Food based dietary patterns and chronic disease prevention
BMJ 2018; 361 doi: https://doi.org/10.1136/bmj.k2396 (Published 13 June 2018) Cite this as: BMJ 2018;361:k2396
Food for thought
Click here to read other articles in this collection

- Matthias B Schulze, professor and department head123,
- Miguel A Martínez-González, professor and department chair456,
- Teresa T Fung, professor67,
- Alice H Lichtenstein, Gershoff professor, director and senior scientist89,
- Nita G Forouhi, professor and programme leader10
- 1Department of Molecular Epidemiology, German Institute of Human Nutrition Potsdam-Rehbruecke, Nuthetal, Germany.
- 2University of Potsdam, Institute of Nutritional Sciences, Nuthetal, Germany
- 3NutriAct—Competence Cluster Nutrition Research Berlin-Potsdam, Germany
- 4Department of Preventive Medicine and Public Health, University of Navarra-IdiSNA, Pamplona, Spain
- 5CIBER Fisiopatología de la Obesidad y Nutrición (CIBERobn), Instituto de Salud Carlos III (ISCIII), Spain
- 6Department of Nutrition, Harvard T H Chan School of Public Health, Boston, USA
- 7Department of Nutrition, Simmons College, Boston, USA
- 8Friedman School of Nutrition Science and Policy, Tufts University, Boston, USA
- 9Cardiovascular Nutrition Laboratory, Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University, Boston, USA
- 10Medical Research Council Epidemiology Unit, University of Cambridge, Cambridge, UK
- Correspondence to: M B Schulze mschulze{at}dife.de
Can specific foods provide health benefits? Will adopting a specific food pattern prevent major chronic diseases such as type 2 diabetes, cardiovascular disease, or cancer? Are exclusion diets—vegetarian or vegan diets or avoidance of foods containing gluten, lactose, or fructose—the key to good health? Should doctors advise patients to follow a paleolithic diet? The wide range of popular diet plans and concepts seems to continuously expand.1 But to what extent are their purported benefits supported by scientific evidence?
We have qualitatively assessed the available evidence from recent systematic reviews of long term studies to summarise current understanding of foods or dietary patterns and risk of major chronic diseases. Given that nutrition research has been criticised for providing apparently implausible results,23 which might contribute to the range of different popular diet concepts, we also discuss methodological approaches and specific challenges of conducting research on food intake patterns and health.
Evaluation of food patterns in nutrition studies
Given the relative stability of caloric intake by individual people, changes in dietary habits are generally characterised by substitution effects, where high consumption of some foods is associated with lower intake of other foods. This makes inferences about individual foods particularly challenging. For this reason, researchers also study food patterns, which account for inter-relations of food choices, represent the cumulative exposure to different diet components, and may have stronger effects on health than any single component.4
Food patterns can be defined as the quantities, proportions, variety, or combination of different foods and drinks in diets, and the frequency with which they are habitually consumed.5 Given that food intake is a multi-dimensional exposure, there are obviously numerous different combinations of foods to potentially investigate. How these combinations are defined in nutrition research largely depends on the research question and study design. In intervention studies food intake is directly manipulated, but in observational studies exposure to food patterns is derived from self reported intake. Two main research methods have been used in this context.46 The first is using a priori defined indices intended to capture specific dietary patterns, such as measuring conformity to dietary guidelines. The second is using data driven (exploratory) statistical methods (predominantly cluster analysis,7 principal component and factor analysis,48 and reduced rank regression 69) to characterise major patterns of food intake. Both approaches allow ranking and quantifying adherence of study participants to these patterns, which is needed to evaluate their association with disease risk. Both approaches and the corresponding statistical methods have their own specific strengths and limitations (table 1).
Strengths and limitations of approaches to measuring food patterns
An evidence based approach can be used to investigate causality between the intake of individual foods or dietary patterns and human health. This approach considers factors such as temporality, consistency, and sources of bias.10 The strongest evidence is usually derived from randomised controlled trials because this design minimises confounding bias. But most of the data available come from observational studies on food intake and risk of chronic diseases. Prospective cohort studies have contributed substantially over the past 60 years to what is known today. Systematic reviews have summarised data from such studies and highlighted the importance of individual foods and dietary patterns in the prevention of chronic diseases.11121314
Health benefits and risks related to food intake and food patterns
Individual foods and health outcomes
Table 2 shows foods and beverages consistently associated in the literature with risk of cancer, type 2 diabetes, coronary heart disease, or stroke. Higher consumption of whole grains is related to lower risk for most endpoints,11121314 whereas processed meat and unprocessed red meat consumption is associated with an increased risk.11121314 Evidence for other foods is less consistent and might be disease specific— for example, fruits and vegetables are associated with lower risk of cancer,14 coronary heart disease, and stroke,1213 but not type 2 diabetes.12 The role of dairy foods remains unclear, with fermented dairy products being more convincingly related to lower cardiometabolic disease risk than others1112 and total dairy consumption seems relevant to colorectal cancer.14 Sugar sweetened drinks are associated with increased risk of type 2 diabetes,1112 coronary heart disease,1213 and stroke,13 and coffee consumption is associated with lower risk of type 2 diabetes,1112 cardiovascular disease,1218 and several cancers,1418 with beneficial effects being most prominent at consumption of 3-5 cups a day.18
Associations between intake of foods and chronic disease risk based on published meta-analyses and reviews
Healthy food patterns and health outcomes
In prospective cohort studies the Mediterranean diet has been associated with lower risk for cancer, type 2 diabetes, and cardiovascular disease.1920 Similar findings were reported for the PREDIMED study, a randomised controlled trial of the Mediterranean diet supplemented with extra virgin olive oil or nuts (fig 1).2122 The primary endpoint of cardiovascular events was about 30% lower in the intervention groups than in the control group,21 and analyses of secondary endpoints support benefits for peripheral artery disease,23 atrial fibrillation,24 type 2 diabetes,22 and breast cancer.25 The Mediterranean diet generally refers to a diet encouraging high intake of fruits, nuts and seeds, vegetables, fish, legumes, and cereals and limiting the intake of meat and dairy products. Moderate intake of alcohol and olive oil as a major fat source have also been considered key components.26

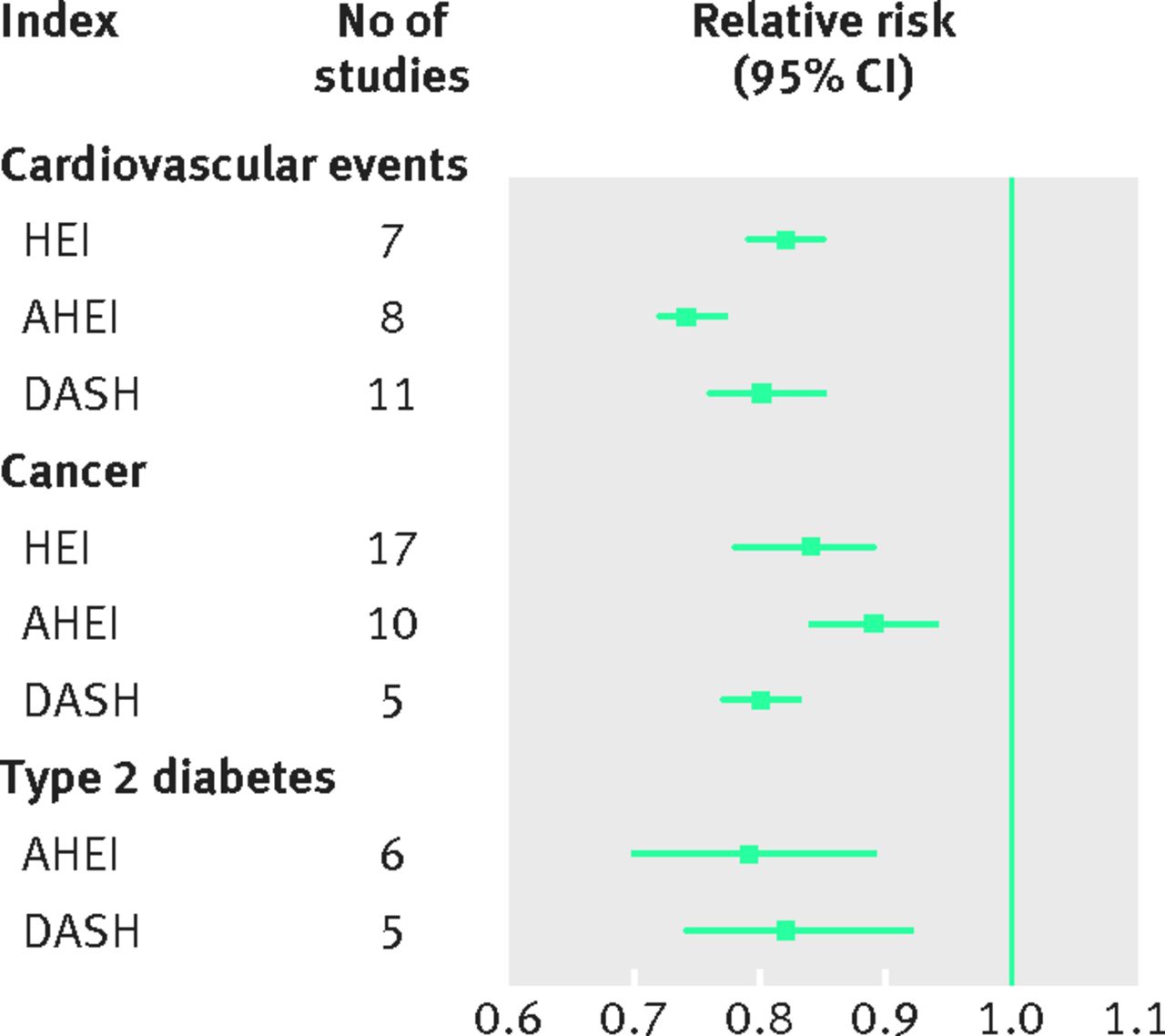
Several other defined food patterns have been evaluated in terms of chronic disease risk. Indices measuring adherence to the Healthy Eating Index,27 Alternative Healthy Eating Index,28 and the Dietary Approaches to Stop Hypertension trial (DASH)2930 have been associated with lower risk of cardiovascular events, cancer, and type 2 diabetes (fig 2).1931Table 3 shows the composition of these diets in comparison to the Mediterranean diet. Heterogeneity regarding the actual composition of these food scores exists between studies.19 Although these diets may be recommendable, only the Mediterranean diet has been shown both in observational studies and a randomised trial to lower disease risk.
{kind=link}
{kind=link}
Key components of the Mediterranean, DASH (Dietary Approaches to Stop Hypertension), and Alternative Healthy Eating dietary pattern scores
Notably, none of the diet plans captures fully the known benefits or detrimental effects of single foods; for example, the Mediterranean diet has traditionally not focused on whole grains or red meat.32 Low fat dairy consumption is encouraged in the DASH diet, but discouraged in the Mediterranean diet, although the evidence for limiting dairy is sparse.29 The Mediterranean diet emphasises olive oil, whereas the DASH diet discourages intake of fats and the Alternative Healthy Eating Index refers to high polyunsaturated fatty acid intakes, which would largely reflect vegetable fat sources other than olive oil. Still, these data corroborate previous findings that increased adherence to dietary patterns that emphasise fruits, vegetables, whole grains, nuts, legumes, vegetable oils, and fish and minimise red meat, processed meat, and added sugars are associated with decreased risk of cardiovascular events, cancer, and type 2 diabetes.5
Lack of long term studies for many popular diets
The evidence base for other popular diets is less consistent. Vegetarian diets have been linked in prospective cohort studies to lower risk of diabetes,33 heart disease, and cancer,34 but few studies have evaluated vegan diets.34 The food patterns of vegetarian and vegan diets are highly heterogeneous, making intra-study comparisons difficult. Exclusion of foods from animal sources may not necessarily result in high intakes of healthy plant based foods. The UK EPIC-Oxford study includes a large proportion of vegetarian and vegan participants, who have higher intakes of fruits, vegetables, legumes and vegetable oils than the general UK population, but their intake is substantially lower than, for example, the Spanish general population.35 A plant based diet could potentially be unhealthy if it consists primarily of refined carbohydrates and processed foods.36
We didn’t find any systematic reviews on the long term health effects of other common diets, such as the paleolithic, Atkins, zone, Ornish, South Beach, or a gluten-free diets. Some recent evidence comes from individual prospective cohorts. A diet low in gluten among those without coeliac disease was associated with higher risk of coronary heart disease, which was explainable by low consumption of beneficial whole grains.37 A paleolithic diet was inversely associated with mortality, although the association was weaker than for the Mediterranean diet.38 The paleolithic diet shares several components of other healthy dietary patterns (including high intake of fruits, vegetables, fish, and oils and low intake of foods with added sugar), but other aspects largely contradict evidence for single foods, specifically whole grains, legumes, and dairy. Many diet concepts have been popularised in the context of weight loss, but longer term data on chronic disease endpoints, which are the focus of our review, are largely not available. Randomised controlled trials show that most popular weight loss diets can achieve a similar magnitude of weight loss and that adherence to the diet is the biggest challenge.3940
Data driven food patterns and health outcomes
Nutrition researchers have also used exploratory statistical methods to evaluate population specific dietary patterns.19 But the evidence from such studies is difficult to generalise.5 Some common components have consistently emerged: for example, patterns high in processed meat, refined grains, high fat dairy, eggs, and fried food are positively associated with risk of type 2 diabetes and colorectal cancer, and patterns high in vegetables, legumes, fruits, poultry, and fish were inversely associated with risk.1941
Some studies have used reduced rank regression as an alternative statistical approach, which includes information on disease related pathways in the process of deriving dietary patterns.6 Dietary patterns commonly characterised by high intakes of refined grains, processed meat, and sugar sweetened beverages have been strongly associated with risk of type 2 diabetes, with results being replicated in multiple cohorts.19 Although reduced rank regression has been applied to other endpoints, the findings have rarely been replicated across other populations.6
Controversies and research gaps in observational studies
Evidence for the benefits of fruits, vegetables, whole grains, fish, nuts, legumes, vegetable oils, dairy, coffee, and tea—and for a lower intake of red and processed meats and sugar sweetened drinks— comes largely from observational studies, which have multiple limitations (box 1).
Limitations of observational nutrition studies on foods and dietary patterns and suggestions for further research
Semiquantitative dietary data
Use new assessment methods; eg, multiple sources to estimate usual intake
Evaluate relative versus quantitative scores for dietary patterns and implications of differences in absolute intake levels
Measurement error
Develop and use measurement error correction methods
Investigate measurement error influences on dietary pattern composition
Investigate validity and reliability of dietary patterns
Develop new biomarkers of food intake and pattern adherence
Correlation of food intake and substitution
Investigate specific food substitution by statistical modelling
Investigate influence of energy adjustment in exploratory pattern analysis
Long term variability of intake
Repeat diet assessments
Investigate change in intake and subsequent risk
Varying scoring systems for defined food patterns
Investigate influences of scoring alternatives
Standardise scoring systems
Population specificity of exploratory patterns
Replicate pattern associations in independent study populations with varying dietary habits
Different food classification and grouping
Evaluate influence of food grouping on pattern structure
Standardise food grouping
Unclear contribution of individual components to pattern association
Systematically evaluate contribution of each component
Semiquantitative nature of food intake data in observational studies
Most prospective cohort studies use semiquantitative food frequency questionnaires. These instruments are not designed to provide an accurate estimate of absolute intake. In studies that use quantitative cut-offs to assign points for individual components of the pattern, uncertainty accumulates. Many pattern indices or scores are based on relative cut-offs, which might better reflect the semiquantitative nature of the underlying assessment instrument.4 Such approaches usually evaluate intakes relative to the average consumption level in the studied population; for example, indices to capture exposure to the Mediterranean diet usually assign points for components based on centiles of population intake.42 Similarly, pattern scores from principal component or factor analysis are based on food variables standardised to the population mean. Consequently, the average and variation in absolute intake of individual components may vary largely among populations investigated for the same dietary pattern. This is a substantial challenge for making inference on specific dose-response relations.
Measurement error
Measurement error is a major limitation of observational nutrition studies.43 Researchers have tried to tackle the varying validity and reliability of dietary questionnaires to assess different components of a dietary pattern,44 but their results have hardly been used in investigations of dietary patterns and health outcomes. Studies evaluating the validity and reliability of dietary patterns are also scarce.4546 New biomarkers of food intake or food pattern exposure may complement or even substitute traditional dietary assessments.47 The use of repeated measurements of food intake over the follow-up period in cohort studies improves accuracy.
Variation in pattern scoring systems
Many studies have evaluated a priori defined dietary patterns, but the composition of patterns has varied considerably.192031 This limitation also applies to randomised trials, where differences in the definition of intervention diets are a major challenge.48 Investigations of both single food groups and food patterns are frequently constrained by the information collected in food frequency questionnaires. Although it seems clear that foods with similar characteristics can be put into aggregated groups, broader groups are less homogeneous than narrower ones. The influence of regional foods and of food classifications in the definition and categorisation of food patterns is still understudied.449 Comparing different definitions for conceptually similar diets would be an important step forward; for example, Tong and colleagues compared different indices of the Mediterranean diet and cardiovascular disease.50
Food patterns versus individual food components
Food patterns pre-empt potential dietary confounding by other aspects of the diet, increase the ability to assess stronger effects due to the cumulative effects of many features of the diet, and allow assessment of the interaction among synergistic components. But observed associations could be due to single components rather than the overall dietary pattern. This can be tackled by systematic analysis of the effect of single components for the overall association; for example, the reduced diabetes risk observed for the Mediterranean diet in the Europe-wide EPIC-InterAct study was partly attributable to moderate alcohol, higher olive oil, and lower meat consumption.51 The evaluation of overall dietary patterns could also mask the effects of individual foods; for example, exploratory patterns including whole grains as components showed only marginal inverse association with diabetes risk,525354555657 whereas whole grains were inversely associated.5859 Also, dietary patterns usually capture only a fraction of variation in food intake, which leaves a large space of potential effects related to foods not included as components of the pattern.
Generalisability of data driven food patterns
Exploratory patterns are specific to the population investigated, so the contribution of single study findings to evidence based recommendations is limited. Although exploratory food patterns might have similar components, clear criteria for their consistency needed to summarise observations in meta-analysis are lacking. Replicating study findings in other populations is important, as has been applied in studies using reduced rank regression.60 A common element of exploratory pattern methods is that investigators must make arbitrary decisions when, for example, selecting the appropriate number of patterns to investigate further (table 1).
Confounding by diet—food substitution
Observational studies are more prone to confounding bias than randomised controlled trials. Confounding is not only related to other lifestyle factors and general risk factors, but to additional food exposures. Food intake is characterised by combinations and substitutions, so appropriate control of correlated foods is essential in studies investigating individual foods as potential risk factors. Cohort studies provide the possibility to model specific isocaloric food substitutions—an underused approach. When evaluating reductions in red meat intake, for example, taking into account the substitution of other protein sources can be informative.61 Pattern analysis might account for intercorrelations among foods.
Timescale of dietary assessment in long term studies
Inferences from observational studies are usually based on comparisons between different groups that differ in baseline intake; for example, comparing study participants who consume sugar sweetened drinks daily with those who consume them less frequently. Cohort studies can, however, evaluate changes in food consumption if repeated measures of intake are available. Increasing diet quality, assessed as adherence to the Alternative Healthy Eating Index, DASH, or Mediterranean diets, has been found to decrease mortality risk compared with unchanged adherence.62 Observational designs that use repeated measurements to assess changes in food patterns can almost simulate interventional trials and provide strong evidence on causality if relevant confounders are controlled.
Potential and limitations of randomised trials
Randomised controlled trials are less prone to confounding bias and have the ability to control exposure differences between groups, allowing for quantification of dose-response relations. But randomised controlled trials testing dietary interventions are considerably more challenging than standard drug trials (box 2).63
Limitations of randomised controlled trials on food intake and health
Recruiting participants for long term changes to diets is difficult, and dropout rates are high
Dietary advice and actual dietary consumption differ
Identifying appropriate control diets is challenging, and treatment intensity between intervention and control arms may be imbalanced
Blinding dietary interventions is frequently unfeasible
Adherence problems limit the difference in exposure between intervention arms
Long term interventions to investigate effects on chronic disease risk are costly
One challenge is the difficulty of identifying an appropriate control when evaluating foods or food patterns.64 If control participants do not receive a placebo or a comparative intervention, there is strong potential for expectation bias (expected benefit in the intervention group versus expected lack of benefit in the control group). The Women’s Health Initiative Dietary Modification Trial, for example, compared a low fat intervention group with intensive behaviour modification counselling to increase fruit, vegetable, and grain consumption with a “usual diet” group receiving diet related education materials only.65 Although active controls can be designed, such trials are difficult to blind.
Studies depending on dietary advice may not result in sufficiently large differences in food consumption between intervention and control groups due to suboptimal compliance of participants—this critique has been raised for large randomised dietary trials, such as the PREDIMED study66 and the Women’s Health Initiative Dietary Modification Trial.67 For large trials with thousands of participants, changing people’s habitual dietary patterns demands an unparalleled workload. In addition, the high costs of running long term intervention studies makes it unlikely that associations for multiple foods, food substitutions, and food patterns can be tested for hard outcome endpoints. Still, randomised controlled trials can support or refute observations using surrogate markers of disease. The DASH trial, for example, was a controlled feeding trial with a dietary pattern rich in fruits, vegetables, and low fat dairy products, which reduced blood pressure.29 This could be extrapolated to a reduction in cardiovascular event risk, although no randomised trial has been conducted to evaluate if the DASH diet affects incidence of cardiovascular disease. Surrogate (intermediate) markers such as blood pressure can be important mediating factors between food intake, food pattern, and disease risk.
Shorter term randomised trials are not only a tool to support (or refute) the biological causality of observations but can also be used to determine potential effect sizes. But the triangulation of evidence from different sources63 might be difficult owing to the different timing and duration of exposures in long term cohort studies versus short term randomised controlled trials of intermediate endpoints, as well as the choice of diet sensitive surrogate markers.68 Still, this approach is useful for the popular diet concepts for which evidence on their long term relevance for chronic disease prevention is currently lacking.
Key messages
Food based prevention of chronic disease risk should prioritise fruits, vegetables, whole grains and fish and lower consumption of red and processed meats and sugar sweetened drinks
Higher consumption of nuts, legumes, vegetable oils, fermented dairy products, and coffee are further likely to confer benefit
Evidence comes from prospective observational and intervention studies, each study design having different strengths and limitations. Both types of studies should contribute to the evidence base
New analytical approaches are needed for nutrition research; eg, to account for measurement error, standardisation of exposure definitions, replication efforts, and the use of repeated dietary assessments
Footnotes
Contributors and sources: The author group spans a wide range of expertise from nutritional epidemiology and public health, all of whom have contributed to past dialogue on foods, dietary patterns, and health. Sources of information for this article included published systematic reviews on foods, dietary patterns, and major chronic diseases (coronary heart disease, stroke, type 2 diabetes, and cancer). All authors contributed to drafting this manuscript, with MBS taking a lead role. All authors gave intellectual input to improve the manuscript and have read and approved the final version. MBS is the guarantor.
Competing interests: We have read and understood BMJ policy on declaration of interests and declare the following: MBS receives funding from the German Federal Ministry of Education and Research (FKZ: 01EA1408A-G). MAM-G has no conflict of interest and has received funding from public agencies, including the European Research Council (Advanced Research Grant, #340918) and from Instituto de Salud Carlos III, CIBEROBN. TTF has nothing to declare. AHL receives funding from the US National Institutes of Health, US Department of Agriculture and the Hass Avocado Board. NGF receives funding from the Medical Research Council Epidemiology Unit (MC_UU_12015/5). She is a member (unpaid) of the Joint SACN/NHS-England/Diabetes-UK Working Group to review the evidence on lower carbohydrate diets compared with current government advice for adults with type 2 diabetes and is a member (unpaid) of ILSI-Europe Qualitative Fat Intake Task Force Expert Group on update on health effects of different saturated fats.
This article is one of a series commissioned by The BMJ. Open access fees for the series were funded by Swiss Re, which had no input into the commissioning or peer review of the articles.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.