
The Chronic Effect of Stair Climbing–Descending Exercises after Meals on Glycemic Control in Individuals with Type 2 Diabetes: A Randomized Controlled Trial
 , and
, and
Abstract
:1. Introduction
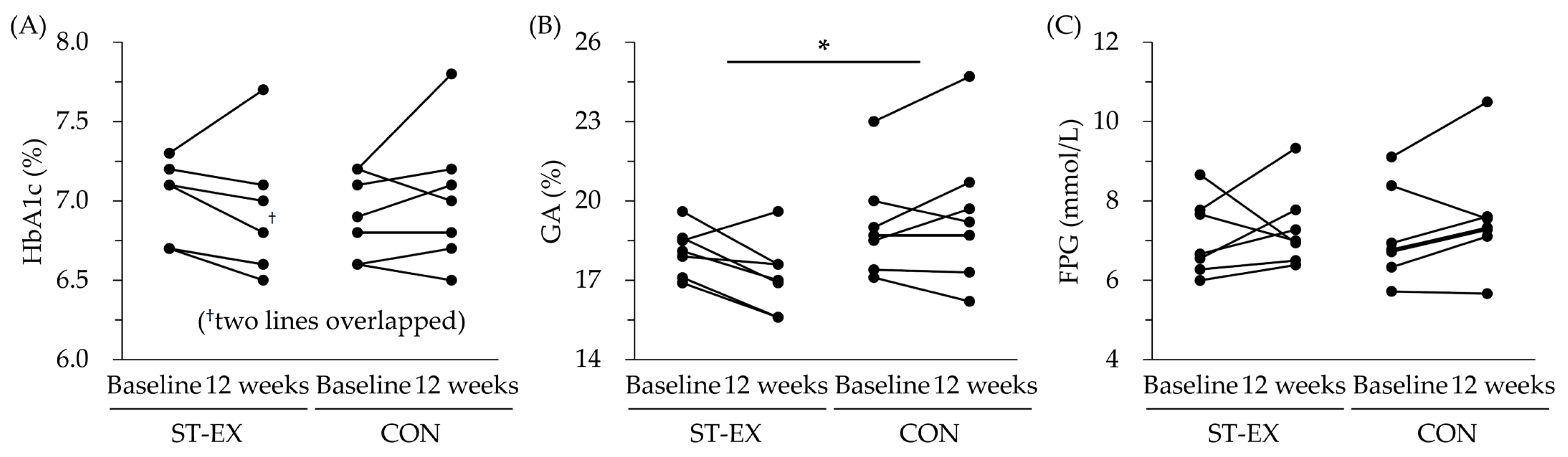
2. Results
3. Discussion
4. Materials and Methods
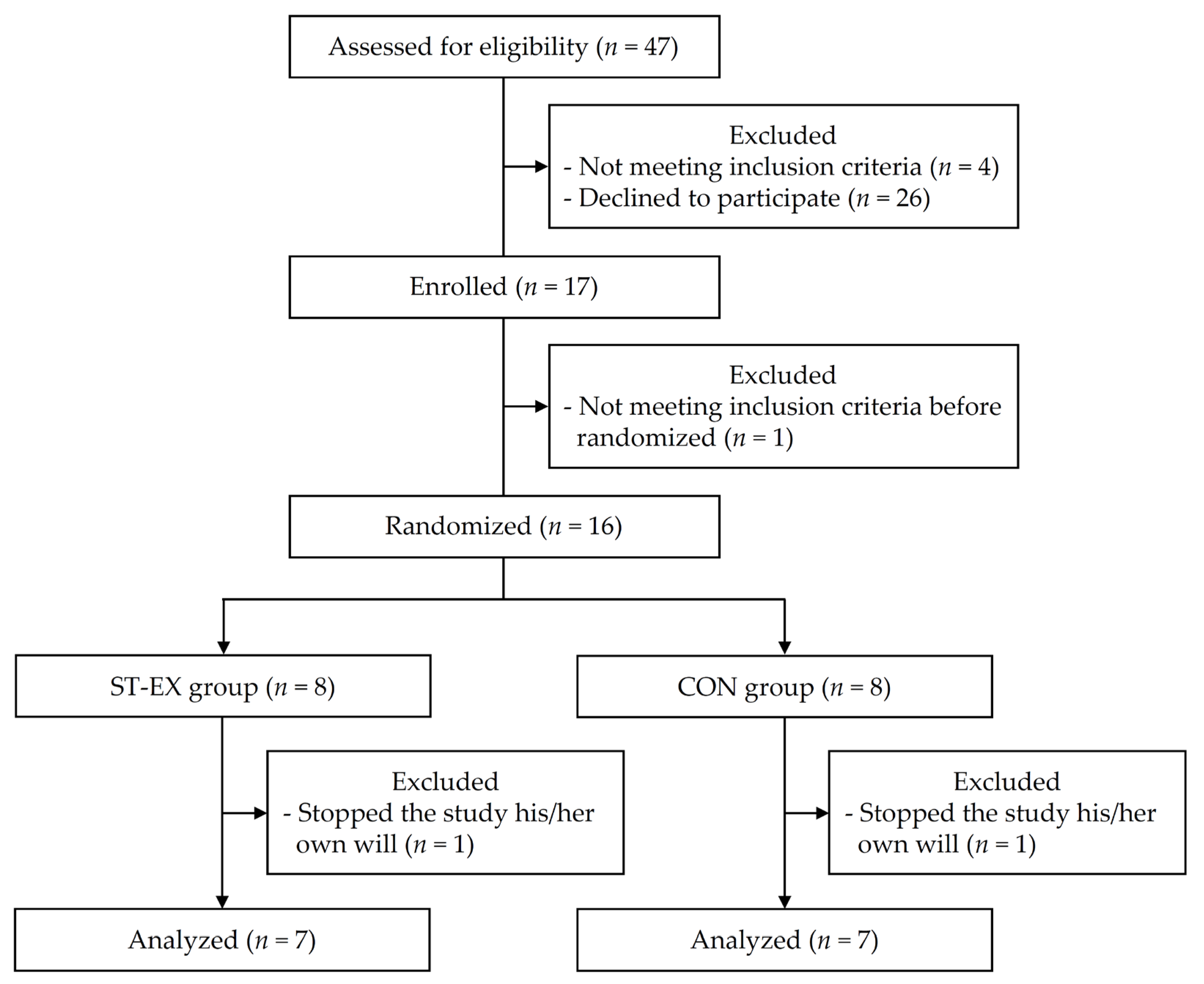
4.1. Participants
4.2. Study Design
4.3. Exercise Protocol
4.4. Measurements
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 5. Facilitating Positive Health Behaviors and Well-being to Improve Health Outcomes: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46, S68–S96. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Xu, J.; Yang, X.; Li, L.; Jia, X.; Yu, J.; Li, N.; Zhang, Y. Acute high intensity interval exercise is similarly effective as moderate intensity continuous exercise on plasma glucose control in type 2 diabetic men aged 30 to 50 years: A randomized controlled trial. J. Sports Med. Phys. Fit. 2022, 62, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Mendes, R.; Sousa, N.; Themudo-Barata, J.L.; Reis, V.M. High-Intensity Interval Training Versus Moderate-Intensity Continuous Training in Middle-Aged and Older Patients with Type 2 Diabetes: A Randomized Controlled Crossover Trial of the Acute Effects of Treadmill Walking on Glycemic Control. Int. J. Environ. Res. Public Health 2019, 16, 4163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francois, M.E.; Baldi, J.C.; Manning, P.J.; Lucas, S.J.; Hawley, J.A.; Williams, M.J.; Cotter, J.D. ‘Exercise snacks’ before meals: A novel strategy to improve glycaemic control in individuals with insulin resistance. Diabetologia 2014, 57, 1437–1445. [Google Scholar] [CrossRef] [PubMed]
- Gillen, J.B.; Little, J.P.; Punthakee, Z.; Tarnopolsky, M.A.; Riddell, M.C.; Gibala, M.J. Acute high-intensity interval exercise reduces the postprandial glucose response and prevalence of hyperglycaemia in patients with type 2 diabetes. Diabetes Obes. Metab. 2012, 14, 575–577. [Google Scholar] [CrossRef]
- Karstoft, K.; Christensen, C.S.; Pedersen, B.K.; Solomon, T.P. The acute effects of interval- Vs continuous-walking exercise on glycemic control in subjects with type 2 diabetes: A crossover, controlled study. J. Clin. Endocrinol. Metab. 2014, 99, 3334–3342. [Google Scholar] [CrossRef] [Green Version]
- Gentil, P.; Silva, L.; Antunes, D.E.; Carneiro, L.B.; de Lira, C.A.B.; Batista, G.; de Oliveira, J.C.M.; Cardoso, J.S.; Souza, D.C.; Rebelo, A.C.S. The effects of three different low-volume aerobic training protocols on cardiometabolic parameters of type 2 diabetes patients: A randomized clinical trial. Front. Endocrinol. 2023, 14, 985404. [Google Scholar] [CrossRef]
- Honda, H.; Igaki, M.; Hatanaka, Y.; Komatsu, M.; Tanaka, S.; Miki, T.; Suzuki, T.; Takaishi, T.; Hayashi, T. Stair climbing/descending exercise for a short time decreases blood glucose levels after a meal in people with type 2 diabetes. BMJ Open Diabetes Res. Care 2016, 4, e000232. [Google Scholar] [CrossRef] [Green Version]
- Honda, H.; Igaki, M.; Komatsu, M.; Tanaka, S.-I.; Takaishi, T.; Hayashi, T. Stair climbing–descending exercise following meals improves 24-hour glucose excursions in people with type 2 diabetes. J. Phys. Fit. Sports Med. 2021, 10, 51–56. [Google Scholar] [CrossRef]
- Honda, H.; Igaki, M.; Hatanaka, Y.; Komatsu, M.; Tanaka, S.I.; Miki, T.; Matsuki, Y.; Takaishi, T.; Hayashi, T. Repeated 3-minute stair climbing-descending exercise after a meal over 2 weeks increases serum 1,5-anhydroglucitol levels in people with type 2 diabetes. J. Phys. Ther. Sci. 2017, 29, 75–78. [Google Scholar] [CrossRef] [Green Version]
- Stettler, C.; Stahl, M.; Allemann, S.; Diem, P.; Schmidlin, K.; Zwahlen, M.; Riesen, W.; Keller, U.; Christ, E. Association of 1,5-anhydroglucitol and 2-h postprandial blood glucose in type 2 diabetic patients. Diabetes Care 2008, 31, 1534–1535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare. Standard Questionnaire of Specific Health Checkups. Available online: http://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/13_44.pdf (accessed on 2 March 2023).
- Portela, P.F.M.; Neto, V.G.C.; Monteiro, E.R.; Santos da Silva, R.; da Silva, V.F.; Nogueira, C.J.; Schutz, S.; Scudese, E.; Salvino, A.K.S.; Valentim-Silva, J.R. HIIT is most effective than mict on glycemic control of older people with glucose metabolism impairments: A systematic review and metanalysis. Prim. Care Diabetes 2023, 17, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Felig, P.; Wahren, J. Fuel homeostasis in exercise. N. Engl. J. Med. 1975, 293, 1078–1084. [Google Scholar] [CrossRef] [PubMed]
- Romijn, J.A.; Coyle, E.F.; Sidossis, L.S.; Gastaldelli, A.; Horowitz, J.F.; Endert, E.; Wolfe, R.R. Regulation of endogenous fat and carbohydrate metabolism in relation to exercise intensity and duration. Am. J. Physiol. 1993, 265, E380–E391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahren, J.; Felig, P.; Ahlborg, G.; Jorfeldt, L. Glucose metabolism during leg exercise in man. J. Clin. Investig. 1971, 50, 2715–2725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, H.; Gillen, J.B. Skeletal muscle mechanisms contributing to improved glycemic control following intense interval exercise and training. Sport. Med. Health Sci. 2023, 5, 20–28. [Google Scholar] [CrossRef]
- Koga, M. Glycated albumin; clinical usefulness. Clin. Chim. Acta 2014, 433, 96–104. [Google Scholar] [CrossRef]
- Sakuma, N.; Omura, M.; Oda, E.; Saito, T. Converse contributions of fasting and postprandial glucose to HbA1c and glycated albumin. Diabetol. Int. 2011, 2, 162–171. [Google Scholar] [CrossRef]
- Terauchi, Y.; Takada, T.; Yoshida, S. A randomized controlled trial of a structured program combining aerobic and resistance exercise for adults with type 2 diabetes in Japan. Diabetol. Int. 2022, 13, 75–84. [Google Scholar] [CrossRef]
- Furusyo, N.; Hayashi, J. Glycated albumin and diabetes mellitus. Biochim. Biophys. Acta 2013, 1830, 5509–5514. [Google Scholar] [CrossRef]
- Desouza, C.V.; Holcomb, R.G.; Rosenstock, J.; Frias, J.P.; Hsia, S.H.; Klein, E.J.; Zhou, R.; Kohzuma, T.; Fonseca, V.A. Results of a Study Comparing Glycated Albumin to Other Glycemic Indices. J. Clin. Endocrinol. Metab. 2020, 105, 677–687. [Google Scholar] [CrossRef] [PubMed]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 6. Glycemic Targets: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46, S97–S110. [Google Scholar] [CrossRef] [PubMed]
- Room, J.; Hannink, E.; Dawes, H.; Barker, K. What interventions are used to improve exercise adherence in older people and what behavioural techniques are they based on? A systematic review. BMJ Open 2017, 7, e019221. [Google Scholar] [CrossRef] [PubMed]
- Slentz, C.A.; Houmard, J.A.; Kraus, W.E. Exercise, abdominal obesity, skeletal muscle, and metabolic risk: Evidence for a dose response. Obesity 2009, 17, S27–S33. [Google Scholar] [CrossRef] [Green Version]
- Tappy, L.; Binnert, C.; Schneiter, P. Energy expenditure, physical activity and body-weight control. Proc. Nutr. Soc. 2003, 62, 663–666. [Google Scholar] [CrossRef] [Green Version]
- Gallo-Villegas, J.; Castro-Valencia, L.A.; Perez, L.; Restrepo, D.; Guerrero, O.; Cardona, S.; Sanchez, Y.L.; Yepes-Calderon, M.; Valbuena, L.H.; Pena, M.; et al. Efficacy of high-intensity interval- or continuous aerobic-training on insulin resistance and muscle function in adults with metabolic syndrome: A clinical trial. Eur. J. Appl. Physiol. 2022, 122, 331–344. [Google Scholar] [CrossRef]
- Sun, S.; Zhang, H.; Kong, Z.; Shi, Q.; Tong, T.K.; Nie, J. Twelve weeks of low volume sprint interval training improves cardio-metabolic health outcomes in overweight females. J. Sports Sci. 2019, 37, 1257–1264. [Google Scholar] [CrossRef]
- Wood, G.; Murrell, A.; van der Touw, T.; Smart, N. HIIT is not superior to MICT in altering blood lipids: A systematic review and meta-analysis. BMJ Open Sport Exerc. Med. 2019, 5, e000647. [Google Scholar] [CrossRef] [Green Version]
- Durstine, J.L.; Grandjean, P.W.; Davis, P.G.; Ferguson, M.A.; Alderson, N.L.; DuBose, K.D. Blood lipid and lipoprotein adaptations to exercise: A quantitative analysis. Sports Med. 2001, 31, 1033–1062. [Google Scholar] [CrossRef]
- Johnson, J.L.; Slentz, C.A.; Houmard, J.A.; Samsa, G.P.; Duscha, B.D.; Aiken, L.B.; McCartney, J.S.; Tanner, C.J.; Kraus, W.E. Exercise training amount and intensity effects on metabolic syndrome (from Studies of a Targeted Risk Reduction Intervention through Defined Exercise). Am. J. Cardiol. 2007, 100, 1759–1766. [Google Scholar] [CrossRef] [Green Version]
- Mazzuca, P.; Montesi, L.; Mazzoni, G.; Grazzi, G.; Micheli, M.M.; Piergiovanni, S.; Pazzini, V.; Forlani, G.; Maietta Latessa, P.; Marchesini, G. Supervised vs. self-selected physical activity for individuals with diabetes and obesity: The Lifestyle Gym program. Intern. Emerg. Med. 2017, 12, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, M.; Yokote, K.; Arai, H.; Iida, M.; Ishigaki, Y.; Ishibashi, S.; Umemoto, S.; Egusa, G.; Ohmura, H.; Okamura, T.; et al. Japan Atherosclerosis Society (JAS) Guidelines for Prevention of Atherosclerotic Cardiovascular Diseases 2017. J. Atheroscler. Thromb. 2018, 25, 846–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umemura, S.; Arima, H.; Arima, S.; Asayama, K.; Dohi, Y.; Hirooka, Y.; Horio, T.; Hoshide, S.; Ikeda, S.; Ishimitsu, T.; et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens. Res. 2019, 42, 1235–1481. [Google Scholar] [CrossRef] [Green Version]
- Yamada, C.; Moriyama, K.; Takahashi, E. Optimal cut-off point for homeostasis model assessment of insulin resistance to discriminate metabolic syndrome in non-diabetic Japanese subjects. J. Diabetes Investig. 2012, 3, 384–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef] [PubMed]
- Bean, J.; Herman, S.; Kiely, D.K.; Callahan, D.; Mizer, K.; Frontera, W.R.; Fielding, R.A. Weighted stair climbing in mobility-limited older people: A pilot study. J. Am. Geriatr. Soc. 2002, 50, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Mair, J.L.; De Vito, G.; Boreham, C.A. Low Volume, Home-Based Weighted Step Exercise Training Can Improve Lower Limb Muscle Power and Functional Ability in Community-Dwelling Older Women. J. Clin. Med. 2019, 8, 41. [Google Scholar] [CrossRef] [Green Version]
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk factors for falls among elderly persons living in the community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef]
- Takaishi, T.; Hayashi, T. Stair climbing/descending exercise—Immediate effect against postprandial hyperglycemia in older people with type 2 diabetes mellitus. Ann. Sports Med. Res. 2015, 2, 1023. [Google Scholar]
- Francois, M.E.; Durrer, C.; Pistawka, K.J.; Halperin, F.A.; Chang, C.; Little, J.P. Combined Interval Training and Post-exercise Nutrition in Type 2 Diabetes: A Randomized Control Trial. Front. Physiol. 2017, 8, 528. [Google Scholar] [CrossRef] [Green Version]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | ST-EX (n = 7) | CON (n = 7) | p-Value |
|---|---|---|---|
| Sex (female) (n) (%) | 3 (42.9) | 4 (57.1) | 1.000 |
| Age (years) | 71.0 (59.0, 73.0) † | 69.0 (63.0, 71.0) † | 0.383 |
| Duration of diabetes (years) | 11.0 (7.1, 14.9) | 9.9 (5.1, 14.6) | 0.657 |
| HbA1c (%) (mmol/mol) | 7.0 (6.7, 7.2) (52.7 (50.0, 55.3)) | 6.9 (6.6, 7.2) (52.1 (49.4, 54.7)) | 0.690 |
| GA (%) | 18.1 (17.2, 19.0) | 19.1 (17.3, 20.9) | 0.249 |
| FPG (mmol/L) | 7.1 (6.2, 8.0) | 7.1 (6.0, 8.2) | 0.925 |
| BMI (kg/m2) | 24.4 (22.5, 26.3) | 23.8 (20.0, 27.5) | 0.711 |
| Medication | |||
| Biguanide (n) (%) | 1 (14.3) | 4 (57.1) | 0.266 |
| Thiazolidine (n) (%) | 0 (0.0) | 1 (14.3) | 1.000 |
| α-glucosidase inhibitor (n) (%) | 0 (0.0) | 4 (57.1) | 0.070 |
| Sodium-glucose cotransporter-2 inhibitor (n) (%) | 1 (14.3) | 2 (28.6) | 1.000 |
| Dipeptidyl peptidase-4 inhibitors (n) (%) | 2 (28.6) | 1 (14.3) | 1.000 |
| Sulfonylurea (n) (%) | 1 (14.3) | 3 (42.9) | 0.559 |
| Hypertension (n) (%) | 4 (57.1) | 4 (57.1) | 1.000 |
| Dyslipidemia (n) (%) | 4 (57.1) | 2 (28.6) | 0.592 |
| Cigarette smoking ‡1 | 0.559 | ||
| Non-smoker (n) (%) | 4 (57.1) | 5 (71.4) | |
| Past smoker (n) (%) | 3 (42.9) | 1 (14.3) | |
| Current smoker (n) (%) | 0 (0.0) | 1 (14.3) | |
| Alcohol drinking (n) (%) ‡2 | 2 (28.6) | 1 (14.3) | 1.000 |
| Exercise habits (n) (%) ‡3 | 0 (0.0) | 0 (0.0) | – |
| Occupation | 1.000 | ||
| Unemployed (n) (%) | 3 (42.9) | 4 (57.1) | |
| Farmer (n) (%) | 2 (28.6) | 1 (14.3) | |
| Sedentary worker (n) (%) | 1 (14.3) | 1 (14.3) | |
| Other (n) (%) | 1 (14.3) | 1 (14.3) |
| Variables | Group | Baseline | 12 Weeks | Change | Effect Size (Cohen’s d, r) | p-Value |
|---|---|---|---|---|---|---|
| HbA1c (%) (mmol/mol) | ST-EX | 7.0 (6.7, 7.2) (52.7 (50.0, 55.3)) | 6.9 (6.5, 7.3) (51.9 (47.7, 56.1)) | −0.1 (−0.2, −0.1) (−1.1 (−2.2, −1.1)) † | 0.420 | 0.128 |
| CON | 6.9 (6.6, 7.2) (52.1 (49.4, 54.7)) | 7.0 (6.6, 7.4) (53.1 (48.9, 57.4)) | 0.1 (−0.1, 0.2) (1.1 (−1.1, 2.2)) † | |||
| GA (%) | ST-EX | 18.1 (17.2, 19.0) | 17.1 (15.9, 18.4) | −1.0 (−2.0, 0.0) | 1.257 | 0.037 * |
| CON | 19.1 (17.3, 20.9) | 19.5 (17.0, 22.0) | 0.4 (−0.6, 1.4) | |||
| FPG (mmol/L) | ST-EX | 7.1 (6.2, 8.0) | 7.3 (6.4, 8.2) | 0.2 (−0.8, 1.3) | 0.221 | 0.687 |
| CON | 7.1 (6.0, 8.2) | 7.6 (6.2, 8.9) | 0.4 (−0.2, 1.1) | |||
| FIRI (pmol/L) | ST-EX | 38.4 (24.6, 67.2) † | 33.0 (21.6, 59.4) † | −3.0 (−7.8, 1.2) † | 0.308 | 0.259 |
| CON | 39.0 (19.2, 51.6) † | 39.0 (19.2, 46.2) † | 0.0 (−4.2, 9.6) † | |||
| HOMA-IR | ST-EX | 1.8 (1.2, 3.1) † | 1.8 (1.4, 2.6) † | 0.0 (−0.8, 0.2) † | 0.290 | 0.318 |
| CON | 1.7 (1.2, 3.2) † | 1.9 (1.5, 2.6) † | 0.1 (0.0, 0.7) † | |||
| SBP (mmHg) | ST-EX | 131.0 (114.0, 138.0) † | 138.0 (121.0, 139.0) † | 3.0 (−2.7, 8.7) | 0.239 | 0.663 |
| CON | 125.0 (111.0, 136.0) † | 128.0 (124.0, 133.0) † | 5.4 (−6.6, 17.5) | |||
| DBP (mmHg) | ST-EX | 74.9 (65.5, 84.3) | 74.6 (65.8, 83.3) | −0.3 (−4.5, 3.9) | 0.093 | 0.864 |
| CON | 73.6 (61.9, 85.3) | 72.7 (62.8, 82.6) | −0.9 (−7.7, 6.0) | |||
| TG (mmol/L) | ST-EX | 1.7 (0.6, 2.6) † | 1.3 (0.6, 2.4) † | −0.2 (−0.5, 0.1) | 0.294 | 0.592 |
| CON | 1.2 (0.9, 1.6) † | 0.9 (0.8, 1.7) † | −0.1 (−0.5, 0.4) | |||
| LDL-C (mmol/L) | ST-EX | 2.9 (2.1, 3.6) | 2.8 (2.3, 3.4) | 0.0 (−0.4, 0.3) | 0.309 | 0.574 |
| CON | 3.0 (2.5, 3.6) | 2.9 (2.0, 3.7) | −0.2 (−0.6, 0.3) | |||
| HDL-C (mmol/L) | ST-EX | 1.4 (1.1, 1.6) † | 1.6 (1.4, 1.7) † | 0.1 (−0.1, 0.2) | 0.096 | 0.861 |
| CON | 1.4 (1.3, 1.9) † | 1.5 (1.4, 1.7) † | 0.1 (−0.1, 0.3) | |||
| Non-HDL-C (mmol/L) | ST-EX | 3.6 (2.8, 4.5) | 3.5 (3.0, 4.0) | −0.1 (−0.6, 0.3) | 0.166 | 0.761 |
| CON | 3.6 (3.0, 4.2) | 3.4 (2.7, 4.1) | −0.2 (−0.6, 0.1) |
| Variables | Group | Baseline | 12 Weeks | Change | Effect Size (Cohen’s d, r) | p-Value |
|---|---|---|---|---|---|---|
| Body weight (kg) | ST-EX | 63.6 (57.7, 69.5) | 63.3 (57.9, 68.7) | −0.3 (−1.4, 0.8) | 0.285 | 0.604 |
| CON | 60.6 (48.5, 72.6) | 60.0 (48.5, 71.5) | −0.6 (−1.5, 0.3) | |||
| BMI (kg/m2) | ST-EX | 24.4 (22.5, 26.3) | 24.3 (22.5, 26.1) | −0.1 (−0.5, 0.3) | 0.327 | 0.552 |
| CON | 23.8 (20.0, 27.5) | 23.5 (20.1, 27.0) | −0.2 (−0.6, 0.1) | |||
| Waist circumference (cm) | ST-EX | 89.1 (84.1, 94.2) | 88.9 (82.7, 95.0) | −2.0 (−2.0, 0.5) † | 0.155 | 0.620 |
| CON | 88.8 (80.2, 97.4) | 87.6 (79.3, 95.9) | −0.5 (−4.0, 1.0) † | |||
| Body fat mass (kg) | ST-EX | 18.9 (15.8, 21.9) | 19.2 (15.8, 22.6) | 0.3 (−0.6, 1.4) | 0.072 | 0.895 |
| CON | 18.2 (10.4, 26.1) | 18.5 (11.5, 25.4) | 0.3 (−0.9, 1.4) | |||
| Lower SMM (kg) | ST-EX | 14.3 (12.7, 15.8) | 14.3 (12.5, 16.1) | 0.0 (−0.6, 0.6) | 0.941 | 0.104 |
| CON | 12.3 (9.6, 14.9) | 11.8 (9.2, 14.4) | −0.5 (−0.8, −0.1) | |||
| SMI (kg/m2) | ST-EX | 7.2 (6.6, 7.9) | 7.2 (6.5, 8.0) | 0.0 (−0.2, 0.3) | 0.945 | 0.102 |
| CON | 6.5 (5.6, 7.3) | 6.3 (5.5, 7.2) | −0.2 (−0.3, −0.1) | |||
| Grip strength (kg) | ST-EX | 25.8 (20.7, 35.7) † | 28.7 (22.9, 36.3) † | 1.7 (−0.5, 3.9) | 0.199 | 0.716 |
| CON | 21.3 (15.2, 27.3) † | 23.2 (17.7, 26.2) † | 1.3 (−0.3, 2.8) | |||
| Knee extension force (Nm/kg) | ST-EX | 0.9 (0.6, 1.3) | 1.1 (0.8, 1.5) | 0.2 (0.1, 0.3) | 1.294 | 0.032 * |
| CON | 1.0 (0.7, 1.3) | 0.9 (0.6, 1.2) | −0.1 (−0.3, 0.1) | |||
| 5R-STS test (s) | ST-EX | 11.5 (7.5, 15.5) | 9.0 (7.5, 10.5) | −0.4 (−5.8, 0.5) † | 0.188 | 0.535 |
| CON | 8.9 (7.1, 10.7) | 8.1 (6.8, 9.3) | −1.3 (−2.3, 1.3) † | |||
| Comfortable gait speed (m/s) | ST-EX | 1.3 (1.1, 1.5) | 1.3 (1.1, 1.5) | 0.0 (−0.2, 0.1) | 0.546 | 0.327 |
| CON | 1.4 (1.2, 1.6) | 1.4 (1.3, 1.6) | 0.1 (−0.1, 0.2) | |||
| Maximum gait speed (m/s) | ST-EX | 1.9 (1.3, 2.4) | 2.0 (1.6, 2.3) | 0.1 (−0.3, 0.5) | 0.002 | 0.996 |
| CON | 1.7 (1.5, 2.0) | 1.8 (1.7, 2.0) | 0.1 (−0.1, 0.3) | |||
| Total daily MVPA (METs-min/day) | ST-EX | 257.5 (54.0, 460.9) | 322.4 (110.6, 534.3) | 65.0 (−70.8, 200.7) | 0.215 | 0.695 |
| CON | 336.1 (1.3, 673.5) | 322.1 (153.6, 490.6) | −14.0 (−475.8, 447.8) | |||
| Total daily EE in MVPA (kcal/day) | ST-EX | 220.9 (62.5, 921.7) † | 271.3 (181.9, 494.9) † | 76.7 (−79.9, 233.2) | 0.274 | 0.618 |
| CON | 240.7 (65.0, 560.0) † | 259.1 (105.7, 634.1) † | −27.1 (−497.5, 443.3) | |||
| Sedentary behavior (min/day) | ST-EX | 240.0 (120.0, 420.0) † | 240.0 (150.0, 420.0) † | 30.0 (−180.0, 90.0) † | 0.137 | 0.620 |
| CON | 271.3 (181.9, 494.9) † | 360.0 (180.0, 480.0) † | 60.0 (−150.0, 120.0) † |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Honda, H.; Fukutomi, H.; Igaki, M.; Tanaka, S.; Takaishi, T.; Hayashi, T. The Chronic Effect of Stair Climbing–Descending Exercises after Meals on Glycemic Control in Individuals with Type 2 Diabetes: A Randomized Controlled Trial. Muscles 2023, 2, 238-249. https://doi.org/10.3390/muscles2020018
Honda H, Fukutomi H, Igaki M, Tanaka S, Takaishi T, Hayashi T. The Chronic Effect of Stair Climbing–Descending Exercises after Meals on Glycemic Control in Individuals with Type 2 Diabetes: A Randomized Controlled Trial. Muscles. 2023; 2(2):238-249. https://doi.org/10.3390/muscles2020018
Chicago/Turabian StyleHonda, Hiroto, Hiromi Fukutomi, Makoto Igaki, Shinichiro Tanaka, Tetsuo Takaishi, and Tatsuya Hayashi. 2023. "The Chronic Effect of Stair Climbing–Descending Exercises after Meals on Glycemic Control in Individuals with Type 2 Diabetes: A Randomized Controlled Trial" Muscles 2, no. 2: 238-249. https://doi.org/10.3390/muscles2020018