
Nanomedicines for Overcoming Cancer Drug Resistance




1
Department of Pharmacy, State Key Laboratory of Biotherapy and Cancer Center, National Clinical Research Center for Geriatrics, West China Hospital, Sichuan University, Chengdu 610041, China
2
Department of Integrated Traditional Chinese and Western Medicine, West China Hospital, Sichuan University, Chengdu 610041, China
3
Key Laboratory of Drug-Targeting and Drug Delivery System of the Education Ministry, Sichuan Engineering Laboratory for Plant-Sourced Drug and Sichuan Research Center for Drug Precision Industrial Technology, West China School of Pharmacy, Sichuan University, Chengdu 610041, China
*
Authors to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Pharmaceutics 2022, 14(8), 1606; https://doi.org/10.3390/pharmaceutics14081606
Submission received: 17 June 2022
/
Revised: 27 July 2022
/
Accepted: 29 July 2022
/
Published: 1 August 2022
(This article belongs to the Special Issue Drug Discovery and Drug Delivery System for Biological Application)
Abstract
:Clinically, cancer drug resistance to chemotherapy, targeted therapy or immunotherapy remains the main impediment towards curative cancer therapy, which leads directly to treatment failure along with extended hospital stays, increased medical costs and high mortality. Therefore, increasing attention has been paid to nanotechnology-based delivery systems for overcoming drug resistance in cancer. In this respect, novel tumor-targeting nanomedicines offer fairly effective therapeutic strategies for surmounting the various limitations of chemotherapy, targeted therapy and immunotherapy, enabling more precise cancer treatment, more convenient monitoring of treatment agents, as well as surmounting cancer drug resistance, including multidrug resistance (MDR). Nanotechnology-based delivery systems, including liposomes, polymer micelles, nanoparticles (NPs), and DNA nanostructures, enable a large number of properly designed therapeutic nanomedicines. In this paper, we review the different mechanisms of cancer drug resistance to chemotherapy, targeted therapy and immunotherapy, and discuss the latest developments in nanomedicines for overcoming cancer drug resistance.
1. Introduction
Chemotherapy, targeted therapy and immunotherapy are the mainstream of cancer therapy; however, the most important challenge in cancer treatment is the development of cancer drug resistance [1,2,3]. Depending on the factors behind it, cancer drug resistance can be divided into primary drug resistance and acquired drug resistance [4,5,6]. Primary drug resistance refers to a complete failure of response to initial antitumor therapy in patients with cancer [7]. Acquired resistance is defined as a cancer that initially responds to antitumor therapy but then relapses or progresses after a period of treatment [8]. The mechanisms of cancer drug resistance are very complex including increased drug outflow, reduced drug intake, drug inactivation, target mutations, altered signaling pathway, defective apoptosis, phenotypic transition, autophagy, gene mutations or amplification, T cell depletion, and antigen deletion [9,10,11,12,13,14]. With the further study of drug resistance mechanisms, cancer stem cells (CSCs) and the tumor microenvironment are also closely related to the development of cancer drug resistance [15,16,17,18]. Therefore, there is a pressing need to develop new methods to surmount cancer drug resistance [19,20,21]. In recent decades, nanomedicines have emerged as promising cancer treatment tools, focusing on the targeted delivery of antitumor agents to tumor site using nanosized formulations such as polymeric micelles, liposomes, polymeric nanoparticles, inorganic nanoparticles, hybrid nanoparticles, and polymeric nanogels. Liposomal nanoparticles have the advantages of good biocompatibility, a long circulation time, tumor targeting ability and controlled release and have become among the most promising drug delivery platforms. Several nanomedicines, including liposome products, are in clinical use (Table 1). Additionally, a variety of liposomal nanoparticles have been widely studied for overcoming cancer drug resistance, especially breast cancer. Since most anticancer drugs are hydrophobic, if injected directly into the circulation, they not only have low bioavailability, but also have great toxicity. To address this conundrum, biodegradable amphiphilic block copolymers have become an attractive carrier material, because they can encapsulate or conjugate anticancer agents and then self-assemble into stable core–shell and nanostructured particles called polymeric micelles or polymeric capsules. Polymeric nanogels are formed with an internal network structure through intermolecular or intramolecular crosslinking, which can enhance the solubility of anticancer drugs by encapsulating hydrophobic or hydrophilic anticancer drugs inside the crosslinking networks. In addition, they have shown delayed drug release or rapid drug release based on the crosslinker degradation in response to the tumor microenvironment (TME). A variety of polymeric nanoplatforms have been widely studied for overcoming cancer drug resistance, including breast cancer, ovarian cancer, pancreatic cancer, and glioblastoma. Inorganic nanoparticles, including gold nanoparticles and silicon nanoparticles, have become a research hotspot in imaging and drug delivery platforms due to their unique physical and chemical properties, easy fabrication, stability and high drug loading ability. A variety of inorganic nanoparticles have been widely studied for overcoming cancer drug resistance, especially breast cancer and hepatocellular carcinoma. Hybrid nanoparticles, including biocompatible polymer-coated inorganic nanoparticles, phospholipid-coated polymeric nanoparticles and biomimetic cell membrane-coated nanoparticles have the advantages of improved biocompatibility, enhanced stability, enhanced drug encapsulation and activated target capacity. A variety of hybrid nanoparticles have been widely studied for overcoming cancer drug resistance, including breast cancer, ovarian cancer, lung cancer, and melanoma. Nanomedicines have therefore been introduced as reliable strategies to improve therapeutic effectiveness, reduce harmful adverse reactions, as well as surmount cancer drug resistance [22,23,24,25]. Nanomedicines have paved the way for effective treatment of cancer by rationally designing strategies such as passive targeted drug delivery, active targeted drug delivery, co-delivery of combinatorial agents and multimodal combination therapy, and have broad prospects in overcoming drug resistance [26,27,28,29,30,31]. In this paper, we review the different mechanisms of cancer drug resistance to chemotherapy, targeted therapy and immunotherapy, and focus on the latest progress in nanomedicines for overcoming cancer drug resistance.
2. Nanomedicines against Drug Resistance in Chemotherapy
2.1. Mechanisms in Drug Resistance of Chemotherapy
Nowadays, chemotherapy is still the most widely used strategy for treating cancer; however, the biggest obstacle to this traditional strategy is the development of cancer drug resistance [43,44,45]. The mechanisms of drug resistance to chemotherapy are extremely complex [45] (Figure 1). Generally, the emergence of chemoresistance may be classified by the following pathways: (1) increased drug efflux by ATP-dependent pumps mediated by transmembrane transporters of the ATP-binding cassette (ABC) superfamily [46,47,48]; (2) reduced drug uptake mediated by altering specific cellular targets [49,50,51]; (3) inactivation of apoptotic pathways mediated by high expression of the Bcl-2 antiapoptotic family such as Bcl-2, Mcl-1 and Bcl-XL, which are mainly responsible for the reason why cancer cells can resist apoptosis [52,53,54]; (4) enhanced DNA repair ability that can contribute to the resistance of cancer by promoting genomic instability and mutation [55,56,57]; (5) alterations in specific drug targets [58,59]; (6) increased drug detoxification mediated by metabolism or biotransformation [11,60]. All in all, these resistance mechanisms can allow cancer cells to survive by easily changing different pathways, and ultimately resulting in chemotherapeutic failure.
2.2. Nanomedicines to Overcome Chemotherapy Resistance
Considering that chemotherapy resistance-related drug efflux proteins mainly reside in the nuclear membranes and blood, but not in the mitochondria [61,62], delivering chemotherapy agents into the mitochondria is an emerging strategy to surmount drug resistance to chemotherapy [63,64,65,66,67,68,69]. Yu et al. [70] constructed a weak acid-activated, charge-reversible, triphenylphosphonium (TPP)-based, “shell–core” nanosystem (DOX-PLGA/CPT/PD) for sequential facilitation of tumor accumulation, cellular uptake, mitochondria targeting, intracellular localization and surmounting drug resistance of MCF-7/ADR breast cancer (Figure 2a). Firstly, positively charged mitochondrial-targeting lipid-polymer hybrid nanoparticles (PLGA/CPT) were prepared from PLGA and C18-PEG2000-TPP (CPT) [71]. Then, DOX was loaded into PLGA/CPT nanoparticles to obtain DOX-PLGA/CPT. Lastly, positively charged PEI-DMMA (PD) shell was wrapped on the surface of positively charged DOX-PLGA/CPT to obtain negatively charged DOX-PLGA/CPT/PD with a diameter of ~150 nm. When DOX-PLGA/CPT/PD was treated at pH 6.5, the hydrolysis of amide in PD occurred, facilitating the elimination of electrostatic interaction between PLGA/CPT and PEI, ultimately resulting in the deshielding of PD to reveal DOX-PLGA/CPT and transformation of the charge from −24 to +19.2 mV (Figure 2b). Then, they studied the pharmacokinetics of DOX-PLGA/CPT/PD, and, the results showed that DOX-PLGA/CPT showed significantly slower clearance with a half-life time 15.84 h. After incubation with MCF-7/ADR cells at pH 6.5, DOX-PLGA/CPT/PD showed effective lysosome escape (Figure 2c), excellent mitochondrial-targeting capacity (Figure 2d) and superior cytotoxicity for overcoming DOX resistance by up-regulating the apoptosis-related proteins as well as down-regulating the antiapoptotic protein Bcl-2 (Figure 2e). Encouraged by the in vitro antitumor effect of DOX-PLGA/CPT/PD, Yu et al. evaluated the in vivo effect in MCF-7/ADR cell-bearing mice. The results show that DOX-PLGA/CPT/PD showed the best inhibitory effect on tumor growth and exhibited the best treatment effect, with a tumor inhibition rate (TIR) of 84.9% with no obvious side effects (Figure 2f).
Studies show that the exposure of tumor cells to chemotherapy drugs can result in hypoxia-inducible factor-1 (HIF-1) activation and stabilization [72,73], where HIF-1 plays an important part in drug resistance by regulating multidrug resistance protein (MRP), P-glycoprotein (P-gp), Bcl-2, etc. [74,75,76]. Moreover, HIF-1 can up-regulate the level of glutathione, which can bind with heavy metal ions, including cisplatin [77,78]. Therefore, inhibiting HIF-1 pathways during chemotherapy might be a promising method to circumvent chemo-resistance [79,80,81,82,83]. Acriflavine (ACF), a potent HIF-1 inhibitor, has been proven to bind to HIF-1α and thereby impede HIF-1α/β dimerization [84,85], which can be a useful strategy for sensitization of chemotherapy. In this regard, Zhang et al. [86] developed a new type of microporous silica-based co-delivery system (PMONA) to reverse the acquired resistance to cisplatin. Firstly, cisplatin was loaded into the polymeric mPEG-silane functionalized mesoporous silica nanoparticles inner core by reverse microemulsion method, where polymeric mPEG-silane was applied to maintain stability during blood circulation. To achieve tumor-specific glutathione (GSH)-triggered drug release, tetrasulfide bond-bridged organosilica was integrated to obtain the nanoparticles. Finally, ACF was loaded into the inner area of mircopores by electrostatic interactions to obtain ACF-loaded nanoparticles with a diameter of ~45 nm. After internalization by cancer cells, the outer organosilica shell of PMONA could be degraded by intracellular GSH, resulting in nanoparticle disassembly, drug release and synergistic regulation of multiple cancer-related signaling pathways. As shown in an in vitro release experiment, cisplatin and ACF had faster and higher cumulative release rates in a medium containing 10 mM GSH than in a medium containing 10 μM GSH, which confirmed that the tetrasulfide bond in organosilica enabled GSH-responsive disassembly and drug release. After incubation with A459 cells, PMONA exhibited stronger cell cytotoxicity, induced more apoptosis than the single drug-loaded nanoparticles by suppressing HIF-1-related proteins and decreased the level of intracellular GSH. Inspired by the result that ACF strengthens the curative effect of cisplatin in vitro, Zhang et al. assessed the in vivo antitumor effect in A459 cell-bearing mice. The results indicated that PMONA showed the best inhibitory effect on tumor growth and exhibited the best therapeutic effect with limited side effects. Additionally, the immunohistochemical experiment showed that PMONA enhanced cell death and apoptosis in tumor tissues mainly by down-regulating the levels of P-gp, MRP2, HIF-1-activated glutamate-cysteine ligase modifier subunit (GCLM), vascular endothelial growth factor (VEGF) and cystine transporter (xCT). Taken together, these results confirmed that ACF could combat cisplatin-acquired resistance by inhibiting HIF-1 function.
Hyperthermia, a non-invasive treatment strategy, has shown a competitive advantage in reversing drug resistance in cancer by suppressing the expression of drug efflux transporters [87,88,89,90,91,92]. Therefore, hyperthermia combined with chemotherapy is a hopeful treatment strategy for overcoming chemotherapeutic resistance [93,94,95,96,97,98]. Huang et al. [99] constructed smart, thermoresponsive, pH low insertion peptide (pHLIP)-modified gold nanocages (DOX@pPGNCs) to realize synergistic thermo-chemotherapy and overcome chemotherapeutic resistance. Firstly, thermoresponsive poly (di (ethylene glycol) methyl ether methacrylate-co-oligo (ethylene glycol) methyl ether methacrylate) (PMEO2MA-OEGMA) polymer was anchored to gold nanocages to PMEO2MA-OEGMA-modified gold nanocages, where PMEO2MA-OEGMA served as a temperature-sensitive gate guard at a lower critical solution temperature of ca. 41.6 °C. In other words, the PMEO2MA-OEGMA chains extended under 41.6 °C, sealing the pore of gold nanocages to prevent the leakage of drug into the blood; however, once the temperature increased up to 41.6 °C due to the NIR-induced photothermal effects, its chains shrunk, leading to opening of the pores of gold nanocages and fast DOX release (Figure 3a). Then, pHLIP was used to decorate PMEO2MA-OEGMA-modified gold nanocages to obtain pPGNCs, where pHLIP was a good candidate to enhance cancer cell internalization by conformational transition at the weakly acidic tumor microenvironment. Lastly, DOX was loaded into pPGNCs to obtain DOX@pPGNCs with a diameter of ~160 nm and a zeta potential of approximately −20 mV. As shown in Figure 3b, PMEO2MA-OEGMA was thermosensitive with a lower critical solution temperature of ca. 41.6 °C. In vitro release experiments indicated that the cumulative release of DOX increased from 3.7 to 20.1% after 5 min of NIR irradiation. More importantly, the rapid release of DOX was consistent under NIR irradiation in another cycle (Figure 3c), indicating that PMEO2MA-OEGMA was a very responsible gatekeeper to precisely control NIR-triggered DOX release from DOX@pPGNCs. Cytotoxicity experiments showed that the antiproliferation ability against MCF-7/ADR cells was strongest in the DOX@pPGNCs and NIR irradiation group at pH 6.5 (Figure 3d), suggesting that pHLIP could enhance cellular uptake of DOX@pPGNCs under a weak acid tumor microenvironment, and, upon NIR irradiation, DOX@pPGNCs could efficiently achieve synergistic thermo-chemotherapy to overcome cancer resistance. In vivo biodistribution experiments showed that DOX accumulation in tumor site of tumor-bearing mice treated with DOX@ pPGNCs and NIR irradiation was highest (Figure 3e), confirming that NIR irradiation-triggered photothermal effects of gold nanocages could further strengthen DOX accumulation. Inspired by the above experimental results, Huang et al. further assessed the in vivo treatment effect in MCF-7/ADR cell-bearing mice. The results indicated that DOX@pPGNCs achieved the strongest antitumor efficacy with a TIR of 97.3% (Figure 3f,g), indicating the highly effective synergistic thermo-chemotherapy in MCF-7/ADR cell-bearing mice.
Figure 3.
DOX@pPGNCs for chemo-photodynamic combination therapy of drug-resistant cancer. Reprinted with permission from Ref. [99]. 2019, NIH. (a) Schematic diagram of the mechanism of DOX@pPGNCs surmounting cancer drug resistance. (b) Transmittance of POEG in PBS. (c) In vitro release curve of DOX@pPGNCs. (d) In vitro cytotoxicity against MCF-7/ADR cells. * p < 0.05, ** p < 0.01. (e) Accumulation of different groups in tumor site of tumor-bearing mice. (f,g) In vivo antitumor effect of DOX@pPGNCs. * p < 0.05, ** p < 0.01, *** p < 0.001. P-gp, an ATP-dependent protein, is overexpressed in different drug-resistant tumor cells and closely related to chemotherapy resistance by promoting drug efflux [100,101,102,103,104]. In recent few years, RNA interference (RNAi) techniques have been used to block the expression of P-gp to reverse drug resistance [105,106,107,108,109]. Zheng et al. [109] constructed a special, siRNA and chemotherapy drug co-delivery system, an siRNA-based nanostructure (siRNAsome), to enhance combination therapy for overcome chemotherapeutic resistance (Figure 4a). Dynamic light scattering (DLS) data show that Dox.HCl-loaded siRNAsome ([email protected]) ranged in particle size from 126 to 135 nm. This novel siRNAsome was based on the self-assembly of siRNA-disulfide-poly (N-isopropylacrylamide) (siRNA-SS-PNIPAM) copolymers, which was very different from traditional siRNA delivery systems. In other words, this distinctive siRNAsome not only possessed an empty aqueous interior that could load hydrophilic agents, but also possessed a thermoresponsive and intracellular reduction-dependent hydrophobic median layer that could load hydrophobic drugs. Moreover, this siRNAsome possessed a siRNA stabilization shell that could load siRNA drugs without using a cationic component. When siRNAsome was incubated with a dithiothreitol (DTT) solution, DOX was rapidly released from the nanostructure, and more than 75% of the encapsulated DOX was released after 24 h incubation with dithiothreitol (Figure 4b), indicating that siRNAsome was sensitive to an intracellular environment and intracellular redox conditions could effectively disintegrate the structure of siRNAsome to control drug release. To test the capacity to efficiently deliver siRNA into tumor cells without the aid of a cationic component, MCF-7/ADR cells were incubated with siRNAsome and confocal laser scanning microscopy showed that siRNAsome could unquestionably promote uptake of siRNAsome (Figure 4c). More importantly, when treated with siRNAsome for 2 days, the P-gp mRNA level of MCF-7/ADR cells decreased by approximately 42% by P-gp gene silencing (Figure 4d). To test the synergistic antitumor effect of the siRNAsome, DOX and anti-P-gp siRNA were co-loaded into the siRNAsome to form [email protected]. As shown in Figure 4e,f, [email protected] showed the strongest cytotoxicity in MCF-7/ADR cancer cells and the strongest antitumor effect in MCF-7/ADR cell-bearing mice, indicating that the knockdown of P-gp mRNA could remarkably improve the activity of DOX to efficiently realize synergistic therapeutic efficacy and this cation-free [email protected] nanostructure could serve as a promising vehicle for reversing drug resistance.
Figure 3.
DOX@pPGNCs for chemo-photodynamic combination therapy of drug-resistant cancer. Reprinted with permission from Ref. [99]. 2019, NIH. (a) Schematic diagram of the mechanism of DOX@pPGNCs surmounting cancer drug resistance. (b) Transmittance of POEG in PBS. (c) In vitro release curve of DOX@pPGNCs. (d) In vitro cytotoxicity against MCF-7/ADR cells. * p < 0.05, ** p < 0.01. (e) Accumulation of different groups in tumor site of tumor-bearing mice. (f,g) In vivo antitumor effect of DOX@pPGNCs. * p < 0.05, ** p < 0.01, *** p < 0.001. P-gp, an ATP-dependent protein, is overexpressed in different drug-resistant tumor cells and closely related to chemotherapy resistance by promoting drug efflux [100,101,102,103,104]. In recent few years, RNA interference (RNAi) techniques have been used to block the expression of P-gp to reverse drug resistance [105,106,107,108,109]. Zheng et al. [109] constructed a special, siRNA and chemotherapy drug co-delivery system, an siRNA-based nanostructure (siRNAsome), to enhance combination therapy for overcome chemotherapeutic resistance (Figure 4a). Dynamic light scattering (DLS) data show that Dox.HCl-loaded siRNAsome ([email protected]) ranged in particle size from 126 to 135 nm. This novel siRNAsome was based on the self-assembly of siRNA-disulfide-poly (N-isopropylacrylamide) (siRNA-SS-PNIPAM) copolymers, which was very different from traditional siRNA delivery systems. In other words, this distinctive siRNAsome not only possessed an empty aqueous interior that could load hydrophilic agents, but also possessed a thermoresponsive and intracellular reduction-dependent hydrophobic median layer that could load hydrophobic drugs. Moreover, this siRNAsome possessed a siRNA stabilization shell that could load siRNA drugs without using a cationic component. When siRNAsome was incubated with a dithiothreitol (DTT) solution, DOX was rapidly released from the nanostructure, and more than 75% of the encapsulated DOX was released after 24 h incubation with dithiothreitol (Figure 4b), indicating that siRNAsome was sensitive to an intracellular environment and intracellular redox conditions could effectively disintegrate the structure of siRNAsome to control drug release. To test the capacity to efficiently deliver siRNA into tumor cells without the aid of a cationic component, MCF-7/ADR cells were incubated with siRNAsome and confocal laser scanning microscopy showed that siRNAsome could unquestionably promote uptake of siRNAsome (Figure 4c). More importantly, when treated with siRNAsome for 2 days, the P-gp mRNA level of MCF-7/ADR cells decreased by approximately 42% by P-gp gene silencing (Figure 4d). To test the synergistic antitumor effect of the siRNAsome, DOX and anti-P-gp siRNA were co-loaded into the siRNAsome to form [email protected]. As shown in Figure 4e,f, [email protected] showed the strongest cytotoxicity in MCF-7/ADR cancer cells and the strongest antitumor effect in MCF-7/ADR cell-bearing mice, indicating that the knockdown of P-gp mRNA could remarkably improve the activity of DOX to efficiently realize synergistic therapeutic efficacy and this cation-free [email protected] nanostructure could serve as a promising vehicle for reversing drug resistance.

Studies have shown that tumor cells can develop drug resistance by enhancing DNA repair [110,111,112,113,114,115], suggesting that drug resistance owing to DNA repair can be overcome by inhibiting the function of related proteins [116,117,118,119]. Recently, Wang et al. [120] constructed a smart delivery system for overcoming cisplatin-related “cascade drug resistance” (CDR) by mild hyperthermia (43 °C) triggered by NIR. Firstly, hydrophobic photothermal-conjugated polymer and biodegradable amphiphilic polymer were mixed to form F-nanoparticles (F-NPs) with photothermal performance. Secondly, biodegradable amphiphilic polymer and C16-CisPt-Suc (a Pt (IV) prodrug) were mixed to form Pt-nanoparticles (Pt-NPs). Lastly, Pt-NPs and F-NPs were mixed to obtain the mixed nanoparticles (F-Pt-NPs). On the basis of DLS data, the average particle size of F-NPs was 91.0 ± 2.6 nm, while that of the Pt-NPs was 105.1 ± 1.6 nm. In vitro experiments showed that, under the treatment of NIR, mild hyperthermia could efficiently facilitate cellular uptake of drug-resistant A549DDP cells, resulting in enhanced cytotoxicity and surmounting CDR of cisplatin by the consumption of GSH and the reduction of Pt (IV) to Pt (II). More importantly, mild hyperthermia could accelerate the binding of Pt to DNA and promote the formation of irreparable crosslinking of Pt-DNA strands, resulting in the destruction of DNA repair. In vivo experiments showed that, under mild hyperthermia conditions, F-Pt-NPs exhibited the best antitumor effect with a TIR of 94% with few side effects, further indicating that NIR-triggered mild hyperthermia could reverse CDR.
In recent years, substantial evidence has confirmed that drug resistance is closely related to the CSC phenotype [121,122]. One proven mechanism of multidrug resistance (MDR) in CSC is the increased expression of ABC transporters [123]. In addition, the CSC phenotype shows increased drug resistance to chemotherapy by modulating many other stem characteristics, including enhanced DNA damage repair capacity and up-regulation of antiapoptotic proteins [124,125]. Therefore, eradication of CSCs is an effective strategy to surmounting cancer drug resistance. Shen et al. [126] constructed an alltrans-retinoic acid (ATRA) and camptothecin (CPT) co-loaded nanoplatform (ATRA/CPT-NPs) to surmount chemotherapeutic resistance of both CSCs and bulk tumor cells. Firstly, ROS-responsive nitroimidazole-modified hyaluronic acid-oxalate-CPT conjugate (n-HA-oxa-CPT) was synthesized. Then, n-HA-oxa-CPT assembled into nanoparticles and physically encapsulated ATRA to obtain ATRA/CPT-NPs with a diameter of ~150 nm. Based on the difference levels of ROS between bulk tumor cells and CSCs, ATRA/CPT-NPS could sequentially release ATRA and CPT during the differentiation of CSCs. After uptake by hypoxia CSCs, ATRA was firstly released, which induced CSC differentiation into reduced stemness and chemoresistance, along with increased ROS level. Then, the increased ROS in differentiated CSCs triggered CPT release for enhanced cytotoxicity towards the differentiated cells with decreased drug resistance. On the other hand, after uptake by bulk tumor cells with hypoxia and high ROS, ATRA/CPT-NPS could simultaneously release ATRA and CPT, resulting powerful synergistic anticancer effects. In their study, ATRA/CPT-NPs showed the strongest inhibition efficacy on the orthotopic BCSC-enriched tumor mouse models, suggesting that the differential drug release realized by ATRA/CPT-NPs was very important to strengthen the synergistic efficacy of ATRA-triggered CSC differentiation and CPT-triggered cytotoxic activity for the treatment of poorly differentiated and highly chemo-resistant heterogeneous tumors.
Additionally, a summary of nanomedicines studied for overcoming chemotherapeutic resistance in recent years is displayed in Table 2.
3. Nanomedicines against Drug Resistance in Targeted Therapy
3.1. Mechanisms in Drug Resistance of Targeted Therapy
Compared with chemotherapy, targeted therapies exhibit superiorities in efficacy and safety, and is thus becoming the mainstream of clinical cancer therapy. Although great strides have made in the past two decades, there are still insurmountable problems that targeted therapy is facing [154,155,156,157,158,159,160]. The biggest problem is drug resistance [161,162]. Almost all targeted therapies encounter drug resistance after use for a period of time, which is mainly related to gene mutations, gene amplification, CSCs, efflux pumps, inactivation of apoptosis and autophagy [161] (Figure 5). Gene mutations are primarily responsible for resistance to targeted anticancer agents [163,164,165]—one argument is that the gene mutations are induced by drugs, and another is that drug-resistant mutations already existed. Gene amplification is another common cause of resistance associated with targeted anticancer agents [166,167]. According to statistics, approximately 20% of EGFR inhibitor-resistant cases are MET amplification. CSCs are also considered to be in charge of drug resistance and tumor recurrence due to their quiescence, epithelial-to-mesenchymal transition, resistance to DNA damage-induced apoptosis and interactions with the tumor microenvironment [168,169,170]. Overexpression of ATP-dependent efflux transporters, especially P-gp, also plays an important role in the drug resistance of targeted anticancer agents [171]. In addition to the resistance mechanisms mentioned above, autophagy [172] and inactivation of apoptosis [173] are also considered be responsible for drug resistance to targeted anticancer agents.
3.2. Nanomedicines to Overcome Targeted Therapy Resistance
AZD9291 (Osimertinib) is the first third-generation growth factor tyrosine kinase inhibitor (EGFR-TKI) approved by the FDA, which has significant effects not only on classical EGFR-sensitive mutations, but also on EGFR-resistant mutations (T790M mutation) [174,175,176]. Even so, it inevitably develops acquired drug resistance and this greatly impedes its benefits [177,178,179,180]. Studies have shown that autophagy allows cancer cells to improve their survival at advanced stages or under therapeutic stress [181,182,183], which ultimately results in small-molecule targeted anticancer drug resistance. On the other hand, fibroblast growth factor receptor 1 (FGFR1) is commonly expressed in all types of cancer and is involved in tumor progression and epithelial-to-mesenchymal transition-related drug resistance to EGFR-TKIs [184,185,186,187]. Thinking together, inhibition of both FGFR1 and autophagy might be an effective method to surmount AZD9291 resistance. Gu et al. [188] constructed a PD173074 (a kind of FGFR1 inhibitor) and chloroquine (CQ) dual-loaded shell–core targeted delivery system (CP@NP-cRGD), which could observably inhibit FGFR1 and autophagy, respectively, to reverse AZD9291 resistance (Figure 6a). Briefly, Gu et al. used DSPE-PEG and DSPE-PEG-cRGD to entrap PD173074 to obtain an interior core, and then utilized cRGD-PEG to load calcium phosphate (CaP) with CQ by a biomineralization method to form a shell. The average size of CP@NP-cRGD was 123.4 ± 0.4 nm, with a zeta potential of −15.1 ± 1.4 mV. CP@NP-cRGD could enhance cellular uptake by active targeting ligand cRGD and the pH-susceptive CaP shell could facilitate effective lysosome escape, thus promoting the successive release of CQ and PD173074. In vitro release experiments showed that CP@NP-cRGD was pH sensitive, where PD173074 exhibited a relatively sustained release behavior, whereas CQ showed a biphasic release behavior with an initial blasting effect and following sustained release (Figure 6b). When incubated with resistant cells, Rhodamine B (RB)-loaded CP@NP-cRGD showed the strongest fluorescence intensity (Figure 6c), indicating that cRGD could significantly promote cellular uptake of integrin αvβ3/αvβ5-rich cancer cells. Under the acidic conditions within lysosomes, the CaP shell of CP@NP-cRGD cracked, ion pairs formed, and the osmotic pressure of lysosomes increased, ultimately leading to lysosome cracking, indicating that CP@NP-cRGD could successfully facilitate lysosome escape to ensure effective drug delivery into the cytoplasm (Figure 6d). In vitro cytotoxicity testing showed that the CP@NP-cRGD and AZD9291 group demonstrated the strongest antiproliferative effect on resistant cells. Flow cytometry analysis and Western blotting tests further confirmed that CP@NP-cRGD and AZD9291 induced the highest rate of apoptosis, the most G0/G1 cell cycle arrest and reduced proliferation of resistant cells by down-regulation of p-ERK and up-regulation of cleaved-caspase 3 (Figure 6e). Moreover, Gu et al. confirmed the inhibitory effect of CP@NP-cRGD on autophagy. As shown in Figure 6f, CP@NP-cRGD and AZD9291 could inhibit autophagosome fusion with lysosomes, leading to the most remarkable accumulation of autophagosomes and the strongest LC3-II levels. Together, these results indicated that CP@NP-cRGD could reverse drug resistance to AZD9291. Inspired by the in vitro results, the in vivo anticancer effect of CP@NP-cRGD was tested in AZD9291-resistant NSCLC xenograft-bearing mice. Compared with other treatment groups, the CP@NP-cRGD and AZD9291 group exhibited the slowest tumor growth curves and showed the strongest antitumor effect (Figure 6g), suggesting that CP@NP-cRGD could effectively surmount drug resistance to AZD9291 in vivo. In addition, the effect of CP@NP-cRGD on apoptosis and autophagy in vivo was also studied. The results indicated that CP@NP-cRGD could efficaciously up-regulate the level of apoptosis-related protein cleaved-caspase 3 and down-regulate the level of proliferation-related protein Ki-67, which were highly consistent with the in vitro results. Autophagosome changes were further tested in tumor biopsies and the results revealed that the CP@NP-cRGD and AZD9291 group showed the most significant accumulation of autophagosomes as with the in vitro results. To sum up, CP@NP-cRGD could observably decrease proliferation and trigger apoptosis by impeding autophagy and the FGFR1 pathway in drug-resistant tumor, which provided a new strategy for reversing AZD9291 resistance.
Hypoxia is the most common pathological phenomena owing to the abnormal blood vessels and rapid cell proliferation at tumor site [189,190,191]. Studies have confirmed that hypoxic tumor cells overexpress HIF-1α and P-gp, which observably promote the progress of cancer cells resistant to small-molecule targeted drugs [192,193,194]. Therefore, there is a pressing need for an effective hypoxia-targeting strategy [195]. Bera et al. [196] constructed a kind of hypoxia-responsive copolymer (CMP-HA-NI-PEI-NBA) containing nitroaromatic subunits, which could self-assemble into nanomicelles to efficiently deliver erlotinib into cancer cells. The average size of erlotinib-loaded nanomicelles was 755.77 ± 51.11 nm, with a zeta potential of 26.62 ± 2.20 mV. After selective bioreduction of the nitroaromatic residues and rapid decomposition of the nanostructures in cancer cells deprived of oxygen, erlotinib could be rapidly released and eventually improve its chemo-sensitivity. When incubated with PBS and sodium dithionite (pH 5.0), erlotinib-loaded nanomicelles were depolymerized, leading to significantly rapid drug release behavior as compared to normal oxygen states. As compared to incubation at 4 °C, cellular uptake was significantly enhanced when incubated at 37 °C, indicating that cellular uptake of erlotinib-loaded nanomicelles was energy dependent. However, cellular uptake was significantly blocked after incubation of the cells with β-cyclodextrin, indicating the mechanism of caveolae/lipid raft-mediated endocytosis for the internalization of nanomicelles. In addition, erlotinib-loaded nanomicelles could trigger more apoptotic cells than erlotinib. Further, interestingly, erlotinib-loaded nanomicelles achieved significantly stronger cytotoxicity under hypoxia conditions than in normoxic conditions, owing to their hypoxia-dependent accelerated drug release.
To date, combinations of chemotherapy and light-mediated therapy have been investigated to surmount cancer drug resistance [197,198,199,200,201]. Sonodynamic therapy (SDT), an alternative treatment strategy, has been shown to be more effective than photodynamic therapy (PDT) because ultrasound penetrates soft tissue to a depth of approximately 10 cm [202,203,204,205,206]. However, the oxygen consumption of SDT increases the hypoxia degree of the tumor tissue, which in turn impedes the efficiency of SDT [207,208,209]. Considering that hypoxia is closely related to drug resistance of EGFR-TKIs, with oxygen being a pivotal substrate of SDT, Zhang et al. [210] developed a nanoplatform (namely CEPH) prepared by erlotinib-conjugated chitosan, which collaboratively delivered sonosensitizer hematoporphyrin (HP) and oxygen storage agent perfluorooctyl bromide (PFOB) to enhance the effect of SDT and overcome EGFR-TKI resistance. The particle size of CEPH was 284.1 nm and the zeta potential of CEPH was −8.4 mV. In their study, CEPH was sensitive to the acidic tumor environment and revealed a rapid release behavior in acidic condition. Moreover, the HP release rate of CEPH was significantly increased after ultrasound irradiation, and was higher than that of CEPH with no irradiation. These results suggested that CEPH was a pH/ultrasound dual-dependent delivery carrier. Under hypoxia conditions, cellular uptake of H1975 cells incubated with CEPH was higher than when incubated with CEH, indicating that PFOB could alleviate the hypoxia state and thus improve the cellular endocytosis of cancer cells with EGFRT790M resistant mutation. In addition, compared with other nanocarriers, the toxicity of CEPH to H1975 cells was significantly enhanced, especially under hypoxic conditions, indicating that erlotinib and PFOB could collectively improve the antitumor effect. Moreover, CEPH and ultrasound showed the strongest antitumor effect due to the synergistic effects of erlotinib and SDT. The above results confirmed that erlotinib, PFOB and HP could generate synergistic effects to improve the antitumor effect and reverse EGFR-TKI resistance by combination of erlotinib and SDT. A three-dimensional spherical model of multicellular tumor showed that the hypoxic condition was aggravated after treatment with ultrasound alone but relieved when treated with CEPH and ultrasound, indicating that SDT was an oxygen-consuming procedure but PFOB in CEPH could alleviate the hypoxia induced by SDT and enhance the SDT effect. Western blotting results further expounded that CEPH and ultrasound was able to observably inhibit the expression of EGFR, down-regulate the level of HIF-1α and increase the level of ROS, which ultimately contribute to the cooperative antitumor effect.
In addition to drug resistance, another big challenge that small-molecule targeted anticancer drugs are facing is metastases [211,212,213]. Studies have shown that approximately 33% of non-small-cell lung cancer (NSCLC) patients with EGFR mutation develop brain metastases (BMs) [214], which was the main cause of mortality in patients with advanced NSCLC. Thereby, there is an urgent need to design an effective strategy for surmounting drug-resistant brain metastases. Yin et al. [215] designed a dual-targeting drug delivery system (T12/P-Lipo) modified with T12 peptide and anti-PD-L1 nanobody for synergistic delivery of simvastatin/gefitinib to surmount the two huge obstacles in the treatment of NSCLC—drug resistance and brain metastases. Where T12 peptide could facilitate blood–brain barrier (BBB) penetration, anti-PD-L1 nanobody was used as a targeting ligand for active targeting and simvastatin was utilized to repolarize the tumor-associated macrophages from the M2 to M1 phenotype for remodeling tumor microenvironments. The average size of the T12/P-Lipo was approximately 153 nm, with a zeta potential of approximately −27 mV. A Transwell culture model was utilized to assess the advantage of T12/P-Lipo in BBB penetration. When incubated with H1975 cells, the levels of transferrin receptor and PD-L1 in the capillary endothelial cells (BCECs) were significantly increased (Figure 7a), suggesting that both transferrin receptor (TfR) and PD-L1 were the promising target receptors in the brain metastases vascular endothelial cells. Moreover, cellular uptake of T12/P-Lipo by H1975 cells was higher than that of any other nanocarriers (Figure 7b), and the fluorescence images further verified the intensive BBB-penetrating capacity of T12/P-Lipo and enhanced cellular uptake (Figure 7c). After incubation with human umbilical vein endothelial cells, simvastatin and gefitinib exhibited significant down-regulation of CD206 (an M2-related marker) and up-regulation of STAT1 and iNOS (an M1-related marker) (Figure 7d), indicating that the combination of simvastatin and gefitinib could effectively repolarize macrophages from M2 to M1. An in vitro cytotoxicity study was performed in EGFRT790M H1975 cells. After treatment, T12/P-Lipo showed the maximum antiproliferation ability with IC50 1.85 μg/mL. Western blotting further expounded that T12/P-Lipo up-regulated the expression of nicotinamide adenine dinucleotide phosphate oxidases 3 (NOX3), down-regulated the levels of methionine sulfoxide reductase (MsrA), antioxidant enzyme glutathione peroxidase 4 (GPX4) and Bcl-2 (Figure 7e), suppressed EGFR/Erk/Akt phosphorylation (Figure 7f) and thereby triggered increased cleaved caspase-3 to reverse drug resistance (Figure 7g). Then, they studied the pharmacokinetics of T12/P-Lipo, and, the results showed that the half-life time of T12/P-Lipo was 5.9 h. Inspired by the in vitro experiments, in vivo antitumor efficacy was evaluated in the BM mouse model. As shown in Figure 7h,i, the antitumor effect of T12/P-Lipo was better than that of other groups, indicating the prospect of dual-targeting drug delivery in improving the treatment of BMs and surmounting the cancer resistance of EGFRT790M mutation. In addition, Western blotting demonstrated that T12/P-Lipo had a strong inhibitory effect on EGFR/Erk/Akt tumor growth signaling pathway, which was highly consistent with the in vitro results. Additionally, the T12/P-Lipo treatment group induced extensive apoptosis of the BMs by down-regulating caspase 3 and Ki 67. To sum up, T12/P-Lipo could efficiently dual-target the brain metastases and tumor-associated macrophages, providing a novel strategy for the treatment of advanced NSCLC with drug-resistant brain metastases.
Additionally, a summary of nanomedicines studied for overcoming resistance to targeted therapy in recent years is displayed in Table 3.
4. Nanomedicines against Drug Resistance in Immunotherapy
4.1. Mechanisms in Drug Resistance of Immunotherapy
The emergence of immunotherapy, such as immune checkpoint inhibitors (ICIs) and adoptive cell metastases (ACT), has changed the pattern of traditional tumor surgery, radiotherapy and chemotherapy and is becoming an important method of clinical tumor treatment, especially hematologic cancers and solid tumors [222,223,224,225]. However, the clinical curative effect of these immunotherapies is restrained by cancer drug resistance, which has become among the important challenges in immunotherapy [226,227,228]. The mechanism of immunotherapy resistance is completely different from that of traditional chemotherapy drug resistance, mainly due to the “loss or deficiency” of antigens [229,230]. An abnormal signal pathway, loss or mutation of tumor suppressor genes, loss or down-regulation of target antigen, JAK1/2, B2M and Apelin receptor gene mutation, TIM/LAG3 expression, inhibitory checkpoint increase, activation checkpoint decrease, T cell depletion, phenotypic changes, tumor microenvironment and drug antigenicity all play important roles in immunotherapy resistance [231,232,233,234,235,236,237,238].
4.2. Nanomedicines to Overcome Immunotherapy Resistance
Recent studies have shown that gene-encoding phosphatase and tensin homolog deleted on chromosome 10 (PTEN) is directly related to the regulation of antitumor immunity. Firstly, there is a significant correlation between loss of PTEN and reduced T cell infiltration, which eventually leads to resistance to PD-1 monoclonal antibody [239,240,241]. In addition, the disfunction of PTEN also promotes the aggregation of suppressive immune cells, such as bone marrow-derived suppressive immune cells (MDSCs) and regulatory T cells (Tregs) [242,243,244,245]. More importantly, the loss of PTEN expression has been shown to down-regulate autophagy [246,247], which can effectively support tumor development. Therefore, Lin et al. [248] constructed a PTEN mRNA nanocarrier (mPTEN@NPs) delivered to tumor cells with PTEN deletion or mutation to restore the immunosuppressive TME, stimulate immune response and improve the efficacy of immune checkpoint blockade (ICB) therapy by inducing autophagy activation and damage-associated molecular patterns (DAMPs) release. The particle size of mPTEN@NPs was 111.8 ± 15.3 nm. In their study, mPTEN@NPs could restore tumor sensitivity to immunotherapy, as well as trigger the release of DAMPs and the function of autophagy, which thereby promoted the formation of autophagosomes. In vivo studies showed that PTEN repair induced a strong response of CD8+ T cells and restored TME by inhibiting the generation of Tregs and monocyte MDSCs and promoting the generation of pro-inflammatory cytokines. In addition, they evaluated the antitumor effect of mPTEN@NPs combined with anti-PD-1 immunotherapy in tumor models with PTEN deletion or mutation, suggesting that this combination therapy strategy had significant therapeutic efficacy and immune memory. All above results suggested that repairing tumor suppressors with mRNA nanomedicine could improve the sensitivity of tumors to ICB therapy and provided an effective cooperative therapy strategy for a variety of malignancies.
Skin is an immune organ containing a large number of resident antigen-presenting cells [249,250,251]. Microneedles can penetrate the immune cell-rich epidermis and induce a strong immune response by stimulating the function T cells [252,253]. In recent years, researchers have used microneedles as an adjunctive immunotherapy for melanoma [254,255,256,257]. Lan et al. [258] constructed a microneedle patch containing pH-dependent tumor-targeting nanoparticles (aPD-1/CDDP@NPs) that could synergistically deliver cisplatin (CDDP) and aPD-1locally to tumor tissues for enhanced antitumor efficacy (Figure 8a). First of all, aPD-1/CDDP@NPs were developed by a reverse-phase microemulsion method. Then, aPD-1/CDDP@NPs were wrapped in dissolved microneedles by a molding method to form aPD-1/CDDP@NPs MNs, which could facilitate immune regions on the skin via transdermal delivery. As shown in Figure 8b, an MN was composed of 9 × 9 needles, where the needle height was 588 μm and the basal diameter was approximately 240 μm. The fluorescent image of the aPD-1/CDDP@NPs MNs also demonstrated the sufficient distribution of aPD-1/CDDP@NPs on the tips of MNs (Figure 8c). The obtained aPD-1/CDDP@NPs MNs could be sufficiently dissolved in water within 5 min and penetrated thoroughly into mouse skin within 20 min. In vivo antitumor results showed that the animal model in their study did not respond to routine aPD-1 immunotherapy. Nevertheless, aPD-1 delivered by MNs showed a remarkable antitumor effect. The tumor weight treated by aPD-1 MNs (0.05 ± 0.017 g) was 8-fold lower than that treated by routine aPD-1 (0.443 ± 0.083 g). More importantly, the tumor regression effect was most significant in the apD-1/CDDP@NP MN group, with a tumor weight of 0.012 ± 0.005 g (Figure 8d). The above results indicated that aPD-1 delivered by MNs could obtain effective anticancer effects in animal models that did not respond to routine aPD-1 immunotherapy, and collaborative delivery of aPD-1 and CDDP by MNs could achieve stronger antitumor effects. To assess T-cell responses, blood was harvested and analyzed. As shown in Figure 8e,f, the positive rates of CD4+ T cells and CD8+ T cells treated by aPD-1 were only 15.0% and 12.13%, while the positive rates of CD4+ T cells and CD8+ T cells in the aPD-1 MN group were 37.50% and 47.98%, respectively. More importantly, aPD-1/CDDP@NP MNs had the highest T-cell infiltration rate (75.95% of CD8+ T cells) of any groups. ELISA results further indicated that the production of IFN-γ increased after aPD-1 nanoencapsulation. Notably, MN-mediated drug delivery promoted greater IFN-γ expression, and the level of IFN-γ was the highest when treated by aPD-1/CDDP@NP MNs (Figure 8g). In addition, they analyzed the infiltration of CD4+Foxp3+ T cells and found a significant decrease in Tregs in the three MN groups (Figure 8h). These results further verified that aPD-1/CDDP@NP MNs could trigger the activity of T cells, as well as kill tumor cells through T cells.
In recent years, natural killer (NK) cell-related immunotherapy has been revealed as an alternative to ICB-based immunotherapy or vaccine-based immunotherapy [259,260,261,262]. However, its therapeutic effect is largely limited by down-regulation of the recognition ligands, and its immunological effect can further be blocked by the secretion of the tumor microenvironment such as transforming growth factor-β (TGF-β) [263,264,265]. Researchers have confirmed the advantages of methods that combine immunotherapy with chemotherapy in the treatment of cancers [266,267,268]. Therefore, there is great interest in developing combined strategies to improve NK cell immunity. Selenium (Se) is a key trace element that plays a crucial role in cancer prevention and immune response. Selenium can promote the generation of CD8+ T cells and increase the secretion of perforin and granulation enzyme [269]. In addition, Se can enhance the immunologic function of adoptive NK cells through TNF-related apoptosis [270]. Therefore, Se-based drugs combined with immunosuppressive ablators can be beneficial to improve the immune activity of NK cells. Liu et al. [271] constructed a nanoemulsion delivery system (SSB NMs) to synergistically load selenocysteine (SeC) and TGF-β inhibitors to realize an amplified immunotherapeutic effect. The particle size of SSB NMs was approximately 130 nm and the zeta potential of SSB NMs was approximately −5.32 mV. In their study, the cytotoxicity of NK92 cells to HCC1937 cells and MMDA-MB-468 cells were significantly increased by SSB NMs pretreatment for 12 h. Moreover, activated NK cells obtained from patients were further used to evaluate the immunosensitization triggered by SSB NMs. Pre-incubation of target cells could improve the lysis efficiency of NK cells from 0.94 to 13.8 with an average increase of 0.2 to 30.6 folds. These results confirmed that SSB NMs could trigger the immunosensitization properties of NK92 cells. Mechanism studies shown that SSB NMs could effectually inhibit TGF-β/TGF-β RI/Smad2/3 pathway and enhance the expression of NKG2DL triggered by DNA destruction-dependent pathway, thus improving the efficacy of immunotherapy on NK92 cells. More importantly, after pretreatment of SSB NMs twice, adoptive therapy of NK92 cells showed the strongest antitumor effect with tumor inhibition rate of 78.15%. In conclusion, the above results demonstrated that the synergistic treatment therapy of SSB NMs and adoptive NK92 cells had a high efficacy in cancer treatment.
Although ICB therapy has greatly improved the survival of treatment-sensitive patients, the overall response rates to ICB therapy remains low [272,273,274], so, combination therapy with other immunomodulators that intercept non-redundant inhibitory pathways is being actively studied to surmount cancer drug resistance to ICB [275,276]. Since ICB are inherent to T cells, lymphocytes and not cancer cells are the target cells of ICB. Taken together, direct targeting of lymphocytes after administration has high prospects [277,278,279]. Francis et al. [280] designed an antibody-modified nanoplatform (ANCs) that could efficiently distribute in lymph nodes and lymphocyte-rich tissues and thus contributed to ICB-mediated antitumor effect. The average particle size of ANCs was approximately 30 nm. In their study, ANCs allowed for the encapsulation of TGF-β inhibitor or adenosine antagonists within the NPs core, while maintaining the binding affinity of surface-conjugated monoclonal antibodies to facilitate targeted delivery of encapsulated agents to lymph nodes or lymphocyte-rich tissues. Utilizing ICB monoclonal antibody as targeting ligand as well as signal-blocking therapy, ANCs slowed the tumor growth, prolonged the animal survival and thus improved the therapeutic effects of TGF-β receptor 1 inhibitor and adenosine 2A antagonist. Over all, the combination formulation strategy enabled multiple immunotherapy agents to be co-delivered to T lymphocytes and had the potential to strengthen immunotherapeutic effect by simultaneously inhibiting non-redundant inhibitory pathways.
Additionally, a summary of nanomedicines studied for overcoming resistance to immunotherapy in recent years is displayed in Table 4.
5. Discussion
Cancer is among the leading causes of death worldwide. Although chemotherapy, targeted therapy and immunotherapy have made significant achievements in the treatment of cancer, current treatment strategies all have serious limitations and often fail in clinical treatment. There are many reasons for treatment failure, such as poor oral bioavailability, and drug-related severe adverse reactions. The most challenging problem is that patients receiving antitumor therapy almost invariably develop drug resistance. In this respect, great progress has been made in uncovering the mechanisms of cancer drug resistance. However, how to overcome drug resistance of cancer is still an unsolved medical problem in clinical treatment. Therefore, cancer drug resistance has become a major obstacle in cancer treatment, and surmounting drug resistance is the goal oncologists are actively exploring now and in the future.
In recent years, nanomedicines, a new and effective strategy for surmounting cancer drug resistance, have attracted increasing attention. Nanomedicines can improve the bioavailability of difficult soluble drugs, extend drug blood circulation, pass through biological barriers, achieve targeted tumor therapy by passive or active targeting, improve the antitumor effect and use their own physical properties (optical, electric or magnetic) for real-time imaging, localization and control of drug release. In addition, nanomedicines can co-deliver therapeutic agent combinations for synergistic treatment or multimodal therapy, making them attractive therapeutic options for overcoming cancer drug resistance. As reviewed in this context, a variety of unique nanomedicines, including liposomes, polymer NPs and hybrid NPs, have been constructed to surmount cancer drug resistance. As more nanomedicines are developed and optimized, the advantages of nanomedicines over current treatment strategies will continue to be exploited. Therefore, it is believed that nanomedicines will be an attractive strategy for reversing or overcoming cancer drug resistance.
However, there is still a long way to go when currently studied nanomedicines can be used in clinic. First of all, due to the rapid development and wide application of nanomedicines or nanomaterials, the research on their potential toxicity has not been fully determined. Therefore, attention should be taken to develop nanomedicines with good safety characteristics to avoid damage from systematic exposure of the nanomaterials themselves, and, more in vivo safety and efficacy data are needed to support the clinical application of nanomedicines. Secondly, more effort should be made to collect clear evidence for the mechanisms of action, rather than to construct many new complex nanomedicines for similar concepts. Among the primary goals of nanomedicines is to ensure therapeutic agents to be delivered into tumor cells at sufficient local concentrations with minimal loss of their activity in the bloodstream. In addition, nanomedicines should reduce potential toxicity to normal tissues and healthy cells. Studies have shown that the composition, size, morphology and surface charge of nanomedicines can all affect their biological effect and distribution in organisms. How to design nanomedicines with a stable structure and good function is still a huge challenge. Nanomedicines larger than 150 nm mainly accumulate in spleen, liver and lungs. Nanomedicines under 5 nm mainly accumulate in kidney. Nanomedicines in between this range are more easily captured in the spleen and liver than in the lungs [289]. Spherical nanomedicines are mostly captured in the liver, while rod-shaped nanomedicines remain in the spleen and liver [290]. The smaller the cell–nanoparticle contact points, the more easily nanomedicines internalize into cancer cells. Thus, spherical and ovoid nanomedicines are more easily internalized than elongated nanomedicines [291]. Positively charged nanomedicines are more likely to be filtered out of blood by spleen, liver and lungs. Additionally, therefore, nanomedicines with a positive charge are the least suitable for maintaining prolonged blood circulation [292]. More importantly, the performance of nanomedicines can be improved by a variety of modifications, such as antibodies, peptides and cell membranes, to improve drug bioavailability, change surface charge, improve pharmacokinetic parameters or promote active targeting [293,294]. Lastly, another challenge that nanomedicines are facing is how to deliver therapeutic agents to defined cells. The difficulty is how to effectively identify the target cell among thousands of non-target cells. In this regard, active targeting nanomedicines offer fairly effective strategies [295]. The passive targeting of nanomedicines mainly depends on the enhanced permeability and retention (EPR) effect, and the distribution of nanomedicines largely relies on their size. Researchers proposed that the optimal size of nanoparticles is approximately 100 nm for long blood circulation and tumor accumulation [296]. However, active targeting nanomedicines can achieve this goal regardless of particle size. Active targeting refers to the modification of nanomedicines’ surface with ligands, such as peptides, antibodies, polysaccharides and aptamers, that can bind specifically to the target spots present on cancer cells, which can lead to a receptor- or antigen-mediated targeting strategy [297]. A large number of studies have shown that active targeting nanomedicines have more advantages than passive targeting nanomedicines. Therefore, active targeting nanomedicines are more suitable for drug delivery to overcome cancer drug resistance.
6. Conclusions
This review introduces the latest research progress of nanomedicines in overcoming cancer drug resistance. The study findings are very encouraging and strongly indicate that nanomedicines have great potential to overcome drug resistance in cancer. Moreover, this review discusses challenges and suggestions for the successful construction of nanomedicines with improved properties for overcoming cancer drug resistance, paving the way for their introduction into the clinic. Lastly, this review also provides a convenient guide for researchers to achieve a better understanding of significant findings in the field of nanomedicines to overcome cancer drug resistance experienced in recent years.
Author Contributions
T.H., data curation, formal analysis, investigation, and writing—original draft. H.G., data curation, funding acquisition, and writing—original draft. J.X., visualization. Y.H., validation. F.W., conceptualization, resources, software, and writing—review and editing. Z.H., conceptualization, funding acquisition, project administration, supervision, and writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Key Research and Development Program of China (2021YFC2009100); the Sichuan Science and Technology program (2019YFG0266); and the 1.3.5 project for disciplines of excellence—clinical research incubation project, West China Hospital, Sichuan University (2021HXFH064).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wu, Q.; Yang, Z.; Nie, Y.; Shi, Y.; Fan, D. Multi-drug resistance in cancer chemotherapeutics: Mechanisms and lab approaches. Cancer Lett. 2014, 347, 159–166. [Google Scholar] [CrossRef]
- Cohen, P.; Cross, D.; Jänne, P.A. Kinase drug discovery 20 years after imatinib: Progress and future directions. Nat. Rev. Drug Discov. 2021, 20, 551–569. [Google Scholar] [CrossRef] [PubMed]
- Bashash, D.; Zandi, Z.; Kashani, B.; Pourbagheri-Sigaroodi, A.; Salari, S.; Ghaffari, S.H. Resistance to immunotherapy in human malignancies: Mechanisms, research progresses, challenges, and opportunities. J. Cell. Physiol. 2022, 237, 346–372. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, M.M. Mechanisms of cancer drug resistance. Annu. Rev. Med. 2002, 53, 615–627. [Google Scholar] [CrossRef] [Green Version]
- Asić, K. Dominant mechanisms of primary resistance differ from dominant mechanisms of secondary resistance to targeted therapies. Crit. Rev. Oncol. Hematol. 2016, 97, 178–196. [Google Scholar] [CrossRef]
- Wang, W.; Sun, Y.; Liu, X.; Kumar, S.K.; Jin, F.; Dai, Y. Dual-targeted therapy circumvents non-genetic drug resistance to targeted therapy. Front. Oncol. 2022, 12, 859455. [Google Scholar] [CrossRef] [PubMed]
- Pluchino, K.M.; Hall, M.D.; Goldsborough, A.S.; Callaghan, R.; Gottesman, M.M. Collateral sensitivity as a strategy against cancer multidrug resistance. Drug Resist. Updat. 2012, 15, 98–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolaou, M.; Pavlopoulou, A.; Georgakilas, A.G.; Kyrodimos, E. The challenge of drug resistance in cancer treatment: A current overview. Clin Exp Metastasis 2018, 35, 309–318. [Google Scholar] [CrossRef]
- Nussinov, R.; Tsai, C.J.; Jang, H. Anticancer drug resistance: An update and perspective. Drug Resist. Updat. 2021, 59, 100796. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Wu, Z.X.; Assaraf, Y.G.; Chen, Z.S.; Wang, L. Overcoming anti-cancer drug resistance via restoration of tumor suppressor gene function. Drug Resist. Updat. 2021, 57, 100770. [Google Scholar] [CrossRef]
- Dallavalle, S.; Dobričić, V.; Lazzarato, L.; Gazzano, E.; Machuqueiro, M.; Pajeva, I.; Tsakovska, I.; Zidar, N.; Fruttero, R. Improvement of conventional anti-cancer drugs as new tools against multidrug resistant tumors. Drug Resist. Updat. 2020, 50, 100682. [Google Scholar] [CrossRef] [PubMed]
- Ravindran Menon, D.; Hammerlindl, H.; Torrano, J.; Schaider, H.; Fujita, M. Epigenetics and metabolism at the crossroads of stress-induced plasticity, stemness and therapeutic resistance in cancer. Theranostics 2020, 10, 6261–6277. [Google Scholar] [CrossRef] [PubMed]
- Barrueto, L.; Caminero, F.; Cash, L.; Makris, C.; Lamichhane, P.; Deshmukh, R.R. Resistance to checkpoint inhibition in cancer immunotherapy. Transl. Oncol. 2020, 13, 100738. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.W.; Barbie, D.A.; Flaherty, K.T. Mechanisms of resistance to immune checkpoint inhibitors. Br. J. Cancer 2018, 118, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Khalaf, K.; Hana, D.; Chou, J.T.; Singh, C.; Mackiewicz, A.; Kaczmarek, M. Aspects of the tumor microenvironment involved in immune resistance and drug resistance. Front. Immunol. 2021, 12, 656364. [Google Scholar] [CrossRef] [PubMed]
- Erin, N.; Grahovac, J.; Brozovic, A.; Efferth, T. Tumor microenvironment and epithelial mesenchymal transition as targets to overcome tumor multidrug resistance. Drug Resist. Updat. 2020, 53, 100715. [Google Scholar] [CrossRef] [PubMed]
- Elgendy, S.M.; Alyammahi, S.K.; Alhamad, D.W.; Abdin, S.M.; Omar, H.A. Ferroptosis: An emerging approach for targeting cancer stem cells and drug resistance. Crit. Rev. Oncol. Hematol. 2020, 155, 103095. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Z.; Ajani, J.A.; Song, S. Drug resistance and cancer stem cells. Cell Commun. Signal. 2021, 19, 19. [Google Scholar] [CrossRef]
- Su, Z.; Dong, S.; Zhao, S.C.; Liu, K.; Tan, Y.; Jiang, X.; Assaraf, Y.G.; Qin, B.; Chen, Z.S.; Zou, C. Novel nanomedicines to overcome cancer multidrug resistance. Drug Resist. Updat. 2021, 58, 100777. [Google Scholar] [CrossRef]
- Martin, J.D.; Cabral, H.; Stylianopoulos, T.; Jain, R.K. Improving cancer immunotherapy using nanomedicines: Progress, opportunities and challenges. Nat. Rev. Clin. Oncol. 2020, 17, 251–266. [Google Scholar] [CrossRef]
- Sharma, M.; Bakshi, A.K.; Mittapelly, N.; Gautam, S.; Marwaha, D.; Rai, N.; Singh, N.; Tiwari, P.; Agarwal, N.; Kumar, A. Recent updates on innovative approaches to overcome drug resistance for better outcomes in cancer. J. Control. Release 2022, 346, 43–70. [Google Scholar] [CrossRef] [PubMed]
- Sanaei, M.J.; Pourbagheri-Sigaroodi, A.; Kaveh, V.; Sheikholeslami, S.A.; Salari, S.; Bashash, D. The application of nano-medicine to overcome the challenges related to immune checkpoint blockades in cancer immunotherapy: Recent advances and opportunities. Crit. Rev. Oncol. Hematol. 2021, 157, 103160. [Google Scholar] [CrossRef]
- Wei, G.; Wang, Y.; Yang, G.; Wang, Y.; Ju, R. Recent progress in nanomedicine for enhanced cancer chemotherapy. Theranostics 2021, 11, 6370–6392. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Zhu, Y.; Wang, W.; Wang, G.; Zhang, S.; Cheng, H. Emerging nano-based strategies against drug resistance in tumor chemotherapy. Front. Bioeng. Biotechnol. 2021, 9, 798882. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Khan, A.R.; Yang, X.; Dong, B.; Ji, J.; Zhai, G. The reversal of chemotherapy-induced multidrug resistance by nanomedicine for cancer therapy. J. Control. Release 2021, 335, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Hong, W.; Ren, W.; Xu, T.; Qian, Z.; He, Z. Recent progress in targeted delivery vectors based on biomimetic nanoparticles. Signal Transduct. Target. Ther. 2021, 6, 225. [Google Scholar] [CrossRef]
- Liu, J.; Song, L.; Liu, S.; Zhao, S.; Jiang, Q.; Ding, B. A tailored DNA nanoplatform for synergistic RNAi-/chemotherapy of multidrug-resistant Tumors. Angew. Chem. Int. Ed. 2018, 57, 15486–15490. [Google Scholar] [CrossRef]
- Yi, S.; Liao, R.; Zhao, W.; Huang, Y.; He, Y. Multifunctional co-transport carriers based on cyclodextrin assembly for cancer synergistic therapy. Theranostics 2022, 12, 2560–2579. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Wang, M.; Wang, H.; Zhou, J.; Chen, J. Multifunctional human serum albumin fusion protein as a docetaxel nanocarrier for chemo-photothermal synergetic therapy of ovarian cancer. ACS Appl. Mater. Interfaces 2022, 14, 19907–19917. [Google Scholar] [CrossRef]
- Li, Z.; Chen, Y.; Yang, Y.; Yu, Y.; Zhang, Y.; Zhu, D.; Yu, X.; Ouyang, X.; Xie, Z.; Zhao, Y.; et al. Recent Advances in nanomaterials-based chemo-photothermal combination therapy for improving cancer treatment. Front. Bioeng. Biotechnol. 2019, 7, 293. [Google Scholar] [CrossRef]
- Zhang, C.; Zhou, X.; Zhang, H.; Han, X.; Li, B.; Yang, R.; Zhou, X. Recent progress of novel nanotechnology challenging the multidrug resistance of cancer. Front. Pharmacol. 2022, 13, 776895. [Google Scholar] [CrossRef] [PubMed]
- Muggia, F.M.; Hainsworth, J.D.; Jeffers, S.; Miller, M.; Groshen, S.; Roman, L.; Uziely, B.; Muderspach, L.; Garcia, A.; Burnett, A.; et al. Phase II study of liposomal doxorubicin in refractory ovarian cancer: Antitumor activity and toxicity modification by liposomal encapsulation. J. Clin. Oncol. 1997, 15, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, E.; Poizot-Martin, I.; Saint-Marc, T.; Spano, J.P.; Cacoub, P. Phase IV study of liposomal daunorubicin (DaunoXome) in AIDS-related Kaposi sarcoma. Am. J. Clin. Oncol. 2002, 25, 57–59. [Google Scholar] [CrossRef] [PubMed]
- Salehi, B.; Selamoglu, Z.; Mileski, K.S.; Pezzani, R.; Redaelli, M.; Cho, W.C.; Kobarfard, F.; Rajabi, S.; Martorell, M.; Kumar, P.; et al. Liposomal cytarabine as cancer therapy: From chemistry to medicine. Biomolecules 2019, 9, 773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berges, R.; Bello, U. Effect of a new leuprorelin formulation on testosterone levels in patients with advanced prostate cancer. Curr. Med. Res. Opin. 2006, 22, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Wang, L.; Xu, H.Q.; Huang, X.E.; Qian, Y.D.; Xiang, J. Clinical comparison between paclitaxel liposome (Lipusu®) and paclitaxel for treatment of patients with metastatic gastric cancer. Asian Pac. J. Cancer Prev. 2013, 14, 2591–2594. [Google Scholar] [CrossRef] [Green Version]
- Fraguas-Sánchez, A.I.; Lozza, I.; Torres-Suárez, A.I. Actively targeted nanomedicines in breast cancer: From pre-clinal investigation to clinic. Cancers 2022, 14, 1198. [Google Scholar] [CrossRef]
- Luo, C.; Wang, Y.; Chen, Q.; Han, X.; Liu, X.; Sun, J.; He, Z. Advances of paclitaxel formulations based on nanosystem delivery technology. Mini. Rev. Med. Chem. 2012, 12, 434–444. [Google Scholar] [CrossRef]
- Douer, D. Efficacy and safety of vincristine sulfate liposome injection in the treatment of adult acute lymphocytic leukemia. Oncologist 2016, 21, 840–847. [Google Scholar] [CrossRef] [Green Version]
- Milano, G.; Innocenti, F.; Minami, H. Liposomal irinotecan (Onivyde): Exemplifying the benefits of nanotherapeutic drugs. Cancer Sci. 2022, 113, 2224–2231. [Google Scholar] [CrossRef]
- Kang, Y.K.; Ryu, M.H.; Park, S.H.; Kim, J.G.; Kim, J.W.; Cho, S.H.; Park, Y.I.; Park, S.R.; Rha, S.Y.; Kang, M.J.; et al. Efficacy and safety findings from DREAM: A phase III study of DHP107 (oral paclitaxel) versus i.v. paclitaxel in patients with advanced gastric cancer after failure of first-line chemotherapy. Ann. Oncol. 2018, 29, 1220–1226. [Google Scholar] [CrossRef] [PubMed]
- Cafaro, A.; Giannini, M.B.; Silimbani, P.; Cangini, D.; Masini, C.; Ghelli Luserna Di Rorà, A.; Simonetti, G.; Martinelli, G.; Cerchione, C. CPX-351 daunorubicin-cytarabine liposome: A novel formulation to treat patients with newly diagnosed secondary acute myeloid leukemia. Minerva Med. 2020, 111, 455–466. [Google Scholar] [CrossRef]
- Bar-Zeev, M.; Livney, Y.D.; Assaraf, Y.G. Targeted nanomedicine for cancer therapeutics: Towards precision medicine overcoming drug resistance. Drug Resist. Updat. 2017, 31, 15–30. [Google Scholar] [CrossRef]
- Lepeltier, E.; Rijo, P.; Rizzolio, F.; Popovtzer, R.; Petrikaite, V.; Assaraf, Y.G.; Passirani, C. Nanomedicine to target multidrug resistant tumors. Drug Resist. Updat. 2020, 52, 100704. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Song, M.; Li, W.; Huang, J.; Yang, G.; Wang, Y. Multifunctional nanoplatforms co-delivering combinatorial dual-drug for eliminating cancer multidrug resistance. Theranostics 2021, 11, 6334–6354. [Google Scholar] [CrossRef]
- Chen, Z.S.; Tiwari, A.K. Multidrug resistance proteins (MRPs/ABCCs) in cancer chemotherapy and genetic diseases. FEBS J. 2011, 278, 3226–3245. [Google Scholar] [CrossRef] [Green Version]
- Amawi, H.; Sim, H.M.; Tiwari, A.K.; Ambudkar, S.V.; Shukla, S. ABC transporter-mediated multidrug-resistant cancer. Adv. Exp. Med. Biol. 2019, 1141, 549–580. [Google Scholar] [CrossRef]
- Muriithi, W.; Macharia, L.W.; Heming, C.P.; Echevarria, J.L.; Nyachieo, A.; Filho, P.N.; Neto, V.M. ABC transporters and the hallmarks of cancer: Roles in cancer aggressiveness beyond multidrug resistance. Cancer Biol. Med. 2020, 17, 253–269. [Google Scholar] [CrossRef]
- Rothem, L.; Ifergan, I.; Kaufman, Y.; Priest, D.G.; Jansen, G.; Assaraf, Y.G. Resistance to multiple novel antifolates is mediated via defective drug transport resulting from clustered mutations in the reduced folate carrier gene in human leukaemia cell lines. Biochem. J. 2002, 367, 741–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosson, G. Reduced folate carrier: Biochemistry and molecular biology of the normal and methotrexate-resistant cell. Br. J. Biomed. Sci. 2003, 60, 117–129. [Google Scholar] [CrossRef]
- Kordus, S.L.; Baughn, A.D. Revitalizing antifolates through understanding mechanisms that govern susceptibility and resistance. Medchemcomm 2019, 10, 880–895. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Bai, L.; Hou, L.; Deng, H.; Luan, S.; Liu, D.; Huang, M.; Zhao, L. Trends in targeting Bcl-2 anti-apoptotic proteins for cancer treatment. Eur. J. Med. Chem. 2022, 232, 114184. [Google Scholar] [CrossRef] [PubMed]
- Cory, S.; Roberts, A.W.; Colman, P.M.; Adams, J.M. Targeting BCL-2-like proteins to kill cancer cells. Trends Cancer 2016, 2, 443–460. [Google Scholar] [CrossRef] [PubMed]
- Sarosiek, K.A.; Letai, A. Directly targeting the mitochondrial pathway of apoptosis for cancer therapy using BH3 mimetics-recent successes, current challenges and future promise. FEBS J. 2016, 283, 3523–3533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.Y.; Guan, Y.D.; Chen, X.S.; Yang, J.M.; Cheng, Y. DNA repair pathways in cancer therapy and resistance. Front. Pharmacol. 2021, 11, 629266. [Google Scholar] [CrossRef] [PubMed]
- Alhmoud, J.F.; Woolley, J.F.; Al Moustafa, A.E.; Malki, M.I. DNA damage/repair management in cancers. Cancers 2020, 12, 1050. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, M.; Kastan, M.B. The DNA damage response: Implications for tumor responses to radiation and chemotherapy. Annu. Rev. Med. 2015, 66, 129–143. [Google Scholar] [CrossRef] [Green Version]
- Dal Bo, M.; De Mattia, E.; Baboci, L.; Mezzalira, S.; Cecchin, E.; Assaraf, Y.G.; Toffoli, G. New insights into the pharmacological, immunological, and CAR-T-cell approaches in the treatment of hepatocellular carcinoma. Drug Resist. Updat. 2020, 51, 100702. [Google Scholar] [CrossRef] [PubMed]
- Holohan, C.; Van Schaeybroeck, S.; Longley, D.B.; Johnston, P.G. Cancer drug resistance: An evolving paradigm. Nat. Rev. Cancer 2013, 13, 714–726. [Google Scholar] [CrossRef] [PubMed]
- Geller, L.T.; Barzily-Rokni, M.; Danino, T.; Jonas, O.H.; Shental, N.; Nejman, D.; Gavert, N.; Zwang, Y.; Cooper, Z.A.; Shee, K.; et al. Potential role of intratumor bacteria in mediating tumor resistance to the chemotherapeutic drug gemcitabine. Science 2017, 357, 1156–1160. [Google Scholar] [CrossRef] [Green Version]
- Dartier, J.; Lemaitre, E.; Chourpa, I.; Goupille, C.; Servais, S.; Chevalier, S.; Mahéo, K.; Dumas, J.F. ATP-dependent activity and mitochondrial localization of drug efflux pumps in doxorubicin-resistant breast cancer cells. Biochim. Biophys. Acta Gen. Subj. 2017, 1861, 1075–1084. [Google Scholar] [CrossRef]
- Ruan, L.; Chen, J.; Du, C.; Lu, H.; Zhang, J.; Cai, X.; Dou, R.; Lin, W.; Chai, Z.; Nie, G.; et al. Mitochondrial temperature-responsive drug delivery reverses drug resistance in lung cancer. Bioact. Mater. 2021, 13, 191–199. [Google Scholar] [CrossRef]
- Cheng, F.; Pan, Q.; Gao, W.; Pu, Y.; Luo, K.; He, B. Reversing chemotherapy resistance by a synergy between lysosomal pH-activated mitochondrial drug delivery and erlotinib-mediated drug efflux inhibition. ACS Appl. Mater. Interfaces 2021, 13, 29257–29268. [Google Scholar] [CrossRef]
- Zhou, M.; Li, L.; Li, L.; Lin, X.; Wang, F.; Li, Q.; Huang, Y. Overcoming chemotherapy resistance via simultaneous drug-efflux circumvention and mitochondrial targeting. Acta Pharm. Sin. B 2019, 9, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, C.; Chen, J.; Liu, L.; Hu, M.; Li, J.; Bi, H. Trackable mitochondria-targeting nanomicellar loaded with doxorubicin for overcoming drug resistance. ACS Appl. Mater. Interfaces 2017, 9, 25152–25163. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Peng, Y.; Qiu, L. Mitochondria-targeted vitamin E succinate delivery for reversal of multidrug resistance. J. Control. Release 2021, 337, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Sun, Y.; Li, Y.; Ma, X.; Zhang, S.; Yuan, Y.; Kohn, J.; Liu, C.; Qian, J. Synergistic combination of bioactive hydroxyapatite nanoparticles and the chemotherapeutic doxorubicin to overcome tumor multidrug resistance. Small 2021, 17, e2007672. [Google Scholar] [CrossRef] [PubMed]
- Gao, D.; Zhu, Q.; Ruan, J.; Sun, T.; Han, L. Polyplexes by polymerized dequalinium and bifunctional aptamer for mitochondrial targeting drug release to overcome drug resistance. ACS Appl. Bio. Mater. 2020, 3, 5182–5192. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, X.; Zhou, M.; Nan, X.; Chen, X.; Zhang, X. Mitochondrial-targeting lonidamine-doxorubicin nanoparticles for synergistic chemotherapy to conquer drug resistance. ACS Appl. Mater. Interfaces 2017, 9, 43498–43507. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Li, J.M.; Deng, K.; Zhou, W.; Wang, C.X.; Wang, Q.; Li, K.H.; Zhao, H.Y.; Huang, S.W. Tumor acidity activated triphenylphosphonium-based mitochondrial targeting nanocarriers for overcoming drug resistance of cancer therapy. Theranostics 2019, 9, 7033–7050. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Yu, H.; Zhang, L.J.; Wu, B.; Wang, C.X.; Wang, Q.; Deng, K.; Zhuo, R.X.; Huang, S.W. Redox-triggered activation of nanocarriers for mitochondria-targeting cancer chemotherapy. Nanoscale 2017, 9, 17044–17053. [Google Scholar] [CrossRef] [PubMed]
- Xiang, L.; Wang, Y.; Lan, J.; Na, F.; Wu, S.; Gong, Y.; Du, H.; Shao, B.; Xie, G. HIF-1-dependent heme synthesis promotes gemcitabine resistance in human non-small cell lung cancers via enhanced ABCB6 expression. Cell. Mol. Life Sci. 2022, 79, 343. [Google Scholar] [CrossRef] [PubMed]
- Samanta, D.; Gilkes, D.M.; Chaturvedi, P.; Xiang, L.; Semenza, G.L. Hypoxia-inducible factors are required for chemotherapy resistance of breast cancer stem cells. Proc. Natl. Acad. Sci. USA 2014, 111, E5429–E5438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karakashev, S.V.; Reginato, M.J. Progress toward overcoming hypoxia-induced resistance to solid tumor therapy. Cancer Manag. Res. 2015, 7, 253–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghattass, K.; Assah, R.; El-Sabban, M.; Gali-Muhtasib, H. Targeting hypoxia for sensitization of tumors to radio- and chemotherapy. Curr. Cancer Drug Targets 2013, 13, 670–685. [Google Scholar] [CrossRef]
- Albadari, N.; Deng, S.; Li, W. The transcriptional factors HIF-1 and HIF-2 and their novel inhibitors in cancer therapy. Expert Opin. Drug Discov. 2019, 14, 667–682. [Google Scholar] [CrossRef]
- Lu, H.; Samanta, D.; Xiang, L.; Zhang, H.; Hu, H.; Chen, I.; Bullen, J.W.; Semenza, G.L. Chemotherapy triggers HIF-1-dependent glutathione synthesis and copper chelation that induces the breast cancer stem cell phenotype. Proc. Natl. Acad. Sci. USA 2015, 112, E4600–E4609. [Google Scholar] [CrossRef] [Green Version]
- Luo, K.; Guo, W.; Yu, Y.; Xu, S.; Zhou, M.; Xiang, K.; Niu, K.; Zhu, X.; Zhu, G.; An, Z.; et al. Reduction-sensitive platinum (IV)-prodrug nano-sensitizer with an ultra-high drug loading for efficient chemo-radiotherapy of Pt-resistant cervical cancer in vivo. J. Control. Release 2020, 326, 25–37. [Google Scholar] [CrossRef]
- Li, J.; Xi, W.; Li, X.; Sun, H.; Li, Y. Advances in inhibition of protein-protein interactions targeting hypoxia-inducible factor-1 for cancer therapy. Bioorg. Med. Chem. 2019, 27, 1145–1158. [Google Scholar] [CrossRef]
- Wang, X.; Du, Z.W.; Xu, T.M.; Wang, X.J.; Li, W.; Gao, J.L.; Li, J.; Zhu, H. HIF-1α is a rational target for future ovarian cancer therapies. Front. Oncol. 2021, 11, 785111. [Google Scholar] [CrossRef]
- Shirai, Y.; Chow, C.C.T.; Kambe, G.; Suwa, T.; Kobayashi, M.; Takahashi, I.; Harada, H.; Nam, J.M. An overview of the recent development of anticancer agents targeting the HIF-1 transcription factor. Cancers 2021, 13, 2813. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Zhao, G. Small molecules targeting HIF-1α pathway for cancer therapy in recent years. Bioorg. Med. Chem. 2020, 28, 115235. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Xiang, X.; Li, S.; Xie, P.; Gong, Q.; Goh, B.C.; Wang, L. Targeting hypoxia-inducible factor-1, for cancer treatment: Recent advances in developing small-molecule inhibitors from natural compounds. Semin. Cancer Biol. 2022, 80, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Montigaud, Y.; Ucakar, B.; Krishnamachary, B.; Bhujwalla, Z.M.; Feron, O.; Préat, V.; Danhier, F.; Gallez, B.; Danhier, P. Optimized acriflavine-loaded lipid nanocapsules as a safe and effective delivery system to treat breast cancer. Int. J. Pharm. 2018, 551, 322–328. [Google Scholar] [CrossRef]
- Weijer, R.; Broekgaarden, M.; Krekorian, M.; Alles, L.K.; van Wijk, A.C.; Mackaaij, C.; Verheij, J.; van der Wal, A.C.; van Gulik, T.M.; Storm, G.; et al. Inhibition of hypoxia inducible factor 1 and topoisomerase with acriflavine sensitizes perihilar cholangiocarcinomas to photodynamic therapy. Oncotarget 2016, 7, 3341–3356. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; He, C.; Liu, X.; Chen, Y.; Zhao, P.; Chen, C.; Yan, R.; Li, M.; Fan, T.; Altine, B.; et al. One-pot synthesis of a microporous organosilica-coated cisplatin nanoplatform for HIF-1-targeted combination cancer therapy. Theranostics 2020, 10, 2918–2929. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Bao, Q.; Chen, Z.; Yao, L.; Ci, Z.; Wei, X.; Wu, Y.; Zhu, J.; Sun, K.; Zhou, G.; et al. Circumventing drug resistance pathways with a nanoparticle-based photodynamic method. Nano Lett. 2021, 21, 9115–9123. [Google Scholar] [CrossRef]
- Li, Y.; Deng, Y.; Tian, X.; Ke, H.; Guo, M.; Zhu, A.; Yang, T.; Guo, Z.; Ge, Z.; Yang, X.; et al. Multipronged design of light-triggered nanoparticles to overcome cisplatin resistance for efficient ablation of resistant tumor. ACS Nano 2015, 9, 9626–9637. [Google Scholar] [CrossRef]
- Yang, G.G.; Pan, Z.Y.; Zhang, D.Y.; Cao, Q.; Ji, L.N.; Mao, Z.W. Precisely assembled nanoparticles against cisplatin resistance via cancer-specific targeting of mitochondria and imaging-guided chemo-photothermal therapy. ACS Appl. Mater. Interfaces 2020, 12, 43444–43455. [Google Scholar] [CrossRef]
- Wang, T.; Wang, D.; Yu, H.; Wang, M.; Liu, J.; Feng, B.; Zhou, F.; Yin, Q.; Zhang, Z.; Huang, Y.; et al. Intracellularly acid-switchable multifunctional micelles for combinational photo/chemotherapy of the drug-resistant tumor. ACS Nano 2016, 10, 3496–3508. [Google Scholar] [CrossRef]
- Souslova, T.; Averill-Bates, D.A. Multidrug-resistant hela cells overexpressing MRP1 exhibit sensitivity to cell killing by hyperthermia: Interactions with etoposide. Int. J Radiat. Oncol. Biol. Phys. 2004, 60, 1538–1551. [Google Scholar] [CrossRef] [PubMed]
- Stein, U.; Jürchott, K.; Walther, W.; Bergmann, S.; Schlag, P.M.; Royer, H.D. Hyperthermia-induced nuclear translocation of transcription factor YB-1 leads to enhanced expression of multidrug resistance-related ABC transporters. J. Biol. Chem. 2001, 276, 28562–28569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, J.B.; Joseph, M.M.; Arya, J.S.; Sreedevi, P.; Sujai, P.T.; Maiti, K.K. Elucidating a thermoresponsive multimodal photo-chemotherapeutic nanodelivery vehicle to overcome the barriers of doxorubicin therapy. ACS Appl. Mater. Interfaces 2020, 12, 43365–43379. [Google Scholar] [CrossRef]
- Jiang, D.; Xu, M.; Pei, Y.; Huang, Y.; Chen, Y.; Ma, F.; Lu, H.; Chen, J. Core-matched nanoassemblies for targeted co-delivery of chemotherapy and photosensitizer to treat drug-resistant cancer. Acta Biomater. 2019, 88, 406–421. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.; Gao, X.; Kang, T.; Feng, X.; Yao, J.; Yang, M.; Jing, Y.; Zhu, Q.; Feng, J.; Chen, J. Actively targeting D-α-tocopheryl polyethylene glycol 1000 succinate-poly(lactic acid) nanoparticles as vesicles for chemo-photodynamic combination therapy of doxorubicin-resistant breast cancer. Nanoscale 2016, 8, 3100–3118. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wang, H.; Chen, Y.; Wang, Y.; Li, H.; Han, H.; Chen, T.; Jin, Q.; Ji, J. pH- and NIR light-responsive polymeric prodrug micelles for hyperthermia-assisted site-specific chemotherapy to reverse drug resistance in cancer treatment. Small 2016, 12, 2731–2740. [Google Scholar] [CrossRef] [PubMed]
- Gaio, E.; Conte, C.; Esposito, D.; Miotto, G.; Quaglia, F.; Moret, F.; Reddi, E. Co-delivery of docetaxel and disulfonate tetraphenyl chlorin in one nanoparticle produces strong synergism between chemo- and photodynamic therapy in drug-sensitive and -resistant cancer cells. Mol. Pharm. 2018, 15, 4599–4611. [Google Scholar] [CrossRef]
- Shi, C.; Huang, H.; Zhou, X.; Zhang, Z.; Ma, H.; Yao, Q.; Shao, K.; Sun, W.; Du, J.; Fan, J.; et al. Reversing multidrug resistance by inducing mitochondrial dysfunction for enhanced chemo-photodynamic therapy in tumor. ACS Appl. Mater. Interfaces 2021, 13, 45259–45268. [Google Scholar] [CrossRef]
- Huang, W.; Zhao, H.; Wan, J.; Zhou, Y.; Xu, Q.; Zhao, Y.; Yang, X.; Gan, L. pH- and photothermal-driven multistage delivery nanoplatform for overcoming cancer drug resistance. Theranostics 2019, 9, 3825–3839. [Google Scholar] [CrossRef]
- Shi, W.; Zhang, P.; Zou, F.; Zhou, J.; Yin, Z.; Cai, Z.; Ghaleb, H.; Jiang, Y.; Huang, W.; Liu, Y.; et al. Exploration of novel phthalazinone derivatives as potential efflux transporter inhibitors for reversing multidrug resistance and improving the oral absorption of paclitaxel. Eur. J. Med. Chem. 2022, 233, 114231. [Google Scholar] [CrossRef]
- Dong, J.; Qin, Z.; Zhang, W.-D.; Cheng, G.; Yehuda, A.G.; Ashby, C.R., Jr.; Chen, Z.-S.; Cheng, X.-D.; Qin, J.-J. Medicinal chemistry strategies to discover P-glycoprotein inhibitors: An update. Drug Resist. Updat. 2020, 49, 100681. [Google Scholar] [CrossRef] [PubMed]
- Halder, J.; Pradhan, D.; Kar, B.; Ghosh, G.; Rath, G. Nanotherapeutics approaches to overcome P-glycoprotein-mediated multi-drug resistance in cancer. Nanomedicine 2022, 40, 102494. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Xu, H.; Ashby, C.R., Jr.; Assaraf, Y.G.; Chen, Z.S.; Liu, H.M. Chemical molecular-based approach to overcome multidrug resistance in cancer by targeting P-glycoprotein (P-gp). Med. Res. Rev. 2021, 41, 525–555. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Shi, T.; Zhang, L.; Zhu, P.; Deng, M.; Huang, C.; Hu, T.; Jiang, L.; Li, J. Mammalian drug efflux transporters of the ATP binding cassette (ABC) family in multidrug resistance: A review of the past decade. Cancer Lett. 2016, 370, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Rana, M.S.; Ediriweera, M.K.; Rajagopalan, U.; Karunaratne, D.N.; Tennekoon, K.H.; Samarakoon, S.R. A new liposomal nanocarrier for co-delivery of gedunin and p-glycoprotein siRNA to target breast cancer stem cells. Nat. Prod. Res. 2022, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Kara, G.; Calin, G.A.; Ozpolat, B. RNAi-based therapeutics and tumor targeted delivery in cancer. Adv. Drug Deliv. Rev. 2022, 182, 114113. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, N.S.; Tekade, R.K.; Chougule, M.B. Nanocarrier mediated delivery of siRNA/miRNA in combination with chemotherapeutic agents for cancer therapy: Current progress and advances. J. Control. Release 2014, 194, 238–256. [Google Scholar] [CrossRef] [Green Version]
- Tsouris, V.; Joo, M.K.; Kim, S.H.; Kwon, I.C.; Won, Y.Y. Nano carriers that enable co-delivery of chemotherapy and RNAi agents for treatment of drug-resistant cancers. Biotechnol. Adv. 2014, 32, 1037–1050. [Google Scholar] [CrossRef]
- Zheng, M.; Jiang, T.; Yang, W.; Zou, Y.; Wu, H.; Liu, X.; Zhu, F.; Qian, R.; Ling, D.; McDonald, K.; et al. The siRNAsome: A cation-free and versatile nanostructure for siRNA and drug co-delivery. Angew. Chem. Int. Ed. 2019, 58, 4938–4942. [Google Scholar] [CrossRef]
- Curtin, N.J. DNA repair dysregulation from cancer driver to therapeutic target. Nat. Rev. Cancer 2012, 12, 801–817. [Google Scholar] [CrossRef]
- Yang, C.; Zang, W.; Tang, Z.; Ji, Y.; Xu, R.; Yang, Y.; Luo, A.; Hu, B.; Zhang, Z.; Liu, Z.; et al. A20/TNFAIP3 regulates the DNA damage response and mediates tumor cell resistance to DNA-damaging therapy. Cancer Res. 2018, 78, 1069–1082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stover, E.H.; Konstantinopoulos, P.A.; Matulonis, U.A.; Swisher, E.M. Biomarkers of response and resistance to DNA repair targeted therapies. Clin. Cancer Res. 2016, 22, 5651–5660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadoughi, F.; Mirsafaei, L.; Dana, P.M.; Hallajzadeh, J.; Asemi, Z.; Mansournia, M.A.; Montazer, M.; Hosseinpour, M.; Yousefi, B. The role of DNA damage response in chemo- and radio-resistance of cancer cells: Can DDR inhibitors sole the problem? DNA Repair 2021, 101, 103074. [Google Scholar] [CrossRef] [PubMed]
- Bouwman, P.; Jonkers, J. The effects of deregulated DNA damage signalling on cancer chemotherapy response and resistance. Nat. Rev. Cancer 2012, 12, 587–598. [Google Scholar] [CrossRef]
- Pilié, P.G.; Tang, C.; Mills, G.B.; Yap, T.A. State-of-the-art strategies for targeting the DNA damage response in cancer. Nat. Rev. Clin. Oncol. 2019, 16, 81–104. [Google Scholar] [CrossRef]
- Sharma, M.; Anand, P.; Padwad, Y.S.; Dogra, V.; Acharya, V. DNA damage response proteins synergistically affect the cancer prognosis and resistance. Free. Radic. Biol. Med. 2022, 178, 174–188. [Google Scholar] [CrossRef]
- Li, L.; Kumar, A.K.; Hu, Z.; Guo, Z. Small molecule inhibitors targeting key proteins in the DNA damage response for cancer therapy. Curr. Med. Chem. 2021, 28, 963–985. [Google Scholar] [CrossRef]
- Zhu, Y.; Hu, J.; Hu, Y.; Liu, W. Targeting DNA repair pathways: A novel approach to reduce cancer therapeutic resistance. Cancer Treat. Rev. 2009, 35, 590–596. [Google Scholar] [CrossRef]
- Helleday, T.; Petermann, E.; Lundin, C.; Hodgson, B.; Sharma, R.A. DNA repair pathways as targets for cancer therapy. Nat. Rev. Cancer 2008, 8, 193–204. [Google Scholar] [CrossRef]
- Wang, L.; Yu, Y.; Wei, D.; Zhang, L.; Zhang, X.; Zhang, G.; Ding, D.; Xiao, H.; Zhang, D. A systematic strategy of combinational blow for overcoming cascade drug resistance via NIR-light-triggered hyperthermia. Adv. Mater. 2021, 33, e2100599. [Google Scholar] [CrossRef]
- Tang, Y.; Chen, Y.; Zhang, Z.; Tang, B.; Zhou, Z.; Chen, H. Nanoparticle-based RNAi therapeutics targeting cancer stem cells: Update and prospective. Pharmaceutics 2021, 13, 2116. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Song, X.; Xu, D.; Tiek, D.; Goenka, A.; Wu, B.; Sastry, N.; Hu, B.; Cheng, S.Y. Stem cell programs in cancer initiation, progression, and therapy resistance. Theranostics 2020, 10, 8721–8743. [Google Scholar] [CrossRef] [PubMed]
- Dean, M.; Fojo, T.; Bates, S. Tumor stem cells and drug resistance. Nat. Rev. Cancer 2005, 5, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Phi, L.T.H.; Sari, I.N.; Yang, Y.G.; Lee, S.H.; Jun, N.; Kim, K.S.; Lee, Y.K.; Kwon, H.Y. Cancer stem cells (CSCs) in drug resistance and their therapeutic implications in cancer treatment. Stem Cells Int. 2018, 2018, 5416923. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Mayea, Y.; Mir, C.; Masson, F.; Paciucci, R.; LLeonart, M.E. Insights into new mechanisms and models of cancer stem cell multidrug resistance. Semin. Cancer Biol. 2020, 60, 166–180. [Google Scholar] [CrossRef]
- Shen, S.; Xu, X.; Lin, S.; Zhang, Y.; Liu, H.; Zhang, C.; Mo, R. A nanotherapeutic strategy to overcome chemotherapeutic resistance of cancer stem-like cells. Nat. Nanotechnol. 2021, 16, 104–113. [Google Scholar] [CrossRef]
- Wei, X.; Liu, L.; Guo, X.; Wang, Y.; Zhao, J.; Zhou, S. Light-activated ROS-responsive nanoplatform co-delivering apatinib and doxorubicin for enhanced chemo-photodynamic therapy of multidrug-resistant tumors. ACS Appl. Mater. Interfaces 2018, 10, 17672–17684. [Google Scholar] [CrossRef]
- Byeon, Y.; Lee, J.W.; Choi, W.S.; Won, J.E.; Kim, G.H.; Kim, M.G.; Wi, T.I.; Lee, J.M.; Kang, T.H.; Jung, I.D.; et al. CD44-targeting PLGA nanoparticles incorporating paclitaxel and FAK siRNA overcome chemoresistance in epithelial ovarian cancer. Cancer Res. 2018, 78, 6247–6256. [Google Scholar] [CrossRef] [Green Version]
- Wei, X.; Liu, L.; Li, X.; Wang, Y.; Guo, X.; Zhao, J.; Zhou, S. Selectively targeting tumor-associated macrophages and tumor cells with polymeric micelles for enhanced cancer chemo-immunotherapy. J. Control. Release 2019, 313, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Xing, Y.; Ding, T.; Wang, Z.; Wang, L.; Guan, H.; Tang, J.; Mo, D.; Zhang, J. Temporally controlled photothermal/photodynamic and combined therapy for overcoming multidrug resistance of cancer by polydopamine nanoclustered micelles. ACS Appl. Mater. Interfaces 2019, 11, 13945–13953. [Google Scholar] [CrossRef]
- Baghbani, F.; Moztarzadeh, F. Bypassing multidrug resistant ovarian cancer using ultrasound responsive doxorubicin/curcumin co-deliver alginate nanodroplets. Colloids Surf. B Biointerfaces 2017, 153, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Liu, X.; Li, G.; Wang, H.; Luo, Y.; Huang, G.; Wang, X.; Zeng, G.; Liu, Z.; Wu, S. Photoactivated H2 nanogenerator for enhanced chemotherapy of bladder cancer. ACS Nano 2020, 14, 8135–8148. [Google Scholar] [CrossRef] [PubMed]
- Younis, M.; Faming, W.; Hongyan, Z.; Mengmeng, T.; Hang, S.; Liudi, Y. Iguratimod encapsulated PLGA-NPs improves therapeutic outcome in glioma, glioma stem-like cells and temozolomide resistant glioma cells. Nanomedicine 2019, 22, 102101. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, M.; Jin, H.; Tang, Y.; Wu, A.; Xu, Q.; Huang, Y. Prodrug-like, PEGylated protein toxin trichosanthin for reversal of chemoresistance. Mol. Pharm. 2017, 14, 1429–1438. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Song, F.; Liu, Y.; Tian, J.; Liu, C.; Li, R.; Zhang, Q. A dual pH-sensitive liposomal system with charge-reversal and NO generation for overcoming multidrug resistance in cancer. Nanoscale 2019, 11, 3814–3826. [Google Scholar] [CrossRef]
- Kommineni, N.; Mahira, S.; Domb, A.J.; Khan, W. Cabazitaxel-loaded nanocarriers for cancer therapy with reduced side effects. Pharmaceutics 2019, 11, 141. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Wu, X.; Yang, H.; Li, L.; Ye, Z.; Rao, Y. A nuclear targeted Dox-aptamer loaded liposome delivery platform for the circumvention of drug resistance in breast cancer. Biomed. Pharmacother. 2019, 117, 109072. [Google Scholar] [CrossRef]
- Zhang, L.; Su, H.; Liu, Y.; Pang, N.; Li, J.; Qi, X.R. Enhancing solid tumor therapy with sequential delivery of dexamethasone and docetaxel engineered in a single carrier to overcome stromal resistance to drug delivery. J. Control. Release 2019, 294, 1–16. [Google Scholar] [CrossRef]
- Chen, Y.; Cheng, Y.; Zhao, P.; Zhang, S.; Li, M.; He, C.; Zhang, X.; Yang, T.; Yan, R.; Ye, P.; et al. Co-delivery of doxorubicin and imatinib by pH sensitive cleavable PEGylated nanoliposomes with folate-mediated targeting to overcome multidrug resistance. Int. J. Pharm. 2018, 542, 266–279. [Google Scholar] [CrossRef]
- Zhu, Y.X.; Jia, H.R.; Duan, Q.Y.; Liu, X.; Yang, J.; Liu, Y.; Wu, F.G. Photosensitizer-doped and plasma membrane-responsive liposomes for nuclear drug delivery and multidrug resistance reversal. ACS Appl. Mater. Interfaces 2020, 12, 36882–36894. [Google Scholar] [CrossRef]
- Wang, C.; Guan, W.; Peng, J.; Chen, Y.; Xu, G.; Dou, H. Gene/paclitaxel co-delivering nanocarriers prepared by framework-induced self-assembly for the inhibition of highly drug-resistant tumors. Acta Biomater. 2020, 103, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Jin, H.; Wang, C.; Zhang, Z.; Ruan, H.; Sun, L.; Yang, C.; Li, Y.; Qin, W.; Wang, C. Synergistic cisplatin/doxorubicin combination chemotherapy for multidrug-resistant cancer via polymeric nanogels targeting delivery. ACS Appl. Mater. Interfaces 2017, 9, 9426–9436. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Tung, C.H. Redox-responsive cisplatin nanogels for anticancer drug delivery. Chem. Commun. 2018, 54, 8367–8370. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, X.; Guo, Y.; Jia, H.R.; Jiang, Y.W.; Wu, F.G. Endosome/lysosome-detained supramolecular nanogels as an efflux retarder and autophagy inhibitor for repeated photodynamic therapy of multidrug-resistant cancer. Nanoscale Horiz. 2020, 5, 481–487. [Google Scholar] [CrossRef]
- Sun, L.; Wang, D.; Chen, Y.; Wang, L.; Huang, P.; Li, Y.; Liu, Z.; Yao, H.; Shi, J. Core-shell hierarchical mesostructured silica nanoparticles for gene/chemo-synergetic stepwise therapy of multidrug-resistant cancer. Biomaterials 2017, 133, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Del Valle, A.C.; Yeh, C.K.; Huang, Y.F. Near infrared-activatable platinum-decorated gold nanostars for synergistic photothermal/ferroptotic therapy in combating cancer drug resistance. Adv. Healthc. Mater. 2020, 9, e2000864. [Google Scholar] [CrossRef]
- Wang, Z.; Chang, Z.M.; Shao, D.; Zhang, F.; Chen, F.; Li, L.; Ge, M.F.; Hu, R.; Zheng, X.; Wang, Y.; et al. Janus gold triangle-mesoporous silica nanoplatforms for hypoxia-activated radio-chemo-photothermal therapy of liver cancer. ACS Appl. Mater. Interfaces 2019, 11, 34755–34765. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Jiang, Z.; Xu, W.; Sun, T.; Zhuang, X.; Ding, J.; Chen, X. Spatiotemporally targeted nanomedicine overcomes hypoxia-induced drug resistance of tumor cells after disrupting neovasculature. Nano Lett. 2020, 20, 6191–6198. [Google Scholar] [CrossRef]
- Zhang, H.; Cui, W.; Qu, X.; Wu, H.; Qu, L.; Zhang, X.; Mäkilä, E.; Salonen, J.; Zhu, Y.; Yang, Z.; et al. Photothermal-responsive nanosized hybrid polymersome as versatile therapeutics codelivery nanovehicle for effective tumor suppression. Proc. Natl. Acad. Sci. USA 2019, 116, 7744–7749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Wang, F.; Wang, S.; Liu, L.; Liu, K.; Ye, Y.; Wang, Z.; Wang, H.; Chen, B.; Jiang, J.; et al. Hyperthermia-triggered on-demand biomimetic nanocarriers for synergetic photothermal and chemotherapy. Adv. Sci. 2020, 7, 1903642. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Xiao, Y.; Yin, Y.; Li, G.; Peng, J. Erythrocyte membrane-camouflaged IR780 and DTX coloading polymeric nanoparticles for imaging-guided cancer photo-chemo combination therapy. Mol. Pharm. 2019, 16, 3208–3220. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lv, F.M.; Wang, D.L.; Du, J.L.; Guo, H.Y.; Chen, H.N.; Zhao, S.J.; Liu, Z.P.; Liu, Y. Synergistic antitumor effects on drug-resistant breast cancer of paclitaxel/lapatinib composite canocrystals. Molecules 2020, 25, 604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; He, D.; Guo, Q.; Zhang, Z.; Ru, D.; Wang, L.; Gong, K.; Liu, F.; Duan, Y.; Li, H. Exosome-liposome hybrid nanoparticle codelivery of TP and miR497 conspicuously overcomes chemoresistant ovarian cancer. J. Nanobiotechnology 2022, 20, 50. [Google Scholar] [CrossRef] [PubMed]
- Russo, E.; Spallarossa, A.; Tasso, B.; Villa, C.; Brullo, C. Nanotechnology of tyrosine kinase inhibitors in cancer therapy: A perspective. Int. J. Mol. Sci. 2021, 22, 6538. [Google Scholar] [CrossRef]
- Liang, X.; Wu, P.; Yang, Q.; Xie, Y.; He, C.; Yin, L.; Yin, Z.; Yue, G.; Zou, Y.; Li, L.; et al. An update of new small-molecule anticancer drugs approved from 2015 to 2020. Eur. J. Med. Chem. 2021, 220, 113473. [Google Scholar] [CrossRef]
- Ferguson, F.M.; Gray, N.S. Kinase inhibitors: The road ahead. Nat. Rev. Drug Discov. 2018, 17, 353–377. [Google Scholar] [CrossRef]
- Attwood, M.M.; Fabbro, D.; Sokolov, A.V.; Knapp, S.; Schiöth, H.B. Trends in kinase drug discovery: Targets, indications and inhibitor design. Nat. Rev. Drug Discov. 2021, 20, 839–861. [Google Scholar] [CrossRef]
- Bergholz, J.S.; Wang, Q.; Kabraji, S.; Zhao, J.J. Integrating immunotherapy and targeted therapy in cancer treatment: Mechanistic insights and clinical implications. Clin. Cancer Res. 2020, 26, 5557–5566. [Google Scholar] [CrossRef]
- Chen, E.Y.; Raghunathan, V.; Prasad, V. An overview of cancer drugs approved by the US food and drug administration based on the surrogate end point of response rate. JAMA Intern. Med. 2019, 179, 915–921. [Google Scholar] [CrossRef]
- Du, J.; Yan, H.; Xu, Z.; Yang, B.; He, Q.; Wang, X.; Luo, P. Cutaneous toxicity of FDA-approved small-molecule kinase inhibitors. Expert Opin. Drug Metab. Toxicol. 2021, 17, 1311–1325. [Google Scholar] [CrossRef]
- Zhong, L.; Li, Y.; Xiong, L.; Wang, W.; Wu, M.; Yuan, T.; Yang, W.; Tian, C.; Miao, Z.; Wang, T.; et al. Small molecules in targeted cancer therapy: Advances, challenges, and future perspectives. Signal Transduct. Target. Ther. 2021, 6, 201. [Google Scholar] [CrossRef] [PubMed]
- Pisa, R.; Kapoor, T.M. Chemical strategies to overcome resistance against targeted anticancer therapeutics. Nat. Chem. Biol. 2020, 16, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Pi, M.; Kuang, H.; Yue, C.; Yang, Q.; Wu, A.; Li, Y.; Assaraf, Y.G.; Yang, D.H.; Wu, S. Targeting metabolism to overcome cancer drug resistance: A promising therapeutic strategy for diffuse large B cell lymphoma. Drug Resist. Updat. 2022, 61, 100822. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Ji, Q.; Li, Q. Resistance to anti-EGFR therapies in metastatic colorectal cancer: Underlying mechanisms and reversal strategies. J. Exp. Clin. Cancer Res. 2021, 40, 328. [Google Scholar] [CrossRef] [PubMed]
- Asao, T.; Takahashi, F.; Takahashi, K. Resistance to molecularly targeted therapy in non-small-cell lung cancer. Respir. Investig. 2019, 57, 20–26. [Google Scholar] [CrossRef]
- Ye, L.; Chen, X.; Zhou, F. EGFR-mutant NSCLC: Emerging novel drugs. Curr. Opin. Oncol. 2021, 33, 87–94. [Google Scholar] [CrossRef]
- Hochart, A.; Leblond, P.; Le Bourhis, X.; Meignan, S.; Tulasne, D. Inhibition du récepteur MET: Un espoir dans la lutte contre les résistances aux thérapies ciblées? [MET receptor inhibition: Hope against resistance to targeted therapies?]. Bull. Cancer. 2017, 104, 157–166. [Google Scholar] [CrossRef]
- Rezayatmand, H.; Razmkhah, M.; Razeghian-Jahromi, I. Drug resistance in cancer therapy: The Pandora’s Box of cancer stem cells. Stem Cell Res. Ther. 2022, 13, 181. [Google Scholar] [CrossRef]
- Adhikari, S.; Bhattacharya, A.; Adhikary, S.; Singh, V.; Gadad, S.S.; Roy, S.; Das, C. The paradigm of drug resistance in cancer: An epigenetic perspective. Biosci. Rep. 2022, 42, BSR20211812. [Google Scholar] [CrossRef]
- Najafi, M.; Farhood, B.; Mortezaee, K. Cancer stem cells (CSCs) in cancer progression and therapy. J. Cell Physiol. 2019, 234, 8381–8395. [Google Scholar] [CrossRef]
- Deng, J.; Shao, J.; Markowitz, J.S.; An, G. ABC transporters in multi-drug resistance and ADME-Tox of small molecule tyrosine kinase inhibitors. Pharm. Res. 2014, 31, 2237–2255. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Ye, J.; Xie, Q.; Liu, B.; Liu, M. Targeting regulated cell death with pharmacological small molecules: An update on autophagy-dependent cell death, ferroptosis, and necroptosis in cancer. J. Med. Chem. 2022, 65, 2989–3001. [Google Scholar] [CrossRef] [PubMed]
- Jones, V.S.; Huang, R.Y.; Chen, L.P.; Chen, Z.S.; Fu, L.; Huang, R.P. Cytokines in cancer drug resistance: Cues to new therapeutic strategies. Biochim. Biophys. Acta 2016, 1865, 255–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skoulidis, F.; Papadimitrakopoulou, V.A. Targeting the gatekeeper: Osimertinib in EGFR T790M mutation-positive non-small cell lung cancer. Clin. Cancer Res. 2017, 23, 618–622. [Google Scholar] [CrossRef] [Green Version]
- Mayor, S. Osimertinib effective in EGFR T790M-positive lung cancer. Lancet Oncol. 2017, 18, e9. [Google Scholar] [CrossRef]
- Carlisle, J.W.; Ramalingam, S.S. Role of osimertinib in the treatment of EGFR-mutation positive non-small-cell lung cancer. Future Oncol. 2019, 15, 805–816. [Google Scholar] [CrossRef]
- Tang, Z.H.; Lu, J.J. Osimertinib resistance in non-small cell lung cancer: Mechanisms and therapeutic strategies. Cancer Lett. 2018, 420, 242–246. [Google Scholar] [CrossRef]
- Lu, X.; Yu, L.; Zhang, Z.; Ren, X.; Smaill, J.B.; Ding, K. Targeting EGFRL858R/T790M and EGFRL858R/T790M/C797S resistance mutations in NSCLC: Current developments in medicinal chemistry. Med. Res. Rev. 2018, 38, 1550–1581. [Google Scholar] [CrossRef]
- Chen, W.; Yu, D.; Sun, S.Y.; Li, F. Nanoparticles for co-delivery of osimertinib and selumetinib to overcome osimertinib-acquired resistance in non-small cell lung cancer. Acta Biomater. 2021, 129, 258–268. [Google Scholar] [CrossRef]
- Lim, S.M.; Yang, S.D.; Lim, S.; Heo, S.G.; Daniel, S.; Markovets, A.; Minoo, R.; Pyo, K.H.; Yun, M.R.; Hong, M.H.; et al. Molecular landscape of osimertinib resistance in patients and patient-derived preclinical models. Ther. Adv. Med. Oncol. 2022, 14, 17588359221079125. [Google Scholar] [CrossRef] [PubMed]
- Chude, C.I.; Amaravadi, R.K. Targeting autophagy in cancer: Update on clinical trials and novel inhibitors. Int. J. Mol. Sci. 2017, 18, 1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, J.M.M.; Towers, C.G.; Thorburn, A. Targeting autophagy in cancer. Nat. Rev. Cancer 2017, 17, 528–542. [Google Scholar] [CrossRef]
- Ishaq, M.; Ojha, R.; Sharma, A.P.; Singh, S.K. Autophagy in cancer: Recent advances and future directions. Semin. Cancer Biol. 2020, 66, 171–181. [Google Scholar] [CrossRef]
- Tan, Q.; Wang, Z.; Wang, Q.; Wang, Y.; Huang, Z.; Su, N.; Jin, M.; Kuang, L.; Qi, H.; Ni, Z.; et al. A novel FGFR1-binding peptide exhibits anti-tumor effect on lung cancer by inhibiting proliferation and angiogenesis. Int. J. Biol. Sci. 2018, 14, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Han, L.L.; Du, F.; Liu, X.M.; Li, J.; Wang, H.H.; Song, M.H.; Li, Z.; Li, G.Y. FGFR1 induces acquired resistance against gefitinib by activating AKT/mTOR pathway in NSCLC. Onco Targets Ther. 2019, 12, 9809–9816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farnsworth, D.A.; Chen, Y.T.; de Rappard Yuswack, G.; Lockwood, W.W. Emerging molecular dependencies of mutant EGFR-Driven non-small cell lung cancer. Cells 2021, 10, 3553. [Google Scholar] [CrossRef]
- Vad-Nielsen, J.; Gammelgaard, K.R.; Daugaard, T.F.; Nielsen, A.L. Cause-and-effect relationship between FGFR1 expression and epithelial-mesenchymal transition in EGFR-mutated non-small cell lung cancer cells. Lung Cancer 2019, 132, 132–140. [Google Scholar] [CrossRef]
- Gu, Y.; Lai, S.; Dong, Y.; Fu, H.; Song, L.; Chen, T.; Duan, Y.; Zhang, Z. AZD9291 resistance reversal activity of a pH-sensitive nanocarrier dual-loaded with chloroquine and FGFR1 inhibitor in NSCLC. Adv. Sci. 2020, 8, 2002922. [Google Scholar] [CrossRef]
- Feng, Y.; Wang, L.; Wang, T.; Li, Y.; Xun, Q.; Zhang, R.; Liu, L.; Li, L.; Wang, W.; Tian, Y.; et al. Tumor cell-secreted exosomal miR-22-3p inhibits transgelin and induces vascular abnormalization to promote tumor budding. Mol. Ther. 2021, 29, 2151–2166. [Google Scholar] [CrossRef]
- Emami Nejad, A.; Najafgholian, S.; Rostami, A.; Sistani, A.; Shojaeifar, S.; Esparvarinha, M.; Nedaeinia, R.; Haghjooy Javanmard, S.; Taherian, M.; Ahmadlou, M.; et al. The role of hypoxia in the tumor microenvironment and development of cancer stem cell: A novel approach to developing treatment. Cancer Cell Int. 2021, 21, 62. [Google Scholar] [CrossRef]
- Mazumdar, J.; Dondeti, V.; Simon, M.C. Hypoxia-inducible factors in stem cells and cancer. J. Cell Mol. Med. 2009, 13, 4319–4328. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.; Huang, F.; Xu, X.; He, H.; Zhang, Y. High expression of hypoxia inducible factor 1α related with acquired resistant to EGFR tyrosine kinase inhibitors in NSCLC. Sci. Rep. 2021, 11, 1199. [Google Scholar] [CrossRef] [PubMed]
- Meng, S.; Wang, G.; Lu, Y.; Fan, Z. Functional cooperation between HIF-1α and c-Jun in mediating primary and acquired resistance to gefitinib in NSCLC cells with activating mutation of EGFR. Lung Cancer 2018, 121, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Liu, Y.; Oeck, S.; Zhang, G.J.; Schramm, A.; Glazer, P.M. Hypoxia induces resistance to EGFR inhibitors in lung cancer cells via upregulation of FGFR1 and the MAPK pathway. Cancer Res. 2020, 80, 4655–4667. [Google Scholar] [CrossRef] [PubMed]
- Bera, H.; Abosheasha, M.A.; Ito, Y.; Ueda, M. Hypoxia-responsive pullulan-based nanoparticles as erlotinib carriers. Int. J. Biol. Macromol. 2021, 191, 764–774. [Google Scholar] [CrossRef] [PubMed]
- Bera, H.; Abosheasha, M.A.; Ito, Y.; Ueda, M. Etherified pullulan-polyethylenimine based nanoscaffolds improved chemosensitivity of erlotinib on hypoxic cancer cells. Carbohydr. Polym. 2021, 271, 118441. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Xu, L.; Li, X.; Li, Z.; Wang, J.; Chen, H.; Li, X.; Gao, Y. Co-delivery of gefitinib and hematoporphyrin by aptamer-modified fluorinated dendrimer for hypoxia alleviation and enhanced synergistic chemo-photodynamic therapy of NSCLC. Eur. J. Pharm. Sci. 2021, 167, 106004. [Google Scholar] [CrossRef] [PubMed]
- Guan, Q.; Li, Y.; Zhang, H.; Liu, S.; Ding, Z.; Fan, Z.; Wang, Q.; Wang, Z.; Han, J.; Liu, M.; et al. Laser-responsive multi-functional nanoparticles for efficient combinational chemo-photodynamic therapy against breast cancer. Colloids Surf. B Biointerfaces 2022, 216, 112574. [Google Scholar] [CrossRef] [PubMed]
- Gong, G.; Pan, J.; He, Y.; Shang, J.; Wang, X.; Zhang, Y.; Zhang, G.; Wang, F.; Zhao, G.; Guo, J. Self-assembly of nanomicelles with rationally designed multifunctional building blocks for synergistic chemo-photodynamic therapy. Theranostics 2022, 12, 2028–2040. [Google Scholar] [CrossRef]
- Wang, Y.; Huo, J.; Li, S.; Huang, R.; Fan, D.; Cheng, H.; Wan, B.; Du, Y.; He, H.; Zhang, G. Self-rectifiable and hypoxia-assisted chemo-photodynamic nanoinhibitor for synergistic cancer therapy. ACS Appl. Mater. Interfaces 2022, 14, 10092–10101. [Google Scholar] [CrossRef]
- Yang, Y.; Chen, F.; Xu, N.; Yao, Q.; Wang, R.; Xie, X.; Zhang, F.; He, Y.; Shao, D.; Dong, W.F.; et al. Red-light-triggered self-destructive mesoporous silica nanoparticles for cascade-amplifying chemo-photodynamic therapy favoring antitumor immune responses. Biomaterials 2022, 281, 121368. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Wang, S.; Deng, D.; Xiao, Z.; Dong, Z.; Wang, Z.; Lei, Q.; Gao, S.; Huang, G.; Zhang, E.; et al. Fluorinated chitosan to enhance transmucosal delivery of sonosensitizer-conjugated catalase for sonodynamic bladder cancer treatment post-intravesical instillation. ACS Nano 2020, 14, 1586–1599. [Google Scholar] [CrossRef] [PubMed]
- She, J.; Zhou, X.; Zhang, Y.; Zhang, R.; Li, Q.; Zhu, W.; Meng, Z.; Liu, Z. Thermo-triggered in situ chitosan-based gelation system for repeated and enhanced sonodynamic therapy post a single injection. Adv. Healthc. Mater. 2021, 10, e2001208. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Liang, S.; Zhou, Y.; Xiao, X.; Liu, B.; Yang, C.; Ma, P.; Cheng, Z.; Lin, J. A robust oxygen-carrying hemoglobin-based natural sonosensitizer for sonodynamic cancer therapy. Nano Lett. 2021, 21, 6042–6050. [Google Scholar] [CrossRef] [PubMed]
- Ren, Q.; Yu, N.; Wang, L.; Wen, M.; Geng, P.; Jiang, Q.; Li, M.; Chen, Z. Nanoarchitectonics with metal-organic frameworks and platinum nanozymes with improved oxygen evolution for enhanced sonodynamic/chemo-therapy. J. Colloid Interface Sci. 2022, 614, 147–159. [Google Scholar] [CrossRef]
- Sun, D.; Pang, X.; Cheng, Y.; Ming, J.; Xiang, S.; Zhang, C.; Lv, P.; Chu, C.; Chen, X.; Liu, G.; et al. Ultrasound-switchable nanozyme augments sonodynamic therapy against multidrug-resistant bacterial infection. ACS Nano 2020, 14, 2063–2076. [Google Scholar] [CrossRef]
- Gong, Z.; Dai, Z. Design and challenges of sonodynamic therapy system for cancer theranostics: From equipment to sensitizers. Adv. Sci. 2021, 8, 2002178. [Google Scholar] [CrossRef]
- Dong, C.; Hu, H.; Sun, L.; Chen, Y. Inorganic chemoreactive nanosonosensitzers with unique physiochemical properties and structural features for versatile sonodynamic nanotherapies. Biomed. Mater. 2021, 16, 032006. [Google Scholar] [CrossRef]
- Li, D.; Yang, Y.; Li, D.; Pan, J.; Chu, C.; Liu, G. Organic sonosensitizers for sonodynamic therapy: From small molecules and nanoparticles toward clinical development. Small 2021, 17, e2101976. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Zhang, L.; Wang, J.; Zhu, L.; Li, Z.; Chen, H.; Gao, Y. An intelligent hypoxia-relieving chitosan-based nanoplatform for enhanced targeted chemo-sonodynamic combination therapy on lung cancer. Carbohydr. Polym. 2021, 274, 118655. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.L.; Pernemalm, M.; Crosbie, P.A.; Whetton, A.D. The role of the tumor-microenvironment in lung cancer-metastasis and its relationship to potential therapeutic targets. Cancer Treat. Rev. 2014, 40, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Breindel, J.L.; Haskins, J.W.; Cowell, E.P.; Zhao, M.; Nguyen, D.X.; Stern, D.F. EGF receptor activates MET through MAPK to enhance non-small cell lung carcinoma invasion and brain metastasis. Cancer Res. 2013, 73, 5053–5065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellerino, A.; Bruno, F.; Rudà, R.; Soffietti, R. Systemic therapy for lung cancer brain metastases. Curr. Treat. Options Oncol. 2021, 22, 110. [Google Scholar] [CrossRef] [PubMed]
- Franchino, F.; Rudà, R.; Soffietti, R. Mechanisms and therapy for cancer metastasis to the brain. Front. Oncol. 2018, 8, 161. [Google Scholar] [CrossRef] [Green Version]
- Yin, W.; Zhao, Y.; Kang, X.; Zhao, P.; Fu, X.; Mo, X.; Wang, Y.; Huang, Y. BBB-penetrating codelivery liposomes treat brain metastasis of non-small cell lung cancer with EGFRT790M mutation. Theranostics 2020, 10, 6122–6135. [Google Scholar] [CrossRef]
- Han, W.; Shi, L.; Ren, L.; Zhou, L.; Li, T.; Qiao, Y.; Wang, H. A nanomedicine approach enables co-delivery of cyclosporin A and gefitinib to potentiate the therapeutic efficacy in drug-resistant lung cancer. Signal Transduct. Target. Ther. 2018, 3, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, D.; Zhang, F.; Wang, J.; He, H.; Duan, S.; Zhu, R.; Chen, C.; Yin, L.; Chen, Y. Biodegradable nanoparticles mediated co-delivery of erlotinib (ELTN) and fedratinib (FDTN) toward the treatment of ELTN-resistant non-small cell lung cancer (NSCLC) via suppression of the JAK2/STAT3 signaling pathway. Front. Pharmacol. 2018, 9, 1214. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Zhang, H.; Zhang, Y.; Lv, T.; Zhang, L.; Li, Z.; Xie, X.; Li, F.; Chen, H.; Jia, L. Erlotinib-guided self-assembled trifunctional click nanotheranostics for distinguishing druggable mutations and synergistic therapy of nonsmall cell lung cancer. Mol. Pharm. 2018, 15, 5146–5161. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.; Yu, X.; Kang, X.; Zhao, Y.; Zhao, P.; Jin, H.; Fu, X.; Wan, Y.; Peng, C.; Huang, Y. Remodeling tumor-associated macrophages and neovascularization overcomes EGFRT790M-associated drug resistance by PD-L1 nanobody-mediated codelivery. Small 2018, 14, e1802372. [Google Scholar] [CrossRef]
- Peng, H.; Chen, B.; Huang, W.; Tang, Y.; Jiang, Y.; Zhang, W.; Huang, Y. Reprogramming tumor-associated macrophages to reverse EGFRT790M resistance by dual-targeting codelivery of gefitinib/vorinostat. Nano Lett. 2017, 17, 7684–7690. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Mei, H.; Gao, Y.; Xie, X.; Nie, H.; Li, T.; Zhang, H.; Jia, L. Co-delivery of oxygen and erlotinib by aptamer-modified liposomal complexes to reverse hypoxia-induced drug resistance in lung cancer. Biomaterials 2017, 145, 56–71. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.B.; Kim, H.R.; Ha, S.J. Immune checkpoint inhibitors in 10 Years: Contribution of basic research and clinical application in cancer immunotherapy. Immune Netw. 2022, 22, e2. [Google Scholar] [CrossRef] [PubMed]
- Seidel, J.A.; Otsuka, A.; Kabashima, K. Anti-PD-1 and anti-CTLA-4 therapies in cancer: Mechanisms of action, efficacy, and limitations. Front. Oncol. 2018, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Pisibon, C.; Ouertani, A.; Bertolotto, C.; Ballotti, R.; Cheli, Y. Immune checkpoints in cancers: From signaling to the clinic. Cancers 2021, 13, 4573. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Man, S.; Sun, R.; Li, Z.; Wu, Y.; Zuo, D. Recent advances and challenges of immune checkpoint inhibitors in immunotherapy of non-small cell lung cancer. Int. Immunopharmacol. 2020, 85, 106613. [Google Scholar] [CrossRef]
- O’Donnell, J.S.; Teng, M.; Smyth, M.J. Cancer immunoediting and resistance to T cell-based immunotherapy. Nat. Rev. Clin. Oncol. 2019, 16, 151–167. [Google Scholar] [CrossRef]
- Haddad, A.F.; Young, J.S.; Gill, S.; Aghi, M.K. Resistance to immune checkpoint blockade: Mechanisms, counter-acting approaches, and future directions. Semin Cancer Biol. 2022, in press. [Google Scholar] [CrossRef]
- Kalbasi, A.; Ribas, A. Tumour-intrinsic resistance to immune checkpoint blockade. Nat. Rev. Immunol. 2020, 20, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Gondhowiardjo, S.A.; Handoko; Jayalie, V.F.; Apriantoni, R.; Barata, A.R.; Senoaji, F.; Utami, I.; Maubere, F.; Nuryadi, E.; Giselvania, A. Tackling resistance to cancer immunotherapy: What do we know? Molecules 2020, 25, 4096. [Google Scholar] [CrossRef] [PubMed]
- Fares, C.M.; Van Allen, E.M.; Drake, C.G.; Allison, J.P.; Hu-Lieskovan, S. Mechanisms of resistance to immune checkpoint blockade: Why does checkpoint inhibitor immunotherapy not work for all patients? Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 147–164. [Google Scholar] [CrossRef]
- Dianat-Moghadam, H.; Mahari, A.; Salahlou, R.; Khalili, M.; Azizi, M.; Sadeghzadeh, H. Immune evader cancer stem cells direct the perspective approaches to cancer immunotherapy. Stem Cell Res. Ther. 2022, 13, 150. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Jia, Y.; Yu, Y.; Zhang, B.; Xu, F.; Guo, H. Targeting the tumor biophysical microenvironment to reduce resistance to immunotherapy. Adv. Drug Deliv. Rev. 2022, 186, 114319. [Google Scholar] [CrossRef] [PubMed]
- Gide, T.N.; Wilmott, J.S.; Scolyer, R.A.; Long, G.V. Primary and acquired resistance to immune checkpoint inhibitors in metastatic melanoma. Clin. Cancer Res. 2018, 24, 1260–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Draghi, A.; Chamberlain, C.A.; Furness, A.; Donia, M. Acquired resistance to cancer immunotherapy. Semin. Immunopathol. 2019, 41, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Saleh, R.; Elkord, E. Treg-mediated acquired resistance to immune checkpoint inhibitors. Cancer Lett. 2019, 457, 168–179. [Google Scholar] [CrossRef] [PubMed]
- Crispen, P.L.; Kusmartsev, S. Mechanisms of immune evasion in bladder cancer. Cancer Immunol. Immunother. 2020, 69, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Saleh, R.; Elkord, E. Acquired resistance to cancer immunotherapy: Role of tumor-mediated immunosuppression. Semin. Cancer Biol. 2020, 65, 13–27. [Google Scholar] [CrossRef]
- Aspeslagh, S.; Chabanon, R.M.; Champiat, S.; Postel-Vinay, S. Understanding genetic determinants of resistance to immune checkpoint blockers. Semin. Cancer Biol. 2020, 65, 123–139. [Google Scholar] [CrossRef]
- Peng, W.; Chen, J.Q.; Liu, C.; Malu, S.; Creasy, C.; Tetzlaff, M.T.; Xu, C.; McKenzie, J.A.; Zhang, C.; Liang, X.; et al. Loss of PTEN promotes resistance to T cell-mediated immunotherapy. Cancer Discov. 2016, 6, 202–216. [Google Scholar] [CrossRef] [Green Version]
- Cretella, D.; Digiacomo, G.; Giovannetti, E.; Cavazzoni, A. PTEN alterations as a potential mechanism for tumor cell escape from PD-1/PD-L1 inhibition. Cancers 2019, 11, 1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cetintas, V.B.; Batada, N.N. Is there a causal link between PTEN deficient tumors and immunosuppressive tumor microenvironment? J. Transl. Med. 2020, 18, 45. [Google Scholar] [CrossRef] [Green Version]
- Feng, S.; Cheng, X.; Zhang, L.; Lu, X.; Chaudhary, S.; Teng, R.; Frederickson, C.; Champion, M.M.; Zhao, R.; Cheng, L.; et al. Myeloid-derived suppressor cells inhibit T cell activation through nitrating LCK in mouse cancers. Proc. Natl. Acad. Sci. USA 2018, 115, 10094–10099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, M.D.; Shinde, R.; McGaha, T.L.; Huang, L.; Holmgaard, R.B.; Wolchok, J.D.; Mautino, M.R.; Celis, E.; Sharpe, A.H.; Francisco, L.M.; et al. The PTEN pathway in Tregs is a critical driver of the suppressive tumor microenvironment. Sci. Adv. 2015, 1, e1500845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piro, G.; Carbone, C.; Carbognin, L.; Pilotto, S.; Ciccarese, C.; Iacovelli, R.; Milella, M.; Bria, E.; Tortora, G. Revising PTEN in the era of immunotherapy: New perspectives for an old story. Cancers 2019, 11, 1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidotto, T.; Melo, C.M.; Castelli, E.; Koti, M.; Dos Reis, R.B.; Squire, J.A. Emerging role of PTEN loss in evasion of the immune response to tumours. Br. J. Cancer. 2020, 122, 1732–1743. [Google Scholar] [CrossRef]
- Conciatori, F.; Bazzichetto, C.; Falcone, I.; Ciuffreda, L.; Ferretti, G.; Vari, S.; Ferraresi, V.; Cognetti, F.; Milella, M. PTEN function at the interface between cancer and tumor microenvironment: Implications for response to immunotherapy. Int. J. Mol. Sci. 2020, 21, 5337. [Google Scholar] [CrossRef]
- Arico, S.; Petiot, A.; Bauvy, C.; Dubbelhuis, P.F.; Meijer, A.J.; Codogno, P.; Ogier-Denis, E. The tumor suppressor PTEN positively regulates macroautophagy by inhibiting the phosphatidylinositol 3-kinase/protein kinase B pathway. J. Biol. Chem. 2001, 276, 35243–35246. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.X.; Wang, Y.; Ding, J.; Jiang, A.; Wang, J.; Yu, M.; Blake, S.; Liu, S.; Bieberich, C.J.; Farokhzad, O.C.; et al. Reactivation of the tumor suppressor PTEN by mRNA nanoparticles enhances antitumor immunity in preclinical models. Sci. Transl. Med. 2021, 13, eaba9772. [Google Scholar] [CrossRef]
- Qu, F.; Geng, R.; Liu, Y.; Zhu, J. Advanced nanocarrier- and microneedle-based transdermal drug delivery strategies for skin diseases treatment. Theranostics 2022, 12, 3372–3406. [Google Scholar] [CrossRef]
- Alimardani, V.; Abolmaali, S.S.; Tamaddon, A.M.; Ashfaq, M. Recent advances on microneedle arrays-mediated technology in cancer diagnosis and therapy. Drug Deliv. Transl. Res. 2021, 11, 788–816. [Google Scholar] [CrossRef]
- Lee, S.J.; Lee, H.S.; Hwang, Y.H.; Kim, J.J.; Kang, K.Y.; Kim, S.J.; Kim, H.K.; Kim, J.D.; Jeong, D.H.; Paik, M.J.; et al. Enhanced anti-tumor immunotherapy by dissolving microneedle patch loaded ovalbumin. PLoS ONE 2019, 14, e0220382. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Hu, D.; Xu, H.; Patra, H.K.; Liu, X.; Zhou, Z.; Tang, J.; Slater, N.; Shen, Y. Progress and perspective of microneedle system for anti-cancer drug delivery. Biomaterials 2021, 264, 120410. [Google Scholar] [CrossRef]
- Kulkarni, D.; Damiri, F.; Rojekar, S.; Zehravi, M.; Ramproshad, S.; Dhoke, D.; Musale, S.; Mulani, A.A.; Modak, P.; Paradhi, R.; et al. Recent advancements in microneedle technology for multifaceted biomedical applications. Pharmaceutics 2022, 14, 1097. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Ye, Y.; Hochu, G.M.; Sadeghifar, H.; Gu, Z. Enhanced cancer immunotherapy by microneedle patch-assisted delivery of anti-PD1 antibody. Nano Lett. 2016, 16, 2334–2340. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Wang, J.; Hu, Q.; Hochu, G.M.; Xin, H.; Wang, C.; Gu, Z. Synergistic transcutaneous immunotherapy enhances antitumor immune responses through delivery of checkpoint inhibitors. ACS Nano 2016, 10, 8956–8963. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Lu, C.; Qin, W.; Chen, M.; Quan, G.; Liu, H.; Wang, L.; Bai, X.; Pan, X.; Wu, C. Construction of a core-shell microneedle system to achieve targeted co-delivery of checkpoint inhibitors for melanoma immunotherapy. Acta Biomater. 2020, 104, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Kanugo, A. Recent advances of nanotechnology in the treatment of skin cancer. Curr. Pharm. Biotechnol. 2022. [Google Scholar] [CrossRef]
- Lan, X.; Zhu, W.; Huang, X.; Yu, Y.; Xiao, H.; Jin, L.; Pu, J.J.; Xie, X.; She, J.; Lui, V.W.Y.; et al. Microneedles loaded with anti-PD-1-cisplatin nanoparticles for synergistic cancer immuno-chemotherapy. Nanoscale 2020, 12, 18885–18898. [Google Scholar] [CrossRef]
- Cifaldi, L.; Di Santo, J.; Olive, D. Editorial: Molecular strategies aimed to boost NK cell-based immunotherapy of cancer. Front. Immunol. 2020, 11, 1132. [Google Scholar] [CrossRef]
- Tarannum, M.; Romee, R.; Shapiro, R.M. Innovative strategies to improve the clinical application of NK cell-based immunotherapy. Front. Immunol. 2022, 13, 859177. [Google Scholar] [CrossRef]
- Guillerey, C.; Huntington, N.D.; Smyth, M.J. Targeting natural killer cells in cancer immunotherapy. Nat. Immunol. 2016, 17, 1025–1036. [Google Scholar] [CrossRef] [PubMed]
- Mikelez-Alonso, I.; Magadán, S.; González-Fernández, Á.; Borrego, F. Natural killer (NK) cell-based immunotherapies and the many faces of NK cell memory: A look into how nanoparticles enhance NK cell activity. Adv. Drug Deliv. Rev. 2021, 176, 113860. [Google Scholar] [CrossRef] [PubMed]
- Otegbeye, F.; Ojo, E.; Moreton, S.; Mackowski, N.; Lee, D.A.; de Lima, M.; Wald, D.N. Inhibiting TGF-beta signaling preserves the function of highly activated, in vitro expanded natural killer cells in AML and colon cancer models. PLoS ONE 2018, 13, e0191358. [Google Scholar] [CrossRef] [Green Version]
- Regis, S.; Dondero, A.; Caliendo, F.; Bottino, C.; Castriconi, R. NK cell function regulation by TGF-β-induced epigenetic mechanisms. Front. Immunol. 2020, 11, 311. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.H.; Liao, Y.J.; Chiou, T.J.; Huang, H.T.; Lin, Y.H.; Twu, Y.C. TGF-β regulated leukemia cell susceptibility against NK targeting through the down-regulation of the CD48 expression. Immunobiology 2019, 224, 649–658. [Google Scholar] [CrossRef]
- Shi, L.; Lin, H.; Li, G.; Sun, Y.; Shen, J.; Xu, J.; Lin, C.; Yeh, S.; Cai, X.; Chang, C. Cisplatin enhances NK cells immunotherapy efficacy to suppress HCC progression via altering the androgen receptor (AR)-ULBP2 signals. Cancer Lett. 2016, 373, 45–56. [Google Scholar] [CrossRef] [Green Version]
- Yoo, J.Y.; Jaime-Ramirez, A.C.; Bolyard, C.; Dai, H.; Nallanagulagari, T.; Wojton, J.; Hurwitz, B.S.; Relation, T.; Lee, T.J.; Lotze, M.T.; et al. Bortezomib treatment sensitizes oncolytic HSV-1-treated tumors to NK cell immunotherapy. Clin. Cancer Res. 2016, 22, 5265–5276. [Google Scholar] [CrossRef] [Green Version]
- Padrón, L.J.; Maurer, D.M.; O’Hara, M.H.; O’Reilly, E.M.; Wolff, R.A.; Wainberg, Z.A.; Ko, A.H.; Fisher, G.; Rahma, O.; Lyman, J.P.; et al. Sotigalimab and/or nivolumab with chemotherapy in first-line metastatic pancreatic cancer: Clinical and immunologic analyses from the randomized phase 2 PRINCE trial. Nat. Med. 2022, 28, 1167–1177. [Google Scholar] [CrossRef] [PubMed]
- Avery, J.C.; Hoffmann, P.R. Selenium, selenoproteins, and immunity. Nutrients 2018, 10, 1203. [Google Scholar] [CrossRef] [Green Version]
- Lai, H.; Zeng, D.; Liu, C.; Zhang, Q.; Wang, X.; Chen, T. Selenium-containing ruthenium complex synergizes with natural killer cells to enhance immunotherapy against prostate cancer via activating TRAIL/FasL signaling. Biomaterials 2019, 219, 119377. [Google Scholar] [CrossRef]
- Liu, C.; Lai, H.; Chen, T. Boosting natural killer cell-based cancer immunotherapy with selenocystine/transforming growth factor-beta inhibitor-encapsulated nanoemulsion. ACS Nano 2020, 14, 11067–11082. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Petit, P.F.; Van den Eynde, B.J. Apoptosis of tumor-infiltrating T lymphocytes: A new immune checkpoint mechanism. Cancer Immunol. Immunother. 2019, 68, 835–847. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, Y.; Mittra, A.; Naqash, A.R.; Takebe, N. A review of mechanisms of resistance to immune checkpoint inhibitors and potential strategies for therapy. Cancer Drug Resist. 2020, 3, 252–275. [Google Scholar] [CrossRef] [PubMed]
- Haibe, Y.; El Husseini, Z.; El Sayed, R.; Shamseddine, A. Resisting resistance to immune checkpoint therapy: A systematic review. Int. J. Mol. Sci. 2020, 21, 6176. [Google Scholar] [CrossRef]
- Patel, S.A.; Minn, A.J. Combination cancer therapy with immune checkpoint blockade: Mechanisms and strategies. Immunity 2018, 48, 417–433. [Google Scholar] [CrossRef] [Green Version]
- Larkin, J.; Hodi, F.S.; Wolchok, J.D. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Eng. J. Med. 2015, 373, 1270–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.; Stephan, M.T.; Gai, S.A.; Abraham, W.; Shearer, A.; Irvine, D.J. In vivo targeting of adoptively transferred T-cells with antibody- and cytokine-conjugated liposomes. J. Control Release 2013, 172, 426–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, D.; Park, C.G.; Hartl, C.A.; Subedi, N.; Cartwright, A.N.; Puerto, R.B.; Zheng, Y.; Maiarana, J.; Freeman, G.J.; Wucherpfennig, K.W.; et al. T cell-targeting nanoparticles focus delivery of immunotherapy to improve antitumor immunity. Nat. Commun. 2017, 8, 1747. [Google Scholar] [CrossRef]
- Manspeaker, M.P.; Thomas, S.N. Lymphatic immunomodulation using engineered drug delivery systems for cancer immunotherapy. Adv. Drug Deliv. Rev. 2020, 160, 19–35. [Google Scholar] [CrossRef]
- Francis, D.M.; Manspeaker, M.P.; Archer, P.A.; Sestito, L.F.; Heiler, A.J.; Schudel, A.; Thomas, S.N. Drug-eluting immune checkpoint blockade antibody-nanoparticle conjugate enhances locoregional and systemic combination cancer immunotherapy through T lymphocyte targeting. Biomaterials 2021, 279, 121184. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wang, W.; Wu, F.; Zheng, T.; Ashley, J.; Mohammadniaei, M.; Zhang, Q.; Wang, M.; Li, L.; Shen, J.; et al. Biodegradable poly(γ-glutamic acid)@glucose oxidase@carbon dot nanoparticles for simultaneous multimodal imaging and synergetic cancer therapy. Biomaterials 2020, 252, 120106. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Xu, Y.; Ji, W.; Zhou, S.; Li, L.; Qiu, L.; Qian, Z.; Wang, X.; Zhang, H. Biomimetic black phosphorus quantum dots-based photothermal therapy combined with anti-PD-L1 treatment inhibits recurrence and metastasis in triple-negative breast cancer. J. Nanobiotechnology 2021, 19, 181. [Google Scholar] [CrossRef]
- Zhao, P.; Xu, Y.; Ji, W.; Li, L.; Qiu, L.; Zhou, S.; Qian, Z.; Zhang, H. Hybrid membrane nanovaccines combined with immune checkpoint blockade to enhance cancer immunotherapy. Int. J. Nanomed. 2022, 17, 73–89. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Xu, L.; Xu, J.; Zhang, R.; Song, G.; Chao, Y.; Feng, L.; Han, F.; Dong, Z.; Li, B.; et al. Smart nanoreactors for pH-responsive tumor homing, mitochondria-targeting, and enhanced photodynamic-immunotherapy of cancer. Nano Lett. 2018, 18, 2475–2484. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Xu, J.; Liang, C.; Chao, Y.; Jin, Q.; Wang, C.; Chen, M.; Liu, Z. Self-supplied tumor oxygenation through separated liposomal delivery of H2O2 and catalase for enhanced radio-immunotherapy of cancer. Nano Lett. 2018, 18, 6360–6368. [Google Scholar] [CrossRef]
- Chung, C.K.; Fransen, M.F.; van der Maaden, K.; Campos, Y.; García-Couce, J.; Kralisch, D.; Chan, A.; Ossendorp, F.; Cruz, L.J. Thermosensitive hydrogels as sustained drug delivery system for CTLA-4 checkpoint blocking antibodies. J. Control. Release 2020, 323, 1–11. [Google Scholar] [CrossRef]
- Ruan, H.; Hu, Q.; Wen, D.; Chen, Q.; Chen, G.; Lu, Y.; Wang, J.; Cheng, H.; Lu, W.; Gu, Z. A dual-bioresponsive drug-delivery depot for combination of epigenetic modulation and immune checkpoint blockade. Adv. Mater. 2019, 31, e1806957. [Google Scholar] [CrossRef]
- Wang, C.; Wang, J.; Zhang, X.; Yu, S.; Wen, D.; Hu, Q.; Ye, Y.; Bomba, H.; Hu, X.; Liu, Z.; et al. In situ formed reactive oxygen species-responsive scaffold with gemcitabine and checkpoint inhibitor for combination therapy. Sci. Transl. Med. 2018, 10, eaan3682. [Google Scholar] [CrossRef] [Green Version]
- Longmire, M.; Choyke, P.L.; Kobayashi, H. Clearance properties of nano-sized particles and molecules as imaging agents: Considerations and caveats. Nanomedicine 2008, 3, 703–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, K.C.; Wang, Y.; Luehmann, H.P.; Cai, X.; Xing, W.; Pang, B.; Zhao, Y.; Cutler, C.S.; Wang, L.V.; Liu, Y.; et al. Radioactive 198Au-doped nanostructures with different shapes for in vivo analyses of their biodistribution, tumor uptake, and intratumoral distribution. ACS Nano 2014, 8, 4385–4394. [Google Scholar] [CrossRef]
- Decuzzi, P.; Pasqualini, R.; Arap, W.; Ferrari, M. Intravascular delivery of particulate systems: Does geometry really matter? Pharm. Res. 2009, 26, 235–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, K.; Li, Y.; Luo, J.; Lee, J.S.; Xiao, W.; Gonik, A.M.; Agarwal, R.G.; Lam, K.S. The effect of surface charge on in vivo biodistribution of PEG-oligocholic acid based micellar nanoparticles. Biomaterials 2011, 32, 3435–3446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanco, E.; Shen, H.; Ferrari, M. Principles of nanoparticle design for overcoming biological barriers to drug delivery. Nat. Biotechnol. 2015, 33, 941–951. [Google Scholar] [CrossRef] [PubMed]
- Nehoff, H.; Parayath, N.N.; Domanovitch, L.; Taurin, S.; Greish, K. Nanomedicine for drug targeting: Strategies beyond the enhanced permeability and retention effect. Int. J. Nanomed. 2014, 9, 2539–2555. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, P.V.; Hervé-Aubert, K.; Chourpa, I.; Allard-Vannier, E. Active targeting strategy in nanomedicines using anti-EGFR ligands-A promising approach for cancer therapy and diagnosis. Int. J. Pharm. 2021, 609, 121134. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Zhou, Z.; Qiu, N.; Shen, Y. Rational design of cancer nanomedicine: Nanoproperty integration and synchronization. Adv. Mater. 2017, 29, 1606628. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.; Park, C.; Yi, G.; Lee, D.; Koo, H. Active targeting strategies using biological ligands for nanoparticle drug delivery systems. Cancers 2019, 11, 640. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Mechanisms in drug resistance of chemotherapy. Reprinted with permission from Ref. [45]. 2021, NIH.
Figure 1.
Mechanisms in drug resistance of chemotherapy. Reprinted with permission from Ref. [45]. 2021, NIH.

Figure 2.
DOX-PLGA/CPT/PD for overcoming cancer drug resistance. Reprinted with permission from Ref. [70]. 2019, NIH. (a) Schematic diagram of the mechanism of DOX-PLGA/CPT/PD surmounting cancer drug resistance. (b) Charge reversal of PLGA/CPT/PD. (c) Lysosome escape of PLGA/CPT/PD, scale bar = 20 μm. (d) Mitochondrial targeting capability of DOX-PLGA/CPT/PD, scale bar = 20 μm. (e) Apoptosis mechanism analysis. (f) Tumor inhibition of DOX-PLGA/CPT/PD after treatment for 18 days.
Figure 2.
DOX-PLGA/CPT/PD for overcoming cancer drug resistance. Reprinted with permission from Ref. [70]. 2019, NIH. (a) Schematic diagram of the mechanism of DOX-PLGA/CPT/PD surmounting cancer drug resistance. (b) Charge reversal of PLGA/CPT/PD. (c) Lysosome escape of PLGA/CPT/PD, scale bar = 20 μm. (d) Mitochondrial targeting capability of DOX-PLGA/CPT/PD, scale bar = 20 μm. (e) Apoptosis mechanism analysis. (f) Tumor inhibition of DOX-PLGA/CPT/PD after treatment for 18 days.

Figure 4.
[email protected] for synergistic therapy against drug-resistant cancer. Reprinted with permission from Ref. [109]. 2019, Wiley. (a) Schematic diagram of the mechanism of [email protected] surmounting cancer drug resistance. (b) Dox.HCl release from [email protected]. (c) Cellular uptake of [email protected]. (d) Gene silencing of Pgp mRNA level in MDR MCF-7 cells. ** p < 0.01. (e) In vitro cytotoxicity against MDR MCF-7 cells. ** p < 0.01. (f) In vivo antitumor effect of [email protected]. ** p < 0.01, *** p < 0.001.
Figure 4.
[email protected] for synergistic therapy against drug-resistant cancer. Reprinted with permission from Ref. [109]. 2019, Wiley. (a) Schematic diagram of the mechanism of [email protected] surmounting cancer drug resistance. (b) Dox.HCl release from [email protected]. (c) Cellular uptake of [email protected]. (d) Gene silencing of Pgp mRNA level in MDR MCF-7 cells. ** p < 0.01. (e) In vitro cytotoxicity against MDR MCF-7 cells. ** p < 0.01. (f) In vivo antitumor effect of [email protected]. ** p < 0.01, *** p < 0.001.

Figure 5.
Mechanisms in drug resistance of targeted anticancer agents. Reprinted with permission from Ref. [161]. 2021, Springer.
Figure 5.
Mechanisms in drug resistance of targeted anticancer agents. Reprinted with permission from Ref. [161]. 2021, Springer.

Figure 6.
CP@NP-cRGD for overcoming cancer drug resistance. Reprinted with permission from Ref. [188]. 2020, Wiley. (a) Diagram of CP@NP-cRGD intracellular mechanisms of overcoming drug resistance. (b) In vitro release curve of CP@NP-cRGD. (c) Cellular uptake of RB-loaded CP@NP-cRGD in AZD9291-resistant cells. ** p < 0.01, *** p < 0.001. (d) The lysosomal escape of CP@NP-cRGD. (e) Antitumor molecular mechanisms of CP@NP-cRGD. (f) CP@NP-cRGD inhibited autophagy of H1975/AR cells. *** p < 0.001. (g) In vivo antitumor efficiency of CP@NP-cRGD. * p < 0.05, ** p < 0.01, *** p < 0.001.
Figure 6.
CP@NP-cRGD for overcoming cancer drug resistance. Reprinted with permission from Ref. [188]. 2020, Wiley. (a) Diagram of CP@NP-cRGD intracellular mechanisms of overcoming drug resistance. (b) In vitro release curve of CP@NP-cRGD. (c) Cellular uptake of RB-loaded CP@NP-cRGD in AZD9291-resistant cells. ** p < 0.01, *** p < 0.001. (d) The lysosomal escape of CP@NP-cRGD. (e) Antitumor molecular mechanisms of CP@NP-cRGD. (f) CP@NP-cRGD inhibited autophagy of H1975/AR cells. *** p < 0.001. (g) In vivo antitumor efficiency of CP@NP-cRGD. * p < 0.05, ** p < 0.01, *** p < 0.001.

Figure 7.
T12/P-Lipo for overcoming cancer drug resistance and brain metastases. Reprinted with permission from Ref. [215]. 2020, NIH. (a) The targeting receptors in BCECs. (b) Uptake of T12/P-Lipo by H1975 cells. (c) Fluorescence images of T12/P-Lipo in H1975 cells. (d) Macrophage repolarization from M2 to M1. (e) The level of NOX3/MsrA/GPX4/Bcl-2 in H1975 cells. (f) The level of phosphorylated EGFR/p-Akt/p-Erk. (g) The level of cleaved caspase 3. (h) The survival curves. (i) Tumor regression after treatment with T12/P-Lipo. * p < 0.05.
Figure 7.
T12/P-Lipo for overcoming cancer drug resistance and brain metastases. Reprinted with permission from Ref. [215]. 2020, NIH. (a) The targeting receptors in BCECs. (b) Uptake of T12/P-Lipo by H1975 cells. (c) Fluorescence images of T12/P-Lipo in H1975 cells. (d) Macrophage repolarization from M2 to M1. (e) The level of NOX3/MsrA/GPX4/Bcl-2 in H1975 cells. (f) The level of phosphorylated EGFR/p-Akt/p-Erk. (g) The level of cleaved caspase 3. (h) The survival curves. (i) Tumor regression after treatment with T12/P-Lipo. * p < 0.05.

Figure 8.
Schematic diagram of synergistic effect of immunochemotherapy by a microneedle patch containing aPD-1/CDDP@NPs. Reprinted with permission from Ref. [258]. 2020, Royal Society of Chemistry. (a) The mechanism of enhanced immunotherapy induced by aPD-1/CDDP@NP MNs. (b) SEM images of dissolving microneedles. (c) Fluorescence microscopy image of the microneedles. (d) Antitumor efficacy in vivo. *** p < 0.001. (e) The positive rate of CD4+ T cells. * p < 0.05. (f) The positive rate of CD8+ T cells. * p < 0.05. (g) IFN-γ expression in the serum. ** p < 0.01. (h) The percentages of CD4+FOXP3+ Tregs. * p < 0.05.
Figure 8.
Schematic diagram of synergistic effect of immunochemotherapy by a microneedle patch containing aPD-1/CDDP@NPs. Reprinted with permission from Ref. [258]. 2020, Royal Society of Chemistry. (a) The mechanism of enhanced immunotherapy induced by aPD-1/CDDP@NP MNs. (b) SEM images of dissolving microneedles. (c) Fluorescence microscopy image of the microneedles. (d) Antitumor efficacy in vivo. *** p < 0.001. (e) The positive rate of CD4+ T cells. * p < 0.05. (f) The positive rate of CD8+ T cells. * p < 0.05. (g) IFN-γ expression in the serum. ** p < 0.01. (h) The percentages of CD4+FOXP3+ Tregs. * p < 0.05.


{kind=link}
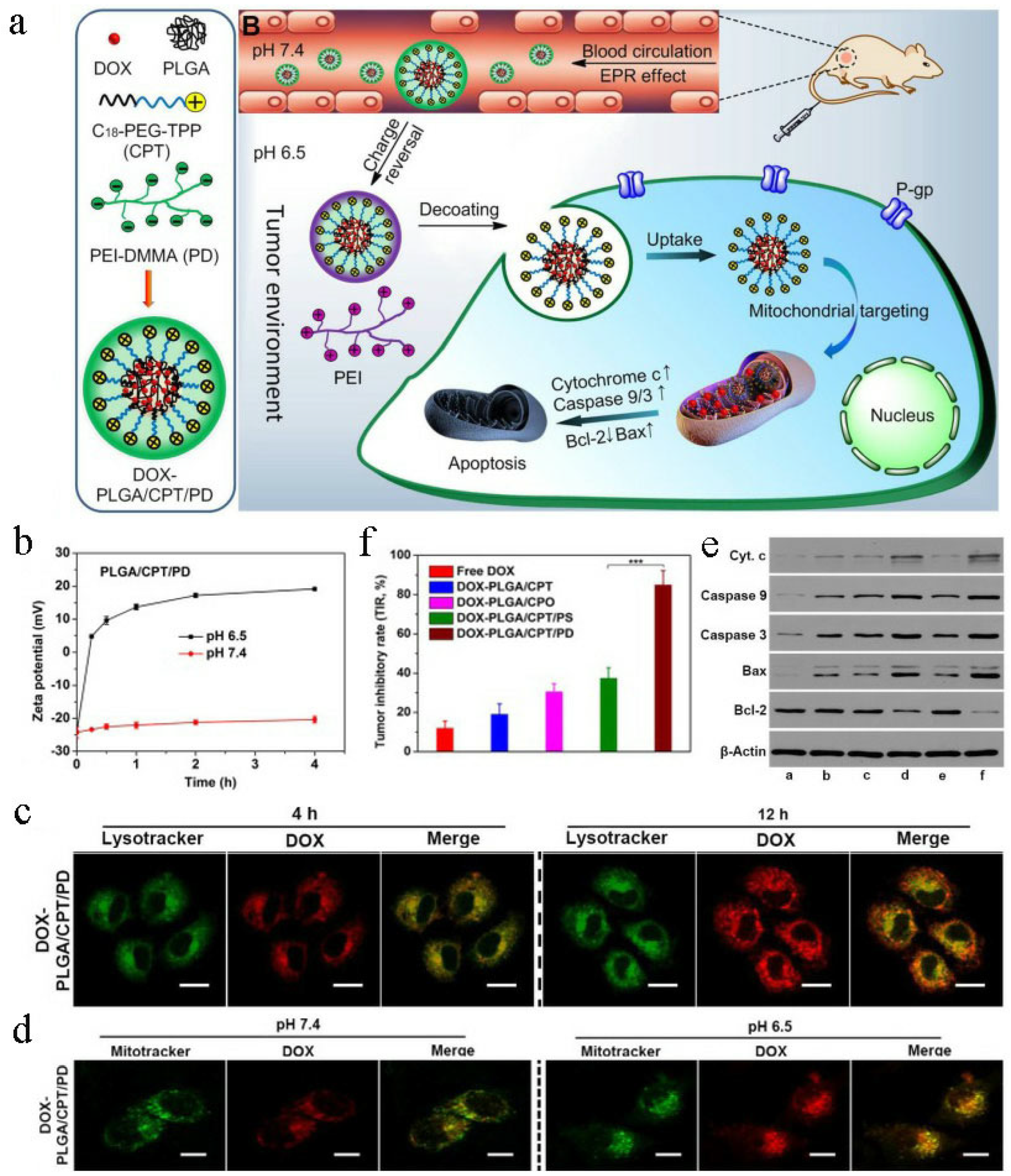{kind=link}
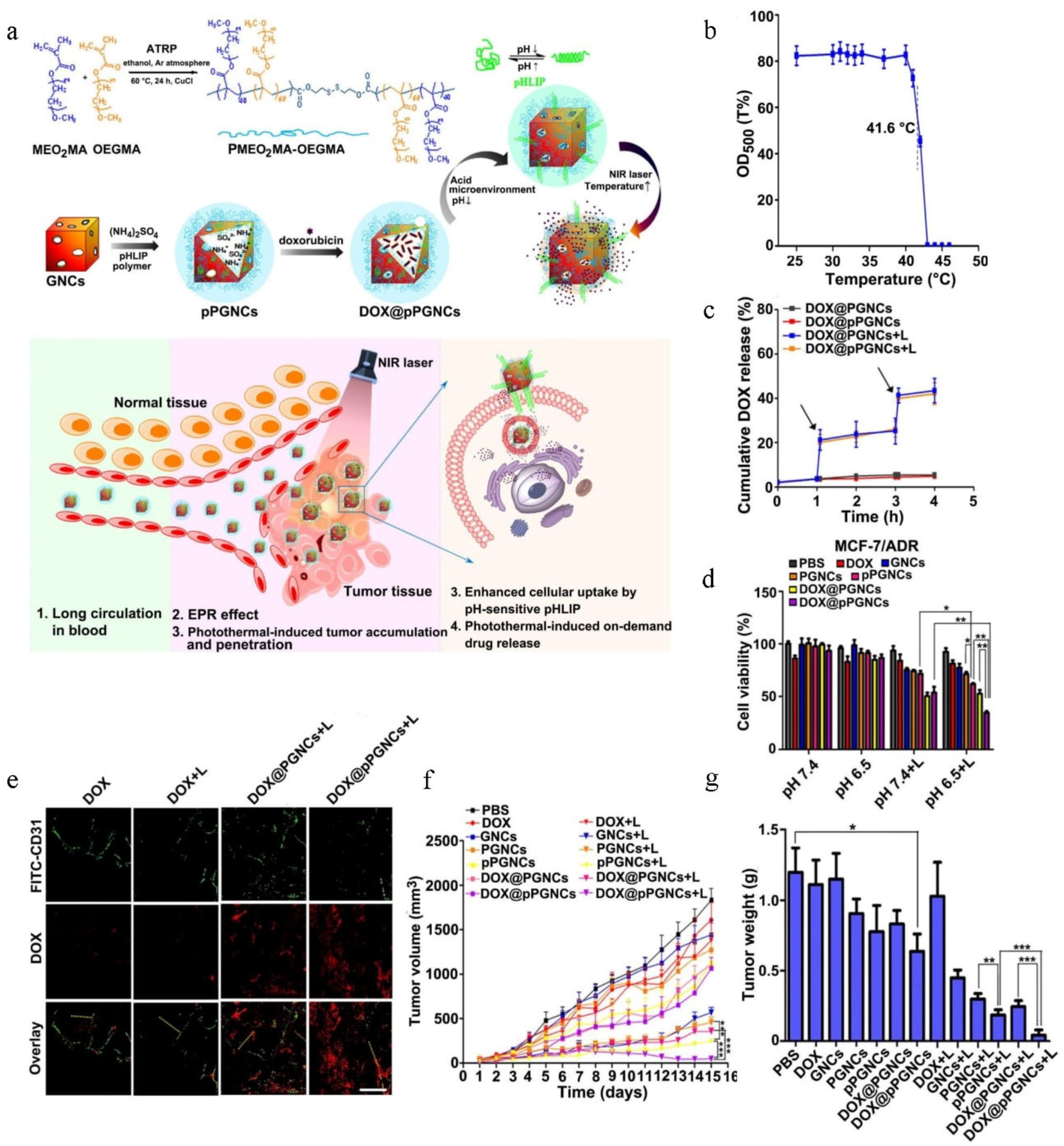{kind=link}
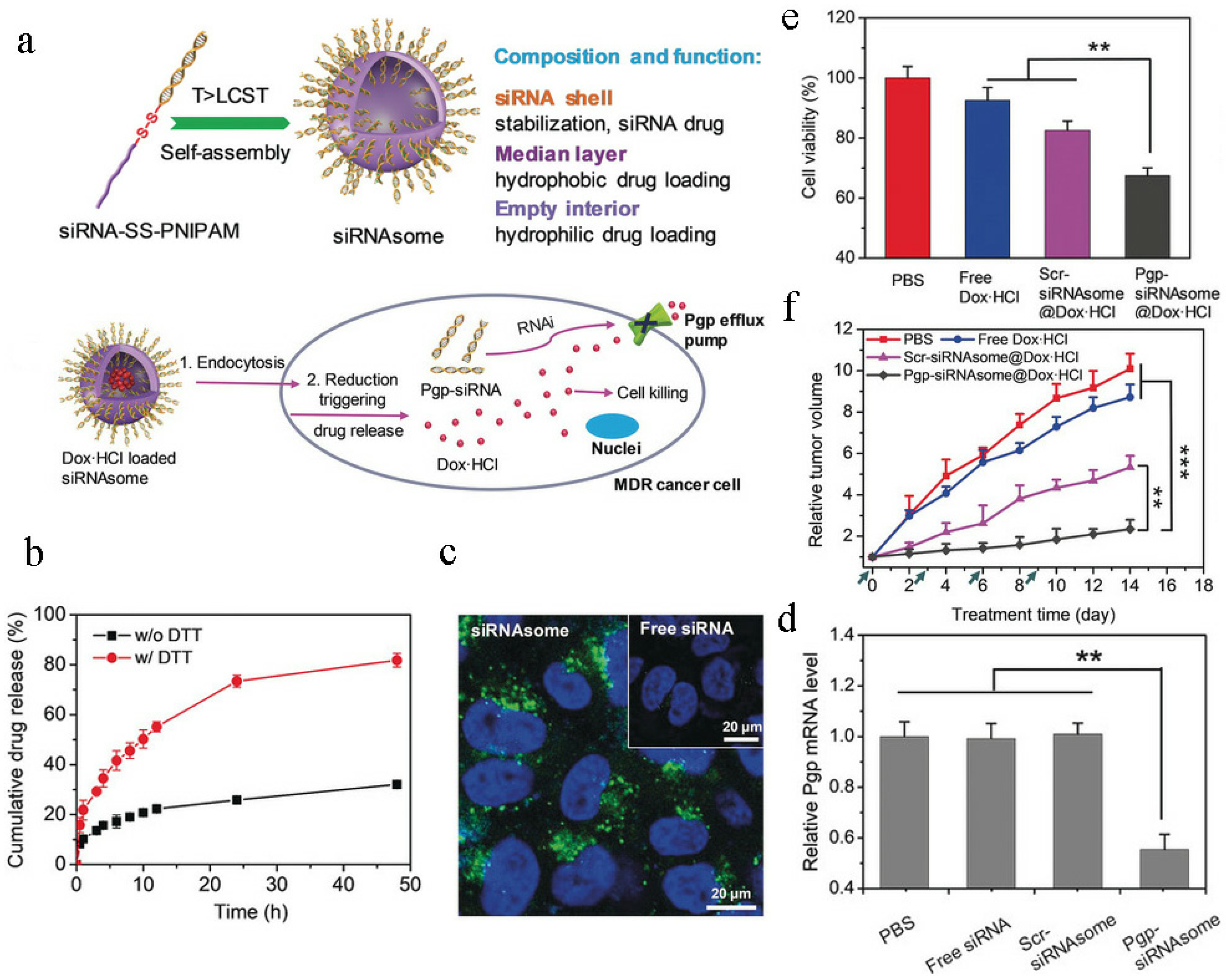{kind=link}
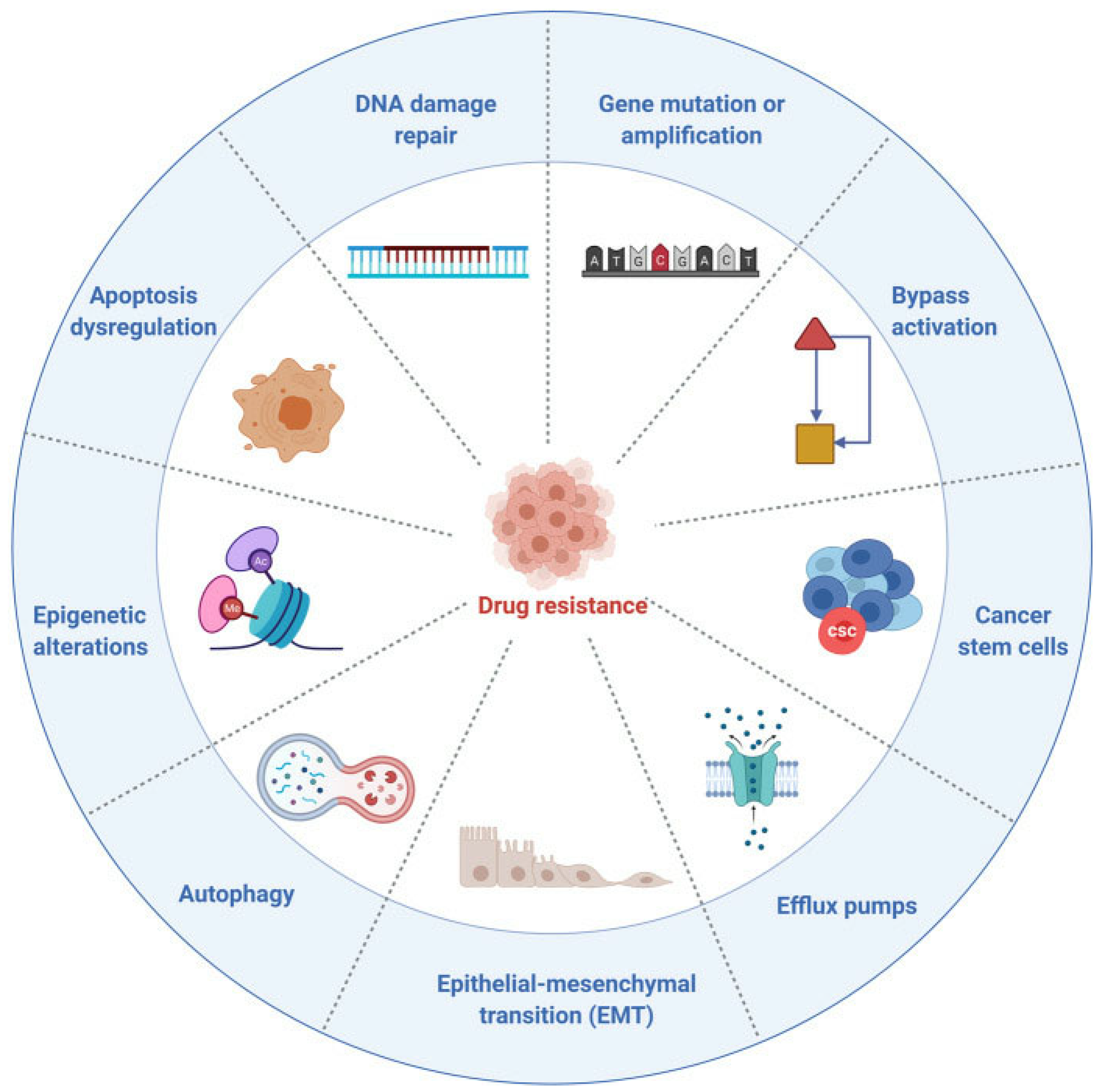{kind=link}
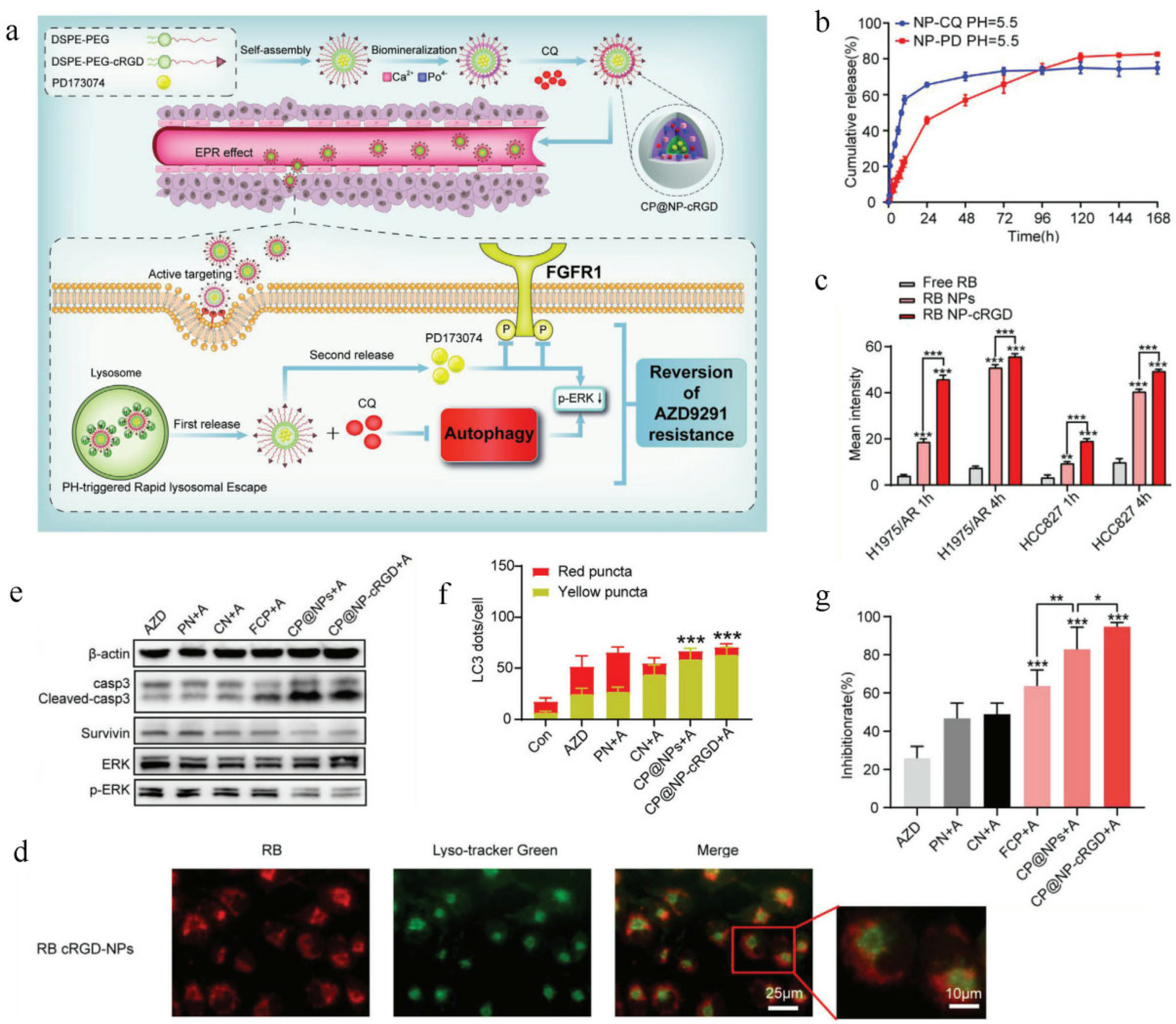{kind=link}
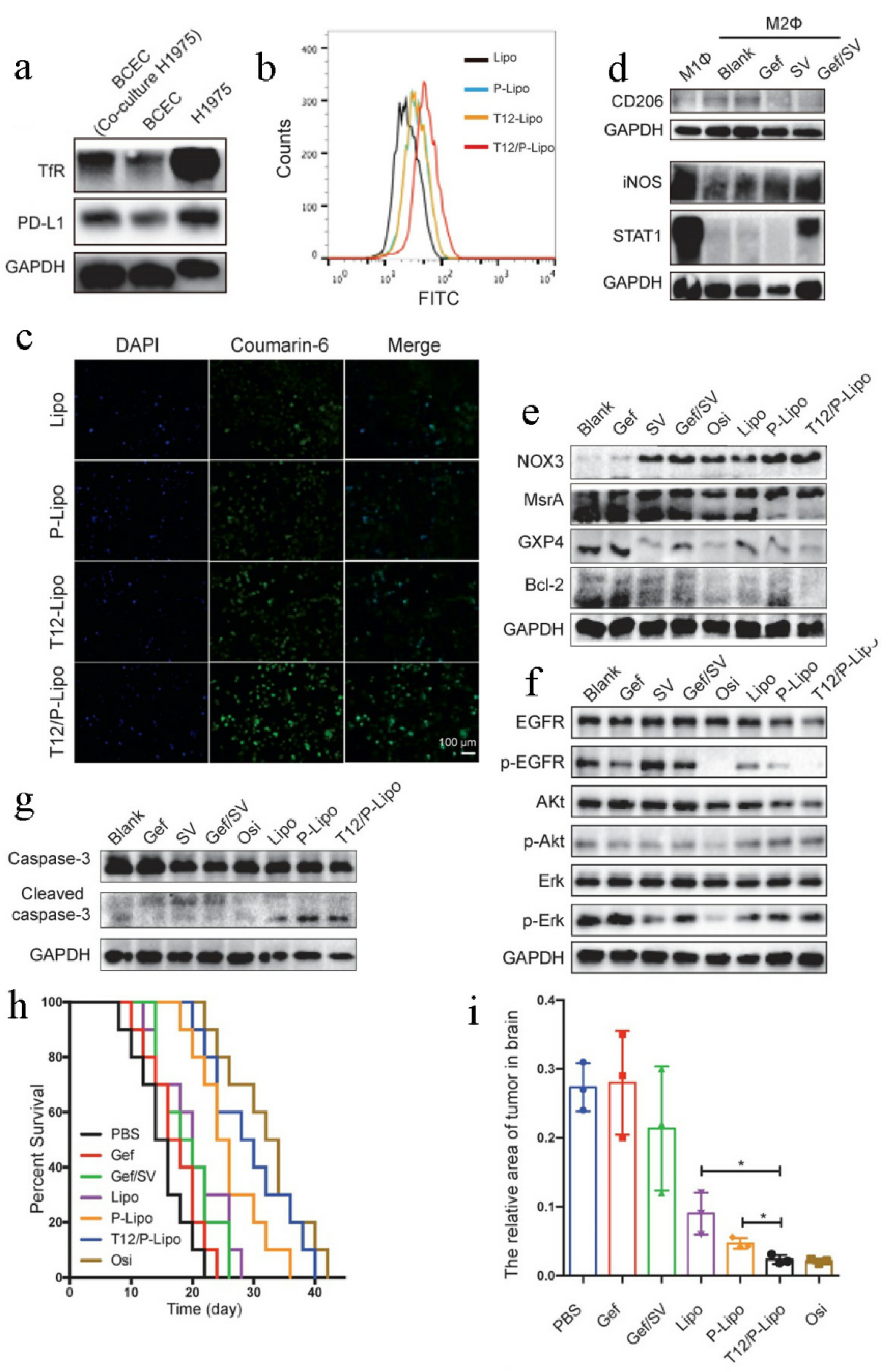{kind=link}
{kind=link}
Table 1.
Examples of the approved nanomedicines.
| Trade Name | Active Ingredient | Nanoformulation | Indications | Approval Date | Clinical Effect | Reference |
|---|---|---|---|---|---|---|
| Doxil® | Doxorubicin | Liposome | Ovarian and breast cancer | 1995 | Fewer and less severe side effects Longer periods of drug circulation in vivo Prolonged interval to progression and progression-free survival time | [32] |
| DaunoXome® | Daunorubicin | Liposome | HIV-related Kaposi’s Sarcoma | 1996 | No obvious cardiotoxicity Longer periods of drug circulation in vivo As effective as the conventional chemotherapy | [33] |
| DepoCyt® | Cytarabine | Liposome | Lymphomatous meningitis | 1999 | Reduced cardiotoxicity Pronounced effectiveness | [34] |
| Eligard® | Leuprolide | Nanosphere | Prostate cancer | 2002 | More sustained testosterone suppression Higher response rates | [35] |
| Lipusu® | Paclitaxel | Liposome | Ovarian cancer and breast cancer | 2003 | Reduced adverse reactions As effective as the paclitaxel | [36] |
| Abraxane® | Paclitaxel | Nanoparticle | Metastatic breast cancer | 2005 | Lower overall toxicity Better anticancer effect | [37] |
| Genexol-PM® | Paclitaxel | Micelle | Breast cancer and Lung cancer | 2007 | Reduced toxicities of paclitaxel Enhanced antitumor efficiency | [38] |
| Marqibo® | Vincristine | Liposome | Acute lymphoid leukemia | 2012 | Reduced neurotoxicity Overall increase in therapeutic index | [39] |
| Onivyde® | Irinotecan | Liposome | Metastatic pancreatic cancer | 2015 | Longer half-life Enhanced anticancer efficiency | [40] |
| Liporaxel® | Paclitaxel | Emulsion | Gastric cancer | 2016 | Reduced neurotoxicity As effective as paclitaxel | [41] |
| Vyxeos® | Daunorubicin and cytarabine | Liposome | Acute myeloid leukemia | 2017 | Prolonged overall survival (OS) and event-free survival (EFS) | [42] |
Table 2.
Recent advances in nanomedicines for overcoming chemotherapeutic resistance.
| Nanoformulation | Name | Particle Size | Payload | Reversal Mechanism of Drug Resistance | Cell Line | Tumor Model | Reference |
|---|---|---|---|---|---|---|---|
| Polymeric micelles | ACP-Dox and Apa micelles | 104 ± 2 nm | DOX and apatinib | Inhibit P-gp activity | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [127] |
| HA-PLGA (PTX and FAK siRNA)-NPs | 232.9 ± 6.9 nm | PTX and FAK siRNA | siRNA-mediated silencing of FAK | HeyA8-MDR and SKOV3-TR cells | Drug-resistant, patient-derived xenograft (PDX) model | [128] | |
| ACP-R837 and PPP-DOX | ~110 nm | R837 and DOX | Synergistic chemo-immunotherapy | 4T1 cells | 4T1 tumor-bearing mice | [129] | |
| NC-DOX | ~122 nm | DOX and IR780 | Combined chemotherapy/PTT/PDT | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [130] | |
| Polymeric nanoparticles | Dox-Cur-NDs | 55.1 ± 3.0 nm | DOX and CUR | Down-regulate the expression of P-gp | A2780 ADR cells | A2780 ADR tumor-bearing mice | [131] |
| [FeFe]TPP/GEM/FCS NPs | 176.0 ± 17.2 nm | Gemcitabine and [FeFe]TPP | Reduce the of function P-gp efflux pump | T24 cells | T24 tumor-bearing mice | [132] | |
| IGU-PLGA-NPs | 199.6 nm | Iguratimod | Facilitate BBB penetration and inhibit GSCs proliferation and stemness | U87 and U251TMZ-R cells | U87 tumor-bearing mice | [133] | |
| Liposomes | rTLM-PEG, PTX liposomes | / | PTX and trichosanthin | Reverse caspase 9 phosphorylation and induce caspase 3-dependent apoptosis | A549/T cells | A549/T tumor-bearing mice | [134] |
| PTX/NO/DMA-L | 146.3 ± 0.82 nm | PTX and DETA NONOate | NO-mediated down-regulation of P-gp | A549/T cells | A549/T tumor-bearing mice | [135] | |
| CBZ liposomes | 108.53 ± 1.5 nm | CBZ | G2/M phase arrest | MCF-7 and MDA-MB-231 cells | Female SD rats | [136] | |
| Lip (Ap-Dox) | 128.6 nm | Ap-Dox complex | Bypass the P-gp-mediated drug efflux | MCF-7/ADR cells | MCF-7/ADR tumor-bearing nude mice | [137] | |
| (DEX and DTX)-Lip | 74.02 ± 0.41 nm | DTX and dexamethasone | Overcome stroma obstacles | Multidrug-resistant KBv cells and 4 T1 cells | Multidrug-resistant KBv and metastatic 4 T1 tumor models | [138] | |
| FPL-DOX/IM | 159 ± 6 nm | DOX and imatinib | Inhibit ABC transporter function | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [139] | |
| PpIX/Dox liposomes | 55.9 ± 20.9 nm | DOX and PpIX | Disrupt the structure of P-gp | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [140] | |
| Nanogels | LNGs-PTX-siRNA | ~100 nm | PTX and MDR1 siRNA | Knockdown MDR1 | DROV cells | DROV tumor-bearing mice | [141] |
| CDDP/DOX-NGs | ~100 nm | CDDP and DOX | Combination chemotherapy | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [142] | |
| HA/Cis/Dox | 45 ± 9.9 nm | DOX | GSH-induced DOX release | A2780cis cells | / | [143] | |
| SiPT75 | 75.5 ± 19.8 nm | TPPS | Elude the drug efflux pumps and retards exocytosis of cells | A549/DDP cells | A549/DDP tumor-bearing mice | [144] | |
| Inorganic nanoparticles | H-MSNs-DOX/siRNA nanoparticles | ~100 nm | P-gp siRNA and DOX | siRNA-mediated silencing of P-gp | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [145] |
| Pt-AuNS | ~85 nm | Pt | GSH depletion and GPX4 inactivation | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [146] | |
| FA-GT-MSNs@TPZ | ~60 nm | TPZ | Synergistic radio-chemo-photothermal therapy | Hypoxic SMMC-7721 cells | SMMC-7721 tumor-bearing mice | [147] | |
| Hybrid nanoparticles | SCA4PNPBTZ | ~150 nm | BTZ and CA4P | Inhibit the overexpression of BCRP/ABCG2 | A549 cells | Human A549 pulmonary adenocarcinoma xenograft model and PDX model of colon cancer | [148] |
| cNPs | 286 ± 79 nm | Afatinib, rapamycin and docetaxel | Synergistic treatment | HER2-positive breast cancer cells, EGFR-positive NSCLC cells and SKBR-3/AR cell lines | HER2-positive breast cancer mouse model | [149] | |
| 4T1-HANG-GNR-DC | 103.1 ± 7.6 nm | CDDP and DOX | Synergistic chemo-photothermal therapy | 4T1 cells | 4T1 tumor-bearing mice | [150] | |
| IR780/DTX-PCEC@RBC | ~150 nm | IR780 and DTX | Combination therapy | MCF-7 cells | MCF-7 tumor-bearing mice | [151] | |
| cNC@PDA-PEG | 170.5 ± 1.4 nm | Paclitaxel/lapatinib | Combination therapy | MCF-7/ADR cells | / | [152] | |
| miR497/TP-HENPs | 125 ± 6 nm | miR497 and triptolide | Synergically suppress mTOR signaling pathway | SKOV3-CDDP cells | SKOV3-CDDP tumor-bearing mice | [153] |
“/”: The original research article did not mention it.
Table 3.
Recent advances in nanomedicines for overcoming resistance to targeted therapy.
| Nanoformulation | Name | Particle Size | Payload | Reversal Mechanism of Drug Resistance | Cell Line | Tumor Model | Reference |
|---|---|---|---|---|---|---|---|
| Polymeric micelles | CP@NP-cRGD | 123.4 ± 0.4 nm | CQ and PD173074 | Dual FGFR1-autophagy blockade | H1975/AR and HCC827/AR cells | H1975/AR tumor-bearing mice | [188] |
| CsA/Gef-NPs | 37.1 ± 13.1 nm | Cyclosporin A and gefitinib | Cyclosporin A-mediated gefitinib sensitization | PC-9-GR cells | PC-9-GR tumor-bearing mice | [216] | |
| Polymeric nanoparticles | ELTN and FDTN@PEG-PLA | ~120 nm | Fedratinib and Erlotinib | Inhibit the JAK2/STAT3 signaling pathway | Erlotinib-resistant H1650 cells | Erlotinib-resistant H1650 xenograft tumor model | [217] |
| CE7Ns | 234.2 ± 8.5 nm | Cy7 and erlotinib | Synergistic erlotinib-targeted therapy and photodynamic therapy | PC-9 and Erlotinib-resistant H1975 cells | PC-9 tumor-bearing mice | [218] | |
| ERL-loaded CMP-HA-NI-PEI-NBA | 755.77 ± 51.11 nm | Erlotinib | Hypoxia-triggered rapid drug release | Drug-resistant hypoxic HeLa cells | / | [196] | |
| Liposomes | T12/P-Lipo | ~153 nm | Simvastatin and gefitinib | TAM targeting and enhanced BBB penetration | EGFRT790M-mutated H1975 cells | EGFRT790M-mutated H1975 brain metastasis model | [215] |
| P-Lipo | 156 nm | Simvastatin and gefitinib | Neovascularization regulation and M2-macrophage repolarization | EGFRT790M-mutated H1975 cells | EGFRT790M-mutated H1975 tumor-bearing mice | [219] | |
| tLGV | ~180 n | Gefitinib and vorinostat | TAM reprogramming | EGFRT790M-mutated H1975 cells | EGFRT790M-positive H1975 tumor model | [220] | |
| Hybrid nanoparticles | ACLEP | 184.8 ± 5.87 nm | Erlotinib and PFOB | Reverse hypoxia-induced drug resistance | A549 and Erlotinib-resistant H1975 cells | A549 tumor-bearing mice | [221] |
“/”: The original research article did not mention it.
Table 4.
Recent advances in nanomedicines for overcoming resistance to immunotherapy.
| Nanoformulation | Name | Particle Size | Payload | Reversal Mechanism of Drug Resistance | Cell Line | Tumor Model | Reference |
|---|---|---|---|---|---|---|---|
| Hybrid nanoparticles | mPTEN@NPs | 111.8 ± 15.3 nm | PTEN mRNA | Improve the sensitivity of ICB therapy | B16F10 cells | B16F10 melanoma tumor-bearing mice | [248] |
| PGA@GOx@Mn, Cu-CDs | ~80 nm | Gox and Mn, Cu-CDs | Combined action of starving therapy/PDT/PTT and checkpoint-blockade immunotherapy | 4T1 cells | 4T1 tumor-bearing mice | [281] | |
| BBPQDs | 30 nm | BPQDs | Reprogram the immunosuppressive TME | 4T1 cells | 4T1 tumor-bearing mice | [282] | |
| R837@HM-NPs | 71 ± 4.1 nm | R837 | Reprogram the immunosuppressive TME | 4T1 cells | 4T1 tumor-bearing mice | [283] | |
| CAT@S/Ce6-CTPP/DPEG | ~100 nm | Catalase and Ce6 | Combined action of PDT and immunotherapy | 4T1 cells | 4T1 tumor-bearing mice | [284] | |
| Liposomes | H2O2@Liposome and CAT@Liposome | ~140 nm | H2O2 and Catalase | Radio-immunotherapy | 4T1 cells | 4T1 tumor-bearing mice | [285] |
| Nanoemulsion | SSB NMs | ~130 nm | SeC and TGF-β inhibitor | Improve the sensitivity of cell-based immunotherapy | MDA-MB-231 cells | MDA-MB-231 tumor-bearing mice | [271] |
| Polymeric nanoparticles | ANCs | ~30 nm | ICB mAb and small-molecule immunomodulators | T lymphocyte targeting and combination therapy | B16F10 and 4T1 cells | B16F10 and 4T1 tumor-bearing mice | [280] |
| Nanogels | P407 hydrogel | ~28 nm | Anti-CTLA-4 antibodies | Sustained antibody release | D1DCs and MC-38 cells | CT26 tumor-bearing mice | [286] |
| Zeb-aPD1-NPs-Gel | ~100 nm | Zebularine and anti-PD1 antibody | Controlled drug release and reversal of immunosuppressive TME | B16F10 cells | B16F10 melanoma-bearing mice | [287] | |
| aPDL1-GEM@Gel | / | Gemcitabine and PD-L1 blocking antibody | Combination therapy | B16F10 and 4T1 cells | B16F10 and 4T1 tumor-bearing mice | [288] |
“/”: The original research article did not mention it.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hu, T.; Gong, H.; Xu, J.; Huang, Y.; Wu, F.; He, Z. Nanomedicines for Overcoming Cancer Drug Resistance. Pharmaceutics 2022, 14, 1606. https://doi.org/10.3390/pharmaceutics14081606
AMA Style
Hu T, Gong H, Xu J, Huang Y, Wu F, He Z. Nanomedicines for Overcoming Cancer Drug Resistance. Pharmaceutics. 2022; 14(8):1606. https://doi.org/10.3390/pharmaceutics14081606
Chicago/Turabian StyleHu, Tingting, Hanlin Gong, Jiayue Xu, Yuan Huang, Fengbo Wu, and Zhiyao He. 2022. "Nanomedicines for Overcoming Cancer Drug Resistance" Pharmaceutics 14, no. 8: 1606. https://doi.org/10.3390/pharmaceutics14081606
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.