

Dual Antiplatelet Therapy and Cancer; Balancing between Ischemic and Bleeding Risk: A Narrative Review

 , ,
, ,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
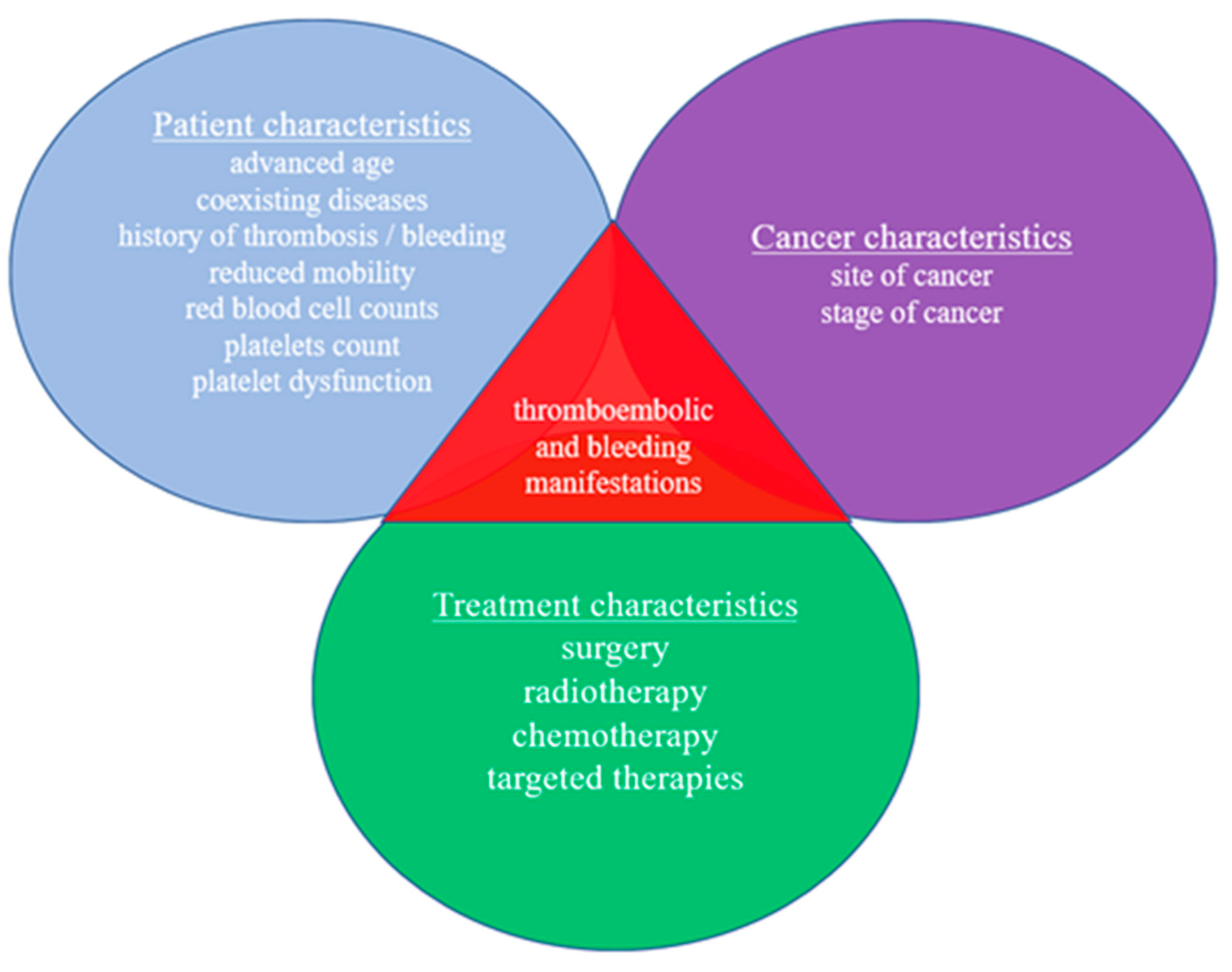
3. Biological and Clinical Aspects of Coagulation in Patients with Cancer
4. Cardiotoxicity Caused by Anticancer Treatment

{kind=link}
{kind=link}
{kind=link}
| Treatment | Incidence | Mechanism |
|---|---|---|
| Radiation [22] | Depends on the prescribed dose and the cardiac radiation exposure | Endothelial injury, acceleration of CAD, ACS |
| 5-Fluorouracil [23,24] | 2–18% | ACS, vasospasm |
| Cisplatin [25,26] | 0.2–12% | ACS, acute thrombosis, acceleration of CAD |
| Bevacizumab [28,36] | 0.52–1.7% | ACS, acute thrombosis |
| Leuprolide (GNRH agonist) [37] | 2.6–5.6% | Angina, ACS, acceleration of CAD |
| Anastrozole (aromatase inhibitor) [29] | 2% | ACS |
| Tyrosine kinase inhibitors: | ||
| Sorafenib [31] | 1% | Acute thrombosis |
| Sunitinib [31] | 5–8% | Acute thrombosis, acceleration of CAD |
| Nilotinib [20,32] | 8–12% | ACS, acceleration of CAD, AF |
| Ponatinib [32] | 2% | ACS, acceleration of CAD |
| Ibrutinib [35] | 8.8% | Bleeding diathesis, AF |
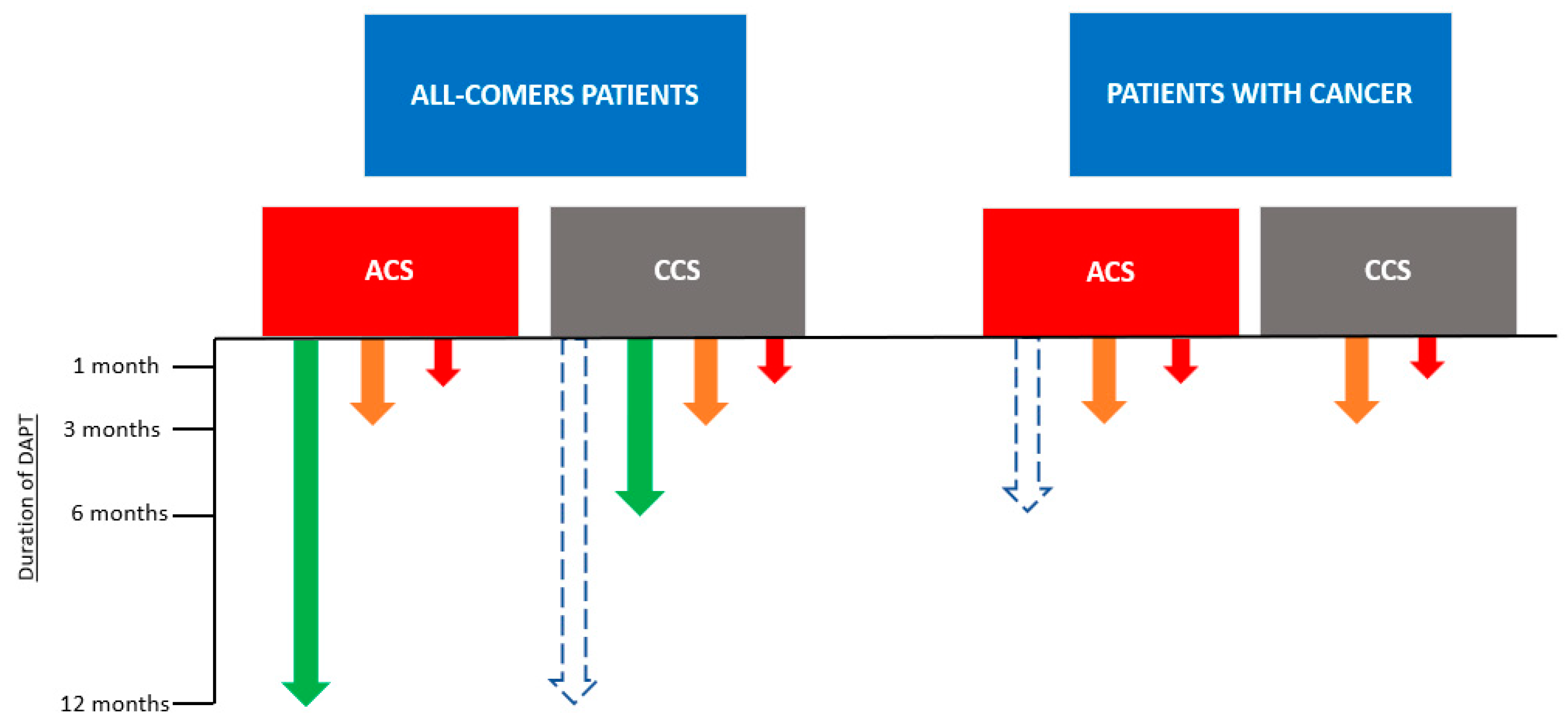
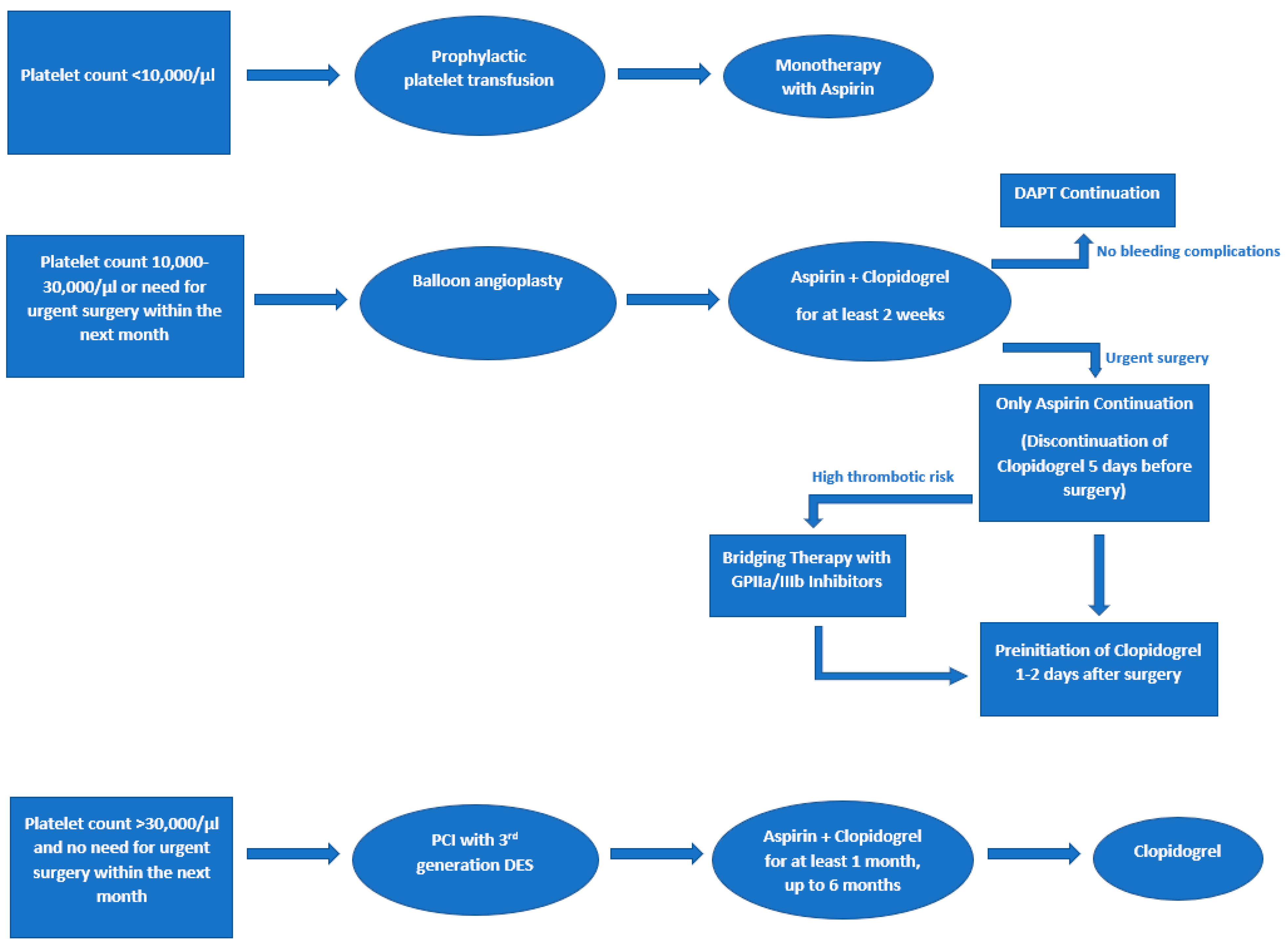
5. DAPT in Patients with Cancer Undergoing Elective PCI
6. DAPT in Patients with ACS and Cancer
7. Antiplatelet Therapy in Patients with Cancer Undergoing CABG
8. Antithrombotic Therapy in Patients with AF and Cancer Undergoing PCI or Suffering from ACS
9. Antiplatelet Therapy in Patients with Cancer Undergoing Cardiac Structural Interventions
9.1. TAVR
9.2. PFO-ASD Closure
9.3. LAA Occlusion
10. Antiplatelet Therapy for Non-Cardiac Diseases in Patients with Cancer
10.1. PAD
10.2. CVAs
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marenzi, G.; Cosentino, N.; Cardinale, D. Ischaemic and bleeding risk in cancer patients undergoing PCI: Another brick in the wall. Eur. Heart J. 2021, 42, 1035–1037. [Google Scholar] [CrossRef] [PubMed]
- Koene, R.J.; Prizment, A.E.; Blaes, A.; Konety, S.H. Shared Risk Factors in Cardiovascular Disease and Cancer. Circulation 2016, 133, 1104–1114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anker, M.S.; Hadzibegovic, S.; Lena, A.; Belenkov, Y.; Bergler-Klein, J.; de Boer, R.A.; Farmakis, D.; von Haehling, S.; Iakobishvili, Z.; Maack, C.; et al. Recent advances in cardio-oncology: A report from the “Heart Failure Association 2019 and World Congress on Acute Heart Failure 2019”. ESC Heart Fail. 2019, 6, 1140–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Boer, R.A.; Meijers, W.C.; van der Meer, P.; van Veldhuisen, D.J. Cancer and heart disease: Associations and relations. Eur. J. Heart Fail. 2019, 21, 1515–1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, S.; Singh, K. Atherosclerosis, Ischemia, and Anticancer Drugs. Heart Views 2021, 22, 127. [Google Scholar]
- Falanga, A.; Marchetti, M.; Vignoli, A. Coagulation and cancer: Biological and clinical aspects. J. Thromb. Haemost. 2013, 11, 223–233. [Google Scholar] [CrossRef]
- Radmilovic, J.; Di Vilio, A.; D’andrea, A.; Pastore, F.; Forni, A.; Desiderio, A.; Ragni, M.; Quaranta, G.; Cimmino, G.; Russo, V.; et al. The Pharmacological Approach to Oncologic Patients with Acute Coronary Syndrome. J. Clin. Med. 2020, 9, 3926. [Google Scholar] [CrossRef]
- Falanga, A.; Russo, L.; Milesi, V. The coagulopathy of cancer. Curr. Opin. Hematol. 2014, 21, 423–429. [Google Scholar] [CrossRef]
- Rohrmann, S.; Witassek, F.; Erne, P.; Rickli, H.; Radovanovic, D. Treatment of patients with myocardial infarction depends on history of cancer. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 639–645. [Google Scholar] [CrossRef]
- Lee, L.H.; Nagarajan, C.; Tan, C.W.; Ng, H.J. Epidemiology of Cancer-Associated Thrombosis in Asia: A Systematic Review. Front. Cardiovasc. Med. 2021, 8, 435. [Google Scholar] [CrossRef]
- Johnstone, C.; Rich, S.E. Bleeding in cancer patients and its treatment: A review. Ann. Palliat. Med. 2018, 7, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Fan, X.; Lewis, B.R.; Johnson, M.P.; Rihal, C.S.; Lerman, A.; Herrmann, J. Cancer Patients Have a Higher Risk of Thrombotic and Ischemic Events After Percutaneous Coronary Intervention. JACC. Cardiovasc. Interv. 2021, 14, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Kamphuisen, P.W.; Beyer-Westendorf, J. Bleeding complications during anticoagulant treatment in patients with cancer. Thromb. Res. 2014, 133 (Suppl. S2), S49–S55. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.P.; Hisada, Y.M.; Kasthuri, R.S.; Reeves, B.N.; MacKman, N. Cancer Therapy-Associated Thrombosis. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 1291–1305. [Google Scholar] [CrossRef]
- Wilts, I.T.; Bleker, S.M.; Van Es, N.; Büller, H.R.; Di Nisio, M.; Kamphuisen, P.W. Safety of anticoagulant treatment in cancer patients. Expert Opin. Drug Saf. 2015, 14, 1227–1236. [Google Scholar] [CrossRef]
- Watson, N.; Al-Samkari, H. Thrombotic and bleeding risk of angiogenesis inhibitors in patients with and without malignancy. J. Thromb. Haemost. 2021, 19, 1852–1863. [Google Scholar] [CrossRef]
- Wun, T.; White, R.H. Epidemiology of cancer-related venous thromboembolism. Best Pract. Res. Clin. Haematol. 2009, 22, 9–23. [Google Scholar] [CrossRef] [Green Version]
- Mantha, S. Bleeding Disorders Associated with Cancer. Cancer Treat. Res. 2019, 179, 191–203. [Google Scholar]
- Prommer, E. Management of bleeding in the terminally ill patient. Hematology 2005, 10, 167–175. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Kwok, C.S.; Wong, C.W.; Kontopantelis, E.; Barac, A.; Brown, S.A.; Velagapudi, P.; Hilliard, A.A.; Bharadwaj, A.S.; Chadi Alraies, M.; Mohamed, M.; et al. Percutaneous coronary intervention in patients with cancer and readmissions within 90 days for acute myocardial infarction and bleeding in the USA. Eur. Heart J. 2021, 42, 1019–1034. [Google Scholar] [CrossRef] [PubMed]
- Belzile-Dugas, E.; Eisenberg, M.J. Radiation-Induced Cardiovascular Disease: Review of an Underrecognized Pathology. J. Am. Heart Assoc. Cardiovasc. Cerebrovasc. Dis. 2021, 10, 21686. [Google Scholar] [CrossRef] [PubMed]
- Das, S.K.; Das, A.K.; William, M. 5-Fluorouracil-induced acute coronary syndrome. Med. J. Aust. 2019, 211, 255–257.e1. [Google Scholar] [CrossRef] [PubMed]
- Polk, A.; Vaage-Nilsen, M.; Vistisen, K.; Nielsen, D.L. Cardiotoxicity in cancer patients treated with 5-fluorouracil or capecitabine: A systematic review of incidence, manifestations and predisposing factors. Cancer Treat. Rev. 2013, 39, 974–984. [Google Scholar] [CrossRef] [PubMed]
- Hanchate, L.P.; Sharma, S.R.; Madyalkar, S. Cisplatin Induced Acute Myocardial Infarction and Dyslipidemia. J. Clin. Diagn. Res. 2017, 11, OD05–OD07. [Google Scholar] [CrossRef] [PubMed]
- Karabay, K.O.; Yildiz, O.; Aytekin, V. Multiple coronary thrombi with cisplatin. J. Invasive Cardiol. 2014, 26, E18–E20. [Google Scholar]
- Chen, X.L.; Lei, Y.H.; Liu, C.F.; Yang, Q.F.; Zuo, P.Y.; Liu, C.Y.; Chen, C.Z.; Liu, Y.W. Angiogenesis inhibitor bevacizumab increases the risk of ischemic heart disease associated with chemotherapy: A meta-analysis. PLoS ONE 2013, 8, e66721. [Google Scholar] [CrossRef] [Green Version]
- Kounis, N.G.; Soufras, G.D.; Tsigkas, G.; Hahalis, G. Adverse cardiac events to monoclonal antibodies used for cancer therapy. Oncoimmunology 2014, 3, e27987. [Google Scholar] [CrossRef] [Green Version]
- Amir, E.; Seruga, B.; Niraula, S.; Carlsson, L.; Ocaña, A. Toxicity of adjuvant endocrine therapy in postmenopausal breast cancer patients: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2011, 103, 1299–1309. [Google Scholar] [CrossRef] [Green Version]
- Ziehr, D.R.; Chen, M.H.; Zhang, D.; Braccioforte, M.H.; Moran, B.J.; Mahal, B.A.; Hyatt, A.S.; Basaria, S.S.; Beard, C.J.; Beckman, J.A.; et al. Association of androgen-deprivation therapy with excess cardiac-specific mortality in men with prostate cancer. BJU Int. 2015, 116, 358–365. [Google Scholar] [CrossRef]
- Naib, T.; Steingart, R.M.; Chen, C.L. Sorafenib-associated multivessel coronary artery vasospasm. Herz 2011, 36, 348–351. [Google Scholar] [CrossRef] [PubMed]
- Costa, I.B.S.D.S.; Andrade, F.T.D.A.; Carter, D.; Seleme, V.B.; Costa, M.S.; Campos, C.M.; Hajjar, L.A. Challenges and Management of Acute Coronary Syndrome in Cancer Patients. Front. Cardiovasc. Med. 2021, 8, 590016. [Google Scholar] [CrossRef] [PubMed]
- Drobni, Z.D.; Alvi, R.M.; Taron, J.; Zafar, A.; Murphy, S.P.; Rambarat, P.K.; Mosarla, R.C.; Lee, C.; Zlotoff, D.A.; Raghu, V.K.; et al. Association Between Immune Checkpoint Inhibitors With Cardiovascular Events and Atherosclerotic Plaque. Circulation 2020, 142, 2299–2311. [Google Scholar] [CrossRef] [PubMed]
- Cornell, R.F.; Ky, B.; Weiss, B.M.; Dahm, C.N.; Gupta, D.K.; Du, L.; Carver, J.R.; Cohen, A.D.; Engelhardt, B.G.; Garfall, A.L.; et al. Prospective Study of Cardiac Events During Proteasome Inhibitor Therapy for Relapsed Multiple Myeloma. J. Clin. Oncol. 2019, 37, 1946–1955. [Google Scholar] [CrossRef]
- Abdel-Qadir, H.; Sabrie, N.; Leong, D.; Pang, A.; Austin, P.C.; Prica, A.; Nanthakumar, K.; Calvillo-Argüelles, O.; Lee, D.S.; Thavendiranathan, P. Cardiovascular Risk Associated With Ibrutinib Use in Chronic Lymphocytic Leukemia: A Population-Based Cohort Study. J. Clin. Oncol. 2021, 39, 3453–3462. [Google Scholar] [CrossRef]
- Kapelakis, I.; Toutouzas, K.; Drakopoulou, M.; Michelongona, A.; Zagouri, F.; Mpamias, A.; Pliatsika, P.; Dimopoulos, M.-A.; Stefanadis, C.; Tousoulis, D. Bevacizumab increases the incidence of cardiovascular events in patients with metastatic breast or colorectal cancer. Hell. J. Cardiol. 2016, 58, 215–219. [Google Scholar] [CrossRef]
- Lopes, R.D.; Higano, C.S.; Slovin, S.F.; Nelson, A.J.; Bigelow, R.; Sørensen, P.S.; Melloni, C.; Goodman, S.G.; Evans, C.P.; Nilsson, J.; et al. Cardiovascular Safety of Degarelix Versus Leuprolide in Patients With Prostate Cancer: The Primary Results of the PRONOUNCE Randomized Trial. Circulation 2021, 144, 1295–1307. [Google Scholar] [CrossRef]
- Banasiak, W.; Zymlinski, R.; Undas, A. Optimal management of cancer patients with acute coronary syndrome. Polish Arch. Intern. Med. 2018, 128, 244–253. [Google Scholar] [CrossRef] [Green Version]
- Apostolos, A.; Trigka, A.; Chlorogiannis, D.; Vasilagkos, G.; Chamakioti, M.; Spyropoulou, P.; Karamasis, G.; Dimitriadis, K.; Moulias, A.; Katsanos, K.; et al. Thirty-days versus standard duration of dual antiplatelet treatment after percutaneous coronary interventions: A systematic review and meta-analysis. Eur. Heart J. 2022, 43, ehac544-2717. [Google Scholar] [CrossRef]
- Tsigkas, G.; Apostolos, A.; Trigka, A.; Chlorogiannis, D.; Katsanos, K.; Toutouzas, K.; Alexopoulos, D.; Brilakis, E.S.; Davlouros, P. Very Short Versus Longer Dual Antiplatelet Treatment After Coronary Interventions: A Systematic Review and Meta-analysis. Am. J. Cardiovasc. Drugs 2022, 23, 35–46. [Google Scholar] [CrossRef]
- Balanescu, D.V.; Aziz, M.K.; Donisan, T.; Palaskas, N.; Lopez-Mattei, J.; Hassan, S.; Kim, P.; Song, J.; Ntim, W.; Cilingiroglu, M.; et al. Cancer treatment resumption in patients with new-generation drug-eluting stents. Coron. Artery Dis. 2021, 32, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T.; Pacha, H.M.; Addoumieh, A.; Koutroumpakis, E.; Song, J.; Charitakis, K.; Boudoulas, K.D.; Cilingiroglu, M.; Marmagkiolis, K.; Grines, C.; et al. Percutaneous coronary intervention in patients with cancer using bare metal stents compared to drug-eluting stents. Front. Cardiovasc. Med. 2022, 9, 901431. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, Y.; Garcia-Garcia, H.M.; Mintz, G.S.; Waksman, R. Supporting evidence from optical coherence tomography for shortening dual antiplatelet therapy after drug-eluting stents implantation. Expert Rev. Cardiovasc. Ther. 2020, 18, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Apostolos, A.; Gerakaris, A.; Tsoni, E.; Pappelis, K.; Vasilagkos, G.; Bousoula, E.; Moulias, A.; Konstantinou, K.; Dimitriadis, K.; Karamasis, G.V.; et al. Imaging of Left Main Coronary Artery; Untangling the Gordian Knot. Rev. Cardiovasc. Med. 2023, 24, 26. [Google Scholar] [CrossRef]
- Iliescu, C.A.; Cilingiroglu, M.; Giza, D.E.; Rosales, O.; Lebeau, J.; Guerrero-Mantilla, I.; Lopez-Mattei, J.; Song, J.; Silva, G.; Loyalka, P.; et al. “Bringing on the light” in a complex clinical scenario: Optical coherence tomography-guided discontinuation of antiplatelet therapy in cancer patients with coronary artery disease (PROTECT-OCT registry). Am. Heart J. 2017, 194, 83–91. [Google Scholar] [CrossRef]
- Doolub, G.; Mamas, M.A. Percutaneous Coronary Angioplasty in Patients with Cancer: Clinical Challenges and Management Strategies. J. Pers. Med. 2022, 12, 1372. [Google Scholar] [CrossRef]
- Bisceglia, I.; Canale, M.L.; Lestuzzi, C.; Parrini, I.; Russo, G.; Colivicchi, F.; Gabrielli, D.; Gulizia, M.M.; Iliescu, C.A. Acute coronary syndromes in cancer patients. J. Cardiovasc. Med. 2020, 21, 944–952. [Google Scholar] [CrossRef]
- Gevaert, S.A.; Halvorsen, S.; Sinnaeve, P.R.; Sambola, A.; Gulati, G.; Lancellotti, P.; Van Der Meer, P.; Lyon, A.R.; Farmakis, D.; Lee, G.; et al. Evaluation and management of cancer patients presenting with acute cardiovascular disease: A Consensus Document of the Acute CardioVascular Care (ACVC) association and the ESC council of Cardio-Oncology-Part 1: Acute coronary syndromes and acute pericardial diseases. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 947–959. [Google Scholar]
- Lucà, F.; Parrini, I.; Abrignani, M.G.; Rao, C.M.; Piccioni, L.; Di Fusco, S.A.; Ceravolo, R.; Bisceglia, I.; Riccio, C.; Gelsomino, S.; et al. Management of Acute Coronary Syndrome in Cancer Patients: It’s High Time We Dealt with It. J. Clin. Med. 2022, 11, 1792. [Google Scholar] [CrossRef]
- Tsigkas, G.; Apostolos, A.; Chlorogiannis, D.-D.; Bousoula, E.; Vasilagkos, G.; Tsalamandris, S.; Tsiafoutis, I.; Katsanos, K.; Toutouzas, K.; Aminian, A.; et al. Thirty-Days versus Longer Duration of Dual Antiplatelet Treatment after Percutaneous Coronary Interventions with Newer Drug-Eluting Stents: A Systematic Review and Meta-Analysis. Life 2023, 13, 666. [Google Scholar] [CrossRef]
- Apostolos, A.; Chlorogiannis, D.; Vasilagkos, G.; Katsanos, K.; Toutouzas, K.; Aminian, A.; Alexopoulos, D.; Davlouros, P.; Tsigkas, G. Safety and efficacy of shortened dual antiplatelet therapy after complex percutaneous coronary intervention: A systematic review and meta-analysis. Hell. J. Cardiol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Bauersachs, J.; Dendale, P.; Edvardsen, T.; Gale, C.P.; Jobs, A.; Lambrinou, E.; Mehilli, J.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sechtem, U.; Banning, A.P.; Bonaros, N.; Bueno, H.; Bugiardini, R.; Chieffo, A.; Crea, F.; Czerny, M.; Delgado, V.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar]
- Baran, D.A.; Grines, C.L.; Bailey, S.; Burkhoff, D.; Hall, S.A.; Henry, T.D.; Hollenberg, S.M.; Kapur, N.K.; O’Neill, W.; Ornato, J.P.; et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock: This document was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), the Society of Critical Care Medicine (SCCM), and the Society of Thoracic Surgeons (STS) in April 2019. Catheter. Cardiovasc. Interv. 2019, 94, 29–37. [Google Scholar]
- McCarthy, C.P.; Steg, G.P.; Bhatt, D.L. The management of antiplatelet therapy in acute coronary syndrome patients with thrombocytopenia: A clinical conundrum. Eur. Heart J. 2017, 38, 3488–3492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiffer, C.A.; Bohlke, K.; Anderson, K.C. Platelet Transfusion for Patients With Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update Summary. J. Oncol. Pract. 2018, 14, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Stucchi, M.; Cantoni, S.; Piccinelli, E.; Savonitto, S.; Morici, N. Anemia and acute coronary syndrome: Current perspectives. Vasc. Health Risk Manag. 2018, 14, 109–118. [Google Scholar] [CrossRef] [Green Version]
- Ueki, Y.; Vögeli, B.; Karagiannis, A.; Zanchin, T.; Zanchin, C.; Rhyner, D.; Otsuka, T.; Praz, F.; Siontis, G.C.M.; Moro, C.; et al. Ischemia and Bleeding in Cancer Patients Undergoing Percutaneous Coronary Intervention. Cardio Oncol. 2019, 1, 145–155. [Google Scholar] [CrossRef]
- Gerotziafas, G.T.; Taher, A.; Abdel-Razeq, H.; AboElnazar, E.; Spyropoulos, A.C.; El Shemmari, S.; Larsen, A.K.; Elalamy, I. A Predictive Score for Thrombosis Associated with Breast, Colorectal, Lung, or Ovarian Cancer: The Prospective COMPASS-Cancer-Associated Thrombosis Study. Oncologist 2017, 22, 1222–1231. [Google Scholar] [CrossRef] [Green Version]
- Sibbing, D.; Aradi, D.; Alexopoulos, D.; ten Berg, J.; Bhatt, D.L.; Bonello, L.; Collet, J.P.; Cuisset, T.; Franchi, F.; Gross, L.; et al. Updated Expert Consensus Statement on Platelet Function and Genetic Testing for Guiding P2Y12 Receptor Inhibitor Treatment in Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2019, 12, 1521–1537. [Google Scholar] [CrossRef]
- Cooke, N.M.; Egan, K.; Mcfadden, S.; Grogan, L.; Breathnach, O.S.; O’Leary, J.; Hennessy, B.T.; Kenny, D. Increased platelet reactivity in patients with late-stage metastatic cancer. Cancer Med. 2013, 2, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Cowman, J.; Richter, L.; Walsh, R.; Keegan, N.; Tinago, W.; Ricco, A.J.; Hennessy, B.T.; Kenny, D.; Dunne, E. Dynamic platelet function is markedly different in patients with cancer compared to healthy donors. Platelets 2019, 30, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Just Vinholt, P.; Højrup Knudsen, G.; Sperling, S.; Frederiksen, H.; Nielsen, C. Platelet function tests predict bleeding in patients with acute myeloid leukemia and thrombocytopenia. Am. J. Hematol. 2019, 94, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Guha, A.; Dey, A.K.; Kalra, A.; Gumina, R.; Lustberg, M.; Lavie, C.J.; Sabik, J.F.; Addison, D. Coronary Artery Bypass Grafting in Cancer Patients: Prevalence and Outcomes in the United States. Mayo Clin. Proc. 2020, 95, 1865–1876. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Kastrati, A.; Kolh, P.; Mauri, L.; Montalescot, G.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–254. [Google Scholar]
- Kulik, A.; Ruel, M.; Jneid, H.; Ferguson, T.B.; Hiratzka, L.F.; Ikonomidis, J.S.; Lopez-Jimenez, F.; McNallan, S.M.; Patel, M.; Roger, V.L.; et al. Secondary prevention after coronary artery bypass graft surgery: A scientific statement from the American Heart Association. Circulation 2015, 131, 927–964. [Google Scholar] [CrossRef] [Green Version]
- Sousa-Uva, M.; Head, S.J.; Milojevic, M.; Collet, J.P.; Landoni, G.; Castella, M.; Dunning, J.; Gudbjartsson, T.; Linker, N.J.; Sandoval, E.; et al. 2017 EACTS Guidelines on perioperative medication in adult cardiac surgery. Eur. J. Cardiothorac. Surg. 2018, 53, 5–33. [Google Scholar] [CrossRef] [Green Version]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, 197–215. [Google Scholar] [CrossRef]
- Vener, C.; Banzi, R.; Ambrogi, F.; Ferrero, A.; Saglio, G.; Pravettoni, G.; Sant, M. First-line imatinib vs second- and third-generation TKIs for chronic-phase CML: A systematic review and meta-analysis. Blood Adv. 2020, 4, 2723–2735. [Google Scholar] [CrossRef]
- Capodanno, D.; Di Maio, M.; Greco, A.; Bhatt, D.L.; Gibson, C.M.; Goette, A.; Lopes, R.D.; Mehran, R.; Vranckx, P.; Angiolillo, D.J. Safety and Efficacy of Double Antithrombotic Therapy With Non-Vitamin K Antagonist Oral Anticoagulants in Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2020, 9, e017212. [Google Scholar] [CrossRef]
- Lopes, R.D.; Hong, H.; Harskamp, R.E.; Bhatt, D.L.; Mehran, R.; Cannon, C.P.; Granger, C.B.; Verheugt, F.W.A.; Li, J.; Ten Berg, J.M.; et al. Optimal Antithrombotic Regimens for Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: An Updated Network Meta-analysis. JAMA Cardiol. 2020, 5, 582–589. [Google Scholar] [CrossRef]
- Lopes, R.D.; Hong, H.; Harskamp, R.E.; Bhatt, D.L.; Mehran, R.; Cannon, C.P.; Granger, C.B.; Verheugt, F.W.A.; Li, J.; Ten Berg, J.M.; et al. Safety and Efficacy of Antithrombotic Strategies in Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: A Network Meta-analysis of Randomized Controlled Trials. JAMA Cardiol. 2019, 4, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Golwala, H.B.; Cannon, C.P.; Steg, P.G.; Doros, G.; Qamar, A.; Ellis, S.G.; Oldgren, J.; Ten Berg, J.M.; Kimura, T.; Hohnloser, S.H.; et al. Safety and efficacy of dual vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: A systematic review and meta-analysis of randomized clinical trials. Eur. Heart J. 2018, 39, 1726–1735. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Huber, K.; Mehran, R.; Lip, G.Y.H.; Faxon, D.P.; Granger, C.B.; Vranckx, P.; Lopes, R.D.; Montalescot, G.; Cannon, C.P.; et al. Management of Antithrombotic Therapy in Atrial Fibrillation Patients Undergoing PCI: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 83–99. [Google Scholar] [CrossRef]
- Buccheri, S.; Angiolillo, D.J.; Capodanno, D. Evolving paradigms in antithrombotic therapy for anticoagulated patients undergoing coronary stenting. Ther. Adv. Cardiovasc. Dis. 2019, 13, 1753944719891688. [Google Scholar] [CrossRef]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.W.; Wildgoose, P.; Birmingham, M.; Ianus, J.; Burton, P.; van Eickels, M.; et al. Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI. N. Engl. J. Med. 2016, 375, 2423–2434. [Google Scholar] [CrossRef] [Green Version]
- Cannon, C.P.; Bhatt, D.L.; Oldgren, J.; Lip, G.Y.H.; Ellis, S.G.; Kimura, T.; Maeng, M.; Merkely, B.; Zeymer, U.; Gropper, S.; et al. Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation. N. Engl. J. Med. 2017, 377, 1513–1524. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic Therapy after Acute Coronary Syndrome or PCI in Atrial Fibrillation. N. Engl. J. Med. 2019, 380, 1509–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batushkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): A randomised, open-label, phase 3b trial. Lancet 2019, 394, 1335–1343. [Google Scholar] [CrossRef]
- Capodanno, D.; Angiolillo, D.J. Dual antithrombotic therapy for atrial fibrillation and PCI. Lancet 2019, 394, 1300–1302. [Google Scholar] [CrossRef]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Schechter, M.; Balanescu, D.V.; Donisan, T.; Dayah, T.J.; Kar, B.; Gregoric, I.; Giza, D.E.; Song, J.; Lopez-Mattei, J.; Kim, P.; et al. An update on the management and outcomes of cancer patients with severe aortic stenosis. Catheter. Cardiovasc. Interv. 2019, 94, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Marmagkiolis, K.; Monlezun, D.J.; Cilingiroglu, M.; Grines, C.; Herrmann, J.; Toutouzas, K.P.; Ates, I.; Iliescu, C. TAVR in Cancer Patients: Comprehensive Review, Meta-Analysis, and Meta-Regression. Front. Cardiovasc. Med. 2021, 8, 641268. [Google Scholar] [CrossRef]
- Karaduman, B.D.; Ayhan, H.; Keleş, T.; Bozkurt, E. Clinical outcomes after transcatheter aortic valve implantation in active cancer patients and cancer survivors. Turk. J. Thorac. Cardiovasc. Surg. 2021, 29, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Drakopoulou, M.; Soulaidopoulos, S.; Oikonomou, G.; Stathogiannis, K.; Latsios, G.; Synetos, A.; Tousoulis, D.; Toutouzas, K. Novel Perspective for Antithrombotic Therapy in TAVI. Curr. Pharm. Des. 2020, 26, 2789–2803. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Collet, J.P.; Dangas, G.; Montalescot, G.; ten Berg, J.M.; Windecker, S.; Angiolillo, D.J. Antithrombotic Therapy After Transcatheter Aortic Valve Replacement. JACC. Cardiovasc. Interv. 2021, 14, 1688–1703. [Google Scholar] [CrossRef]
- Kuno, T.; Takagi, H.; Sugiyama, T.; Ando, T.; Miyashita, S.; Valentin, N.; Shimada, Y.J.; Kodaira, M.; Numasawa, Y.; Kanei, Y.; et al. Antithrombotic strategies after transcatheter aortic valve implantation: Insights from a network meta-analysis. Catheter. Cardiovasc. Interv. 2020, 96, E177–E186. [Google Scholar] [CrossRef]
- Kobari, Y.; Inohara, T.; Tsuruta, H.; Yashima, F.; Shimizu, H.; Fukuda, K.; Naganuma, T.; Mizutani, K.; Yamawaki, M.; Tada, N.; et al. No Antithrombotic Therapy After Transcatheter Aortic Valve Replacement: Insight From the OCEAN-TAVI Registry. JACC. Cardiovasc. Interv. 2023, 16, 79–91. [Google Scholar] [CrossRef]
- Drakopoulou, M.; Soulaidopoulos, S.; Stathogiannis, K.; Oikonomou, G.; Papanikolaou, A.; Toutouzas, K.; Tousoulis, D. Antiplatelet and Antithrombotic Therapy After Patent Foramen Oval and Atrial Septal Defect Closure. Curr. Pharm. Des. 2020, 26, 2769–2779. [Google Scholar] [CrossRef]
- Apostolos, A.; Drakopoulou, M.; Gregoriou, S.; Synetos, A.; Trantalis, G.; Tsivgoulis, G.; Deftereos, S.; Tsioufis, K.; Toutouzas, K. Nickel Hypersensitivity to Atrial Septal Occluders: Smoke Without Fire? Clin. Rev. Allergy Immunol. 2022, 62, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Apostolos, A.; Drakopoulou, M.; Toutouzas, K. New migraines after atrial septal defect occlusion. Is the nickel hypersensitivity the start of everything? Med. Hypotheses 2021, 146, 110442. [Google Scholar] [CrossRef] [PubMed]
- Pristipino, C.; Sievert, H.; D’Ascenzo, F.; Louis Mas, J.; Meier, B.; Scacciatella, P.; Hildick-Smith, D.; Gaita, F.; Toni, D.; Kyrle, P.; et al. European position paper on the management of patients with patent foramen ovale. General approach and left circulation thromboembolism. Eur. Heart J. 2019, 40, 3182–3195. [Google Scholar] [CrossRef] [PubMed]
- Mas, J.-L.; Derumeaux, G.; Guillon, B.; Massardier, E.; Hosseini, H.; Mechtouff, L.; Arquizan, C.; Béjot, Y.; Vuillier, F.; Detante, O.; et al. Patent Foramen Ovale Closure or Anticoagulation vs. Antiplatelets after Stroke. N. Engl. J. Med. 2017, 377, 1011–1021. [Google Scholar] [CrossRef]
- Lee, P.H.; Song, J.K.; Kim, J.S.; Heo, R.; Lee, S.; Kim, D.H.; Song, J.M.; Kang, D.H.; Kwon, S.U.; Kang, D.W.; et al. Cryptogenic Stroke and High-Risk Patent Foramen Ovale: The DEFENSE-PFO Trial. J. Am. Coll. Cardiol. 2018, 71, 2335–2342. [Google Scholar] [CrossRef] [PubMed]
- Meier, B. Closure of patent foramen ovale: Technique, pitfalls, complications, and follow up. Heart 2005, 91, 444–448. [Google Scholar] [CrossRef] [Green Version]
- Hobohm, L.; von Bardeleben, R.S.; Ostad, M.A.; Wenzel, P.; Münzel, T.; Gori, T.; Keller, K. 5-Year Experience of In-Hospital Outcomes After Percutaneous Left Atrial Appendage Closure in Germany. JACC. Cardiovasc. Interv. 2019, 12, 1044–1052. [Google Scholar] [CrossRef]
- Chen, S.; Weise, F.K.; Chun, K.R.J.; Schmidt, B. Antithrombotic strategies after interventional left atrial appendage closure: An update. Expert Rev. Cardiovasc. Ther. 2018, 16, 675–678. [Google Scholar] [CrossRef]
- Ledwoch, J.; Sievert, K.; Boersma, L.V.A.; Bergmann, M.W.; Ince, H.; Kische, S.; Pokushalov, E.; Schmitz, T.; Schmidt, B.; Gori, T.; et al. Initial and long-term antithrombotic therapy after left atrial appendage closure with the WATCHMAN. Europace 2020, 22, 1036–1043. [Google Scholar] [CrossRef]
- Patti, G.; Sticchi, A.; Verolino, G.; Pasceri, V.; Vizzi, V.; Brscic, E.; Casu, G.; Golino, P.; Russo, V.; Rapacciuolo, A.; et al. Safety and Efficacy of Single Versus Dual Antiplatelet Therapy After Left Atrial Appendage Occlusion. Am. J. Cardiol. 2020, 134, 83–90. [Google Scholar] [CrossRef]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.L.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vasc. Eur. Heart J. 2018, 39, 763–816. [Google Scholar]
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fonseca, A.C.; Merwick, Á.; Dennis, M.; Ferrari, J.; Ferro, J.M.; Kelly, P.; Lal, A.; Ois, A.; Olivot, J.M.; Purroy, F. European Stroke Organisation (ESO) guidelines on management of transient ischaemic attack. Eur. Stroke J. 2021, 6, CLXIII–CLXXXVI. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, K.; Jain, V.; Aggarwal, D.; Vaduganathan, M.; Arora, S.; Hussain, Z.; Uberoi, G.; Tafur, A.; Zhang, C.; Ricciardi, M.; et al. Dual Antiplatelet Therapy Versus Aspirin in Patients With Stroke or Transient Ischemic Attack: Meta-Analysis of Randomized Controlled Trials. Stroke 2021, 52, E217–E223. [Google Scholar] [CrossRef] [PubMed]
- Zaorsky, N.G.; Zhang, Y.; Tchelebi, L.T.; Mackley, H.B.; Chinchilli, V.M.; Zacharia, B.E. Stroke among cancer patients. Nat. Commun. 2019, 10, 5172. [Google Scholar] [CrossRef] [Green Version]
- Bang, O.Y.; Chung, J.W.; Lee, M.J.; Seo, W.K.; Kim, G.M.; Ahn, M.J. Cancer-Related Stroke: An Emerging Subtype of Ischemic Stroke with Unique Pathomechanisms. J. Stroke 2020, 22, 1–10. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsigkas, G.; Vakka, A.; Apostolos, A.; Bousoula, E.; Vythoulkas-Biotis, N.; Koufou, E.-E.; Vasilagkos, G.; Tsiafoutis, I.; Hamilos, M.; Aminian, A.; et al. Dual Antiplatelet Therapy and Cancer; Balancing between Ischemic and Bleeding Risk: A Narrative Review. J. Cardiovasc. Dev. Dis. 2023, 10, 135. https://doi.org/10.3390/jcdd10040135
Tsigkas G, Vakka A, Apostolos A, Bousoula E, Vythoulkas-Biotis N, Koufou E-E, Vasilagkos G, Tsiafoutis I, Hamilos M, Aminian A, et al. Dual Antiplatelet Therapy and Cancer; Balancing between Ischemic and Bleeding Risk: A Narrative Review. Journal of Cardiovascular Development and Disease. 2023; 10(4):135. https://doi.org/10.3390/jcdd10040135
Chicago/Turabian StyleTsigkas, Grigorios, Angeliki Vakka, Anastasios Apostolos, Eleni Bousoula, Nikolaos Vythoulkas-Biotis, Eleni-Evangelia Koufou, Georgios Vasilagkos, Ioannis Tsiafoutis, Michalis Hamilos, Adel Aminian, and et al. 2023. "Dual Antiplatelet Therapy and Cancer; Balancing between Ischemic and Bleeding Risk: A Narrative Review" Journal of Cardiovascular Development and Disease 10, no. 4: 135. https://doi.org/10.3390/jcdd10040135