Towards an Evidence-Based Recommendation for a Balanced Breakfast—A Proposal from the International Breakfast Research Initiative

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Assessment of Diet Quality
2.3. Data Compilation
3. Results
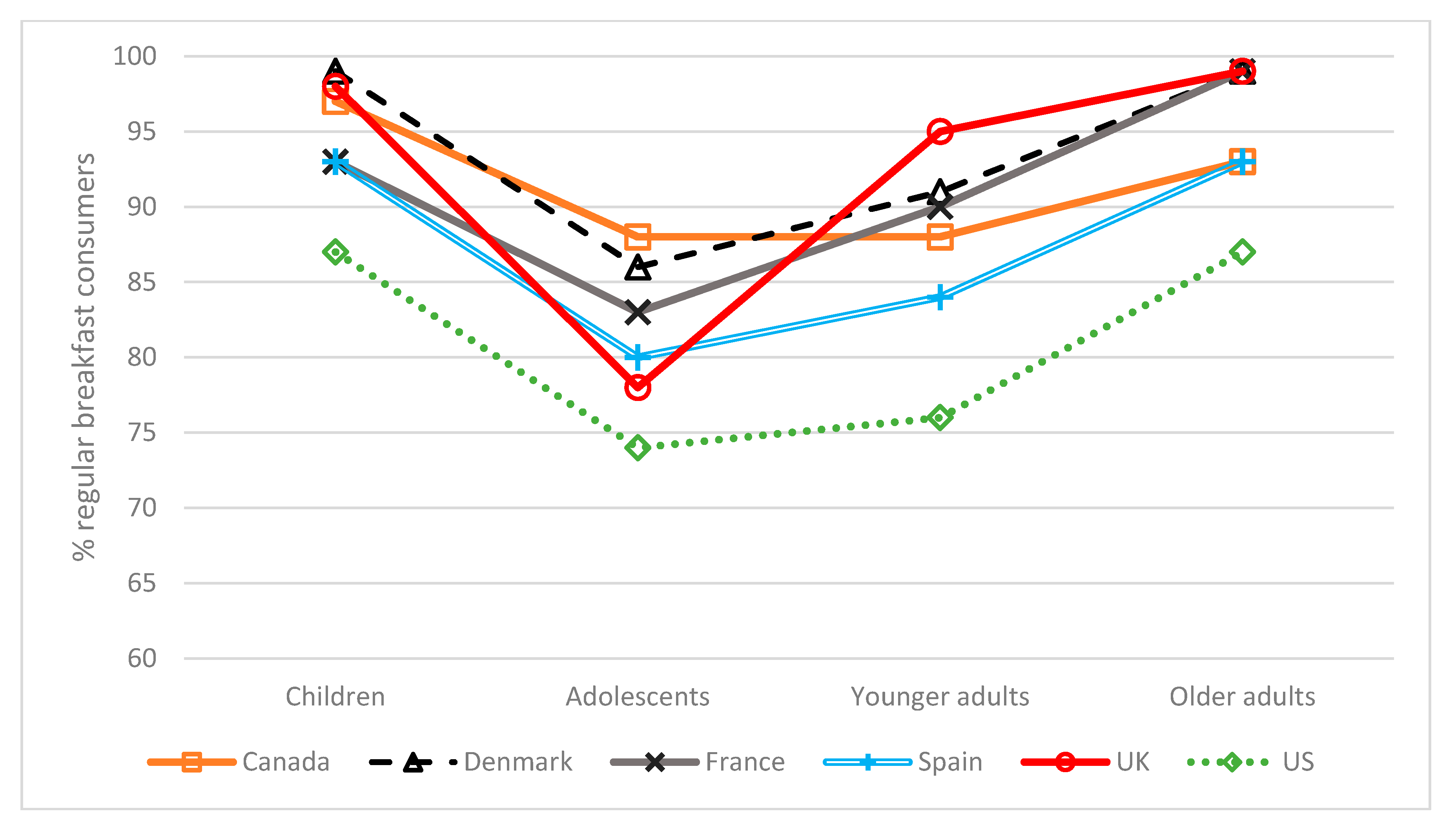
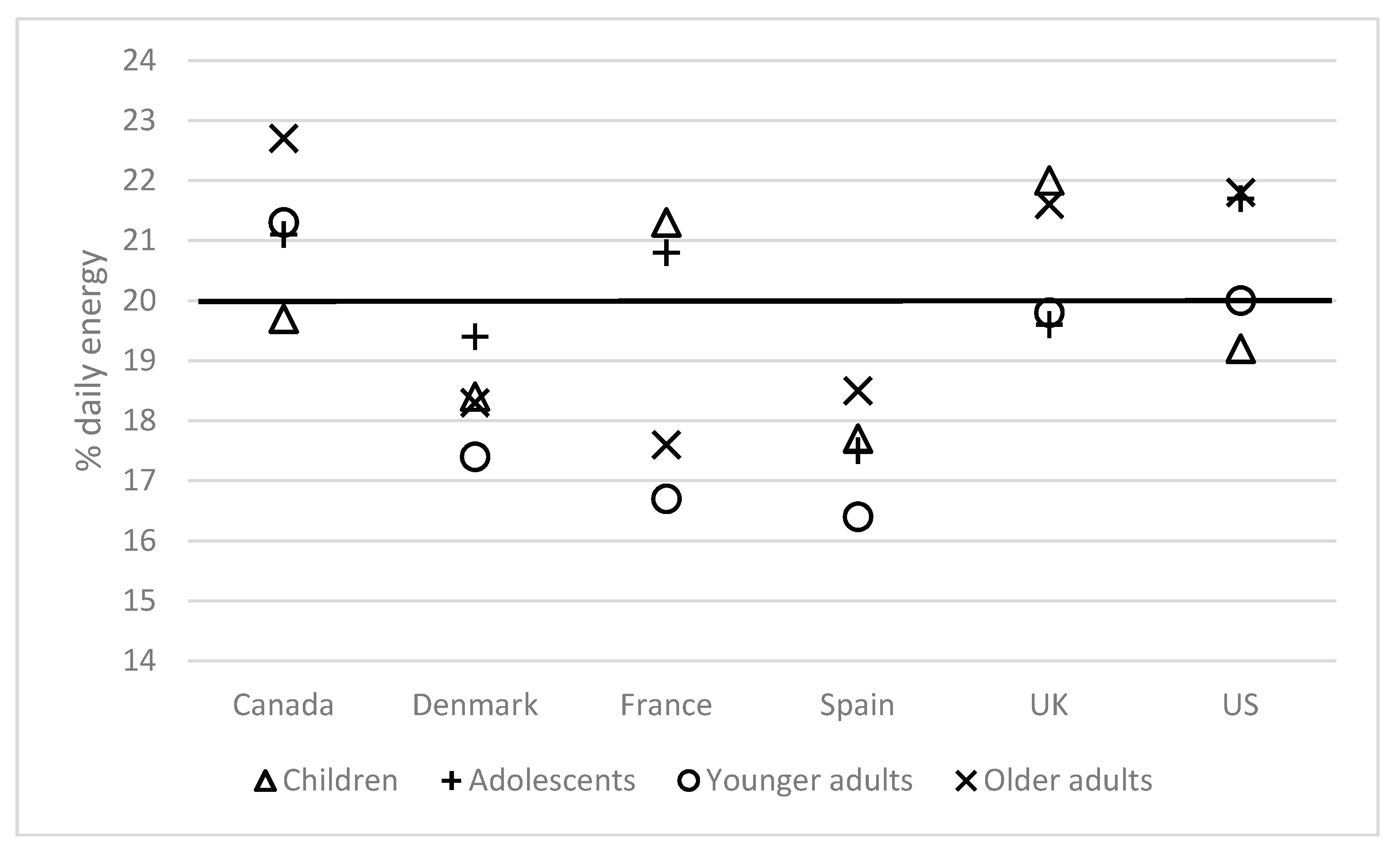
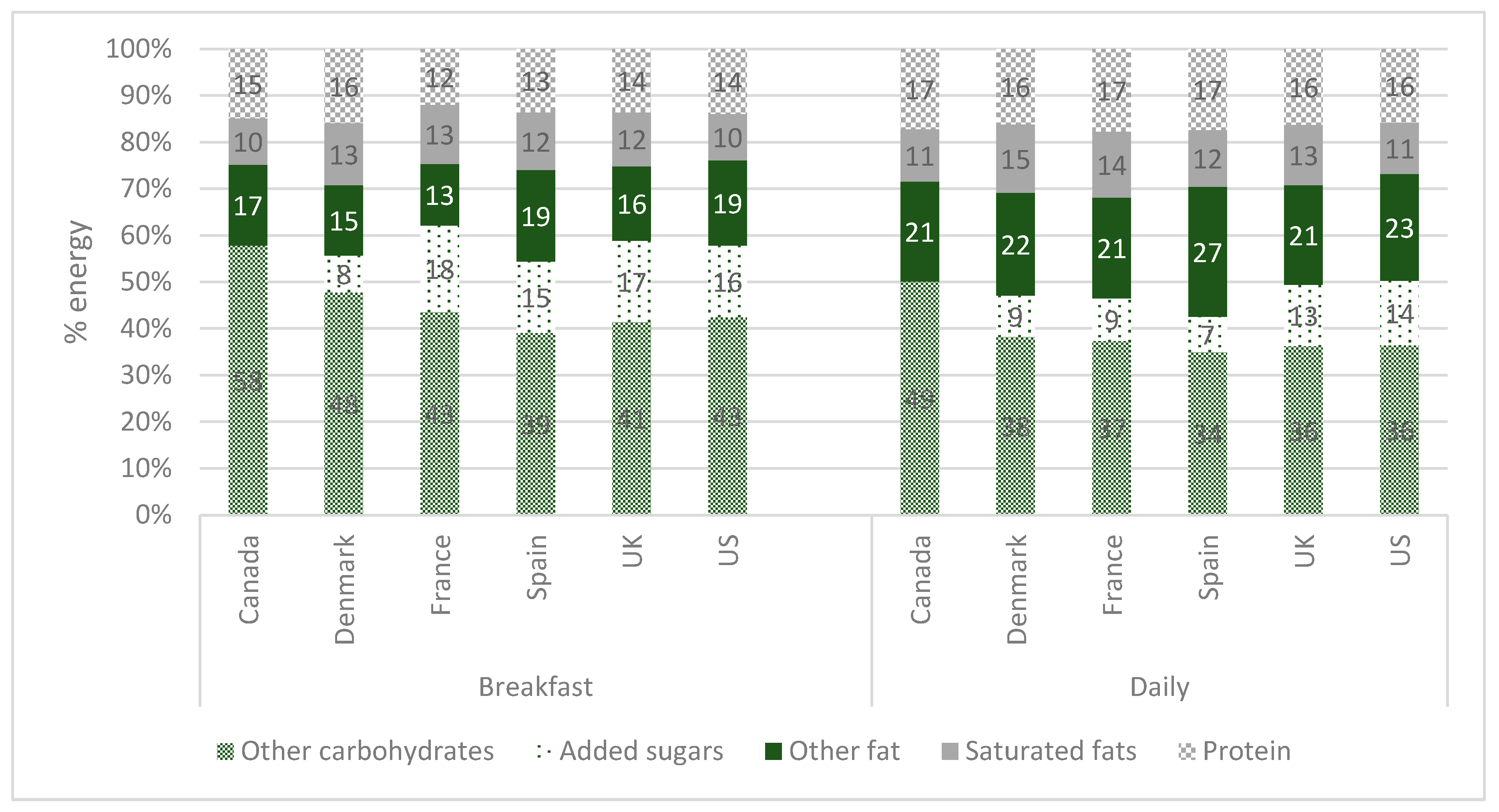
3.1. Consumption of Breakfast and Its Nutritional Pattern in the 6 Countries
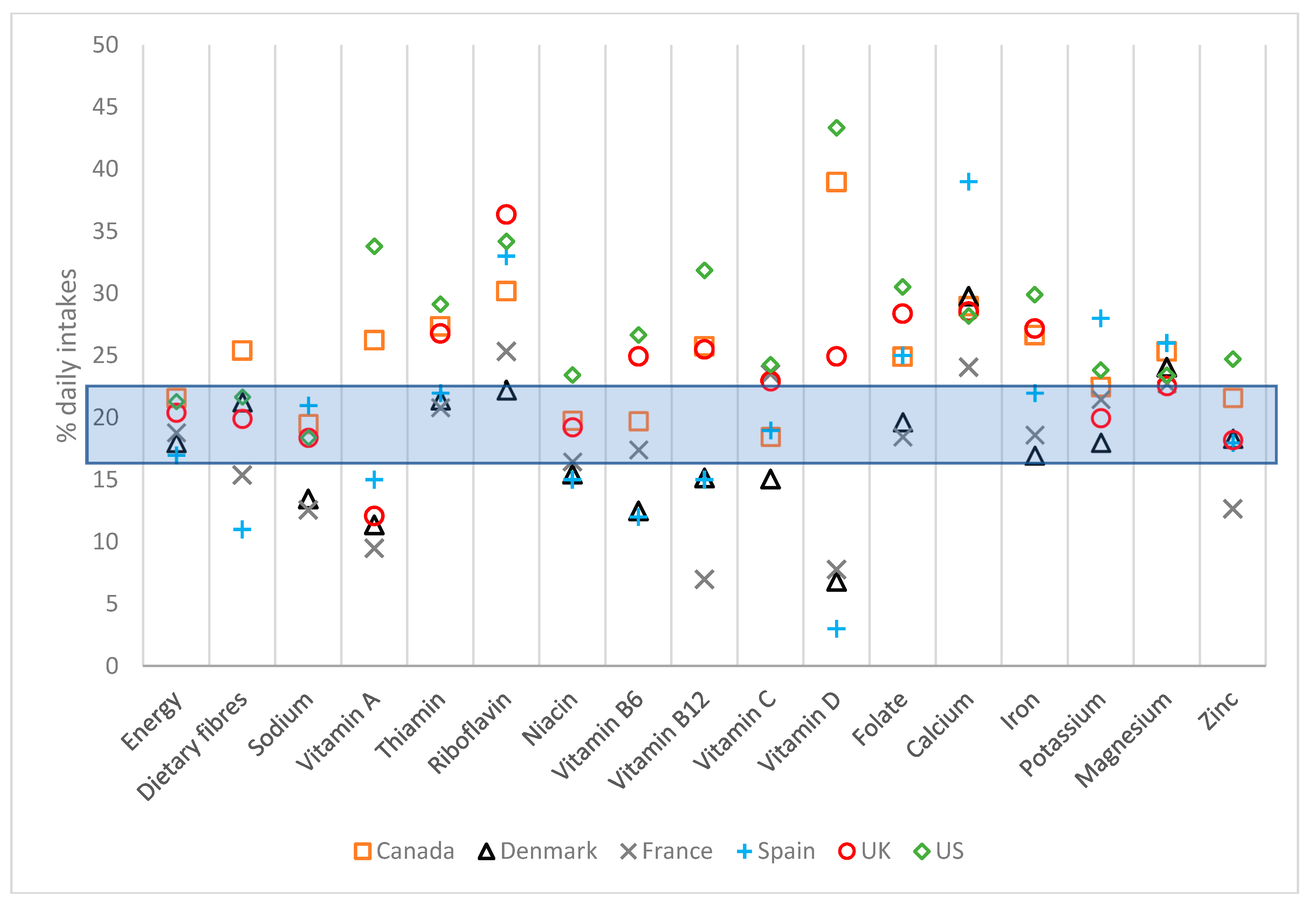
3.2. Nutritional Intakes at Breakfast among Individuals with Highest Overall Diet Quality
3.3. Principles for the Development of Nutrient Recommendation for Breakfast
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Currie, C.; Zanotti, C.; Morgan, A.; Currie, D.; Looze, M.D.; Roberts, C.; Samdal, O.; Smith, O.R.F.; Barnekow, V. (Eds.) Social Determinants of Health and Well-Being among Young People. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2009/2010 Survey; WHO Europe: Copenhagen, Denmark, 2012; ISBN 978 92 890 1423 6. [Google Scholar]
- St-Onge, M.-P.; Ard, J.; Baskin, M.L.; Chiuve, S.E.; Johnson, H.M.; Kris-Etherton, P.; Varady, K.; American Heart Association Obesity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; Stroke Council. Meal Timing and Frequency: Implications for Cardiovascular Disease Prevention: A Scientific Statement From the American Heart Association. Circulation 2017, 135, e96–e121. [Google Scholar] [CrossRef] [PubMed]
- Purslow, L.R.; Sandhu, M.S.; Forouhi, N.; Young, E.H.; Luben, R.N.; Welch, A.A.; Khaw, K.-T.; Bingham, S.A.; Wareham, N.J. Energy Intake at Breakfast and Weight Change: Prospective Study of 6,764 Middle-aged Men and Women. Am. J. Epidemiol. 2007, 167, 188–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Heijden, A.A.W.A.; Hu, F.B.; Rimm, E.B.; van Dam, R.M. A Prospective Study of Breakfast Consumption and Weight Gain among U.S. Men. Obesity 2007, 15, 2463–2469. [Google Scholar] [CrossRef] [PubMed]
- Dhurandhar, E.J.; Dawson, J.; Alcorn, A.; Larsen, L.H.; Thomas, E.A.; Cardel, M.; Bourland, A.C.; Astrup, A.; St-Onge, M.-P.; Hill, J.O.; et al. The effectiveness of breakfast recommendations on weight loss: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 100, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Gibney, M.; Uzhova, I. Breakfast—Shaping Guidelines from Food and Nutrient Patterns. Available online: https://www.nestlenutrition-institute.org/resources/videos/details/breakfast-shaping-guidelines-from-food-and-nutrient-patterns (accessed on 9 August 2018).
- Porter, S. Healthy Breakfast Food Fact Sheet. Available online: https://www.bda.uk.com/foodfacts/breakfast.pdf (accessed on 9 August 2018).
- Dietitians Association of Australia Breakfast—How to Eat Brekkie Like a Boss! Available online: https://daa.asn.au/smart-eating-for-you/smart-eating-fast-facts/breakfast-how-to-eat-brekkie-like-a-boss/ (accessed on 9 August 2018).
- Secretaria de educacion pública. ACUERDO mediante el cual se establecen los lineamientos generales para el expendio y distribución de alimentos y bebidas preparados y procesados en las escuelas del Sistema Educativo Nacional. Diario Of. 2014. [Google Scholar]
- Institute of Medicine (US) Committee on Nutrition Standards for National School Lunch and Breakfast Programs. Nutrition Standards and Meal Requirements for National School Lunch and Breakfast Programs: Phase I. Proposed Approach for Recommending Revisions; Stallings, V.A., Taylor, C.L., Eds.; National Academies Press (US): Washington, DC, USA, 2008; ISBN 9780309127950.
- O’Neil, C.E.; Byrd-Bredbenner, C.; Hayes, D.; Jana, L.; Klinger, S.E.; Stephenson-Martin, S. The Role of Breakfast in Health: Definition and Criteria for a Quality Breakfast. J. Acad. Nutr. Diet. 2014, 114, S8–S26. [Google Scholar] [CrossRef] [PubMed]
- Marangoni, F.; Poli, A.; Paoletti, R.; Agostoni, C.; Di Pietro, P.; Cricelli, C.; Brignoli, O.; Fatati, G.; Giovannini, M.; Riva, E.; et al. Documento di Consenso sul Ruolo Della Prima Colazione Nella Ricerca e nel Mantenimento della Buona Salute e del Benessere. Available online: http://www.nutrition-foundation.it/pubblicazioni/documento-di-consenso-sul-ruolo-della-prima-colazione-nella-ricerca-e-nel-mantenimento-della-buona-salute-e-del-benessere.aspx (accessed on 29 August 2018).
- Institute of Medicine (US) Committee on Nutrition Standards for National School Lunch and Breakfast Programs. School Meals: Building Blocks for Healthy Children; Stallings, V., West Suitor, C., Taylor, C., Eds.; National Academies Press: Washington, DC, USA, 2010; ISBN 978-0-309-14436-0.
- Gordon, A.; Foy, M.K.; Mathematica Policy Research Inc. School Nutrition Dietary Assessment Study-III Summary of Findings; USDA Food and Nutrition Service: Alexandria, VA, USA, 2007.
- Gibney, M.; Barr, S.; Bellisle, F.; Drewnowski, A.; Fagt, S.; Livingstone, B.; Masset, G.; Varela Moreiras, G.; Moreno, L.; Smith, J.; et al. Breakfast in Human Nutrition: The International Breakfast Research Initiative. Nutrients 2018, 10, 559. [Google Scholar] [CrossRef] [PubMed]
- Fagt, S.; Matthiessen, J.; Thyregod, C.; Kørup, K.; Biltoft-Jensen, A.; Fagt, S.; Matthiessen, J.; Thyregod, C.; Kørup, K.; Biltoft-Jensen, A. Breakfast in Denmark. Prevalence of Consumption, Intake of Foods, Nutrients and Dietary Quality. A Study from the International Breakfast Research Initiative. Nutrients 2018, 10, 1085. [Google Scholar] [CrossRef] [PubMed]
- Gaal, S.; Kerr, M.A.; Ward, M.; McNulty, H.; Livingstone, M.B.E. Breakfast Consumption in the UK: Patterns, Nutrient Intake and Diet Quality. A Study from the International Breakfast Research Initiative Group. Nutrients 2018, 10, 999. [Google Scholar] [CrossRef] [PubMed]
- Bellisle, F.; Hébel, P.; Salmon-Legagneur, A.; Vieux, F. Breakfast Consumption in French Children, Adolescents, and Adults: A Nationally Representative Cross-Sectional Survey Examined in the Context of the International Breakfast Research Initiative. Nutrients 2018, 10, 1056. [Google Scholar] [CrossRef] [PubMed]
- Barr, S.I.; Vatanparast, H.; Smith, J. Breakfast in Canada: Prevalence of Consumption, Contribution to Nutrient and Food Group Intakes, and Variability across Tertiles of Daily Diet Quality. A Study from the International Breakfast Research Initiative. Nutrients 2018, 10, 985. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Rehm, C.; Vieux, F. Breakfast in the United States: Food and Nutrient Intakes in Relation to Diet Quality in National Health and Examination Survey 2011–2014. A Study from the International Breakfast Research Initiative. Nutrients 2018, 10, 1200. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, E.; Ávila, J.; Valero, T.; Rodriguez, P.; Varela-Moreiras, G. Breakfast Consumption in Spain: Patterns, Nutrient Intake and Quality. Findings from the ANIBES Study, a Study from the International Breakfast Research Initiative. Nutrients 2018, 10, 1324. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada Canadian Community Health Survey—Nutrition (CCHS). Available online: http://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&SDDS=5049 (accessed on 10 August 2018).
- National Food Institute; Technical University of Denmark Publikationer fra De Nationale Kostundersøgelser. DTU Fødevareinstituttet. Available online: http://www.food.dtu.dk/publikationer/ernaering-og-kostvaner/de_nationale_kostundersoegelser (accessed on 10 August 2018).
- Hébel, P.; Tavoularis, G.; Mathé, T. Comportements et Consommations Alimentaires en France; Hébel, P., Ed.; Tec & Doc Lavoisier: Paris, France, 2012; ISBN 978-2743014735. [Google Scholar]
- Ruiz, E.; Ávila, J.; Castillo, A.; Valero, T.; del Pozo, S.; Rodriguez, P.; Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.; et al. The ANIBES Study on Energy Balance in Spain: Design, Protocol and Methodology. Nutrients 2015, 7, 970–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Public Health England National Diet and Nutrition Survey. Available online: https://www.gov.uk/government/collections/national-diet-and-nutrition-survey (accessed on 10 August 2018).
- Centers for Disease Control and Prevention NHANES. About the National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 10 August 2018).
- Drewnowski, A. Uses of nutrient profiling to address public health needs: From regulation to reformulation. Proc. Nutr. Soc. 2017, 76, 220–229. [Google Scholar] [CrossRef] [PubMed]
- European Parliament. European Council Regulation (EU) No. 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the provision of food information to consumers. Off. J. Eur. Union 2011, L304/18, 18–63. [Google Scholar]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific Opinion on Dietary Reference Values for carbohydrates and dietary fibre. EFSA J. 2010, 8. [Google Scholar] [CrossRef] [Green Version]
- Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture; U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA, 2015.
- Health Canada Table of Daily Values. Available online: https://www.canada.ca/en/health-canada/services/technical-documents-labelling-requirements/table-daily-values.html (accessed on 9 August 2018).
- Food and Agriculture Organization of the United Nations. World Health Organization Guidelines on Nutrition Labelling CAC/GL 2-1985. 2017 Revision. Available online: http://www.fao.org/fao-who-codexalimentarius/sh-proxy/en/?lnk=1&url=https%253A%252F%252Fworkspace.fao.org%252Fsites%252Fcodex%252FStandards%252FCAC%2BGL%2B2-1985%252FCXG_002e.pdf (accessed on 9 August 2018).
- World Health Organization Healthy Diet—Fact Sheet n. 394. Available online: http://www.who.int/mediacentre/factsheets/fs394/en/ (accessed on 10 August 2018).
- Mann, J.; Cummings, J.H.; Englyst, H.N.; Key, T.; Liu, S.; Riccardi, G.; Summerbell, C.; Uauy, R.; van Dam, R.M.; Venn, B.; et al. FAO/WHO Scientific Update on carbohydrates in human nutrition: Conclusions. Eur. J. Clin. Nutr. 2007, 61, S132–S137. [Google Scholar] [CrossRef] [PubMed]
- USDA Food and Nutrition Service School Breakfast Program (SBP). Available online: https://www.fns.usda.gov/sbp/school-breakfast-program-sbp (accessed on 10 August 2018).
- Calvo, M.S.; Whiting, S.J.; Barton, C.N. Vitamin D fortification in the United States and Canada: Current status and data needs. Am. J. Clin. Nutr. 2004, 80, 1710S–1716S. [Google Scholar] [CrossRef] [PubMed]
- Canadian Food Inspection Agency Foods to Which Vitamins. Mineral Nutrients and Amino Acids May or Must be Added [D.03.002, FDR]. Available online: http://inspection.gc.ca/food/labelling/food-labelling-for-industry/nutrient-content/reference-information/eng/1389908857542/1389908896254?chap=1 (accessed on 10 August 2018).
- US Food & Drug Administration Guidance for Industry: Questions and Answers on FDA’s Fortification Policy. Available online: https://www.fda.gov/Food/GuidanceRegulation/GuidanceDocumentsRegulatoryInformation/ucm470756.htm (accessed on 10 August 2018).
- Institute of Medicine (US) Committee on Use of Dietary Reference Intakes in Nutrition Labeling. Overview of Food Fortification in the United States and Canada. In Dietary Reference Intakes: Guiding Principles for Nutrition Labeling and Fortification; National Academies Press (US): Washington, DC, USA, 2003. [Google Scholar]
- Arbeitskreis Jodmangel Discussion Paper on the Setting of Maximum and Minimum Amounts for Vitamins and Minerals in Foodstuffs. Available online: https://ec.europa.eu/food/sites/food/files/safety/docs/labelling_nutrition-supplements-responses-akj_en.pdf (accessed on 10 August 2018).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Study Name, Year and Reference | Diet Assessment Method | Breakfast Definition | Number of Participants with Complete Dietary Information | |||
|---|---|---|---|---|---|---|---|
| Children (6–12 Years) | Adolescents (13–17 Years) | Younger Adults (18–54 Years) | Older Adults (55+ Years) | ||||
| Canada | CCHS-Nutrition 2015 [22] | 1-day 24 h recall | Self-defined | 2331 | 2026 | 7631 | 6279 |
| Denmark | Danish national survey of diet and physical activity 2011-2013 [23] | 7-day food record | Section in questionnaire | 476 | 272 | 1791 | 1118 |
| France | CCAF 2013 [24] | 7-day food record | Self-defined | 426 | 250 | 595 | 445 |
| Spain $ | ANIBES 2013 [25] | 3-day diet recall | Section in questionnaire | 213 | 211 | 1655 | 206 |
| UK * | NDNS 2008-14 [26] | 4-day estimated food diary | All items consumed between 6–11 a.m. | 1947 | 1534 | 3619 | 1074 |
| US | NHANES 2011-14 [27] | 1-day 24 h recall | Self-defined. Intake > 50 kcal | 2511 | 1546 | 6594 | 3837 |
| Nutrient | Breakfast Intakes in NRF T3 (Quantity) | Intakes as % Breakfast Energy or % NRV 1 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Canada | Denmark | France | Spain | UK 4 | US | Canada | Denmark | France | Spain | UK 4 | US | |
| Energy (kcal) | 368 | 387 | 384 | 348 | 347 | 366 | ||||||
| Total Carbohydrates (g) 1 | 56 | 62 | 60 | 47 | 54 | 57 | 61.5 | 62.5 | 63.0 | 55.0 | 61.0 | 65.0 |
| Added sugars (g) 1,2 | n/a | 6.6 | 16.4 | 12.4 | 13 | 12.2 | n/a | 6.8 | 16.0 | 15.5 | 14.0 | 14.0 |
| Total Fat (g) 1 | 10.4 | 9.2 | 10.8 | 11.6 | 10 | 10.1 | 23.1 | 21.3 | 25.0 | 31.0 | 25.0 | 23.0 |
| Saturated Fat (g) 1 | 4 | 3.9 | 5.4 | 5 | 4 | 4 | 9.4 | 9.1 | 12.5 | 15.6 | 11.0 | 10.0 |
| Protein (g) 1 | 14.4 | 15.7 | 11.8 | 11.5 | 12 | 13.7 | 28.8 | 31.3 | 23.4 | 23.0 | 24.0 | 27.4 |
| Fiber 3 (g) | 4.1 | 5 | 2.8 | 1.3 | 3.7 | 3.4 | 16.2 | 20.0 | 11.2 | 5.4 | 14.8 | 13.6 |
| Sodium (mg) | 424 | 386 | 350 | 385 | 356 | 454 | 21.2 | 19.3 | 16.9 | 19.3 | 17.8 | 22.7 |
| Vitamin A (mg) | 181 | 102 | 80 | 57 | 107 | 294 | 22.6 | 12.8 | 10.1 | 7.1 | 13.4 | 36.8 |
| Thiamin (mg) | 0.5 | 0.3 | 0.4 | 0.3 | 0.4 | 0.6 | 43.3 | 26.7 | 33.3 | 20.8 | 33.3 | 50.0 |
| Riboflavin (mg) | 0.6 | 0.5 | 0.6 | 0.5 | 0.7 | 0.9 | 52.5 | 40.8 | 50.0 | 41.7 | 58.3 | 75.0 |
| Niacin (mg) | 6.4 | 4.0 | 3.8 | 4.1 | 7 | 6.3 | 42.4 | 26.5 | 25.3 | 27.3 | 46.7 | 42.0 |
| Vitamin B6 (mg) | 0.4 | 0.3 | 0.5 | 0.3 | 0.6 | 0.7 | 27.7 | 19.2 | 38.5 | 23.1 | 46.2 | 53.8 |
| Vitamin B12 (mcg) | 1.2 | 1.1 | 0.6 | 0.7 | 1.4 | 2.4 | 50.8 | 45.0 | 25.0 | 29.2 | 58.3 | 100.0 |
| Vitamin C (mg) | 20.7 | 16.0 | 28 | 8.5 | 22 | 28 | 20.7 | 16.0 | 33.0 | 8.5 | 22.0 | 28.0 |
| Vitamin D (mcg) | 2.5 | 0.3 | 0.2 | 0.2 | 0.7 | 3.4 | 50.8 | 5.0 | 4.0 | 4.8 | 14.0 | 68.0 |
| Folate (mcg) | 95 | 64 | 67 | 38 | 79 | 167 | 23.9 | 16.0 | 17.5 | 9.5 | 19.8 | 41.8 |
| Calcium (mg) | 328 | 339 | 320 | 304 | 260 | 370 | 32.8 | 33.9 | 32.1 | 30.4 | 26.0 | 37.0 |
| Iron (mg) | 4.1 | 2.2 | 3.5 | 2 | 3.3 | 6.3 | 29.0 | 15.6 | 24.3 | 14.3 | 23.6 | 45.0 |
| Potassium (mg) | 590 | 600 | 630 | 541 | 523 | 581 | 16.9 | 17.1 | 18.3 | 15.5 | 14.9 | 16.6 |
| Magnesium (mg) | 72 | 99 | 73 | 42 | 53 | 63 | 23.4 | 31.9 | 23.5 | 13.5 | 17.1 | 20.3 |
| Zinc (mg) | 2.2 | 2.2 | 1.6 | 1.2 | 1.5 | 3.5 | 20.4 | 19.8 | 14.5 | 10.9 | 13.6 | 31.8 |
| Nutrient | Breakfast Intakes in NRF T3 (Quantity) | Intakes as % Breakfast Energy or % NRV 1 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Canada | Denmark | France | Spain | UK 4 | US | Canada | Denmark | France | Spain | UK 4 | US | |
| Energy (kcal) | 381 | 402 | 343 | 290 | 325 | 415 | ||||||
| Total Carbohydrates (g) 1 | 57.4 | 61 | 54.6 | 39.2 | 52 | 63.3 | 57.4 | 58.4 | 63.6 | 56.2 | 61.0 | 62.9 |
| Added sugars (g) 1,2 | n/a | 6.8 | 12.4 | 6.2 | 11 | 11.6 | n/a | 6.5 | 16.0 | 11.6 | 12.0 | 11.5 |
| Total Fat (g) 1 | 11.4 | 11.2 | 9.5 | 8.8 | 9 | 12.3 | 24.4 | 24.5 | 24.2 | 28.4 | 24.0 | 24.6 |
| Saturated Fat (g) 1 | 3.7 | 4.7 | 4.5 | 3.1 | 3 | 4 | 8.2 | 10.3 | 11.5 | 11.7 | 9.0 | 8.2 |
| Protein (g) 1 | 15 | 16.8 | 9.9 | 10.1 | 12 | 16.4 | 30.0 | 33.6 | 19.8 | 20.2 | 24.0 | 32.8 |
| Fiber 3 (g) | 6 | 5.8 | 3.3 | 1.8 | 4.6 | 5.5 | 23.8 | 23.2 | 13.2 | 7.0 | 18.4 | 22.2 |
| Sodium (mg) | 423 | 409 | 400 | 293 | 337 | 507 | 21.2 | 20.5 | 20.0 | 14.7 | 16.9 | 25.4 |
| Vitamin A (mg) | 166 | 112 | 81.6 | 27.7 | 97 | 306 | 20.8 | 14.0 | 10.2 | 3.5 | 12.1 | 38.3 |
| Thiamin (mg) | 0.5 | 0.3 | 0.2 | 0.2 | 0.4 | 0.6 | 40.8 | 24.2 | 16.7 | 17.5 | 33.3 | 46.7 |
| Riboflavin (mg) | 0.6 | 0.5 | 0.4 | 0.4 | 0.6 | 0.9 | 49.2 | 37.5 | 33.3 | 33.3 | 50.0 | 75.8 |
| Niacin (mg) | 7.3 | 5.6 | 3.3 | 3.7 | 7 | 6.6 | 48.5 | 37.2 | 22.0 | 24.7 | 46.7 | 43.8 |
| Vitamin B6 (mg) | 0.4 | 0.3 | 0.3 | 0.2 | 0.5 | 0.8 | 29.2 | 19.2 | 23.1 | 16.2 | 38.5 | 62.3 |
| Vitamin B12 (mcg) | 1.0 | 1.0 | 0.4 | 0.5 | 1.3 | 2.3 | 39.6 | 42.1 | 16.7 | 21.3 | 54.2 | 95.8 |
| Vitamin C (mg) | 28 | 21 | 22 | 10 | 23 | 35 | 27.8 | 21.4 | 21.8 | 10.0 | 23.0 | 34.7 |
| Vitamin D (mcg) | 1.8 | 0.4 | 0.2 | 0.1 | 0.8 | 2.8 | 36.0 | 8.2 | 4.0 | 1.0 | 16.0 | 55.8 |
| Folate (mcg) | 103 | 72.2 | 49.3 | 29 | 76 | 265 | 25.8 | 18.1 | 12.3 | 7.4 | 19.0 | 66.3 |
| Calcium (mg) | 262 | 357 | 228 | 221 | 232 | 348 | 26.2 | 35.7 | 22.8 | 22.1 | 23.2 | 34.8 |
| Iron (mg) | 3.8 | 2.2 | 2.5 | 1.7 | 3 | 6.8 | 26.9 | 15.6 | 17.9 | 11.9 | 21.4 | 48.5 |
| Potassium (mg) | 695 | 726 | 665 | 477 | 637 | 789 | 19.9 | 20.7 | 19.0 | 13.6 | 18.2 | 22.5 |
| Magnesium (mg) | 96.1 | 111 | 82.3 | 46.6 | 68 | 95.3 | 31.0 | 35.8 | 26.5 | 15.0 | 21.9 | 30.7 |
| Zinc (mg) | 2.4 | 2.4 | 1.5 | 1.2 | 1.6 | 3.7 | 21.3 | 21.7 | 13.6 | 10.6 | 14.5 | 33.9 |
| Nutrient | Children and Adolescents | Adults | World Health Organization (WHO)/CODEX International Food Standards Daily Recommended Value [33,34,35] |
|---|---|---|---|
| Principle 1 | |||
| Energy (kcal) | 300–500 | 300–500 | |
| Principle 2 | |||
| Protein (% NRV) | >20 | >20 | 50 g |
| Vitamin A (% NRV) | >10 | >10 | 800 mg |
| Thiamin (B1) (% NRV) | >25 | >20 | 1.2 mg |
| Riboflavin (B2) (% NRV) | >35 | >30 | 1.2 mg |
| Niacin (B3) (% NRV) | >25 | >25 | 15 mg |
| Vitamin B6 (% NRV) | >20 | >20 | 1.3 mg |
| Vitamin B12 (% NRV) | >25 | >20 | 2.4 mcg |
| Principle 3 | |||
| Calcium (% NRV) | >30 | >25 | 1000 mg |
| Total carbohydrates (%en) | 55–75 | 55–75 | 55–75 %energy |
| Principle 4 | |||
| Fiber (% NRV) | >20 | >20 | 25 g |
| Vitamin C (% NRV) | >20 | >20 | 100 mg |
| Vitamin D (% NRV) | >20 | >20 | 5 mcg |
| Folate (% NRV) | >20 | >20 | 400 mcg |
| Iron (% NRV) | >20 | >20 | 14 mg |
| Potassium (% NRV) | >20 | >20 | 3500 mg |
| Magnesium (% NRV) | >20 | >20 | 310 mg |
| Zinc (% NRV) | >20 | >20 | 11 mg |
| Sodium (% NRV) | <20 | <20 | 2000 mg |
| Principle 5 | |||
| Added sugars (%en) | <10 | <10 | <10 %energy |
| Total Fat (%en) | 20–30 | 20–30 | <30 %energy |
| Saturated Fat (%en) | <10 | <10 | <10 %energy |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gibney, M.J.; Barr, S.I.; Bellisle, F.; Drewnowski, A.; Fagt, S.; Hopkins, S.; Livingstone, B.; Varela-Moreiras, G.; Moreno, L.; Smith, J.; et al. Towards an Evidence-Based Recommendation for a Balanced Breakfast—A Proposal from the International Breakfast Research Initiative. Nutrients 2018, 10, 1540. https://doi.org/10.3390/nu10101540
Gibney MJ, Barr SI, Bellisle F, Drewnowski A, Fagt S, Hopkins S, Livingstone B, Varela-Moreiras G, Moreno L, Smith J, et al. Towards an Evidence-Based Recommendation for a Balanced Breakfast—A Proposal from the International Breakfast Research Initiative. Nutrients. 2018; 10(10):1540. https://doi.org/10.3390/nu10101540
Chicago/Turabian StyleGibney, Michael J., Susan I. Barr, France Bellisle, Adam Drewnowski, Sisse Fagt, Sinead Hopkins, Barbara Livingstone, Gregorio Varela-Moreiras, Luis Moreno, Jessica Smith, and et al. 2018. "Towards an Evidence-Based Recommendation for a Balanced Breakfast—A Proposal from the International Breakfast Research Initiative" Nutrients 10, no. 10: 1540. https://doi.org/10.3390/nu10101540