
Cultural Adaptation, Validation and Evaluation of the Psychometric Properties of an Obstetric Violence Scale in the Spanish Context

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Phase 1
2.1.1. Content Validity
2.1.2. Face Validity
2.2. Phase 2
2.2.1. Design
2.2.2. Study Population
2.2.3. Sampling and Sample Size
2.2.4. Data Collection Tool and Variables of the Study
2.2.5. Data Collection
2.2.6. Data Analysis and Interpretation
- -
- Descriptive analysis of the sample and the items: A descriptive analysis of the studied variables and the involved items was conducted. Qualitative variables were expressed in percentages and frequencies; quantitative variables were expressed in measures of central tendency (mean) and dispersion (standard deviation; minimum–maximum values). Symmetry and kurtosis were calculated for each item on the scale;
- -
- Construct validity by factor analysis: A CFA was carried out based on the unidimensional model proposed by Cárdenas and Salinero [40]. The suitability of data for a FA was assessed with the Kaiser–Meyer–Olkin index (KMO) and Bartlett’s statistic. KMO values higher than 0.75 were considered adequate and p values ≤ 0.05 were considered statistically significant for Bartlett’s statistic [44].
- -
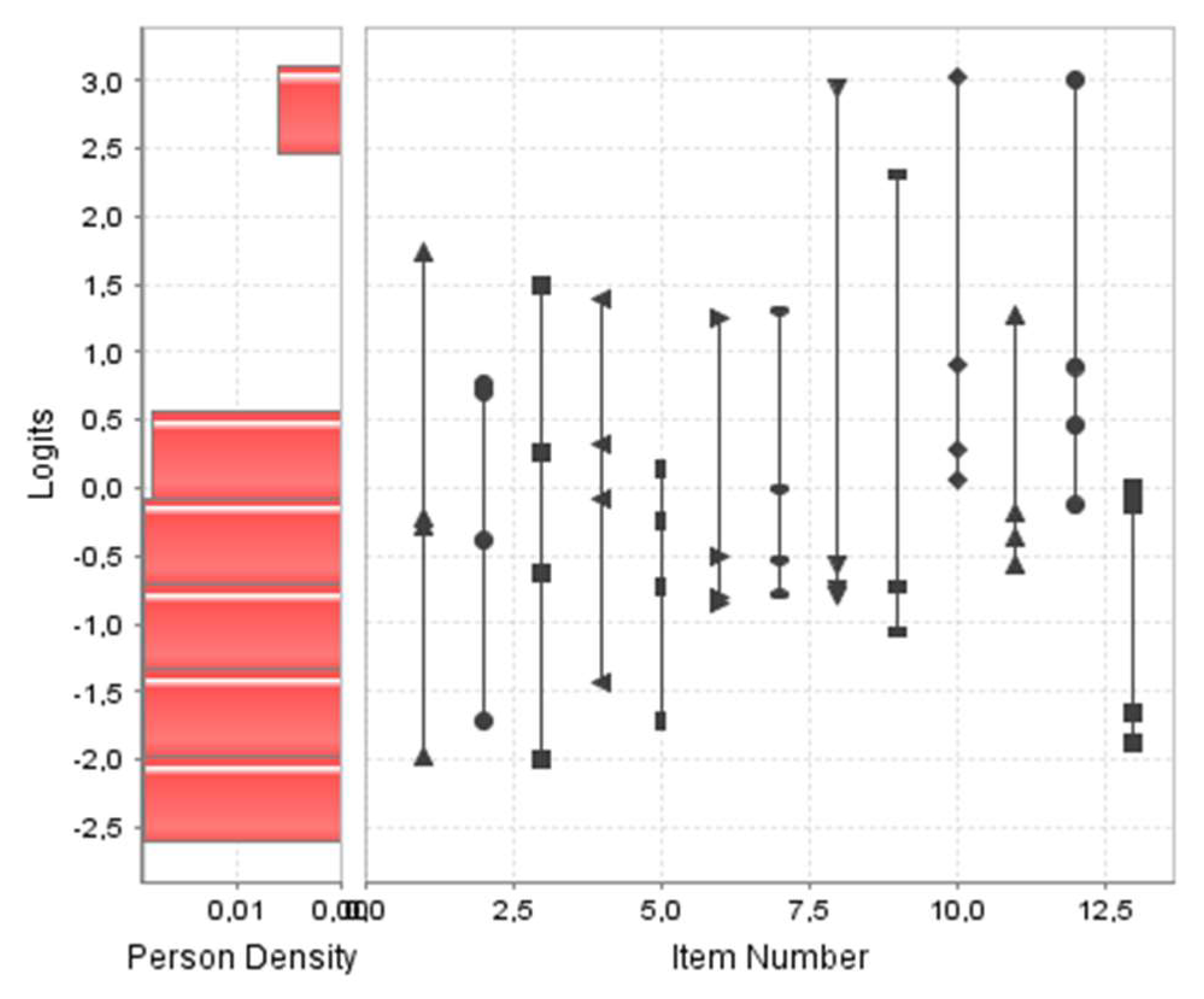
- Construct structural validity by Rasch analysis: After verifying that the model was unidimensional, a Rasch analysis was performed. To that end, the OV scores were adapted from a 1–5 range to a 0–4 range.
- -
- Reliability: The Omega and Alpha coefficients were calculated, as well as the Bayes expected a posteriori estimation (EAP scores) [50] reliability of the factorial structure;
- -
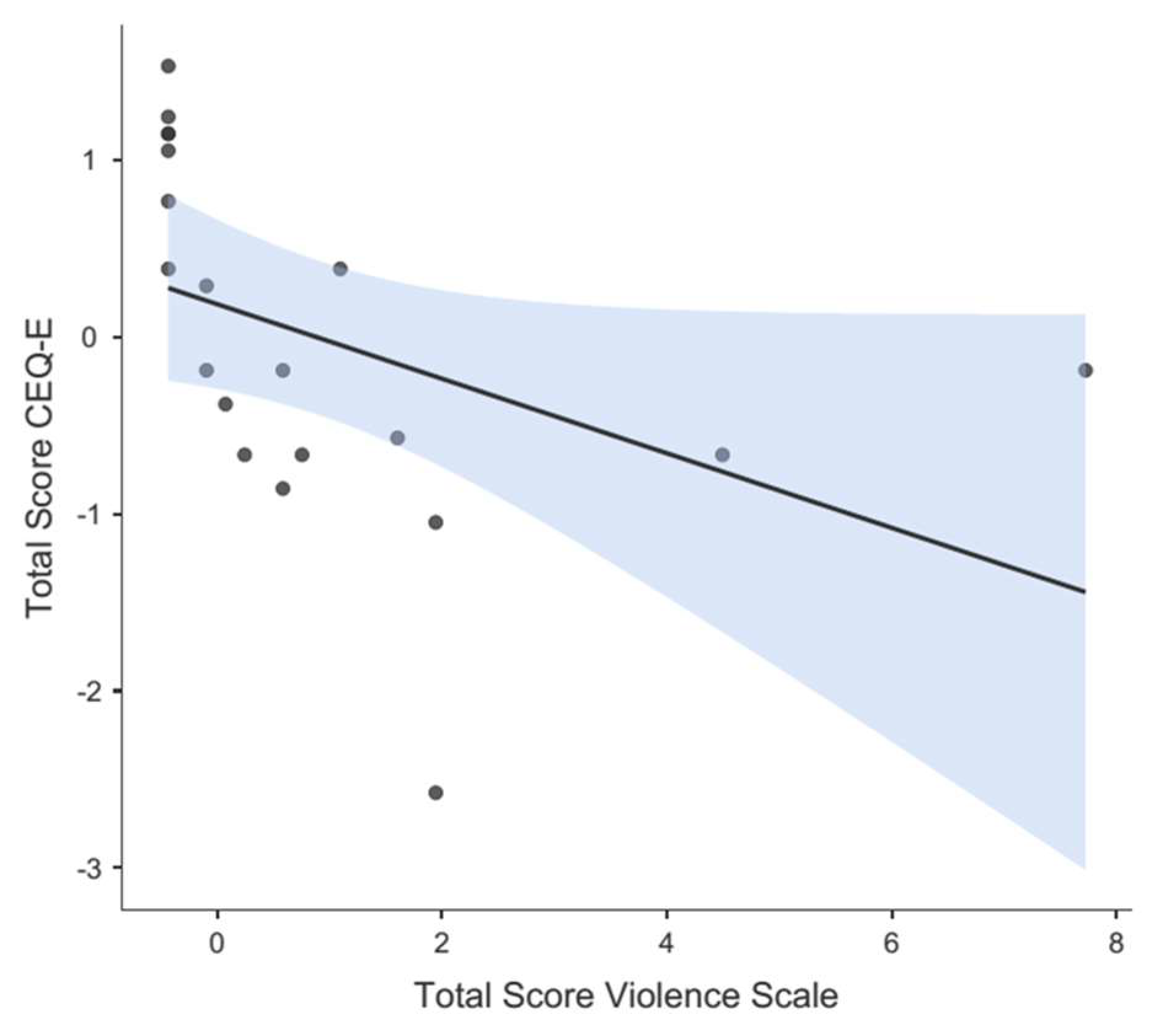
- Divergent validity: To explore a possible negative correlation between the OV scale and the CEQ-E questionnaire, the Spearman correlation coefficient was used since the normality test (Shapiro–Wilk test) showed non-symmetry for the OV scale scores’ distribution—considering negative correlation for coefficients (r) higher than −0.5. Standardized scores (z-values) were used to compare both tools;
- -
- Final proposed scale and known-groups validation: Once a final structure of the OV scale was reached, an inferential analysis was conducted to explore the association between the different variables and the score, by comparing groups of women likely to have experienced OV according to several aspects described in the literature. Since data were asymmetric, as evidenced by the Kolmogorov–Smirnov test, the non-parametric Mann–Whitney U test was used to compare means between two groups and the Kruskal–Wallis contrast test was used to compare means between more than two groups, followed by a post hoc contrast (Dwass–Steel–Critchlow–Fligne test) to identify the group comparisons that showed the differences; α values ≤ 0.05 were considered statistically significant. The effect size was calculated for each evaluated association using the Hedges’ formula (Hedges’ g) and Kelley’s epsilon squared measure.
2.2.7. Ethical Considerations
3. Results
3.1. Phase 1
3.1.1. Content Validity
3.1.2. Face Validity and Pilot Study in a Target Population
3.2. Phase 2
3.2.1. Descriptive Analysis of the Sample and the Items
3.2.2. Construct Validity by Factor Analysis
3.2.3. Construct Structural Validity by Rasch Analysis
3.2.4. Reliability
3.2.5. Divergent Validity
3.2.6. Final Proposed Scale and Known-Groups Validation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Public Involvement Statement
Guidelines and Standards Statement
References
- Mena-Tudela, D.; Iglesias-Casás, S.; González-Chordá, V.M.; Cervera-Gasch, Á.; Andreu-Pejó, L.; Valero-Chilleron, M.J. Obstetric violence in Spain (Part I): Women’s perception and interterritorial differences. Int. J. Environ. Res. Public Health 2020, 17, 7726. [Google Scholar] [CrossRef] [PubMed]
- Mena-Tudela, D.; Roman, P.; González-Chordá, V.M.; Rodriguez-Arrastia, M.; Gutiérrez-Cascajares, L.; Ropero-Padilla, C. Experiences with obstetric violence among healthcare professionals and students in Spain: A constructivist grounded theory study. Women Birth 2023, 36, e219–e226. [Google Scholar] [CrossRef] [PubMed]
- Darilek, U. A Woman’s Right to Dignified, Respectful Healthcare During Childbirth: A Review of the Literature on Obstetric Mistreatment. Issues Ment. Health Nurs. 2018, 39, 538–541. [Google Scholar] [CrossRef]
- Savage, V.; Castro, A. Measuring mistreatment of women during childbirth: A review of terminology and methodological approaches. Reprod. Health 2017, 14, 138. [Google Scholar] [CrossRef] [PubMed]
- Betron, M.L.; McClair, T.L.; Currie, S.; Banerje, J. Expanding the agenda for addressing mistreatment in maternity care: A mapping review and gender analysis. Reprod. Health 2018, 15, 143. [Google Scholar] [CrossRef]
- Rodríguez Mir, J.; Martínez Gandolfi, A. La violencia obstétrica: Una práctica invisibilizada en la atención médica en España [Obstetric violence. A hidden practice in medical care in Spain]. Gac. Sanit. 2021, 35, 211–212. [Google Scholar] [CrossRef] [PubMed]
- Araujo-Cuauro, J.C. Obstetric violence: A hidden dehumanizing practice, exercised by medical care personnel: Is it a public health and human rights problem? Rev. Mex. Med. Forense 2019, 4, 1–11. [Google Scholar]
- WHO Statement. World Health Organization [Internet]. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/134588/WHO_RHR_14.23_cze.pdf (accessed on 24 November 2022).
- Martínez-Galiano, J.M.; Rodríguez-Almagro, J.; Rubio-Álvarez, A.; Ortiz-Esquinas, I.; Ballesta-Castillejos, A.; Hernández-Martínez, A. Obstetric Violence from a Midwife Perspective. Int. J. Environ. Res. Public Health 2023, 20, 4930. [Google Scholar] [CrossRef]
- Faheem, A. The nature of obstetric violence and the organisational context of its manifestation in India: A systematic review. Sex. Reprod. Health Matters 2021, 29, 2004634. [Google Scholar] [CrossRef]
- Mena-Tudela, D.; Iglesias-Casás, S.; González-Chordá, V.M.; Cervera-Gasch, Á.; Andreu-Pejó, L.; Valero-Chilleron, M.J. Obstetric Violence in Spain (Part II): Interventionism and Medicalization during Birth. Int. J. Environ. Res. Public Health 2020, 18, 199. [Google Scholar] [CrossRef]
- Jiang, H.; Qian, X.; Carroli, G.; Garner, P. Selective versus routine use of episiotomy for vaginal birth. Cochrane Database Syst. Rev. 2017, 2, CD000081. [Google Scholar] [CrossRef] [PubMed]
- Lurie, J.M.; Weidman, A.; Huynh, S.; Delgado, D.; Easthausen, I.; Kaur, G. Painful gynecologic and obstetric complications of female genital mutilation/cutting: A systematic review and meta-analysis. PLoS Med. 2020, 17, e1003088. [Google Scholar] [CrossRef] [PubMed]
- Pereira, G.M.V.; Hosoume, R.S.; de Castro Monteiro, M.V.; Juliato, C.R.T.; Brito, L.G.O. Selective episiotomy versus no episiotomy for severe perineal trauma: A systematic review with meta-analysis. Int. Urogynecol. J. 2020, 31, 2291–2299. [Google Scholar] [CrossRef] [PubMed]
- Shabot, S.C. We birth with others: Towards a Beauvoirian understanding of obstetric violence. Eur. J. Womens Stud. 2021, 28, 213–228. [Google Scholar] [CrossRef]
- Sadler, M.; Santos, M.J.; Ruiz-Berdún, D.; Rojas, G.L.; Skoko, E.; Gillen, P.; Clausen, J.A. Moving beyond disrespect and abuse: Addressing the structural dimensions of obstetric violence. Reprod. Health Matters 2016, 24, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Bohren, M.A.; Vogel, J.P.; Hunter, E.C.; Lutsiv, O.; Makh, S.K.; Souza, J.P.; Aguiar, C.; Saraiva Coneglian, F.; Diniz, A.L.; Tunçalp, Ö.; et al. The Mistreatment of Women during Childbirth in Health Facilities Globally: A Mixed-Methods Systematic Review. PLoS Med. 2015, 12, e1001847. [Google Scholar] [CrossRef]
- Lai, X.; Chen, J.; Li, H.; Zhou, L.; Huang, Q.; Liao, Y.; Krewski, D.; Wen, S.W.; Zhang, L.; Xie, R.H. The incidence of post-traumatic stress disorder following traumatic childbirth: A systematic review and meta-analysis. Int. J. Gynaecol. Obstet. 2023, 162, 211–221. [Google Scholar] [CrossRef]
- Ertan, D.; Hingray, C.; Burlacu, E.; Sterlé, A.; El-Hage, W. Post-traumatic stress disorder following childbirth. BMC Psychiatry 2021, 21, 155. [Google Scholar] [CrossRef]
- Beck, C.T.; Gable, R.K. A mixed methods study of secondary traumatic stress in labor and delivery nurses. J. Obstet. Gynecol. Neonatal Nurs. 2012, 41, 747–760. [Google Scholar] [CrossRef]
- Reshef, S.; Mouadeb, D.; Sela, Y.; Weiniger, F.C.; Freedman, S.A. Childbirth, trauma and family relationships. Eur. J. Psychotraumatol. 2023, 14, 2157481. [Google Scholar] [CrossRef]
- Martínez-Vázquez, S.; Hernández-Martínez, A.; Rodríguez-Almagro, J.; Delgado-Rodríguez, M.; Martínez-Galiano, J.M. Relationship between perceived obstetric violence and the risk of postpartum depression: An observational study. Midwifery 2022, 108, 103297. [Google Scholar] [CrossRef] [PubMed]
- Reuther, M.L. Prevalence of Obstetric Violence in Europe: Exploring Associations with Trust, and Care-Seeking Intention. Bachelor’s Thesis, University of Twente, Enschede, The Netherlands, 2021. [Google Scholar]
- Miller, S.; Lalonde, A. The global epidemic of abuse and disrespect during childbirth: History, evidence, interventions, and FIGO’s mother-baby friendly birthing facilities initiative. Int. J. Gynaecol. Obstet. 2015, 131, S49–S52. [Google Scholar] [CrossRef]
- Khalil, M.; Carasso, K.B.; Kabakian-Khasholian, T. Exposing Obstetric Violence in the Eastern Mediterranean Region: A Review of Women’s Narratives of Disrespect and Abuse in Childbirth. Front. Glob. Womens Health 2022, 3, 850796. [Google Scholar] [CrossRef] [PubMed]
- Santiago, R.V.; Solórzano, E.H.; Iñiguez, M.M.; Monreal, L.M.A. Nueva evidencia a un viejo problema: El abuso de las mujeres en las salas de parto. Rev. Conamed 2015, 18, 14–20. [Google Scholar]
- Terán, P.; Castellanos, C.; Gonzalez Blanco, M.; Ramos, D. Violencia obstétrica: Percepción de las usuarias. Rev. Obstet. Ginecol. Venez. 2013, 73, 171–180. [Google Scholar]
- Molla, W.; Wudneh, A.; Tilahun, R. Obstetric violence and associated factors among women during facility based childbirth at Gedeo Zone, South Ethiopia. BMC Pregnancy Childbirth 2022, 22, 565. [Google Scholar] [CrossRef]
- Sando, D.; Ratcliffe, H.; McDonald, K.; Spiegelman, D.; Lyatuu, G.; Mwanyika-Sando, M.; Emil, F.; Wegner, M.N.; Chalamilla, G.; Langer, A. The prevalence of disrespect and abuse during facility-based childbirth in urban Tanzania. BMC Pregnancy Childbirth 2016, 16, 236. [Google Scholar] [CrossRef]
- Yalley, A.A. “We Beat Them to Help Them Push”: Midwives’ Perceptions on Obstetric Violence in the Ashante and Western Regions of Ghana. Women 2023, 3, 22–40. [Google Scholar] [CrossRef]
- Ferrão, A.C.; Sim-Sim, M.; Almeida, V.S.; Zangão, M.O. Analysis of the Concept of Obstetric Violence: Scoping Review Protocol. J. Pers. Med. 2022, 12, 1090. [Google Scholar] [CrossRef] [PubMed]
- Mena-Tudela, D.; Iglesias-Casás, S.; González-Chordá, V.M.; Valero-Chillerón, M.J.; Andreu-Pejó, L.; Cervera-Gasch, Á. Obstetric Violence in Spain (Part III): Healthcare Professionals, Times, and Areas. Int. J. Environ. Res. Public Health 2021, 18, 3359. [Google Scholar] [CrossRef] [PubMed]
- Swahnberg, I.M.; Wijma, B. The NorVold Abuse Questionnaire (NorAQ): Validation of new measures of emotional, physical, and sexual abuse, and abuse in the health care system among women. Eur. J. Public Health 2003, 13, 361–366. [Google Scholar] [CrossRef]
- Dhakal, P.; Gamble, J.; Creedy, D.K.; Newnham, E. Development of a tool to assess students’ perceptions of respectful maternity care. Midwifery 2022, 105, 103228. [Google Scholar] [CrossRef]
- Dhakal, P.; Creedy, D.K.; Gamble, J.; Newnham, E.; McInnes, R. Effectiveness of an online education intervention to enhance student perceptions of Respectful Maternity Care: A quasi-experimental study. Nurse Educ. Today 2022, 114, 105405. [Google Scholar] [CrossRef]
- Çamlibel, M.; Uludağ, E. The Turkish version of the students’ perceptions of respectful maternity care scale: An assessment of psychometric properties. Nurse Educ. Pract. 2023, 70, 103684. [Google Scholar] [CrossRef] [PubMed]
- Mena-Tudela, D.; Cervera-Gasch, A.; Alemany-Anchel, M.J.; Andreu-Pejó, L.; González-Chordá, V.M. Design and Validation of the PercOV-S Questionnaire for Measuring Perceived Obstetric Violence in Nursing, Midwifery and Medical Students. Int. J. Environ. Res. Public Health 2020, 17, 8022. [Google Scholar] [CrossRef] [PubMed]
- Mena-Tudela, D.; Cervera-Gasch, Á.; Andreu-Pejó, L.; Alemany-Anchel, M.J.; Valero-Chillerón, M.J.; Peris-Ferrando, E.; Mahiques-Llopis, J.; González-Chordá, V.M. Perception of obstetric violence in a sample of Spanish health sciences students: A cross-sectional study. Nurse Educ. Today 2022, 110, 105266. [Google Scholar] [CrossRef]
- Biurrun-Garrido, A.; Brigidi, S.; Mena-Tudela, D. Perception of health sciences and feminist medical students about obstetric violence. Enferm. Clin. (Engl. Ed.) 2023, 33, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Cárdenas, M.; Salinero, S. Validación de la escala de violencia obstétrica y pruebas de la invarianza factorial en una muestra de mujeres chilenas. Interdisciplinaria 2021, 38, 209–223. [Google Scholar] [CrossRef]
- El Parto es Nuestro. Test de Violencia Obstétrica. Available online: https://www.elpartoesnuestro.es/blog/2014/08/18/test-de-violencia-obstetrica (accessed on 25 September 2022).
- Penfield, R.D.; Giacobbi, P.R., Jr. Applying a score confidence interval to Aiken’s item content-relevance index. Meas. Phys. Educ. Exerc. Sci. 2004, 8, 213–225. [Google Scholar] [CrossRef]
- Barrio-Cantalejo, I.M.; Simón-Lorda, P.; Melguizo, M.; Escalona, I.; Marijuán, M.I.; Hernando, P. Validación de la Escala INFLESZ para evaluar la legibilidad de los textos dirigidos a pacientes. An. Sist. Sanit. Navar. 2008, 31, 135–152. [Google Scholar] [CrossRef]
- Ferrando, P.J.; Lorenzo-Seva, U.; Hernández-Dorado, A.; Muñiz, J. Decalogue for the Factor Analysis of Test Items. Psicothema 2022, 34, 7–17. [Google Scholar] [CrossRef]
- Lloret-Segura, S.; Ferreres-Traver, A.; Hernández-Baeza, A.; Tomás-Marco, I. Exploratory Item Factor Analysis: A practical guide revised and updated. Anal. Psicol. 2014, 30, 1151–1169. [Google Scholar] [CrossRef]
- Soriano-Vidal, F.J.; Oliver-Roig, A.; Cabrero-García, J.; Congost-Maestre, N.; Dencker, A.; Richart-Martínez, M. The Spanish version of the Childbirth Experience Questionnaire (CEQ-E): Reliability and validity assessment. BMC Pregnancy Childbirth 2016, 16, 372. [Google Scholar] [CrossRef]
- González-de la Torre, H.; Miñarro-Jiménez, S.; Palma-Arjona, I.; Jeppesen-Gutierrez, J.; Berenguer-Pérez, M.; Verdú-Soriano, J. Perceived satisfaction of women during labour at the Hospital Universitario Materno-Infantil of the Canary Islands through the Childbirth Experience Questionnaire (CEQ-E). Enferm. Clin. (Engl. Ed.) 2021, 31, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Lloret-Segura, S.; Ferreres-Traver, A.; Hernández-Baeza, A.; Tomás-Marco, I. The exploratory factor analysis of items: Guided analysis based on empirical data and software. Anal. Psicol. 2017, 33, 417–432. [Google Scholar] [CrossRef]
- Hancock, G.R.; Mueller, R.O. Rethinking Construct Reliability within Latent Variable Systems. In Structural Equation Modeling: Present and Future; Cudeck, R., du Toit, S., Sörbom, D., Eds.; Scientific Software: Lincolnwood, IL, USA, 2001; pp. 195–216. [Google Scholar]
- Ferrando, P.J.; Lorenzo-Seva, U. Assessing the quality and appropriateness of factor solutions and factor score estimates in exploratory item factor analysis. Educ. Psychol. Meas. 2018, 78, 762–780. [Google Scholar] [CrossRef] [PubMed]
- Bond, T.G.; Fox, C.M. Applying the Rasch Model: Fundamental Measurement in the Human Sciences, 2nd ed.; Lawrence Erlbaum: Mahwah, NJ, USA, 2007. [Google Scholar] [CrossRef]
- Christensen, K.B.; Makransky, G.; Horton, M. Critical Values for Yen’s Q3: Identification of Local Dependence in the Rasch Model Using Residual Correlations. Appl. Psychol. Meas. 2017, 41, 178–194. [Google Scholar] [CrossRef]
- Rodríguez Mir, J.; Martínez Gandolfi, A. Obstetric violence denied in Spain. Enferm. Clin. (Engl. Ed.) 2022, 32 (Suppl. 1), S82–S83. [Google Scholar] [CrossRef] [PubMed]
- Khsim, I.E.F.; Rodríguez, M.M.; Riquelme Gallego, B.; Caparros-González, R.A.; Amezcua-Prieto, C. Risk Factors for Post-Traumatic Stress Disorder after Childbirth: A Systematic Review. Diagnostics 2022, 12, 2598. [Google Scholar] [CrossRef]
- Soto, C.M.; Segovia, J.L. Confidence intervals for the content validity: A Visual Basic computer program for the Aiken’s V. Anal. Psicol. 2009, 25, 169–171. [Google Scholar]
- Charter, R.A. A breakdown of reliability coefficients by test type and reliability method and the clinical implications of low reliability. J. Gen. Psychol. 2003, 130, 290–304. [Google Scholar] [CrossRef] [PubMed]
- Fraser, C.; McDonald, R.P. NOHARM: Least squares item factor analysis. Multivar. Behav. Res. 1988, 23, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, P.J.; Lorenzo-Seva, U. El Análisis Factorial Exploratorio de los Ítems: Algunas consideraciones adicionales. Anal. Psicol. 2014, 30, 1170–1175. [Google Scholar] [CrossRef]
- Lord, F.M. Applications of Item Response Theory to Practical Testing Problems, 1st ed.; Routledge Taylor and Francis Group: New York, NY, USA, 2012. [Google Scholar]
- Escobar Bravo, M.A. Adaptación transcultural de instrumentos de medida relacionados con la salud. Enferm. Clin. 2004, 14, 102–106. [Google Scholar] [CrossRef]
- Stolt, M.; Kottorp, A.; Suhonen, R. The use and quality of reporting of Rasch analysis in nursing research: A methodological scoping review. Int. J. Nurs. Stud. 2022, 132, 104244. [Google Scholar] [CrossRef]
- McNeish, D. Thanks coefficient alpha, we’ll take it from here. Psychol. Methods 2018, 23, 412–433. [Google Scholar] [CrossRef]
- Martínez-Galiano, J.M.; Martínez-Vazquez, S.; Rodríguez-Almagro, J.; Hernández-Martinez, A. The magnitude of the problem of obstetric violence and its associated factors: A cross-sectional study. Women Birth 2021, 34, e526–e536. [Google Scholar] [CrossRef]
- BOE-A-2002-22188. Ley 41/2002, de 14 de Noviembre, Básica Reguladora de la Autonomía del Paciente y de Derechos y Obligaciones en Materia de Información y Documentación Clínica. Spain. 2002. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-2002-22188 (accessed on 14 June 2023).
- Medeiros, R.M.K.; Figueiredo, G.; Correa, Á.C.P.; Barbieri, M. Repercussions of using the birth plan in the parturition process. Rev. Gauch. Enferm. 2019, 40, e20180233. [Google Scholar] [CrossRef]
- Mirghafourvand, M.; Mohammad Alizadeh Charandabi, S.; Ghanbari-Homayi, S.; Jahangiry, L.; Nahaee, J.; Hadian, T. Effect of birth plans on childbirth experience: A systematic review. Int. J. Nurs. Pract. 2019, 25, e12722. [Google Scholar] [CrossRef]
- Bell, C.H.; Muggleton, S.; Davis, D.L. Birth plans: A systematic, integrative review into their purpose, process, and impact. Midwifery 2022, 111, 103388. [Google Scholar] [CrossRef]
- Baranowska, B.; Doroszewska, A.; Kubicka-Kraszyńska, U.; Pietrusiewicz, J.; Adamska-Sala, I.; Kajdy, A.; Sys, D.; Tataj-Puzyna, U.; Bączek, G.; Crowther, S. Is there respectful maternity care in Poland? Women’s views about care during labor and birth. BMC Pregnancy Childbirth 2019, 19, 520. [Google Scholar] [CrossRef] [PubMed]
- Brazy-Nancy, E.; Mattern, C.; Rakotonandrasana, B.I.; Ravololomihanta, V.; Norolalao, P.; Kapesa, L. A qualitative analysis of obstetric violence in rural Madagascar. Heliyon 2023, 9, e13905. [Google Scholar] [CrossRef] [PubMed]
- Galera-Barbero, T.M.; Aguilera-Manrique, G. Women’s reasons and motivations around planning a home birth with a qualified midwife in Spain. J. Adv. Nurs. 2022, 78, 2608–2621. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Expert 1 | Expert 2 | Expert 3 | Expert 4 | Expert 5 | Expert 6 | Expert 7 | Expert 8 | CVI-i [95%CI] * | |
|---|---|---|---|---|---|---|---|---|---|
| Item 1 | 4 | 4 | 4 | 4 | 3 | 4 | 4 | 3 | 0.92 [0.74–0.98] |
| Item 2 | 3 | 4 | 4 | 2 | 3 | 4 | 3 | 2 | 0.71 [0.51–0.85] |
| Item 3 | 3 | 4 | 4 | 1 | 3 | 4 | 4 | 4 | 0.79 [0.60–0.91] |
| Item 4 | 3 | 4 | 4 | 2 | 4 | 4 | 4 | 3 | 0.83 [0.64–0.93] |
| Item 5 | 4 | 4 | 4 | 2 | 4 | 4 | 4 | 3 | 0.88 [0.69–0.96] |
| Item 6 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 1.00 [0.86–1.00] |
| Item 7 | 3 | 4 | 4 | 3 | 3 | 4 | 3 | 3 | 0.79 [0.60–0.91] |
| Item 8 | 4 | 4 | 4 | 3 | 3 | 4 | 3 | 3 | 0.83 [0.74–0.93] |
| Item 9 | 4 | 4 | 4 | 3 | 3 | 4 | 4 | 3 | 0.88 [0.69–0.96] |
| Item 10 | 4 | 4 | 4 | 3 | 3 | 4 | 3 | 3 | 0.83 [0.64–0.93] |
| Item 11 | 4 | 4 | 4 | 3 | 4 | 4 | 4 | 3 | 0.92 [0.74–0.98] |
| Item 12 | 3 | 4 | 4 | 4 | 3 | 3 | 3 | 2 | 0.75 [0.55–0.88] |
| Item 13 | 4 | 4 | 4 | 3 | 2 | 3 | 3 | 3 | 0.75 [0.55–0.88] |
| Item 14 | 4 | 4 | 4 | 3 | 3 | 4 | 4 | 3 | 0.88 [0.69–0.96] |
| Item | M [95%CI] * | SD ** | Symmetry *** | Kurtosis *** |
|---|---|---|---|---|
| 1—Members of the healthcare staff made ironic or derogative comments or made jokes about your behavior. | 1.22 [1.09–1.36] | 0.85 | 3.90 | 13.91 |
| 2—You were addressed to with nicknames or diminutives (e.g., mummy, chubby, etc.) or treated as if you were unable to understand the processes you were going through. | 1.10 [1.02–1.19] | 0.55 | 5.90 | 35.06 |
| 3—You felt treated as a child or neglected by the staff, as if you were unable to make decisions about what was happening to you before, during or after delivery. | 1.25 [1.13–1.39] | 0.82 | 3.55 | 12.11 |
| 4—You were somehow criticized for expressing your emotions (cry, scream of pain, etc.) during labor or delivery. | 1.24 [1.10–1.38] | 0.86 | 3.70 | 12.54 |
| 5—It was impossible for you to ask queries or express your fears or concerns because nobody answered, or they answered in a bad way. | 1.18 [1.07–1.31] | 0.74 | 4.34 | 18.20 |
| 6—You were subjected to medical procedures without being asked for your consent or without explanation as to why such procedures were needed. | 1.37 [1.21–1.54] | 1.03 | 2.79 | 6.47 |
| 7—At the moment of delivery, you were compelled to keep lying on your back despite expressing your discomfort with that position. | 1.27 [1.13–1.42] | 0.90 | 3.32 | 9.83 |
| 8—You were compelled to stay in bed and prevented from walking or seeking the position you needed. | 1.21 [1.09–1.35] | 0.79 | 3.88 | 14.26 |
| 9—You were not allowed to be accompanied by someone you trusted. | 1.15 [1.04–1.27] | 0.71 | 4.75 | 21.46 |
| 10—You were prevented from having immediate contact with your newborn, before the doctor took him/her away (caressing, holding him/her in your arms, etc.). | 1.21 [1.09–1.35] | 0.83 | 3.83 | 13.36 |
| 11—After delivery, they made you feel you had not behaved up to what was expected of you (that you had not “helped”). | 1.08 [1.00–1.16] | 0.48 | 6.55 | 44.21 |
| 12—Your childbirth care experience made you feel vulnerable, guilty or insecure in any sense. | 1.23 [1.11–1.37] | 0.80 | 3.59 | 12.22 |
| 13—After delivery, you were denied the opportunity to use a birth control device or procedure (IUD, tubal ligation, etc.). | 1.09 [1.01–1.17] | 0.50 | 6.17 | 39.37 |
| 14—During or after labor, you felt exposed to the gaze of other people unknown to you (exposure to strangers). | 1.46 [1.28–1.65] | 1.16 | 2.41 | 4.24 |
| Items | Factor 1 | 95%IC * |
|---|---|---|
| 1—Members of the healthcare staff made ironic or derogative comments or made jokes about your behavior. | 0.721 | [0.354–0.878] |
| 2—You were addressed to with nicknames or diminutives (e.g., mummy, chubby, etc.) or treated as if you were unable to understand the processes you were going through. | 0.645 | [0.299–0.892] |
| 3—You felt treated as a child or neglected by the staff, as if you were unable to make decisions about what was happening to you before, during or after delivery. | 0.842 | [0.594–0.963] |
| 4—You were somehow criticized for expressing your emotions (cry, scream of pain, etc.) during labor or delivery. | 0.748 | [0.387–0.912] |
| 5—It was impossible for you to ask queries or express your fears or concerns because nobody answered, or they answered in a bad way. | 0.884 | [0.470–1.000] |
| 6—You were subjected to medical procedures without being asked for your consent or without explanation as to why such procedures were needed. | 0.745 | [0.364–0.868] |
| 7—At the moment of delivery, you were compelled to keep lying on your back despite expressing your discomfort with that position. | 0.486 | [0.188–0.739] |
| 8—You were compelled to stay in bed and prevented from walking or seeking the position you needed. | 0.790 | [0.377–0.918] |
| 9—You were not allowed to be accompanied by someone you trusted. | 0.695 | [0.334–0.898] |
| 10—You were prevented from having immediate contact with your newborn, before the doctor took him/her away (caressing, holding him/her in your arms, etc.). | 0.771 | [0.375–0.911] |
| 11—After delivery, they made you feel you had not behaved up to what was expected of you (that you had not “helped”). | 0.891 | [0.491–1.000] |
| 12—Your childbirth care experience made you feel vulnerable, guilty or insecure in any sense. | 0.957 | [0.734–1.000] |
| 13—After delivery, you were denied the opportunity to use a birth control device or procedure (IUD, tubal ligation, etc.). | 0.473 | [−0.489–0.764] |
| 14—During or after labor, you felt exposed to the gaze of other people unknown to you (exposure to strangers). | 0.755 | [0.460–0.949] |
| Item | Difficulty Index * | Infit WMS ** | Outfit UMS ** |
|---|---|---|---|
| 1—Members of the healthcare staff made ironic or derogative comments or made jokes about your behavior. | −0.09 | 1.09 | 1.17 |
| 3—You felt treated as a child or neglected by the staff, as if you were unable to make decisions about what was happening to you before, during or after delivery. | −0.08 | 0.85 | 0.83 |
| 4—You were somehow criticized for expressing your emotions (cry, scream of pain, etc.) during labor or delivery. | −0.11 | 1.18 | 1.39 |
| 5—It was impossible for you to ask queries or express your fears or concerns because nobody answered, or they answered in a bad way. | 0.02 | 0.77 | 0.58 |
| 6—You were subjected to medical procedures without being asked for your consent or without explanation as to why such procedures were needed. | −0.32 | 1.08 | 1.06 |
| 7—At the moment of delivery, you were compelled to keep lying on your back despite expressing your discomfort with that position. | −0.11 | 1.06 | 1.08 |
| 8—You were compelled to stay in bed and prevented from walking or seeking the position you needed. | −0.00 | 0.93 | 0.76 |
| 9—You were not allowed to be accompanied by someone you trusted. | 0.10 | 1.16 | 1.16 |
| 10—You were prevented from having immediate contact with your newborn, before the doctor took him/her away (caressing, holding him/her in your arms, etc.). | −0.03 | 1.02 | 0.95 |
| 11—After delivery, they made you feel you had not behaved up to what was expected of you (that you had not “helped”). | 0.54 | 0.86 | 0.37 |
| 12—Your childbirth care experience made you feel vulnerable, guilty or insecure in any sense. | 0.02 | 0.58 | 0.45 |
| 13—After delivery, you were denied the opportunity to use a birth control device or procedure (IUD, tubal ligation, etc.). | 0.53 | 1.09 | 1.13 |
| 14—During or after labor, you felt exposed to the gaze of other people unknown to you (exposure to strangers). | −0.46 | 1.21 | 1.17 |
| Variables | M (SD) * | p-Value ** | Effect Size *** |
|---|---|---|---|
| Parity | |||
| Primiparous (n = 159) | 3.59 (7.39) | 0.040 ** | 0.23 |
| Multiparous (n = 97) | 2.11 (4.75) | ||
| Episiotomy | |||
| No (n = 224) | 2.63 (5.97) | 0.012 ** | 0.50 |
| Yes (n = 32) | 5.84 (9.32) | ||
| You were asked consent for episiotomy | |||
| No (n = 15) | 8.93 (9.87) | 0.010 ** | 0.65 |
| Yes (n = 17) | 3.12 (8.13) | ||
| Artificial rupture of membranes (ARM) | |||
| No (n = 173) | 2.38 (6.43) | ≤0.001 ** | 0.31 |
| Yes (n = 83) | 4.40 (6.62) | ||
| You were asked consent for ARM | |||
| No (n = 18) | 9.78 (7.26) | ≤0.001 ** | 1.14 |
| Yes (n = 65) | 2.91 (5.63) | ||
| Inducing labor | |||
| No (n = 140) | 2.81 (6.80) | 0.195 | 0.07 |
| Yes (n = 116) | 3.29 (6.24) | ||
| You were asked consent for inducing labor | |||
| No (n = 18) | 6.83 (7.23) | ≤0.001 ** | 0.68 |
| Yes (n = 99) | 2.70 (5.85) | ||
| Prohibition of receiving food | |||
| No (n = 192) | 2.74 (6.52) | 0.018 ** | 0.18 |
| Yes (n = 64) | 3.89 (6.61) | ||
| Epidural analgesia | |||
| No (n = 70) | 1.56 (3.84) | 0.006 ** | 0.31 |
| Yes (n = 186) | 3.59 (7.24) | ||
| Presentation of a childbirth plan | |||
| No (n = 182) | 2.40 (5.75) | 0.066 | 0.34 |
| Yes (n = 74) | 4.58 (8.03) | ||
| Your childbirth plan was observed | |||
| No (n = 12) | 12.42 (12.93) | ≤0.001 ** | 1.28 |
| Yes (n = 62) | 3.04 (5.70) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-de la Torre, H.; González-Artero, P.N.; Muñoz de León-Ortega, D.; Lancha-de la Cruz, M.R.; Verdú-Soriano, J. Cultural Adaptation, Validation and Evaluation of the Psychometric Properties of an Obstetric Violence Scale in the Spanish Context. Nurs. Rep. 2023, 13, 1368-1387. https://doi.org/10.3390/nursrep13040115
González-de la Torre H, González-Artero PN, Muñoz de León-Ortega D, Lancha-de la Cruz MR, Verdú-Soriano J. Cultural Adaptation, Validation and Evaluation of the Psychometric Properties of an Obstetric Violence Scale in the Spanish Context. Nursing Reports. 2023; 13(4):1368-1387. https://doi.org/10.3390/nursrep13040115
Chicago/Turabian StyleGonzález-de la Torre, Héctor, Paula Nikola González-Artero, Daniel Muñoz de León-Ortega, María Reyes Lancha-de la Cruz, and José Verdú-Soriano. 2023. "Cultural Adaptation, Validation and Evaluation of the Psychometric Properties of an Obstetric Violence Scale in the Spanish Context" Nursing Reports 13, no. 4: 1368-1387. https://doi.org/10.3390/nursrep13040115