic power. Economic growth, late marriage, nuclearization of the family, and an increase in double-income families all contributed to low birth rates and, at the same time, the system of public health insurance for the whole nation and enhanced medical technology promoted higher life expectancy. By 2025, almost 20% of Japan’s population will be over the age of 80. No country in the world has ever experienced such a situation.
Even the elderly who live longer and healthier lives need physical and spiritual care. When the population in Japan began to decline in 2017, business and government officials foresaw welfare problems given that there would be relatively fewer young working people to pay taxes. However, the problem is not how many people pay taxes, but how much tax and labor each citizen contributes during a lifetime (Becker 2010).
In super-aging Japan, there are many problems such as old people looking after weaker and older people, people leaving jobs to care for sick and aging family members, and so on. Adopting Western civilization’s trend toward nuclear rather than extended family units has weakened Japanese people’s interactions with and strong ties to local communities. Asian people once preferred extended family, town-centered traditions, and communal lifestyles. Societal changes have increased preferences for dining out, and led to numerous restaurants, catering businesses, and street purveyors of everything from dim sum and rice porridge to sweets and noodles in urban areas (Figure 7). However, dining out is a typical Asian style downward from the far past and even these older customs are facing challenges due to the super-aging society in Japan; food delivery services are on the rise in urban areas of Japan. While other heavily populated areas such as Hong Kong and Singapore are also facing aging populations, the problem of old people looking after weaker and older people is much greater in Japan than in other Asian countries. This limits the elderly’s activities to what the stronger partner can manage such that even shopping in urban or rural areas can be reduced to just procuring the daily necessities, unless they can engage in mutual-aid activities with neighbors.
Japan’s aging society has led to a medical environment in which doctors are increasingly encouraged to focus on preventing rather than treating diseases to reduce total health spending. Preventive medicine cuts social costs and protects the health of Japanese people as they age. This is a return to Japanese writer Shūgorou Yamamoto’s trusted town doctor, Red Beard (Akahige), the protagonist in movie director Akira Kurosawa’s film of the same name, which was honored in Venice with the Mostra Internazionale d’Arte Cinematografica’s San Giorgio Prize in 1965 (Becker 2010). Sawayaka-Aichi’s 24/7 mutual aid is one locally sustainable example of how this can work, and their services form a familiar gratis custom common among Japanese people more than 150 years ago.
Another historic parallel is the Sannai-Maruyama special historical site in the north of Japan, which features the remains of a large, long-term settlement that dates from the Early to the Middle Jomon period (approximately 5500 to 4000 years ago) (Figure 8). To keep the environment clean, the Jomon people separated their garbage into two types—what could be burned and what could not. The Jomon people also planted Japanese chestnut trees and stocked nuts in raised granaries, establishing a sustainable lifestyle with hunting and fishing. Each house was about the same size and a large assembly hall (32 m by 11 m) functioned to maintain Jomon communal living (Sannai-Maruyama Special Historical Site 2013). The Jomon people gathered in this assembly hall like Sawayaka Town. If modern-day Japan embraced some of these traditions from its original culture and lead the return to a sustainable, locally supportable lifestyle with innovative technologies, it could become a model for world development. Japan is at an inflection point.
5. Imperfect Human Life with Imperfect Robots
Aalto said, “Human life is a combination of tragedy and comedy. The shapes and designs [that] surround us are the music accompanying this tragedy and this comedy. The furniture, the fabrics, the color schemes and the structures can be earnestly and happily made so that they produce no contrast to the tragedy and comedy of human life” (Saito 2008). When people become old, the support of family or neighbors is necessary. Although the invention of reading glasses helped eyes weakened by the vanishing elasticity of their aging crystalline lenses (Wyszecki and Stiles 1982), nothing but hands could support people with hypokinesia (decreased body movement) in daily activities. Instead of human support, Japan’s innovators are intent on introducing robots into the daily lives of the elderly and disabled. According to a whitepaper from The Fifth Generation Mobile Communications Promotion Forum (5GMF) (2017), the wave of 5th ICT (5G) will also change lives dramatically by providing simultaneous connectivity worldwide (about 106 devices/km2), ultra-high speeds (about 20 Gbps), ultra-low latency (transmission latency over the radio link: about 1ms), and improved battery life.
An infrastructure using 5G mobile communications (and beyond) will further connect things with people through the IoT, lowering barriers and enhancing capabilities. Open architecture for autonomous robot systems originally aimed at entertainment applications has been proposed (Fujita and Kageyama 1997). Whereas the hurdles are still too high for the widespread use of robot systems in real life, this is not the case for entertainment—neither are robotic applications in manufacturing hindered by as many hurdles, as simple robots following canned routines in controlled environments such as factories have been in use since the 1930s. Advancements such as machine learning and adaptive methods have overcome the limitations of those original industrial robots (Wang et al. 2009; Doya 2000; Kawato et al. 1987), but we are still some distance away from practical robots. Even moving from point to point while avoiding obstacles can be a tough task for robots outside of a lab, let alone in the natural environment.
Our social infrastructure will continue to change with the effects of low birth rates and higher life expectancy in the near future. Maintaining economic growth, social services, and traditional infrastructure will grow more difficult due to manpower shortage, which is one reason the IoT and robots are expected to become a critical alternative technology to human services. Robotics as a field is still too underdeveloped to be implemented extensively in the natural environment, but experts predict that current circumstances will ramp up efforts to improve the lives of the elderly and disabled using new assistive technologies. Already, new biomimetic approaches have been explored to broaden the capability of robots to adapt to unknown environmental situations (Shimoda and Kimura 2010; Shimoda et al. 2013). Sensing technology such as mimicking gustatory and olfactory sensors has progressed (Tahara and Toko 2013; Toko 2013; Onodera and Toko 2014).
Consider the state of the remote communication of human senses. Sight and hearing have been addressed in various ways—television, radio, mobile phones, and numerous types of scanners. Tactile sensing has taken a wide range of approaches since the 1980s, with sensors based on visual feedback (e.g., shape sensing), slippage, and sound reflection developed in the 1990s and further refined in past few years (Ito et al. 2011a, 2011b; Tanaka et al. 2015). Vision-based tactile sensors can predict the shape of things from a single camera (Ito et al. 2011b). Simple but high-performance tactile sensing using reflected sound has been used to determine the softness and surface roughness of objects (Tanaka et al. 2015, 2016a). This tactile sensing can be made mobile, portable, wearable, and remote controllable, and the sensed tactile data can be shared by multiple people simultaneously. In clinical research, tactile technology has been adapted to enhance medical tools, especially those used in gastroenterological surgery (Ly et al. 2017; Fukuda et al. 2015, 2018; Tanaka et al. 2014, 2016b). Surface display, which presents the surface of the object near the contact point between the object and the body with a robot arm (Hirota and Hirose 1995; Hirose and Hirota 1993), robotic graphics (McNeely 1993), and partial surface display (Hirota and Hirose 1998) have become staples of virtual reality, including wearable devices. Robotic sensors can detect light, proximity, sound, temperature, and acceleration, among other useful elements of our surroundings. Such capabilities have applications that could be life-changing for the elderly and disabled in terms of mobility assistance, fall and burn prevention, and spatial awareness. Since tasting and smelling involve chemical reactions, they have been more difficult to translate into remote communication, but those sensors also have potential for assistive devices.
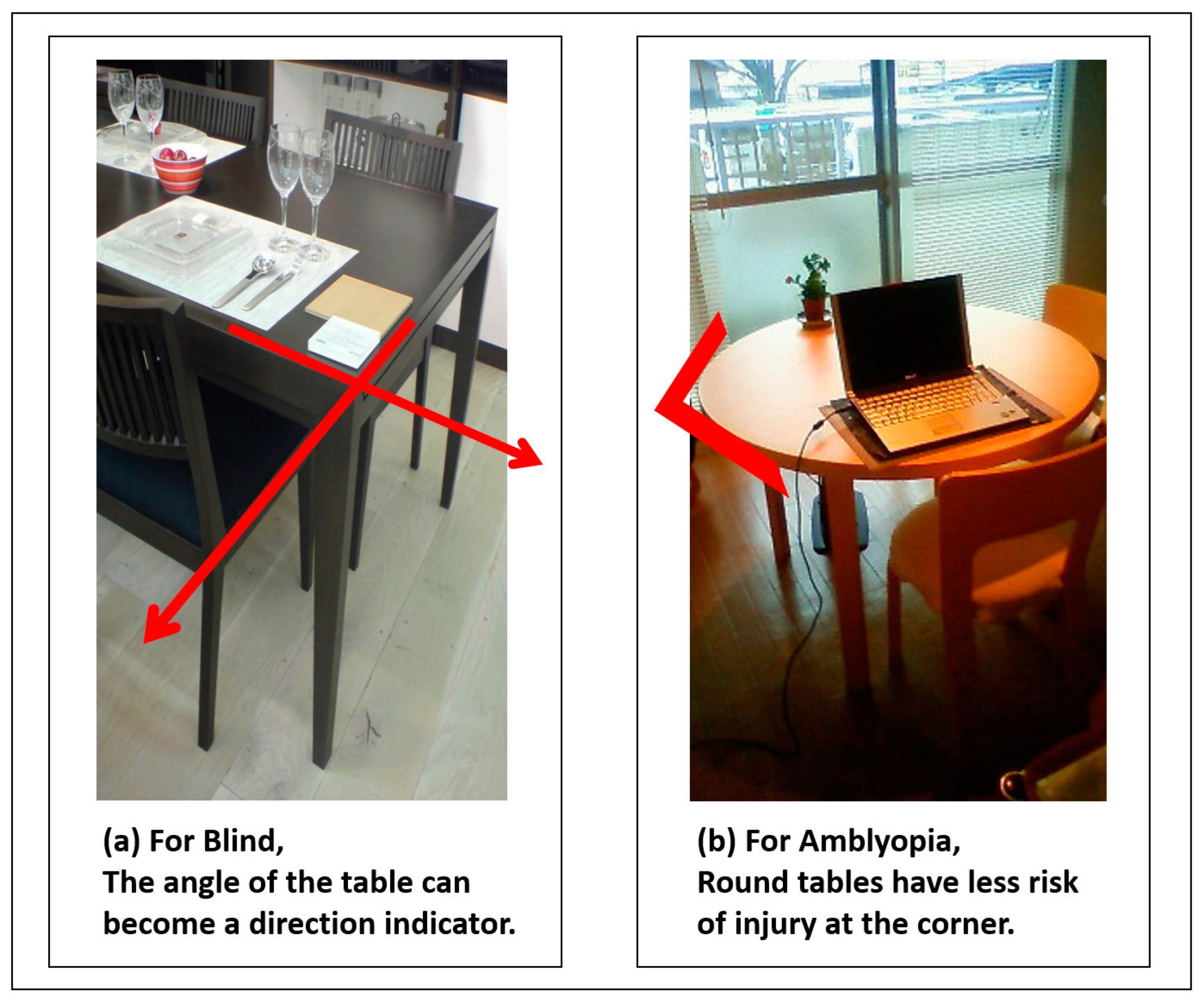
Engineers strive to organize the environment to draw the best performance of the devices they develop; but few of us live in laboratory conditions. The natural environment is cluttered and sometimes chaotic. Figure 9 shows a type of hearing aid that uses thin plastic discs to deliver 5 dB amplification of volume in the audible range (about 2 kHz at the peak) and clarification of words for elderly people, even in a normal (cluttered) environment (Yamada et al. 2013). To address the reality of an aging population requires both empathy and the ability to think hypothetically as preconditions, and engineers need to ensure that innovative products have practical uses in the real world. In the same way, architects, ergonomic engineers, and designers need to understand the components that make the environment suitable for the elderly and disabled (Figure 10). Since human variety is too diverse for truly universal design, engineers and designers will need to work even more closely than they do now with medical care experts and elderly and disabled people to make the most of biomimetic sensors, 5G, robotics, and ergonomics in the aging society.
6. The Characteristics of Elderly People
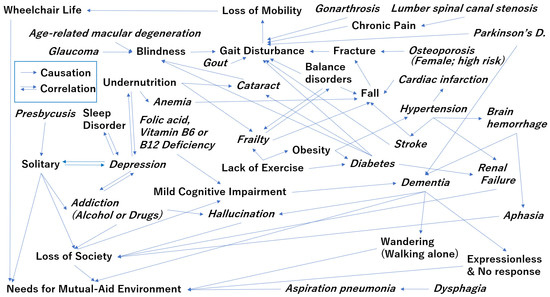
The super-aging of Japan has increased its cancer prevalence (Hori et al. 2015). As a 2007 article in Nature pointed out, some strategies that protect us from cancer (e.g., cellular senescence or telomere shortening) can hasten the rate of aging, while others (e.g., autophagy or protection from genomic instability) share common rather than antagonistic etiologies (Finkel et al. 2007). The number of cancer survivors increased with the strenuous efforts of medical specialists and the number of elderly without cancers also increased. The causal and correlative relationships between gerontology and geriatrics without cancers are shown in Figure 11: causal relationships (one-way arrows) are quite different from correlative relationships (bidirectional arrows), since one way from a cause to an effect appears on the causal relationships, and bidirectional substitution among a cause and an effect can appear on the correlative relationships (Yamada et al. 2017). These relationships sometimes confuse engineers, medical professionals and researchers. For elderly individuals to avoid such common geriatric diseases, preventive medicine becomes very important. The expense of trying to treat everyone’s geriatric diseases could potentially bankrupt the national healthcare budget in our aging society.
What individuals can do now to try to prevent geriatric illness later is establish habits that maintain adequate exercise, sleep, nutrition, and balance ability. Gait disturbance is one important checkpoint for geriatric illness, as can be seen in Figure 11, which is why the mobility-assistance market (e.g., canes, walking frames) has grown so dramatically. As the figure emphasizes, when assisted walking becomes “wheelchair life”, eventually, elderly people have been exposed to various additional stressors involving physical, biological, chemical, social, and psychological factors that induce biological responses in the body that are collectively called general adaptation syndrome. These responses (e.g., glucocorticoid and catecholamine secretion) are necessary parts of the “fight-or-flight” survival response, and they also exert effects on our circadian rhythms. Human life in contemporary society is too stressful and complicates human study about stress. Sakakibara et al. reviewed the relationship between stressors and the stress response on biological rhythms, mainly through animal studies (Sakakibara et al. 2016). Circadian rhythm sleep disorders are well known but correlation between sleep efficiency and geriatric diseases has not been clarified, although it is known that sleep efficiency continues to significantly decrease after 60 years of age (Ohayon et al. 2004).
“Let food be thy medicine and medicine be thy food.” This maxim has been attributed to Hippocrates, a physician and philosopher in Classical Greece (c. 460–370 BC) (Hipocrates 1963). A similar idea arose in ancient China—that is, eating wisely aids health. More recently, a controlled multidisciplinary cohort study on postoperative nutritional care confirmed that an increase in energy and protein intake by elderly patients recovering from hip fractures did better than those following the regular hospital guidelines and, three months later, they exhibited less undernutrition and improved quality of life (QoL) (Hoekstra et al. 2011). Similarly, when strict energy management by dieticians was used as an intervention of nutrition care, a randomized, controlled study showed that tight calorie control in geriatric patients following hip fracture decreased complications (Anbar et al. 2014). Likewise, according to a randomized, controlled study of acute stroke patients with low nutritional risk, individualized nutritional care was more effective in suppressing weight loss and improving QoL and grip strength than routine care (Ha et al. 2010).
Nutritional support for elderly patients improves their QoL. While it is best to begin eating wisely when we are still young, late-life modifications can help reduce risks. For example, higher intakes of processed meat lead to a higher mortality rate from arteriosclerosis, stroke, myocardial infarction, and cancer (Wang et al. 2016). A large epidemiological cohort study of individuals aged 35–70 years in 18 countries with a median follow-up of 7.4 years showed that a higher carbohydrate intake was also associated with an increased risk of total mortality (although not from cardiovascular disease), while intake of total fat and saturated and unsaturated fats was not significantly associated with risk of myocardial infarction or cardiovascular disease mortality (Dehghan et al. 2017). Estruch et al. reported that a Mediterranean diet supplemented with extra-virgin olive oil or nuts can reduce the incidence of major cardiovascular events among people at high cardiovascular risk (Estruch et al. 2013, 2018). In adult males, intake of milk-processed products was reported to increase the risk of prostate cancer (Aune et al. 2015), and people with higher intake of yoghurt had lower incidence of diabetes (Gijsbers et al. 2016; Salas-Salvadó et al. 2017). Although it has not yet been replicated with humans, miso was found to suppress the occurrence of chemical-induced breast cancer in rodents (Gotoh et al. 1998a, 1998b).
It is believed that fermented foods are good for the body because of how fermentation changes foods and how fermentation-enriched chemicals (e.g., lactoferrin, bioactive peptides) and newly formed phytochemicals (e.g., flavonoids) interact with our intestinal microbiota. In Japan, there are many traditional fermented foods such as nattō (straw-wrapped fermented soybeans), miso (fermented soybeans paste), and narezushi (fermented sushi), funazushi (fermented crucian carp sushi), or kaburazushi (salted turnip and yellowtail sushi with lactic acid fermentation). The intake by elderly people of yogurt and other fermented foods has increased, as have delivery services of fermented foods (Kawai et al. 1998; Marotta et al. 2009; Kawai and Matsuura 1997).
Everyday dietary habits matter to our health. Ordinary natural foods should not be overlooked in favor of pharmaceuticals, supplements with flashy packaging and vague claims, and fast food and prepared food. Recently, the diet of the Japanese has changed from meals focusing mainly on fish and vegetables to a more meat-based diet. As a consequence, the prevalence rate of breast cancer and colorectal cancer is now increasing as it has in Europe and the United States (Hori et al. 2015). Obesity, another risk to health, is also increasing. Guidance to replace ingredients seems to be more effective than suggesting reduced food intake (Ludwig and Friedman 2014), which should be done only with great caution in the case of obesity of elderly people, who are more prone to low nutrition or malnutrition. The food stalls and home deliveries that are readily available in urban areas are less so in rural areas, and shops and fresh-food markets are also less plentiful. This suggests the need for finding ways to ensure that the elderly and disabled everywhere have access to not just enough food but the right food.
According to Fried et al., frailty is not synonymous with either comorbidity or disability, but comorbidity is an etiologic risk factor for, and disability is an outcome of, frailty (Fried et al. 2001). For elderly people with frailty, nutritional guidance and exercise therapy have mainly been used in the past, with a focus on muscle strengthening, locomotion training, and aerobic exercise (Pollock et al. 2012). Recently, we have also realized the importance of rehabilitation that trains balance ability (Ozaki et al. 2017). In addition, a relationship has been noted between mild cognitive impairment (MCI) and frailty (Shimada et al. 2013; Saji and Sakurai 2017). MCI is one criterion in gauging cognitive decline, based on six evaluation indices of memory, awareness, judgment, social adaptation, family and hobby interest, and self-care (Petersen et al. 1999). Many elderly people complain of memory decline as they age. People with MCI have a normal daily life but a half of them tend to acquire Alzheimer’s disease (AD) over time, and MCI is reversible but increases the risk of dependency, institutionalization, and mortality (Petersen et al. 1999; Almkvist et al. 1998).
Barrier-free information accessibility is important in elderly care. Uchida et al. called age-related hearing loss in Japan an issue of national importance, with 32.5% of those aged 60–64 and 62.5% of those aged 70–74 experiencing hearing impairment (Uchida et al. 2012). Presbycusis is considered to be induced by decreased inner ear function and advanced retro-cochlear disturbance (Shimoda 1995). Hearing loss affects the motivation and behavior patterns of the aged (Klotz and Kilbane 1962). Its profound effect on communication has been linked to mood changes, reduced QoL, and higher rates of depression. However, Lin et al. found that hearing loss is independently associated with the incidence of all-cause dementia (Lin et al. 2011).
7. Dementia Is a High Risk in the Super-Aging Society
Summarizing the onset process of the most common Alzheimer’s-type dementia, first amyloid β begins to accumulate for more than 10 years, then tau accumulates, then neurons of the brain die, and eventually memory impairment and cognitive function decline to the point of Alzheimer’s-type dementia (Jack et al. 2010). Based on the Hisayama Study, by 2020, 6.31 million people in Japan (18% of the population) could have some form of dementia; just five years later, that number could be 7.3 million people (20.6% of the population) (Health and Welfare Bureau for the Elderly, Ministry of Health, Labour and Welfare, Japan 2016; Ozawa et al. 2013; Kishimoto et al. 2016; Ninomiya et al. 2011; Hokama et al. 2014). It is only an estimate, however. The Medical Research Council on Cognitive Function and Aging Studies (CFAS I and II), a two-decade dementia incidence comparison in England and Wales, showed a reduction of the generation-specific incidence (Matthews et al. 2013), suggesting that the number of people estimated to develop dementia in any year has remained relatively stable (Matthews et al. 2016). It is noted that the background of sociodemographic characteristics was quite different for the education period in comparison with CFAS I and II (Jagger et al. 2016), so a simple comparison cannot be done, but the implication is that a longer education period can help lower the incidence of dementia.
Acetylcholinesterase inhibitors that suppress the decline of the neurotransmitter acetylcholine and N-methyl-D-aspartate (NMDA) receptor antagonists that suppress excitotoxicity by the neurotransmitter glutamate are used as therapeutic agents for AD (Winblad et al. 2006; Nakamura et al. 2011; Zhao et al. 2002; Samochocki et al. 2003; Tariot et al. 2004). Although they give temporary relief of symptoms and suppress dementia progression, they have not reached the level of fundamental treatment. The cost of drugs for dementia such as AD is ¥150 billion annually in Japan (Okumura and Sakata 2018).
In France, there is a public organization called Haute Autorité de Santé (HAS), founded in 2005, that evaluates the clinical effect of medicines and medical technology covered by medical insurance. In October 2016, HAS published the results of the study on the clinical utility of Alzheimer’s disease treatment drugs and concluded that there was insufficient evidence that the drugs helped enough to delay patients’ entry to a facility and suppress severe illness (HAS 2016). HAS further advised that adverse events involving the digestive and cardiovascular systems could not be ignored and thus it was inappropriate to cover the drugs with medical insurance; on 1 August, 2018, drugs used for treating AD were removed from medical insurance coverage in France (Ministère des Solidarités et de la Santé, Duquesne, Paris, France 2018). Unfortunately, at the present time, no new drugs have been approved or are even suggested candidates for removing the causal substances of dementia, leaving the development of therapeutic AD drugs in a difficult state (Cummings et al. 2017). The pharmaceutical treatment of advanced dementia being so difficult, research has increased in the areas of prevention and prediction, and it has become possible to identify the high-risk group by biomarkers such as amyloid β and tau proteins before onset; the establishment of an effective treatment method at an early stage, before onset, is strongly desired (Nakamura et al. 2018; Shinotoh et al. 2019). To further study the dementia risk associated with MCI, a multicenter prospective cohort study for individuals with MCI or early-stage dementia was launched in Japan and is expected to accelerate clinical trials of novel therapeutic agents and improve effective care management (Saji et al. 2016).
8. Aging and Physical Surroundings
In the case of dementia, social costs are considerable; the cost of nursing care and the family burden are large. Japan’s Ministry of Health, Labour and Welfare has formulated the New Orange Plan aimed at realizing a society in which the will of patients with dementia is respected and so they can remain living independently or at least in a familiar environment for as long as is safely possible (Health and Welfare Bureau for the Elderly, Ministry of Health, Labour and Welfare, Japan 2016). The Japanese government’s Annual Report on the Aging Society found that 54.6% of respondents said they wanted to spend their final days at home (Cabinet Office 2017a). This means that many homes will need to be built or renovated to support people in various stages of physical and mental decline.
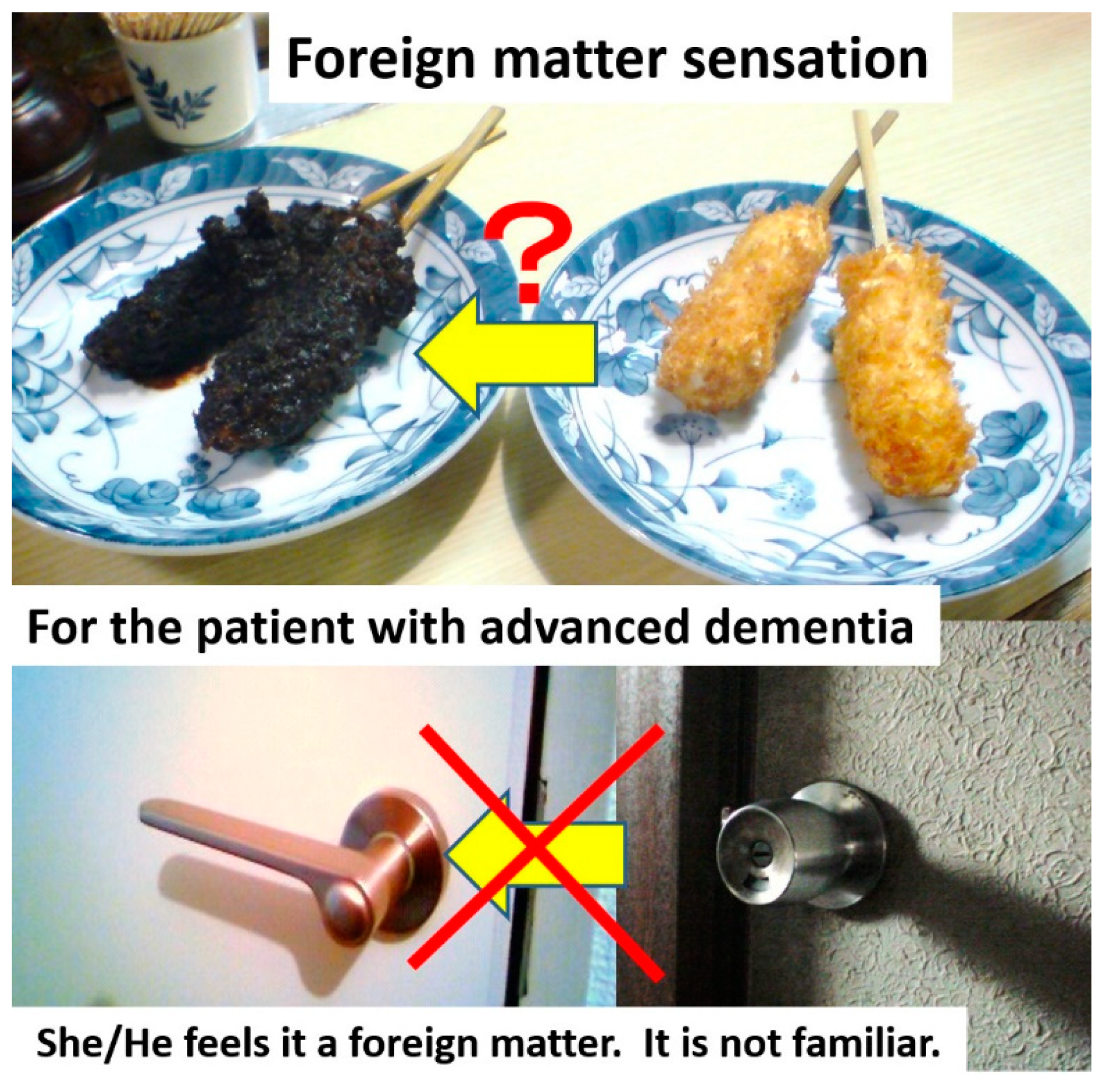
Many of the issues are easily anticipated: as people age, they tend to lose muscle strength, dexterity, and stamina, and their senses are not as sharp. However, let us consider home renovation for elderly residents. You might think you should automatically change doorknobs to lever-type knobs for the elderly residents because the latter style requires less grip strength to operate in Figure 12. For residents with dementia, however, changing the doorknobs introduces unfamiliar foreign matter than can make them feel helpless and confined. In Figure 12, the deep-fried skewer in the upper left image has been dipped in miso sauce, turning it black. Although this is a very familiar local food in Nagoya City, Japan, and has been served for decades in one restaurant with a long history, you would not try to eat it spontaneously. Patients with dementia might balk at its unusual appearance in such a situation like you.
Ideally, houses should be renovated before the onset of dementia so residents have time to become familiar with any new features in the house and surroundings. Patients with dementia have been known to wander away from where they have been rehoused, looking for familiar houses or landmarks from where they grew up. They are not walking without purpose but searching. Studies have found that patients with Alzheimer’s-type dementia have higher recognition rates for red and yellow objects (Wijk et al. 1999), so designs incorporating these are preferable. In Sawayaka Town, for example, stair railings and grab-rails are orange or red (Figure 13). Sawayaka-Aichi uses what Sawayaka Town calls the Longevity Stairs as training spots for the elderly.
Some regions of Japan have implemented similar measures for traffic safety, using blue-colored intersections to warn drivers to decelerate and use caution as there may be pedestrians or cyclists crossing. Some elderly people who lived in a neighborhood with a blue intersection said, “we are always going into a pool when we across the intersection.” Blue is a reminder of water and reminiscent of flood disasters for Japanese. Therefore, it may cause some elderly people anxiety; one nursing home found that a single blue tile embedded in the middle of a hall in a nursing home stopped patients with mild dementia from crossing it, as they wanted to avoid the “pond.” Many color vision studies have been undertaken over the years, some perhaps inspired by Newton’s words, “For the Rays to speak properly are not coloured. In them there is nothing else than a certain Power and Disposition to stir up a Sensation of this or that Colour” (Katz 1935; Boynton 1979; Kaneko 1988, 1995). Color is a response to cerebral innervation corresponding to the wavelength component of light, and it can play three roles: discrimination or detection; segregation of shapes; and identification of things (Uchikawa 1998). The elderly referred to above had difficulty using the color blue for the segregation of shapes and object identification because it sent an ambiguous message to their brains and suggested the presence of water where there was none.
Is it possible to prevent dementia? There is an important report suggesting that some leisure activities, such as playing board games (HRD 0.17–0.57) or playing a musical instrument (HRD 0.11–0.90), may reduce the Hazard Ratio for Dementia (HRD), while others, such as bicycling (HRD 0.97–4.49), team games (HRD 0.14–7.79), and babysitting (HRD 0.11–6.01) (Verghese et al. 2003), yield extremely divergent results. Sawayaka Town incorporated these kinds of studies in its design, adding in a piano, karaoke, and a space for board games (Figure 4). Combined physical and unfamiliar cognitive exercises, such as walking while subtracting 100 from 7, seem better for persons with MCI (Shimada et al. 2017, 2018).
Since gait disturbance is such an important checkpoint in geriatric evaluations (Figure 11) and because combining walking with mental exercise can be a valuable preventive method, more Japanese towns show plan areas or methods where elderly people can walk safely even though they may be lost in thought. There have been numerous studies in the United States on improving the QoL and cognitive health of patients with dementia and elderly persons using music programs (Thomas et al. 2017; Vinoo et al. 2017). One was described in the documentary movie Alive Inside: A Story of Music and Memory (filmmaker: Michael Rossato Bennett), which premiered at the 2014 Sundance Film Festival.
In home remodeling, elderly residents’ responses to changes in the surroundings can depend on whether the elderly residents accept their disease or disability. They may have self-directed negative emotions about causing inconvenience to family members or providers, being a financial burden, or just about their reduced abilities, and these can increase their anxiety. Caregiver fatigue, seeing parents’ decline, financial worries, resentments, insecurities about their own caregiving skills, and reminders of mortality can also increase the anxiety and mixed feelings of family members. Such tensions can hinder even minor renovations like removing bumps, installing grab-rails, replacing steps with ramps, and so on. A house is not barrier free if the hearts of the whole family are filled with barriers.
Lifestyles vary greatly due to diseases or disabilities. Wheelchair architect Kazuo Abe has said that architects should understand the psychological state of all stakeholders and know what kinds and degree of changes the residents and their families desire when planning the renovations (Abe 2018). There are NPOs in Japan that have been given home remodeling advisories for over 20 years (Asai and Ohtani 2001). It may take time for the elderly to feel positive about changes, and it is necessary to consult professionals such as doctors, physical and occupational therapists, care managers, social workers, medical equipment suppliers, nursing care providers, administrative officials, and so forth. Therefore, architects should consider physical space improvement only after having gained a comprehensive understanding of the elderly and other residents.
9. Designing for Resident-Centered Care
We are born. We age. With aging comes decline, pain, and illness. We become patients, often requiring medical doctor-centered treatments, which can lead to the white coat effect when the stress of having our vitals measured in a medical setting raises those vital signs into unhealthy ranges, and normal communication becomes garbled by filters of anxiety, pain, and fear of the unknown. Faced with an increase in the proportion of patients who are closer to the end of life (EoL) than the beginning, the best practitioners use straightforward, approachable language that is technical and accurate but easily understandable by anyone with a junior high education, even if their patients are experienced academics and doctors themselves. Regardless, information gaps and misunderstandings will occur. We await orders and explanations from medical experts and rely on medical doctor-centered treatment. However, we must all be the lead actors in our own lives. This means that the aging population will have to speak up, ask questions, and maybe even do a little research, even if they have not been raised that way. It may be in our nature to endure pain or troubling symptoms without complaint, but doing so can lead to the rapid worsening of a condition that later requires even more “inconvenience” to family or “bother” to medical staff. This happens frequently.
However, it is often the case as well that if patients’ pain can be controlled, their QoL can be improved. This would lead to more patient-centered care. This idea inspired us to develop Pain Memory, a tablet application that enables users to visualize and record their pain levels both instantly and over time, so patients can observe their pain objectively and medical staff can accurately grasp the patients’ condition, which is especially useful for pain of diurnal variability (Hirazawa et al. 2015). Pain is a subjective feeling but, as Nakata et al. reported, the sensation of pain can be alleviated by tactile stimuli (Nakata et al. 2004). Although attention should be paid to the risk of fracture to people with conditions such as osteoporosis, massage can be effective for alleviating pain. Indeed, massage with massage equipment and paraphernalia is popular in Sawayaka Town. It is worth considering, when renovating spaces for the elderly, whether an easily accessible spa tub such as a walk-in unit with jets might be advantageous.
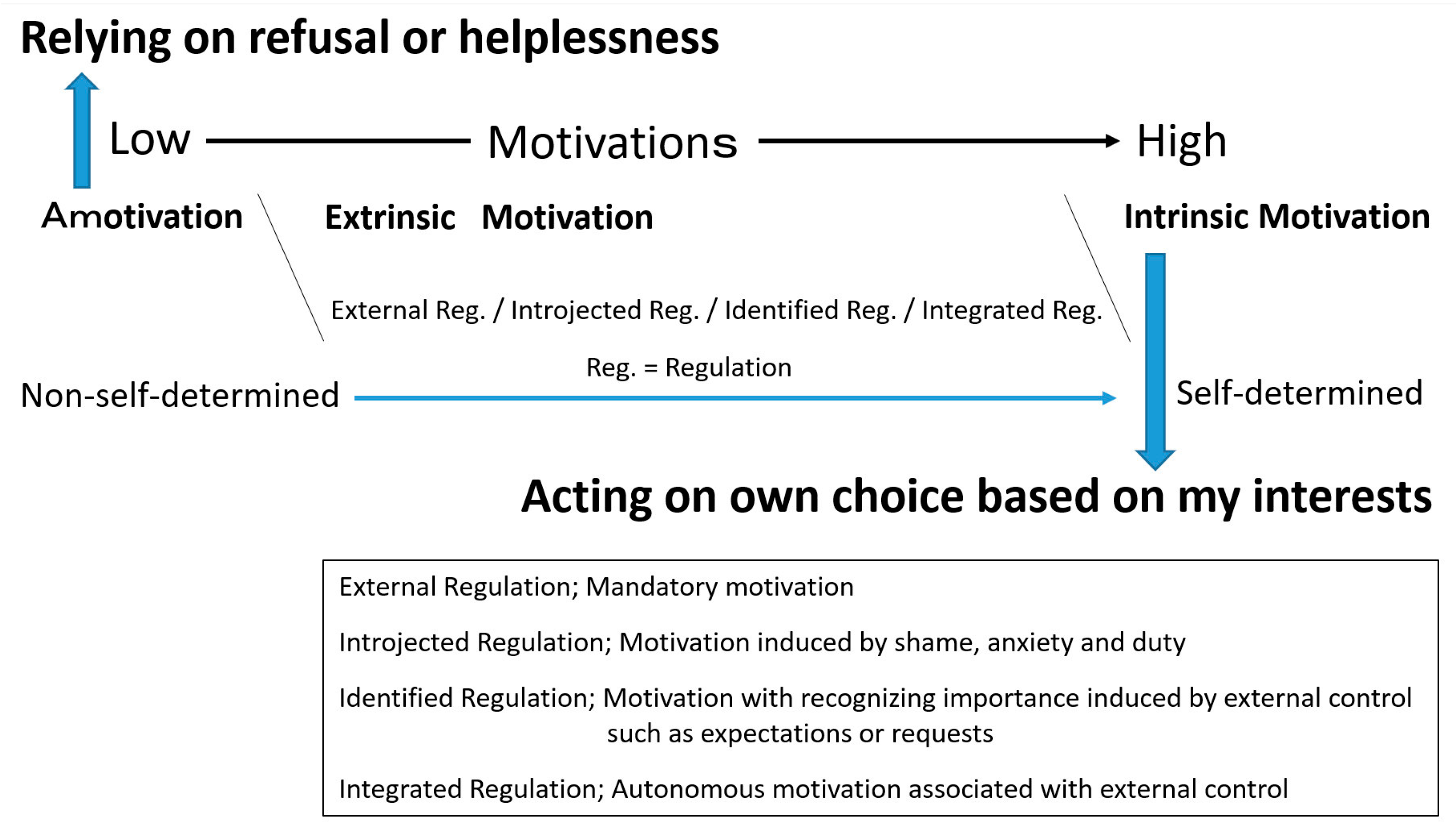
When renovations or construction includes the implementation of IoT devices and robots, once these are more practical in our natural environment, these devices must be desired such that they can be operated (or at least understood) by the elderly residents themselves. Implementation based on intrinsic motivation is ideal, as elderly residents want to be more connected with others rather than monitored by them. However, when deciding whether such an implementation is advisable, consider whether the elderly resident has extrinsic motivations when evaluating new products. Deci and Ryan indicated that extrinsic motivation has four regulatory styles: external, introjected, identified, and integrated (Deci and Ryan 2000). Here, external regulations are those motivated by compulsion; introjected regulations are those motivated by shame, anxiety, or obligation; identified regulations are those motivated by the recognition of importance by an external control such as expectation or request; and integrated regulations are those associated with external control and are autonomously motivated. The relationship among intrinsic and extrinsic motivations is summarized in Figure 14. It is better that device-developing companies make efforts for their devices to induce integrated regulations of the elderly residents in the aging society.
10. The Final Stage: What the Elderly Really Want
Typical Japanese houses have two serial tatami rooms that can become one big room for family ceremonies such as weddings and funerals. Japanese people take off their shoes and sit Japanese seiza-style or cross-legged together so that many people can share the narrow space. Japanese people feel pleasure in taking people and nature inside the house since Japanese people believe that God dwells in people and nature. Japanese people worship nature in awe. Juraku-tuchi is used to plaster the walls of the best tea rooms representative of Japanese culture. Mud-plastered walls are highly hygroscopic, and their value is being revised upwards. This rare juraku-tuchi can be collected only from the old central town of Kyoto; juraku means the first age of peace after the Warring States period in Japan. Using this soil captures the effect of a peaceful and natural landscape of Kyoto, incorporating the external, natural world into the internal, built world of Japanese houses. The Japanese associate this with happiness.
Almost all Japanese people want to return to nature; a recent questionnaire indicated that over 90% of Japanese people want to die naturally (Cabinet Office 2017b). Over half of Japanese people want to spend their final moments at home (Cabinet Office 2017a). Therefore, their houses must serve the functions needed at the End of Life (EoL). The problem is that how the elderly person wants to spend their EoL is not always compatible with the ability to build an environment that respects those intentions. In other words, it is necessary for the elderly to select their treatment at the terminal stage. The ways and means of a person’s EoL depend on their selections; so it is important that, while they are still of sound mind and able to communicate, they have discussions, even documentation, of their wishes regarding EoL interventions and assistance such as cardiopulmonary resuscitation, endotracheal intubation, artificial respiration, and procedures such as tracheotomies, gastrostomy, and so on. Their ability to talk or eat and the functions required of the space are all affected by these selections.
More than 150 years ago, most people were more familiar with death than they are today and, in Japan, this is especially true since the region has experienced numerous natural disasters and wars. Relatives, friends, and acquaintances hold an anniversary memorial service, called houji, gathering 7 days, 49 days, 1 year, and 2 years after a death in Japan. In the United States and the United Kingdom, grief care parties are a reference to this Japanese custom and a time to remember and honor the deceased (Becker and Sengoku 2015). Participants seem to gain mental stability and inner peace through this custom. In Japan, between 1960 and 1990, hospital deaths outnumbered home deaths, and Japan has dramatically changed into a nation that fears death (Schumaker et al. 1991; Schumaker 1991). Views of life and death are quite different between Western and Eastern thought, as well as between generations. In Asia, views of life and death also differ among regions; funerals are solemn ceremonies for relatives in Japan, whereas funerals are town festivals in Indonesia. We have experienced wedding ceremonies and funerals at the Fukkatsu Lutheran Church—its sanctuary design elicits mountain images reminiscent of the Sermon on the Mount, and there we felt the differences and equivalence of Western and Asian thought.
Fewer than 1% of the population in Japan is Christian, largely because the strong influence of the ban on Christianity from 1612 to 1873 still lingers. In a citizen study of the aging community, the late Yutaka Toda, a pastor in Fukkatsu Lutheran Church in Japan, taught us Christian rituals (Mizuno et al. 2014) and said that the church was expressed as Kyou-Kai (“teaching meeting,” in Chinese characters), but the true meaning of church is assembly hall. We knew the reason for the existence of the church in our town and felt that Christian life—which, for us, meant walking at least once a week to the assembly hall, meeting companions, playing the organ or ringing hand bells, reading the Christian Bible, singing hymns, saying prayers, serving communities, having meals with companions and chatting—seemed to cover all the best ways to prevent geriatric diseases.
Wearing shoes improves the degree of knee rise when walking and prevents falls. It is vital at osteogenesis to bathe in the sun, and if you get sunshine for over five minutes a day, this helps prevent osteoporosis. Town walking is an economical and healthy hobby, as is walking anywhere you find places you love, such as memorable buildings, unique forms, and nature; walking is also a fine preventive of geriatric diseases (Mizuno et al. 2015). Creating a town that enables safe and enjoyable walking is essential in town planning. Therefore, round-trip walks to the church are a wonderful practice and a fine way to gird yourself against geriatric diseases. At Sawayaka Town, the elderly are requested to wear shoes when walking, stretching, and working out to build strength (see Figure 15). These days, Japanese people rarely go to temples except to attend funerals, houji gatherings, or for sightseeing.
Christian culture encourages the practice of altruism and helping neighbors in need as part of its rules of life and living well (Becker 2012). This altruism is exactly the same as Sawayaka-Aichi’s “mutual-aid activities in 24 h of 365 days” and gratis customs common among Japanese people more than 150 years ago. When Ms. Kawakami first started her NGO’s mutual-aid activities, her services were free, too, but she soon learned that users found it more difficult to ask for free service than if these activities were paid for, so there are now nominal fees.
11. Beyond the Super-Aging Society
This paper has summarized the assistive technology and knowledge relevant to Japan’s super-aging society, with frequent references to Sawayaka-Aichi and Sawayaka Town as exemplars. We need further examination of the benefits of such age-focused services, with both qualitative evidence (e.g., delights and successes of the users and helpers) and the quantitative, scientific data. We look forward to creating similar spaces suitable for establishing a sustainable society that supports healthy longevity. Such spaces will be filled with mutual aid, humanity and assistive robots in the near future, with advancements driven as much by love, empathy, and compassion as by motives of profits and necessity.
In Japan, positive thinking tells us that there is no ordeal, including super-aging, that cannot be overcome. To realize a sustainable society, Japan must persevere, for no matter how social circumstances may change in the future, contraction in the industry in both scale and form seems inevitable in Japan (Andō 2010). We must continue our innovations in physiochemical technology combined with and shaped by familiar customs and traditional culture, just as the dental services and remedies that have existed since ancient Egypt have been refined into what we are accustomed to today (Forshaw 2009). The implementation of new technologies will affect our lifestyle and change the world well beyond the super-aging society.
French philosopher Blaise Pascal said that man is but a reed, the most feeble thing in nature, but he is a thinking reed (Miki 1980). Frank Lloyd Wright was always learning, and change was a vital principle in his nature; in the Taliesin Fellowships, established in 1932, he frequently quoted the Greek philosopher Heraclitus, who was stoned in the streets of Athens some two thousand or more years ago for stating that the only immutable, unchangeable law is the Law of Change (Pfeiffer 1989). Aalto was an advocate of developing local hubs in rural areas throughout his career (Mizusawa et al. 2018). The number of staff who came and went from Aalto’s firm from the time it opened totaled some 360 Swiss, Danes, and Swedes, and, after World War II, Americans, Italians, Japanese, Indians, and other nationalities (Göran and Aalto 1994).
What advancements do we need to break through our super-aging problems? For one, we should encourage more learning, including studying the past with an eye to the future. International interdisciplinary knowledge-building efforts such as Wright’s Taliesin Fellowship or Aalto’s firm are important models. We must embrace the possibilities in Pascal’s words, “l’homme passe infiniment l’homme” (human beings can pass infinitely far beyond human beings) (Miki 1980). Laotze said, “The master of living does not distinguish between work and play, labor and leisure, mind and body, education and entertainment, love and religion. Whatever the master of living does [is to] aim for excellence on that road” (Laotze 2008; Seelig 2013). Moreover, we must learn from the 101.7 years of the Christian life of Sister Mary from The Nun Study; she showed successful cognitive aging in a longitudinal study of 678 Catholic sisters aged 75 to 107, although her neuropathologic postmortem found that her brain contained abundant neurofibrillary tangles and senile plaques, the classic neuropathologic lesions of Alzheimer’s disease (Snowdon et al. 1996, 1997; Snowdon 1997). As civilization advances, society becomes more complex. However, walking and continuing to learn remain the secrets of health and the essence of human beings, and continuing to support these customs will be the foundation of a new civilization extending beyond the aging society.
Funding
This research received no external funding.
Acknowledgments
The author is grateful to late pastor Yutaka Toda and his wife Shizu for teaching him about the Western lifestyle, and to Satomi Kawakami, Fuyume Maruyama, and the NPO Sawayaka-Aichi for their cooperation.
Conflicts of Interest
The author declares no conflict of interest.
References
- Abe, Kazuo. 2018. Barrier-free house with spiritual barrier-free. Architect Aichi 695: 16–17. (In Japanese). [Google Scholar]
- Almkvist, Ove, Hans Basun, Lars Bäckman, Agneta Herlitz, Lars Lannfelt, Brent J. Small, Matti Viitanen, Lars-Olof Wahlund, and Bengt G. Winblad. 1998. Mild cognitive impairment—An early stage of Alzheimer’s disease? Journal of Neural Transmission Supplementum 54: 21–29. [Google Scholar] [CrossRef] [PubMed]
- Anbar, Ronit, Yichayaou Beloosesky, Johnathan D. Cohen, Zecharia Madar, Avraham T. Weiss, Miriam Theilla, Tamar Koren-Hakim, Sigal Frishman, and Pierre P. Singer. 2014. Tight calorie control in geriatric patients following hip fracture decreases complications: A randomized, controlled study. Clinical Nutrition 33: 23–28. [Google Scholar] [CrossRef]
- Andō, Tadao. 2010. Tadao Ando 0: Process and Idea. Tokyo: Tōtōshuppan, ISBN 978-4-88706-309-9. [Google Scholar]
- Asai, Kiyoko, and Kyoko Ohtani. 2001. Example reporting: 20 people’s dwellings and livings. In Living in the Area. Finally Realized Living with Entrance! Edited by A. Kiyoko. Nagoya: Fubaisha, Inc., ISBN 4-8331-1057-1. (In Japanese) [Google Scholar]
- Aune, Dagfinn, Deborah A. Navarro Rosenblatt, Doris Sm Chan, Ana Rita Vieira, Rui Vieira, Darren C. Greenwood, Lars J. Vatten, and Teresa Norat. 2015. Dairy products, calcium, and prostate cancer risk: A systematic review and meta-analysis of cohort studies. The American Journal of Clinical Nutrition 101: 87–117. [Google Scholar] [CrossRef]
- Becker, Carl. 2010. Japan’s Wisdom: How It Can Save the Future. Tokyo: EIHŌSHA. [Google Scholar]
- Becker, Carl. 2012. American and English Ideals. Tokyo: EIHŌSHA, ISBN 978-4-269-13008-1. [Google Scholar]
- Becker, Carl, and Mari Sengoku. 2015. Japanese view of life and death. In Loved Ones Live on: The Wisdom of the East. Edited by C. Becker. Kyoto: Koyo Shobo Corporation, pp. 1–25. ISBN 978-4-7710-2535-6. (In Japanese) [Google Scholar]
- Boynton, Robert. M. 1979. Human Color Vision. New York: Holt, Rinehart and Winston. [Google Scholar]
- Cabinet Office. 1995. The Basic Law on Measures for the Aging Society; Law No. 129; Tokyo: Cabinet Office. Available online: https://www8.cao.go.jp/kourei/english/measure/kihon-e.html (accessed on 5 January 2019).
- Cabinet Office. 2017a. Annual Report on the Aging Society; [Summary] FY2017; Tokyo: Cabinet Office, pp. 27–28. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2017/2017pdf_e.html (accessed on 5 January 2019).
- Cabinet Office. 2017b. Annual Report on the Aging Society, The entire ed.; FY2017; Tokyo: Cabinet Office, pp. 29–31, Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2017/zenbun/pdf/1s2s_03.pdf and https://www8.cao.go.jp/kourei/whitepaper/w-2017/zenbun/pdf/1s2s_04.pdf. (accessed on 5 January 2019). (In Japanese)
- Cummings, Jeffrey, Garam Lee, Travis Mortsdorf, Aaron Ritter, and Kate Zhong. 2017. Alzheimer’s disease drug development pipeline: 2017. Alzheimer’s & Dementia (New York, N. Y.) 3: 367–84. [Google Scholar] [CrossRef]
- Deci, Edward L., and Richard M. Ryan. 2000. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychological Inquiry 11: 227–68. [Google Scholar] [CrossRef]
- Dehghan, Mahshid, Andrew Mente, Xiaohe Zhang, Sumathi Swaminathan, Wei Li, Viswanathan Mohan, Romaina Iqbal, Rajesh Kumar, Edelweiss Wentzel-Viljoen, Annika Rosengren, and et al. 2017. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): A prospective cohort study. The Lancet 390: 2050–62. [Google Scholar] [CrossRef]
- Doya, Kenji. 2000. Reinforcement learning in continuous time and space. Neural Computation 12: 219–45. [Google Scholar] [CrossRef] [PubMed]
- Estruch, Ramon, Emilio Ros, Jordi Salas-Salvadó, María-Isabel Covas, Dolores Corella, Fernando Arós, Enrique Gomez-Gracia, Valentina Ruiz-Gutierrez, Miquel Fiol, Jose Lapetra, and et al. 2013. Primary prevention of cardiovascular disease with a Mediterranean diet. New England Journal of Medicine 368: 1279–90. [Google Scholar] [CrossRef]
- Estruch, Ramón, Emilio Ros, Jordi Salas-Salvadó, María-Isabel Covas, Dolores Corella, Fernando Arós, Enrique Gomez-Gracia, Valentina Ruiz-Gutierrez, Miquel Fiol, Jose Lapetra, and et al. 2018. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. New England Journal of Medicine 378: e34. [Google Scholar] [CrossRef] [PubMed]
- Euglena Co., Ltd. 2018. Press Release: Japan’s First Biojet and Diesel Fuel Production Demonstration Plant Was Completed and Euglena Co., Ltd. Declare “GREEN OIL JAPAN” Aiming to Make Japan a Biofuel Developed Country. Available online: https://www.euglena.jp/news/20181102-2/ (accessed on 5 January 2019).
- Finkel, Toren, Manuel Serrano, and Maria A. Blasco. 2007. The common biology of cancer and ageing. Nature 448: 767–74. [Google Scholar] [CrossRef] [PubMed]
- Forshaw, Roger J. 2009. The practice of dentistry in ancient Egypt. British Dental Journal 206: 481–86. [Google Scholar] [CrossRef] [PubMed]
- Fried, Linda P., Catherine M. Tangen, Jeremy Walston, Anne B. Newman, Calvin Hirsch, John Gottdiener, Teresa Seeman, Russell Tracy, Willem J. Kop, Gregory Burke, and et al. 2001. Frailty in older adults: Evidence for a phenotype. The Journals of Gerontology Series A Biological Sciences and Medical Sciences 56: M146–M157. [Google Scholar] [CrossRef]
- Fujita, Masahiro, and Koji Kageyama. 1997. An Open Architecture for Robot Entertainment. Paper presented at the AGENTS ’97: Proceeding of the First International Conference on Autonomous Agents, Marina del Rey, CA, USA, February 5–8; pp. 435–42, ISBN 0-89791-877-0. [Google Scholar]
- Fukuda, Tomohiro, Yoshihiro Tanaka, Michitaka Fujiwara, and Akihito Sano. 2015. Softness measurement by forceps-type tactile sensor using acoustic reflection. Paper presented at the IEEE/RSJ International Conference on Intelligent Robots and Systems, Hamburg, Germany, September 28–October 2. [Google Scholar]
- Fukuda, Tomohiro, Yoshihiro Tanaka, Michitaka Fujiwara, Akihito Sano, and Astrid M. L. Kappers. 2018. Visual and tactile feedback for a direct-manipulating tactile sensor in laparoscopic palpation. The International Journal of Medical Robotics and Computer Assisted Surgery 14: E1879. [Google Scholar] [CrossRef]
- Gijsbers, Lieke, Eric L. Ding, Vasanti S. Malik, Janette De Goede, Johanna M. Geleijnse, and Sabita S. Soedamah-Muthu. 2016. Consumption of dairy foods and diabetes incidence: A dose-response meta-analysis of observational studies. The American Journal of Clinical Nutrition 103: 1111–24. [Google Scholar] [CrossRef] [PubMed]
- Göran, Schildt, and Alvar Aalto. 1994. The Complete Catalogue of Architecture, Design and Art. New York: Rizzoli International Publications, ISBN 978-0-84781-818-1. [Google Scholar]
- Gotoh, Takahiko, Kazumasa Yamada, Akihiro Ito, Hong Yin, Tsuyoshi Kataoka, and Kiyohiko Dohi. 1998a. Chemoprevention of N-Nitroso-N-methylurea-induced rat mammary cancer by miso and tamoxifen, alone and in combination. Japanese Journal of Cancer Research 89: 487–95. [Google Scholar] [CrossRef]
- Gotoh, Takahiko, Kazumasa Yamada, Akihiro Ito, Hong Yin, Tsuyoshi Kataoka, and Kiyohiko Dohi. 1998b. Chemoprevention of N-Nitroso-N-methylurea-induced rat mammary carcinogenesis by soy foods or biochanin A. Japanese Journal of Cancer Research 89: 137–42. [Google Scholar] [CrossRef]
- Ha, Lisa, Truls Hauge, Anne Bente Spenning, and Per Ole Iversen. 2010. Individual, nutritional support prevents undernutrition, increases muscle strength and improves QoL among elderly at nutritional risk hospitalized for acute stroke: A randomized, controlled trial. Clinical Nutrition 29: 567–73. [Google Scholar] [CrossRef]
- HAS (Haute Autorité de Santé). 2016. La Plaine-Saint-Denis, Ile-De-France, France. COMMISSION DE LA TRANSPARENCE Avis 19 Octobre 2016. Available online: https://www.has-sante.fr/portail/upload/docs/application/pdf/2016-10/aricept_pic_reev_ri_avispostaud_ct15053.pdf (accessed on 5 January 2019).
- Health and Welfare Bureau for the Elderly, Ministry of Health, Labour and Welfare, Japan. 2016. Long-Term Care Insurance System of Japan. Available online: https://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/dl/ltcisj_e.pdf (accessed on 5 January 2019).
- Hipocrates. 1963. On Ancient Medicine and Other 8 Episodes. Tokyo: Iwanami Shoten, Publishers, ISBN 4003390113. (In Japanese) [Google Scholar]
- Hirazawa, Hirotaka, Shoko Ando, Takako Mitsuyuki, Yoko Yamamoto, Hiromi Kuroda, Kazumasa Yamada, and Goro Obinata. 2015. Usefulness of “Tablet PC application for Pain Memory” on cancer pain assessment. Palliative Care Research 10: 312–17. [Google Scholar] [CrossRef]
- Hirose, Michitaka, and Koichi Hirota. 1993. Surface display and synthetic force sensation. Advances in Human Factors/Ergonomics 19: 645. [Google Scholar]
- Hirota, Koichi, and Michitaka Hirose. 1995. Surface display: Presentation of curved surface in virtual reality environment. Advances in Human Factors/Ergonomics 20: 461–65. [Google Scholar] [CrossRef]
- Hirota, Koichi, and Michitaka Hirose. 1998. Implementation of partial surface display. Presence 7: 638–49. [Google Scholar] [CrossRef]
- Hoekstra, Jellie C., Jon H. M. Goosen, G. Sander De Wolf, and Cees C. P. M. Verheyen. 2011. Effectiveness of multidisciplinary nutritional care on nutritional intake, nutritional status and quality of life in patients with hip fractures: A controlled prospective cohort study. Clinical Nutrition 30: 455–61. [Google Scholar] [CrossRef] [PubMed]
- Hokama, Masaaki, Sugako Oka, Julio Leon, Toshiharu Ninomiya, Hiroyuki Honda, Kensuke Sasaki, Toru Iwaki, Tomoyuki Ohara, Tomio Sasaki, Frank M. LaFerla, and et al. 2014. Altered expression of diabetes-related genes in Alzheimer’s disease brains: The Hisayama study. Cerebral Cortex 24: 2476–88. [Google Scholar] [CrossRef]
- Hori, Megumi, Tomohiro Matsuda, Akiko Shibata, Kota Katanoda, Tomotaka Sobue, and Hiroshi Nishimoto. 2015. Cancer incidence and incidence rates in Japan in 2009: A study of 32 population-based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Japanese Journal of Clinical Oncology 45: 884–91. [Google Scholar] [CrossRef] [PubMed]
- Ito, Yuji, Youngwoo Kim, and Goro Obinata. 2011a. Robust slippage degree estimation based on reference update of vision-based tactile sensor. IEEE Sensors Journal 11: 2037–204. [Google Scholar] [CrossRef]
- Ito, Yuji, Youngwoo Kim, Chikara Nagai, and Goro Obinata. 2011b. Contact state estimation by vision-based tactile sensors for dexterous manipulation with robot hands based on shape-sensing. International Journal of Advanced Robotic Systems 8: 225–34. [Google Scholar] [CrossRef]
- Iwata, Michinori. 1993. Encyclopedia Nipponica 2001. Tokyo: Shogakukan, ISBN 978-4-09526-930-6. (In Japanese) [Google Scholar]
- Jack, Clifford R., David S. Knopman, William J. Jagust, Leslie M. Shaw, Paul S. Aisen, Michael W. Weiner, Ronald C. Petersen, and John Q. Trojanowski. 2010. Hypothetical model of dynamic biomarkers of the Alzheimer’s pathological cascade. The Lancet Neurology 9: 119–28. [Google Scholar] [CrossRef]
- Jagger, Carol, Fiona E. Matthews, Pia Wohland, Tony Fouweather, Blossom C. M. Stephan, Louise Robinson, Antony Arthur, and Carol Brayne. 2016. A comparison of health expectancies over two decades in England: Results of the Cognitive Function and Ageing Study I and II. The Lancet 387: 779–86. [Google Scholar] [CrossRef]
- Kaneko, Takayoshi. 1988. Color Science. Tokyo: Iwanami Shoten, Publishers, ISBN 978-400430041. (In Japanese) [Google Scholar]
- Kaneko, Takayoshi. 1995. Color Science: Its Psychology, Physiology, and Physics. Tokyo: Asakura Publishing Co., Ltd., ISBN 978-4-254-10537-7. (In Japanese) [Google Scholar]
- Katō, Shūichi. 2007. Heibonsha’s World Encyclopedia. Tokyo: Heibonsha, ISBN 978-4-58203-400-4. (In Japanese) [Google Scholar]
- Katz, David. 1935. The World of Colour. Translated from the 2nd German ed. (1930) by R. B. MacLeod and C. W. Fox. London: Kegan Paul, Trench, Trubner & Co. Ltd. [Google Scholar]
- Kawai, Motoko, and Shingoro Matsuura. 1997. Manda suppresses emotional stress-induced stomach ulcer in rats. International Journal of Stress Management 4: 63–69. [Google Scholar] [CrossRef]
- Kawai, Motoko, Shingoro Matsuura, Masato Asanuma, and Norio Ogawa. 1998. Manda, a fermented natural food, suppresses lipid peroxidation in the senescent rat brain. Neurochemical Research 23: 455–61. [Google Scholar] [CrossRef]
- Kawato, Mitsuo, Kazunori Furukawa, and Ryoji Suzuki. 1987. A hierarchical neural-network model for control and learning of voluntary movement. Biological Cybernetics 57: 169–85. [Google Scholar] [CrossRef]
- Kishimoto, Hiro, Tomoyuki Ohara, Jun Hata, Toshiharu Ninomiya, Daigo Yoshida, Naoko Mukai, Masaharu Nagata, Fumie Ikeda, Masayo Fukuhara, Shuzo Kumagai, and et al. 2016. The long-term association between physical activity and risk of dementia in the community: The Hisayama Study. European Journal of Epidemiology 31: 267–74. [Google Scholar] [CrossRef] [PubMed]
- Klotz, Robert E., and Marjorie Kilbane. 1962. Hearing in an aging population. Preliminary report. New England Journal of Medicine 266: 277–80. [Google Scholar] [CrossRef]
- Laotze. 2008. Laotze (Japanese). Tokyo: Iwanami Shoten, ISBN 978-4-00-332051-8. [Google Scholar]
- Lin, Frank R., E. Jeffrey Metter, Richard J. O’Brien, Susan M. Resnick, Alan B. Zonderman, and Luigi Ferrucci. 2011. Hearing loss and incident dementia. Archives of Neurology 68: 214–20. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, David S., and Mark I. Friedman. 2014. Increasing adiposity: Consequence or cause of overeating? JAMA 311: 2167–68. [Google Scholar] [CrossRef] [PubMed]
- Ly, Hiep Hoang, Yoshihiro Tanaka, Akihito Sano, and Tomohiro Fukuda. 2017. Grasper having tactile sensing function using acoustic reflection for laparoscopic surgery. International Journal of Computer Assisted Radiology and Surgery 12: 1333–43. [Google Scholar] [CrossRef] [PubMed]
- Marotta, Francesco, Hariom Yadav, S. Pathak, E. Minelli, Paola Signorelli, A. Lorenzetti, and P. Marandola. 2009. Inhibition of human breast cancer cell growth and enzymatic activity by a fermented nutraceutical. Annals of the New York Academy of Sciences 1155: 273–77. [Google Scholar] [CrossRef]
- Matthews, Fiona E., Antony Arthur, Linda E. Barnes, John Bond, Carol Jagger, Louise Robinson, and Carol Brayne. 2013. A two-decade comparison of prevalence of dementia in individuals aged 65 years and older from three geographical areas of England: Results of the Cognitive Function and Ageing Study I and II. The Lancet 382: 1405–12. [Google Scholar] [CrossRef]
- Matthews, Fiona E., Blossom C. M. Stephan, Louise Robinson, Carol Jagger, Linda E. Barnes, Antony Arthur, Carol Brayne, and Cognitive Function and Ageing Studies (CFAS) Collaboration. 2016. A two decade dementia incidence comparison from the Cognitive Function and Ageing Studies I and II. Nature Communications 7: 11398. [Google Scholar] [CrossRef] [Green Version]
- McNeely, William A. 1993. Robotic Graphics: A New Approach to Force Feedback for Virtual Reality. Paper presented at the VRAIS ’93, Seattle, WA, USA, September 18–22; pp. 336–41. [Google Scholar]
- Miki, Kiyoshi. 1980. Human Study on Pascal. Tokyo: Iwanami Shoten, Publishers, ISBN 4-00-331491-3. (In Japanese) [Google Scholar]
- Ministère des Solidarités et de la Santé, Duquesne, Paris, France. 2018. Press Release Jun 1. Available online: https://solidarites-sante.gouv.fr/IMG/pdf/cp_dss-dgs_alzheimer_01_06_18.pdf (accessed on 5 January 2019).
- Ministry of Internal Affairs and Communications Statistics Bureau, Japan. 2018. News Bulletin. Available online: https://www.stat.go.jp/english/info/news/pdf/20181130.pdf (accessed on 5 January 2019).
- Mizuno, Kouichi, Masuo Awata, Kazuyoshi Tominaga, Eitaro Mizutani, Kazuo Oyake, Kazumasa Yamada, and Mikiko Yamada. 2014. Citizen Research Report of Nagoya Urban Institute Research Reports. pp. 75–76. Available online: http://www.nup.or.jp/nui/user/media/document/investigation/h25/shimin.pdf (accessed on 5 January 2019). (In Japanese).
- Mizuno, Kouichi, Masuo Awata, Kazuyoshi Tominaga, Eitaro Mizutani, Kazuo Oyake, and Kazumasa Yamada. 2015. Secreted Nagoya: Treasure Town You Want to Visit. Nagoya: Fubaisha, Inc., ISBN 978-4-8331-0166-0. (In Japanese) [Google Scholar]
- Mizusawa, Tsutomu, Marc Zehntner, Mateo Kries, Tommi Lindh, Jochen Eisenbrand, Nahoko Wada, Masao Momiyama, Anni Hayashi, Jun Matsumoto, Yoshinori Kakino, and et al. 2018. Alvar Aalto: Second Nature. Edited by N. Wada. Tokyo: TOTO Kokushokankoukai, Inc., ISBN 978-4-336-06289-5. [Google Scholar]
- Nakamura, Yu, Yukimichi Imai, Masahiro Shigeta, Ana Graf, Toru Shirahase, Hyosung Kim, Akifumi Fujii, Joji Mori, and Akira Homma. 2011. A 24-week, randomized, double-blind, placebo-controlled study to evaluate the efficacy, safety and tolerability of the rivastigmine patch in Japanese patients with Alzheimer’s disease. Dementia and Geriatric Cognitive Disorders Extra 1: 163–79. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Akinori, Naoki Kaneko, Victor L. Villemagne, Takashi Kato, James Doecke, Vincent Doré, Chris Fowler, Qiao-Xin Li, Ralph Martins, Christopher Rowe, and et al. 2018. High performance plasma amyloid-beta biomarkers for Alzheimer’s disease. Nature 554: 249–54. [Google Scholar] [CrossRef]
- Nakata, Hiroki, Koji Inui, Toshiaki Wasaka, Yohei Tamura, Tuan Diep Tran, Yunhai Qiu, Xiaohong Wang, Thi Binh Nguyen, and Ryusuke Kakigi. 2004. Movements modulate cortical activities evoked by noxious stimulation. Pain 107: 91–98. [Google Scholar] [CrossRef]
- Ninomiya, T., T. Ohara, Y. Hirakawa, D. Yoshida, Y. Doi, J. Hata, S. Kanba, T. Iwaki, and Y. Kiyohara. 2011. Midlife and late-life blood pressure and dementia in Japanese elderly: The Hisayama study. Hypertension 58: 22–28. [Google Scholar] [CrossRef] [PubMed]
- Nordrum, Amy. 2019. Cyberdyne’s HAL Exoskeleton Helps Patients Walk again in First Treatments at U.S. Facility. Available online: https://spectrum.ieee.org/the-human-os/biomedical/bionics/cyberdynes-hal-medical-exoskeleton-helps-patients-walk-again-at-first-us-facility (accessed on 15 January 2019).
- Ohayon, Maurice M., Mary A. Carskadon, Christian Guilleminault, and Michael V. Vitiello. 2004. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: Developing normative sleep values across the human lifespan. Sleep 27: 1255–73. [Google Scholar] [CrossRef]
- Okumura, Yasuyuki, and Nobuo Sakata. 2018. Antidementia drug use in Japan: Bridging the research-to-practice gap. International Journal of Geriatric Psychiatry. [Google Scholar] [CrossRef]
- Onodera, Takeshi, and Kiyoshi Toko. 2014. Towards an electronic dog nose: Surface plasmon resonance immunosensor for security and safety. Sensors 14: 16586–616. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, Kenichi, Izumi Kondo, Satoshi Hirano, Hitoshi Kagaya, Eiichi Saitoh, Aiko Osawa, and Yoichi Fujinori. 2017. Training with a balance exercise assist robot is more effective than conventional training for frail older adults. Geriatrics & Gerontology International 17: 1982–990. [Google Scholar] [CrossRef]
- Ozawa, Mio, Toshiharu Ninomiya, Tomoyuki Ohara, Yasufumi Doi, Kazuhiro Uchida, Tomoko Shirota, Koji Yonemoto, Takanari Kitazono, and Yutaka Kiyohara. 2013. Dietary patterns and risk of dementia in an elderly Japanese population: The Hisayama Study. The American Journal of Clinical Nutrition 97: 1076–82. [Google Scholar] [CrossRef]
- Petersen, Ronald C., Glenn E. Smith, Stephen C. Waring, Robert J. Ivnik, Eric G. Tangalos, and Emre Kokmen. 1999. Mild cognitive impairment: Clinical characterization and outcome. Archives of Neurology 56: 303–8. [Google Scholar] [CrossRef]
- Pfeiffer, Bruce Brooks. 1989. Frank Lloyd Wright Selected Houses 3: Taliesin West. Tokyo: A.D.A. Edita, ISBN 4-87140-545-1. [Google Scholar]
- Pollock, Ross D., Finbarr C. Martin, and Di J. Newham. 2012. Whole-body vibration in addition to strength and balance exercise for falls-related functional mobility of frail older adults: A single-blind randomized controlled trial. Clinical Rehabilitation 26: 915–23. [Google Scholar] [CrossRef] [PubMed]
- Redcord AS. 2014. Available online: https://redcord.com/ (accessed on 22 February 2019).
- Saito, Yutaka. 2008. Aalto: 10 Selected Houses. Tokyo: Tōtōshuppan, ISBN 978-4-88706-290-0. [Google Scholar]
- Saji, Naoki, and Takashi Sakurai. 2017. Is gait speed a risk factor for dementia? Geriatrics & Gerontology International 17: 75–76. [Google Scholar] [CrossRef] [Green Version]
- Saji, Naoki, Takashi Sakurai, Keisuke Suzuki, Hidehiro Mizusawa, and Kenji Toba. 2016. ORANGE’s challenge: Developing wide-ranging dementia research in Japan. The Lancet Neurology 15: 661–62. [Google Scholar] [CrossRef]
- Sakakibara, Hiroyuki, Michiko Torii Yasuda, and Kayoko Shimoi. 2016. Effects of environmental and social stressors on biological rhythms. The Journal of Physical Fitness and Sports Medicine 5: 143–52. [Google Scholar] [CrossRef]
- Salas-Salvadó, Jordi, Marta Guasch-Ferre, Andres Díaz-López, and Nancy Babio. 2017. Yogurt and diabetes: Overview of recent observational studies. The Journal of Nutrition 147: 1452S–1461S. [Google Scholar] [CrossRef]
- Samochocki, Marek, Anja Höffle, Andreas Fehrenbacher, Ruth Jostock, Jurgen Ludwig, Claudia Christner, Martin Radina, Marion Zerlin, Christoph Ullmer, Edna F. R. Pereira, and et al. 2003. Galantamine is an allosterically potentiating ligand of neuronal nicotinic but not of muscarinic acetylcholine receptors. Journal of Pharmacology and Experimental Therapeutics 305: 1024–36. [Google Scholar] [CrossRef]
- Sannai-Maruyama Special Historical Site. 2013. Available online: http://sannaimaruyama.pref.aomori.jp/english/ (accessed on 15 January 2019).
- Sano, Akihito. 2017. ACSIVE: A Non-powered Gait Assist Suit Based on Passive Walking. Spinal Surgery 31: 242–45. [Google Scholar] [CrossRef]
- Schumaker, John F. 1991. The adaptive value of suggestibility and dissociation. In Human Suggestibility: Advances in Theory, Research, and Application. Edited by J. F. Schumaker. Florence: Taylor & Frances/Routledge, pp. 108–31. ISBN 978-0415902151. [Google Scholar]
- Schumaker, John F., William G. Warren, and Gary Groth-Marnat. 1991. Death anxiety in Japan and Australia. The Journal of Social Psychology 131: 511–18. [Google Scholar] [CrossRef] [PubMed]
- Seelig, Tina. 2013. What I Wish I Knew When I Was 20. Tokyo: CCC Media House Co., Ltd., ISBN 978-4-4841-0101-9. (In Japanese) [Google Scholar]
- Shimada, Hiroyuki, Hyuma Makizako, Takehiko Doi, Daisuke Yoshida, Kota Tsutsumimoto, Yuya Anan, Kazuki Uemura, Tadashi Ito, Sangyoon Lee, Hyuntae Park, and et al. 2013. Combined prevalence of frailty and mild cognitive impairment in a population of elderly Japanese people. Journal of the American Medical Directors Association 14: 518–24. [Google Scholar] [CrossRef]
- Shimada, Hiroyuki, Kenji Ishii, Hyuma Makizako, Kiichi Ishiwata, Keiichi Oda, and Megumi Suzukawa. 2017. Effects of exercise on brain activity during walking in older adults: A randomized controlled trial. Journal of Neuroengineering and Rehabilitation 14. [Google Scholar] [CrossRef]
- Shimada, Hiroyuki, Hyuma Makizako, Takehiko Doi, Hyuntae Park, Kota Tsutsumimoto, Joe Verghese, and Takao Suzuki. 2018. Effects of combined physical and cognitive exercises on cognition and mobility in patients with mild cognitive impairment: A randomized clinical trial. Journal of the American Medical Directors Association 19: 584–91. [Google Scholar] [CrossRef] [PubMed]
- Shimoda, Katsuhiro. 1995. A study of audiologic findings in the elderly. Nihon Jibiinkoka Gakkai Kaiho 98: 1426–39. [Google Scholar] [CrossRef]
- Shimoda, Shingo, and Hidenori Kimura. 2010. Biomimetic approach to tacit learning based on compound control. IEEE Transactions on Systems, Man and Cybernetics, Part B (Cybernetics) 40: 77–90. [Google Scholar] [CrossRef] [PubMed]
- Shimoda, Shingo, Yuki Yoshihara, and Hidenori Kimura. 2013. Adaptability of tacit learning in bipedal locomotion. IEEE Transactions on Autonomous Mental Development 5: 152–61. [Google Scholar] [CrossRef]
- Shimonaka, Kunihiko. 1964. Heibonsha’s World Encyclopedia. Tokyo: Heibonsha. (In Japanese) [Google Scholar]
- Shinotoh, Hitoshi, Hitoshi Shimada, Yasumasa Kokubo, Kenji Tagai, Fumitoshi Niwa, Soichiro Kitamura, Hironobu Endo, Maiko Ono, Yasuyuki Kimura, Shigeki Hirano, and et al. 2019. Tau imaging detects distinctive distribution of tau pathology in ALS/PDC on the Kii Peninsula. Neurology 92: e136–e147. [Google Scholar] [CrossRef]
- Snowdon, David A. 1997. Aging and Alzheimer’s disease: Lessons from the Nun Study. Gerontologist 37: 150–56. [Google Scholar] [CrossRef]
- Snowdon, David A., Susan J. Kemper, James A. Mortimer, Lydia H. Greiner, David R. Wekstein, and William R. Markesbery. 1996. Linguistic ability in early life and cognitive function and Alzheimer’s disease: Findings from the Nun Study. JAMA 275: 528–32. [Google Scholar] [CrossRef] [PubMed]
- Snowdon, David A., Lydia H. Greiner, James A. Mortimer, Kathryn P. Riley, and William R. Markesbery. 1997. Brain infarction and the clinical expression of Alzheimer disease: The Nun Study. JAMA 277: 813–17. [Google Scholar] [CrossRef] [PubMed]
- Tahara, Yusuke, and Kiyoshi Toko. 2013. Electronic Tongues—A Review. IEEE Sensors Journal 13: 3001–11. [Google Scholar] [CrossRef]
- Tanabe, Seiichi. 1975. Britannica International Encyclopædia. Tokyo: TBS-Britannica Co., Ltd. (In Japanese) [Google Scholar]
- Tanaka, Yoshihiro, Shuji Aragaki, Tomohiro Fukuda, Michitaka Fujiwara, and Akihito Sano. 2014. A study on tactile display for haptic sensing system with sensory feedback for laparoscopic surgery. Paper presented at the 25th International Symposium on Micro-Nanomechatronics and Human Science, Nagoya, Japan, November 10–12. [Google Scholar]
- Tanaka, Yoshihiro, Tomohiro Fukuda, Michitaka Fujiwara, and Akihito Sano. 2015. Tactile sensor using acoustic reflection for lump detection in laparoscopic surgery. International Journal of Computer Assisted Radiology and Surgery 10: 183–93. [Google Scholar] [CrossRef]
- Tanaka, Yoshihiro, Yuichiro Udeda, and Akihito Sano. 2016a. Roughness evaluation by wearable tactile sensor utilizing human active sensing. Mechanical Engineering Journal 3: 15-00460. [Google Scholar] [CrossRef]
- Tanaka, Yoshihiro, Yuki Goto, and Akihito Sano. 2016b. Haptic display of micro surface undulation based on discrete mechanical stimuli to whole fingers. Advanced Robotics 31: 155–67. [Google Scholar] [CrossRef]
- Tanaka, Eiichiro, Keiichi Muramatsu, Yusuke Osawa, Shozo Saegusa, Louis Yuge, and Keiichi Watanuki. 2017. A Walking Promotion Method Using the Tuning of a Beat Sound Based on a Two-Dimensional Emotion Map. In Advances in Affective and Pleasurable Design, Proceedings of the AHFE 2016 International Conference on Affective and Pleasurable Design, Orlando, FL, USA, 27–31 July 2016. Edited by W. Chung and C. Shin. Cham: Springer International Publishing, Advances in Intelligent Systems and Computing, vol. 483, pp. 519–25. [Google Scholar] [CrossRef]
- Tariot, Pierre N., Martin R. Farlow, George T. Grossberg, Stephen M. Graham, Scott McDonald, Ivan Gergel, and for the Memantine Study Group. 2004. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: A randomized controlled trial. JAMA 291: 317–24. [Google Scholar] [CrossRef]
- Taylor, Anne. 2009. Linking Architecture and Education: Sustainable Design of Learning Environments. Albuquerque: University of New Mexico Press, ISBN 978-0-8263-3407-7. [Google Scholar]
- Taylor, Anne, Alison Marshal, and George Vlastos. 1991. Architecture and Children: Teachers Guide. Washington: Architecture and Children Institute, ISBN 0-913947-06-7. [Google Scholar]
- The Fifth Generation Mobile Communications Promotion Forum (5GMF). 2017. 5GMF White Paper “5G Mobile Communications Systems for 2020 and beyond” Ver. 1.1. September 29. Available online: https://5gmf.jp/en/ (accessed on 5 January 2019).
- Thomas, Kali S., Rosa Baier, Cyrus Kosar, Jessica Ogarek, Alissa Trepman, and Vincent Mor. 2017. Individualized music program is associated with improved outcomes for US nursing home residents with dementia. The American Journal of Geriatric Psychiatry 25: 931–38. [Google Scholar] [CrossRef]
- Toko, Kiyoshi. 2013. Biochemical Sensors: Mimicking Gustatory Senses. Boca Raton: Taylor & Francis Group, LLC, ISBN 978-981-4303-42-2. [Google Scholar]
- Uchida, Yasue, Saiko Sugiura, Fujiko Ando, Tsutomu Nakashima, and Hiroshi Shimokata. 2012. Estimates of the size of the hearing-impaired elderly population in Japan and 10-year incidence of hearing loss by age, based on data from the National Institute for Longevity Sciences-Longitudinal Study of Aging (NILS-LSA). Nihon Ronen Igakkai Zasshi 49: 222–27. [Google Scholar] [CrossRef]
- Uchikawa, Keiji. 1998. Color-Vision Mechanism: Mechanism to Look at Colors. Tokyo: Asakura Publishing Co. Ltd., ISBN 978-4-254-10540-7. (In Japanese) [Google Scholar]
- United Nations, Department of Economic and Social Affairs, Population Division. 2017. World Population Prospects: The 2017 Revision: Volume 1: Comprehensive Tables. ST/ESA/SER.A/399. New York: United Nations, Department of Economic and Social Affairs, Population Division, pp. 168–205. Available online: https://population.un.org/wpp/Publications/Files/WPP2017_Volume-I_Comprehensive-Tables.pdf (accessed on 5 January 2019).
- United Nations, Department of Public Information. 2015. Transforming Our World: The 2030 Agenda for Sustainable Development. New York: United Nations, Department of Public Information, Available online: https://sustainabledevelopment.un.org/content/documents/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf (accessed on 5 January 2019).
- Verghese, Joe, Richard B. Lipton, Mindy J. Katz, Charles B. Hall, Carol A. Derby, Gail Kuslansky, Anne F. Ambrose, Martin Sliwinski, and Herman Buschke. 2003. Leisure activities and the risk of dementia in the elderly. New England Journal of Medicine 348: 2508–16. [Google Scholar] [CrossRef]
- Vinoo, Deepa, Jove May Santos, Milana Leviyev, Paul Quimbo, Jennifer Dizon, Frankie Diaz, Christopher Wittman, Ioana Dulgheru, Robert Hughes, Leah Matias, and et al. 2017. Music and memory in dementia care. International Journal of Neurorehabilitation 4. [Google Scholar] [CrossRef]
- Wang, Hongfeng, Shengxiang Yang, W. H. Ip, and Dingwei Wang. 2009. Adaptive primal-dual genetic algorithms in dynamic environments. IEEE Transactions on Systems, Man, and Cybernetics, Part B 39: 1348–61. [Google Scholar] [CrossRef]
- Wang, Xia, Xinying Lin, Ying Y. Ouyang, Jun Liu, Gang Zhao, An Pan, and Frank B. Hu. 2016. Red and processed meat consumption and mortality: Dose-response meta-analysis of prospective cohort studies. Public Health Nutrition 19: 893–905. [Google Scholar] [CrossRef] [PubMed]
- Wijk, Helle, Stig Berg, Lars Sivik, and Bertil Steen. 1999. Colour discrimination, colour naming and colour preferences among individuals with Alzheimer’s disease. International Journal of Geriatric Psychiatry 14: 1000–5. [Google Scholar] [CrossRef]
- Winblad, Bengt, Lena Kilander, Sture Eriksson, Lennart Minthon, Stellan Båtsman, Anna-Lena Wetterholm, Catarina Jansson-Blixt, and Anders Haglund. 2006. Donepezil in patients with severe Alzheimer’s disease: Double-blind, parallel-group, placebo-controlled study. The Lancet 367: 1057–65. [Google Scholar] [CrossRef]
- Wright, Frank Lloyd. 1957. A Testament. New York: Horizon Press, ISBN 978-1-1312-9178-9. [Google Scholar]
- Wyszecki, G., and W. S. Stiles. 1982. Color Science: Concepts and Methods, Quantitative Data and Formulae, 2nd ed.New York: John Wiley and Sons. [Google Scholar]
- Yamada, Kazumasa, Hitomi Inoue, Misa Hagino, and Goro Obinata. 2013. Assist for consonant discriminative ability of early stage presbycusis by using a new type of non-electric hearing aid. Paper presented at the Society of Instrument and Control Engineers (SICE) Annual Conference 2013, Nagoya, Japan, September 14–17; pp. 1604–5, ISBN 978-4-907764-43-2. [Google Scholar]
- Yamada, Kazumasa, Norio Sugimoto, and Kenta Murotani. 2017. Handbook of Statistical Analysis: Visually Understanding and Choosing a Statistical Method. Tokyo: The Chemical Daily Co., Ltd., ISBN 978-4-87326-692-3. (In Japanese) [Google Scholar]
- Zaoba Corporation. 2012. Available online: http://zaoba.co.jp/ (accessed on 22 February 2019).
- Zhao, Qinying, Martin Brett, Nancy Van Osselaer, Fenglei Huang, Alain Raoult, Achiel Van Peer, Tom Verhaeghe, and Rita Hust. 2002. Galantamine pharmacokinetics, safety, and tolerability profiles are similar in healthy Caucasian and Japanese subjects. The Journal of Clinical Pharmacology 42: 1002–10. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Jyun Rong, Ya Jing Guan, Hayato Nagayoshi, Louis Yuge, HeeHyol Lee, and Eiichiro Tanaka. 2019. Two-Dimensional Emotion Evaluation with Multiple Physiological Signals. In Advances in Affective and Pleasurable Design, Proceedings of the AHFE 2018 International Conference on Affective and Pleasurable Design. Edited by S. Fukuda. Cham: Springer International Publishing, Advances in Intelligent Systems and Computing, vol. 774, pp. 158–68. [Google Scholar] [CrossRef]
Figure 1.
Countries or areas with the highest life expectancy at birth, before and after ten years.

Figure 2.
The developing market of welfare products in Japan.

Figure 3.
The nonprofit organization (NPO) Sawayaka-Aichi in a Japanese suburb.

Figure 4.
Functional areas of Sawayaka Town. Illustration: Sawayaka-Aichi brochure (used with permission and translated by the author).
Figure 4.
Functional areas of Sawayaka Town. Illustration: Sawayaka-Aichi brochure (used with permission and translated by the author).

Figure 5.
Challenge of an expiring, nearly extinct community in a rural mountain area of Japan.

Figure 6.
Technology adoption and inventions in Japan.

Figure 7.
A cluster of street stands in Singapore.

Figure 8.
Sannai-Maruyama special historical site in Japan.

Figure 9.
Non-electric hearing aids (Japanese Patent No. 6082676).

Figure 10.
Shape-sensing information: (a) positional information for the blind persons; (b) round tables are less suited for the blind but good for patients with amblyopia.
Figure 10.
Shape-sensing information: (a) positional information for the blind persons; (b) round tables are less suited for the blind but good for patients with amblyopia.

Figure 11.
Relationships between gerontology and geriatrics without cancers.

Figure 12.
Confusing changes for patients with dementia.

Figure 13.
Red or orange handrails in Sawayaka Town.

Figure 14.
Extrinsic and intrinsic motivation.

Figure 15.
Stretching devices (Redcord AS 2014) and hydraulic training gym (Zaoba Corporation 2012) in Sawayaka Town.
Figure 15.
Stretching devices (Redcord AS 2014) and hydraulic training gym (Zaoba Corporation 2012) in Sawayaka Town.

© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yamada, K. An Acquaintance with An Aging Society. Soc. Sci. 2019, 8, 110. https://doi.org/10.3390/socsci8040110
AMA Style
Yamada K. An Acquaintance with An Aging Society. Social Sciences. 2019; 8(4):110. https://doi.org/10.3390/socsci8040110
Chicago/Turabian StyleYamada, Kazumasa. 2019. "An Acquaintance with An Aging Society" Social Sciences 8, no. 4: 110. https://doi.org/10.3390/socsci8040110
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.