
Exploring the Role of Circulating Cell-Free RNA in the Development of Colorectal Cancer
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Blood-Based Liquid Biopsy in CRC

{kind=link}
| Liquid Biopsy Component | Strengths | Limitation |
|---|---|---|
| ctDNA | ||
| ctRNA |
| |
| CTC | ||
| EV |
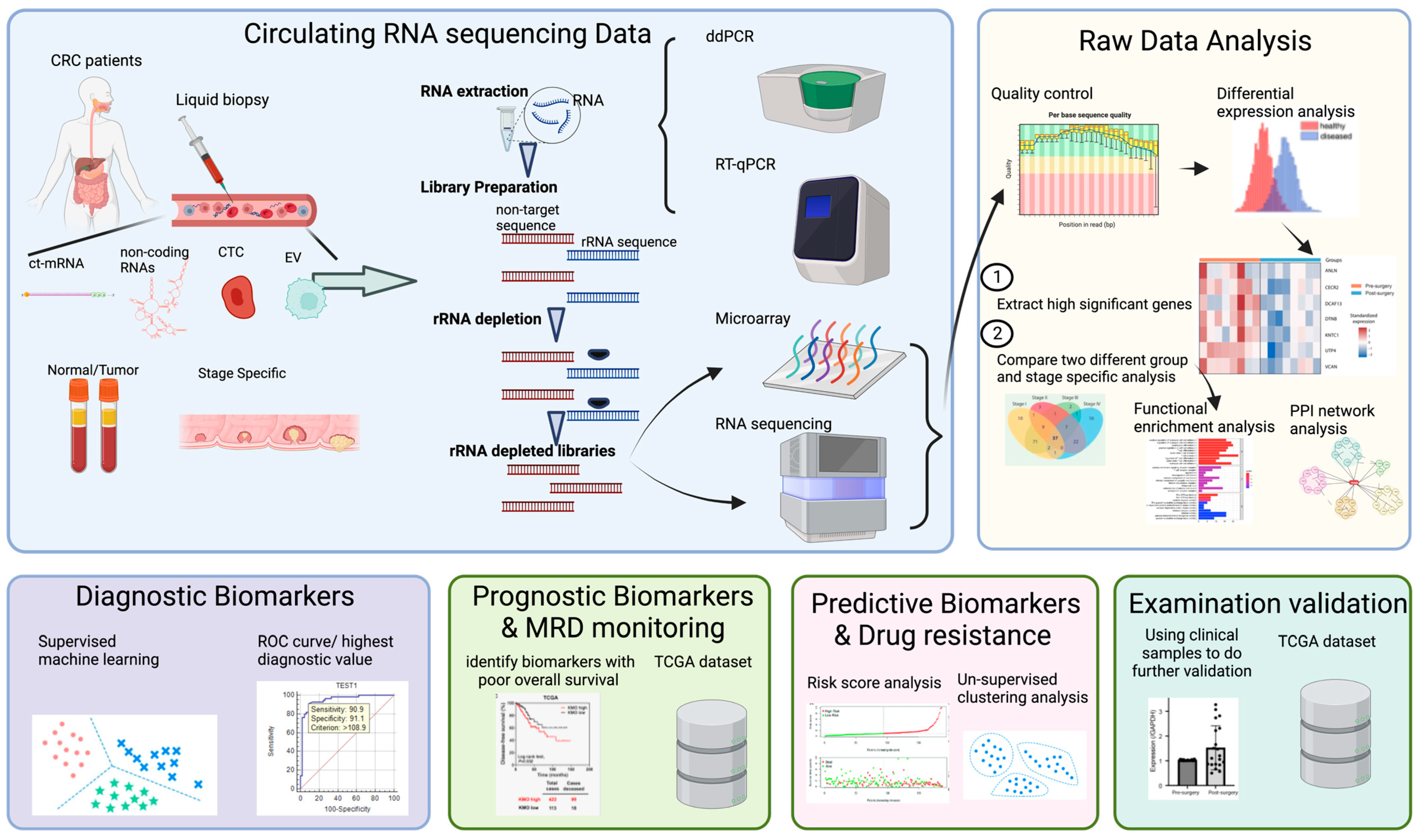
3. Application of Circulating RNA Sequencing in Colorectal Cancer
4. Circulating Cell-Free RNA as a Diagnostic Biomarker in CRC
| Year | Biomarker | Biomarker Type | Samples | Up-/Downregulated in CRC Patients | Value | Technology | Reference |
|---|---|---|---|---|---|---|---|
| 2019 | RHOA, GSK3A | mRNA | 40 plasma adenoma CRC 39 plasma normal | Down | Diagnosis | Target-Seq | [79] |
| 2023 | SOX9 | mRNA | 34 plasma adenoma CRC 19 plasma normal | Up | Diagnosis | Target-Seq | [84] |
| 2021 | PTGS2, GUCY2C, and JAG1 | mRNA | 59 serum mCRC | Up | Diagnosis | ddPCR | [86] |
| 2023 | B2M, TIM-1, and CLU | mRNA | 107 plasma mCRC 53 plasma control | Up | Diagnosis | RT-qPCR | [87] |
| 2022 | miR-21, miR-145, miR-203, miR-155, miR-210, miR-31, miR-345 | miRNA | Up | Diagnosis | RT-qPCR | [88] | |
| 2022 | miR-21-5p, miR-29a-3p, miR-92a-3p, miR-196b-5p, miR-135b-5p | miRNA | 41 CRC tissue and adjacent tumor tissue 36 plasma CRC | Up Down | Diagnosis | RT-qPCR | [89] |
| 2023 | miRNA-133a, miRNA-574-3p, miRNA-27a | miRNA | 100 serum CRC 20 control | Down Up | Diagnosis | RT-qPCR | [91] |
| 2021 | miR-28-3p, let-7e-5p, miR-106a-5p, and miR-542-5p | miRNA | 109 plasma | Up | Diagnostic | RT-qPCR | [90] |
| 2019 | ATB and CCAT1 | IncRNA | 74 plasma CRC 74 control | Up | Diagnosis | RT-qPCR | [95,106] |
| 2020 | DANCR | IncRNA | 40 serum CRC 40 control | Up | Diagnosis | RT-qPCR | [94] |
| 2021 | hsa_circ_0001445, hsa_circ_0003028, hsa_circ_0007915, and hsa_circ_0008717 | circRNA | 150 plasma CRC | Up | Diagnosis | RT-qPCR | [96] |
5. Circulating Cell-Free RNA as a Prognostic Biomarker in CRC
6. Circulating Cell-Free RNA as a Response to Therapy and Drug Resistance in CRC
7. Challenges in Circulating RNA Sequencing in Plasma
8. Future Perspectives
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37,513,025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, R.; Guo, F.; Heisser, T.; De Schutter, H.; Van Damme, N.; Nilbert, M.C.; Christensen, J.; Bouvier, A.-M.; Bouvier, V.; Launoy, G.; et al. Overall and stage-specific survival of patients with screen-detected colorectal cancer in European countries: A population-based study in 9 countries. Lancet Reg. Health Eur. 2022, 21, 100458. [Google Scholar] [CrossRef] [PubMed]
- Kotani, D.; Oki, E.; Nakamura, Y.; Yukami, H.; Mishima, S.; Bando, H.; Shirasu, H.; Yamazaki, K.; Watanabe, J.; Kotaka, M.; et al. Molecular residual disease and efficacy of adjuvant chemotherapy in patients with colorectal cancer. Nat. Med. 2023, 29, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Loupakis, F.; Sharma, S.; Derouazi, M.; Murgioni, S.; Biason, P.; Rizzato, M.D.; Rasola, C.; Renner, D.; Shchegrova, S.; Koyen Malashevich, A.; et al. Detection of Molecular Residual Disease Using Personalized Circulating Tumor DNA Assay in Patients With Colorectal Cancer Undergoing Resection of Metastases. JCO Precis. Oncol. 2021, 5, 1166–1177. [Google Scholar] [CrossRef]
- Faulkner, L.G.; Howells, L.M.; Pepper, C.; Shaw, J.A.; Thomas, A.L. The utility of ctDNA in detecting minimal residual disease following curative surgery in colorectal cancer: A systematic review and meta-analysis. Br. J. Cancer 2023, 128, 297–309. [Google Scholar] [CrossRef]
- Smith, G.E.; Carey, F.A.; Beattie, J.A.; Wilkie, M.J.V.; Lightfoot, T.; Coxhead, J.; Garner, R.C.; Steele, R.; Wolf, C.R. Mutations in APC, Kirsten-Ras, and P53—Alternative Genetic Pathways to Colorectal Cancer. Proc. Natl. Acad. Sci. USA 2002, 99, 9433–9438. [Google Scholar] [CrossRef] [PubMed]
- Lao, V.V.; Grady, W.M. Epigenetics and Colorectal Cancer. Nat. Rev. Gastroenterol. Hepatol. 2011, 8, 686–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Z.; Yu, T.; Zhao, X.; Gao, X.; Zhao, Y.; Liu, G. Intratumor heterogeneity: A new perspective on colorectal cancer researh. Cancer Med. 2020, 9, 7637–7645. [Google Scholar] [CrossRef]
- Bramsen, J.B.; Rasmussen, M.H.; Ongen, H.; Mattesen, T.B.; Ørntoft, M.-B.W.; Arnadottir, S.S.; Sandoval, J.; Laguna, T.; Vang, S.; Øster, B. Molecular-subtype-specific biomarkers improve prediction of prognosis in colorectal cancer. Cell Rep. 2017, 19, 1268–1280. [Google Scholar] [CrossRef] [Green Version]
- Russano, M.; Napolitano, A.; Ribelli, G.; Iuliani, M.; Simonetti, S.; Citarella, F.; Pantano, F.; Dell’Aquila, E.; Anesi, C.; Silvestris, N.; et al. Liquid biopsy and tumor heterogeneity in metastatic solid tumors: The potentiality of blood samples. J. Exp. Clin. Cancer Res. 2020, 39, 95. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.; Shehzad, A.; Khan, S.A.; Miran, W.; Khan, S.; Lee, Y.S. Diagnostic and Therapeutic Potential of Circulating-Free DNA and Cell-Free RNA in Cancer Management. Biomedicines 2022, 10, 2047. [Google Scholar] [CrossRef] [PubMed]
- Lone, S.N.; Nisar, S.; Masoodi, T.; Singh, M.; Rizwan, A.; Hashem, S.; El-Rifai, W.; Bedognetti, D.; Batra, S.K.; Haris, M.; et al. Liquid biopsy: A step closer to transform diagnosis, prognosis and future of cancer treatments. Mol. Cancer 2022, 21, 79. [Google Scholar] [CrossRef] [PubMed]
- Larson, M.H.; Pan, W.; Kim, H.J.; Mauntz, R.E.; Stuart, S.M.; Pimentel, M.; Zhou, Y.; Knudsgaard, P.; Demas, V.; Aravanis, A.M.; et al. A comprehensive characterization of the cell-free transcriptome reveals tissue- and subtype-specific biomarkers for cancer detection. Nat. Commun. 2021, 12, 2357. [Google Scholar] [CrossRef]
- Kolenda, T.; Guglas, K.; Baranowski, D.; Sobocińska, J.; Kopczyńska, M.; Teresiak, A.; Bliźniak, R.; Lamperska, K. cfRNAs as biomarkers in oncology—Still experimental or applied tool for personalized medicine already? Rep. Pract. Oncol. Radiother. 2020, 25, 783–792. [Google Scholar] [CrossRef]
- Diez-Fraile, A.; Ceulaer, J.D.; Derpoorter, C.; Spaas, C.; Backer, T.D.; Lamoral, P.; Abeloos, J.; Lammens, T. Circulating non-coding RNAs in head and neck cancer: Roles in diagnosis, prognosis, and therapy monitoring. Cells 2020, 10, 48. [Google Scholar] [CrossRef]
- Kim, W.T.; Jeong, P.; Yan, C.; Kim, Y.H.; Lee, I.-S.; Kang, H.-W.; Kim, Y.-J.; Lee, S.-C.; Kim, S.J.; Kim, Y.T. UBE2C cell-free RNA in urine can discriminate between bladder cancer and hematuria. Oncotarget 2016, 7, 58193. [Google Scholar] [CrossRef] [Green Version]
- Zhao, A.; Péoc’h, M.; Cottier, M.; Genin, C.; Mottet, N.; Li, G. Cell-free RNA content in urine as a possible molecular diagnostic tool for clear cell renal cell carcinoma. Int. J. Cancer 2015, 136, 2610–2615. [Google Scholar] [CrossRef]
- Fettke, H.; Kwan, E.M.; Docanto, M.M.; Bukczynska, P.; Ng, N.; Graham, L.-J.K.; Mahon, K.; Hauser, C.; Tan, W.; Wang, X.H. Combined cell-free DNA and RNA profiling of the androgen receptor: Clinical utility of a novel multianalyte liquid biopsy assay for metastatic prostate cancer. Eur. Urol. 2020, 78, 173–180. [Google Scholar] [CrossRef]
- Misale, S.; Di Nicolantonio, F.; Sartore-Bianchi, A.; Siena, S.; Bardelli, A. Resistance to anti-EGFR therapy in colorectal cancer: From heterogeneity to convergent evolution. Cancer Discov. 2014, 4, 1269–1280. [Google Scholar] [CrossRef] [Green Version]
- Montagut, C.; Dalmases, A.; Bellosillo, B.; Crespo, M.; Pairet, S.; Iglesias, M.; Salido, M.; Gallen, M.; Marsters, S.; Tsai, S.P. Identification of a mutation in the extracellular domain of the Epidermal Growth Factor Receptor conferring cetuximab resistance in colorectal cancer. Nat. Med. 2012, 18, 221–223. [Google Scholar] [CrossRef]
- Parikh, A.R.; Corcoran, R.B. Monitoring resistance through liquid biopsy. Ann. Oncol. 2018, 29, 8–11. [Google Scholar] [CrossRef]
- Murtaza, M.; Dawson, S.J.; Pogrebniak, K.; Rueda, O.M.; Provenzano, E.; Grant, J.; Chin, S.F.; Tsui, D.W.Y.; Marass, F.; Gale, D.; et al. Multifocal clonal evolution characterized using circulating tumour DNA in a case of metastatic breast cancer. Nat. Commun. 2015, 6, 8760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, N.; Kan, C.-M.; Pei, X.M.; Cheung, W.L.; Ng, S.S.M.; Wong, H.T.; Cheng, H.Y.-L.; Leung, W.W.; Wong, Y.N.; Tsang, H.F.; et al. Cell-free circulating tumor RNAs in plasma as the potential prognostic biomarkers in colorectal cancer. Front. Oncol. 2023, 13, 113444. [Google Scholar] [CrossRef] [PubMed]
- Cheung, P.K.; Ma, M.H.; Tse, H.F.; Yeung, K.F.; Tsang, H.F.; Chu, M.K.M.; Kan, C.M.; Cho, W.C.S.; Ng, L.B.W.; Chan, L.W.C.; et al. The applications of metabolomics in the molecular diagnostics of cancer. Expert Rev. Mol. Diagn. 2019, 19, 785–793. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, A.R.; Hamilton, S.R.; Allegra, C.J.; Grody, W.W.; Cushman-Vokoun, A.M.; Funkhouser, W.K.; Kopetz, S.; Lieu, C.H.; Lindor, N.M.; Minsky, B.D.; et al. Molecular Biomarkers for the Evaluation of Colorectal Cancer. J. Mol. Diagn. 2017, 19, 187–225. [Google Scholar] [CrossRef] [Green Version]
- Nicolazzo, C.; Belardinilli, F.; Vestri, A.; Magri, V.; Renzi, G.D.; Meo, M.D.; Caponnetto, S.; Nicolantonio, F.D.; Cortesi, E.; Giannini, G.; et al. RAS Mutation Conversion in Bevacizumab-Treated Metastatic Colorectal Cancer Patients: A Liquid Biopsy Based Study. Cancers 2022, 14, 802. [Google Scholar] [CrossRef]
- Cheung, K.W.E.; Choi, S.R.; Lee, L.T.C.; Lee, N.L.E.; Tsang, H.F.; Cheng, Y.T.; Cho, W.C.S.; Wong, E.Y.L.; Wong, S.C.C. The potential of circulating cell free RNA as a biomarker in cancer. Expert Rev. Mol. Diagn. 2019, 19, 579–590. [Google Scholar] [CrossRef]
- Lo, K.W.; Lo, Y.M.; Leung, S.F.; Tsang, Y.S.; Chan, L.Y.; Johnson, P.J.; Hjelm, N.M.; Lee, J.C.; Huang, D.P. Analysis of cell-free Epstein-Barr virus associated RNA in the plasma of patients with nasopharyngeal carcinoma. Clin. Chem. 1999, 45, 1292–1294. [Google Scholar] [CrossRef]
- Kopreski, M.S.; Benko, F.A.; Kwak, L.W.; Gocke, C.D. Detection of tumor messenger RNA in the serum of patients with malignant melanoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 1999, 5, 1961–1965. [Google Scholar]
- Wong, S.C.; Lo, S.F.; Cheung, M.T.; Ng, K.O.; Tse, C.W.; Lai, B.S.; Lee, K.C.; Lo, Y.M. Quantification of plasma beta-catenin mRNA in colorectal cancer and adenoma patients. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2004, 10, 1613–1617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, W.; Chen, Y.; Yang, J.; Zhuo, C.; Huang, S.; Zhang, H.; Shi, Y. Clinical Perspectives on Liquid Biopsy in Metastatic Colorectal Cancer. Front. Genet. 2021, 12, 634642. [Google Scholar] [CrossRef] [PubMed]
- Drag, M.H.; Kilpeläinen, T.O. Cell-free DNA and RNA—Measurement and applications in clinical diagnostics with focus on metabolic disorders. Physiol. Genomics 2021, 53, 33–46. [Google Scholar] [CrossRef]
- De Rubis, G.; Rajeev Krishnan, S.; Bebawy, M. Liquid Biopsies in Cancer Diagnosis, Monitoring, and Prognosis. Trends Pharmacol. Sci. 2019, 40, 172–186. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.T.; Lv, L.L.; Lan, H.Y.; Liu, B.C. Extracellular Vesicles: Opportunities and Challenges for the Treatment of Renal Diseases. Front. Physiol. 2019, 10, 226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chemi, F.; Mohan, S.; Guevara, T.; Clipson, A.; Rothwell, D.G.; Dive, C. Early Dissemination of Circulating Tumor Cells: Biological and Clinical Insights. Front. Oncol. 2021, 11, 672195. [Google Scholar] [CrossRef]
- Ma, B.; King, A.D.; Leung, L.; Wang, K.; Poon, A.; Ho, W.M.; Mo, F.; Chan, C.M.L.; Chan, A.T.C.; Wong, S.C.C. Identifying an early indicator of drug efficacy in patients with metastatic colorectal cancer-a prospective evaluation of circulating tumor cells, 18F-fluorodeoxyglucose positron-emission tomography and the RECIST criteria. Ann. Oncol. 2017, 28, 1576–1581. [Google Scholar] [CrossRef]
- Wong, S.C.; Chan, C.M.; Ma, B.B.; Hui, E.P.; Ng, S.S.; Lai, P.B.; Cheung, M.T.; Lo, E.S.; Chan, A.K.; Lam, M.Y.; et al. Clinical significance of cytokeratin 20-positive circulating tumor cells detected by a refined immunomagnetic enrichment assay in colorectal cancer patients. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2009, 15, 1005–1012. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.C.; Ng, S.S.; Cheung, M.T.; Luk, L.Y.; Chan, C.M.; Cheung, A.H.; Lee, V.H.; Lai, P.B.; Ma, B.B.; Hui, E.P.; et al. Clinical significance of CDX2-positive circulating tumour cells in colorectal cancer patients. Br. J. Cancer 2011, 104, 1000–1006. [Google Scholar] [CrossRef] [Green Version]
- Pei, X.M.; Wong, H.T.; Ng, S.S.M.; Leung, W.W.; Wong, Y.N.; Tsang, H.F.; Chan, A.K.C.; Wong, Y.K.E.; Yu, A.C.S.; Yim, A.K.Y.; et al. The diagnostic significance of CDH17-positive circulating tumor cells in patients with colorectal cancer. Expert Rev. Mol. Diagn. 2023, 23, 171–179. [Google Scholar] [CrossRef]
- Yang, C.; Zhuang, W.; Hu, Y.; Zhu, L. Clinical Significance of Peripheral Circulating Tumor Cell Counts in Colorectal Polyps and Non-Metastatic Colorectal Cancer. World J. Surg. Oncol. 2018, 16, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinert, G.; Schölch, S.; Niemietz, T.; Iwata, N.; García, S.; Behrens, B.; Voigt, A.Y.; Kloor, M.; Benner, A.; Bork, U.; et al. Immune Escape and Survival Mechanisms in Circulating Tumor Cells of Colorectal Cancer. Cancer Res. 2014, 74, 1694–1704. [Google Scholar] [CrossRef] [Green Version]
- Cabel, L.; Proudhon, C.; Gortais, H.; Loirat, D.; Coussy, F.; Pierga, J.-Y.; Bidard, F.-C. Circulating Tumor Cells: Clinical Validity and Utility. Int. J. Clin. Oncol. 2017, 22, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Gögenur, M.; Hillig, T.; Gögenur, I. CytoTrack Analysis Reveals Low Presence of Circulating Tumor Cells in the Perioperative Period in Patients With Non-Metastatic Colorectal Cancer. AntiCancer Res. 2017, 37, 3099–3103. [Google Scholar] [CrossRef] [PubMed]
- Witek, M.A.; Aufforth, R.D.; Wang, H.; Kamande, J.W.; Jackson, J.J.; Pullagurla, S.R.; Hupert, M.L.; Usary, J.; Wysham, W.Z.; Hilliard, D.; et al. Discrete Microfluidics for the Isolation of Circulating Tumor Cell Subpopulations Targeting Fibroblast Activation Protein Alpha and Epithelial Cell Adhesion Molecule. NPJ Precis. Oncol. 2017, 1, 24. [Google Scholar] [CrossRef] [Green Version]
- Burz, C.; Pop, V.-V.; Buiga, R.; Daniel, S.; Samasca, G.; Aldea, C.; Lupan, I. Circulating Tumor Cells in Clinical Research and Monitoring Patients With Colorectal Cancer. Oncotarget 2018, 9, 24561–24571. [Google Scholar] [CrossRef] [Green Version]
- Kowalik, A.; Kowalewska, M.; Góźdź, S. Current approaches for avoiding the limitations of circulating tumor cells detection methods—Implications for diagnosis and treatment of patients with solid tumors. Transl. Res. 2017, 185, 58–84.e15. [Google Scholar] [CrossRef] [Green Version]
- Eslami-S, Z.; Cortés-Hernández, L.E.; Thomas, F.; Pantel, K.; Alix-Panabières, C. Functional analysis of circulating tumour cells: The KEY to understand the biology of the metastatic cascade. Br. J. Cancer 2022, 127, 800–810. [Google Scholar] [CrossRef]
- Ladurner, M.; Wieser, M.; Eigentler, A.; Seewald, M.; Dobler, G.; Neuwirt, H.; Kafka, M.; Heidegger, I.; Horninger, W.; Bektic, J.; et al. Validation of Cell-Free RNA and Circulating Tumor Cells for Molecular Marker Analysis in Metastatic Prostate Cancer. Biomedicines 2021, 9, 1004. [Google Scholar] [CrossRef]
- Luzentales-Simpson, M.; Pang, Y.; Zhang, A.; Sousa, J.A.; Sly, L.M. Vedolizumab: Potential Mechanisms of Action for Reducing Pathological Inflammation in Inflammatory Bowel Diseases. Front. Cell Dev. Biol. 2021, 9, 612830. [Google Scholar] [CrossRef]
- Joosse, S.A.; Gorges, T.M.; Pantel, K. Biology, Detection, and Clinical Implications of Circulating Tumor Cells. Embo Mol. Med. 2014, 7, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Ding, H.-m.; Lin, M.; Yin, F.; Song, L.; Mao, X.; Li, F.; Ge, Z.; Wang, L.; Zuo, X.; et al. DNA Framework-Programmed Cell Capture via Topology-Engineered Receptor–Ligand Interactions. J. Am. Chem. Soc. 2019, 141, 18910–18915. [Google Scholar] [CrossRef] [PubMed]
- Cheshomi, H.; Matin, M.M. Exosomes and Their Importance in Metastasis, Diagnosis, and Therapy of Colorectal Cancer. J. Cell. Biochem. 2018, 120, 2671–2686. [Google Scholar] [CrossRef] [PubMed]
- Ye, S.-B.; Li, Z.L.; Luo, D.H.; Huang, B.J.; Chen, Y.S.; Zhang, X.; Cui, J.; Zeng, Y.X.; Li, J. Tumor-Derived Exosomes Promote Tumor Progression and T-Cell Dysfunction Through the Regulation of Enriched Exosomal microRNAs in Human Nasopharyngeal Carcinoma. Oncotarget 2014, 5, 5439–5452. [Google Scholar] [CrossRef] [Green Version]
- Raez, L.E.; Danenberg, K.; Sumarriva, D.; Usher, J.; Sands, J.; Castrellon, A.; Ferraro, P.; Milillo, A.; Huang, E.; Soon-Shiong, P.; et al. Using cfRNA as a tool to evaluate clinical treatment outcomes in patients with metastatic lung cancers and other tumors. Cancer Drug Resist. 2021, 4, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Park, Y.S.; Choi, J.Y.; Chang, W.J.; Lee, S.; Sung, J.S.; Kim, B.; Lee, S.B.; Lee, S.Y.; Choi, J.; et al. Genetic Characteristics Associated With Drug Resistance in Lung Cancer and Colorectal Cancer Using Whole Exome Sequencing of Cell-Free DNA. Front. Oncol. 2022, 12, 843561. [Google Scholar] [CrossRef]
- Raghav, K.P.S.; Ou, F.-S.; Venook, A.P.; Innocenti, F.; Sun, R.; Lenz, H.-J.; Kopetz, S. Acquired Genomic Alterations on First-Line Chemotherapy With Cetuximab in Advanced Colorectal Cancer: Circulating Tumor DNA Analysis of the CALGB/SWOG-80405 Trial (Alliance). J. Clin. Oncol. 2023, 41, 472–478. [Google Scholar] [CrossRef]
- Wan, J.C.M.; Heider, K.; Gale, D.; Murphy, S.; Fisher, E.; Mouliere, F.; Ruiz-Valdepeñas, A.; Santonja, A.; Morris, J.; Chandrananda, D.; et al. ctDNA Monitoring Using Patient-Specific Sequencing and Integration of Variant Reads. Sci. Transl. Med. 2020, 12, eaaz8084. [Google Scholar] [CrossRef]
- McDonald, B.R.; Contente-Cuomo, T.; Sammut, S.J.; Odenheimer-Bergman, A.; Ernst, B.; Perdigones, N.; Chin, S.-F.; Farooq, M.; Mejia, R.; Cronin, P.; et al. Personalized Circulating Tumor DNA Analysis to Detect Residual Disease After Neoadjuvant Therapy in Breast Cancer. Sci. Transl. Med. 2019, 11, eaax7392. [Google Scholar] [CrossRef]
- Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Swanton, C.; Seiden, M.V. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Ann. Oncol. 2020, 31, 745–759. [Google Scholar] [CrossRef]
- Tsui, N.B.; Ng, E.K.; Lo, Y.D. Stability of endogenous and added RNA in blood specimens, serum, and plasma. Clin. Chem. 2002, 48, 1647–1653. [Google Scholar] [CrossRef] [PubMed]
- Kopreski, M.S.; Benko, F.A.; Gocke, C.D. Circulating RNA as a tumor marker: Detection of 5T4 mRNA in breast and lung cancer patient serum. Ann. N. Y. Acad. Sci. 2001, 945, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Ekine-Afolabi, B.A.; Njan, A.A.; Rotimi, S.O.; Ri, A.; Elbehi, A.M.; Cash, E.; Adeyeye, A. The Impact of Diet on the Involvement of Non-Coding RNAs, Extracellular Vesicles, and Gut Microbiome-Virome in Colorectal Cancer Initiation and Progression. Front. Oncol. Front. Oncol. 2020, 10, 583372. [Google Scholar] [CrossRef]
- Choi, E.-J.; Kim, Y.J. Liquid Biopsy for Early Detection and Therapeutic Monitoring of Hepatocellular Carcinoma. J. Liver Cancer 2022, 22, 103–114. [Google Scholar] [CrossRef]
- Gao, Y.; Wang, H.; Chen, S.-P.; An, R.; Chu, Y.; Li, G.; Wang, Y.; Xie, X.; Zhang, J. Single-Cell N6-Methyladenosine Regulator Patterns Guide Intercellular Communication of Tumor Microenvironment That Contribute to Colorectal Cancer Progression and Immunotherapy. J. Transl. Med. 2022, 20, 197. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Xu, X.; Zhuozhuo, W.; Shan, Q.; Wang, Z.; Wu, Z.; Ding, X.; Huang, W.; Wang, Z. Integrated Single-Cell RNA-seq Analysis Identifies Immune Heterogeneity Associated With KRAS/TP53 Mutation Status and Tumor-Sideness in Colorectal Cancers. Front. Immunol. 2022, 13, 961350. [Google Scholar] [CrossRef] [PubMed]
- Debattista, J.; Grech, L.; Scerri, C.; Grech, G. Copy Number Variations as Determinants of Colorectal Tumor Progression in Liquid Biopsies. Int. J. Mol. Sci. 2023, 24, 1738. [Google Scholar] [CrossRef]
- Boussios, S.; Ozturk, M.A.; Moschetta, M.; Karathanasi, A.; Zakynthinakis-Kyriakou, N.; Katsanos, K.H.; Roukos, D.H.; Pavlidis, N. The Developing Story of Predictive Biomarkers in Colorectal Cancer. J. Pers. Med. 2019, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Albrecht, L.J.; Höwner, A.; Griewank, K.; Lueong, S.S.; Neuhoff, N.v.; Horn, P.A.; Sucker, A.; Paschen, A.; Livingstone, E.; Ugurel, S.; et al. Circulating Cell-free Messenger RNA Enables Non-invasive Pan-tumour Monitoring of Melanoma Therapy Independent of the Mutational Genotype. Clin. Transl. Med. 2022, 12, e1090. [Google Scholar] [CrossRef]
- Cha, D.J.; Franklin, J.L.; Dou, Y.; Liu, Q.; Higginbotham, J.; Beckler, M.D.; Weaver, A.M.; Vickers, K.C.; Prasad, N.; Levy, S.; et al. KRAS-dependent Sorting of miRNA to Exosomes. Elife 2015, 4, e07197. [Google Scholar] [CrossRef]
- Zhang, W.; Hu, X.-X.; Jiang, Z. Small Extracellular Vesicles: Key Forces Mediating the Development and Metastasis of Colorectal Cancer. Cells 2022, 11, 1780. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Kasashima, H.; Fukui, Y.; Tsujio, G.; Yashiro, M.; Maeda, K. The Heterogeneity of Cancer-associated Fibroblast Subpopulations: Their Origins, Biomarkers, and Roles in the Tumor Microenvironment. Cancer Sci. 2022, 114, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, C.C.; Grady, W.M. Colorectal Cancer Molecular Biology Moves Into Clinical Practice. Gut 2010, 60, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Roskams-Hieter, B.; Kim, H.J.; Anur, P.; Wagner, J.T.; Callahan, R.; Spiliotopoulos, E.; Kirschbaum, C.W.; Civitci, F.; Spellman, P.T.; Thompson, R.F.; et al. Plasma cell-free RNA profiling distinguishes cancers from pre-malignant conditions in solid and hematologic malignancies. NPJ Precis. Oncol. 2022, 6, 28. [Google Scholar] [CrossRef]
- Pucciarelli, S.; Rampazzo, E.; Briarava, M.; Maretto, I.; Agostini, M.; Digito, M.; Keppel, S.; Friso, M.L.; Lonardi, S.; De Paoli, A.; et al. Telomere-Specific Reverse Transcriptase (hTERT) and Cell-free RNA in Plasma as Predictors of Pathologic Tumor Response in Rectal Cancer Patients Receiving Neoadjuvant Chemoradiotherapy. Ann. Surg. Oncol. 2012, 19, 3089–3096. [Google Scholar] [CrossRef] [PubMed]
- Dratwa, M.; Wysoczańska, B.; Łacina, P.; Kubik, T.; Bogunia-Kubik, K. TERT—Regulation and Roles in Cancer Formation. Front. Immunol. 2020, 11, 589929. [Google Scholar] [CrossRef]
- Vorperian, S.K.; Moufarrej, M.N.; Jones, R.C.; Karkanias, J.; Krasnow, M.; Pisco, A.O.; Quake, S.R.; Salzman, J.; Yosef, N.; Bulthaup, B.; et al. Cell types of origin of the cell-free transcriptome. Nat. Biotechnol. 2022, 40, 855–861. [Google Scholar] [CrossRef]
- Halvorsen, A.R.; Ragle Aure, M.; Õjlert, Å.K.; Brustugun, O.T.; Solberg, S.; Nebdal, D.; Helland, Å. Identification of microRNAs involved in pathways which characterize the expression subtypes of NSCLC. Mol. Oncol. 2019, 13, 2604–2615. [Google Scholar] [CrossRef] [Green Version]
- Xue, V.W.; Cheung, M.T.; Chan, P.T.; Luk, L.L.Y.; Lee, V.H.; Au, T.C.; Yu, A.C.; Cho, W.C.S.; Tsang, H.F.A.; Chan, A.K.; et al. Non-invasive Potential Circulating mRNA Markers for Colorectal Adenoma Using Targeted Sequencing. Sci. Rep. 2019, 9, 12943. [Google Scholar] [CrossRef] [Green Version]
- Ng, E.K.; Tsui, N.B.; Lam, N.Y.; Chiu, R.W.; Yu, S.C.; Wong, S.C.; Lo, E.S.; Rainer, T.H.; Johnson, P.J.; Lo, Y.M. Presence of filterable and nonfilterable mRNA in the plasma of cancer patients and healthy individuals. Clin. Chem. 2002, 48, 1212–1217. [Google Scholar] [CrossRef]
- Kourou, K.; Exarchos, T.P.; Exarchos, K.P.; Karamouzis, M.V.; Fotiadis, D.I. Machine learning applications in cancer prognosis and prediction. Comput. Struct. Biotechnol. J. 2015, 13, 8–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, A.N.N.; He, Z.; Leung, K.L.; To, C.C.K.; Wong, C.Y.; Wong, S.C.C.; Yoo, J.S.; Chan, C.K.R.; Chan, A.Z.; Lacambra, M.D.; et al. Current Developments of Artificial Intelligence in Digital Pathology and Its Future Clinical Applications in Gastrointestinal Cancers. Cancers 2022, 14, 3780. [Google Scholar] [CrossRef] [PubMed]
- Ou, F.-S.; Michiels, S.; Shyr, Y.; Adjei, A.A.; Oberg, A.L. Biomarker Discovery and Validation: Statistical Considerations. J. Thorac. Oncol. 2021, 16, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Xue, V.W.; Ng, S.S.M.; Tsang, H.F.; Wong, H.T.; Leung, W.W.; Wong, Y.N.; Wong, Y.K.E.; Yu, A.C.S.; Yim, A.K.Y.; Cho, W.C.S.; et al. The non-invasive diagnosis of colorectal cancer via a SOX9-based gene panel. Clin. Exp. Med. 2023. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.; García, V.; García, J.M.; Peña, C.; Domínguez, G.; Díaz, R.; Lorenzo, Y.; Hurtado, A.; Sánchez, A.; Bonilla, F. Circulating Bmi-1 mRNA as a possible prognostic factor for advanced breast cancer patients. Breast Cancer Res. 2007, 9, R55. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Luna, C.; González-Flores, E.; Ortiz, R.; Martínez-González, L.J.; Antúnez-Rodríguez, A.; Expósito-Ruiz, M.; Melguizo, C.; Caba, O.; Prados, J. Circulating PTGS2, JAG1, GUCY2C and PGF mRNA in Peripheral Blood and Serum as Potential Biomarkers for Patients with Metastatic Colon Cancer. J. Clin. Med. 2021, 10, 2248. [Google Scholar] [CrossRef]
- Grosgeorges, M.; Picque Lasorsa, L.; Pastor, B.; Prévostel, C.; Crapez, E.; Sanchez, C.; Frayssinoux, F.; Jarlier, M.; Pezzella, V.; Monard, L.; et al. A straightforward method to quantify circulating mRNAs as biomarkers of colorectal cancer. Sci. Rep. 2023, 13, 2739. [Google Scholar] [CrossRef]
- Nassar, F.J.; Msheik, Z.S.; Itani, M.M.; Helou, R.E.; Hadla, R.; Kreidieh, F.; Bejjany, R.; Mukherji, D.; Shamseddine, A.; Nasr, R.R. Circulating miRNA as biomarkers for colorectal cancer diagnosis and liver metastasis. Diagnostics 2021, 11, 341. [Google Scholar] [CrossRef]
- Fellizar, A.; Refuerzo, V.; Ramos, J.D.; Albano, P.M. Expression of specific microRNAs in tissue and plasma in colorectal cancer. . Pathol. Transl. Med. 2022, 57, 147–157. [Google Scholar] [CrossRef]
- Silva, C.M.S.; Barros-Filho, M.C.; Wong, D.V.T.; Mello, J.B.H.; Nobre, L.M.S.; Wanderley, C.W.S.; Lucetti, L.T.; Muniz, H.A.; Paiva, I.K.D.; Kuasne, H.; et al. Circulating let-7e-5p, miR-106a-5p, miR-28-3p, and miR-542-5p as a Promising microRNA Signature for the Detection of Colorectal Cancer. Cancers 2021, 13, 1493. [Google Scholar] [CrossRef]
- Abo-elela, D.A.; Salem, A.M.; Swellam, M.; Hegazy, M.G. Potential diagnostic role of circulating MiRNAs in colorectal cancer. Int. J. Immunopathol. Pharmacol. 2023, 37, 03946320221144565. [Google Scholar] [CrossRef] [PubMed]
- Poursheikhani, A.; Abbaszadegan, M.R.; Kerachian, M.A. Mechanisms of long non-coding RNA function in colorectal cancer tumorigenesis. Asia-Pac. J. Clin. Oncol. 2021, 17, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Sole, C.; Arnaiz, E.; Manterola, L.; Otaegui, D.; Lawrie, C.H. The circulating transcriptome as a source of cancer liquid biopsy biomarkers. Semin. Cancer Biol. 2019, 58, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Xue, Y.; Cong, H.; Wang, X.; Fan, Z.; Cui, X.; Ju, S. Circulating lncRNA DANCR as a potential auxillary biomarker for the diagnosis and prognostic prediction of colorectal cancer. Biosci. Rep. 2020, 40, BSR20191481. [Google Scholar] [CrossRef] [Green Version]
- Abedini, P.; Fattahi, A.; Agah, S.; Talebi, A.; Beygi, A.H.; Amini, S.M.; Mirzaei, A.; Akbari, A. Expression analysis of circulating plasma long noncoding RNAs in colorectal cancer: The relevance of lncRNAs ATB and CCAT1 as potential clinical hallmarks. J. Cell. Physiol. 2019, 234, 22028–22033. [Google Scholar] [CrossRef]
- Radanova, M.; Mihaylova, G.; Tasinov, O.; Ivanova, D.P.; Stoyanov, G.S.; Nazifova-Tasinova, N.; Manev, R.; Salim, A.; Nikolova, M.; Ivanova, D.G.; et al. New Circulating Circular RNAs with Diagnostic and Prognostic Potential in Advanced Colorectal Cancer. Int. J. Mol. Sci. 2021, 22, 13283. [Google Scholar] [CrossRef]
- Topol, L.; Chen, W.; Song, H.; Day, T.F.; Yang, Y. Sox9 inhibits Wnt signaling by promoting beta-catenin phosphorylation in the nucleus. J. Biol. Chem. 2009, 284, 3323–3333. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Masiero, M.; Banham, A.H.; Harris, A.L. The Notch Ligand Jagged1 as a Target for Anti-Tumor Therapy. Front. Oncol. 2014, 4, 254. [Google Scholar] [CrossRef] [Green Version]
- Johnson, C.R.; Esquela-Kerscher, A.; Stefani, G.; Byrom, M.; Kelnar, K.; Ovcharenko, D.; Wilson, M.R.; Wang, X.; Shelton, J.; Shingara, J.; et al. The let-7 MicroRNA Represses Cell Proliferation Pathways in Human Cells. Cancer Res. 2007, 67, 7713–7722. [Google Scholar] [CrossRef] [Green Version]
- Koga, Y.; Yamazaki, N.; Yamamoto, Y.; Yamamoto, S.; Saito, N.; Kakugawa, Y.; Otake, Y.; Matsumoto, M.; Matsumura, Y. Fecal miR-106a Is a Useful Marker for Colorectal Cancer Patients With False-Negative Results in Immunochemical Fecal Occult Blood Test. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1844–1852. [Google Scholar] [CrossRef] [Green Version]
- Zhou, G.; Han, F.; Shi, Z.; Yu, L.; Li, X.; Yu, C.; Shen, C.; Wan, D.; Zhu, X.; Li, R.; et al. miR-133a-3p Targets SUMO-Specific Protease 1 to Inhibit Cell Proliferation and Cell Cycle Progress in Colorectal Cancer. Oncol. Res. Featur. Preclin. Clin. Cancer Ther. 2018, 26, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Toiyama, Y.; Okugawa, Y.; Fleshman, J.W.; Boland, C.R.; Goel, A. MicroRNAs as Potential Liquid Biopsy Biomarkers in Colorectal Cancer: A Systematic Review. Biochim. Biophys. Acta Rev. Cancer 2018, 1870, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Yamada, A.; Horimatsu, T.; Okugawa, Y.; Nishida, N.; Honjo, H.; Ida, H.; Kou, T.; Kusaka, T.; Sasaki, Y.; Yagi, M.; et al. Serum miR-21, miR-29a, and miR-125b Are Promising Biomarkers for the Early Detection of Colorectal Neoplasia. Clin. Cancer Res. 2015, 21, 4234–4242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eliason, S.; Hong, L.; Sweat, Y.; Chalkley, C.; Cao, H.; Liu, Q.; Qi, H.; Xu, H.; Zhan, F.; Amendt, B.A. Extracellular Vesicle Expansion of PMIS-miR-210 Expression Inhibits Colorectal Tumour Growth via Apoptosis and an XIST/NME1 Regulatory Mechanism. Clin. Transl. Med. 2022, 12, e1037. [Google Scholar] [CrossRef]
- Arun, G.; Diermeier, S.D.; Spector, D.L. Therapeutic Targeting of Long Non-Coding RNAs in Cancer. Trends Mol. Med. 2018, 24, 257–277. [Google Scholar] [CrossRef]
- Kang, E.; Jung, S.C.; Nam, S.K.; Park, Y.; Seo, S.H.; Park, K.U.; Oh, H.-K.; Kim, D.-W.; Kang, S.-B.; Lee, H.S. Tissue miR-200c-3p and circulating miR-1290 as potential prognostic biomarkers for colorectal cancer. Sci. Rep. 2022, 12, 2292. [Google Scholar] [CrossRef]
- Pu, X.-x.; Huang, G.-l.; Guo, H.-q.; Guo, C.-c.; Li, H.; Ye, S.; Ling, S.; Jiang, L.; Tian, Y.; Lin, T.-y. Circulating miR-221 directly amplified from plasma is a potential diagnostic and prognostic marker of colorectal cancer and is correlated with p53 expression. J. Gastroenterol. Hepatol. 2010, 25, 1674–1680. [Google Scholar] [CrossRef]
- Pun, J.C.S.; Chan, J.Y.J.; Chun, B.K.M.; Ng, K.W.; Tsui, S.Y.K.; Wan, T.M.H.; Lo, O.; Poon, J.T.C.; Ng, L.; Pang, R. Plasma Bmi1 mRNA as a potential prognostic biomarker for distant metastasis in colorectal cancer patients. Mol. Clin. Oncol. 2014, 2, 817–820. [Google Scholar] [CrossRef] [Green Version]
- He, W.; Wang, B.; He, J.; Zhao, Y.; Zhao, W. SSR4 as a prognostic biomarker and related with immune infiltration cells in colon adenocarcinoma. Expert Rev. Mol. Diagn. 2022, 22, 223–231. [Google Scholar] [CrossRef]
- Cui, C.; Zhang, R.; Gu, F.; Pei, Y.; Sun, L.; Huang, Y.; Niu, G.; Li, J. Plasma CXCL3 Levels Are Associated with Tumor Progression and an Unfavorable Colorectal Cancer Prognosis. J. Immunol. Res. 2022, 2022, 1336509. [Google Scholar] [CrossRef]
- Kudelova, E.; Holubekova, V.; Grendar, M.; Kolkova, Z.; Samec, M.; Vanova, B.; Mikolajcik, P.; Smolar, M.; Kudela, E.; Laca, L.; et al. Circulating miRNA expression over the course of colorectal cancer treatment. Oncol. Lett. 2022, 23, 18. [Google Scholar] [CrossRef]
- Hao, Y.-J.; Yang, C.-Y.; Chen, M.-H.; Chang, L.-W.; Lin, C.-P.; Lo, L.-C.; Huang, S.-C.; Lyu, Y.-Y.; Jiang, J.-K.; Tseng, F.-G. Potential Values of Circulating microRNA-21 to Predict Early Recurrence in Patients with Colorectal Cancer after Treatments. J. Clin. Med. 2022, 11, 2400. [Google Scholar] [CrossRef] [PubMed]
- Angerilli, V.; Galuppini, F.; Businello, G.; Dal Santo, L.; Savarino, E.; Realdon, S.; Guzzardo, V.; Nicolè, L.; Lazzarin, V.; Lonardi, S. MicroRNAs as Predictive Biomarkers of Resistance to Targeted Therapies in Gastrointestinal Tumors. Biomedicines 2021, 9, 318. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Xia, H.-W.; Ge, X.-J.; Zhang, Y.-C.; Tang, Q.-L.; Bi, F. Serum miR-19a predicts resistance to FOLFOX chemotherapy in advanced colorectal cancer cases. Asian Pac. J. Cancer Prev. 2013, 14, 7421–7426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kjersem, J.; Ikdahl, T.; Lingjaerde, O.; Guren, T.; Tveit, K.; Kure, E. Plasma microRNAs predicting clinical outcome in metastatic colorectal cancer patients receiving first-line oxaliplatin-based treatment. Mol. Oncol. 2014, 8, 59–67. [Google Scholar] [CrossRef]
- Hu, J.; Cai, G.; Xu, Y.; Cai, S. The Plasma microRNA miR-1914* and-1915 Suppresses Chemoresistant in Colorectal Cancer Patients by Down-regulating NFIX. Curr. Mol. Med. 2016, 16, 70–82. [Google Scholar] [CrossRef]
- Ge, T.; Xiang, P.; Mao, H.; Tang, S.; Zhou, J.; Zhang, Y. Inhibition of miR-96 enhances the sensitivity of colorectal cancer cells to oxaliplatin by targeting TPM1. Exp. Therap. Med. 2020, 20, 2134–2140. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, K.; Bi, M.; Jiao, X.; Zhang, D.; Dong, Q. Circulating microRNA expressions in colorectal cancer as predictors of response to chemotherapy. Anticancer Drugs 2014, 25, 346–352. [Google Scholar] [CrossRef]
- Ye, D.; Liu, H.; Zhao, G.; Chen, A.; Jiang, Y.; Hu, Y.; Liu, D.; Xie, N.; Liang, W.; Chen, X.; et al. LncGMDS-AS1 promotes the tumorigenesis of colorectal cancer through HuR-STAT3/Wnt axis. Cell Death Dis. 2023, 14, 165. [Google Scholar] [CrossRef]
- Ghanbari, R.; Mosakhani, N.; Sarhadi, V.K.; Armengol, G.; Nouraee, N.; Mohammadkhani, A.; Khorrami, S.; Arefian, E.; Paryan, M.; Malekzadeh, R. Simultaneous underexpression of let-7a-5p and let-7f-5p microRNAs in plasma and stool samples from early stage colorectal carcinoma: Supplementary issue: Biomarkers for colon cancer. Biomark. Cancer 2015, 7, BIC-S25252. [Google Scholar] [CrossRef] [Green Version]
- Chirshev, E.; Oberg, K.C.; Ioffe, Y.J.; Unternaehrer, J.J. Let-7 as biomarker, prognostic indicator, and therapy for precision medicine in cancer. Clin. Transl. Med. 2019, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Igarashi, H.; Kurihara, H.; Mitsuhashi, K.; Ito, M.; Okuda, H.; Kanno, S.; Naito, T.; Yoshii, S.; Takahashi, H.; Kusumi, T. Association of microRNA-31-5p with clinical efficacy of anti-EGFR therapy in patients with metastatic colorectal cancer. Ann. Surg. Oncol. 2015, 22, 2640–2648. [Google Scholar] [CrossRef]
- Peng, X.; Wang, J.; Zhang, C.; Liu, K.; Zhao, L.; Chen, X.; Huang, G.; Lai, Y. A three-miRNA panel in serum as a noninvasive biomarker for colorectal cancer detection. Int. J. Biol. Markers 2020, 35, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Schou, J.V.; Rossi, S.; Jensen, B.V.; Nielsen, D.L.; Pfeiffer, P.; Høgdall, E.; Yilmaz, M.; Tejpar, S.; Delorenzi, M.; Kruhøffer, M.; et al. miR-345 in metastatic colorectal cancer: A non-invasive biomarker for clinical outcome in non-KRAS mutant patients treated with 3rd line cetuximab and irinotecan. PLoS ONE 2014, 9, e99886. [Google Scholar] [CrossRef] [PubMed]
- Le, A.P.H.; Huong, H.T.T. The Role of Cell-Free RNA in Clinical Diagnosis and Evaluation of Cell-Free RNA Extraction Methods. In Proceedings of the 8th International Conference on the Development of Biomedical Engineering in Vietnam, Ho Chi Minh, Vietnam, 20–22 July 2020; Springer International Publishing: Cham, Switzerland; pp. 637–656. [Google Scholar]
- Kirschner, M.; Edelman, J.J.; Kao, S.; Vallely, M.; Van Zandwijk, N.; Reid, G. The Impact of Hemolysis on Cell-Free microRNA Biomarkers. Front. Genet. 2013, 4, 94. [Google Scholar] [CrossRef] [Green Version]
- Van Paemel, R.; De Koker, A.; Caggiano, C.; Morlion, A.; Mestdagh, P.; De Wilde, B.; Vandesompele, J.; De Preter, K. Genome-wide study of the effect of blood collection tubes on the cell-free DNA methylome. Epigenetics 2021, 16, 797–807. [Google Scholar] [CrossRef]
- Fernando, M.R.; Norton, S.E.; Luna, K.K.; Lechner, J.M.; Qin, J. Stabilization of cell-free RNA in blood samples using a new collection device. Clin. Biochem. 2012, 45, 1497–1502. [Google Scholar] [CrossRef] [Green Version]
- Toro, P.V.; Erlanger, B.; Beaver, J.A.; Cochran, R.L.; VanDenBerg, D.A.; Yakim, E.; Cravero, K.; Chu, D.; Zabransky, D.J.; Wong, H.Y.; et al. Comparison of cell stabilizing blood collection tubes for circulating plasma tumor DNA. Clin. Biochem. 2015, 48, 993–998. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.C.; Ma, B.B.; Lai, P.B.; Ng, S.S.; Lee, J.F.; Hui, E.P.; Lam, M.Y.; Chan, C.M.; Chan, A.T. The effect of centrifugation on circulating mRNA quantitation opens up a new scenario in expression profiling from patients with metastatic colorectal cancer. Clin. Biochem. 2007, 40, 1277–1284. [Google Scholar] [CrossRef]
- Xue, V.W.; Ng, S.S.M.; Leung, W.W.; Ma, B.B.Y.; Cho, W.C.S.; Au, T.C.C.; Yu, A.C.S.; Tsang, H.F.A.; Wong, S.C.C. The Effect of Centrifugal Force in Quantification of Colorectal Cancer-Related mRNA in Plasma Using Targeted Sequencing. Front. Genet. 2018, 9, 165. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.C.; Lo, E.S.; Cheung, M.T. An optimised protocol for the extraction of non-viral mRNA from human plasma frozen for three years. J. Clin. Pathol. 2004, 57, 766–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, K.; de Silva, K.; Purdie, A.C.; Plain, K.M. Comparison of methods for miRNA isolation and quantification from ovine plasma. Sci. Rep. 2020, 10, 825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.K.; Yeo, J.; Kim, B.; Ha, M.; Kim, V.N. Short structured RNAs with low GC content are selectively lost during extraction from a small number of cells. Mol. Cell 2012, 46, 893–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Mauro, M.; Williams, Z. Comparison of plasma extracellular RNA isolation kits reveals kit-dependent biases. BioTechniques 2015, 59, 13–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulstaert, E.; Morlion, A.; Avila Cobos, F.; Verniers, K.; Nuytens, J.; Vanden Eynde, E.; Yigit, N.; Anckaert, J.; Geerts, A.; Hindryckx, P.; et al. Charting Extracellular Transcriptomes in The Human Biofluid RNA Atlas. Cell Rep. 2020, 33, 108552. [Google Scholar] [CrossRef]
- Buschmann, D.; Haberberger, A.; Kirchner, B.; Spornraft, M.; Riedmaier, I.; Schelling, G.; Pfaffl, M.W. Toward reliable biomarker signatures in the age of liquid biopsies—How to standardize the small RNA-Seq workflow. Nucleic Acids Res. 2016, 44, 5995–6018. [Google Scholar] [CrossRef]
- Ozsolak, F.; Milos, P.M. RNA sequencing: Advances, challenges and opportunities. Nat. Rev. Genet. 2011, 12, 87–98. [Google Scholar] [CrossRef]
- Holcar, M.; Kandušer, M.; Lenassi, M. Blood Nanoparticles—Influence on Extracellular Vesicle Isolation and Characterization. Front. Pharmacol. 2021, 12, 773844. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, J.P.; Saha, I.; Lancucki, A.; Ghosh, N.; Wlasnowolski, M.; Bokota, G.; Dey, A.; Lipinski, P.; Plewczynski, D. Identification of miRNA Biomarkers for Diverse Cancer Types Using Statistical Learning Methods at the Whole-Genome Scale. Front. Genet. 2020, 11, 982. [Google Scholar] [CrossRef]
- Wolfien, M.; Rimmbach, C.; Schmitz, U.; Jung, J.J.; Krebs, S.; Steinhoff, G.; David, R.; Wolkenhauer, O. TRAPLINE: A standardized and automated pipeline for RNA sequencing data analysis, evaluation and annotation. BMC Bioinform. 2016, 17, 21. [Google Scholar] [CrossRef] [Green Version]
- Tieng, F.Y.F.; Baharudin, R.; Abu, N.; Mohd Yunos, R.-I.; Lee, L.-H.; Ab Mutalib, N.-S. Single Cell Transcriptome in Colorectal Cancer—Current Updates on Its Application in Metastasis, Chemoresistance and the Roles of Circulating Tumor Cells. Front. Pharmacol. 2020, 11, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, P.; Lo, Y.M.D. Enhanced cancer detection from cell-free DNA. Nat. Biotechnol. 2022, 40, 473–474. [Google Scholar] [CrossRef]
- Ding, S.C.; Lo, Y.M.D. Cell-Free DNA Fragmentomics in Liquid Biopsy. Diagnostics 2022, 12, 978. [Google Scholar] [CrossRef] [PubMed]
- Lampronti, I.; Allegretti, M.; Gasparello, J.; Giacomini, P.; Spandidos, D.A.; Spoto, G.; Gambari, R. Liquid Biopsy and PCR-free Ultrasensitive Detection Systems in Oncology (Review). Int. J. Oncol. 2018, 53, 1395–1434. [Google Scholar] [CrossRef]

| Year | Biomarker | Biomarker Type | Samples | Up-/Downregulated in CRC Patients | Value | Technology | Reference |
|---|---|---|---|---|---|---|---|
| 2023 | HPGD, TDP2, PACS1 | mRNA | 8 plasma pre-surgery CRC and post-surgery CRC; 8 tumor tissue and adjacent tumor tissue | Down Up | Prognosis | Transcriptome Seq | [24] |
| 2021 | SSR4 | mRNA | Up | Prognosis | Data Mining | [109] | |
| 2022 | CXCL3 | mRNA | 228 CRC vs. 216 control | Up | Diagnosis and Prognosis | RT-qPCR | [110] |
| 2014 | Bm1 | mRNA | 45 CRC | Down | Prognosis | RT-qPCR | [108] |
| 2022 | miR-1290 | miRNA | Up | Prognosis | ddPCR | [106] | |
| 2022 | miR-155-5p, miR-21-5p, miR-191-5p miR-16-5p | miRNA | 110 plasma CRC | Up Down | Prognosis | RT-qPCR | [111] |
| 2022 | miR-21 | miRNA | 113 CRC | Up | Prognosis | RT-qPCR | [112] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kan, C.-M.; Pei, X.M.; Yeung, M.H.Y.; Jin, N.; Ng, S.S.M.; Tsang, H.F.; Cho, W.C.S.; Yim, A.K.-Y.; Yu, A.C.-S.; Wong, S.C.C. Exploring the Role of Circulating Cell-Free RNA in the Development of Colorectal Cancer. Int. J. Mol. Sci. 2023, 24, 11026. https://doi.org/10.3390/ijms241311026
Kan C-M, Pei XM, Yeung MHY, Jin N, Ng SSM, Tsang HF, Cho WCS, Yim AK-Y, Yu AC-S, Wong SCC. Exploring the Role of Circulating Cell-Free RNA in the Development of Colorectal Cancer. International Journal of Molecular Sciences. 2023; 24(13):11026. https://doi.org/10.3390/ijms241311026
Chicago/Turabian StyleKan, Chau-Ming, Xiao Meng Pei, Martin Ho Yin Yeung, Nana Jin, Simon Siu Man Ng, Hin Fung Tsang, William Chi Shing Cho, Aldrin Kay-Yuen Yim, Allen Chi-Shing Yu, and Sze Chuen Cesar Wong. 2023. "Exploring the Role of Circulating Cell-Free RNA in the Development of Colorectal Cancer" International Journal of Molecular Sciences 24, no. 13: 11026. https://doi.org/10.3390/ijms241311026