
Current Evidence Using Pulsed Electromagnetic Fields in Osteoarthritis: A Systematic Review
 ,
,  ,
,
Abstract
:1. Introduction
1.1. Definition and Classification
1.2. Epidemiology
1.3. Risk Factors
1.4. Sign and Symptoms
1.5. Diagnostic Methods and Treatment Options
1.6. Study Objectives
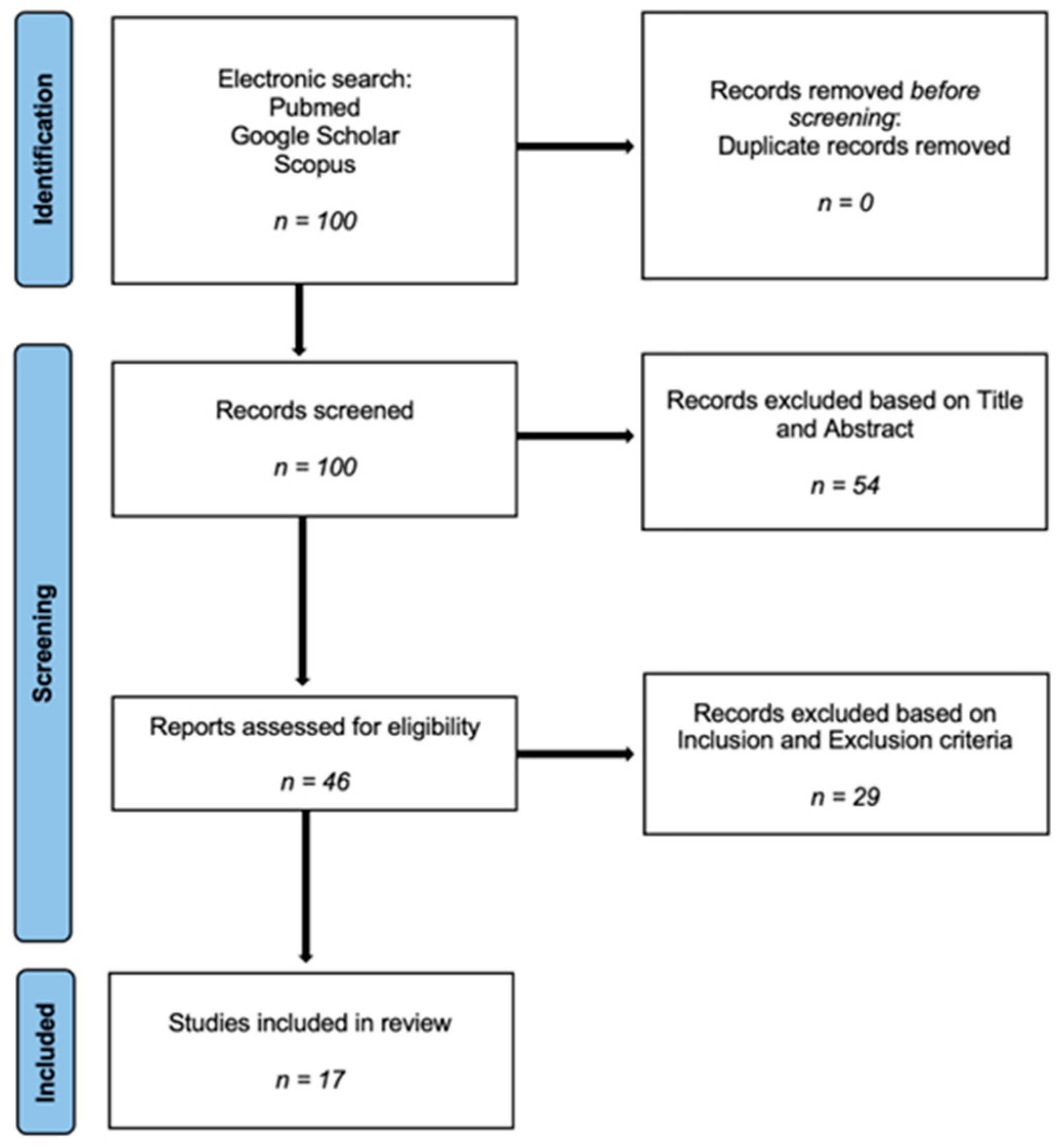
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Extraction and Outcome Measure
3. Results
3.1. Demographics
3.2. Type of PEMF Device
3.3. Treatment Duration
3.4. Anatomical Districts Involved
3.5. Outcomes

{kind=link}
| Research Study |
Number of Patients | Type of PEMF Device | Treatment Duration | Anatomical District | Assessment Scales | Outcomes | |
|---|---|---|---|---|---|---|---|
| 1 | Bagnato et al. (2016) [27] | 60 (43 F, 17 M) | Bioelectronics Corporation (27.12 MHz) | 12 h per day for 1 month | Knee | WOMAC, VAS, SF-36 | Pain reduction (primary outcome), assessment of quality of life (secondary outcome) |
| 2 | Wuschech et al. (2015) [31] | 57 | Magcell Arthro | 18 days (twice a day for 5 min) | Knee | WOMAC, VAS | Pain reduction, stiffness, and disability; tolerability and efficacy |
| 3 | HF Liu et al. (2015) [33] | 50 (F) | XT-2000 B | 5 weeks | Spine | Vas, SF-36, ODI; MMT score; BBS score; TUGscore | Primary outcome (change in femur bone mineral density); secondary outcome (change in mineral bone density of lumbar spine) |
| 4 | Dündar et al. (2016) [36] | 40 | 4 weeks | Knee | VAS, WOMAC | Pain reduction; utility of YKL-40 in assessing the severity of the condition | |
| 5 | Gobbi A et al. (2014) [20] | 22 (11 M; 11 F) | I-ONE IGEA | 45 days (4 h per day) | Knee | VAS, IKDC objective (KOOS); Tegner score | ROM, pain relief, improvement of symptoms, and improvement of activity level |
| 6 | Iannitti T et al. (2013) [37] | 28 | F&B International | 6 weeks | knee | VAS, WOMAC | Pain relief, stiffness, physical function |
| 7 | Nelson et al. (2012) [38] | 34 (24 F; 10 M) | knee | VAS | Pain relief | ||
| 8 | Ozgüçlü et al. (2010) [28] | 40 (29 F; 11 M) | Device Elettronica Pagani | 2 weeks | knee | VAS, WOMAC | Greater effectiveness than other non-surgical treatments |
| 9 | Khami et al. (2020) [35] | 40 (M) | Fisiofield Maxi | 18 sessions (3 times a week for 6 weeks) | Knee | Pettersson radiographic criteria, clinical signs, QoL, VAS, HJHS | The application of PEMFs could help to prevent further joint damage and prevent functional decline in patients |
| 10 | Xiang et al. (2022) [30] | 428 | Better Health Corporation (15 Hz, 30 mT) | 6 weeks (40 min/day, 5 days a week) | Knee | WOMAC pain index, WOMAC function and stiffness, pain, quality of life, 6-min-walk-test, responder index | |
| 11 | Yabroudi et al. (2023) [39] | 34 | 24 sessions (approximately 2 months) | Knee | KOOS, NPRS; walking speed and 5-times chair stand test | Decreasing pain and improving physical function | |
| 12 | Zorzi et al. (2007) [32] | 31 (15 M, 16 F) | I-ONE IGEA | 6 h per day for 90 days | Lower limbs | KOOS | Improving physical function |
| 13 | Ay et al. (2008) [40] | 55 (15 M, 40 F) | Knee | VAS, Likert, WOMAC | Pain relief, range of motion (ROM) | ||
| 14 | Stubeyaz et al. (2005) [34] | 34 | 30 min per session, twice a day for 3 weeks | Spine | VAS, NPDS | Pain, range of motion (ROM) and functional status | |
| 15 | Thamsborg et al. (2005) [41] | 83 | Biofields Aps | 2 h daily days per week for 6 weeks | Knee | WOMAC | Pain at all evaluations and stiffness |
| 16 | Pipitone et al. (2001) [42] | 75 | Medicur Devices | Three times a day | Knee | WOOMAC, Euro-QoL, SF-36 | Reduction in overall pain |
| 17 | Danao Camara et al. (2001) [43] | 167 | Knee and Spine | VAS, modified Ritchie scale | Pain and physician global assessment |
4. Discussion
4.1. Parameters
4.2. Type of PEMF Device
4.3. Treatment Duration and Frequency
4.4. Outcomes and Result Heterogeneity
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giorgino, R.; Albano, D.; Fusco, S.; Peretti, G.M.; Mangiavini, L.; Messina, C. Knee Osteoarthritis: Epidemiology, Pathogenesis, and Mesenchymal Stem Cells: What Else Is New? An Update. Int. J. Mol. Sci. 2013, 24, 6405. [Google Scholar] [CrossRef] [PubMed]
- Martel-Pelletier, J.; Barr, A.J.; Cicuttini, F.M.; Conaghan, P.G.; Cooper, C.; Goldring, M.B.; Goldring, S.R.; Jones, G.; Teichtahl, A.J.; Pelletier, J.-P. Osteoarthritis. Nat. Rev. Dis. Primers 2016, 2, 16072. [Google Scholar] [CrossRef]
- Vina, E.R.; Kwoh, C.K. Epidemiology of osteoarthritis: Literature update. Curr. Opin. Rheumatol. 2018, 30, 160–167. [Google Scholar] [CrossRef]
- Hall, A.J.; Stubbs, B.; Mamas, M.A.; Myint, P.K.; Smith, T.O. Association between osteoarthritis and cardiovascular disease: Systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2016, 23, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Bai, J.; He, B.; Hu, X.; Liu, D. Osteoarthritis and the risk of cardiovascular disease: A meta-analysis of observational studies. Sci. Rep. 2016, 6, 39672. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.H.; Seok, H.; Kim, J.; Song, G.G.; Choi, S.J. Association between osteoarthritis and mental health in a Korean population: A nationwide study. Int. J. Rheum. Dis. 2018, 21, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Cameron, M.L.; Briggs, K.K.; Steadman, J.R. Reproducibility and reliability of the outerbridge classification for grading chondral lesions of the knee arthroscopically. Am. J. Sports Med. 2003, 31, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Slattery, C.; Kweon, C.Y. Classifications in Brief: Outerbridge Classification of Chondral Lesions. Clin. Orthop. Relat. Res. 2018, 476, 2101–2104. [Google Scholar] [CrossRef] [PubMed]
- Johnson, V.L.; Hunter, D.J. The epidemiology of osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2014, 28, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Morales-Ivorra, I.; Romera-Baures, M.; Roman-Viñas, B.; Serra-Majem, L. Osteoarthritis and the Mediterranean Diet: A Systematic Review. Nutrients 2018, 10, 1030. [Google Scholar] [CrossRef] [PubMed]
- Perry, T.A.; Wang, X.; Gates, L.; Parsons, C.M.; Sanchez-Santos, M.T.; Garriga, C.; Cooper, C.; Nevitt, M.C.; Hunter, D.J.; Arden, N.K. Occupation and risk of knee osteoarthritis and knee replacement: A longitudinal, multiple-cohort study. Semin. Arthritis Rheum. 2020, 50, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Kiełbowski, K.; Herian, M.; Bakinowska, E.; Banach, B.; Sroczyński, T.; Pawlik, A. The Role of Genetics and Epigenetic Regulation in the Pathogenesis of Osteoarthritis. Int. J. Mol. Sci. 2023, 24, 11655. [Google Scholar] [CrossRef]
- Palazzo, C.; Nguyen, C.; Lefevre-Colau, M.M.; Rannou, F.; Poiraudeau, S. Risk factors and burden of osteoarthritis. Ann. Phys. Rehabil. Med. 2016, 59, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Mak, C.C.H.; Sharma, V.; To, K.; Khan, W. Mendelian Randomization Studies of Lifestyle-Related Risk Factors for Osteoarthritis: A PRISMA Review and Meta-Analysis. Int. J. Mol. Sci. 2022, 23, 11906. [Google Scholar] [CrossRef]
- Abramoff, B.; Caldera, F.E. Osteoarthritis: Pathology, Diagnosis, and Treatment Options. Med. Clin. N. Am. 2020, 104, 293–311. [Google Scholar] [CrossRef] [PubMed]
- Kohn, M.D.; Sassoon, A.A.; Fernando, N.D. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin. Orthop. Relat. Res. 2016, 474, 1886–1893. [Google Scholar] [CrossRef] [PubMed]
- Majeed, M.H.; Sherazi, S.A.A.; Bacon, D.; Bajwa, Z.H. Pharmacological Treatment of Pain in Osteoarthritis: A Descriptive Review. Curr. Rheumatol. Rep. 2018, 20, 88. [Google Scholar] [CrossRef] [PubMed]
- Postler, A.E.; Lützner, C.; Goronzy, J.; Lange, T.; Deckert, S.; Günther, K.P.; Lützner, J. When are patients with osteoarthritis referred for surgery? Best Pract. Res. Clin. Rheumatol. 2023, 37, 101835. [Google Scholar] [CrossRef] [PubMed]
- Previ, L.; Guidi, M.; Rescigno, G.; Di Niccolo, R.; Marzilli, F.; Perugia, D. First Metatarsal Bilateral Stress Fracture: A Case Report. J. Orthop. Case Rep. 2023, 13, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, A.; Lad, D.; Petrera, M.; Karnatzikos, G. Symptomatic Early Osteoarthritis of the Knee Treated with Pulsed Electromagnetic Fields: Two-Year Follow-up. Cartilage 2014, 5, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Xie, W.; Ye, W.; He, C. Effects of electromagnetic fields on osteoarthritis. Biomed. Pharmacother. 2019, 118, 109282. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Guo, H.; Ye, W.; Yang, L.; He, C. Pulsed Electromagnetic Field Attenuates Osteoarthritis Progression in a Murine Destabilization-Induced Model through Inhibition of TNF-α and IL-6 Signaling. Cartilage 2021, 13, 1665S–1675S. [Google Scholar] [CrossRef] [PubMed]
- Petecchia, L.; Sbrana, F.; Utzeri, R.; Vercellino, M.; Usai, C.; Visai, L.; Vassalli, M.; Gavazzo, P. Electro-magnetic field promotes osteogenic differentiation of BM-hMSCs through a selective action on Ca2+-related mechanisms. Sci. Rep. 2015, 5, 13856. [Google Scholar] [CrossRef] [PubMed]
- Brighton, C.T.; Wang, W.; Seldes, R.; Zhang, G.; Pollack, S.R. Signal transduction in electrically stimulated bone cells. J. Bone Jt. Surg. 2001, 83, 1514–1523. [Google Scholar] [CrossRef] [PubMed]
- Sollazzo, V.; Palmieri, A.; Pezzetti, F.; Massari, L.; Carinci, F. Effects of pulsed electromagnetic fields on human osteoblastlike cells (MG-63): A pilot study. Clin. Orthop. Relat. Res. 2010, 468, 2260–2277. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Yang, W.; Zeng, Q.; Chen, W.; Zhu, Y.; Liu, W.; Wang, S.; Wang, B.; Shao, Z.; Zhang, Y. Promising application of Pulsed Electromagnetic Fields (PEMFs) in musculoskeletal disorders. Biomed. Pharmacother. 2020, 131, 110767. [Google Scholar] [CrossRef] [PubMed]
- Bagnato, G.L.; Miceli, G.; Marino, N.; Sciortino, D.; Bagnato, G.F. Pulsed electromagnetic fields in knee osteoarthritis: A double blind, placebo-controlled, randomized clinical trial. Rheumatology 2015, 55, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Özgüçlü, E.; Çetin, A.; Çetin, M.; Calp, E. Additional effect of pulsed electromagnetic field therapy on knee osteoarthritis treatment: A randomized, placebo-controlled study. Clin. Rheumatol. 2010, 29, 927–931. [Google Scholar] [CrossRef]
- Markovic, L.; Wagner, B.; Crevenna, R. Effects of pulsed electromagnetic field therapy on outcomes associated with osteoarthritis: A systematic review of systematic reviews. Wien. Klin. Wochenschr. 2022, 134, 425–433. [Google Scholar] [CrossRef]
- Xiang, X.-N.; Zhu, S.-Y.; Song, K.-P.; Wang, X.-Y.; Liu, H.-Z.; Yang, W.-J.; Wang, H.; Zhang, C.; Yang, L.; He, C. Pulsed electromagnetic fields for the management of knee osteoarthritis: Multicentre, randomised, controlled, non-inferiority trial protocol. BMJ Open 2022, 12, e060350. [Google Scholar] [CrossRef] [PubMed]
- Wuschech, H.; von Hehn, U.; Mikus, E.; Funk, R.H. Effects of PEMF on patients with osteoarthritis: Results of a prospective, placebo-controlled, double-blind study. Bioelectromagnetics 2015, 36, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Zorzi, C.; Dall’Oca, C.; Cadossi, R.; Setti, S. Effects of pulsed electromagnetic fields on patients’ recovery after arthroscopic surgery: Prospective, randomized and double-blind study. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.-F.; He, H.-C.; Yang, L.; Yang, Z.-Y.; Yao, K.; Wu, Y.-C.; Yang, X.-B.; He, C.-Q. Pulsed electromagnetic fields for postmenopausal osteoporosis and concomitant lumbar osteoarthritis in southwest China using proximal femur bone mineral density as the primary endpoint: Study protocol for a randomized controlled trial. Trials 2015, 16, 265. [Google Scholar] [CrossRef] [PubMed]
- Sutbeyaz, S.T.; Sezer, N.; Koseoglu, B.F. The effect of pulsed electromagnetic fields in the treatment of cervical osteoarthritis: A randomized, double-blind, sham-controlled trial. Rheumatol. Int. 2005, 26, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Khami, A.; Roostayi, M.M.; Parhampour, B.; Heidari, Z.; Baharlouei, H.; Hoorfar, H. Effect of Pulsed Electromagnetic Fields on Clinical Signs and Quality of Life in Patients with Hemophilic Arthropathy of the Knee Joint: A Randomized Controlled Trial. Adv. Biomed. Res. 2020, 9, 81. [Google Scholar] [CrossRef]
- Dündar, Ü.; Aşık, G.; Ulaşlı, A.M.; Sınıcı, Ş.; Yaman, F.; Solak, Ö.; Toktaş, H.; Eroğlu, S. Assessment of pulsed electromagnetic field therapy with Serum YKL-40 and ultrasonography in patients with knee osteoarthritis. Int. J. Rheum. Dis. 2015, 19, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Iannitti, T.; Fistetto, G.; Esposito, A.; Rottigni, V.; Palmieri, B. Pulsed electromagnetic field therapy for management of osteoarthritis-related pain, stiffness and physical function: Clinical experience in the elderly. Clin. Interv. Aging 2013, 8, 1289–1293. [Google Scholar] [CrossRef] [PubMed]
- Nelson, F.R.; Zvirbulis, R.; Pilla, A.A. Non-invasive electromagnetic field therapy produces rapid and substantial pain reduction in early knee osteoarthritis: A randomized double-blind pilot study. Rheumatol. Int. 2013, 33, 2169–2173. [Google Scholar] [CrossRef] [PubMed]
- Yabroudi, M.A.; Aldardour, A.; Nawasreh, Z.H.; Obaidat, S.M.; Altubasi, I.M.; Bashaireh, K. Effects of the combination of pulsed electromagnetic field with progressive resistance exercise on knee osteoarthritis: A randomized controlled trial. J. Back Musculoskelet. Rehabil. 2024, 37, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Ay, S.; Evcik, D. The effects of pulsed electromagnetic fields in the treatment of knee osteoarthritis: A randomized, placebo-controlled trial. Rheumatol. Int. 2009, 29, 663–666. [Google Scholar] [CrossRef] [PubMed]
- Thamsborg, G.; Florescu, A.; Oturai, P.; Fallentin, E.; Tritsaris, K.; Dissing, S. Treatment of knee osteoarthritis with pulsed electromagnetic fields: A randomized, double-blind, placebo-controlled study. Osteoarthr. Cartil. 2005, 13, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Pipitone, N.; Scott, D.L. Magnetic Pulse Treatment for Knee Osteoarthritis: A Randomised, Double-Blind, Placebo-Controlled Study. Curr. Med. Res. Opin. 2001, 17, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Danao-Camara, T.; Tabrah, F.L. The use of pulsed electromagnetic fields (PEMF) in osteoarthritis (OA) of the knee preliminary report. Hawaii Med. J. 2001, 60, 288–300. [Google Scholar] [PubMed]

| Results | |||
|---|---|---|---|
| Total enrolled patients | 1197 | 35.8% M | 64.1% F |
| Treatment duration | 15 days to 90 days (median 52.5) | ||
| Anatomical district | 77% knee osteoarthritis (71% KL 2–3°, 14.2% KL 0–2°) | 20% spine osteoarthritis | |
| Decrease in the VAS scale | 60 ± 11% | ||
| Improvement WOMAC score | 42% (95% CI −85 to 17) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cianni, L.; Di Gialleonardo, E.; Coppola, D.; Capece, G.; Libutti, E.; Nannerini, M.; Maccauro, G.; Vitiello, R. Current Evidence Using Pulsed Electromagnetic Fields in Osteoarthritis: A Systematic Review. J. Clin. Med. 2024, 13, 1959. https://doi.org/10.3390/jcm13071959
Cianni L, Di Gialleonardo E, Coppola D, Capece G, Libutti E, Nannerini M, Maccauro G, Vitiello R. Current Evidence Using Pulsed Electromagnetic Fields in Osteoarthritis: A Systematic Review. Journal of Clinical Medicine. 2024; 13(7):1959. https://doi.org/10.3390/jcm13071959
Chicago/Turabian StyleCianni, Luigi, Emidio Di Gialleonardo, Donato Coppola, Giacomo Capece, Eugenio Libutti, Massimiliano Nannerini, Giulio Maccauro, and Raffaele Vitiello. 2024. "Current Evidence Using Pulsed Electromagnetic Fields in Osteoarthritis: A Systematic Review" Journal of Clinical Medicine 13, no. 7: 1959. https://doi.org/10.3390/jcm13071959