
Prevalence of Self-Reported Anosmia and Ageusia in Elderly Patients Who Had Been Previously Hospitalized by SARS-CoV-2: The LONG-COVID-EXP Multicenter Study

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Procedure
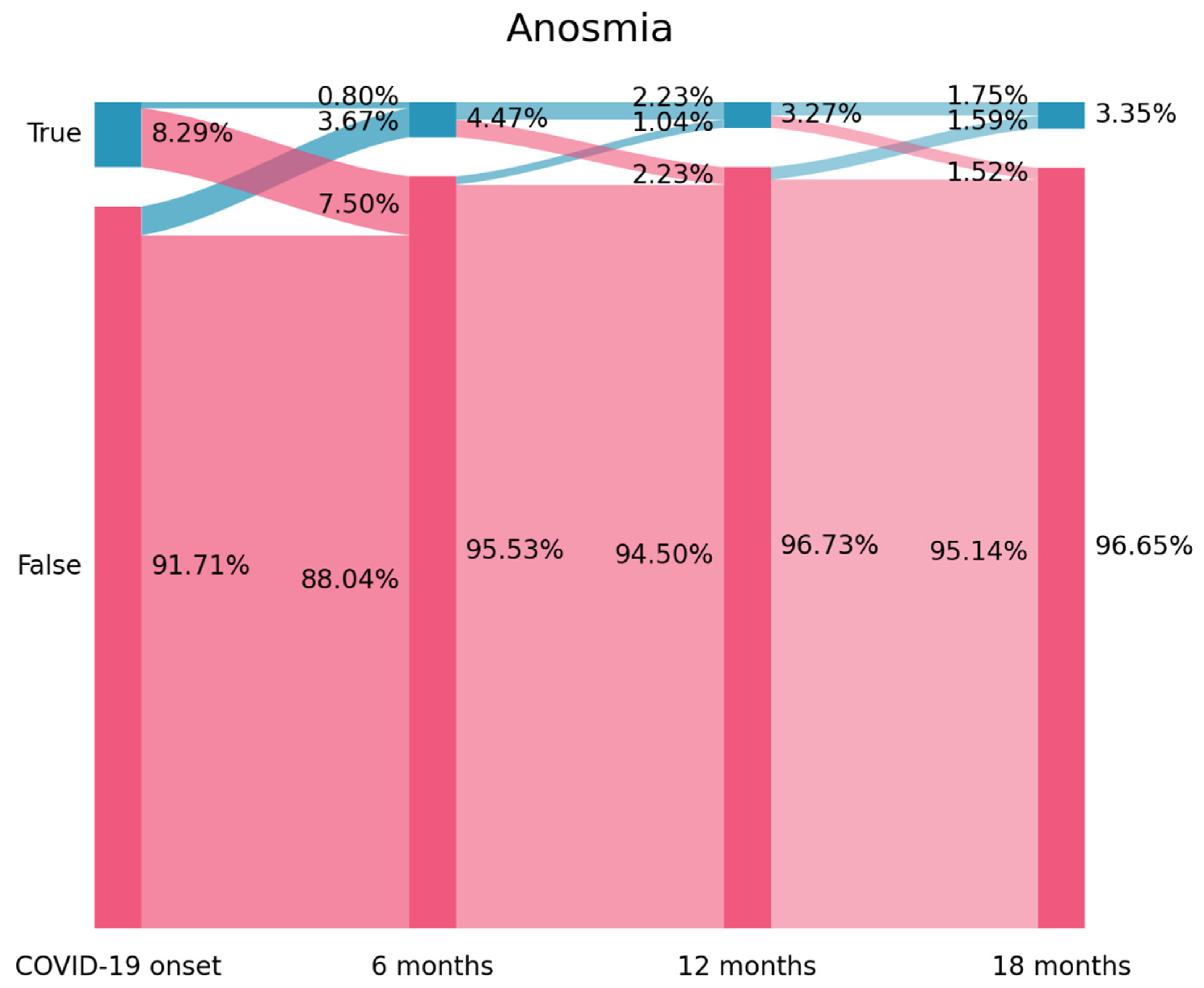
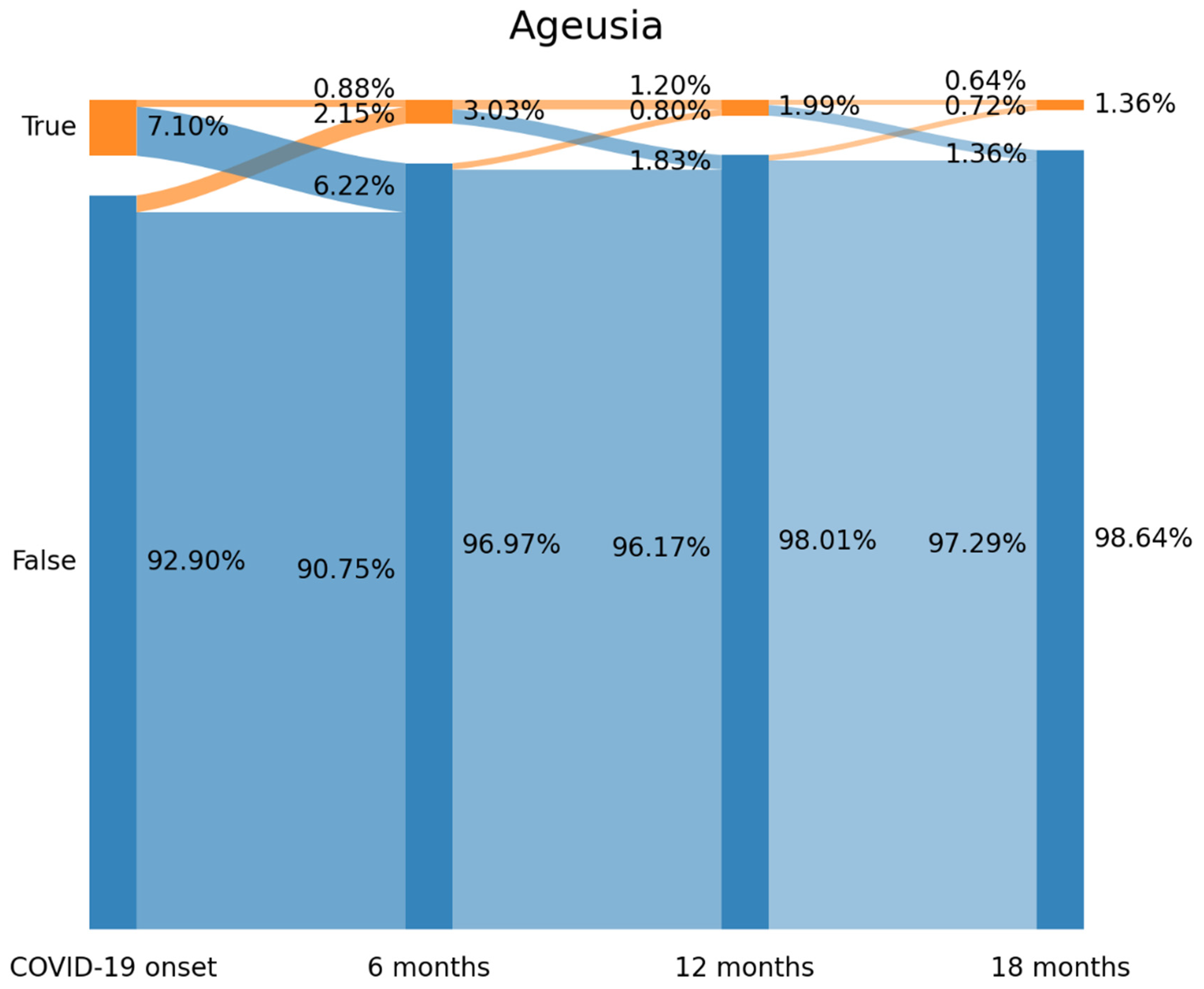
2.3. Sankey Plots
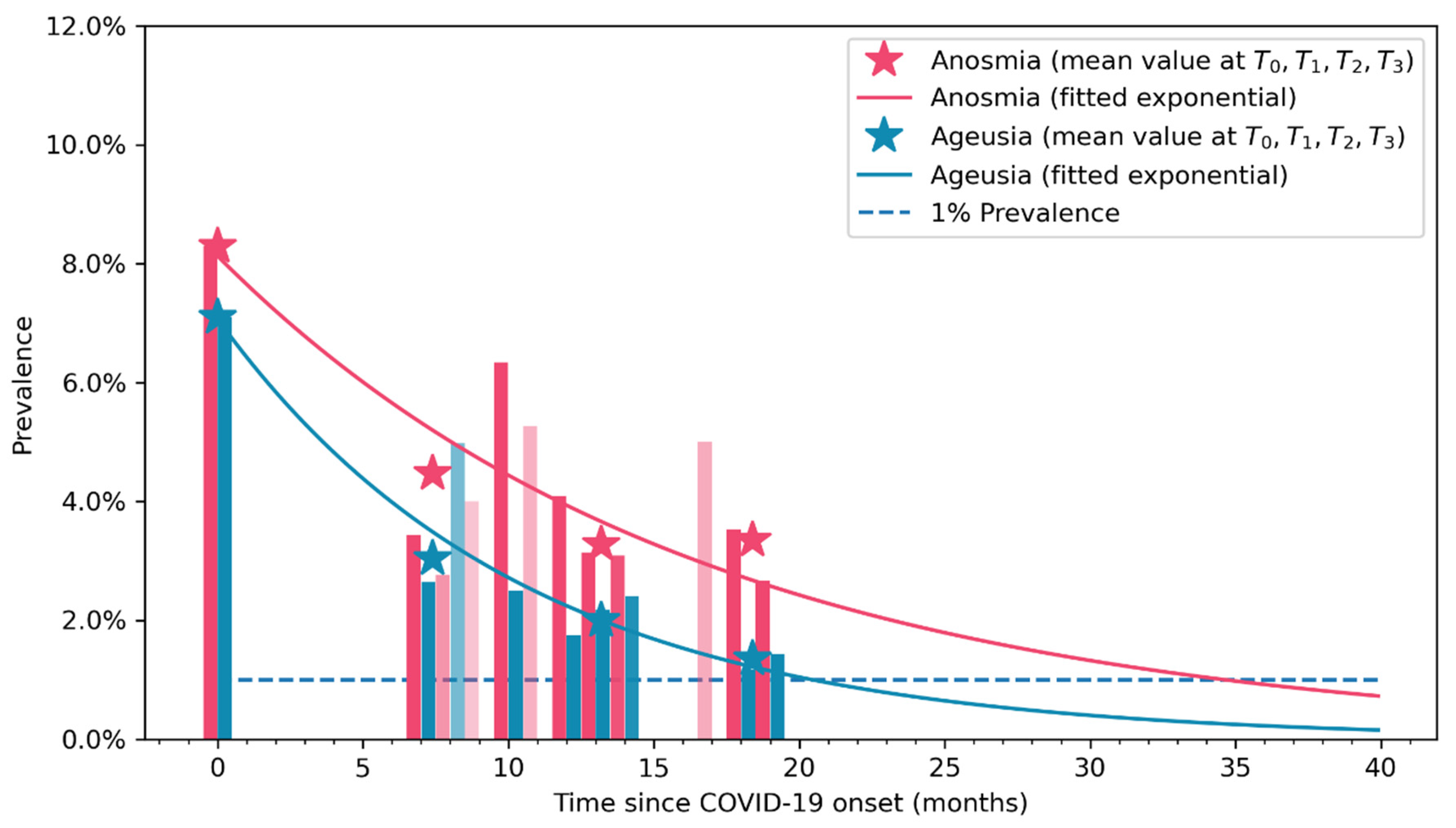
2.4. Exponential Bar Plots
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rabaan, A.A.; Smajlović, S.; Tombuloglu, H.; Ćordić, S.; Hajdarević, A.; Kudić, N.; Al Mutai, A.; Turkistani, S.A.; Al-Ahmed, S.H.; Al-Zaki, N.A.; et al. SARS-CoV-2 infection and multi-organ system damage: A review. Biomol. Biomed. 2023, 23, 37–52. [Google Scholar] [CrossRef] [PubMed]
- Borges do Nascimento, I.J.; O’Mathúna, D.P.; von Groote, T.C.; Abdulazeem, H.M.; Weerasekara, I.; Marusic, A.; Puljak, L.; Civile, V.T.; Zakarija-Grkovic, I.; Pericic, T.P.; et al. International Network of Coronavirus Disease 2019 (InterNetCOVID-19). Coronavirus disease (COVID-19) pandemic: An overview of systematic reviews. BMC Infect. Dis. 2021, 21, 52. [Google Scholar]
- Rocke, J.; Hopkins, C.; Philpott, C.M.; Kumar, N. Is loss of sense of smell a diagnostic marker in COVID-19: A systematic review and meta-analysis. Clin. Otolaryngol. 2020, 45, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.; Spijker, R.; Hooft, L.; Emperador, D.; Domen, J.; et al. Cochrane COVID-19 Diagnostic Test Accuracy Group. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19. Cochrane Database Syst. Rev. 2022, 5, CD013665. [Google Scholar]
- Aziz, M.; Goyal, H.; Haghbin, H.; Lee-Smith, W.M.; Gajendran, M.; Perisetti, A. The association of “loss of smell” to COVID-19: A systematic review and meta-analysis. Am. J. Med. Sci. 2021, 361, 216–225. [Google Scholar] [CrossRef]
- de Melo, E.G.M.; Andrade, R.M.; de Abreu de Vasconcellos, S.J.; Dos Santos, P.L.; Tanajura, D.; Quintans-Júnior, L.; Quintans, J.; Martins-Filho, P. Association between chemosensory dysfunctions and inflammatory biomarkers in patients with SARS-CoV-2 infection: A systematic review and meta-analysis. Inflammopharmacology 2022, 30, 2079–2087. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C. Long COVID: Current definition. Infection 2022, 50, 285–286. [Google Scholar] [CrossRef]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V.; WHO Clinical Case Definition Working Group on Post-COVID-19 Condition. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Hayes, L.D.; Ingram, J.; Sculthorpe, N.F. More than 100 persistent symptoms of SARS-CoV-2 (Long COVID): A scoping review. Front. Med. 2021, 8, 750378. [Google Scholar] [CrossRef]
- Hanson, S.W.; Abbafati, C.; Aerts, J.G.; Al-Aly, Z.; Ashbaugh, C.; Ballouz, T.; Blyuss, O.; Bobkova, P.; Bonsel, G.; et al.; Global Burden of Disease Long COVID Collaborators Estimated global proportions of individuals with persistent fatigue, cognitive, and respiratory symptom clusters following symptomatic COVID-19 in 2020 and 2021. JAMA 2022, 328, 1604–1615. [Google Scholar]
- Trott, M.; Driscoll, R.; Pardhan, S. The prevalence of sensory changes in post-COVID syndrome: A systematic review and meta-analysis. Front. Med. 2022, 9, 980253. [Google Scholar] [CrossRef] [PubMed]
- Premraj, L.; Kannapadi, N.V.; Briggs, J.; Seal, S.M.; Battaglini, D.; Fanning, J.; Suen, J.; Robba, C.; Fraser, J.; Cho, S.-M. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J. Neurol. Sci. 2022, 434, 120162. [Google Scholar] [CrossRef] [PubMed]
- Fernández-De-Las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.L.B.; Campbell, M.; Hopkins, C.; Smith, B.; Kelly, C.; Deary, V. Altered smell and taste: Anosmia, parosmia and the impact of long COVID-19. PLoS ONE 2021, 16, e0256998. [Google Scholar]
- Vaira, L.A.; Gessa, C.; Deiana, G.; Salzano, G.; Maglitto, F.; Lechien, J.R.; Saussez, S.; Piombino, P.; Biglio, A.; Biglioli, F.; et al. The effects of persistent olfactory and gustatory dysfunctions on quality of life in long-COVID-19 patients. Life 2022, 12, 141. [Google Scholar] [CrossRef]
- Lechien, J.R.; Journe, F.; Hans, S.; Chiesa-Estomba, C.M.; Mustin, V.; Beckers, E.; Vaira, L.A.; De Riu, G.; Hopkins, C.; Saussez, S. Severity of anosmia as an early symptom of COVID-19 infection may predict lasting loss of smell. Front. Med. 2020, 7, 582802. [Google Scholar] [CrossRef]
- Nguyen, N.N.; Hoang, V.T.; Dao, T.L.; Meddeb, L.; Cortaredona, S.; Lagier, J.-C.; Million, M.; Raoult, D.; Gautret, P. Long-term persistence of olfactory and gustatory disorders in COVID-19 patients. Front. Med. 2022, 9, 794550. [Google Scholar] [CrossRef]
- Tan, B.K.J.; Han, R.; Zhao, J.J.; Tan, N.K.W.; Quah, E.S.H.; Tan, C.J.-W.; Chan, Y.H.; Teo, N.W.Y.; Charn, T.C.; See, A.; et al. Prognosis and persistence of smell and taste dysfunction in patients with COVID-19: Meta-analysis with parametric cure modelling of recovery curves. BMJ 2022, 378, e069503. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Martín-Guerrero, J.D.; Navarro-Pardo, E.; Cancela-Cilleruelo, I.; Moro-López-Menchero, P.; Pellicer-Valero, O.J. Exploring trajectory curves from loss of smell and taste in previously hospitalized COVID-19 survivors: The LONG-COVID-EXP-CM Multicenter Study. J. Gen. Intern. Med. 2022, 37, 1821–1823. [Google Scholar] [CrossRef]
- Otto, E.; Culakova, E.; Meng, S.; Zhang, Z.; Xu, H.; Mohile, S.; Flannery, M.A. Overview of Sankey flow diagrams: Focusing on symptom trajectories in older adults with advanced cancer. J. Geriatr. Oncol. 2022, 13, 742–746. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Torres-Macho, J.; Guijarro, C.; Martín-Guerrero, J.D.; Pellicer-Valero, O.J.; Plaza-Manzano, G. Trajectory of gastrointestinal symptoms in previously hospitalized COVID-19 survivors: The Long COVID Experience Multicenter Study. Viruses 2023, 15, 1134. [Google Scholar] [CrossRef] [PubMed]
- Chung, T.W.-H.; Sridhar, S.; Zhang, A.J.; Chan, K.-H.; Li, H.-L.; Wong, F.K.-C.; Ng, M.-Y.; Tsang, R.K.-Y.; Lee, A.C.-Y.; Fan, Z.; et al. Olfactory dysfunction in coronavirus disease 2019 patients: Observational cohort study and systematic review. Open Forum Infect. Dis. 2020, 7, ofaa199. [Google Scholar] [CrossRef] [PubMed]
- Yuan, N.; Lv, Z.-H.; Sun, C.-R.; Wen, Y.-Y.; Tao, T.-Y.; Qian, D.; Tao, F.-P.; Yu, J.-H. Post-acute COVID-19 symptom risk in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Front. Public Health 2023, 11, 1112383. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C. Are patients exhibiting post-Coronavirus Disease (COVID) symptoms at 12 months the same at 5 or 9 months? The fluctuating nature of post-COVID. Clin. Infect. Dis. 2022, 75, e1208. [Google Scholar] [CrossRef] [PubMed]
- Fernández-De-Las-Peñas, C.; Florencio, L.L.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Palacios-Ceña, D.; Raveendran, A.V. Proposed integrative model for post-COVID symptoms. Diabetes Metab. Syndr. 2021, 15, 102159. [Google Scholar] [CrossRef]
- Ahmed, A.K.; Sayad, R.; Mahmoud, I.A.; El-Monem, A.M.A.; Badry, S.H.; Ibrahim, I.H. “Anosmia” the mysterious collateral damage of COVID-19. J. Neurovirol. 2022, 28, 189–200. [Google Scholar] [CrossRef]
- Doty, R.L. Olfactory dysfunction in COVID-19: Pathology and long-term implications for brain health. Trends Mol. Med. 2022, 28, 781–794. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Hans, S.; Saussez, S. Pathophysiological mechanisms and management of patients with long-time anosmia related to COVID-19. J. Intern. Med. 2021, 290, 464–465. [Google Scholar] [CrossRef]
- Locatello, L.G.; Oreste, G. Long-term recovery from COVID-19 anosmia: Promising findings and unanswered questions. J. Intern. Med. 2021, 290, 462–463. [Google Scholar] [CrossRef]
- Iqbal, F.M.; Lam, K.; Sounderajah, V.; Clarke, J.M.; Ashrafian, H.; Darzi, A. Characteristics and predictors of acute and chronic post-COVID syndrome: A systematic review and meta-analysis. EClinicalMedicine 2021, 36, 100899. [Google Scholar] [CrossRef]
- Tsampasian, V.; Elghazaly, H.; Chattopadhyay, R.; Debski, M.; Naing, T.K.P.; Garg, P.; Clark, A.; Ntatsaki, E.; Vassiliou, V.S. Risk factors associated with post-COVID-19 condition: A systematic review and meta-analysis. JAMA Intern. Med. 2023, 23, e230750. [Google Scholar] [CrossRef] [PubMed]
- Dirican, E.; Bal, T. COVID-19 disease severity to predict persistent symptoms: A systematic review and meta-analysis. Prim. Health Care Res. Dev. 2022, 23, e69. [Google Scholar] [CrossRef] [PubMed]
- O’Byrne, L.; Webster, K.E.; MacKeith, S.; Philpott, C.; Hopkins, C.; Burton, M.J. Interventions for the treatment of persistent post-COVID-19 olfactory dysfunction. Cochrane Database Syst. Rev. 2022, 9, CD013876. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age, mean (SD), years | 61 (16.5) |
| Female (%) | 578 (45.6%) |
| Weight, mean (SD), kg. | 74.5 (14.5) |
| Height, mean (SD), cm. | 165 (19.0) |
| COVID-19 symptoms at hospital admission, n (%)—T0 | |
| Fever | 948 (74.9%) |
| Dyspnea | 361 (28.5%) |
| Myalgia | 374 (29.5%) |
| Cough | 360 (28.4%) |
| Headache | 135 (16.7%) |
| Diarrhea | 105 (8.3%) |
| Anosmia | 105 (8.3%) |
| Ageusia | 66 (7.0%) |
| Throat Pain | 66 (5.2%) |
| Vomiting | 39 (3.0%) |
| Medical co-morbidities | |
| Hypertension | 336 (26.5%) |
| Other (Cancer, Kidney Disease) | 207 (16.3%) |
| Diabetes | 158 (12.5%) |
| Cardiovascular Disease | 141 (11.2%) |
| Asthma | 85 (6.7%) |
| Obesity | 57 (4.5%) |
| Chronic Obstructive Pulmonary Disease | 47 (3.7%) |
| Rheumatological Disease | 16 (1.3%) |
| Stay at the hospital, mean (SD), days | 10.5 (10.8) |
| Intensive Care Unit (ICU) admission | 78 (6.2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-de-las-Peñas, C.; Ortega-Santiago, R.; Cancela-Cilleruelo, I.; Rodríguez-Jiménez, J.; Fuensalida-Novo, S.; Martín-Guerrero, J.D.; Pellicer-Valero, Ó.J.; Cigarán-Méndez, M. Prevalence of Self-Reported Anosmia and Ageusia in Elderly Patients Who Had Been Previously Hospitalized by SARS-CoV-2: The LONG-COVID-EXP Multicenter Study. J. Clin. Med. 2023, 12, 4391. https://doi.org/10.3390/jcm12134391
Fernández-de-las-Peñas C, Ortega-Santiago R, Cancela-Cilleruelo I, Rodríguez-Jiménez J, Fuensalida-Novo S, Martín-Guerrero JD, Pellicer-Valero ÓJ, Cigarán-Méndez M. Prevalence of Self-Reported Anosmia and Ageusia in Elderly Patients Who Had Been Previously Hospitalized by SARS-CoV-2: The LONG-COVID-EXP Multicenter Study. Journal of Clinical Medicine. 2023; 12(13):4391. https://doi.org/10.3390/jcm12134391
Chicago/Turabian StyleFernández-de-las-Peñas, César, Ricardo Ortega-Santiago, Ignacio Cancela-Cilleruelo, Jorge Rodríguez-Jiménez, Stella Fuensalida-Novo, José D. Martín-Guerrero, Óscar J. Pellicer-Valero, and Margarita Cigarán-Méndez. 2023. "Prevalence of Self-Reported Anosmia and Ageusia in Elderly Patients Who Had Been Previously Hospitalized by SARS-CoV-2: The LONG-COVID-EXP Multicenter Study" Journal of Clinical Medicine 12, no. 13: 4391. https://doi.org/10.3390/jcm12134391