
Effect of Dietary Approaches on Glycemic Control in Patients with Type 2 Diabetes: A Systematic Review with Network Meta-Analysis of Randomized Trials

Abstract
:1. Introduction
2. Method
2.1. Registration
2.2. Search Strategy
2.2.1. Inclusion Criteria
- Randomized controlled trials between different dietary approaches (energy-restricted diets, iso-caloric, or ad libitum diets):
- (1)
- Low-carbohydrate diet: less than 25% carbohydrate intake of total energy intake [31];
- (2)
- Moderate-carbohydrate diet: 25% to 45% carbohydrate intake of total energy intake [31];
- (3)
- Ketogenic diet: 5% to 10% carbohydrate intake of total energy intake, replacing the remaining with dietary fat and adequate protein (1 g/kg) [32];
- (4)
- Low-fat diet: less than 30% fat of total energy intake; high intake of cereals and grains; 10–15% protein intake [31];
- (5)
- High-protein diet: 25% to 35% protein intake of total energy intake [33];
- (6)
- Mediterranean diet: a daily abundance of vegetables, a variety of minimally processed whole grain bread, and other cereals and legumes as the staple food, nuts and seeds, fresh fruit as the typical daily dessert; sweets based on nuts, olive oil, and honey consumed only during celebratory occasions; cold pressed extra-virgin olive oil (EVOO), nuts and seeds as the principal source of fat; a low to moderate consumption of dairy products (mainly local cheese and yogurt) consumed in low amounts; a moderate consumption of fish, poultry, and eggs, a low consumption of red meat (once a week approximately), and a moderate consumption of wine, normally with meals [34];
- (7)
- Paleolithic diet: consumption of lean meat, fish, fruit, leafy and cruciferous vegetables, root vegetables, eggs, and nuts, while excluding dairy products, cereal grains, beans, refined fats, sugar, candy, soft drinks, beer, and extra addition of salt [35];
- (8)
- Nordic diet: consumption of traditional foods from the Nordic countries (the Scandinavian region), including whole grains, fruits (such as apples, pears, and berries), low-fat dairy products, fatty fish such as salmon, cabbage and root vegetables [18];
- (9)
- DASH (dietary approach to stop hypertension): high intake of fruits, vegetables, low-fat dairy products, and whole grains, and low in sodium [36];
- (10)
- Vegetarian/vegan diet: no meat and fish/ no animal products [37];
- (11)
- (12)
- Portfolio dietary pattern: 1–3 g/day plant sterols (plant-sterol containing margarines, supplements), 15–25 g/day viscous fibers (gel-forming fibers, such as from oats, barley, psyllium, legumes, eggplants, okra), 35–50 g/day plant protein (such as from soy and pulses) and 25–50 g/day nuts (including tree nuts and peanuts [39];
- (13)
- (14)
- Control diet/usual diet (e.g., not changing usual diet) [25]: The control diet was used as our reference diet and presented results for the other diets against the reference diet.
The classification of dietary approaches was derived from the original studies whenever possible. However, some dietary approaches can have important overlap with others in the macronutrient distribution. When a dietary approach could be classified as one of the specific dietary approaches (i.e., Mediterranean diet, Paleolithic diet), such classification was preferred over the classification based on macronutrient distribution of the diet. Meanwhile, if a dietary approach was initially claimed to be a low-carbohydrate diet, it would be priorly classified as a moderate-carbohydrate diet rather than a low-fat diet (based on the macronutrient classification in the original study) when it does not meet the criteria for a low-carbohydrate diet. For instance, a trial that was initially categorized as a low-carbohydrate diet [44] was reclassified as a moderate-carbohydrate diet in this study, based on the inclusion criteria for moderate-carbohydrate diets. Adjustments were made to ensure consistency with the classification standards used in our research.
- 2.
- Minimum intervention period of 6 months;
- 3.
- Participants with a mean age ≥ 18 years;
- 4.
- T2DM patients follow the diagnosis criteria of the ADA or according to internationally recognized standards [1].
- 5.
- The outcomes include at least one of HbA1c (%) and fasting glucose (mmol/L), as the main outcomes.
2.2.2. Exclusion Criteria
- Randomized trials including pregnant women, children, and adolescents, patients with abnormal glucose metabolism, chronic kidney disease, and disordered eating patterns;
- Cross-over trials, single-arm trials, and study protocols; nonoriginal studies, including reviews, letters, case reports, or papers that did not provide accurate and clear data;
- Intervention studies solely based on dietary supplements or single foods;
- Intervention studies using dietary supplements as placebo;
- Intervention studies using the medication as a placebo;
- The same type of diet only changes one or a few of its components (e.g., a Mediterranean diet with avocados vs. a Mediterranean diet with nuts);
- Interventions based on very low energy diets (i.e., <600 kcal/day);
- Interventions claimed to be some kind of dietary pattern, but did not meet our criteria.
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Dealing with Missing Data
2.6. Statistical Analysis
2.7. Subgroup and Sensitivity Analyses
2.8. Credibility of the Evidence
3. Results
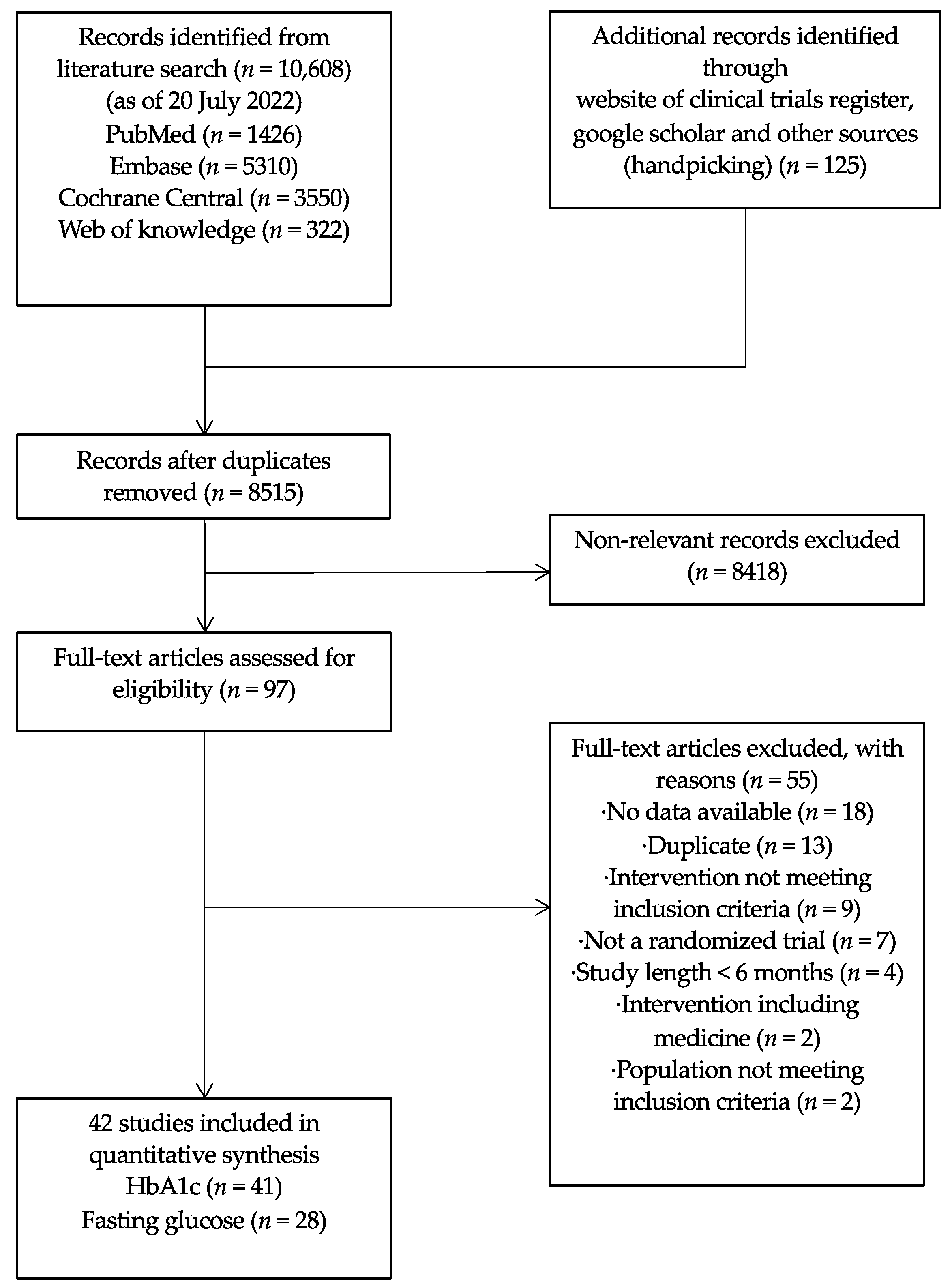
3.1. Search Results and Study Selection
3.2. Study Characteristics
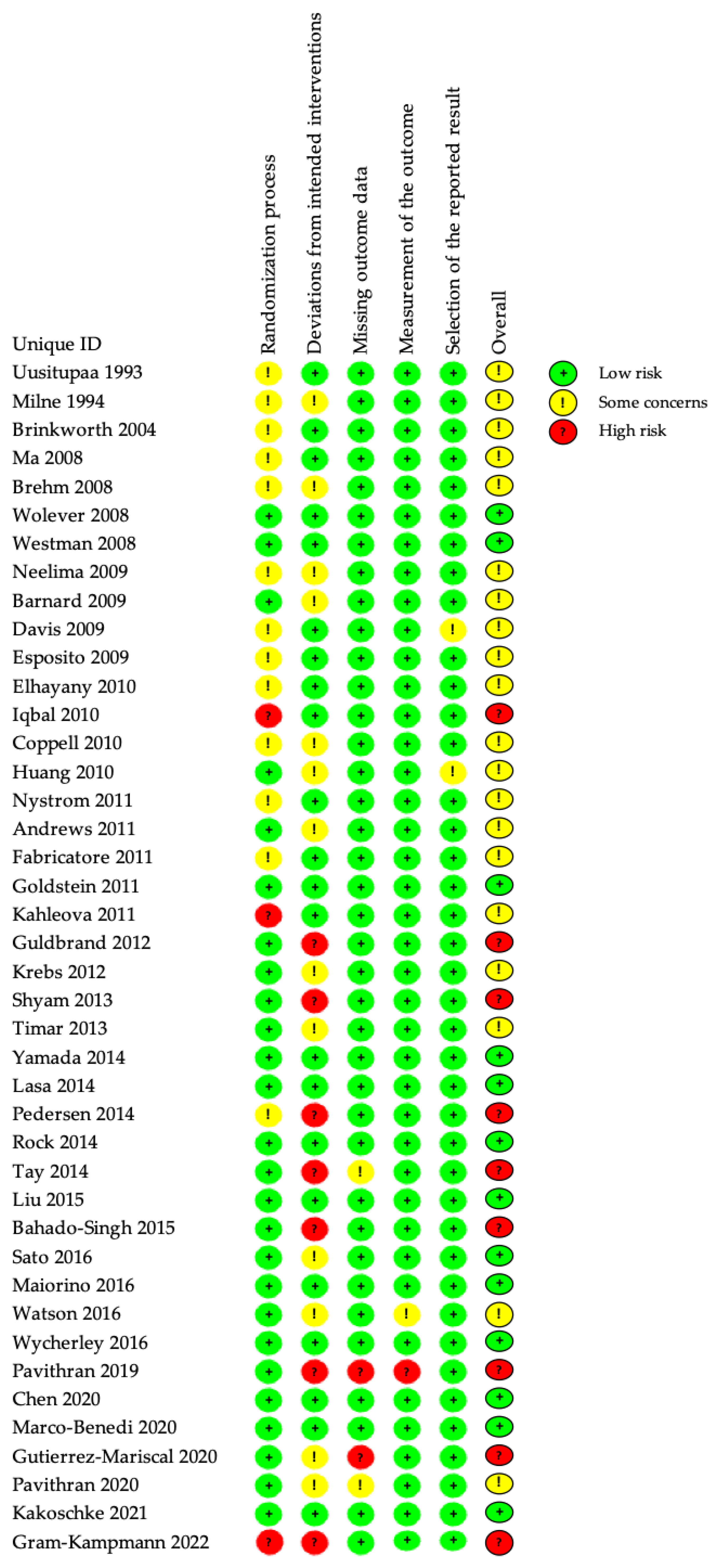
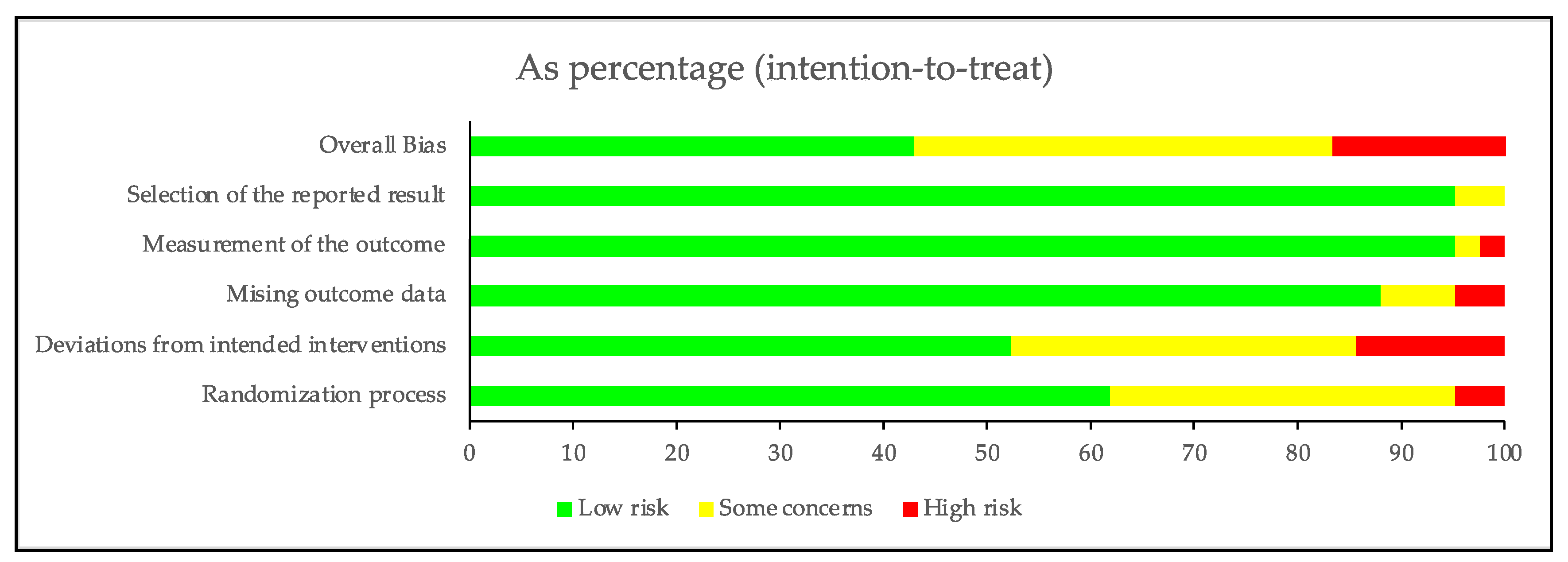
3.3. Risk of Bias in Included Studies
3.4. Effects of the Interventions
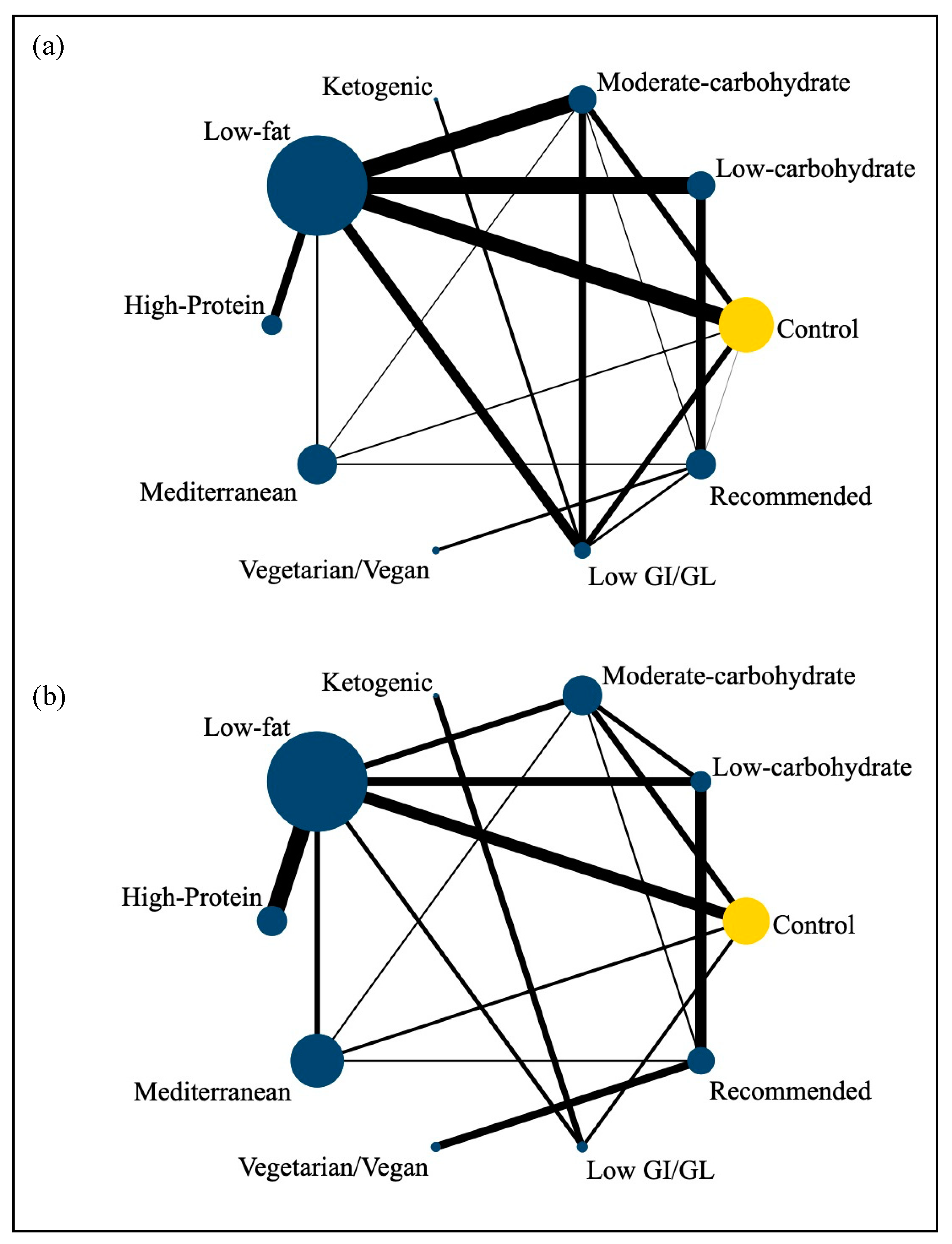
3.4.1. Network Meta-Analysis of the Association between Dietary Patterns and the Glycemic Control
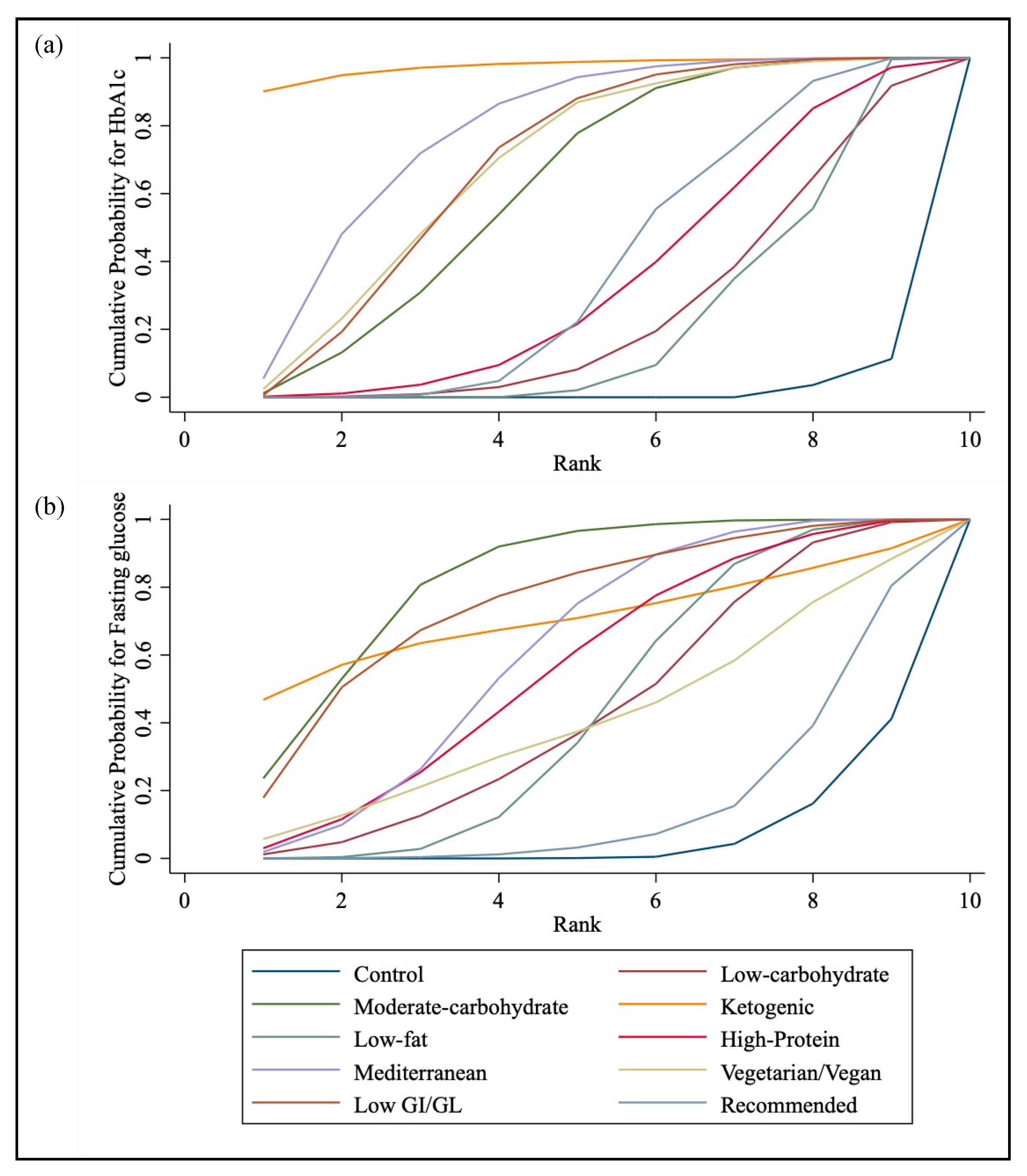
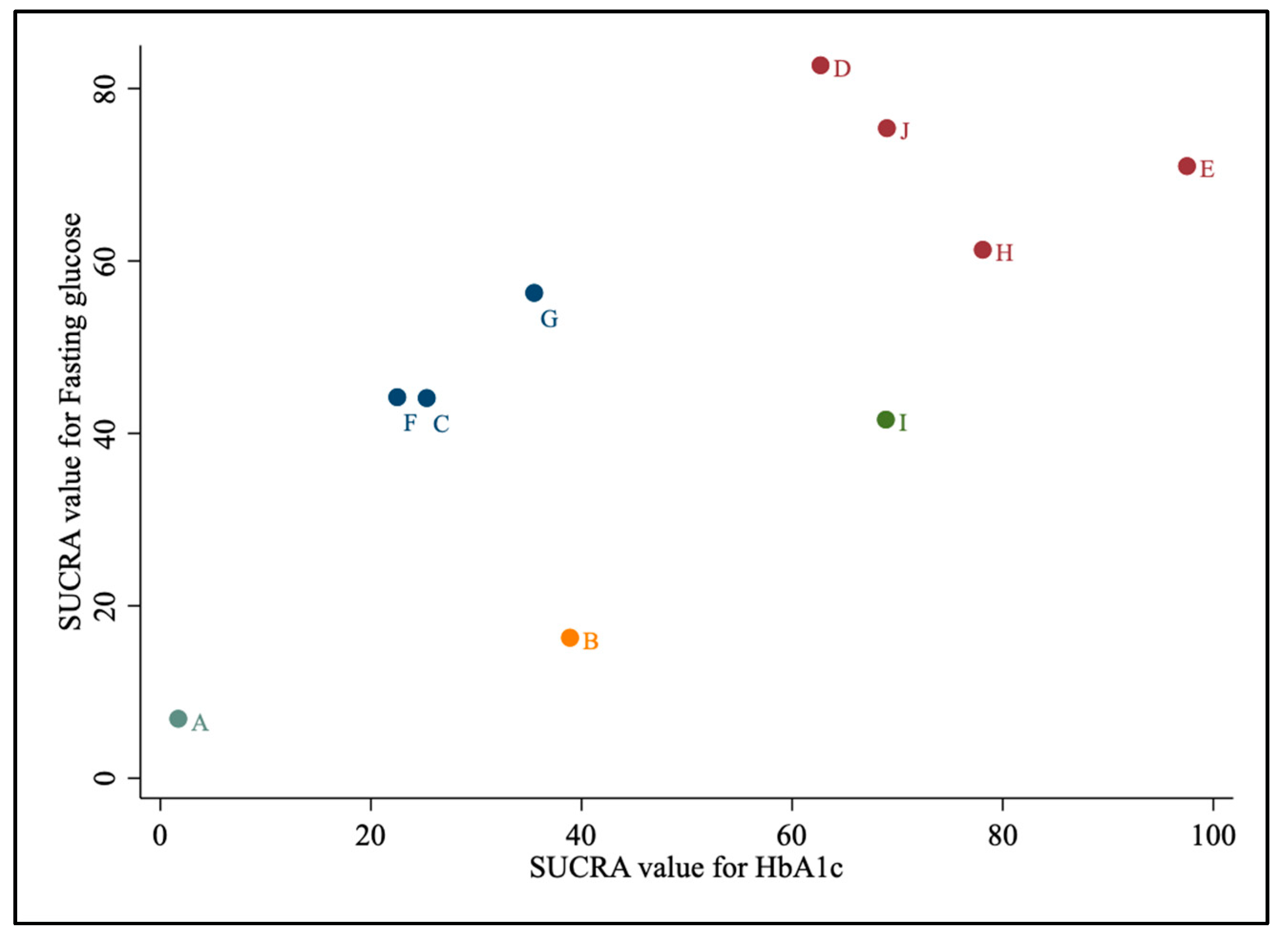
3.4.2. SUCRA
3.5. Inconsistency
3.6. Subgroup and Sensitivity Analyses
3.7. Small Study Effects and Publication Bias
3.8. Meta-Regression and Additional Analyses
3.9. Adverse Events
3.10. Credibility of the Evidence
4. Discussion
Strength and Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44 (Suppl. 1), S15–S33. [Google Scholar] [CrossRef]
- World Health Organization. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harding, J.L.; Pavkov, M.E.; Magliano, D.J.; Shaw, J.E.; Gregg, E.W. Global trends in diabetes complications: A review of current evidence. Diabetologia 2019, 62, 3–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, X.R.; Li, G.W.; Hu, Y.H.; Wang, J.X.; Yang, W.Y.; An, Z.X.; Hu, Z.X.; Lin, J.; Xiao, J.Z.; Cao, H.B.; et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care 1997, 20, 537–544. [Google Scholar] [CrossRef] [PubMed]
- The Diabetes Prevention Program (DPP). Description of lifestyle intervention. Diabetes Care 2002, 25, 2165–2171. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Standards of medical care in diabetes—2015 abridged for primary care providers. Clin. Diabetes 2015, 33, 97–111. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 14. Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S165–S172. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association; Bantle, J.P.; Wylie-Rosett, J.; Albright, A.L.; Apovian, C.M.; Clark, N.G.; Franz, M.J.; Hoogwerf, B.J.; Lichtenstein, A.H.; Mayer-Davis, E.; et al. Nutrition recommendations and interventions for diabetes: A position statement of the American Diabetes Association. Diabetes Care 2008, 31 (Suppl. 1), S61–S78. [Google Scholar] [CrossRef] [Green Version]
- Ajala, O.; English, P.; Pinkney, J. Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes. Am. J. Clin. Nutr. 2013, 97, 505–516. [Google Scholar] [CrossRef] [Green Version]
- Brand-Miller, J.; Hayne, S.; Petocz, P.; Colagiuri, S. Low-glycemic index diets in the management of diabetes: A meta-analysis of randomized controlled trials. Diabetes Care 2003, 26, 2261–2267. [Google Scholar] [CrossRef] [Green Version]
- Esposito, K.; Maiorino, M.I.; Ceriello, A.; Giugliano, D. Prevention and control of type 2 diabetes by Mediterranean diet: A systematic review. Diabetes Res. Clin. Pract. 2010, 89, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, J.Z.; Day, A.; Brinkworth, G.D.; Sato, J.; Yamada, S.; Jonsson, T.; Beardsley, J.; Johnson, J.A.; Thabane, L.; Johnston, B.C. Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission: Systematic review and meta-analysis of published and unpublished randomized trial data. BMJ 2021, 372, m4743. [Google Scholar] [CrossRef] [PubMed]
- Alarim, R.A.; Alasmre, F.A.; Alotaibi, H.A.; Alshehri, M.A.; Hussain, S.A. Effects of the Ketogenic Diet on Glycemic Control in Diabetic Patients: Meta-Analysis of Clinical Trials. Cureus 2020, 12, e10796. [Google Scholar] [CrossRef] [PubMed]
- Carter, P.; Achana, F.; Troughton, J.; Gray, L.J.; Khunti, K.; Davies, M.J. A Mediterranean diet improves HbA1c but not fasting blood glucose compared to alternative dietary strategies: A network meta-analysis. J. Hum. Nutr. Diet. 2014, 27, 280–297. [Google Scholar] [CrossRef] [Green Version]
- Emadian, A.; Andrews, R.C.; England, C.Y.; Wallace, V.; Thompson, J.L. The effect of macronutrients on glycaemic control: A systematic review of dietary randomised controlled trials in overweight and obese adults with type 2 diabetes in which there was no difference in weight loss between treatment groups. Br. J. Nutr. 2015, 114, 1656–1666. [Google Scholar] [CrossRef] [Green Version]
- Paoli, A.; Rubini, A.; Volek, J.S.; Grimaldi, K.A. Beyond weight loss: A review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur. J. Clin. Nutr. 2013, 67, 789–796. [Google Scholar] [CrossRef] [Green Version]
- Zimorovat, A.; Mohammadi, M.; Ramezani-Jolfaie, N.; Salehi-Abargouei, A. The healthy Nordic diet for blood glucose control: A systematic review and meta-analysis of randomized controlled clinical trials. Acta Diabetol. 2020, 57, 1–12. [Google Scholar] [CrossRef]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S.; et al. Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report. Diabetes Care 2019, 42, 731–754. [Google Scholar] [CrossRef] [Green Version]
- Schulze, M.B.; Martinez-Gonzalez, M.A.; Fung, T.T.; Lichtenstein, A.H.; Forouhi, N.G. Food based dietary patterns and chronic disease prevention. BMJ 2018, 361, k2396. [Google Scholar] [CrossRef] [Green Version]
- Leucht, S.; Chaimani, A.; Cipriani, A.S.; Davis, J.M.; Furukawa, T.A.; Salanti, G. Network meta-analyses should be the highest level of evidence in treatment guidelines. Eur. Arch. Psychiatry Clin. Neurosci. 2016, 266, 477–480. [Google Scholar] [CrossRef] [Green Version]
- Mavridis, D.; Giannatsi, M.; Cipriani, A.; Salanti, G. A primer on network meta-analysis with emphasis on mental health. Evid.-Based Ment. Health 2015, 18, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Buyken, A.; Chaimani, A. Network meta-analysis reaches nutrition research. Eur. J. Nutr. 2019, 58, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Schwarzer, G.; Rucker, G.; Meerpohl, J.J. Perspective: Network Meta-analysis Reaches Nutrition Research: Current Status, Scientific Concepts, and Future Directions. Adv. Nutr. 2019, 10, 739–754. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Chaimani, A.; Hoffmann, G.; Schwedhelm, C.; Boeing, H. A network meta-analysis on the comparative efficacy of different dietary approaches on glycaemic control in patients with type 2 diabetes mellitus. Eur. J. Epidemiol. 2018, 33, 157–170. [Google Scholar] [CrossRef] [Green Version]
- Pan, B.; Wu, Y.; Yang, Q.; Ge, L.; Gao, C.; Xun, Y.; Tian, J.; Ding, G. The impact of major dietary patterns on glycemic control, cardiovascular risk factors, and weight loss in patients with type 2 diabetes: A network meta-analysis. J. Evid. Based Med. 2019, 12, 29–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonekamp, N.E.; van Damme, I.; Geleijnse, J.M.; Winkels, R.M.; Visseren, F.L.J.; Morris, P.B.; Koopal, C. Effect of dietary patterns on cardiovascular risk factors in people with type 2 diabetes. A systematic review and network meta-analysis. Diabetes Res. Clin. Pract. 2023, 195, 110207. [Google Scholar] [CrossRef]
- Zeng, B.T.; Pan, H.Q.; Li, F.D.; Ye, Z.Y.; Liu, Y.; Du, J.W. Comparative efficacy of different eating patterns in the management of type 2 diabetes and prediabetes: An arm-based Bayesian network meta-analysis. J. Diabetes Investig. 2023, 14, 263–288. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Chaimani, A.; Caldwell, D.M.; Li, T.; Higgins, J.P.T.; Salanti, G. Additional considerations are required when preparing a protocol for a systematic review with multiple interventions. J. Clin. Epidemiol. 2017, 83, 65–74. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Comparison of effects of long-term low-fat vs high-fat diets on blood lipid levels in overweight or obese patients: A systematic review and meta-analysis. J. Acad. Nutr. Diet. 2013, 113, 1640–1661. [Google Scholar] [CrossRef]
- Choi, Y.J.; Jeon, S.-M.; Shin, S. Impact of a ketogenic diet on metabolic parameters in patients with obesity or overweight and with or without type 2 diabetes: A meta-analysis of randomized controlled trials. Nutrients 2020, 12, 2005. [Google Scholar] [CrossRef]
- Clifton, P.M.; Keogh, J. Metabolic effects of high-protein diets. Curr. Atheroscler. Rep. 2007, 9, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health Benefits of the Mediterranean Diet: Metabolic and Molecular Mechanisms. J. Gerontol. 2018, 73, 318–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonsson, T.; Granfeldt, Y.; Ahren, B.; Branell, U.C.; Palsson, G.; Hansson, A.; Soderstrom, M.; Lindeberg, S. Beneficial effects of a Paleolithic diet on cardiovascular risk factors in type 2 diabetes: A randomized cross-over pilot study. Cardiovasc. Diabetol. 2009, 8, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M. A clinical trial of the effects of dietary patterns on blood pressure. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haider, L.M.; Schwingshackl, L.; Hoffmann, G.; Ekmekcioglu, C. The effect of vegetarian diets on iron status in adults: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2017, 58, 1359–1374. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hobl, L.P.; Hoffmann, G. Effects of low glycaemic index/low glycaemic load vs. high glycaemic index/ high glycaemic load diets on overweight/obesity and associated risk factors in children and adolescents: A systematic review and meta-analysis. Nutr. J. 2015, 14, 87. [Google Scholar] [CrossRef] [Green Version]
- Chiavaroli, L.; Nishi, S.K.; Khan, T.A.; Braunstein, C.R.; Glenn, A.J.; Mejia, S.B.; Rahelić, D.; Kahleová, H.; Salas-Salvadó, J.; Jenkins, D.J.A.; et al. Portfolio Dietary Pattern and Cardiovascular Disease: A Systematic Review and Meta-analysis of Controlled Trials. Prog. Cardiovasc. Dis. 2018, 61, 43–53. [Google Scholar] [CrossRef]
- Franz, M.J.; Bantle, J.P.; Beebe, C.A.; Brunzell, J.D.; Chiasson, J.L.; Garg, A.; Holzmeister, L.A.; Hoogwerf, B.; Mayer-Davis, E.; Mooradian, A.D.; et al. Evidence-based nutrition principles and recommendations for the treatment and prevention of diabetes and related complications. Diabetes Care 2002, 25, 148–198. [Google Scholar] [CrossRef] [Green Version]
- Mann, J.; De Leeuw, I.; Hermansen, K.; Karamanos, B.; Karlström, B.; Katsilambros, N.; Riccardi, G.; Rivellese, A.; Rizkalla, S.; Slama, G. Diabetes and Nutrition Study Group (DNSG) of the European Association. Evidence-based nutritional approaches to the treatment and prevention of diabetes mellitus. Nutr. Metab. Cardiovasc. Dis.—NMCD 2004, 14, 373–394. [Google Scholar] [CrossRef]
- National Institutes of Health. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report; National Heart, Lung, and Blood Institute: Bethesda, MD, USA, 1998. [Google Scholar]
- Evert, A.B.; Boucher, J.L.; Cypress, M.; Dunbar, S.A.; Franz, M.J.; Mayer-Davis, E.J.; Neumiller, J.J.; Nwankwo, R.; Verdi, C.L.; Urbanski, P.; et al. Nutrition therapy recommendations for the management of adults with diabetes. Diabetes Care 2014, 37 (Suppl. 1), S120–S143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rock, C.L.; Flatt, S.W.; Pakiz, B.; Taylor, K.S.; Leone, A.F.; Brelje, K.; Heath, D.D.; Quintana, E.L.; Sherwood, N.E. Weight loss, glycemic control, and cardiovascular disease risk factors in response to differential diet composition in a weight loss program in type 2 diabetes: A randomized controlled trial. Diabetes Care 2014, 37, 1573–1580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Sterne, J.A.; Savovic, J.; Page, M.J.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst. Rev. 2016, 10, 29–31. [Google Scholar]
- Higgins, J.P. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011; Available online: www.cochrane-handbook.org (accessed on 1 August 2022).
- White, I.R. Network meta-analysis. Stata J. 2015, 15, 951–985. [Google Scholar] [CrossRef] [Green Version]
- Chaimani, A.; Salanti, G. Visualizing assumptions and results in network meta-analysis: The network graphs package. Stata J. 2015, 15, 905–950. [Google Scholar] [CrossRef] [Green Version]
- Chaimani, A.; Higgins, J.P.; Mavridis, D.; Spyridonos, P.; Salanti, G. Graphical tools for network meta-analysis in STATA. PLoS ONE 2013, 8, e76654. [Google Scholar] [CrossRef] [Green Version]
- Dias, S.; Welton, N.J.; Caldwell, D.; Ades, A.E. Checking consistency in mixed treatment comparison meta-analysis. Stat. Med. 2010, 29, 932–944. [Google Scholar] [CrossRef]
- Harbord, R.M.; Egger, M.; Sterne, J.A. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat. Med. 2006, 25, 3443–3457. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Nikolakopoulou, A.; Higgins, J.P.T.; Papakonstantinou, T.; Chaimani, A.; Del Giovane, C.; Egger, M.; Salanti, G. CINeMA: An approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 2020, 17, e1003082. [Google Scholar] [CrossRef] [Green Version]
- Uusitupa, M.; Laitinen, J.; Siitonen, O.; Vanninen, E.; Pyörälä, K. The maintenance of improved metabolic control after intensified diet therapy in recent type 2 diabetes. Diabetes Res. Clin. Pract. 1993, 19, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Milne, R.M.; Mann, J.I.; Chisholm, A.W.; Williams, S.M. Long-term comparison of three dietary prescriptions in the treatment of NIDDM. Diabetes Care 1994, 17, 74–80. [Google Scholar] [CrossRef]
- Brinkworth, G.D.; Noakes, M.; Parker, B.; Foster, P.; Clifton, P.M. Long-term effects of advice to consume a high-protein, low-fat diet, rather than a conventional weight-loss diet, in obese adults with type 2 diabetes: One-year follow-up of a randomised trial. Diabetologia 2004, 47, 1677–1686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Olendzki, B.C.; Merriam, P.A.; Chiriboga, D.E.; Culver, A.L.; Li, W.; Hebert, J.R.; Ockene, I.S.; Griffith, J.A.; Pagoto, S.L. A randomized clinical trial comparing low-glycemic index versus ADA dietary education among individuals with type 2 diabetes. Nutrition 2008, 24, 45–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westman, E.C.; Yancy Jr, W.S.; Mavropoulos, J.C.; Marquart, M.; McDuffie, J.R. The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in type 2 diabetes mellitus. Nutr. Metab. 2008, 5, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolever, T.M.; Gibbs, A.L.; Mehling, C.; Chiasson, J.L.; Connelly, P.W.; Josse, R.G.; Leiter, L.A.; Maheux, P.; Rabasa-Lhoret, R.; Rodger, N.W.; et al. The Canadian Trial of Carbohydrates in Diabetes (CCD), a 1-y controlled trial of low-glycemic-index dietary carbohydrate in type 2 diabetes: No effect on glycated hemoglobin but reduction in C-reactive protein. Am. J. Clin. Nutr. 2008, 87, 114–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnard, N.D.; Cohen, J.; Jenkins, D.J.A.; Turner-McGrievy, G.; Gloede, L.; Green, A.; Ferdowsian, H. A low-fat vegan diet and a conventional diabetes diet in the treatment of type 2 diabetes: A randomized, controlled, 74-wk clinical trial. Am. J. Clin. Nutr. 2009, 89, S1588–S1596. [Google Scholar] [CrossRef] [Green Version]
- Brehm, B.J.; Lattin, B.L.; Summer, S.S.; Boback, J.A.; Gilchrist, G.M.; Jandacek, R.J.; D’alessio, D.A. One-year comparison of a high–monounsaturated fat diet with a high-carbohydrate diet in type 2 diabetes. Diabetes Care 2009, 32, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Davis, N.J.; Tomuta, N.; Schechter, C.; Isasi, C.R.; Segal-Isaacson, C.J.; Stein, D.; Zonszein, J.; Wylie-Rosett, J. Comparative study of the effects of a 1-year dietary intervention of a low-carbohydrate diet versus a low-fat diet on weight and glycemic control in type 2 diabetes. Diabetes Care 2009, 32, 1147–1152. [Google Scholar] [CrossRef] [Green Version]
- Esposito, K.; Maiorino, M.I.; Ciotola, M.; Di Palo, C.; Scognamiglio, P.; Gicchino, M.; Petrizzo, M.; Saccomanno, F.; Beneduce, F.; Ceriello, A.; et al. Effects of a Mediterranean-style diet on the need for antihyperglycemic drug therapy in patients with newly diagnosed type 2 diabetes: A randomized trial. Ann. Intern. Med. 2009, 151, 306–314. [Google Scholar] [CrossRef]
- Neelima, G.R.; Chandrakala, G.; Arpana, G.; Jain, A.K.; Rao, P.V. Long-term (3-year) effects of a reduced-fat diet in type 2 diabetes. Diabetes 2009, 58, A45. [Google Scholar]
- Coppell, K.J.; Kataoka, M.; Williams, S.M.; Chisholm, A.W.; Vorgers, S.M.; Mann, J.I. Nutritional intervention in patients with type 2 diabetes who are hyperglycaemic despite optimised drug treatment—Lifestyle Over and Above Drugs in Diabetes (LOADD) study: Randomised controlled trial. BMJ 2010, 341, c3337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elhayany, A.; Lustman, A.; Abel, R.; Attal-Singer, J.; Vinker, S. A low carbohydrate Mediterranean diet improves cardiovascular risk factors and diabetes control among overweight patients with type 2 diabetes mellitus: A 1-year prospective randomized intervention study. Diabetes Obes. Metab. 2010, 12, 204–209. [Google Scholar] [CrossRef]
- Huang, M.; Hsu, C.; Wang, H.; Shin, S. Prospective randomized controlled trial to evaluate effectiveness of registered dietitian–led diabetes management on glycemic and diet control in a primary care setting in Taiwan. Diabetes Care 2010, 33, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, N.; Vetter, M.L.; Moore, R.H.; Chittams, J.L.; Dalton-Bakes, C.V.; Dowd, M.; Williams-Smith, C.; Cardillo, S.; Wadden, T.A. Effects of a low-intensity intervention that prescribed a low-carbohydrate vs. a low-fat diet in obese, diabetic participants. Obesity 2010, 18, 1733–1738. [Google Scholar] [CrossRef]
- Andrews, R.; Cooper, A.; Montgomery, A.; Norcross, A.J.; Peters, T.; Sharp, D.; Jackson, N.; Fitzsimons, K.; Bright, J.; Coulman, K. Diet or diet plus physical activity versus usual care in patients with newly diagnosed type 2 diabetes: The Early ACTID randomised controlled trial. Lancet 2011, 378, 129–139. [Google Scholar] [CrossRef] [Green Version]
- Fabricatore, A.N.; Wadden, T.A.; Ebbeling, C.B.; Thomas, J.G.; Stallings, V.A.; Schwartz, S.; Ludwig, D.S. Targeting dietary fat or glycemic load in the treatment of obesity and type 2 diabetes: A randomized controlled trial. Diabetes Res. Clin. Pract. 2011, 92, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, T.; Kark, J.D.; Berry, E.M.; Adler, B.; Ziv, E.; Raz, I. The effect of a low carbohydrate energy-unrestricted diet on weight loss in obese type 2 diabetes patients–a randomized controlled trial. e-SPEN Eur. E-J. Clin. Nutr. Metab. 2011, 6, e178–e186. [Google Scholar] [CrossRef] [Green Version]
- Kahleova, H.; Matoulek, M.; Malinska, H.; Oliyarnik, O.; Kazdova, L.; Neskudla, T.; Skoch, A.; Hajek, M.; Hill, M.; Kahle, M.; et al. Vegetarian diet improves insulin resistance and oxidative stress markers more than conventional diet in subjects with Type 2 diabetes. Diabet. Med. 2011, 28, 549–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nystrom, F.; Ostgren, C.; Lindstrom, T.; Bachrach-Lindstrom, M.; Schold, A.-K.; Dizdar, B.; Fredrikson, M.; Guldbrand, H. A high fat diet improves glycaemic control compared with low fat diet: A 24-month randomised prospective study of patients with type 2 diabetes in primary health care. Diabetologia 2011, 54, S358. [Google Scholar]
- Guldbrand, H.; Dizdar, B.; Bunjaku, B.; Lindstrom, T.; Bachrach-Lindstrom, M.; Fredrikson, M.; Ostgren, C.J.; Nystrom, F.H. In type 2 diabetes, randomisation to advice to follow a low-carbohydrate diet transiently improves glycaemic control compared with advice to follow a low-fat diet producing a similar weight loss. Diabetologia 2012, 55, 2118–2127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebs, J.D.; Elley, C.R.; Parry-Strong, A.; Lunt, H.; Drury, P.L.; Bell, D.A.; Robinson, E.; Moyes, S.A.; Mann, J.I. The Diabetes Excess Weight Loss (DEWL) Trial: A randomised controlled trial of high-protein versus high-carbohydrate diets over 2 years in type 2 diabetes. Diabetologia 2012, 55, 905–914. [Google Scholar] [CrossRef] [Green Version]
- Timar, R.; Timar, B.; Horhat, F.; Oancea, C. The impact of Mediterranean diet on glycemic control and cardiovascular risk factors in type 2 diabetic patients. J. Food Agric. Environ. 2013, 11, 561–563. [Google Scholar]
- Lasa, A.; Miranda, J.; Bullo, M.; Casas, R.; Salas-Salvado, J.; Larretxi, I.; Estruch, R.; Ruiz-Gutierrez, V.; Portillo, M.P. Comparative effect of two Mediterranean diets versus a low-fat diet on glycaemic control in individuals with type 2 diabetes. Eur. J. Clin. Nutr. 2014, 68, 767–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, E.; Jesudason, D.R.; Clifton, P.M. High protein weight loss diets in obese subjects with type 2 diabetes mellitus. Nutr. Metab. Cardiovasc. Dis.—NMCD 2014, 24, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Tay, J.; Luscombe-Marsh, N.; Thompson, C.; Noakes, M.; Buckley, J.; Wittert, G.; Yancy, W., Jr.; Brinkworth, G. Long-term effects of a low carbohydrate, low saturated fat diet versus a conventional high carbohydrate, low fat diet in type 2 diabetes: A randomised trial. Diabetes Res. Clin. Pract. 2014, 106, S34. [Google Scholar] [CrossRef]
- Yamada, Y.; Uchida, J.; Izumi, H.; Tsukamoto, Y.; Inoue, G.; Watanabe, Y.; Irie, J.; Yamada, S. A non-calorie-restricted low-carbohydrate diet is effective as an alternative therapy for patients with type 2 diabetes. Intern. Med. 2014, 53, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Bahado-Singh, P.S.; Riley, C.K.; Wheatley, A.O.; Boyne, M.S.; Morrison, E.Y.; Asemota, H.N. High Fiber Caribbean Diets with Low-Intermediate GI Improve Glycemic Control, Cardiovascular and Inflammatory Indicators in Overweight Persons with Type 2 Diabetes: A Randomized Control Study. Curr. Res. Nutr. Food Sci. 2015, 3, 36–45. [Google Scholar] [CrossRef]
- Liu, H.; Zhang, M.; Wu, X.; Wang, C.; Li, Z. Effectiveness of a public dietitian-led diabetes nutrition intervention on glycemic control in a community setting in China. Asia Pac. J. Clin. Nutr. 2015, 24, 525–532. [Google Scholar] [CrossRef]
- Watson, N.; Dyer, K.; Buckley, J.; Brinkworth, G.; Coates, A.; Parfitt, G.; Howe, P.; Noakes, M.; Murphy, K. Effects of Low-Fat Diets Differing in Protein and Carbohydrate Content on Cardiometabolic Risk Factors during Weight Loss and Weight Maintenance in Obese Adults with Type 2 Diabetes. Nutrients 2016, 8, 289. [Google Scholar] [CrossRef] [Green Version]
- Wycherley, T.P.; Thompson, C.H.; Buckley, J.D.; Luscombe-Marsh, N.D.; Noakes, M.; Wittert, G.A.; Brinkworth, G.D. Long-term effects of weight loss with a very-low carbohydrate, low saturated fat diet on flow mediated dilatation in patients with type 2 diabetes: A randomised controlled trial. Atherosclerosis 2016, 252, 28–31. [Google Scholar] [CrossRef] [Green Version]
- Maiorino, M.I.; Bellastella, G.; Petrizzo, M.; Gicchino, M.; Caputo, M.; Giugliano, D.; Esposito, K. Effect of a Mediterranean diet on endothelial progenitor cells and carotid intima-media thickness in type 2 diabetes: Follow-up of a randomized trial. Eur. J. Prev. Cardiol. 2017, 24, 399–408. [Google Scholar] [CrossRef]
- Sato, J.; Kanazawa, A.; Makita, S.; Hatae, C.; Komiya, K.; Shimizu, T.; Ikeda, F.; Tamura, Y.; Ogihara, T.; Mita, T.; et al. A randomized controlled trial of 130 g/day low-carbohydrate diet in type 2 diabetes with poor glycemic control. Clin. Nutr. 2017, 36, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Pavithran, N.; Kumar, H.; Menon, A.; Ragasudha, P.; Pillai, M.; Sundaram, K. 24-Week, Low GI Diet Decreases Truncal Fat Mass In South Indians With Type 2 Diabetes: A Randomized Study. Clin. Nutr. 2019, 38, S222. [Google Scholar] [CrossRef]
- Chen, C.Y.; Huang, W.S.; Chen, H.C.; Chang, C.H.; Lee, L.T.; Chen, H.S.; Kang, Y.D.; Chie, W.C.; Jan, C.F.; Wang, W.D.; et al. Effect of a 90 g/day low-carbohydrate diet on glycaemic control, small, dense low-density lipoprotein and carotid intima-media thickness in type 2 diabetic patients: An 18-month randomised controlled trial. PLoS ONE 2020, 15, e0240158. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Mariscal, F.M.; Cardelo, M.P.; de la Cruz, S.; Alcala-Diaz, J.F.; Roncero-Ramos, I.; Guler, I.; Vals-Delgado, C.; Lopez-Moreno, A.; Luque, R.M.; Delgado-Lista, J.; et al. Reduction in Circulating Advanced Glycation End Products by Mediterranean Diet is Associated with Increased Likelihood of type 2 Diabetes Remission in Patients with Coronary Heart Disease: From the Cordioprev Study. Mol. Nutr. Food Res. 2021, 65, e1901290. [Google Scholar] [CrossRef]
- Marco-Benedi, V.; Perez-Calahorra, S.; Bea, A.M.; Lamiquiz-Moneo, I.; Baila-Rueda, L.; Cenarro, A.; Civeira, F.; Mateo-Gallego, R. High-protein energy-restricted diets induce greater improvement in glucose homeostasis but not in adipokines comparing to standard-protein diets in early-onset diabetic adults with overweight or obesity. Clin. Nutr. 2020, 39, 1354–1363. [Google Scholar] [CrossRef]
- Pavithran, N.; Kumar, H.; Menon, A.S.; Pillai, G.K.; Sundaram, K.R.; Ojo, O. The Effect of a Low GI Diet on Truncal Fat Mass and Glycated Hemoglobin in South Indians with Type 2 Diabetes-A Single Centre Randomized Prospective Study. Nutrients 2020, 12, 179. [Google Scholar] [CrossRef] [Green Version]
- Kakoschke, N.; Zajac, I.T.; Tay, J.; Luscombe-Marsh, N.D.; Thompson, C.H.; Noakes, M.; Buckley, J.D.; Wittert, G.; Brinkworth, G.D. Effects of very low-carbohydrate vs. high-carbohydrate weight loss diets on psychological health in adults with obesity and type 2 diabetes: A 2-year randomized controlled trial. Eur. J. Nutr. 2021, 60, 4251–4262. [Google Scholar] [CrossRef]
- Zahedi, M.; Akhlagh, S.A.; Aboomardani, M.; Alipoor, R.; Hosseini, S.A.; Shahmirzadi, A.R. Efficacy of mediterranean diet on blood biochemical factors in type II diabetic patients: A randomized controlled trial. Gazi Med. J. 2021, 31, 714–718. [Google Scholar] [CrossRef]
- Gram-Kampmann, E.M.; Hansen, C.D.; Hugger, M.B.; Jensen, J.M.; Brønd, J.C.; Hermann, A.P.; Krag, A.; Olsen, M.H.; Beck-Nielsen, H.; Højlund, K. Effects of a 6-month, low-carbohydrate diet on glycaemic control, body composition, and cardiovascular risk factors in patients with type 2 diabetes: An open-label randomized controlled trial. Diabetes Obes. Metab. 2022, 24, 693–703. [Google Scholar] [CrossRef]
- Salanti, G.; Del Giovane, C.; Chaimani, A.; Caldwell, D.M.; Higgins, J.P. Evaluating the quality of evidence from a network meta-analysis. PLoS ONE 2014, 9, e99682. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Wang, M.; Liang, J.; He, G.; Chen, N. Ketogenic Diet Benefits to Weight Loss, Glycemic Control, and Lipid Profiles in Overweight Patients with Type 2 Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trails. Int. J. Environ. Res. Public Health 2022, 19, 10429. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Xia, W.; Zhao, Z.; Zhang, H. Effects comparison between low glycemic index diets and high glycemic index diets on HbA1c and fructosamine for patients with diabetes: A systematic review and meta-analysis. Prim. Care Diabetes 2015, 9, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Huo, R.; Du, T.; Xu, Y.; Xu, W.; Chen, X.; Sun, K.; Yu, X. Effects of Mediterranean-style diet on glycemic control, weight loss and cardiovascular risk factors among type 2 diabetes individuals: A meta-analysis. Eur. J. Clin. Nutr. 2015, 69, 1200–1208. [Google Scholar] [CrossRef]
- O’Neill, B.J. Effect of low-carbohydrate diets on cardiometabolic risk, insulin resistance, and metabolic syndrome. Curr. Opin. Endocrinol. Diabetes Obes. 2020, 27, 301–307. [Google Scholar] [CrossRef]
- Kumar, S.; Behl, T.; Sachdeva, M.; Sehgal, A.; Kumari, S.; Kumar, A.; Kaur, G.; Yadav, H.N.; Bungau, S. Implicating the effect of ketogenic diet as a preventive measure to obesity and diabetes mellitus. Life Sci. 2021, 264, 118661. [Google Scholar] [CrossRef]
- Qian, F.; Korat, A.A.; Malik, V.; Hu, F.B. Metabolic effects of monounsaturated fatty acid–enriched diets compared with carbohydrate or polyunsaturated fatty acid–enriched diets in patients with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Diabetes Care 2016, 39, 1448–1457. [Google Scholar] [CrossRef] [Green Version]
- Chandalia, M.; Garg, A.; Lutjohann, D.; Von Bergmann, K.; Grundy, S.M.; Brinkley, L.J. Beneficial effects of high dietary fiber intake in patients with type 2 diabetes mellitus. N. Engl. J. Med. 2000, 342, 1392–1398. [Google Scholar] [CrossRef]
- Churuangsuk, C.; Kherouf, M.; Combet, E.; Lean, M. Low-carbohydrate diets for overweight and obesity: A systematic review of the systematic reviews. Obes. Rev. 2018, 19, 1700–1718. [Google Scholar] [CrossRef] [Green Version]
- Stumvoll, M.; Goldstein, B.J.; van Haeften, T.W. Type 2 diabetes: Principles of pathogenesis and therapy. Lancet 2005, 365, 1333–1346. [Google Scholar] [CrossRef]
- Bolla, A.M.; Caretto, A.; Laurenzi, A.; Scavini, M.; Piemonti, L. Low-Carb and Ketogenic Diets in Type 1 and Type 2 Diabetes. Nutrients 2019, 11, 962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Hoffmann, G. Long-term effects of low glycemic index/load vs. high glycemic index/load diets on parameters of obesity and obesity-associated risks: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis.—NMCD 2013, 23, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Wang, J.; Yang, S.; Gao, M.; Cao, L.; Li, X.; Hong, D.; Tian, S.; Sun, C. Effect of the ketogenic diet on glycemic control, insulin resistance, and lipid metabolism in patients with T2DM: A systematic review and meta-analysis. Nutr. Diabetes 2020, 10, 38. [Google Scholar] [CrossRef] [PubMed]
- Manheimer, E.W.; van Zuuren, E.J.; Fedorowicz, Z.; Pijl, H. Paleolithic nutrition for metabolic syndrome: Systematic review and meta-analysis. Am. J. Clin. Nutr. 2015, 102, 922–932. [Google Scholar] [CrossRef] [Green Version]
- Caprio, M.; Infante, M.; Moriconi, E.; Armani, A.; Fabbri, A.; Mantovani, G.; Mariani, S.; Lubrano, C.; Poggiogalle, E.; Migliaccio, S.; et al. Very-low-calorie ketogenic diet (VLCKD) in the management of metabolic diseases: Systematic review and consensus statement from the Italian Society of Endocrinology (SIE). J. Endocrinol. Investig. 2019, 42, 1365–1386. [Google Scholar] [CrossRef]
- Paoli, A.; Bianco, A.; Grimaldi, K.A.; Lodi, A.; Bosco, G. Long term successful weight loss with a combination biphasic ketogenic Mediterranean diet and Mediterranean diet maintenance protocol. Nutrients 2013, 5, 5205–5217. [Google Scholar] [CrossRef]
- Pan, B.; Ge, L.; Xun, Y.Q.; Chen, Y.J.; Gao, C.Y.; Han, X.; Zuo, L.Q.; Shan, H.Q.; Yang, K.H.; Ding, G.W.; et al. Exercise training modalities in patients with type 2 diabetes mellitus: A systematic review and network meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 72. [Google Scholar] [CrossRef] [Green Version]
- de Bont, A.J.; Baker, I.A.; St Leger, A.S.; Sweetnam, P.M.; Wragg, K.G.; Stephens, S.M.; Hayes, T.M. A randomised controlled trial of the effect of low fat diet advice on dietary response in insulin independent diabetic women. Diabetologia 1981, 21, 529–533. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, J.V.; Jönsson, E.; Nilsson, A.K. Lasting improvement of hyperglycaemia and bodyweight: Low-carbohydrate diet in type 2 diabetes. A brief report. Ups. J. Med. Sci. 2005, 110, 179–183. [Google Scholar] [CrossRef]
- Fraser, A.; Abel, R.; Lawlor, D.A.; Fraser, D.; Elhayany, A. A modified Mediterranean diet is associated with the greatest reduction in alanine aminotransferase levels in obese type 2 diabetes patients: Results of a quasi-randomised controlled trial. Diabetologia 2008, 51, 1616–1622. [Google Scholar] [CrossRef] [Green Version]
- Wolever, T.M.S.; Mehling, C.; Chiasson, J.L.; Josse, R.G.; Leiter, L.A.; Maheux, P.; Rabasa-Lhoret, R.; Rodger, N.W.; Ryan, E.A. Low glycaemic index diet and disposition index in type 2 diabetes (the Canadian trial of Carbohydrates in Diabetes): A randomised controlled trial. Diabetologia 2008, 51, 1607–1615. [Google Scholar] [CrossRef] [Green Version]
- Haimoto, H.; Iwata, M.; Wakai, K.; Umegaki, H. Long-term effects of a diet loosely restricting carbohydrates on HbA1c levels, BMI and tapering of sulfonylureas in type 2 diabetes: A 2-year follow-up study. Diabetes Res. Clin. Pract. 2008, 79, 350–356. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Kendall, C.W.; McKeown-Eyssen, G.; Josse, R.G.; Silverberg, J.; Booth, G.L.; Vidgen, E.; Josse, A.R.; Nguyen, T.H.; Corrigan, S.; et al. Effect of a low-glycemic index or a high-cereal fiber diet on type 2 diabetes: A randomized trial. JAMA 2008, 300, 2742–2753. [Google Scholar] [CrossRef] [Green Version]
- Haimoto, H.; Sasakabe, T.; Wakai, K.; Umegaki, H. Effects of a low-carbohydrate diet on glycemic control in outpatients with severe type 2 diabetes. Nutr. Metab. 2009, 6, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Moses, R.G.; Barker, M.; Winter, M.; Petocz, P.; Brand-Miller, J.C. Can a low-glycemic index diet reduce the need for insulin in gestational diabetes mellitus? A randomized trial. Diabetes Care 2009, 32, 996–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner-McGrievy, G.M.; Barnard, N.; Jenkins, D.; Cohen, J.; Gloede, L.; Green, A. Relation of the Glycemic Index with Body Weight and Glycemic Control Among Participants with Type 2 Diabetes Following a Low-Fat Vegan Diet or a Conventional Diabetes Diet for 22 Weeks. In Proceedings of the 27th Annual Scientific Meeting of the Obesity-Society, Washington, DC, USA, 24–28 October 2009; p. S131. [Google Scholar]
- Cao, A.; Sun, L.; Cui, J. Effects of A Low-Carbohydrate Diet and A Low-Fat Diet on Weight and Glycemic Control in Type 2 Diabetics Mellitus. Chin. Gen. Prac. 2011, 14, 52–53, 56. [Google Scholar] [CrossRef]
- Larsen, R.N.; Mann, N.J.; Maclean, E.; Shaw, J.E. The effect of high-protein, low-carbohydrate diets in the treatment of type 2 diabetes: A 12 month randomised controlled trial. Diabetologia 2011, 54, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Shyam, S.; Arshad, F.; Nisak, M.Y.B.; Safie, N.S.; Kamaruddin, N.A.; Abdul Ghani, R.; Abdul Wahab, N.A. Effect of low gi diet vs low fat diet on metabolic risk markers in women post gestational diabetes mellitus (PGDM): A preliminary finding. In Proceedings of the 4th International Congress on Prediabetes and the Metabolic Syndrome, Madrid, Spain, 6–9 April 2011; p. 87. [Google Scholar]
- Krebs, J.D.; Elley, C.R.; Parry-Strong, A.; Lunt, H.; Drury, P.L.; Bell, D.A.; Robinson, E.; Moyes, S.A.; Mann, J. Two Year Randomised Controlled Trial of High-Protein Versus High-Carbohydrate Diet in Type 2 Diabetes: Diabetes Excess Weight Loss (DEWL). In Proceedings of the 71st Scientific Sessions of the American Diabetes Association, San Diego, CA, USA, 24–28 June 2011; p. A213. [Google Scholar]
- Tobias, D.K.; Hu, F.B.; Chavarro, J.; Rosner, B.; Mozaffarian, D.; Zhang, C. Healthful dietary patterns and type 2 diabetes mellitus risk among women with a history of gestational diabetes mellitus. Arch. Gerontol. Geriatr. 2012, 172, 1566–1572. [Google Scholar] [CrossRef] [Green Version]
- Davis, N.J.; Tomuta, N.; Isasi, C.R.; Leung, V.; Wylie-Rosett, J. Diabetes-specific quality of life after a low-carbohydrate and low-fat dietary intervention. Diabetes Educ. 2012, 38, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Jesudason, D.R.; Pedersen, E.; Clifton, P.M. Weight-loss diets in people with type 2 diabetes and renal disease: A randomized controlled trial of the effect of different dietary protein amounts. Am. J. Clin. Nutr. 2013, 98, 494–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shyam, S.; Arshad, F.; Abdul Ghani, R.; Wahab, N.A.; Safii, N.S.; Nisak, M.Y.B.; Chinna, K.; Kamaruddin, N.A. Low glycaemic index diets improve glucose tolerance and body weight in women with previous history of gestational diabetes: A six months randomized trial. Nutr. J. 2013, 12, 68. [Google Scholar] [CrossRef] [Green Version]
- Fernemark, H.; Jaredsson, C.; Bunjaku, B.; Rosenqvist, U.; Nystrom, F.H.; Guldbrand, H. A randomized cross-over trial of the postprandial effects of three different diets in patients with type 2 diabetes. PLoS ONE 2013, 8, e79324. [Google Scholar] [CrossRef]
- Shyam, S.; Arshad, F.; Ghani, R.A.; Wahab, N.A.; Mohd Yusof, B.N.; Safii, N.S.; Chinna, K.; Kamaruddin, N.A. Low glycaemic index diet aids management of fasting blood sugar and body weight in asian women with previous history of gestational diabetes mellitus. J. Diabetes 2013, 5 (Suppl. 1), 27. [Google Scholar] [CrossRef]
- Mayer, S.B.; Jeffreys, A.S.; Olsen, M.K.; McDuffie, J.R.; Feinglos, M.N.; Yancy, W.S., Jr. Two diets with different haemoglobin A1c and antiglycaemic medication effects despite similar weight loss in type 2 diabetes. Diabetes Obes. Metab. 2014, 16, 90–93. [Google Scholar] [CrossRef]
- Tay, J.; Luscombe-Marsh, N.D.; Thompson, C.H.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Yancy, W.S., Jr.; Brinkworth, G.D. A Very Low-Carbohydrate, Low-Saturated Fat Diet for Type 2 Diabetes Management: A Randomized Trial. Diabetes Care 2015, 37, 2909–2918. [Google Scholar] [CrossRef] [Green Version]
- Watson, N.A.; Dyer, K.A.; Buckley, J.D.; Brinkworth, G.D.; Coates, A.M.; Parfitt, G.; Howe, P.R.C.; Noakes, M.; Dye, L.; Chadwick, H.; et al. A randomised trial comparing low-fat diets differing in carbohydrate and protein ratio, combined with regular moderate intensity exercise, on glycaemic control, cardiometabolic risk factors, food cravings, cognitive function and psychological wellbeing in adults with type 2 diabetes: Study protocol. Contemp. Clin. Trials 2015, 45, 217–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louie, J.C.; Markovic, T.P.; Ross, G.P.; Foote, D.; Brand-Miller, J.C. Effect of a low glycaemic index diet in gestational diabetes mellitus on post-natal outcomes after 3 months of birth: A pilot follow-up study. Matern. Child. Nutr. 2015, 11, 409–414. [Google Scholar] [CrossRef]
- Tay, J.; Zajac, I.T.; Thompson, C.H.; Luscombe-Marsh, N.D.; Danthiir, V.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Brinkworth, G.D. A randomised-controlled trial of the effects of very low-carbohydrate and high-carbohydrate diets on cognitive performance in patients with type 2 diabetes. Br. J. Nutr. 2016, 23, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stentz, F.B.; Brewer, A.; Wan, J.; Garber, C.; Daniels, B.; Sands, C.; Kitabchi, A.E. Remission of pre-diabetes to normal glucose tolerance in obese adults with high protein versus high carbohydrate diet: Randomized control trial. BMJ Open Diabetes Res. Care 2016, 4, e000258. [Google Scholar] [CrossRef] [Green Version]
- Wolever, T.M.; Chiasson, J.L.; Josse, R.G.; Leiter, L.A.; Maheux, P.; Rabasa-Lhoret, R.; Rodger, N.W.; Ryan, E.A. Effects of Changing the Amount and Source of Dietary Carbohydrates on Symptoms and Dietary Satisfaction Over a 1-Year Period in Subjects with Type 2 Diabetes: Canadian Trial of Carbohydrates in Diabetes (CCD). Can. J. Diabetes 2017, 41, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Kahleova, H.; Klementova, M.; Herynek, V.; Skoch, A.; Herynek, S.; Hill, M.; Mari, A.; Pelikanova, T. The Effect of a Vegetarian vs Conventional Hypocaloric Diabetic Diet on Thigh Adipose Tissue Distribution in Subjects with Type 2 Diabetes: A Randomized Study. J. Am. Coll. Nutr. 2017, 36, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Crowley, M.J.; Edelman, D.; Voils, C.I.; Maciejewski, M.L.; Coffman, C.J.; Jeffreys, A.S.; Turner, M.J.; Gaillard, L.A.; Hinton, T.A.; Strawbridge, E.; et al. Jump starting shared medical appointments for diabetes with weight management: Rationale and design of a randomized controlled trial. Contemp. Clin. Trials 2017, 58, 1–12. [Google Scholar] [CrossRef]
- Marco-Benedi, M.V.; Perez Calahorra, S.; Bea Sanz, A.M.; Baila Rueda, L.; Lamiquiz Moneo, I.; Cenarro, A.; Civeira, F.; Mateo Gallego, R. A Randomized, Open-Label Study to Investigate the Effect of a High Protein Diet Compared to a Normoprotein Diet on Hydrocarbon Metabolism in Patients with Diabetes or Prediabetes and Obesity. Atherosclerosis 2017, 263, E263. [Google Scholar] [CrossRef]
- Beck-Nielsen, H. A Reduced-Carbohydrate Diet High in Monounsaturated Fats in Type 2 Diabetes. 2017. Available online: https://clinicaltrials.gov/show/NCT03068078 (accessed on 1 August 2022).
- Asle Mohammadi Zadeh, M.; Kargarfard, M.; Marandi, S.M.; Habibi, A. Diets along with interval training regimes improves inflammatory & anti-inflammatory condition in obesity with type 2 diabetes subjects. J. Diabetes Metab. Disord. 2018, 17, 253–267. [Google Scholar] [CrossRef]
- Tay, J.; Thompson, C.H.; Luscombe-Marsh, N.D.; Wycherley, T.P.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Yancy, W.S.; Brinkworth, G.D. Effects of an energy-restricted low-carbohydrate, high unsaturated fat/low saturated fat diet versus a high-carbohydrate, low-fat diet in type 2 diabetes: A 2-year randomized clinical trial. Diabetes Obes. Metab. 2018, 20, 858–871. [Google Scholar] [CrossRef]
- Torres-Peña, J.D.; Garcia-Rios, A.; Delgado-Casado, N.; Gomez-Luna, P.; Alcala-Diaz, J.F.; Yubero-Serrano, E.M.; Gomez-Delgado, F.; Leon-Acuña, A.; Lopez-Moreno, J.; Camargo, A.; et al. Mediterranean diet improves endothelial function in patients with diabetes and prediabetes: A report from the CORDIOPREV study. Atherosclerosis 2018, 269, 50–56. [Google Scholar] [CrossRef]
- Björklund, A. Comparison of Low, Moderate and High Carbohydrate Diet on Insulin Requirements and Metabolic Control in Type 1 Diabetes. 2018. Available online: https://clinicaltrials.gov/show/NCT03761186 (accessed on 1 August 2022).
- Mattei, J.; Bigornia, S.J.; Sotos-Prieto, M.; Scott, T.; Gao, X.; Tucker, K.L. The mediterranean diet and two-year changes in cognitive function in puerto rican adults with vs. Without Type 2 Diabetes. Diabetes 2018, 67 (Suppl. 1), 192-LB. [Google Scholar] [CrossRef]
- Crowder, C.M.; Jelley, D.; Condren, M.; Chalmers, L.; Graef, J.L. The T1dlocho study: Effects of a low-carbohydrate, nonketogenic diet vs. standard diabetes diet on glycemic control in young adults with type 1 diabetes. Diabetes 2019, 68. [Google Scholar] [CrossRef]
- Mason, A.E.; Saslow, L.R.; Moran, P.J.; Kim, S.; Abousleiman, H.; Richler, R.; Schleicher, S.; Goldman, V.M.; Hartman, A.; Leung, C.; et al. Lipid findings from the Diabetes Education to Lower Insulin, Sugars, and Hunger (DELISH) Study. Nutr. Metab. 2019, 16, 58. [Google Scholar] [CrossRef] [Green Version]
- Stentz, F. Pathobiology of Remission of Type 2 Diabetes. 2019. Available online: https://clinicaltrials.gov/show/NCT03832725 (accessed on 1 August 2022).
- Garbutt, J.D.W.; England, C.; Jones, A.G.; Andrews, R.C.; Johnson, L. Are changes in a low-carbohydrate, high-fat diet pattern associated with subsequent changes in HbA1c during an intensive diet and physical activity intervention? Diabet. Med. 2020, 37, 44. [Google Scholar] [CrossRef]
- Gram-Kampmann, E.M.; Hansen, C.D.; Hugger, M.B.; Jensen, J.M.; Brond, J.C.; Hermann, P.; Olsen, M.H.; Krag, A.; Beck-Nielsen, H.; Hojlund, K. Effects of a six-month low-carbohydrate diet in patients with type 2 diabetes on glycaemic control, body composition and cardiovascular risk factors. Diabetologia 2020, 63, S297. [Google Scholar] [CrossRef]
- Tucker, S.; Stentz, F. Effect of macronutrients on metabolic parameters and remission of type 2 diabetes. J. Investig. Med. 2020, 68, 656–657. [Google Scholar]
- Athinarayanan, S.J.; Hallberg, S.J.; McKenzie, A.L.; Lechner, K.; King, S.; McCarter, J.P.; Volek, J.S.; Phinney, S.D.; Krauss, R.M. Impact of a 2-year trial of nutritional ketosis on indices of cardiovascular disease risk in patients with type 2 diabetes. Cardiovasc. Diabetol. 2020, 19, 208. [Google Scholar] [CrossRef] [PubMed]
- Blindbaek, S.L.; Moller, D.M.; Gram-Kampmann, E.M.; Olsen, M.H.; Hojlund, K.; Grauslund, J. Changes in Retinal Microvasculature Parameters after Low-Carbohydrate, High-Fat Diet in Type 2 Diabetes: A Randomized-Controlled Trial of Danish Type 2 Diabetic Patients. Eur. J. Ophthalmol. 2020, 30, 30. [Google Scholar] [CrossRef]
- Kobayashi, M.; Miura, T.; Miura, K.; Hiroyama, N.; Akashi, K. Effect of a Moderate Carbohydrate-Restricted Diet on DPP-4 Inhibitor Action among Individuals with Type 2 Diabetes Mellitus: A 6-Month Intervention Study. J. Nutr. Sci. Vitaminol. 2020, 66, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Tay, J.; Thompson, C.H.; Luscombe-Marsh, N.D.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Brinkworth, G.D. Nutritional adequacy of very low- and high-carbohydrate, low saturated fat diets in adults with type 2 diabetes: A secondary analysis of a 2-year randomised controlled trial. Diabetes Res. Clin. Pract. 2020, 170, 108501. [Google Scholar] [CrossRef]
- Ren, M.; Zhang, H.; Qi, J.; Hu, A.; Jiang, Q.; Hou, Y.; Feng, Q.; Ojo, O.; Wang, X. An almond-based low carbohydrate diet improves depression and glycometabolism in patients with type 2 diabetes through modulating gut microbiota and glp-1: A randomized controlled trial. Nutrients 2020, 12, 3036. [Google Scholar] [CrossRef] [PubMed]
- Lawson, D.; Stentz, F. Myonectin is a marker of remission of type 2 diabetes in obese human subjects. J. Investig. Med. 2021, 69, 516. [Google Scholar]
- Buso, M.E.C.; Seimon, R.V.; McClintock, S.; Muirhead, R.; Atkinson, F.S.; Brodie, S.; Dodds, J.; Zibellini, J.; Das, A.; Wild-Taylor, A.L.; et al. Can a Higher Protein/Low Glycemic Index vs. a Conventional Diet Attenuate Changes in Appetite and Gut Hormones Following Weight Loss? A 3-Year PREVIEW Sub-study. Front. Nutr. 2021, 8, 640538. [Google Scholar] [CrossRef]
- Dorans, K.S.; Bazzano, L.A.; Qi, L.; He, H.; Appel, L.J.; Samet, J.M.; Chen, J.; Mills, K.T.; Nguyen, B.T.; O’Brien, M.J.; et al. Low-carbohydrate dietary pattern on glycemic outcomes trial (ADEPT) among individuals with elevated hemoglobin A1c: Study protocol for a randomized controlled trial. Trials 2021, 22, 108. [Google Scholar] [CrossRef] [PubMed]
- Moriconi, E.; Camajani, E.; Fabbri, A.; Lenzi, A.; Caprio, M. Very-low-calorie ketogenic diet as a safe and valuable tool for long-term glycemic management in patients with obesity and type 2 diabetes. Nutrients 2021, 13, 758. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Cheng, B.; Guo, Y.; Wang, Q.; Yang, N.; Lin, P. A Low-Carbohydrate Diet Realizes Medication Withdrawal: A Possible Opportunity for Effective Glycemic Control. Front. Endocrinol. 2021, 12, 779636. [Google Scholar] [CrossRef] [PubMed]
- Papamichou, D.; Panagiotakos, D.B.; Holmes, E.; Koutsakis, P.; Katsoulotos, H.; Loo, R.L.; Itsiopoulos, C. The rationale and design of a Mediterranean diet accompanied by time restricted feeding to optimise the management of type 2 diabetes: The MedDietFast randomised controlled trial. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 220–230. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Country | n | Duration (Months) | % of Female | RCT Condition a | Outcome(s) | Energy Restriction | Exercise | Diabetes Medications | Drop-Out | Adverse Event(s) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||||||||
| Uusitupaa 1993 [54], Sweden | 86 | 12 | 43 | LF (50.7/53.7) b | CON (54.0/54.4) b | — | HbA1c, FG | Yes. | No. | Yes. | 0% | / |
| Milne 1994 [55], New Zealand | 64 | 18 | 54.7 | MC (59) | LF (60) | CON (58) | HbA1c | Yes. | No. | Yes. | 8.5% | / |
| Brinkworth 2004 [56], Australia | 38 | 16 | 60.5 | HP (60.9) | LF (62.7) | — | HbA1c, FG | No. | / | Yes. | 40.6% | / |
| Westman 2008 [58], USA | 50 | 6 | 79 | KD (51.2) | LGI (50.0) | — | HbA1c, FG | Yes. | No. | Yes. | 40.5% | Headache, constipation, diarrhea, insomnia, and back pain (p > 0.05). |
| Wolever 2008 [59], Canada | 156 | 12 | 54 | LF (60.4) | LGI (60.6) | MC (58.6) | HbA1c | Yes. | Yes. | Yes. | 19.75% | 2 adverse events in LF and MC, respectively. |
| Ma 2008 [57], USA | 40 | 12 | 53 | REC (53) c | LGI | — | HbA1c | No. | No. | Yes. | 0% | / |
| Barnard 2009 [60], USA | 99 | 18.5 | 60.6 | VEG (56.7) | REC (54.6) | — | HbA1c, FG | Yes. | No. | Yes. | 28.3% | No adverse events. |
| Brehm 2008 [61], USA | 95 | 12 | 62.9 | MC (56.5) c | LF | — | HbA1c, FG | Yes. | No. | / | 23% | / |
| Esposito 2009 [63], Italy | 215 | 48 | 50.6 | MD (52.4) | LF (51.9) | — | HbA1c, FG | Yes. | Yes. | Yes. | 9.3% | 21% in MD and 23% in LF reported at least 1 adverse event. |
| Davis 2009 [62], USA | 105 | 12 | 78.1 | LC (54) | LF (53) | — | HbA1c | No. | No. | Yes. | 13.33% | / |
| Neelima 2009 [64], USA | 89 | 36 | / | LF (/) | CON (/) | — | HbA1c | / | / | / | / | / |
| Elhayany 2010 [66], Israel | 194 | 12 | 44.3 | REC (55) c | MD | MC | HbA1c, FG | No. | No. | / | 30.9% | / |
| Iqbal 2010 [68], USA | 68 | 24 | 10.4 | LC (59.4) c | LF | — | HbA1c, FG | Yes. | No. | Yes. | 52.78% | No adverse events. |
| Coppell 2010 [65], New Zealand | 93 | 6 | 59.1 | LF (56.6) | CON (58.4) | — | HbA1c, FG | Yes. | Yes. | Yes. | 9.62% | / |
| Huang 2010 [67], Taiwan, China | 154 | 12 | 56.5 | LF (56.6) | CON (56.9) | — | HbA1c, FG | No. | No. | Yes. | 20.2% | / |
| Nystrom 2011 [73], Sweden | 61 | 24 | / | LF (/) | LC (/) | — | HbA1c | Yes. | / | / | 0% | / |
| Goldstein 2011 [71], Israel | 30 | 12 | 48.1 | LC (57) | REC (55) | — | HbA1c, FG | LC: No. REC: Yes. | No. | / | 42.3% | / |
| Kahleova 2011 [72], Czech Republic | 74 | 6 | 52.7 | VEG (54.6) | REC (57.7) | — | HbA1c, FG | Yes. | Yes. | Yes. | 32.4% | / |
| Fabricatore 2011 [70], USA | 79 | 10 | 79.7 | LF (52.5) | LGI (52.8) | — | HbA1c, FG | Yes. | Yes. | / | 36.7% | / |
| Andrews 2011 [69], UK | 347 | 12 | 36.6 | LF (60.1) | CON (59.5) | — | HbA1c | LF: Yes. CON: No. | No. | Yes. | 2.3% | / |
| Guldbrand 2012 [74], Sweden | 61 | 24 | 55.8 | LC (62.7) | LF (61.2) | — | HbA1c | Yes. | / | Yes. | 0% | / |
| Krebs 2012 [75], New Zealand | 419 | 24 | 60 | HP (57.7) | LF (58.0) | — | HbA1c, FG | Yes. | / | Yes. | 30% | / |
| Timar 2013 [76], Romania | 223 | 12 | / | MD (/) | REC (/) | CON (/) | HbA1c | MD: Yes. REC: Yes. CON: No. | No. | Yes. | / | / |
| Pedersen 2014 [78], Australia | 64 | 12 | 22.2 | HP (59.4) | LF (62.4) | — | HbA1c, FG | Yes. | / | Yes. | 29.7% | No adverse events. |
| Tay 2014 [79], USA | 78 | 13 | 42.6 | LC (/) | LF (/) | — | HbA1c, FG | Yes. | Yes. | / | 32% | / |
| Yamada 2014 [80], Japan | 24 | 6 | 50 | LC (63.3) | LF (63.2) | — | HbA1c, FG | LC: No. LF: Yes. | / | / | 0% | / |
| Lasa 2014 [77], Spain | 141 | 12 | 59.7 | MD (67.4) | LF (67.2) | — | FG | No. | No. | / | 0% | No adverse effects. |
| Rock 2014 [44], USA | 227 | 12 | 51.1 | LF (55.5) | MC (57.3) | CON (56.8) | HbA1c, FG | Yes. | No. | Yes. | 10% | / |
| Bahado-Singh 2015 [81], Jamaica | 65 | 6 | 55 | LGI (42.5) | CON (43.0) | — | HbA1c, FG | / | / | / | 18.5% | / |
| Liu 2015 [82], China | 117 | 12 | 60.7 | LF (63.3) | CON (62.0) | — | HbA1c, FG | / | No. | / | 0% | / |
| Watson 2016 [83], Australia | 61 | 6 | 45.9 | HP (54) | LF (55) | — | HbA1c, FG | Yes. | Yes. | Yes. | 27.9% | / |
| Wycherley 2016 [84], Australia | 115 | 12 | 42.6 | LC (58.4) c | LF | — | HbA1c | Yes. | Yes. | / | 32.1% | / |
| Sato 2016 [86], Japan | 62 | 6 | 24.2 | LC (60.5) | REC (58.4) | — | HbA1c | No. | No. | Yes. | 6.1% | / |
| Maiorino 2016 [85], Italy | 201 | 42 | 50.7 | MD (52.4) | LF (51.9) | — | HbA1c, FG | Yes. | No. | / | 9.3% | / |
| Pavithran 2019 [87], India | 30 | 6 | 46.7 | LGI (52) c | CON | — | HbA1c | / | / | / | / | / |
| Pavithran 2020 [91], India | 36 | 6 | 41.7 | LGI (52) c | CON | — | HbA1c | / | / | / | 10% | / |
| Chen 2020 [88], Taiwan, China | 85 | 18 | 61.1 | LC (63.1) | REC (64.1) | — | HbA1c, FG | No. | No. | Yes. | 7.6% | No adverse effects on lipid profiles. |
| Gutierrez-Mariscal 2020 [89], Spain | 183 | 60 | 16.9 | MD (60.3) | LF (59.9) | — | HbA1c, FG | No. | No. | / | 2.2% | / |
| Marco-Benedi 2020 [90], Spain | 73 | 6 | 56.2 | HP (56.6) | LF (54.5) | — | HbA1c, FG | Yes. | Yes. | Yes. | 8.2% | / |
| Kakoschke 2021 [92], Australia | 115 | 48 | 42.6 | LC (58.5) c | LF | — | HbA1c | Yes. | Yes. | / | 47% | / |
| Zahedi 2021 [93], Iran | 228 | 6 | 77.2 | MD (57.3) c | CON | — | HbA1c, FG | / | / | / | 7.9% | / |
| Gram-Kampmann 2022 [94], Denmark | 64 | 6 | 56.3 | LC (57.3) | REC (55.2) | — | HbA1c, FG | No. | No. | Yes. | 9.8% | An increased frequency of gastrointestinal complaints (p = 0.03) such as constipation (n = 5), diarrhea (n = 2), and abdominal discomfort (n = 3) was found in LC group |
| Fasting Glucose (mmol/L) | |||||||||
| KD | −0.53 (−2.86,1.79) | −0.21 (−2.28,1.85) | −0.86 (−3.46,1.75) | −0.18 (−2.53,2.17) | −1.23 (−3.63,1.18) | −0.59 (−2.95,1.77) | −0.78 (−3.18,1.62) | −0.72 (−3.03,1.58) | −1.48 (−3.77,0.82) |
| −0.86 (−2.06,0.34) | MD | 0.32 (−0.75,1.39) | −0.32 (−1.57,0.93) | 0.35 (−0.25,0.95) | −0.69 (−1.44,0.06) | −0.06 (−0.71,0.59) | −0.25 (−1.01,0.51) | −0.19 (−0.58,0.20) | −0.95 (−1.51,−0.38) |
| −1.00 (−2.05,0.05) | −0.14 (−0.73,0.45) | LGI | −0.64 (−2.23,0.95) | 0.03 (−1.08,1.15) | −1.01 (−2.25,0.22) | −0.37 (−1.51,0.76) | −0.57 (−1.79,0.66) | −0.51 (−1.52,0.50) | −1.26 (−2.26,−0.27) |
| −1.01 (−2.21,0.20) | −0.15 (−0.80,0.50) | −0.01 (−0.60,0.59) | VEG | 0.68 (−0.58,1.94) | −0.37 (−1.37,0.63) | 0.27 (−1.08,1.62) | 0.08 (−1.12,1.27) | 0.13 (−1.11,1.38) | −0.62 (−1.93,0.68) |
| −1.09 (−2.29,0.11) | −0.23 (−0.87,0.42) | −0.09 (−0.68,0.50) | −0.08 (−0.73,0.57) | MC | −1.04 (−1.81,−0.28) | −0.41 (−1.18,0.36) | −0.60 (−1.38,0.18) | −0.54 (−1.11,0.02) | −1.30 (−1.92,−0.67) |
| −1.33 (−2.48,−0.19) | −0.47 (−1.00,0.06) | −0.33 (−0.79,0.13) | −0.32 (−0.71,0.06) | −0.24 (−0.77,0.28) | RECOM | 0.64 (−0.27,1.54) | 0.44 (−0.20,1.09) | 0.50 (−0.24,1.24) | −0.25 (−1.09,0.58) |
| −1.40 (−2.62,−0.17) | −0.53 (−1.22,0.15) | −0.40 (−1.03,0.24) | −0.39 (−1.08,0.31) | −0.31 (−0.82,0.20) | −0.06 (−0.64,0.52) | HP | −0.19 (−1.07,0.69) | −0.13 (−0.65,0.38) | −0.89 (−1.60,−0.18) |
| −1.49 (−2.71,−0.27) | −0.63 (−1.30,0.05) | −0.49 (−1.11,0.13) | −0.48 (−1.16,0.20) | −0.40 (−0.90,0.09) | −0.16 (−0.72,0.41) | −0.09 (−0.39,0.20) | LC | 0.06 (−0.65,0.77) | −0.70 (−1.52,0.13) |
| −1.45 (−2.66,−0.25) | −0.59 (−1.24,0.06) | −0.45 (−1.05,0.14) | −0.45 (−1.10,0.21) | −0.37 (−0.82,0.09) | −0.12 (−0.66,0.41) | −0.06 (−0.28,0.17) | 0.04 (−0.15,0.22) | LF | −0.75 (−1.24,−0.27) |
| −0.73 (−1.19,−0.28) | −0.47 (−1.27,0.34) | −0.37 (−0.83,0.10) | −0.48 (−3.10,2.15) | −0.33 (−0.83,0.17) | −0.43 (−0.94,0.09) | 0.06 (−0.45,0.57) | −0.69 (−1.32,−0.06) | −1.82 (−2.93,−0.71) | CON |
| HbA1c (%) | |||||||||
| HbA1c | SUCRA (%) | Fasting Glucose | SUCRA (%) | |
|---|---|---|---|---|
| 1 | Ketogenic | 97.5 | Moderate-carbohydrate | 82.7 |
| 2 | Mediterranean | 78.1 | Low GI/GL | 75.4 |
| 3 | Low GI/GL | 69.0 | Ketogenic | 71.0 |
| 4 | Vegetarian/Vegan | 68.9 | Mediterranean | 61.3 |
| 5 | Moderate-carbohydrate | 62.7 | High-protein | 56.3 |
| 6 | Recommended | 38.9 | Low-fat | 44.2 |
| 7 | High-protein | 35.5 | Low-carbohydrate | 44.1 |
| 8 | Low-carbohydrate | 25.3 | Vegetarian/Vegan | 41.6 |
| 9 | Low-fat | 22.5 | Recommended | 16.3 |
| 10 | Control | 1.7 | Control | 6.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jing, T.; Zhang, S.; Bai, M.; Chen, Z.; Gao, S.; Li, S.; Zhang, J. Effect of Dietary Approaches on Glycemic Control in Patients with Type 2 Diabetes: A Systematic Review with Network Meta-Analysis of Randomized Trials. Nutrients 2023, 15, 3156. https://doi.org/10.3390/nu15143156
Jing T, Zhang S, Bai M, Chen Z, Gao S, Li S, Zhang J. Effect of Dietary Approaches on Glycemic Control in Patients with Type 2 Diabetes: A Systematic Review with Network Meta-Analysis of Randomized Trials. Nutrients. 2023; 15(14):3156. https://doi.org/10.3390/nu15143156
Chicago/Turabian StyleJing, Tiantian, Shunxing Zhang, Mayangzong Bai, Zhongwan Chen, Sihan Gao, Sisi Li, and Jing Zhang. 2023. "Effect of Dietary Approaches on Glycemic Control in Patients with Type 2 Diabetes: A Systematic Review with Network Meta-Analysis of Randomized Trials" Nutrients 15, no. 14: 3156. https://doi.org/10.3390/nu15143156