1. Introduction
Evidence suggests that regular breakfast consumption is associated with lower body mass index (BMI) [
1,
2,
3,
4], cardiovascular risk [
5,
6,
7,
8,
9] and enhanced cognitive function [
10]. However, although the UK government has been actively promoting breakfast consumption as part of a balanced diet through the “Change4Life” campaign [
11], it is estimated that 6% of children aged 7–10 years, 15–26% of adolescents aged 11–15 years and 31% of adults regularly skip breakfast [
11].
Dietary recommendations in the UK suggest that a healthy breakfast should contribute around 20–25% to total daily energy and nutrient intake [
12] and foods should be selected from five main food groups, namely: Starchy foods (cereals, pasta, bread), fruit and vegetables, milk and dairy, protein sources and low-fat spreads and oils [
12]. In children aged 5–18 years, the Caroline Walker Trust recommends that breakfast energy and macronutrient contribution should be 20% of the estimated average requirement (EAR) and food energy respectively and that the contribution of breakfast to overall micronutrient intake should be 20% of the Reference Nutrient Intake (RNI) [
13]. However, these guidelines are based on the Eatwell Guide and not on actual breakfast food and nutrient intakes of the population [
14]. While regular breakfast consumers are reported to have higher nutrient intakes [
2,
15,
16,
17,
18], and better overall dietary adequacy [
15,
18] and quality [
16,
19,
20] than non-regular consumers, there is no quantitative nutrient guidance in relation to an appropriate breakfast composition.
Among UK adults, a cereal based breakfast has been associated with significantly lower intakes of total fat, saturated fatty acid (SFA) and non-milk extrinsic sugars (NMES) and higher intakes of protein, carbohydrate, fibre, B vitamins, vitamin C, D, calcium and iron in comparison to a non-cereal based breakfast or no breakfast [
21]. Among UK children (aged 4–10 years) and adolescents (aged 11–18 years), regular breakfast consumers are reported to have significantly higher energy adjusted intakes of dietary fibre, vitamin C, folate, calcium, iron and iodine in comparison to breakfast skippers of the same age [
22]. Furthermore, higher total dietary adequacy, in terms of meeting the RNI for vitamin C, folate, calcium, iron and iodine is more readily achieved among children who report regular breakfast consumption compared with children who report breakfast skipping [
22].
One of the major limitations in generating quantitative recommendations for breakfast has been the lack of consensus on how breakfast should be defined [
14]. Previous UK studies investigating breakfast consumption based on National Diet and Nutrition Survey data applied an arbitrary time frame for any item consumed between 6 a.m.–10 a.m. [
21] and 6 a.m.–8:59 a.m. with a 100 kcal cut off [
22]. Other time frames, energy contribution values and inclusion/exclusion of specific food and beverage groups have also been used as breakfast definitions [
23]. A recent definition by O’Neil et al. [
23] has been proposed as the basis for providing a consistent approach in future studies: “
Breakfast is the first meal of the day that breaks the fast after the longest period of sleep and is consumed within 2 to 3 h of waking;
it is comprised of food or beverage from at least one food group,
and may be consumed at any location” [
23]. The application of the above definition however could lead to inaccurate profiling of breakfast intakes due to differences in dietary survey methodologies [
14]. In the UK National Diet and Nutrition Survey (NDNS), breakfast is not pre-defined in the food diary, nor self-defined among NDNS participants. In addition, there is no report of waking time.
The International Breakfast Research Initiative (IBRI) was established to provide evidence based dietary guidelines for nutrient intakes at breakfast by assessing breakfast consumption in representative dietary surveys of the following six countries: Canada, Denmark, France, Spain, UK and the US. The objective of the current paper was to present breakfast consumption patterns, nutrient and food group intakes at breakfast and their contribution to daily intakes in a representative sample of the UK population. Breakfast was defined as any food or beverage item consumed between 6 a.m.–11 a.m. to accommodate different consumption patterns between weekdays and weekend days. The relationship between nutrient and food group intakes at breakfast and overall diet quality using the Nutrient Rich Food Index 9.3 scoring method is also examined according to age.
4. Discussion
The collaborative International Breakfast Research Initiative (IBRI) aims to provide evidence based dietary guidelines for nutrient intakes at breakfast based on nationally representative dietary surveys across six countries: Canada, Denmark, France, Spain, UK and US. This paper presents breakfast consumption patterns, nutrient and food group intakes at breakfast and their contribution to daily intakes in a representative sample of the UK population. The relationship between nutrient and food group intakes at breakfast and overall diet quality are also examined according to age.
Although the aim of the IBRI collaboration was to apply a harmonised approach to defining breakfast, it was evident that the application of a standard breakfast definition proposed by O’Neil et al. [
23] to the UK data presented a particular challenge and it would not fully account for breakfast eating behaviour in the UK. Specifically, breakfast was not defined in the food diary or self-defined by the NDNS participants and no information was provided on waking time. Furthermore, out of the first reported NDNS eating occasions each day (from midnight to midnight), 2.7% took place between midnight and 6 a.m. and 3.3% took place between midday and 11 pm, time frames which may not necessarily include consumption of a typical breakfast meal. Based on an iterative process it was concluded in the current study that the time window of 6 a.m. and 11 a.m. including weekdays and weekend days would best capture breakfast eating behaviour in the UK.
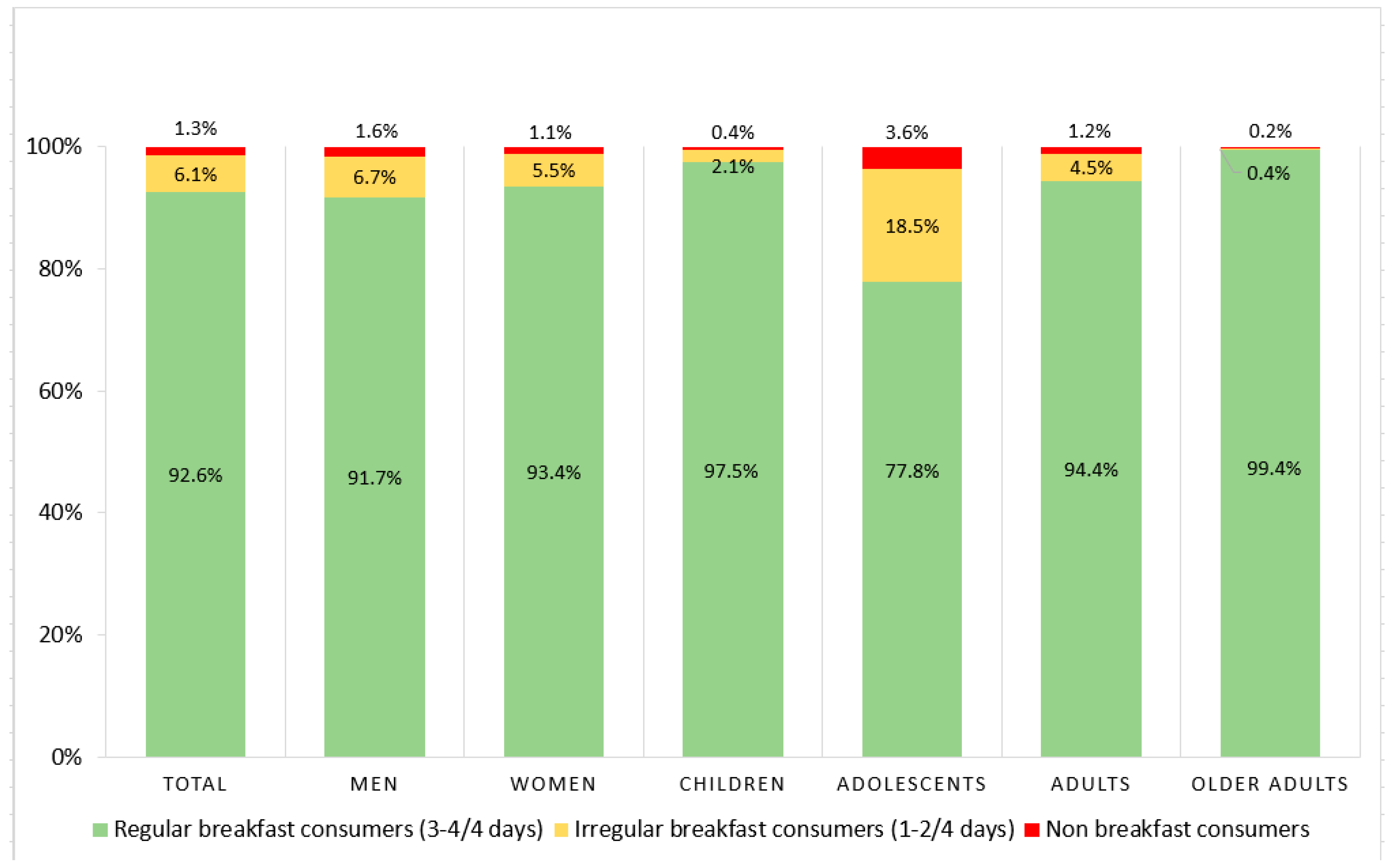
The present study has shown that the majority of the UK population (92.6%) are regular breakfast consumers, consuming breakfast on at least 3 of the 4 days examined. The prevalence of irregular breakfast consumption, defined as consumption of breakfast on 2 or less days, was found to be highest among adolescents aged 13–18 years (18.5%). This is consistent with findings from previous studies conducted among adolescents in the UK and elsewhere [
22,
34,
35] with differences in family structures, ethnicity [
36], lower socioeconomic status [
37,
38,
39], time constraints [
40,
41] and lack of enjoyment of food in the morning [
41] reported to play a role in these trends.
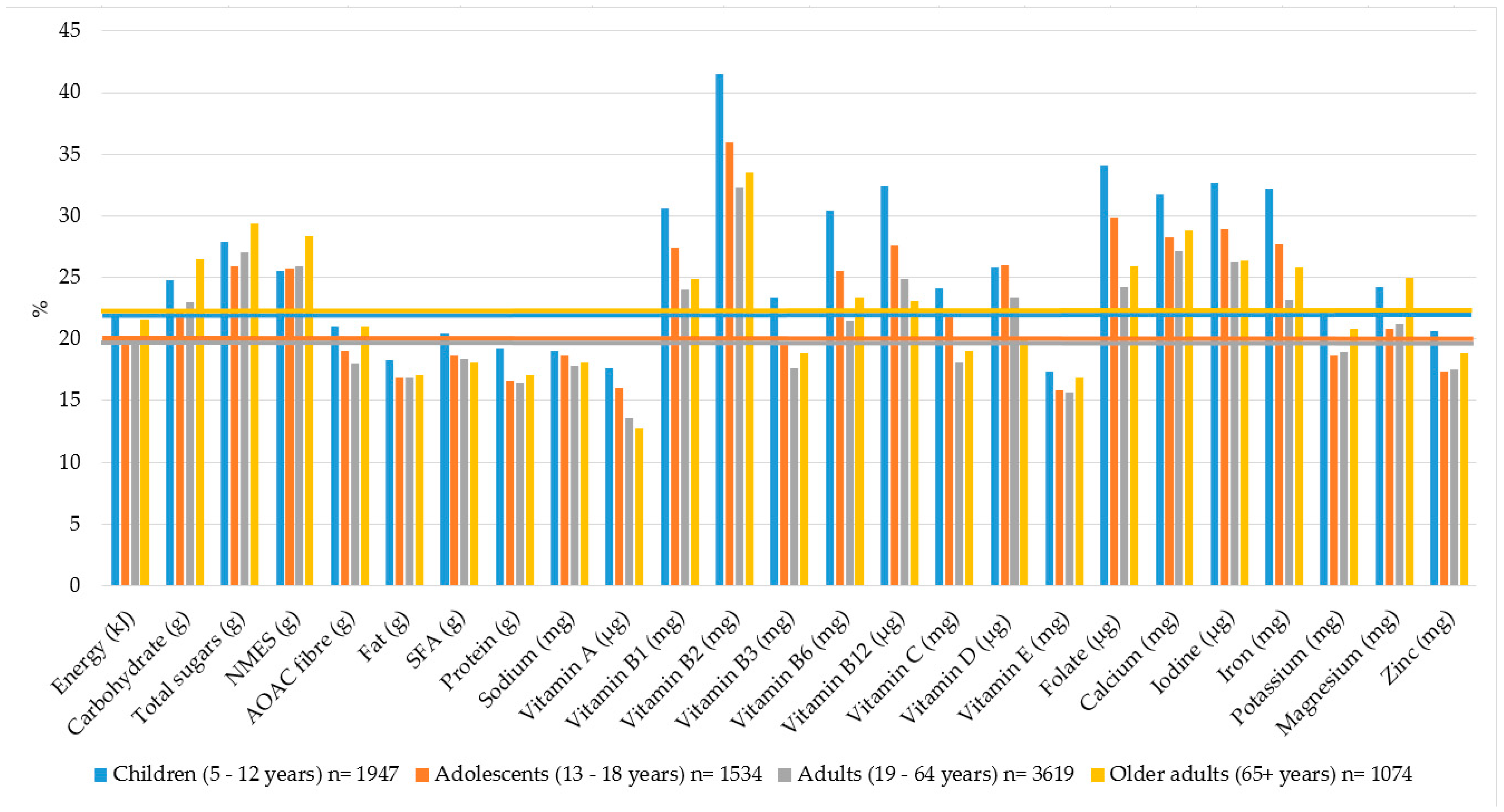
The key findings of the present study are that breakfast contributed 20–22% to total daily energy intake across all age groups which is consistent with existing recommendations [
23]. Notably, however, breakfast contributed marginally more to daily intake of carbohydrate, total sugars and NMES (22–29%) and less to total daily intake of protein, total fat, SFA and dietary fibre (16–21%) compared to the recommended 20–25% by the BDA and the Caroline Walker Trust [
12,
13]. The recent UK “Sugar reduction programme” aims to reduce total sugar intake and where possible energy without the increase of SFA and salt from the highest contributing food groups by 20% by 2020 [
42]. In the first year of the programme, the sugar reduction target of 5% has been largely achieved through reformulation of foods commonly consumed at breakfast such as breakfast cereals [
42]. In addition, soft drink reformulation is promoted by the Soft Drinks Industry Levy (SDIL), which took effect in April 2018 and aims to tax soft drinks containing 5–8 g of sugar per 100 mL [
42]. The longer-term consequence of the reformulation of foods and drinks typically consumed at breakfast remain to be established.
Opinions vary as to the optimal macronutrient composition of breakfast [
43]. Some studies suggest that a high Glycemic Index (GI)/Glycemic Load (GL) breakfast may have a beneficial effect on cognitive function in participants with normal glucose metabolism, whereas a low-GI/GL breakfast may be more effective on cognition in participants with impaired glucose metabolism [
44]. On the other hand, total carbohydrate intake in the highest quintile in comparison to the lowest is reported to increase type 2 diabetes risk whereas partial replacement with dietary fibre may have more favourable metabolic health outcomes [
43]. Evidence shows no significant difference in appetite and ad libitum energy intake between a high protein (58.1% protein, 14.1% carbohydrate) versus a high-carbohydrate (19.3% protein, 47.3% carbohydrate) breakfast, although a high-protein breakfast was more effective at reducing postprandial ghrelin concentrations in healthy men [
45]. Further recent research has shown that a high-fat breakfast (35% carbohydrate, 20% protein, 45% fat) may be more effective at reducing metabolic disease risk in healthy adults compared to a high-carbohydrate breakfast (60% carbohydrate, 20% protein, 20% fat) [
46]. These findings suggest that breakfast compositions higher in protein, fat and fibre and lower in carbohydrate may have a more favourable effect on metabolic disease risk.
Current available UK-based breakfast recommendations suggest that breakfast should contribute 20% to daily micronutrient intakes [
13]. In the present study, the contribution of breakfast to total daily intake of B vitamins, vitamin D, calcium, iodine and iron ranged from 20–41% across all age groups. Thus, breakfast is a particularly nutrient-dense meal in the UK. Previous studies have also observed higher micronutrient intakes [
2,
15,
16,
17,
18] and improved overall dietary adequacy [
15,
18] in breakfast consumers. This was found to be mostly the case for children aged 5–12 years in the present study, with lower contributions noted with increasing age. Age differences in breakfast micronutrient intakes were also observed in a previous UK study where children aged 4–10 years had higher intakes of fibre, folate, vitamin C and iodine on breakfast consuming days, whereas no significant differences in intakes were observed among adolescents aged 11–18 years [
22]. These findings highlight the importance of maintaining consumption patterns and nutrient intakes from childhood into adolescent age and beyond, especially as eating habits established during childhood tend to track into adulthood [
47].
The higher micronutrient intakes at breakfast observed in the current study are likely to be at least partially driven by current UK fortification practices. For example, white bread is mandatorily fortified with vitamin B1, B3, iron and calcium [
48]. Furthermore, breakfast cereals, dairy products and fat spreads are fortified on a voluntary basis with vitamin A, D, C, B12 and folate [
48]. Consequently, high-fibre and other breakfast cereals, milk, white bread and reduced fat spread were the highest contributors to micronutrient intakes, as well as to energy and fibre. Similarly, ready-to-eat breakfast cereal consumption has been associated with higher fibre and micronutrient intake in other population groups including older American adults [
17], Australian children and adolescents [
49], low-income UK population [
50], Spanish children and adolescents [
16] and Black adolescents [
51]. Notably, fortified breakfast cereal consumption has been associated with higher dietary adequacy, specifically in relation to the B vitamins, vitamin D and iron, without the risk of exceeding the Tolerable Upper Intake Level intake [
52].
This study is the first to investigate the relationship between nutrient intakes at breakfast and overall diet quality in the UK by using the Nutrient Rich Food Index 9.3 (NRF 9.3) scoring method and a positive impact of breakfast was observed on overall DQ in both children and adults. The Healthy Eating Index (HEI) and Dietary Diversity Score (DDS) have been used previously to assess the association between breakfast consumption, skippers and diet quality in Iranian women [
19], in American adults [
53] and American women [
54]. It must be noted, however, that in the present study, comparisons of nutrient and food intakes were made based on tertiles of overall DQ in breakfast consumers only; therefore, our results cannot be compared with findings of previous studies which differentiated between breakfast consumers and breakfast skippers [
19,
53,
54]. Nevertheless, higher DQ in the current study corresponded to higher carbohydrate, protein and fibre intakes and lower NMES, total fat and SFA intakes at breakfast. Furthermore, intakes of folate, calcium, iodine, iron, potassium and magnesium and lower intake of sodium at breakfast were observed in the highest DQ tertile in both children and adults. It is also important to note however that actual mean intakes particularly of fibre, calcium, potassium and magnesium differed between children and adults, suggesting the need for age-specific dietary guidelines at breakfast.
Significant differences were observed in food (g) and beverage (mL) group intakes at breakfast across tertiles of DQ at the total population level; however, intakes were similar across the DQ tertiles in consumers only. These results suggest that there is a tendency towards the choice and consumption of the same food groups. Importantly, also, food group intakes observed in the current study within the highest DQ tertile are consistent with existing UK breakfast recommendations, which suggests the selection of breakfast cereals, wholegrain varieties, semi skimmed milk, fruit, low fat spreads, egg dishes and the limitation of fizzy drinks, biscuits and crisps at breakfast [
12]. Future studies could consider the development of coding systems [
55,
56] and the use of Principal Component Analysis (PCA) to identify key food patterns in relation to nutrient intakes [
55,
56], which may help to inform the evidence base.
There are various limitations to the current study which must be acknowledged. Firstly, the cross-sectional design of the study only provides data on prevalence and trends of breakfast patterns in the UK population and a direct link between breakfast intake and dietary adequacy cannot be confirmed. In addition, the breakfast definition used in the current study included both weekdays and weekend days and bias cannot be ruled out due to different associated consumption patterns. Furthermore, weekend days were overrepresented in the NDNS between 2008–2012 [
24]. It is also important to note that the contribution of dietary supplements was excluded from the data analysis; however, supplement users, who generally have higher dietary intakes of micronutrients regardless of supplementation [
24], were retained. Finally, misreporting of food intake cannot be ruled out in dietary surveys. Exclusion of either under- or over-reporters could, however, have introduced selection and unknown bias [
57], for the purpose of the current study, therefore, implausible reporters were not excluded; instead, energy intake was controlled for in statistical analysis.
In conclusion, the current study has observed that the majority of the UK population are regular breakfast consumers, and breakfast typically contributes 20–22% to total daily energy intake across all age groups. Furthermore, intakes of carbohydrate and NMES at breakfast are typically higher and intakes of protein, total fat and SFA are typically lower at breakfast than for the total day in this cohort. The current study has also provided evidence that the UK breakfast is a micronutrient rich meal across all age groups, impacting particularly on daily intakes of key nutrients including vitamin D, calcium and folate. The results from this study also provide strong evidence for a positive impact of breakfast consumption on overall diet quality. These findings could help to inform the development of nutrient based recommendations for a balanced breakfast for the first time in the UK.





{kind=link}
{kind=link}