
The Prevalence of Gastrointestinal Bleeding in COVID-19 Patients: A Systematic Review and Meta-Analysis
 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol and Guidelines
2.2. Eligibility Criteria
2.3. Search Strategy and Selection Process
2.4. Data Collection Process and Data Items
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
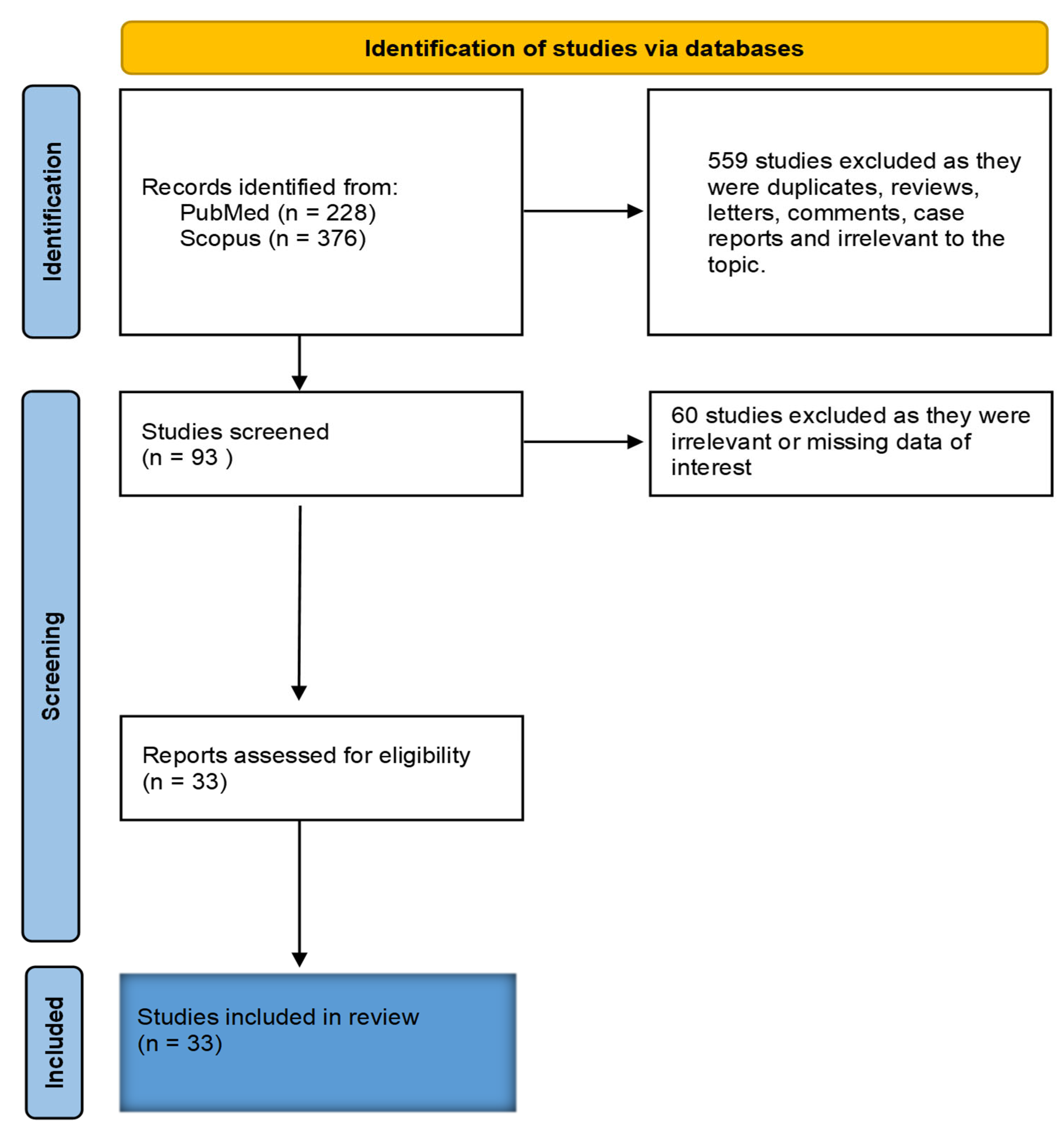
3.1. Study Selection
3.2. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Location |
Total Subjects (% Male/Median Age) | Study Type | Gastrointestinal Bleeding Cases (Prevalence %) |
|---|---|---|---|---|
| Chen et al., 2021 [25] | China | 2552 (50.4/57.8) | ORCS | 40 (1.6) |
| Alakuş et al., 2022 [26] | Turkey | 5484 (73/70.1) | ORCS | 44 (0.8) |
| Mauro et al., 2021 [27] | Italy | 4871 (78.3/75) | ORCS | 23 (0.47) |
| Trindade et al., 2021 [28] | USA | 11,158 | CCS | 314 (3) |
| Makker et al., 2021 [29] | Finland | 1206 (60.8/62) | ORCS | 37 (3.1) |
| Popa et al., 2022 [30] | Romania | 1881 (66.6%) | ORCS | 11 (0.58) |
| Prasoppokakorn et al., 2022 [31] | Thailand | 6373 (65.1/69.1) | ORCS | 43 (0.7) |
| González et al., 2022 [32] | Spain | 74,814 | ORCS | 83 (1.11) |
| Lak et al., 2022 [33] | China | 381 (61.4/62.6) | CS | 16 (4.2) |
| Rosevics et al., 2021 [34] | Brazil | 631(54.2/56.7) | CS | 10 (1.6) |
| Zellmer et al., 2021 [35] | NM | 5344 (57.1%) | SR | 97 (1.8) |
| Abowali et al., 2022 [36] | USA | 651 (54.2/66) | ORCS | 16 (2.85) |
| Abulawi et al., 2022 [37] | USA | 1007 (56/63) | CCS | 76 (8) |
| Shalimar et al., 2021 [38] | India | 1342 (70.8/45.8) | ORCS | 24 (1.8) |
| Lin et al., 2020 [39] | China | 95 (47/45.3) | ORCS | 6 (6.3) |
| Shao et al., 2020 [40] | China | 18 (72.2/73.5) | ORCS | 1 (5.6) |
| Fanning et al., 2023 [41] | NM | 11,969 | ORCS | 276 (2.3) |
| Zhao et al., 2021 [42] | China | 368 (51.7/59) | ORCS | 43 (11.7) |
| Martin et al., 2020 [43] | USA | 987 | CCS | 41 (4.15) |
| Xiao et al., 2020 [44] | China | 73 (56.1/43) | ORCS | 10 (13.7) |
| Al-Samkari et al., 2020 [45] | USA | 400 | ORCS | 19 (4.8) |
| Wan et al., 2020 [46] | China | 232 (56/47) | ORCS | 10 (4) |
| Mattioli et al., 2021 [47] | Italy | 105 (58/73.7) | ORCS | 2 (1.9) |
| Patell et al., 2020 [48] | USA | 398 (52.5%) | ORCS | 33 (8.29) |
| Bunch et al., 2021 [49] | USA | 79 (65.8/71) | ORCS | 2 (2.81) |
| Qiu et al., 2021 [50] | China | 34 (71/66) | ORCS | 6 (17.6) |
| Russell et al., 2022 [51] | Denmark | 1377 (68/68) | ORCS | 108 (8) |
| Bychinin et al., 2022 [52] | Russia | 442 (43.5/78) | ORCS | 9 (2) |
| Bonafni et al., 2022 [53] | Italy | 30 (63/68.5) | ORCS | 3 (10) |
| Abdelmohsen et al., 2021 [54] | Kuwait | 30 (70/57.7) | ORCS | 6 (20) |
| Neuberger et al., 2022 [55] | Germany | 51 | ORCS | 2 (3.90) |
| Nikolay N. et al., 2022 [56] | Russia | 387 (29.9/65.4) | ORCS | 22 (5.7) |
| Demelo-Rodriguez et al., 2021 [57] | Spain | 132 (47%) | ORCS | 25 (19) |
3.3. Clinical Findings
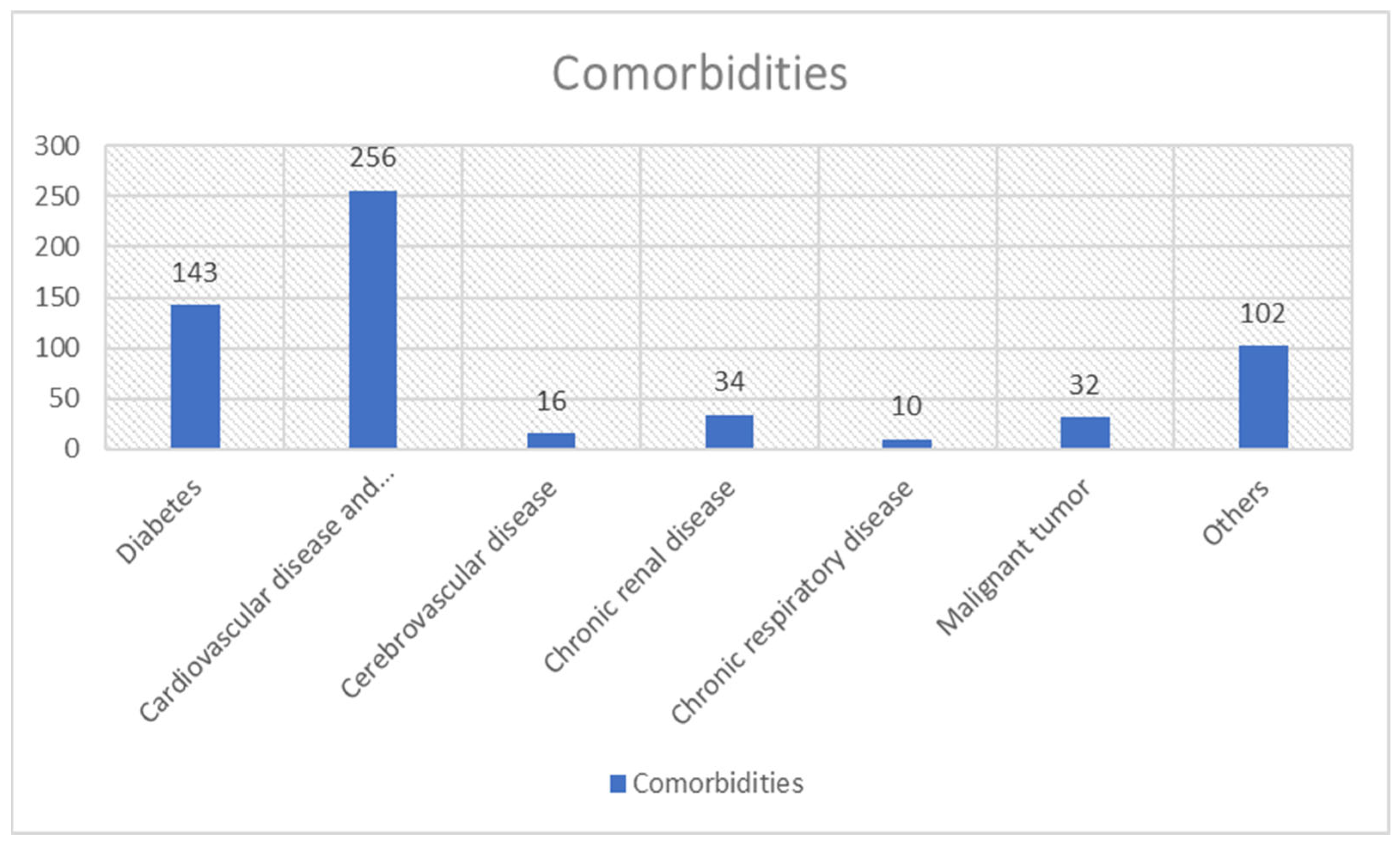
3.3.1. Comorbidities
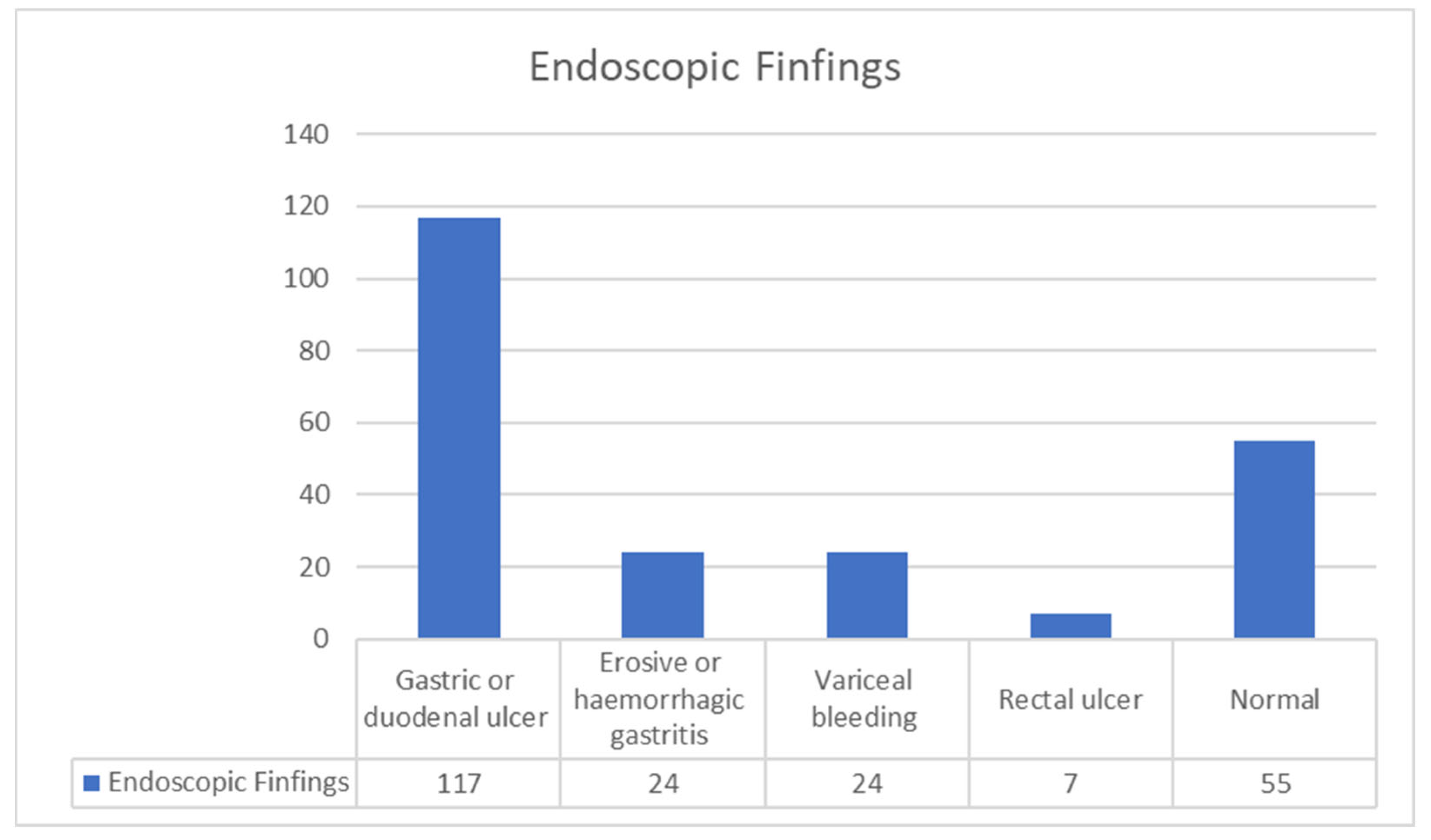
3.3.2. Endoscopy Characteristics
3.3.3. Laboratory Findings
3.3.4. COVID-19 Treatments during Hospitalization in Patients with GIB
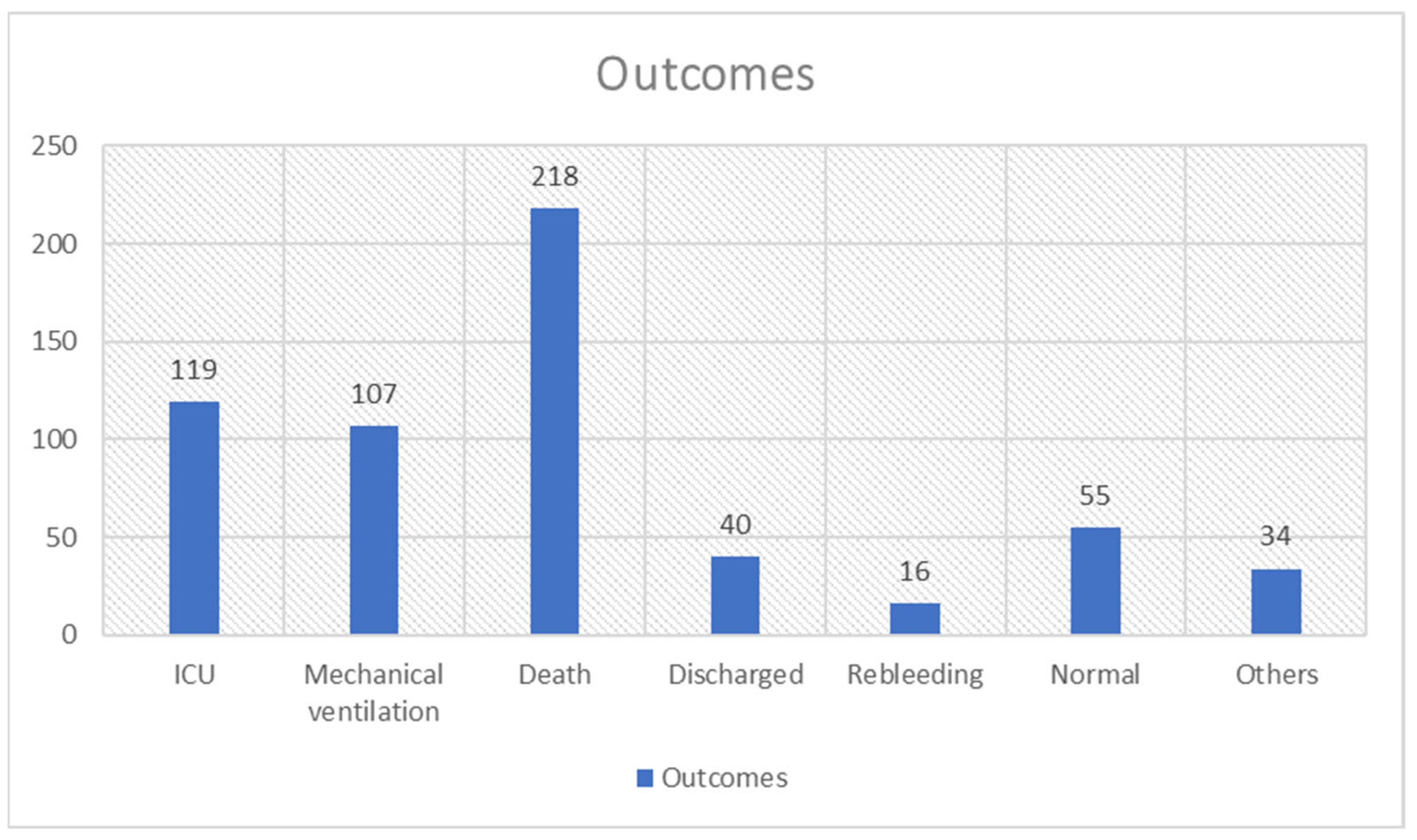
3.3.5. Outcomes
3.4. Quality Assessment
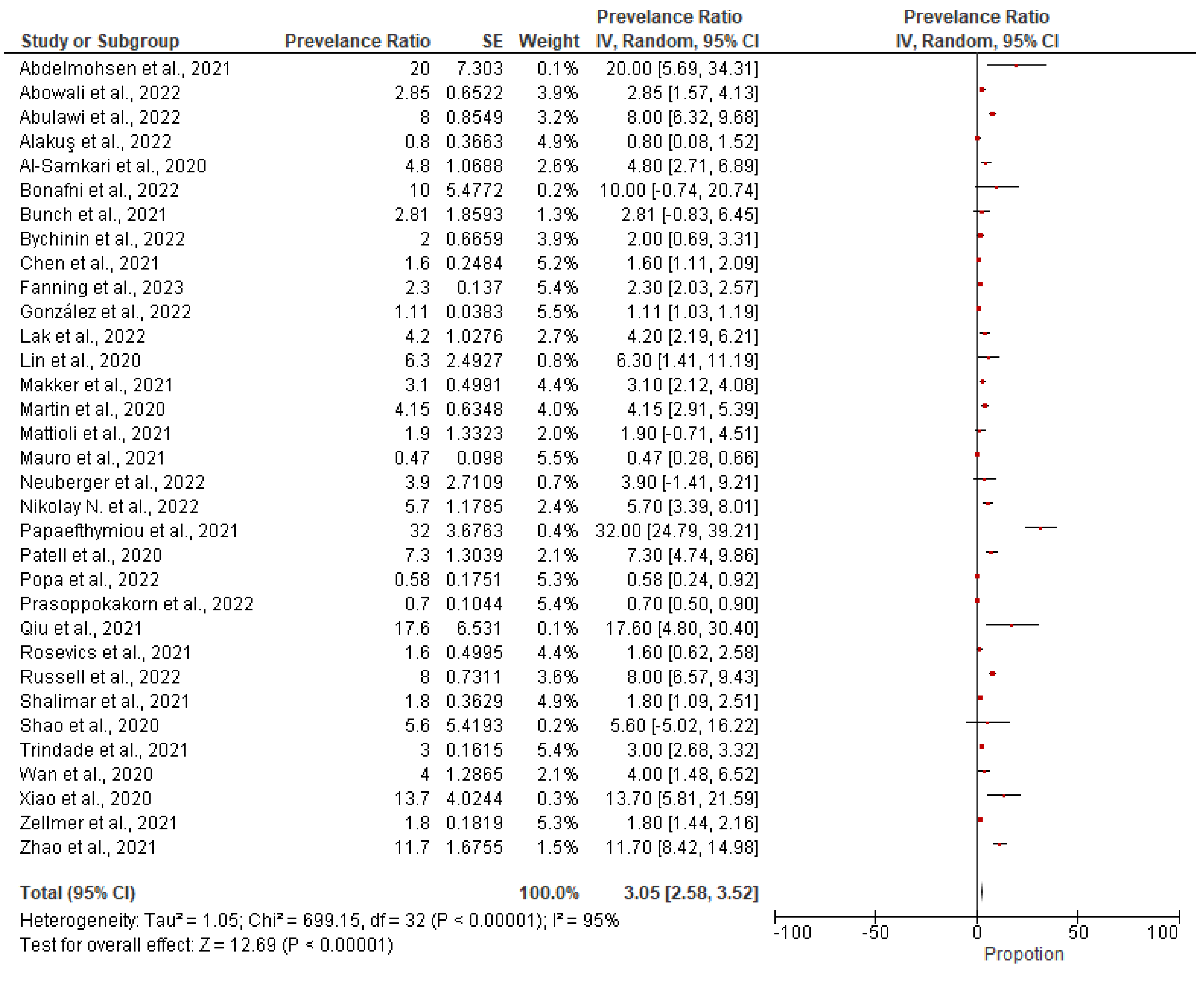
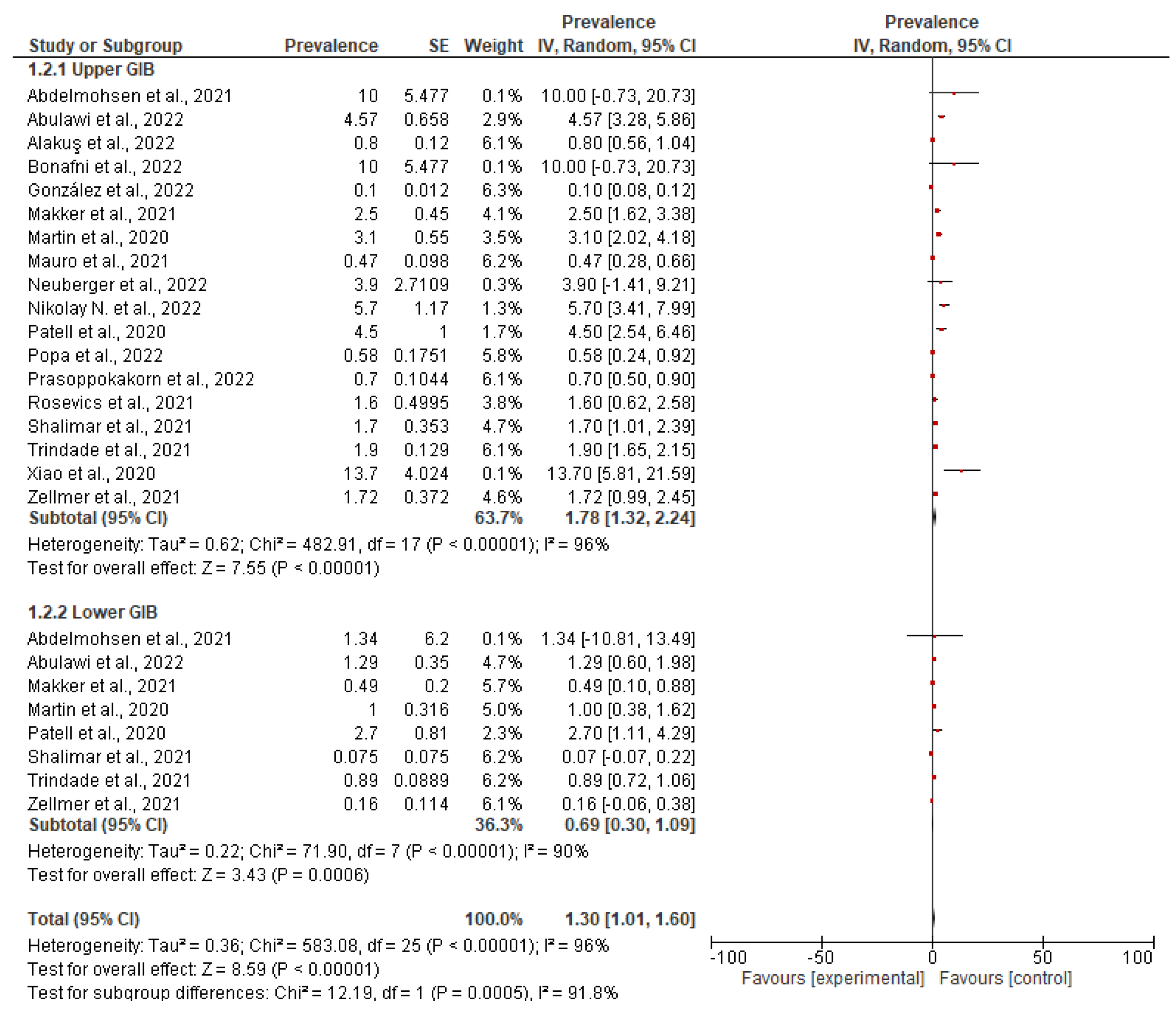
3.5. Meta-Analysis Results
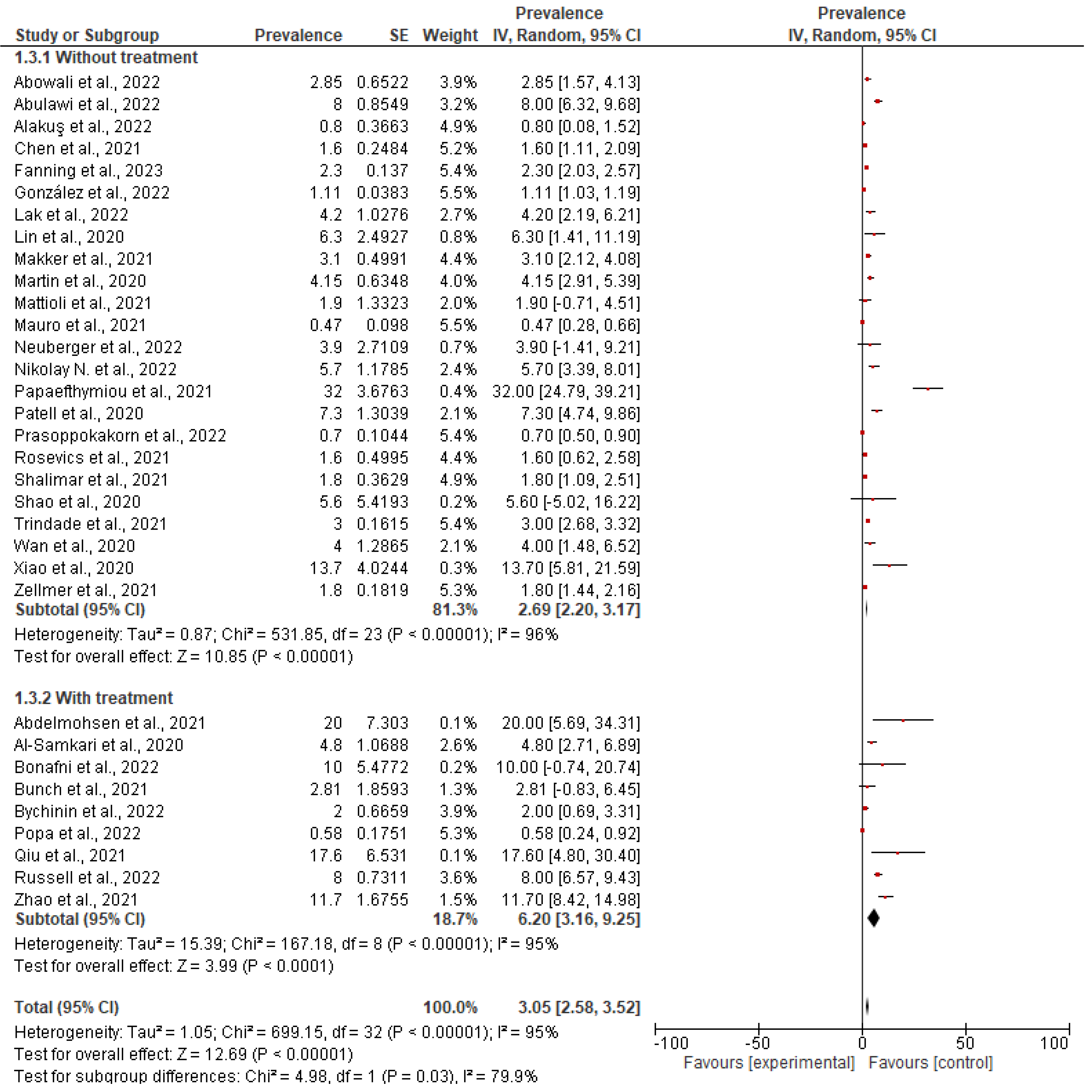
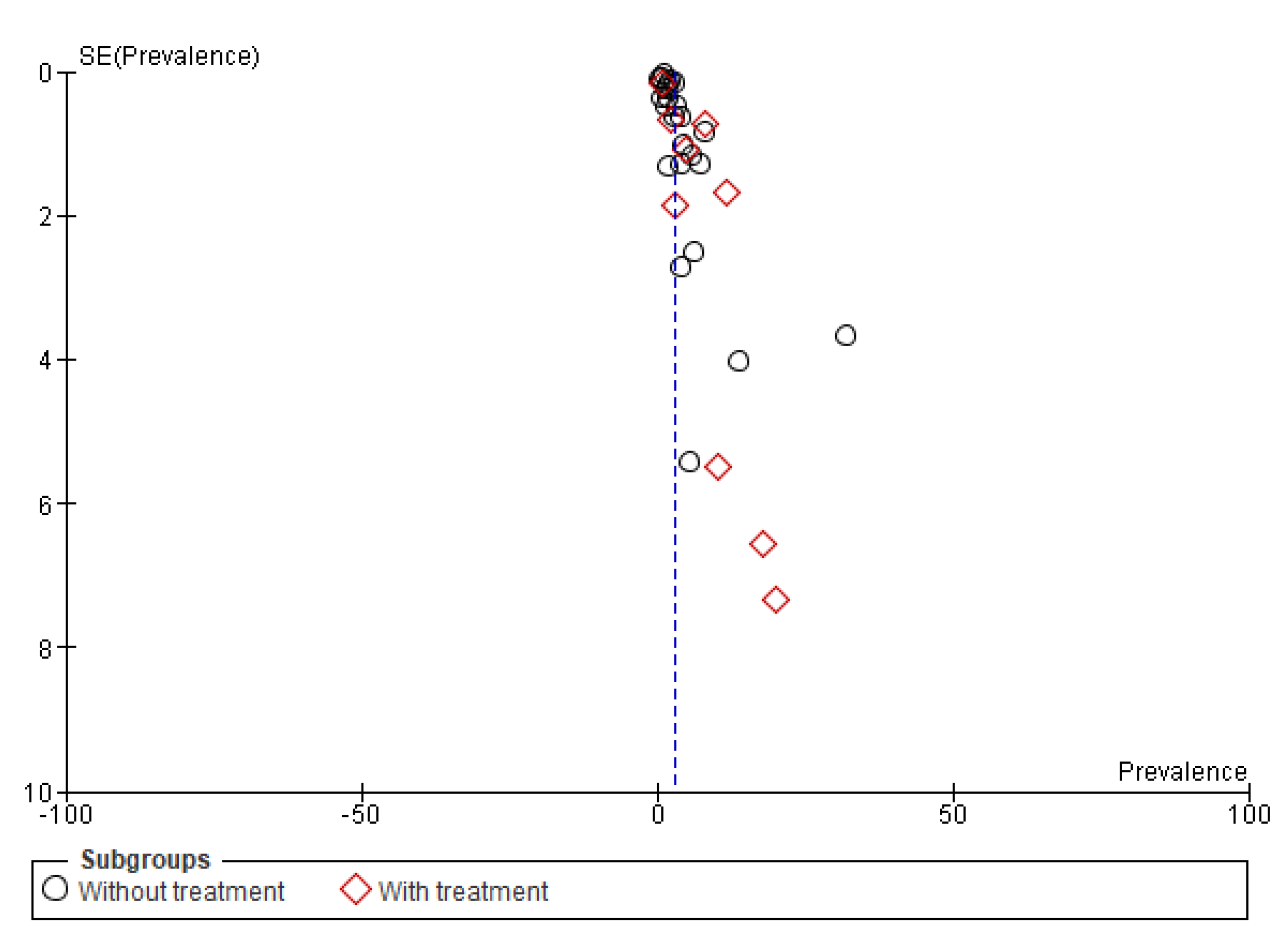
Subgroup Analysis
Subgroup (1) According to Treatment
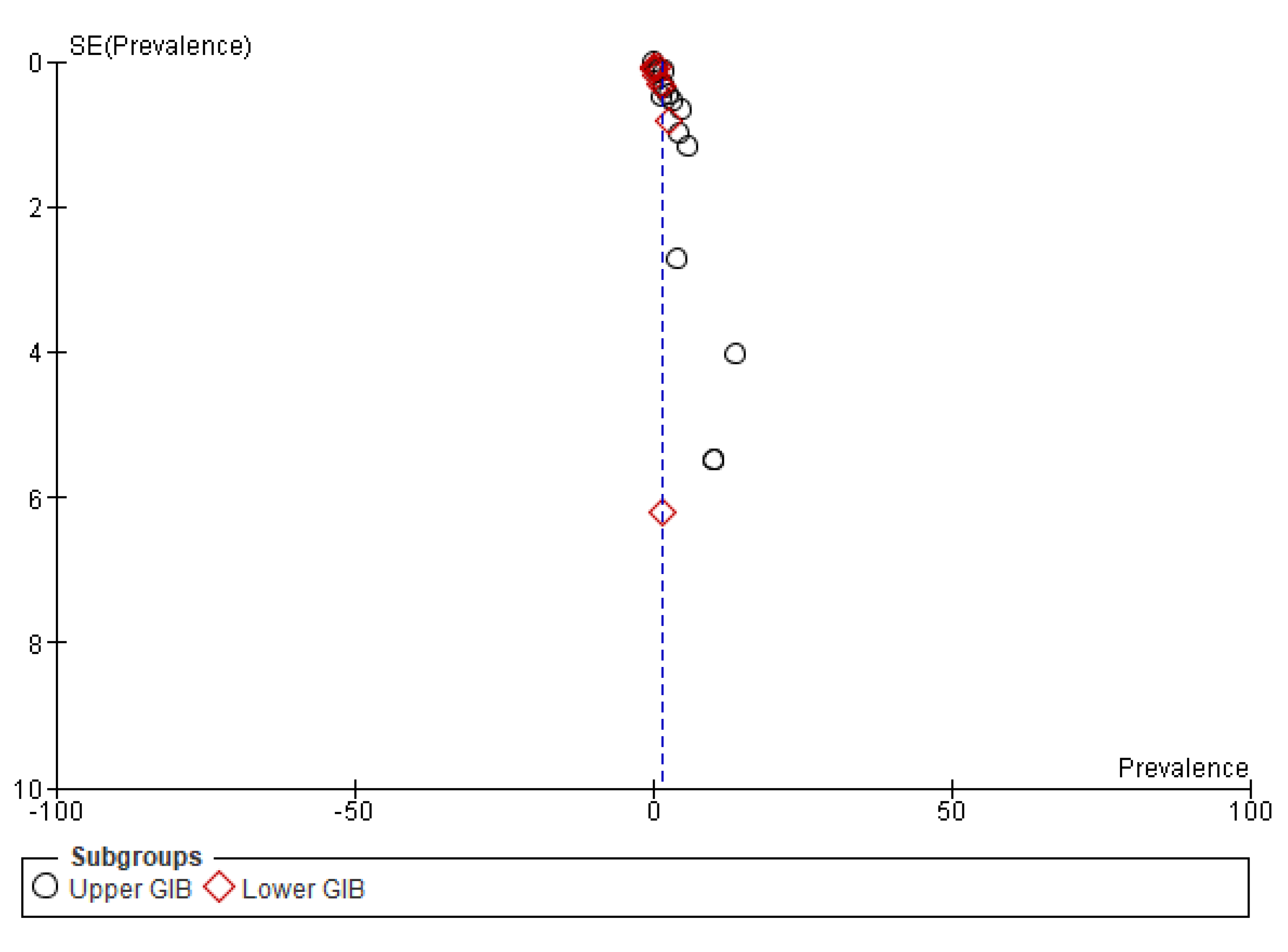
Subgroup (2) According to Location of Bleeding
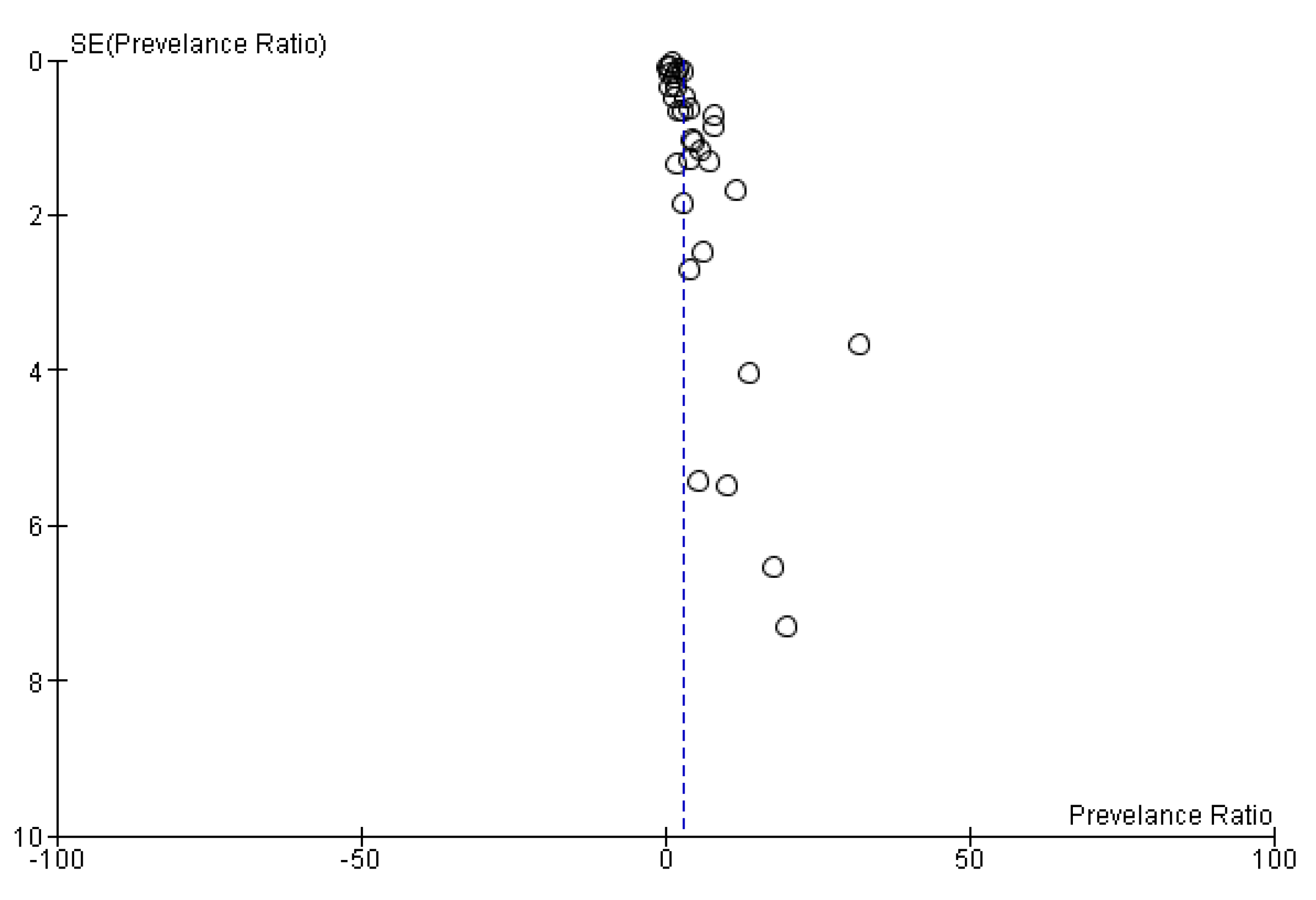
3.6. Publication Bias
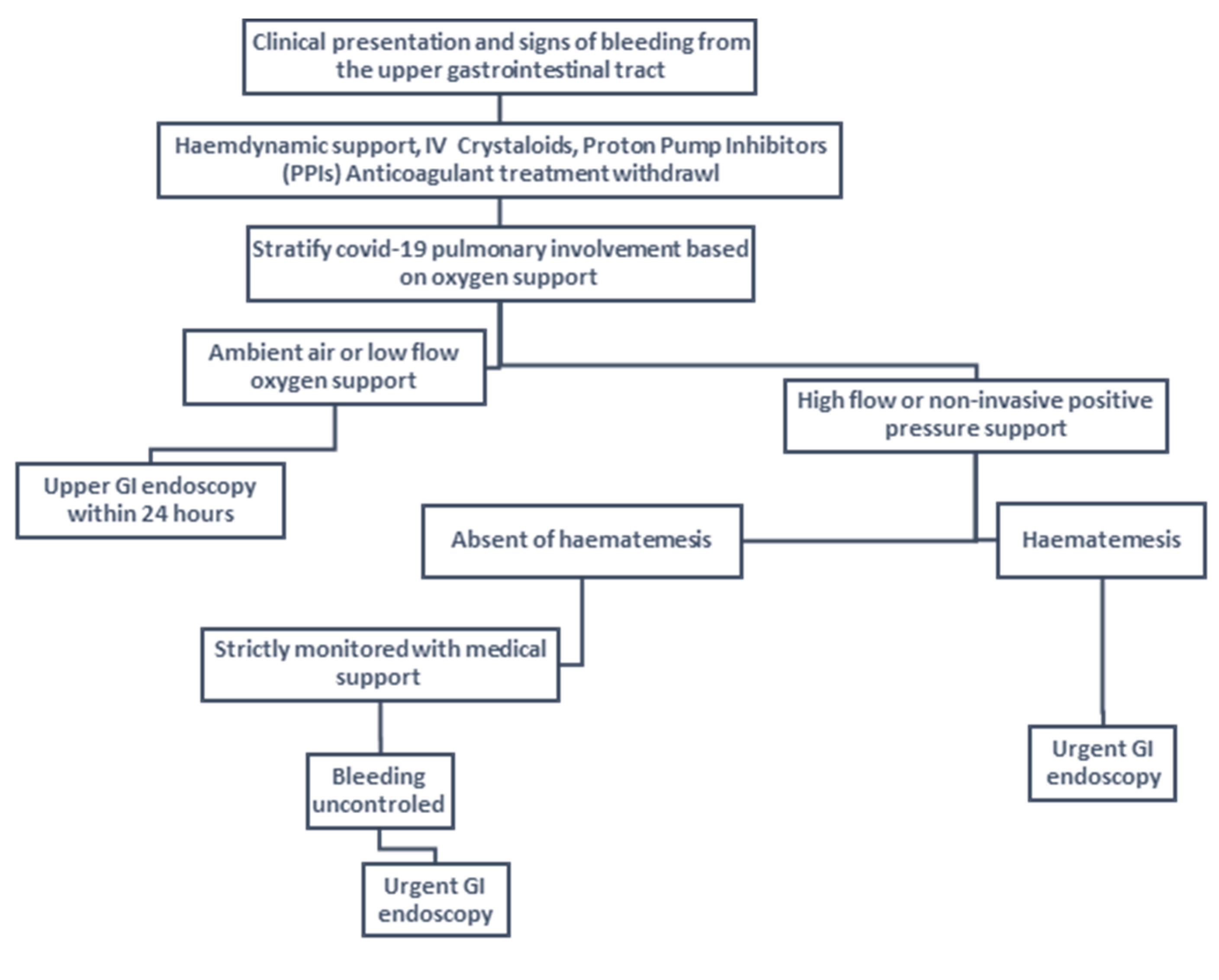
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leao, J.C.; Gusmao, T.P.d.L.; Zarzar, A.M.; Filho, J.C.L.; de Faria, A.B.S.; Silva, I.H.M.; Gueiros, L.A.M.; Robinson, N.A.; Porter, S.; Carvalho, A.d.A.T. Coronaviridae—Old friends, new enemy! Oral Dis. 2022, 28, 858–866. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19). JAMA 2020, 324, 782. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Wang, G.; Cai, X.-P.; Deng, J.-W.; Zheng, L.; Zhu, H.-H.; Zheng, M.; Yang, B.; Chen, Z. An overview of COVID-19. J. Zhejiang Univ. Sci. B 2020, 21, 343–360. [Google Scholar] [CrossRef] [PubMed]
- Salian, V.S.; Wright, J.A.; Vedell, P.T.; Nair, S.; Li, C.; Kandimalla, M.; Tang, X.; Porquera, E.M.C.; Kalari, K.R.; Kandimalla, K.K. COVID-19 Transmission, Current Treatment, and Future Therapeutic Strategies. Mol. Pharm. 2021, 18, 754–771. [Google Scholar] [CrossRef] [PubMed]
- Kevadiya, B.D.; Machhi, J.; Herskovitz, J.; Oleynikov, M.D.; Blomberg, W.R.; Bajwa, N.; Soni, D.; Das, S.; Hasan, M.; Patel, M.; et al. Diagnostics for SARS-CoV-2 infections. Nat. Mater. 2021, 20, 593–605. [Google Scholar] [CrossRef]
- D’Cruz, R.J.; Currier, A.W.; Sampson, V.B. Laboratory Testing Methods for Novel Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-CoV-2). Front. Cell Dev. Biol. 2020, 8, 468. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Heymann, D.L.; Teo, Y.-Y.; Garcia, P.J. Diagnostics for COVID-19: Moving from pandemic response to control. Lancet 2022, 399, 757–768. [Google Scholar] [CrossRef]
- Karlafti, E.; Tsavdaris, D.; Kotzakioulafi, E.; Kaiafa, G.; Savopoulos, C.; Netta, S.; Michalopoulos, A.; Paramythiotis, D. The Diagnostic Accuracy of SARS-CoV-2 Nasal Rapid Antigen Self-Test: A Systematic Review and Meta-Analysis. Life 2023, 13, 281. [Google Scholar] [CrossRef]
- Sharif, N.; Alzahrani, K.J.; Ahmed, S.N.; Dey, S.K. Efficacy, Immunogenicity and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 714170. [Google Scholar] [CrossRef]
- Kariyawasam, J.C.; Jayarajah, U.; Riza, R.; Abeysuriya, V.; Seneviratne, S.L. Gastrointestinal manifestations in COVID-19. Trans. R Soc. Trop. Med. Hyg. 2021, 115, 1362–1388. [Google Scholar] [CrossRef]
- Jin, B.; Singh, R.; Ha, S.E.; Zogg, H.; Park, P.J.; Ro, S. Pathophysiological mechanisms underlying gastrointestinal symptoms in patients with COVID-19. World J. Gastroenterol. 2021, 27, 2341–2352. [Google Scholar] [CrossRef] [PubMed]
- Anka, A.U.; Tahir, M.I.; Abubakar, S.D.; Alsabbagh, M.; Zian, Z.; Hamedifar, H.; Sabzevari, A.; Azizi, G. Coronavirus disease 2019 (COVID-19): An overview of the immunopathology, serological diagnosis and management. Scand J. Immunol. 2021, 93, e12998. [Google Scholar] [CrossRef] [PubMed]
- Owensby, S.; Taylor, K.; Wilkins, T. Diagnosis and Management of Upper Gastrointestinal Bleeding in Children. J. Am. Board Fam. Med. 2015, 28, 134–145. [Google Scholar] [CrossRef] [PubMed]
- Kamboj, A.K.; Hoversten, P.; Leggett, C.L. Upper Gastrointestinal Bleeding: Etiologies and Management. Mayo Clin. Proc. 2019, 94, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Aoki, T.; Hirata, Y.; Yamada, A.; Koike, K. Initial management for acute lower gastrointestinal bleeding. World J. Gastroenterol. 2019, 25, 69–84. [Google Scholar] [CrossRef] [PubMed]
- Hawks, M.K.; Svarverud, J.E. Acute Lower Gastrointestinal Bleeding: Evaluation and Management. Am. Fam. Physician 2020, 101, 206–212. [Google Scholar]
- Ye, Q.; Wang, B.; Zhang, T.; Xu, J.; Shang, S. The mechanism and treatment of gastrointestinal symptoms in patients with COVID-19. Am. J. Physiol.-Gastrointest. Liver Physiol. 2020, 319, G245–G252. [Google Scholar] [CrossRef]
- Dioscoridi, L.; Giannetti, A.; Massad, M.; Forti, E.; Pugliese, F.; Cintolo, M.; Bonato, G.; Rosa, R.; Mutignani, M. A ‘double-hit’ damage mechanism can explain self-limited GI bleeding in COVID-19 pneumonia. Gastrointest Endosc. 2021, 93, 1192–1193. [Google Scholar] [CrossRef]
- Sarkar, M.; Madabhavi, I.V.; Quy, P.N.; Govindagoudar, M.B. COVID-19 and coagulopathy. Clin. Respir. J. 2021, 15, 1259–1274. [Google Scholar] [CrossRef]
- Cook, D.; Guyatt, G. Prophylaxis against Upper Gastrointestinal Bleeding in Hospitalized Patients. N. Engl. J. Med. 2018, 378, 2506–2516. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021, 156, 787. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Tong, Z.; Ma, Z.; Luo, L.; Tang, Y.; Teng, Y.; Yu, H.; Meng, H.; Peng, C.; Zhang, Q.; et al. Gastrointestinal Bleeding, but Not Other Gastrointestinal Symptoms, Is Associated with Worse Outcomes in COVID-19 Patients. Front. Med. 2021, 8, 759152. [Google Scholar] [CrossRef] [PubMed]
- Alakuş, Ü. Upper gastrointestinal system bleedings in COVID-19 patients: Risk factors and management / A retrospective Cohort Study. Turk. J. Trauma Emerg. Surg. 2021, 28, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Mauro, A.; De Grazia, F.; Lenti, M.V.; Penagini, R.; Frego, R.; Ardizzone, S.; Savarino, E.; Radaelli, F.; Bosani, M.; Orlando, S.; et al. Upper gastrointestinal bleeding in COVID-19 inpatients: Incidence and management in a multicenter experience from Northern Italy. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101521. [Google Scholar] [CrossRef] [PubMed]
- Trindade, A.J.; Izard, S.; Coppa, K.; Hirsch, J.S.; Lee, C.; Satapathy, S.K. Gastrointestinal bleeding in hospitalized COVID-19 patients: A propensity score matched cohort study. J. Intern. Med. 2021, 289, 887–894. [Google Scholar] [CrossRef]
- Makker, J.; Mantri, N.; Patel, H.K.; Abbas, H.; Baiomi, A.; Sun, H.; Choi, Y.; Chilimuri, S.; Nayudu, S.K. The Incidence and Mortality Impact of Gastrointestinal Bleeding in Hospitalized COVID-19 Patients. Clin. Exp. Gastroenterol. 2021, 14, 405–411. [Google Scholar] [CrossRef]
- Popa, P.; Iordache, S.; Florescu, D.N.; Iovanescu, V.F.; Vieru, A.; Barbu, V.; Bezna, M.-C.; Alexandru, D.O.; Ungureanu, B.S.; Cazacu, S.M. Mortality Rate in Upper Gastrointestinal Bleeding Associated with Anti-Thrombotic Therapy Before and During Covid-19 Pandemic. J. Multidiscip. Healthc. 2022, 15, 2679–2692. [Google Scholar] [CrossRef]
- Prasoppokakorn, T.; Kullavanijaya, P.; Pittayanon, R. Risk factors of active upper gastrointestinal bleeding in patients with COVID-19 infection and the effectiveness of PPI prophylaxis. BMC Gastroenterol. 2022, 22, 465. [Google Scholar] [CrossRef] [PubMed]
- González, R.G.; Jacob, J.; Miró, Ò.; Llorens, P.; Jiménez, S.; del Castillo, J.G.; Burillo-Putze, G.; Martín, A.; Martín-Sánchez, F.J.; Lamberechts, J.G.; et al. Incidence, Clinical Characteristics, Risk Factors, and Outcomes of Upper Gastrointestinal Bleeding in Patients With COVID-19. J. Clin. Gastroenterol. 2022, 56, e38–e46. [Google Scholar] [CrossRef] [PubMed]
- Lak, E.; Sheikholeslami, S.; Ghorbi, M.; Shafei, M.; Yosefi, H. Association between gastrointestinal symptoms and disease severity in patients with COVID-19 in Tehran City, Iran. Gastroenterol. Rev. 2022, 17, 52–58. [Google Scholar] [CrossRef]
- Rosevics, L.; Fossati, B.S.; Teixeira, S.; de Bem, R.S.; de Souza, R.C.A. COVID-19 and Digestive Endoscopy: Emergency Endoscopic Procedures and Risk Factors for Upper Gastrointestinal Bleeding. Arq. Gastroenterol. 2021, 58, 337–343. [Google Scholar] [CrossRef]
- Zellmer, S.; Hanses, F.; Muzalyova, A.; Classen, J.; Braun, G.; Piepel, C.; Erber, J.; Pilgram, L.; Walter, L.; Göpel, S.; et al. Gastrointestinal bleeding and endoscopic findings in critically and non-critically ill patients with corona virus disease 2019 (COVID-19): Results from Lean European Open Survey on SARS-CoV-2 (LEOSS) and COKA registries. United Eur. Gastroenterol. J. 2021, 9, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Abowali, H.; Pacifico, A.; Erdinc, B.; Elkholy, K.; Burkhanova, U.; Aroriode, T.; Watson, A.; Ahmed, M.F.; Uwagbale, E.; Visweshwar, N.; et al. Assessment of Bleeding Risk in Hospitalized COVID-19 Patients: A Tertiary Hospital Experience during the Pandemic in a Predominant Minority Population—Bleeding Risk Factors in COVID-19 Patients. J. Clin. Med. 2022, 11, 2754. [Google Scholar] [CrossRef]
- Abulawi, A.; Al-Tarbsheh, A.; Leamon, A.; Feustel, P.; Chopra, A.; Batool, A. Clinical Characteristics of Hospitalized COVID-19 Patients Who Have Gastrointestinal Bleeds Requiring Intervention: A Case-Control Study. Cureus 2022, 14, e26538. [Google Scholar] [CrossRef]
- Shalimar; Vaishnav, M.; Elhence, A.; Kumar, R.; Mohta, S.; Palle, C.; Kumar, P.; Ranjan, M.; Vajpai, T.; Prasad, S.; et al. Outcome of Conservative Therapy in Coronavirus disease-2019 Patients Presenting With Gastrointestinal Bleeding. J. Clin. Exp. Hepatol. 2021, 11, 327–333. [Google Scholar] [CrossRef]
- Lin, L.; Jiang, X.; Zhang, Z.; Huang, S.; Zhang, Z.; Fang, Z.; Gu, Z.; Gao, L.; Shi, H.; Mai, L.; et al. Gastrointestinal symptoms of 95 cases with SARS-CoV-2 infection. Gut 2020, 69, 997–1001. [Google Scholar] [CrossRef]
- Shao, L.; Li, X.; Zhou, Y.; Yu, Y.; Liu, Y.; Liu, M.; Zhang, R.; Zhang, H.; Wang, X.; Zhou, F. Novel Insights into Illness Progression and Risk Profiles for Mortality in Non-survivors of COVID-19. Front. Med. 2020, 7, 246. [Google Scholar] [CrossRef]
- Fanning, J.P.; Weaver, N.; Fanning, R.B.; Griffee, M.J.; Cho, S.-M.; Panigada, M.; Obonyo, N.G.; Zaaqoq, A.M.; Rando, H.; Chia, Y.W.; et al. Hemorrhage, Disseminated Intravascular Coagulopathy, and Thrombosis Complications Among Critically Ill Patients with COVID-19: An International COVID-19 Critical Care Consortium Study. Crit. Care Med. 2023, 51, 619–631. [Google Scholar] [CrossRef]
- Zhao, X.; Tao, M.; Chen, C.; Zhang, Y.; Fu, Y. Clinical Features and Factors Associated with Occult Gastrointestinal Bleeding in COVID-19 Patients. Infect. Drug Resist. 2021, 14, 4217–4226. [Google Scholar] [CrossRef] [PubMed]
- Martin, T.A.; Wan, D.W.; Hajifathalian, K.; Tewani, S.; Shah, S.L.; Mehta, A.; Kaplan, A.; Ghosh, G.; Choi, A.J.; Krisko, T.I.; et al. Gastrointestinal Bleeding in Patients with Coronavirus Disease 2019: A Matched Case-Control Study. Am. J. Gastroenterol. 2020, 115, 1609–1616. [Google Scholar] [CrossRef]
- Xiao, F.; Tang, M.; Zheng, X.; Liu, Y.; Li, X.; Shan, H. Evidence for Gastrointestinal Infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833.e3. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Leaf, R.S.K.; Dzik, W.H.; Carlson, J.C.T.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID-19 and coagulation: Bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef]
- Wan, Y.; Li, J.; Shen, L.; Zou, Y.; Hou, L.; Zhu, L.; Faden, H.S.; Tang, Z.; Shi, M.; Jiao, N.; et al. Enteric involvement in hospitalised patients with COVID-19 outside Wuhan. Lancet Gastroenterol. Hepatol. 2020, 5, 534–535. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, M.; Benfaremo, D.; Mancini, M.; Mucci, L.; Mainquà, P.; Polenta, A.; Baldini, P.M.; Fulgenzi, F.; Dennetta, D.; Bedetta, S.; et al. Safety of intermediate dose of low molecular weight heparin in COVID-19 patients. J. Thromb. Thrombolysis 2021, 51, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Patell, R.; Bogue, T.; Bindal, P.; Koshy, A.; Merrill, M.; Aird, W.C.; Bauer, K.A.; Zwicker, J.I. Incidence of thrombosis and hemorrhage in hospitalized cancer patients with COVID-19. J. Thromb. Haemost. 2020, 18, 2349–2357. [Google Scholar] [CrossRef]
- Bunch, C.M.; Thomas, A.V.; Stillson, J.E.; Gillespie, L.; Khan, R.Z.; Zackariya, N.; Shariff, F.; Al-Fadhl, M.; Mjaess, N.; Miller, P.D.; et al. Preventing Thrombohemorrhagic Complications of Heparinized COVID-19 Patients Using Adjunctive Thromboelastography: A Retrospective Study. J. Clin. Med. 2021, 10, 3097. [Google Scholar] [CrossRef]
- Qiu, C.; Li, T.; Wei, G.; Xu, J.; Yu, W.; Wu, Z.; Li, D.; He, Y.; Chen, T.; Zhang, J.; et al. Hemorrhage and venous thromboembolism in critically ill patients with COVID-19. SAGE Open Med. 2021, 9, 1–8. [Google Scholar] [CrossRef]
- Russell, L.; Weihe, S.; Madsen, E.K.; Hvas, C.L.; Leistner, J.W.; Michelsen, J.; Brøchner, A.C.; Bastiansen, A.; Nielsen, F.M.; Meier, N.; et al. Thromboembolic and bleeding events in ICU patients with COVID-19: A nationwide, observational study. Acta Anaesthesiol. Scand. 2023, 67, 76–85. [Google Scholar] [CrossRef]
- Bychinin, M.V.; Klypa, T.V.; Mandel, I.A.; Avdonin, P.V.; Korshunov, D.I. Thrombotic and hemorrhagic complications in patients with severe and extremely severe COVID-19. Anesteziol. Reanimatol. 2022, 2, 24–32. [Google Scholar] [CrossRef]
- Bonaffini, P.A.; Franco, P.N.; Bonanomi, A.; Giaccherini, C.; Valle, C.; Marra, P.; Norsa, L.; Marchetti, M.; Falanga, A.; Sironi, S. Ischemic and hemorrhagic abdominal complications in COVID-19 patients: Experience from the first Italian wave. Eur. J. Med. Res. 2022, 27, 165. [Google Scholar] [CrossRef]
- Abdelmohsen, M.A.; Alkandari, B.M.; Gupta, V.K.; Elsebaie, N. Gastrointestinal tract imaging findings in confirmed COVID-19 patients: A non-comparative observational study. Egypt. J. Radiol. Nucl. Med. 2021, 52, 52. [Google Scholar] [CrossRef]
- Neuberger, M.; Jungbluth, A.; Irlbeck, M.; Streitparth, F.; Burian, M.; Kirchner, T.; Werner, J.; Rudelius, M.; Knösel, T. Duodenal tropism of SARS-CoV-2 and clinical findings in critically ill COVID-19 patients. Infection 2022, 50, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Butorin, N.N.; Tsukanov, V.V.; Asyayev, R.V.; Butorina, M.N.; Vasyutin, A.V.; Tonkikh, J.L. The frequency of ulcerative-erosive defects and ulcerative bleeding of the gastroduodenal zone in patients with coronavirus infection COVID-19. Exp. Clin. Gastroenterol. 2022, 5–11. [Google Scholar] [CrossRef]
- Demelo-Rodriguez, P.; Galeano-Valle, F.; Ordieres-Ortega, L.; Siniscalchi, C.; Del Pozo, M.M.; Fidalgo, Á.; Gil-Díaz, A.; Lobo, J.L.; De Ancos, C.; Monreal, M.; et al. Validation of a Prognostic Score to Identify Hospitalized Patients with COVID-19 at Increased Risk for Bleeding. Viruses 2021, 13, 2278. [Google Scholar] [CrossRef]
- Kalra, P.R.; Greenlaw, N.; Ferrari, R.; Ford, I.; Tardif, J.C.; Tendera, M.; Reid, C.M.; Danchin, N.; Stepinska, J.; Steg, P.G.; et al. Hemoglobin and Change in Hemoglobin Status Predict Mortality, Cardiovascular Events, and Bleeding in Stable Coronary Artery Disease. Am. J. Med. 2017, 130, 720–730. [Google Scholar] [CrossRef]
- Barcellona, D.; Fenu, L.; Marongiu, F. Point-of-care testing INR: An overview. Clin. Chem. Lab. Med. CCLM 2017, 55, 800–805. [Google Scholar] [CrossRef]
- Yang, R.; Moosavi, L. Prothrombin Time; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Weitz, J.I.; Fredenburgh, J.C.; Eikelboom, J.W. A Test in Context: D-Dimer. J. Am. Coll. Cardiol. 2017, 70, 2411–2420. [Google Scholar] [CrossRef]
- Kim, J.S.; Lee, J.Y.; Yang, J.W.; Lee, K.H.; Effenberger, M.; Szpirt, W.; Kronbichler, A.; Shin, J.I. Immunopathogenesis and treatment of cytokine storm in COVID-19. Theranostics 2021, 11, 316–329. [Google Scholar] [CrossRef]
- Wagner, C.; Griesel, M.; Mikolajewska, A.; Mueller, A.; Nothacker, M.; Kley, K.; Metzendorf, M.-I.; Fischer, A.-L.; Kopp, M.; Stegemann, M.; et al. Systemic corticosteroids for the treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 2021, CD014963. [Google Scholar] [CrossRef]
- Chaudhuri, D.; Sasaki, K.; Karkar, A.; Sharif, S.; Lewis, K.; Mammen, M.J.; Alexander, P.; Ye, Z.; Lozano, L.E.C.; Munch, M.W.; et al. Corticosteroids in COVID-19 and non-COVID-19 ARDS: A systematic review and meta-analysis. Intensive Care Med. 2021, 47, 521–537. [Google Scholar] [CrossRef]
- Halpin, D.M.G.; Singh, D.; Hadfield, R.M. Inhaled corticosteroids and COVID-19: A systematic review and clinical perspective. Eur. Respir. J. 2020, 55, 2001009. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Siegal, D.M. Anticoagulant-associated gastrointestinal bleeding: Framework for decisions about whether, when and how to resume anticoagulants. J. Thromb. Haemost. 2021, 19, 2383–2393. [Google Scholar] [CrossRef] [PubMed]
- Barnes, G.D.; Burnett, A.; Allen, A.; Ansell, J.; Blumenstein, M.; Clark, N.P.; Crowther, M.; Dager, W.E.; Deitelzweig, S.B.; Ellsworth, S.; et al. Thromboembolic prevention and anticoagulant therapy during the COVID-19 pandemic: Updated clinical guidance from the anticoagulation forum. J. Thromb. Thrombolysis 2022, 54, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Asakura, H.; Ogawa, H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int. J. Hematol. 2021, 113, 45–57. [Google Scholar] [CrossRef]
- Gómez-Mesa, J.E.; Galindo-Coral, S.; Montes, M.C.; Martin, A.J.M. Thrombosis and Coagulopathy in COVID-19. Curr. Probl. Cardiol. 2021, 46, 100742. [Google Scholar] [CrossRef]
- Miesbach, W.; Makris, M. COVID-19: Coagulopathy, Risk of Thrombosis, and the Rationale for Anticoagulation. Clin. Appl. Thromb. Hemost. 2020, 26, 1–7. [Google Scholar] [CrossRef]
- Iba, T.; Connors, J.M.; Levy, J.H. The coagulopathy, endotheliopathy, and vasculitis of COVID-19. Inflamm. Res. 2020, 69, 1181–1189. [Google Scholar] [CrossRef]
- Kherad, O.; Restellini, S.; Martel, M.; Barkun, A. Proton pump inhibitors for upper gastrointestinal bleeding. Best Pract. Res. Clin. Gastroenterol. 2019, 42–43, 101609. [Google Scholar] [CrossRef] [PubMed]
- Barkun, A.N.; Almadi, M.; Kuipers, E.J.; Laine, L.; Sung, J.; Tse, F.; Leontiadis, G.I.; Abraham, N.S.; Calvet, X.; Chan, F.K.; et al. Management of Nonvariceal Upper Gastrointestinal Bleeding: Guideline Recommendations from the International Consensus Group. Ann. Intern. Med. 2019, 171, 805. [Google Scholar] [CrossRef] [PubMed]
- Laine, L.; Jensen, D.M. Management of Patients with Ulcer Bleeding. Am. J. Gastroenterol. 2012, 107, 345–360. [Google Scholar] [CrossRef] [PubMed]
- Cavaliere, K.; Levine, C.; Wander, P.; Sejpal, D.V.; Trindade, A.J. Management of upper GI bleeding in patients with COVID-19 pneumonia. Gastrointest. Endosc. 2020, 92, 454–455. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Sengupta, N. PPIs and Beyond: A Framework for Managing Anticoagulation-Related Gastrointestinal Bleeding in the Era of COVID-19. Dig. Dis. Sci. 2020, 65, 2181–2186. [Google Scholar] [CrossRef] [PubMed]
- Sauerbruch, T.; Fischer, G. Conservative treatment of upper gastrointestinal bleeding in portal hypertension. Hepatogastroenterology 1991, 38, 350–354. [Google Scholar] [PubMed]
- Gralnek, I.M.; Stanley, A.J.; Morris, A.J.; Camus, M.; Lau, J.; Lanas, A.; Laursen, S.B.; Radaelli, F.; Papanikolaou, I.S.; Gonçalves, T.C.; et al. Endoscopic diagnosis and management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH): European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2021. Endoscopy 2021, 53, 300–332. [Google Scholar] [CrossRef]
- Strate, L.L.; Gralnek, I.M. ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding. Am. J. Gastroenterol. 2016, 111, 459–474. [Google Scholar] [CrossRef]
- Nett, A.; Binmoeller, K.F. Endoscopic Management of Portal Hypertension–related Bleeding. Gastrointest. Endosc. Clin. N. Am. 2019, 29, 321–337. [Google Scholar] [CrossRef]
- Bujanda, L.; Arratibel, P.; Gil, I.; Torrente, S.; Martos, M.; Enriquez-Navascues, J.M. Surgery and emergency gastrointestinal endoscopy during the Covid-19 pandemic. Gastroenterol. Hepatol. 2021, 44, 294–296. [Google Scholar] [CrossRef]
- Benites-Goñi, H.; Pascacio-Fiori, M.; Valle, F.M.-D.; Plácido-Damián, Z.; Gonzales-Carazas, E.; Padilla-Espinoza, M.; Prado-Bustamante, J.; Llatas-Pérez, J.; Dávalos-Moscol, M. Impact of the COVID-19 pandemic in the time to endoscopy in patients with upper gastrointestinal bleedin. Rev. Gastroenterol. Peru 2020, 40, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Ierardi, A.M.; Coppola, A.; Tortora, S.; Valconi, E.; Piacentino, F.; Fontana, F.; Stellato, E.; Cogliati, C.B.; Torzillo, D.; Giampalma, E.; et al. Gastrointestinal Bleeding in Patients with SARS-CoV-2 Infection Managed by Interventional Radiology. J. Clin. Med. 2021, 10, 4758. [Google Scholar] [CrossRef]
- Ierardi, A.M.; Del Giudice, C.; Coppola, A.; Carnevale, A.; Giganti, M.; Renzulli, M.; Tacher, V.; Urbano, J.; Kobeiter, H.; Loffroy, R.; et al. Gastrointestinal Hemorrhages in Patients With COVID-19 Managed With Transarterial Embolization. Am. J. Gastroenterol. 2021, 116, 838–840. [Google Scholar] [CrossRef]
- Tavabie, O.D.; Clough, J.N.; Blackwell, J.; Bashyam, M.; Martin, H.; Soubieres, A.; Direkze, N.; Graham, D.; Groves, C.; Preston, S.L.; et al. Reduced survival after upper gastrointestinal bleed endoscopy in the COVID-19 era is a secondary effect of the response to the global pandemic: A retrospective cohort study. Frontline Gastroenterol. 2021, 12, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Barrett, L.F.; Lo, K.B.; Stanek, S.R.; Walter, J.W. Self-limited gastrointestinal bleeding in COVID-19. Clin. Res. Hepatol. Gastroenterol. 2020, 44, e77–e80. [Google Scholar] [CrossRef] [PubMed]
- Blackett, J.W.; Kumta, N.A.; Dixon, R.E.; David, Y.; Nagula, S.; DiMaio, C.J.; Greenwald, D.; Sharaiha, R.Z.; Sampath, K.; Carr-Locke, D.; et al. Characteristics and Outcomes of Patients Undergoing Endoscopy during the COVID-19 Pandemic: A Multicenter Study from New York City. Dig. Dis. Sci. 2021, 66, 2545–2554. [Google Scholar] [CrossRef] [PubMed]
- Adekunle, A.D.; Rubens, M.; Sedarous, M.; Tariq, T.; Okafor, P.N. Trends in gastrointestinal disease hospitalizations and outcomes during the first year of the coronavirus pandemic. World J. Gastroenterol. 2023, 29, 744–757. [Google Scholar] [CrossRef]
- Rehana, R.W.; Fahad, H.; Sadiq, O.; Schairer, J. Outcomes of Gastrointestinal Bleeding During the COVID-19 Pandemic. Gastro Hep Adv. 2022, 1, 342–343. [Google Scholar] [CrossRef]
- Iqbal, U.; Patel, P.D.; Pluskota, C.A.; Berger, A.L.; Khara, H.S.; Confer, B.D. Outcomes of Acute Gastrointestinal Bleeding in Patients With COVID-19: A Case-Control Study. Gastroenterol. Res. 2022, 15, 13–18. [Google Scholar] [CrossRef]
- Reddy, S.; Patel, B.; Baldelli, L.; Majithia, R.T.; Dougherty, M.K. Decreased Rate of Presentation, but Worsened Racial-Ethnic Disparity in Acute Gastrointestinal Bleeding During Coronavirus 2019 Shutdown: A Retrospective Cohort Study. Clin. Exp. Gastroenterol. 2022, 15, 67–77. [Google Scholar] [CrossRef]
- Smith, R.; Brooks, C.; Rammage, J. Short report on acute gastro-intestinal bleeding admissions during the COVID-19 pandemic. JGH Open 2022, 6, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, T.; Wheeler, B.; Carpenter, M. Upper Gastrointestinal Bleeding in Adults: Evaluation and Management. Am. Fam. Physician 2020, 101, 294–300. [Google Scholar] [PubMed]
- Samuel, R.; Bilal, M.; Tayyem, O.; Guturu, P. Evaluation and management of Non-variceal upper gastrointestinal bleeding. Dis. A Mon. 2018, 64, 333–343. [Google Scholar] [CrossRef] [PubMed]
- García-Rayado, G.; Lanas, A. Upper gastrointestinal bleeding in critically ill patients: Proton-pump inhibitors, histamine-2 receptor antagonists or placebo? Many questions remain unanswered. Curr. Med. Res. Opin. 2018, 34, 1881–1883. [Google Scholar] [CrossRef] [PubMed]
- Bardou, M.; Quenot, J.-P.; Barkun, A. Stress-related mucosal disease in the critically ill patient. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- Abu-Ssaydeh, D.A.; Rechnitzer, T.W.; Knowles, B.P.; Richmond, T.S. Major haemorrhage associated with the Flexi-Seal® Fecal Management System. Anaesth. Intensive Care 2018, 46, 140. [Google Scholar] [PubMed]
- Tiwari, A.; Sharma, H.; Qamar, K.; Alastal, Y.; Sodeman, T.; Nawras, A. The Traumatic Tube: Bleeding Rectal Ulcer Caused by Flexi-Seal Device. Case Rep. Gastrointest Med. 2017, 2017, 5278971. [Google Scholar] [CrossRef]
- Padmanabhan, A.; Stern, M.; Wishin, J.; Mangino, M.; Richey, K.; DeSane, M.; Flexi-Seal Clinical Trial Investigators Group. Clinical evaluation of a flexible fecal incontinence management system. Am. J. Crit. Care 2007, 16, 384–393. [Google Scholar] [CrossRef]
- Akinosoglou, K.; Savopoulos, C.; Pouliakis, A.; Triantafyllidis, C.; Markatis, E.; Golemi, F.; Liontos, A.; Vadala, C.; Papanikolaou, I.C.; Dimakopoulou, V.; et al. Intensive-Dose Tinzaparin in Hospitalized COVID-19 Patients: The INTERACT Study. Viruses 2022, 14, 767. [Google Scholar] [CrossRef]
- Goligher, E.C.; Bradbury, C.A.; McVerry, B.J.; Lawler, P.R.; Berger, J.S.; Gong, M.N. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with Covid-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar] [CrossRef]
- Cate, H.T. Surviving Covid-19 with Heparin? N. Engl. J. Med. 2021, 385, 845–846. [Google Scholar] [CrossRef]
- Leung, W.K.; To, K.-F.; Chan, P.K.; Chan, H.L.; Wu, A.K.; Lee, N.; Yuen, K.Y.; Sung, J.J. Enteric involvement of severe acute respiratory syndrome-associated coronavirus infection. Gastroenterology 2003, 125, 1011–1017. [Google Scholar] [CrossRef]
- Marasco, G.; Maida, M.; Morreale, G.C.; Licata, M.; Renzulli, M.; Cremon, C.; Stanghellini, V.; Barbara, G. Gastrointestinal Bleeding in COVID-19 Patients: A Systematic Review with Meta-Analysis. Can. J. Gastroenterol. Hepatol. 2021, 2021, 2534975. [Google Scholar] [CrossRef]












| P (patient/population) | General Population |
| I (intervention/exposure) | COVID-19 infection |
| C (comparison) | - |
| O (outcome) | Gastrointestinal Bleeding events/prevalence of GI bleeding |
| Study ID | Hematocrit (%) | Hemoglobin (g/dL) | Platelet (×103/mm3) | Protomobin Time (s.) | International Normalized Ratio (INR) | D-Dimer (μg/mL) |
|---|---|---|---|---|---|---|
| Alakuş et al., 2022 [26] | 22.1–33.8 | 7.2–11.2 | 88–192 | 13.3–15.2 | 1.16–1.3 | 1.8–2.3 |
| Mauro et al., 2021 [27] | NM | 9 (8.1–10.8) | NM | NM | NM | 0.919 (0.621–2.046) |
| Trindade et al., 2021 [28] | NM | 7.80 (6.80, 10.00) | NM | NM | NM | NM |
| Makker et al., 2021 [29] | NM | 12 (±3) | 236 (±143) | 13 | NM | 1.034 |
| Prasoppokakorn et al., 2022 [31] | 22.5 ± 5.3 | 7.5 ± 1.8 (baseline: 12.6 ± 1.7) | NM | 15.6 ± 5.8 | 1.41 ± 0.54 | NM |
| González et al., 2022 [32] | NM | 10.4 (3.2) | NM | NM | NM | NM |
| Zellmer et al., 2021 [35] | NM | In 22.2% of patients, it was <12 | In 57.3% of patients, it was <200 | NM | In 8.6% of patients, it was >1.25 | NM |
| Abowali et al., 2022 [36] | NM | NM | NM | 14.6 (13.5–16.8) | NM | 0.905 (0.508–4.924) |
| Abulawi et al., 2022 [37] | NM | 10.1 ± 2.2 | NM | NM | NM | 2.10 (1.17–10.16) |
| Shalimar et al., 2021 [38] | NM | 7.2 (5.8–9.0) | 90.5 (52–135) | NM | 1.2 (1.2–1.4) | NM |
| Shao et al., 2020 [40] | NM | 11.9 ± 3.2 | 177.50 ± 110.57 | 12.20 (11.50–13.40) | NM | 0.49 (0.27–2.13) |
| Zhao et al., 2021 [42] | NM | 12.6 (11.7–14.4) | 161.0 (113.0–238.0) | 14.2 (12.9–15.7) | NM | 2.1 (0.9–11.4) |
| Martin et al., 2020 [43] | NM | 7.5 | 250 | NM | 1.2 | 4.34 |
| Al-Samkari et al., 2020 [45] | NM | NM | 124 (95–154) | 16.3 (14.6–17.4) | 1.3 (1.2–1.4) | 3.6(2.1–4.7) |
| Mattioli et al., 2021 [47] | NM | 12.1 (10.9–13) | 278.5 (186–348) | NM | 1.25 (1.2–1.4) | 1.4 (0.9–2.3) |
| Russell et al., 2022 [51] | NM | 7.9 (6.7–8.6) | 214 (155–290) | NM | 1.1 (1.0–1.2) | 1.7 (1.0–4.2) |
| Bychinin et al., 2022 [52] | NM | NM | 189 (83.3–243) | NM | NM | 0.98 (0.2–1.5) |
| Bonafni et al., 2022 [53] | NM | NM | 239 (184–356) | NM | 1.17 (1.08–1.49) | 1.8 (1.1–3.1) |
| Demelo-Rodriguez et al., 2021 [57] | 34% of patients were anemic | 34% of patients were anemic | In 6% of patients, it was <100,000 | In 32.5% of patients, it was >13.5 s | NM | In 94% of patients, it was >upper normal limit |
| COVID-19 Treatments during Hospitalization in Patients with GIB | |
|---|---|
| Corticosteroids | 112 |
| Anticoagulant and antiplatelet therapy | 215 |
| LMWH | 110 |
| PPI | 141 |
| Study ID | Selection | Comparability | Outcome | Total | Quality | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the Exposed Cohort | Selection of the Non-Exposed Cohort | Ascertainment of Exposure | Demonstration that Outcome of Interest was not Present at the Start of the Study | Comparability of Cohorts on the Basis of the Design or Analysis Controlled for Confounders | Assessment of Outcome | Was Follow-Up Long enough for Outcomes to Occur | Adequacy of Follow-Up of Cohorts | |||
| Abdelmohsen et al., 2021 [54] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Abowali et al., 2022 [36] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Abulawi et al., 2022 [37] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Alakuş et al., 2022 [26] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Al-Samkari et al., 2020 [45] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Bonafni et al., 2022 [53] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Bunch et al., 2021 [49] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Bychinin et al., 2022 [52] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Chen et al., 2021 [25] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Fanning et al., 2023 [41] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| González et al., 2022 [32] | * | * | * | * | ** | * | * | * | 9/9 | GOOD |
| Lak et al., 2022 [33] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Lin et al., 2020 [39] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Makker et al., 2021 [29] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Martin et al., 2020 [43] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Mattioli et al., 2021 [47] | * | * | * | * | ** | * | * | * | 9/9 | GOOD |
| Mauro et al., 2021 [27] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Neuberger et al., 2022 [55] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Nikolay N. et al., 2022 [56] | * | * | ** | * | * | * | 7/9 | GOOD | ||
| Patell et al., 2020 [48] | * | * | ** | * | * | * | 8/9 | GOOD | ||
| Popa et al., 2022 [30] | * | * | * | * | ** | * | * | * | 9/9 | GOOD |
| Prasoppokakorn et al., 2022 [31] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Qiu et al., 2021 [50] | * | * | * | * | ** | * | * | * | 9/9 | GOOD |
| Rosevics et al., 2021 [34] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Russell et al., 2022 [51] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Shalimar et al., 2021 [38] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Shao et al., 2020 [40] | * | * | ** | * | 5/9 | FAIR* | ||||
| Trindade et al., 2021 [28] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Wan et al., 2020 [46] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Xiao et al., 2020 [44] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Zellmer et al., 2021 [35] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
| Zhao et al., 2021 [42] | * | * | * | ** | * | * | * | 8/9 | GOOD | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karlafti, E.; Tsavdaris, D.; Kotzakioulafi, E.; Protopapas, A.A.; Kaiafa, G.; Netta, S.; Savopoulos, C.; Michalopoulos, A.; Paramythiotis, D. The Prevalence of Gastrointestinal Bleeding in COVID-19 Patients: A Systematic Review and Meta-Analysis. Medicina 2023, 59, 1500. https://doi.org/10.3390/medicina59081500
Karlafti E, Tsavdaris D, Kotzakioulafi E, Protopapas AA, Kaiafa G, Netta S, Savopoulos C, Michalopoulos A, Paramythiotis D. The Prevalence of Gastrointestinal Bleeding in COVID-19 Patients: A Systematic Review and Meta-Analysis. Medicina. 2023; 59(8):1500. https://doi.org/10.3390/medicina59081500
Chicago/Turabian StyleKarlafti, Eleni, Dimitrios Tsavdaris, Evangelia Kotzakioulafi, Adonis A. Protopapas, Georgia Kaiafa, Smaro Netta, Christos Savopoulos, Antonios Michalopoulos, and Daniel Paramythiotis. 2023. "The Prevalence of Gastrointestinal Bleeding in COVID-19 Patients: A Systematic Review and Meta-Analysis" Medicina 59, no. 8: 1500. https://doi.org/10.3390/medicina59081500