
Validation of a Prognostic Score to Identify Hospitalized Patients with COVID-19 at Increased Risk for Bleeding

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Study Design
2.3. Variables of Interest
2.4. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Cui, S.; Chen, S.; Li, X.; Liu, S.; Wang, F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 1421–1424. [Google Scholar] [CrossRef]
- Fernández-Capitán, C.; Barba, R.; Díaz-Pedroche, M.D.C.; Sigüenza, P.; Demelo-Rodriguez, P.; Siniscalchi, C.; Pedrajas, J.M.; Farfán-Sedano, A.I.; Olivera, P.E.; Gómez-Cuervo, C.; et al. Presenting Characteristics, Treatment Patterns, and Outcomes among Patients with Venous Thromboembolism during Hospitalization for COVID-19. Semin. Thromb. Hemost. 2020, 47, 351–361. [Google Scholar] [CrossRef]
- Martín-Rojas, R.M.; Pérez-Rus, G.; Delgado-Pinos, V.E.; Domingo-González, A.; Regalado-Artamendi, I.; Alba-Urdiales, N.; Demelo-Rodríguez, P.; Monsalvo, S.; Rodríguez-Macías, G.; Ballesteros, M.; et al. COVID-19 coagulopathy: An in-depth analysis of the coagulation system. Eur. J. Haematol. 2020, 105, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, D.; García-Sanchez, A.; Rali, P.; Muriel, A.; Bikdeli, B.; Ruiz-Artacho, P.; Le Mao, R.; Rodríguez, C.; Hunt, B.J.; Monreal, M. Incidence of venous thromboembolism and bleeding among hospitalized patients with COVID-19: A systematic review and meta-analysis. Chest 2020, 159, 1182–1196. [Google Scholar] [CrossRef]
- Marchandot, B.; Trimaille, A.; Curtiaud, A.; Matsushita, K.; Jesel, L.; Morel, O. Thromboprophylaxis: Balancing evidence and experience during the COVID-19 pandemic. J. Thromb. Thrombolysis 2020, 50, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Moores, K.; Tritschler, T.; Brosnahan, S.; Carrier, M.; Collen, J.F.; Doerschug, K.; Holley, A.B.; Jimenz, D.; Wells, P.; Le Gal, G.; et al. Prevention, diagnosis, and treatment of VTE in patients with coronavirus disease 2019: CHEST guideline and expert panel report. Chest 2020, 158, 1143–1163. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Levy, J.H.; Ageno, W.; Connors, J.M.; Hunt, B.J.; Iba, T.; Levi, M.; Samama, C.M.; Giannis, D. Scientific and Standardization Committee communication: Clinical guidance on the diagnosis, prevention, and treatment of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb Haemost. 2020, 18, 1859–1865. [Google Scholar] [CrossRef] [PubMed]
- Tritschler, T.; Mathieu, M.; Skeith, L.; Rodger, M.; Middeldorp, S.; Brighton, T.; Sandset, P.M.; Kahn, S.R.; Angus, D.C.; Blondon, M.; et al. Anticoagulant interventions in hospitalized patients with COVID-19: A scoping review of randomized controlled trials and call for international collaboration. J. Thromb. Haemost. 2020, 18, 2958–2967. [Google Scholar] [CrossRef]
- Sadeghipour, P.; Talasaz, A.H.; Rashidi, F.; Sharif-Kashani, B.; Beigmohammadi, M.T.; Farrokhpour, M.; The INSPIRATION Investigators. Effect of Intermediate-Dose vs Standard-Dose Prophylactic Anticoagulation on Thrombotic Events, Extracorporeal Membrane Oxygenation Treatment, or Mortality Among Patients With COVID-19 Admitted to the Intensive Care Unit: The INSPIRATION Randomized Clinical Trial. JAMA 2021, 27, 1620–1630. [Google Scholar]
- The REMAP-CAP, ACTIV-4a, and ATTACC Investigators. Therapeutic anticoagulation with heparin in critically ill patients with Covid-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar] [CrossRef]
- The ATTACC, ACTIV-4a, and REMAP-CAP Investigators. Therapeutic anticoagulation with heparin in noncritically ill patients with Covid-19. N. Engl. J. Med. 2021, 385, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; de Barros, E.; Silva, P.G.M.; Furtado, R.H.M.; Macedo, A.V.S.; Bronhara, B.; Damiani, L.P. Therapeutic versus prophylactic anticoagulation for patients admitted to hospital with COVID-19 and elevated D-dimer concentration (ACTION): An open-label, multicentre, randomised, controlled trial. Lancet 2021, 397, 2253–2263. [Google Scholar] [CrossRef]
- Bikdeli, B.; Jimenez, D.; Hawkins, M.; Ortíz, S.; Prandoni, P.; Brenner, B.; Decousus, H.; Masoudi, F.A.; Trujillo-Santos, J.; Krumholz, H.M.; et al. Rationale, Design and Methodology of the Computerized Registry of Patients with Venous Thromboembolism (RIETE). Thromb. Haemost. 2018, 118, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Demelo-Rodriguez, P.; Farfán-Sedano, A.I.; Pedrajas, J.M.; Llamas, P.; Sigüenza, P.; Jaras, M.J.; Quintana-Diaz, M.; Fernández-Capitán, C.; Bikdeli, B.; Jiménez, D.; et al. Bleeding risk in hospitalized patients with COVID-19 receiving intermediate- or therapeutic doses of thromboprophylaxis. J. Thromb. Haemost. 2021, 19, 1981–1989. [Google Scholar] [CrossRef] [PubMed]
- Bilaloglu, S.; Aphinyanaphongs, Y.; Jones, S.; Iturrate, E.; Hochman, J.; Berger, J.S. Thrombosis in Hospitalized Patients with COVID-19 in a New York City Health System. JAMA 2020, 324, 799. [Google Scholar] [CrossRef] [PubMed]
- Paranjpe, I.; Fuster, V.; Lala, A.; Russak, A.J.; Glicksberg, B.S.; Levin, M.A.; Charney, A.W.; Narula, J.; Fayad, Z.A.; Bagiella, E.; et al. Association of Treatment Dose Anticoagulation With In-Hospital Survival Among Hospitalized Patients With COVID-19. J. Am. Coll. Cardiol. 2020, 76, 122–124. [Google Scholar] [CrossRef]
- Llitjos, J.-F.; Leclerc, M.; Chochois, C.; Monsallier, J.-M.; Ramakers, M.; Auvray, M.; Merouani, K. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J. Thromb. Haemost. 2020, 18, 1743–1746. [Google Scholar] [CrossRef]
- Demelo-Rodríguez, P.; Cervilla-Muñoz, E.; Ordieres-Ortega, L.; Parra-Virto, A.; Toledano-Macías, M.; Toledo-Samaniego, N.; García-García, A.; García-Fernández-Bravo, I.; Ji, Z.; De-Miguel-Diez, J.; et al. Incidence of Asymptomatic Deep Vein Thrombosis in Patients With COVID-19 Pneumonia and Elevated D-dimer Levels. Thromb. Res. 2020, 192, 23–26. [Google Scholar] [CrossRef]
- Weinberg, I.; Fernández-Capitán, C.; Quintana-Díaz, M.; Demelo-Rodriguez, P.; de Casasola, G.G.; Fidalgo, Á.; Suriñach, J.M.; Díaz-Pedroche, C.; Galeano-Valle, F.; Siniscalchi, C.; et al. Systematic testing for venous thromboembolism in hospitalized patients with COVID-19 and raised D-dimer levels. Thromb. Update 2020, 2, 100029. [Google Scholar] [CrossRef]
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M.; Clark, C.; Iba, T. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 1023–1026. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patell, R.; Bogue, T.; Bindal, P.; Koshy, A.; Merrill, M.; Aird, W.C.; Bauer, K.A.; Zwicker, J.I. Incidence of thrombosis and hemorrhage in hospitalized cancer patients with COVID-19. J. Thromb. Haemost. 2020, 18. [Google Scholar] [CrossRef] [PubMed]
- Pesavento, R.; Ceccato, D.; Pasquetto, G.; Monticelli, J.; Leone, L.; Frigo, A.; Gorgi, D.; Postal, A.; Marchese, G.M.; Cipriani, A.; et al. The hazard of (sub)therapeutic doses of anticoagulants in non-critically ill patients with Covid-19: The Padua province experience. J. Thromb. Haemost. 2020, 18. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Tacquard, C.; Severac, F. CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis). High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Karp Leaf, R.S.; Dzik, W.H.; Carlson, J.C.T.; Fogerty, A.E.; Waheed, A. COVID-19 and coagulation: Bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef]
- Ten Cate, H. Surviving COVID-19 with heparin? N. Eng. J. Med. 2021, 385, 845–846. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N | Standard Doses | Intermediate Doses | Therapeutic Doses | Other Drugs | |
|---|---|---|---|---|---|
| Patients, N | 972 | 280 | 412 | 157 | 123 |
| Clinical characteristics, | |||||
| Male gender | 613 (63%) | 173 (62%) | 257 (62%) | 112 (71%) * | 71 (58%) |
| Age <70 years | 562 (58%) | 142 (51%) | 266 (65%) ‡ | 98 (62%) * | 56 (46%) |
| Body weight <70 kg | 157 (22%) | 54 (27%) | 73 (25%) | 16 (13%) † | 14 (17%) |
| Admitted in ICUs | 464 (48%) | 136 (49%) | 177 (43%) | 91 (58%) | 60 (50%) |
| Recent major bleeding | 10 (1.0%) | 2 (0.7%) | 5 (1.2%) | 1 (0.6%) | 2 (1.7%) |
| Blood tests, | |||||
| Anemia | 287 (30%) | 84 (30%) | 106 (26%) | 45 (29%) | 52 (42%) * |
| Platelet count <100,000/μL | 51 (5.3%) | 15 (5.4%) | 13 (3.2%) | 6 (3.8%) | 17 (14%) † |
| Fibrinogen <1000 mg/dL | 813 (89%) | 234 (91%) | 342 (87%) | 134 (88%) | 103 (95%) |
| Prothrombin time > 13.5 s | 360 (38%) | 88 (32%) | 126 (31%) | 61 (41%) | 85 (73%) ‡ |
| D-dimer > upper normal limit | 845 (90%) | 254 (93%) | 362 (91%) | 137 (91%) | 92 (79%) ‡ |
| D-dimer >10 × upper limit | 336 (36%) | 93 (34%) | 130 (33%) | 72 (48%) † | 41 (35%) |
| Ferritin >500 ng/mL (N = 809) | 569 (70%) | 169 (70%) | 242 (69%) | 99 (74%) | 59 (68%) |
| CrCl < 60 mL/min | 460 (47%) | 143 (51%) | 177 (43%) * | 53 (34%) ‡ | 87 (71%) ‡ |
| Concomitant therapies, | |||||
| Antiplatelet drugs | 144 (15%) | 39 (14%) | 57 (14%) | 18 (11%) | 30 (25%) † |
| VTE prophylaxis, | |||||
| Duration (median days, IQR) | 14.7 ± 10.3 | 15.7 ± 10.5 | 14.9 ± 10.1 | 14.9 ± 10.4 | 11.8 ± 9.7 ‡ |
| Prognostic score, | |||||
| Very low risk | 203 (21%) | 55 (20%) | 111 (27%) * | 0 | 37 (30%) * |
| Low risk | 285 (29%) | 96 (34%) | 124 (30%) | 34 (22%) † | 31 (25%) |
| Intermediate risk | 263 (27%) | 85 (30%) | 106 (26%) | 36 (23%) | 36 (29%) |
| High risk | 221 (23%) | 44 (16%) | 71 (17%) | 87 (55%) ‡ | 19 (15%) |
| Outcomes, | |||||
| Non-major bleeding | 67 (6.9%) | 21 (7.5%) | 23 (5.6%) | 15 (9.6%) | 8 (6.5%) |
| Major bleeding | 65 (6.7%) | 18 (6.4%) | 21 (5.1%) | 11 (7.0%) | 15 (12%) |
| Bleeding-related death | 30 (3.1%) | 7 (2.5%) | 10 (2.4%) | 5 (3.2%) | 8 (6.5%) |
| All-cause mortality, | |||||
| Yes | 230 (24%) | 53 (19%) | 79 (19%) | 46 (29%) * | 52 (43%) ‡ |
| Major Bleeding | Non-Major Bleeding | No Bleeding | All Patients | |
|---|---|---|---|---|
| Patients, N | 65 | 67 | 840 | 972 |
| Clinical characteristics, | ||||
| Male gender | 47 (72%) | 45 (67%) | 521 (62%) | 613 (63%) |
| Age <70 years | 37 (57%) | 46 (69%) | 479 (57%) | 562 (58%) |
| Body weight <70 kg | 7 (13%) | 11 (22%) | 139 (23%) | 157 (22%) |
| Admitted in ICUs | 54 (83%) ‡ | 59 (88%) ‡ | 351 (42%) | 464 (48%) |
| Recent major bleeding | 0 | 1 (1.5%) | 9 (1.1%) | 10 (1.0%) |
| Blood tests, | ||||
| Anemia | 17 (26%) | 28 (42%) * | 242 (29%) | 287 (30%) |
| Platelet count <100,000/μL | 4 (6.2%) | 4 (6.0%) | 43 (5.1%) | 51 (5.3%) |
| Fibrinogen <1000 mg/dL | 52 (84%) | 55 (89%) | 706 (90%) | 813 (89%) |
| Prothrombin time >13.5 s | 21 (32%) | 22 (33%) | 317 (39%) | 360 (38%) |
| D-dimer > upper normal limit | 63 (98%) † | 62 (97%) | 720 (89%) | 845 (90%) |
| D-dimer >10 × upper limit | 46 (72%) ‡ | 37 (58%) ‡ | 253 (31%) | 336 (36%) |
| Ferritin >500 ng/mL (N = 809) | 48 (84%) † | 53 (80%) * | 463 (67%) | 564 (70%) |
| CrCl <60 mL/min | 33 (51%) | 27 (40%) | 400 (48%) | 460 (47%) |
| Concomitant therapies, | ||||
| Antiplatelets | 15 (23%) * | 14 (21%) | 115 (14%) | 144 (15%) |
| VTE prophylaxis, | ||||
| Standard doses | 18 (28%) | 21 (31%) | 241 (29%) | 280 (29%) |
| Intermediate doses | 21 (32%) | 23 (34%) | 368 (44%) | 412 (42%) |
| Therapeutic doses | 11 (17%) | 15 (22%) | 131 (16%) | 157 (16%) |
| Other drugs | 15 (23%) * | 8 (12%) | 100 (12%) | 123 (13%) |
| Duration (median days, IQR) | 16 (10–26) | 15 (10–23) | 12 (7–18) | 12 (7–19) |
| Duration (>10 days) | 46 (71%) * | 48 (72%) * | 473 (56%) | 567 (58%) |
| 30-day mortality, | ||||
| Yes | 30 (46%) ‡ | 22 (33%) * | 178 (21%) | 230 (24%) |
| Major Bleeding | Bleeding-Related Death | Non-Major Bleeding | All Patients | |
|---|---|---|---|---|
| Patients, N | 65 | 30 | 67 | 132 |
| Orotracheal | 14 (22%) | 8 (27%) | 15 (22%) | 29 (22%) |
| Gastrointestinal | 18 (28%) | 7 (23%) | 7 (10%) | 25 (19%) |
| Hematoma | 10 (15%) | 5 (17%) | 7 (10%) | 17 (13%) |
| Genitourinary | 4 (6.2%) | 1 (3.3%) | 4 (6.0%) | 8 (6.1%) |
| Alveolar | 4 (6.2%) | 1 (3.3%) | 4 (6.0%) | 8 (6.1%) |
| Abdominal | 5 (7.7%) | 1 (3.3%) | 0 | 5 (3.8%) |
| Muscular | 4 (6.2%) | 1 (3.3%) | 1 (1.5%) | 5 (3.8%) |
| Intracranial | 3 (4.6%) | 1 (3.3%) | 0 | 3 (2.3%) |
| Other | 3 (4.6%) | 5 (17%) | 29 (43%) | 32 (24%) |
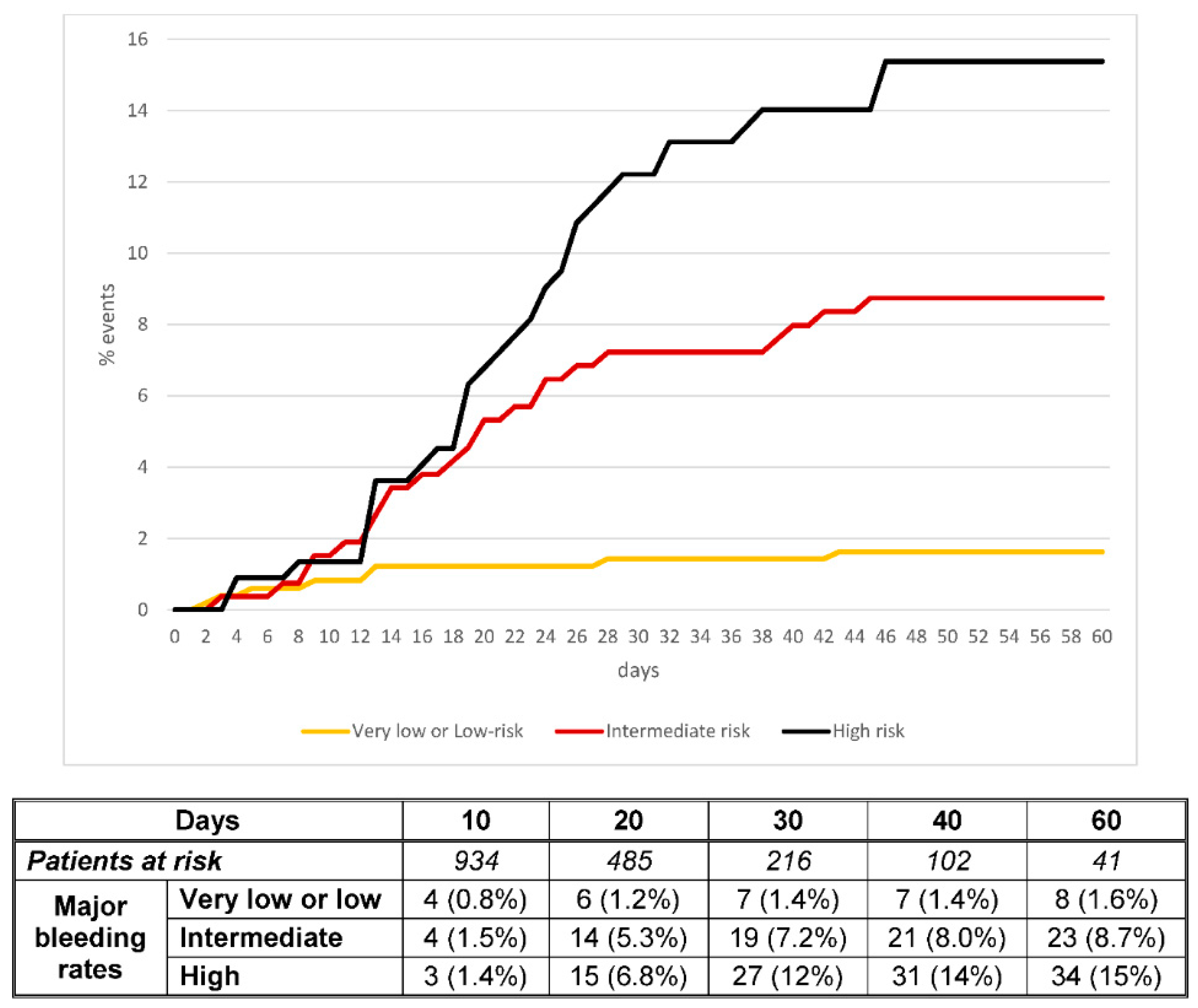
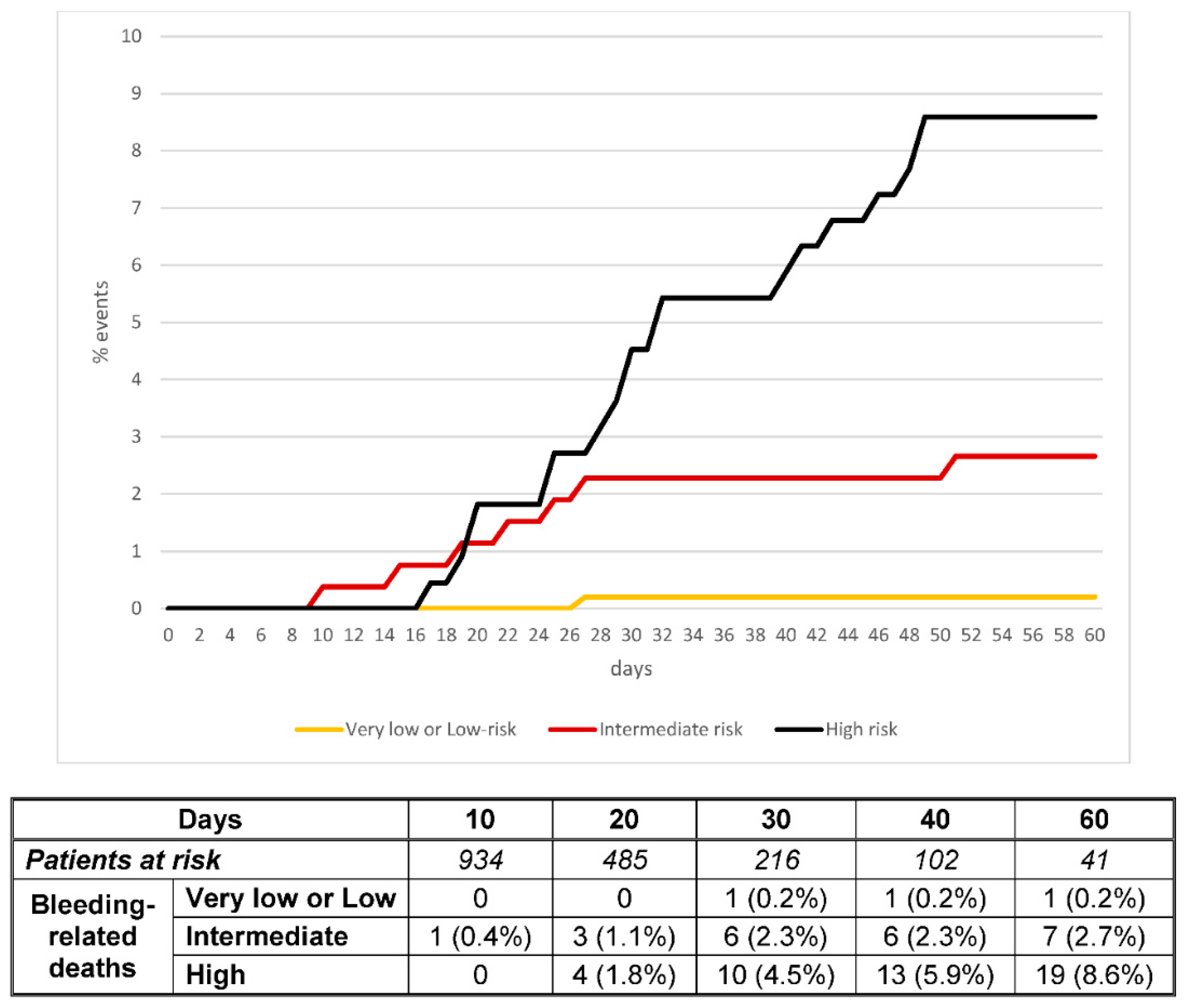
| Patients, N | Major Bleeding | Non-Major Bleeding | Bleeding-Related Death | |
|---|---|---|---|---|
| Estimated risk | ||||
| All patients | 972 | 65 (6.7%) | 67 (6.9%) | 30 (3.09%) |
| Very low risk (0 points) | 203 | 2 (1.0%) | 1 (0.5%) | 0 |
| Low risk (1 point) | 285 | 6 (2.1%) | 10 (3.5%) | 1 (0.35%) |
| Intermediate risk (2 points) | 263 | 23 (8.7%) | 25 (9.5%) | 7 (2.6%) |
| High risk (3–4 points) | 221 | 34 (15.4%) | 31 (14.2%) | 22 (9.9%) |
| C-statistics (95%CI) | ||||
| All patients | 972 | 0.74 (0.68–0.79) | 0.73 (0.67–0.78) | 0.82 (0.76–0.87) |
| Standard doses | 280 | 0.72 (0.60–0.84) | 0.72 (0.63–0.82) | 0.85 (0.70–1.00) |
| Intermediate doses | 412 | 0.76 (0.68–0.86) | 0.72 (0.63–0.82) | 0.84 (0.76–0.91) |
| Therapeutic doses | 157 | 0.66 (0.51–0.80) | 0.76 (0.63–0.88) | 0.79 (0.66–0.92) |
| Other drugs | 123 | 0.82 (0.72–0.92) | 0.74 (0.61–0.86) | 0.86 (0.77–0.95) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demelo-Rodriguez, P.; Galeano-Valle, F.; Ordieres-Ortega, L.; Siniscalchi, C.; Martín Del Pozo, M.; Fidalgo, Á.; Gil-Díaz, A.; Lobo, J.L.; De Ancos, C.; Monreal, M.; et al. Validation of a Prognostic Score to Identify Hospitalized Patients with COVID-19 at Increased Risk for Bleeding. Viruses 2021, 13, 2278. https://doi.org/10.3390/v13112278
Demelo-Rodriguez P, Galeano-Valle F, Ordieres-Ortega L, Siniscalchi C, Martín Del Pozo M, Fidalgo Á, Gil-Díaz A, Lobo JL, De Ancos C, Monreal M, et al. Validation of a Prognostic Score to Identify Hospitalized Patients with COVID-19 at Increased Risk for Bleeding. Viruses. 2021; 13(11):2278. https://doi.org/10.3390/v13112278
Chicago/Turabian StyleDemelo-Rodriguez, Pablo, Francisco Galeano-Valle, Lucía Ordieres-Ortega, Carmine Siniscalchi, Mar Martín Del Pozo, Ángeles Fidalgo, Aída Gil-Díaz, José Luis Lobo, Cristina De Ancos, Manuel Monreal, and et al. 2021. "Validation of a Prognostic Score to Identify Hospitalized Patients with COVID-19 at Increased Risk for Bleeding" Viruses 13, no. 11: 2278. https://doi.org/10.3390/v13112278