
The Clinical Characteristics and Prognostic Factors of Primary Extramammary Paget’s Disease Treated with Surgery in Anogenital Regions: A Large Population Study from the SEER Database and Our Centre

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
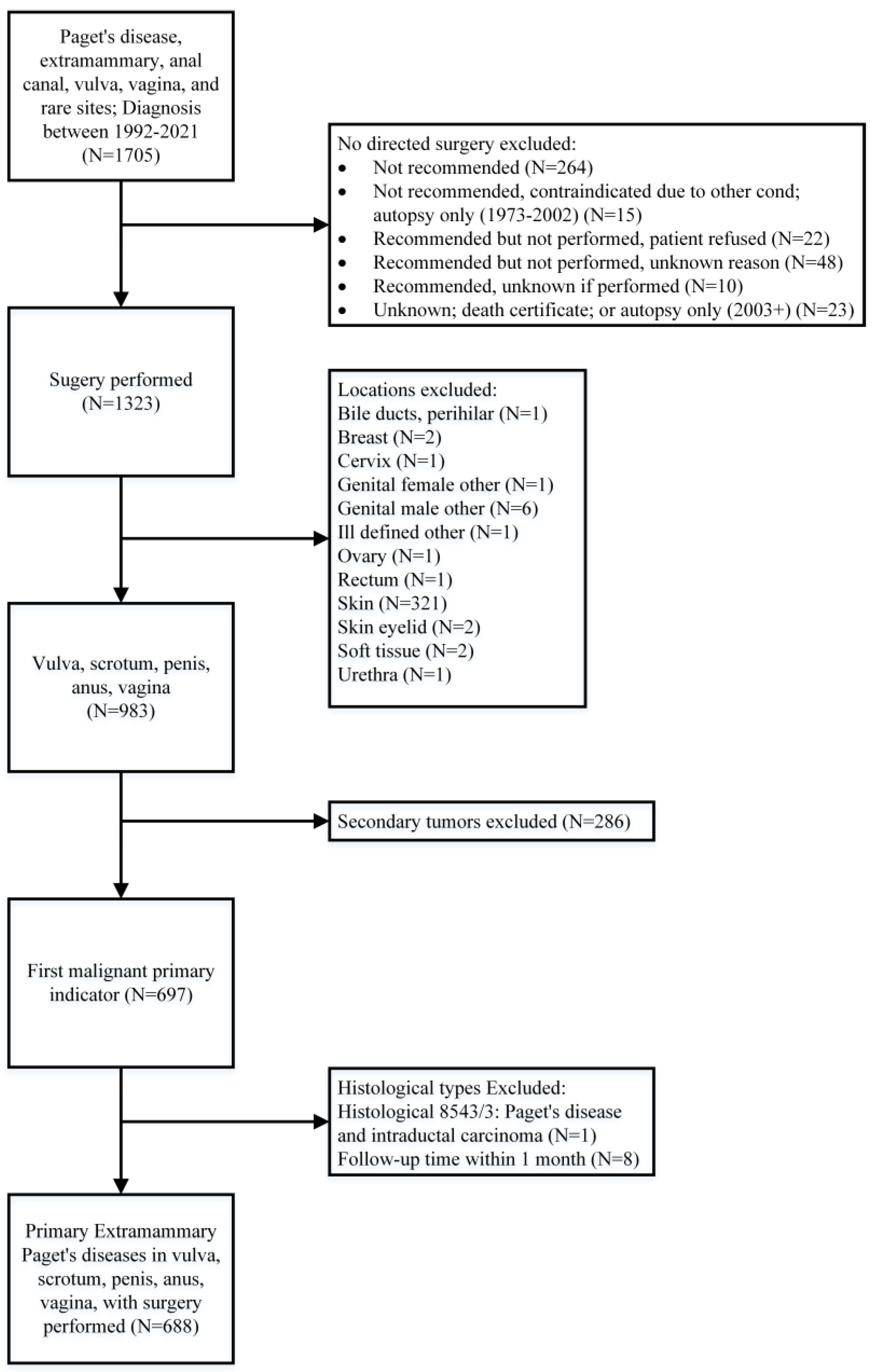
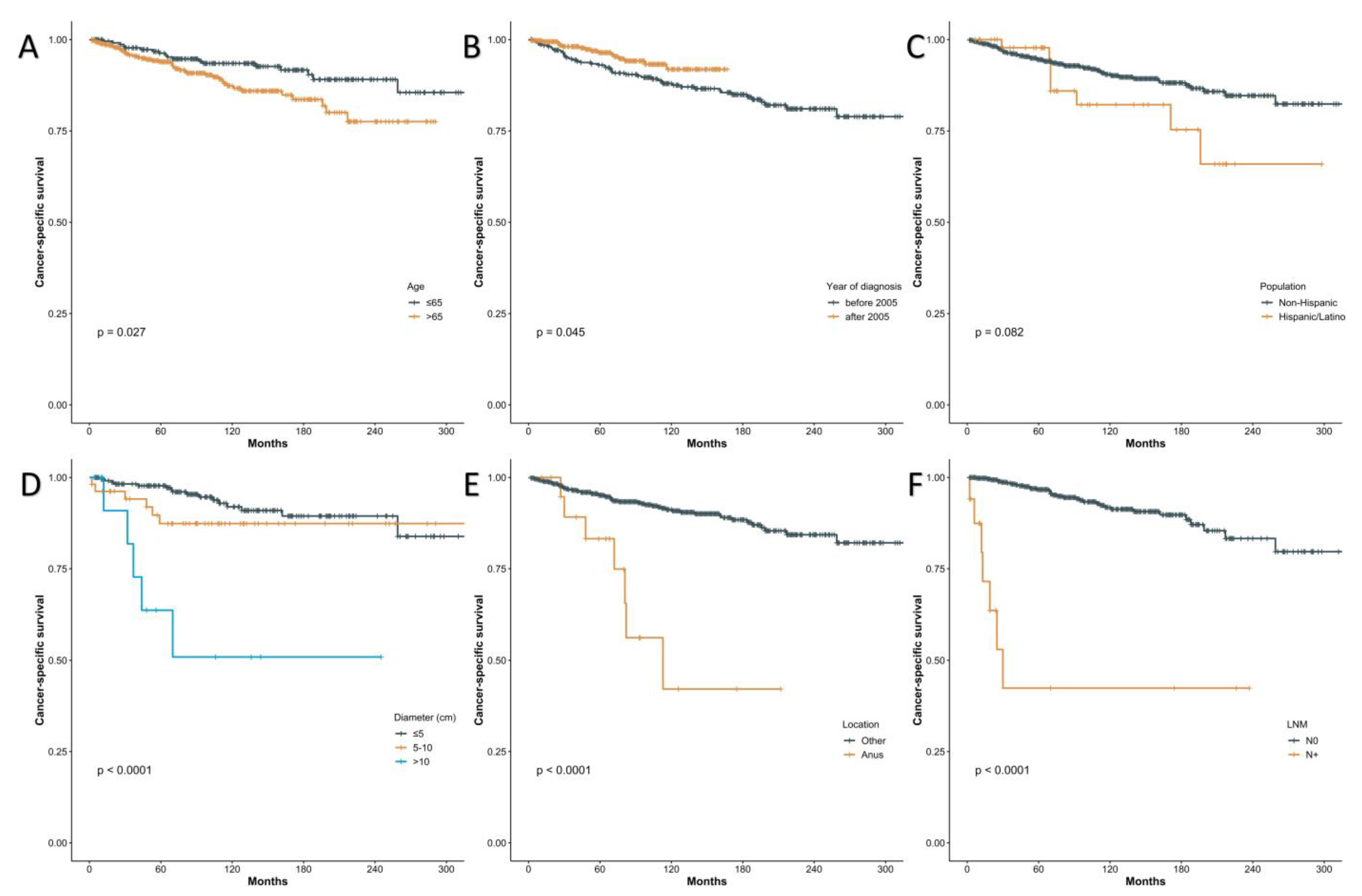
3.1. Data from the SEER Program
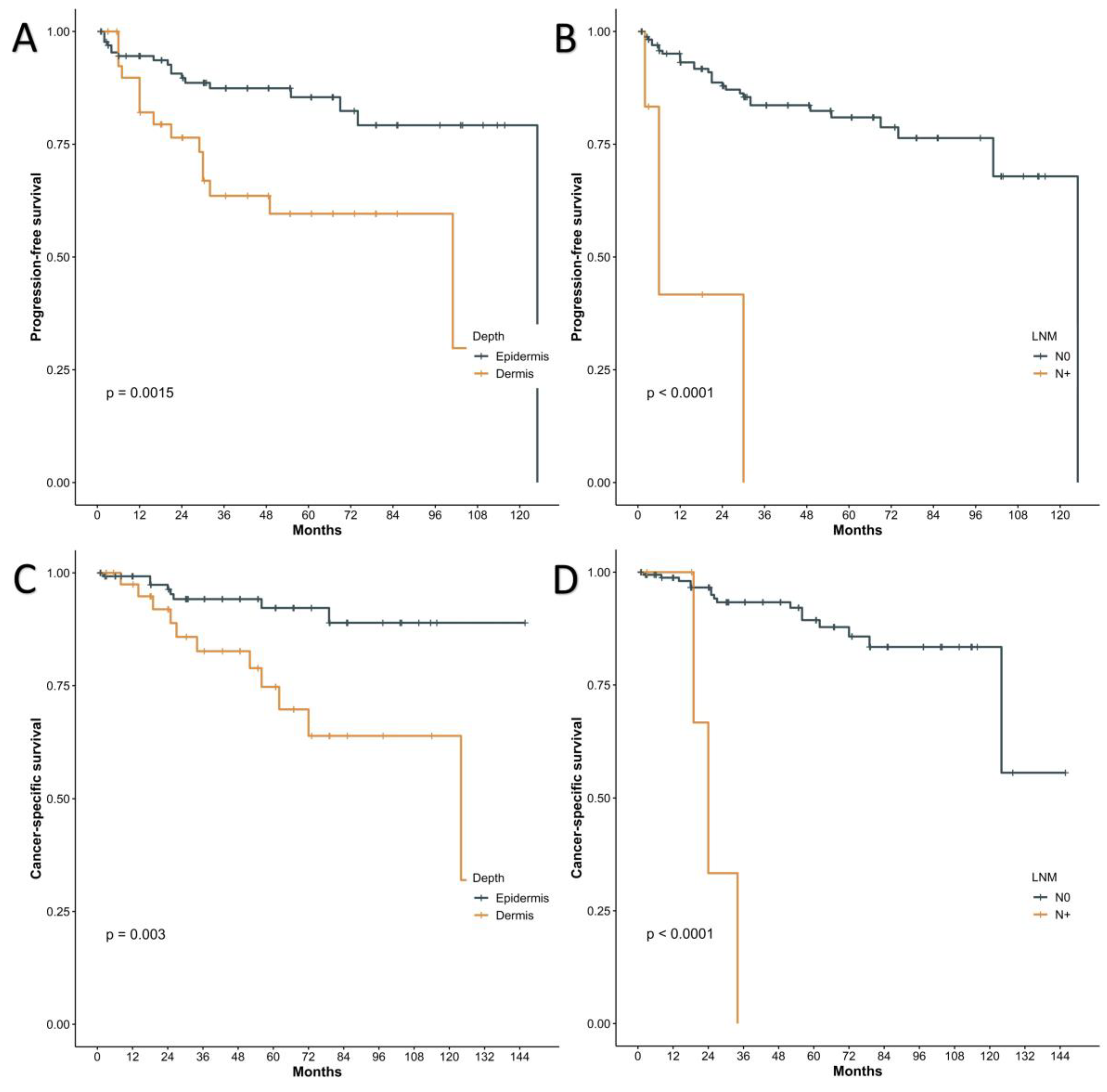
3.2. Participants from Our Centre
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kanitakis, J. Mammary and extramammary Paget’s disease. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-C.; Li, A.F.-Y.; Yang, S.-H.; Ma, H.-H.; Liang, W.-Y. Perianal Paget’s Disease: The 17-Year-Experience of a Single Institution in Taiwan. Gastroenterol. Res. Pract. 2019, 2019, 2603279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weng, S.; Zhu, N.; Li, D.; Chen, Y.; Tan, Y.; Chen, J.; Yuan, Y. Clinical Characteristics, Treatment, and Prognostic Factors of Patients With Primary Extramammary Paget’s Disease (EMPD): A Retrospective Analysis of 44 Patients From a Single Center and an Analysis of Data From the Surveillance, Epidemiology, and End Results (SEER) Database. Front. Oncol. 2020, 10, 1114. [Google Scholar] [CrossRef]
- Merritt, B.G.; Degesys, C.A.; Brodland, D.G. Extramammary Paget Disease. Dermatol. Clin. 2019, 37, 261–267. [Google Scholar] [CrossRef]
- Kim, S.J.; Thompson, A.K.; Zubair, A.S.; Otley, C.C.; Arpey, C.J.; Baum, C.L.; Roenigk, R.K.; Lohse, C.M.; Brewer, J.D. Surgical Treatment and Outcomes of Patients With Extramammary Paget Disease: A Cohort Study. Dermatol. Surg. 2017, 43, 708–714. [Google Scholar] [CrossRef]
- Liao, X.; Liu, X.; Fan, X.; Lai, J.; Zhang, D. Perianal Paget’s disease: A clinicopathological and immunohistochemical study of 13 cases. Diagn. Pathol. 2020, 15, 29. [Google Scholar] [CrossRef] [Green Version]
- Molina, G.E.; Khalifian, S.; Mull, J.L.; Chen, L.; Rosman, I.S.; Faulkner-Jones, B.E.; Ngo, K.H.; Demehri, S.; Cornelius, L.A.; Wu, P.A. Topical Combination of Fluorouracil and Calcipotriene as a Palliative Therapy for Refractory Extramammary Paget Disease. JAMA Dermatol. 2019, 155, 599–603. [Google Scholar] [CrossRef]
- Ichiyama, T.; Gomi, D.; Fukushima, T.; Kobayashi, T.; Sekiguchi, N.; Sakamoto, A.; Sasaki, S.; Mamiya, K.; Koizumi, T.; Hama, Y. Successful and long-term response to trastuzumab plus paclitaxel combination therapy in human epidermal growth factor receptor 2-positive extramammary Paget’s disease: A case report and review of the literature. Mol. Clin. Oncol. 2017, 7, 763–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Wang, P.; Li, C.; Zhou, Z.; Zhang, L.; Zhang, G.; Wang, X. Efficacy and safety of HpD-PDT for Extramammary Paget’s Disease refractory to conventional therapy: A prospective, open-label and single arm pilot study. Photodiagn. Photodyn. Ther. 2022, 37, 102670. [Google Scholar] [CrossRef]
- Pittman, M.E.; Milsom, J.; Yantiss, R.K. Treatment Effects Can Mimic Recurrent Extramammary Paget Disease in Perianal Skin. Am. J. Surg. Pathol. 2018, 42, 1472–1479. [Google Scholar] [CrossRef]
- Hatta, N. Prognostic Factors of Extramammary Paget’s Disease. Curr. Treat. Options Oncol. 2018, 19, 47. [Google Scholar] [CrossRef] [PubMed]
- Nagai, Y.; Kazama, S.; Yamada, D.; Miyagawa, T.; Murono, K.; Yasuda, K.; Nishikawa, T.; Tanaka, T.; Kiyomatsu, T.; Hata, K.; et al. Perianal and Vulvar Extramammary Paget Disease: A Report of Six Cases and Mapping Biopsy of the Anal Canal. Ann. Dermatol. 2016, 28, 624–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karam, A.; Dorigo, O. Treatment outcomes in a large cohort of patients with invasive Extramammary Paget’s disease. Gynecol. Oncol. 2012, 125, 346–351. [Google Scholar] [CrossRef]
- Akaike, H. A New Look at the Statistical Model Identification. In Selected Papers of Hirotugu Akaike; Parzen, E., Tanabe, K., Kitagawa, G., Eds.; Springer: New York, NY, USA, 1998; pp. 215–222. [Google Scholar]
- Ito, T.; Kaku-Ito, Y.; Furue, M. The diagnosis and management of extramammary Paget’s disease. Expert Rev. Anticancer Ther. 2018, 18, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Hata, M.; Koike, I.; Wada, H.; Miyagi, E.; Kasuya, T.; Kaizu, H.; Mukai, Y.; Inoue, T. Postoperative radiation therapy for extramammary Paget’s disease. Br. J. Dermatol. 2015, 172, 1014–1020. [Google Scholar] [CrossRef]
- Herrel, L.A.; Weiss, A.D.; Goodman, M.; Johnson, T.V.; Osunkoya, A.O.; Delman, K.A.; Master, V.A. Extramammary Paget’s disease in males: Survival outcomes in 495 patients. Ann. Surg. Oncol. 2015, 22, 1625–1630. [Google Scholar] [CrossRef]
- Hatta, N.; Yamada, M.; Hirano, T.; Fujimoto, A.; Morita, R. Extramammary Paget’s disease: Treatment, prognostic factors and outcome in 76 patients. Br. J. Dermatol. 2008, 158, 313–318. [Google Scholar] [CrossRef]
- Dai, B.; Kong, Y.-Y.; Chang, K.; Qu, Y.-Y.; Ye, D.-W.; Zhang, S.-L.; Zhang, H.-L. Primary invasive carcinoma associated with penoscrotal extramammary Paget’s disease: A clinicopathological analysis of 56 cases. BJU Int. 2015, 115, 153–160. [Google Scholar] [CrossRef]
- Yao, H.; Xie, M.; Fu, S.; Guo, J.; Peng, Y.; Cai, Z.; Jiang, Y.; Zheng, D.; Wang, Z. Survival analysis of patients with invasive extramammary Paget disease: Implications of anatomic sites. BMC Cancer 2018, 18, 403. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Kaku, Y.; Nagae, K.; Nakano-Nakamura, M.; Nakahara, T.; Oda, Y.; Hagihara, A.; Furue, M.; Uchi, H. Tumor thickness as a prognostic factor in extramammary Paget’s disease. J. Dermatol. 2015, 42, 269–275. [Google Scholar] [CrossRef]
- Mengjun, B.; Zheng-Qiang, W.; Tasleem, M.M. Extramammary Paget’s disease of the perianal region: A review of the literature emphasizing management. Dermatol. Surg. 2013, 39, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Trofymenko, O.; Garcia, V.; Zeitouni, N.C. Primary extramammary Paget’s disease of the skin: Treatment and survival. Int. J. Dermatol. 2018, 57, e76–e78. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.M.; Choi, Y.Y.; Kim, H.; Oh, B.H.; Roh, M.R.; Nam, K.; Chung, K.Y. Mohs micrographic surgery for extramammary Paget disease: A pooled analysis of individual patient data. J. Am. Acad. Dermatol. 2013, 68, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Nishio, S.; Matsuzaki, S.; Iwase, H.; Kagami, S.; Soeda, S.; Usui, H.; Nishikawa, R.; Mikami, M.; Enomoto, T. Surgical margin status and recurrence pattern in invasive vulvar Paget’s disease: A Japanese Gynecologic Oncology Group study. Gynecol. Oncol. 2021, 160, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Parashurama, R.; Nama, V.; Hutson, R. Paget’s Disease of the Vulva: A Review of 20 Years’ Experience. Int. J. Gynecol. Cancer 2017, 27, 791–793. [Google Scholar] [CrossRef]
- Morris, C.R.; Hurst, E.A. Extramammary Paget’s Disease: A Review of the Literature Part II: Treatment and Prognosis. Dermatol. Surg 2020, 46, 305–311. [Google Scholar] [CrossRef]
- Shu, B.; Shen, X.-X.; Chen, P.; Fang, X.-Z.; Guo, Y.-L.; Kong, Y.-Y. Primary invasive extramammary Paget disease on penoscrotum: A clinicopathological analysis of 41 cases. Hum. Pathol. 2016, 47, 70–77. [Google Scholar] [CrossRef]
- Shen, K.; Luo, H.; Hu, J.; Xie, Z. Perianal Paget disease treated with wide excision and thigh skin flap reconstruction: A case report and review of literature. Medicine 2018, 97, e11638. [Google Scholar] [CrossRef]
- Gentileschi, S.; Servillo, M.; Garganese, G.; Fragomeni, S.; De Bonis, F.; Scambia, G.; Salgarello, M. Surgical therapy of vulvar cancer: How to choose the correct reconstruction? J. Gynecol. Oncol. 2016, 27, e60. [Google Scholar] [CrossRef] [Green Version]
- Ohara, K.; Fujisawa, Y.; Yoshino, K.; Kiyohara, Y.; Kadono, T.; Murata, Y.; Uhara, H.; Hatta, N.; Uchi, H.; Matsushita, S.; et al. A proposal for a TNM staging system for extramammary Paget disease: Retrospective analysis of 301 patients with invasive primary tumors. J. Dermatol. Sci. 2016, 83, 234–239. [Google Scholar] [CrossRef]
- Kyriazanos, I.D.; Stamos, N.P.; Miliadis, L.; Noussis, G.; Stoidis, C.N. Extra-mammary Paget’s disease of the perianal region: A review of the literature emphasizing the operative management technique. Surg. Oncol. 2011, 20, e61–e71. [Google Scholar] [CrossRef]
- Ogata, D.; Kiyohara, Y.; Yoshikawa, S.; Tsuchida, T. Usefulness of sentinel lymph node biopsy for prognostic prediction in extramammary Paget’s disease. Eur. J. Dermatol. 2016, 26, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, Y.; Yoshino, K.; Kiyohara, Y.; Kadono, T.; Murata, Y.; Uhara, H.; Hatta, N.; Uchi, H.; Matsushita, S.; Takenouchi, T.; et al. The role of sentinel lymph node biopsy in the management of invasive extramammary Paget’s disease: Multi-center, retrospective study of 151 patients. J. Dermatol. Sci. 2015, 79, 38–42. [Google Scholar] [CrossRef] [PubMed]
- van der Putte, S.C. Clear cells of Toker in the developing anogenital region of male and female fetuses. Am. J. Dermatopathol. 2011, 33, 811–818. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Univariate | Multivariate (BSR) | ||
|---|---|---|---|---|
| Hazard Ratio | p Value | Hazard Ratio | p Value | |
| Age > 65 years | 1.85 [1.06–3.22] | 0.030 | 8.51 (1.67–43.42) | 0.010 |
| Male | 1.29 [0.75–2.21] | 0.359 | ||
| Year > 2005 | 0.55 [0.3–0.99] | 0.048 | 0.30 (0.07–1.22) | 0.093 |
| Races | ||||
| White | 1.00 | |||
| American Indian/Alaska Native | 2.61 [0.36–18.96] | 0.343 | ||
| Asian or Pacific Islander | 0.67 [0.37–1.22] | 0.194 | ||
| Black | 0.00 [0-Inf] | 0.997 | ||
| Unknown | 0.00 [0-Inf] | 0.998 | ||
| SEER stage | ||||
| Localized | 1.00 | |||
| Regional | 2.57 [1.47–4.49] | 0.001 | 0.24 (0.04–1.61) | 0.142 |
| Distant | 16.47 [6.4–42.4] | <0.001 | 2.93 (0.13–65.53) | 0.498 |
| N+ | 12.40 [5.42–28.37] | <0.001 | 214.24 (8.36–5493.13) | 0.001 |
| Spanish-Hispanic-Latino | 1.91 [0.91–4.02] | 0.087 | 13.44 (2.47–73.19) | 0.003 |
| Diameter (cm) | ||||
| <5 | ||||
| 5–10 | 1.76 [0.69–4.49] | 0.239 | 2.33 (0.52–10.38) | 0.268 |
| >10 | 8.78 [3.18–24.23] | <0.001 | 14.35 (2.57–80.15) | 0.002 |
| Site | ||||
| Vulva | 1.00 | 1.00 | ||
| Penis | 0.60 [0.08–4.36] | 0.614 | 0 (0-Inf) | 0.998 |
| Scrotum | 1.00 [0.53–1.9] | 0.998 | 2.61 (0.44–15.63) | 0.293 |
| Vagina | 0.00 [0-Inf] | 0.995 | NA (NA-NA) | NA |
| Anus | 5.50 [2.45–12.34] | <0.001 | 115.38 (6.77–1966.79) | 0.001 |
| Variables | Univariate | Multivariate (BSR) | ||
|---|---|---|---|---|
| Hazard Ratio | p Value | Hazard Ratio | p Value | |
| Age > 65 years | 1.15 [0.57–2.32] | 0.695 | ||
| BMI > 25 | 1.28 [0.64–2.57] | 0.488 | ||
| Female | 1.99 [0.82–4.83] | 0.13 | ||
| ASA > 2 | 0.67 [0.2–2.2] | 0.505 | ||
| Comorbidity | 1.22 [0.6–2.47] | 0.582 | ||
| SEER stage | ||||
| Localized | ||||
| Regional | 2.39 [1.16–4.94] | 0.018 | ||
| Distant | 4.33 [0.57–32.76] | 0.156 | ||
| Diameter (cm) | ||||
| <5 | 1.00 | |||
| 5–10 | 0.79 [0.37–1.68] | 0.542 | ||
| >10 | 0.87 [0.25–3.01] | 0.831 | ||
| Margin+ | 1.9 [0.87–4.16] | 0.107 | ||
| Lymphadenectomy | 2.6 [0.79–8.61] | 0.117 | ||
| N+ | 11.66 [3.92–34.67] | <0.001 | 6.31 [1.91–20.88] | 0.003 |
| Invasion level | ||||
| Level 1 | 1.00 | |||
| Level 2 | 2.53 [0.85–7.54] | 0.095 | ||
| Level 3 | 3.12 [1.46–6.67] | 0.003 | ||
| Invasion level (extend through epidermis) | 2.94 [1.47–5.89] | 0.002 | 2.29 (1.06–4.98) | 0.035 |
| LVI | 7.67 [2.3–25.58] | 0.001 | 3.11 [0.82–11.86] | 0.096 |
| Chemotherapy | 3.75 [0.89–15.8] | 0.072 | ||
| Radiation | 1.1 [0.54–2.23] | 0.795 | ||
| Sites | ||||
| Vulva | 1.00 | |||
| Penis | 0.34 [0.07–1.71] | 0.193 | ||
| Scrotum (and pubis) | 0.52 [0.21–1.28] | 0.157 | ||
| Reconstruction | ||||
| Direct closure | 1.00 | 1.000 | ||
| Free skin flaps | 3.58 [1.29–9.92] | 0.014 | ||
| Skin grafting | 2.29 [0.95–5.53] | 0.066 | ||
| MMS | 0.43 [0.21–0.87] | 0.019 | ||
| Intervals > 2 years | 2.33 [0.96–5.67] | 0.062 | 1.00 [1.00–1.01] | 0.064 |
| Variables | Univariate | Multivariate (BSR) | ||
|---|---|---|---|---|
| Hazard Ratio | p Value | Hazard Ratio | p Value | |
| Age > 65 years | 1.42 [0.55–3.67] | 0.469 | ||
| BMI > 25 | 0.97 [0.39–2.42] | 0.945 | ||
| Female | 0.88 [0.2–3.9] | 0.87 | ||
| ASA > 2 | 1.24 [0.36–4.3] | 0.731 | ||
| Comorbidity | 0.99 [0.39–2.5] | 0.979 | ||
| SEER stage | ||||
| Localized | ||||
| Regional | 2.1 [0.82–5.35] | 0.12 | ||
| Distant | 0 [0-Inf] | 0.998 | ||
| Diameter (cm) | ||||
| <5 | ||||
| 5–10 | 0.46 [0.16–1.31] | 0.147 | ||
| >10 | 0.68 [0.15–3.06] | 0.612 | ||
| Margin+ | 2.61 [1.02–6.65] | 0.045 | ||
| N+ | 16.73 [4.32–64.79] | <0.001 | 10.33 (2.57–41.48) | <0.001 |
| Invasion level | ||||
| Level 1 | 1.00 | |||
| Level 2 | 4.17 [1.1–15.73] | 0.035 | ||
| Level 3 | 3.52 [1.29–9.55] | 0.014 | ||
| Invasion level (extend through epidermis) | 3.68 [1.47–9.25] | 0.006 | 2.96 (1.14–7.7) | 0.026 |
| LVI | 9.53 [2.11–43.09] | 0.003 | ||
| Chemotherapy | 3.23 [0.42–24.54] | 0.258 | ||
| Radiation | 0.64 [0.23–1.8] | 0.397 | ||
| Sites | ||||
| Vulva | 1.00 | |||
| Penis | 1.34 [0.18–9.76] | 0.774 | ||
| Scrotum | 1.11 [0.25–4.95] | 0.89 | ||
| Reconstruction | ||||
| Direct closure | 1.00 | 1.000 | ||
| Free skin flaps | 5.49 [1.6–18.86] | 0.007 | ||
| Skin grafting | 1.87 [0.56–6.26] | 0.307 | ||
| MMS | 0.48 [0.19–1.22] | 0.122 | ||
| Intervals > 2 years | 1.8 [0.6–5.42] | 0.299 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Liu, Z.; Pan, S.; Liu, J.; Zuo, S.; Wang, P. The Clinical Characteristics and Prognostic Factors of Primary Extramammary Paget’s Disease Treated with Surgery in Anogenital Regions: A Large Population Study from the SEER Database and Our Centre. J. Clin. Med. 2023, 12, 582. https://doi.org/10.3390/jcm12020582
Chen Z, Liu Z, Pan S, Liu J, Zuo S, Wang P. The Clinical Characteristics and Prognostic Factors of Primary Extramammary Paget’s Disease Treated with Surgery in Anogenital Regions: A Large Population Study from the SEER Database and Our Centre. Journal of Clinical Medicine. 2023; 12(2):582. https://doi.org/10.3390/jcm12020582
Chicago/Turabian StyleChen, Zeyang, Zining Liu, Shaorong Pan, Jin Liu, Shuai Zuo, and Pengyuan Wang. 2023. "The Clinical Characteristics and Prognostic Factors of Primary Extramammary Paget’s Disease Treated with Surgery in Anogenital Regions: A Large Population Study from the SEER Database and Our Centre" Journal of Clinical Medicine 12, no. 2: 582. https://doi.org/10.3390/jcm12020582