1. Introduction
Although poverty affects all groups, it disproportionately affects those whose access to coping resources is most limited, such as rural households [
1]. It is not limited to any single geographical region, income level, or age group [
2]. Poverty is higher in rural areas than urban areas, and higher in non-metropolitan areas than in metropolitan areas. According to the Global Donor Platform for Rural Development, rural poverty must be tackled in order to meet the Millennium Development Goal because “three-quarters of the poor live in rural areas of developing countries.” [
3]. Rural people in general were most affected by chronic poverty, and many rural households in emerging nations experience poverty even during prosperous years. Rural households are more likely to experience physical and psychological health issues due to poverty. Poverty has an adverse effect on people’s access to commodities and the quality of services, which has a bad effect on their health, according to the material pathway. In the psychological pathway, psychological stress (depression or pressure) may lead to poor consequences on mental health or physical health through behavior (smoking or alcohol abuse). Since the 1950s, sociological health research has routinely employed rural households’ assessments of various health outcomes for themselves as a typical indicator of health [
4]. In China, as in the rest of the world, rural households have borne the brunt of poverty’s effects [
5]. There are still large numbers of poor rural households in China and suffering from illness is the biggest cause of individual or temporary poverty in rural China today, while a lack of natural endowments, poor geography, and a fragile ecology are the main drivers of persistent poverty [
6]. The term “poor families” refers to rural households classified as such by the Chinese government’s card-building procedure from 2020. In 2011, China’s rural poverty income benchmark was CNY 2300, and in 2020, it was CNY 4000. In 2020, absolute poverty was defined as having a net annual income per capita of less than CNY 627, while relative poverty was defined as having a net annual income per capita of CNY 865.
Although poverty was found everywhere and among all groups in China, it disproportionately puts certain groups at greater risk for well-being. After the implementation of large-scale poverty alleviation [
7] and development, such phenomena have been alleviated and great achievements have been made [
8]. From 1986 to 1993, China carried out large-scale developmental poverty alleviation, such as establishing special poverty alleviation work units and allocating special funds. During the 1994–2000 poverty alleviation period, the “8–7” poverty alleviation program was implemented, with the goal of solving the basic food and clothing problem of 80,000 rural poor people in about seven years; since the beginning of the current century, China has issued two new rural poverty alleviation and development programs; and in 2013, Chinese President Xi Jinping proposed the Targeted Poverty Alleviation (TPA) strategy [
9]. The statistics from
Fifth Series of Reports on the Achievements of Economic and
Social Development in the 40 Years of Reform and Opening Up showed that the result was a dramatic decline in poverty rates, from 97.5% in 1978 to 0.6% in 2019. In 2020, the incidence of poverty was 0%. Currently, 98.99 million rural Chinese people who were living in poverty have been helped out of it. The complete victory in the fight against poverty marks the elimination of absolute poverty [
10] based on income and the beginning of the transition to multidimensional poverty [
11]. Absolute poverty is also called subsistence poverty. It is the inability of individuals and families to maintain their basic subsistence needs by relying on the income they earn from their labor and other legitimate income under certain social production and lifestyle patterns. As indicated, absolute poverty has been eliminated in China; there is no need to indulge on it. We focus on the concept of multidimensional poverty which somehow goes beyond the definitions of absolute and relative poverty and is a much more appropriate instrument to holistically measure poverty.
Contrary to the widespread use of absolute poverty, there is no single global standard for measuring relative poverty. When poverty was first defined, it meant not having enough money to cover the bare necessities of existence [
12]. However, as socio-economic development has progressed, academics have continued to study poverty in new ways and comprehend it from perspectives other than just income [
13]. Absolute poverty refers to subsistence poverty, which focuses on the basic survival and livelihood of individuals. Relative poverty refers to developmental poverty, which focuses on an individual’s ability to develop sustainably. The relative poverty theory proposed by Townsend (1979) [
14] is a deepening and sublimation of the absolute poverty theory, which shifts scholars’ focus on poverty research from the basic survival needs of human beings to the inequality of income distribution and social deprivation, and puts more emphasis on all people sharing the benefits of economic and social development. Therefore, the understanding and assessment of poverty should encompass factors connected to an individual’s total development, such as health care, education, and standard of living, in addition to the single “income” dimension [
15]. The “dual cut-off method” is the most commonly used method to create multidimensional poverty indexes [
16]. By calculating the poverty line for each dimension, this method establishes an individual’s status as being below the poverty line in that dimension. Individuals who fall below the specified threshold for poverty in any one or more of the dimensions are then considered to be poor. This paper examines multidimensional poverty.
Poverty increases the risk of low health through poor environment, nutrition, and risky behaviors such as smoking, alcohol, and other things [
17]. However, the relationship between poverty and rural households’ self-rated health is complicated by the vicious circle of poverty, unhealthy, and low income [
18]. Self-rated health is a valid proxy for an individual’s health status because it is a subjective metric that depends on an individual’s nuanced appraisal of his or her own entirety [
17,
19,
20]. Poverty hinders the improvement of rural household’ self-rated health; for example, it has a negative impact on the health level [
21].
In addition, according to previous research, social relationships, networks, trust, and conventions are thought to form a relatively stable and institutionalized network known as social capital, which can improve social efficiency through cooperation. Social capital is a type of resource that helps members of the social structure live more comfortably or obtain financial advantages [
22]. As for the rural households, social capital was considered to plays a mediating role between poverty and health [
23], which can effectively alleviate the low health level caused by poverty [
4]. First, social capital raises the human capital level and reward of rural households by increasing the probability of employment and income levels, health care expenditures, socioeconomic status, and borrowing capacity, thus reducing the probability of falling into poverty and avoiding a return to poverty [
24]. Second, as a (semi-)acquaintance society, social capital plays a prominent influence in rural China, which helps rural households access health resources and has a significant positive effect on the health level of out-of-poverty households [
25]. Therefore, social capital can reduce the occurrence of poverty and fundamentally avoid the low health level caused by poverty [
26]. In addition, social capital can form a social environment of beneficial social interactions and mutual trust, which helps to obtain health information and effectively reduce health risks, thus affecting the level of health positively.
The impact of family care on mental health is a crucial area of current research. The more positive the family caregiving behavior for the care recipient, the higher the health index [
27]. Meanwhile, family care can improve the physical and mental health, life happiness, and sense of accomplishment of caregivers [
28]. Through reciprocal interactions, family care for the elderly and the children can result in a two-way exchange of resources, promoting the family’s social capital, the physical and emotional health of the individuals being cared for [
4]. According to the
Role Enhancement theory [
29], providing care for a family increases social and familial support, emotional fulfillment, and caregivers’ ability to lead healthier lifestyles [
30]. Research has also shown that providing care for family members might be detrimental to their physical and mental well-being [
31]. Given the disparities between urban and rural areas, urban caregivers have better physical and mental health than rural caregivers [
32]. According to the
Role Strain idea [
33], family caregivers may experience stress as a result of their duties, and high-intensity family care may take a toll on the health of caregivers [
34]. This study broadens the definition of family care to include both childcare and elder care, in contrast to prior studies [
24]. The care given by rural households to school-age children under the age of 16 is referred to as “child care,” while the care given to seniors over the age of 60 who need assistive technology to do daily tasks is referred to as “elder care.” Family care may operate as a moderator, even if the current findings have shown how social capital affects rural household health.
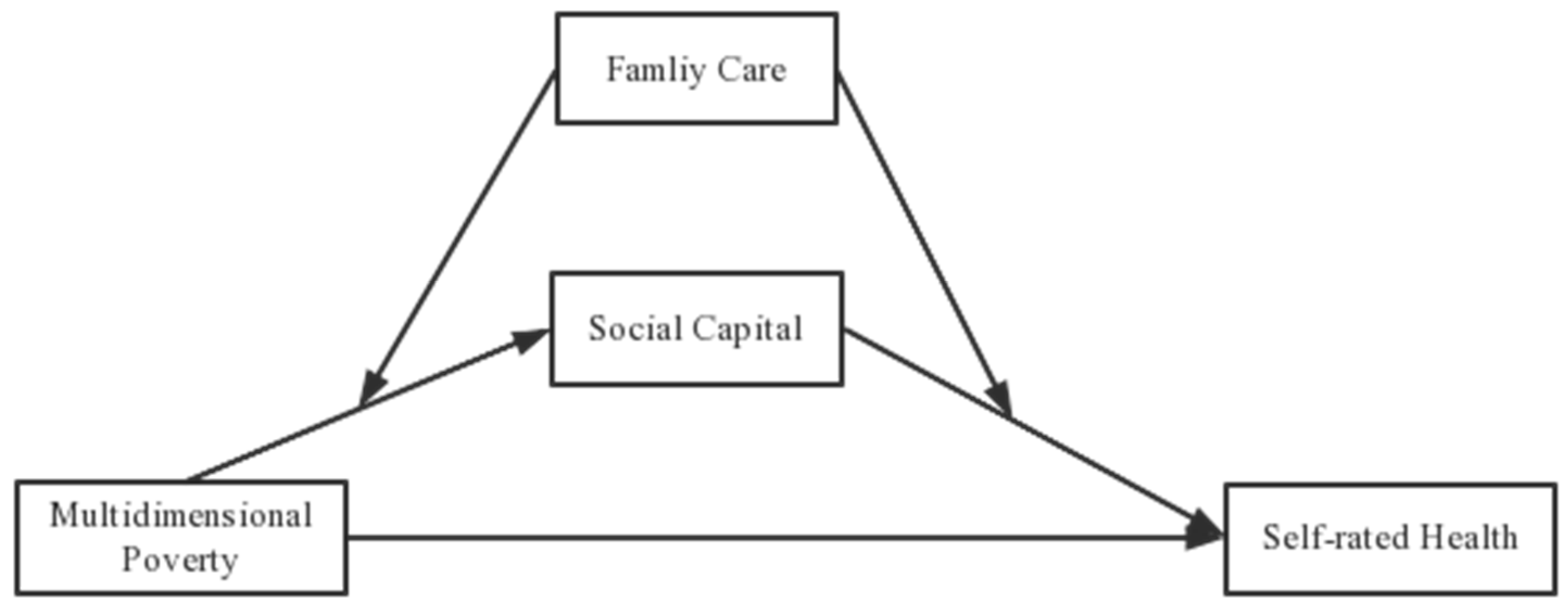
Thus, the objective of the research is to analyze the impact of multidimensional poverty on rural households’ self-rated health through theoretical modeling of rural households’ self-rated health. Since the independent variable in this paper is multidimensional poverty, it determines whether a farmer is in developmental poverty from all aspects of his or her life. The social capital is also the developmental capital formed from the trust, participation, support, and network established between the rural household and the outside world, which can influence the level of multidimensional poverty. Family care is a very common behavior in rural households, and through the care of the elderly and children can achieve a resource swap that affects the social capital of the caregiver by providing resources or taking up the opportunity cost of the caregiver. Meanwhile this study empirically tests the conclusions obtained from the theoretical model based on the survey data of 382 rural households lifted out of poverty in Jiangxi Province, China, in 2020. Our findings have important practical implications for the health and sustainability of rural households.
Previous literature discussing globally relevant documents on research topics has focused on the factors that influence multidimensional poverty. Battiston et al. (2013) [
35] have analyzed multidimensional poverty indices for six Latin American countries, including Argentina, Brazil, Chile, and so on, over the period 1992–2006 and found that a lack of adequate sanitation and education for household heads were the biggest factors in overall multidimensional poverty. Pinilla-Roncancio et al. (2020) [
36] compared the multidimensional poverty levels of people with and without disabilities in Guatemala, Cameroon, and India, with health-related indicators having the greatest impact on the multidimensional poverty levels of people with disabilities. Fransman and Yu (2019) [
37] have calculated an annual multidimensional poverty index for South Africa, which shows that Africans experience more than 95% of multidimensional poverty and that unemployment, years of schooling, and disability are the three indicators that cause the most poverty. Martinez and Perales (2017) [
38] have examined how year-to-year changes in multidimensional poverty in Australia in recent years have been driven primarily by fluctuations in social support, health, and material resources, suggesting that the effectiveness and efficiency of poverty reduction policies should be improved by focusing on improving disadvantage in the areas of health and material resources. Based on different measurement methods, Padda and Hameed (2018) [
39] estimated the level of multidimensional deprivation and poverty in rural Pakistan through socio-economic scores and found that 44% of rural households endured sustainable deprivation and well-being issues, particularly in the areas of health, stunting, the standard of living, and so on. Based on the Colombian Multidimensional Poverty Index (CMPI), Angulo et al. (2016) [
40] have concluded that multidimensional poverty in rural Colombia decreased between 1997 and 2010, but imbalances remain. It can be seen that multidimensional poverty has received widespread attention at the international level. In practice, the European Union (EU) has adopted a multidimensional poverty and social exclusion target for 2020, justified by the fact that the calculation of a multidimensional poverty index is an effective way of communicating in a political context and a necessary tool for monitoring the situation in different countries [
41].
Compared with the existing literature, the possible marginal contributions of this paper are mainly manifested in the following basic aspects. First, in the context of absolute poverty alleviation, we use the MPI (Multidimensional Poverty Index) [
42] mentioned in the Sustainability Development Goals (SDGs) guidelines to select multidimensional indicators that can cover all aspects of life to judge rural households who are in relative poverty [
43]. To ascertain if rural households are multidimensionally poor, the income indicator is also used as a separate dimension. This study develops a comprehensive income-based multidimensional poverty identification and assessment method. Second, previous research has looked at the impact of social capital and multidimensional poverty on rural households’ health separately, with the majority of the literature focusing on just one aspect of social capital. In order to provide a more accurate and robust estimate of rural households’ social capital, the impact of social capital is examined in this study by evaluating the entire social capital index of farmers across four dimensions: social networks, social trust, social participation, and social support. We investigate the impact of multidimensional poverty on rural households’ self-rated health, and further investigate the mitigating or facilitating effect of entropy-valued social capital on the self-rated health of rural households affected by multidimensional poverty based on Bootstrap [
44], which can be reliably obtained by running Bootstrap independent sampling 5000 times. Third, we introduce family care into the empirical model and examine the moderating effect of family care on the mediating effect based on Bootstrap. Rural households regularly engage in family care, but less research has been conducted on the factors affecting the health of rural households in light of this widespread life behavior. We investigate whether multidimensional poverty has an impact on rural households’ health at the micro level and study its mechanisms of influence to determine whether low-intensity family care and high-intensity social capital can be a significant opportunity to improve the health of rural households. Thus, our study on multidimensional poverty and rural household’ health has both significant theoretical and real-world implications.
The rest of the paper is organized as follows.
Section 2 presents the theoretical hypothesis of this paper based on relevant theories and existing studies.
Section 3 introduces the data sources and the basic setup of the model and analyzes the moderating or facilitating role of social capital in the impact of multidimensional poverty on rural households’ self-rated health and the moderating role of family care in the framework of this theoretical model.
Section 4 conducts an empirical analysis to verify the conclusions obtained from the theoretical model based on the survey data from Jiangxi Province, China. Finally, we draw discussions and conclusions in
Section 5.
5. Discussion and Conclusions
In the past, academic research and hot research topics have concentrated on alleviating and reducing income poverty as one of the major barriers to economic development in rural China. Though few studies have concentrated on the effects of relative poverty and multidimensional poverty on rural households’ health in the “post-poverty era,” the majority of the literature has addressed poverty and the impact of it on rural households’ lives from the perspective of income. In order to quantify the impact of multidimensional poverty on health and examine its mechanism, we used a sample of 382 out-of-poverty households in Jiangxi Province in 2020, with social capital as a mediating variable and family care as a moderating variable.
The contributions of this study were primarily reflected in the following three dimensions. First, in contrast to the majority of earlier studies, we looked at the multidimensional poverty effect from a variety of angles when choosing the poverty indicators for rural households. The income indicator was added and utilized as a separate dimension in addition to the three dimensions of health, education, and living standard in the MPI. While multidimensional relative poverty captures the sustainability of rural households, absolute poverty, assessed by income, merely shows the bare necessities of survival for rural households. In the sample area, rural poor households have been raised out of poverty on the basis of income alone, but according to the data from this study, 35% of these households have been lifted out of poverty but are still at risk of falling back into it on a multidimensional basis. We also measured the total social capital index of rural households. The entropy value of four indicators—social networks, social trust, social participation, and social support—was calculated to increase the variable’s representativeness when it came to the selection of the social capital variable for rural households. We took into account children under the age of 16 and elderly above the age of 60 who need assistive technology to do daily tasks when determining the degree of family care for rural households.
The self-rated health of rural households was typically shown to be very negatively impacted by multidimensional poverty. Poor rural households may be more susceptible to exposure to harmful physical health factors due to a lack of living resources, health awareness, and constrained income levels. As a result, the self-rated health of the rural households may be impacted. The results support both hypothesis 1 and earlier research, which is consistent with previous findings [
17]. Due to a mix of chronic economic and life stress, a lack of resources, and subjective assessments of relative poverty, people suffer from reduced health.
The article indicated that multidimensional poverty of rural households had a positive impact on the self-rated health of the rural households primarily through social capital, which was employed as a mediating variable. That is, the negative impact of multidimensional poverty on the level of health in rural households was positively tempered by social capital. Social capital increases resource endowment and social engagement, this reduces the impact of multidimensional poverty on the self-rated health of rural households.
However, this study’s results differ from others [
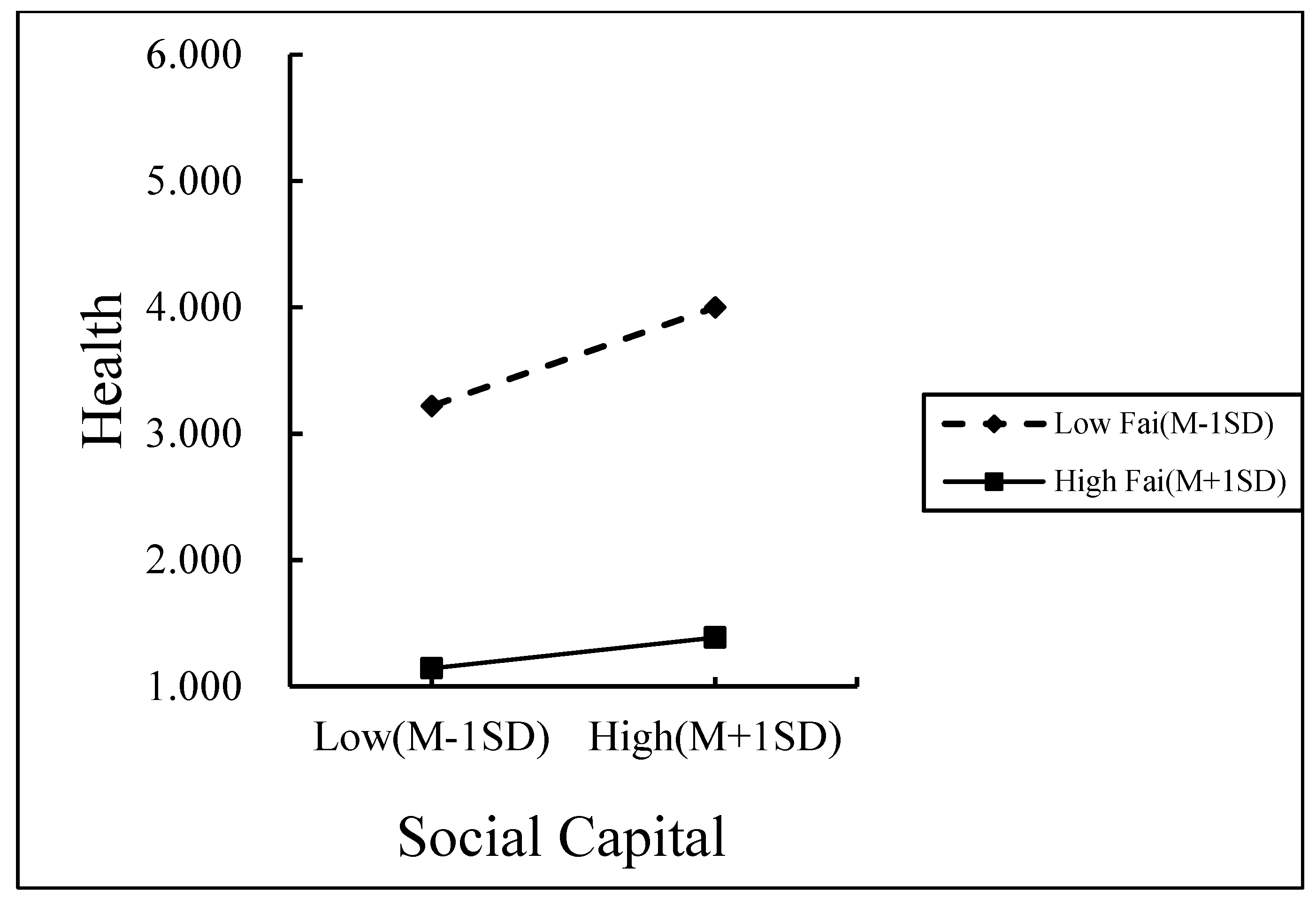
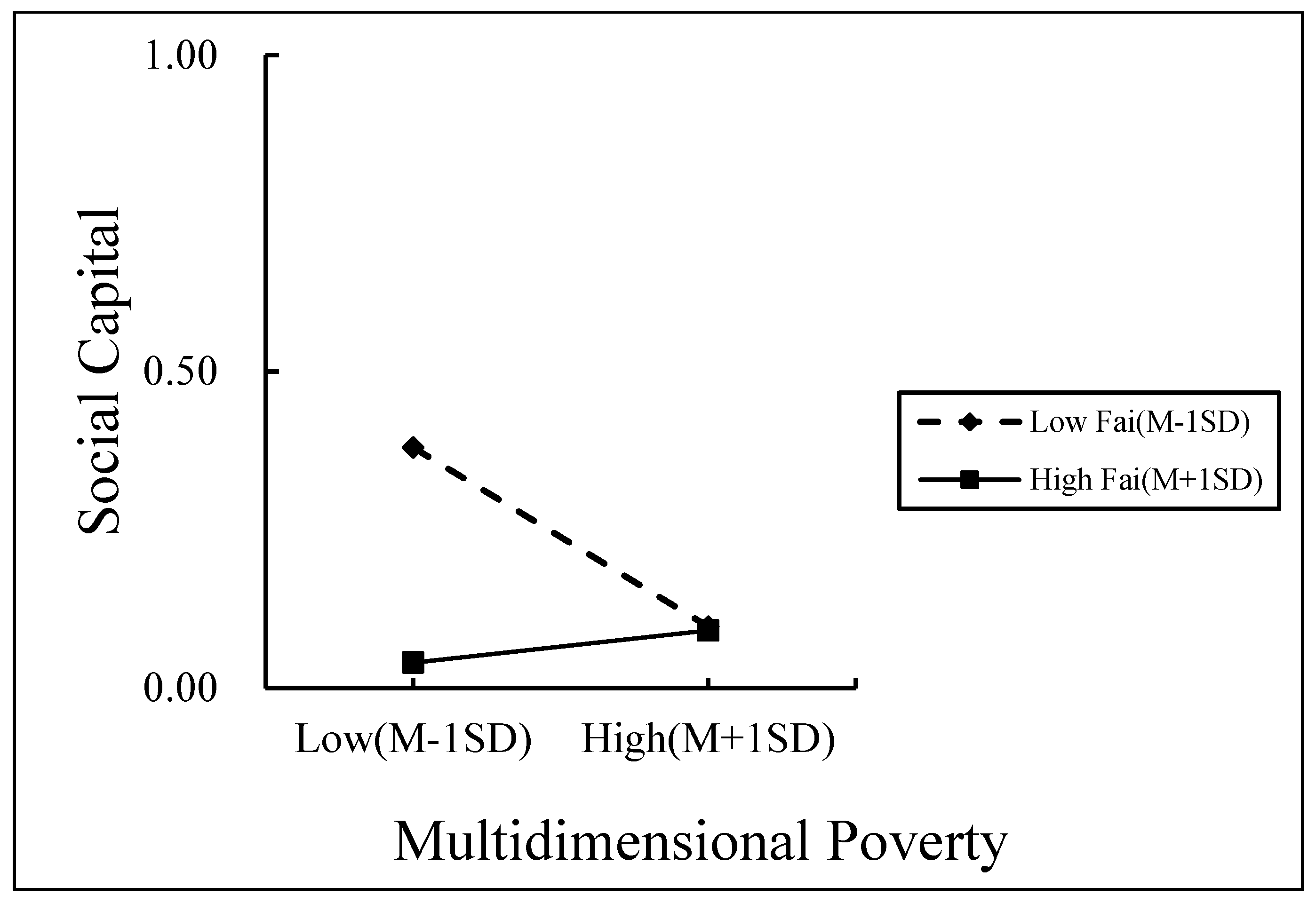
54], which do not consider the burden of non-labor resources in rural households, that is the level of family care in rural households. High-intensity family care implies that caregivers expend more energy and bear more opportunity costs (such as time expenses and leisure costs), which has an impact on rural households’ capacity to build up social capital. In other words, the role of social capital as a mediating factor in the impact of multidimensional poverty on the self-rated health of rural households is moderated by family care as a moderating variable. This affected the level of social capital of the rural households. The research showed that family care decreased the self-rated health of rural households and primarily evaluated that multidimensional poverty’s detrimental impact on rural households’ social capital increased with lower levels of family care. The impact of multidimensional poverty on the self-rated health of rural households becomes increasingly important as the level of family care rises. Social capital is less likely to affect the health of rural households by lowering their level of multidimensional poverty and subsequently their level of health as the amount of family care grows.
Second, to address how multidimensional poverty affected the self-rated health of rural households, our econometric research was based on a survey data and a moderated mediation model. The survey data allowed us to more effectively evaluated the question of the objectivity of indicators and, as a result, came to more trustworthy findings because both multidimensional poverty and social capital were measured from various aspects. Our research had shown that the likelihood of social capital attenuating the negative effects of multidimensional poverty on rural households’ self-rated health decreased as the burden of family care increased. In Jiangxi province of China, policy priority should be to increase the social capital of rural households [
87].
Third, multiple effects of the same issue may be seen in the self-rated health of rural households. It has been found that social capital partially mediates the effect of multidimensional poverty on the levels of self-rated health in rural households [
54]. However, we tested the mediating role of social capital in the effect of multidimensional poverty on the self-rated health of the rural households by examining the post-entropy value of social capital and found that social capital played a fully mediating role. Looking at multiple aspects of the household’s life helps us assess the level of social capital of a rural household as well as establish whether the household is experiencing multidimensional poverty. Thus, social capital plays a fully mediating role in the effect of rural households’ multidimensional poverty on self-rated health.
The conclusive disparities can be explained in several different ways. First, multidimensional social capital has not been taken into account in prior research. Meanwhile, the majority of earlier studies portrayed social capital using a one-dimensional model (such as social trust, social support, and social networks). However, this social capital is not strictly social capital because it is one-dimensional. In this study, we estimate the total index of social capital after the entropy value using the four dimensions: social networks, social trust, social participation, and social support. This is partially due to the fact that there are several ways in which various social capital categories and definitions might influence an individual’s degree of health. Second, earlier research used survey data from different geological terrains (such as the plains, hills, and mountains), yet terrain conditions, social conditions, and income levels in different locations will impact rural households’ subjective assessments of their social capital position. In this study, we also considered rural households in different conditions geological terrains as sample selection in order to classify the different effects of the geological factors.
These findings shed new light on the relationship between multidimensional poverty and rural households’ self-rated health. The level of family care is used as a moderating variable and social capital is used as a mediating variable following entropy in the article. A moderated mediating model is then used to test the hypothesis. This supports earlier findings that a greater portion of the influence of rural households’ self-rated health is explained by the mediating effect of social capital [
53]. By enhancing our knowledge of the impact of multidimensional poverty on the self-rated health of rural households, this study adds to the body of literature. Additionally, the research uses mediated and moderated methods to identify variables linked to rural households’ self-rated health.
Even though the relationship between multidimensional poverty and the self-rated health of rural households has been better understood as a result of this study, there still exist some deficiencies that need further research.
First, the Jiangxi province of China has been the sole subject of this study. Thus, it is important to be cautious when interpreting our results. There should be more effort put into examining differences in the self-rated health of rural households between regions with various socioeconomic and cultural characteristics. At the same time, a lot of indicators and data are needed for the scientific measurement of health levels, and there is still a significant gap between the indicators used by the academic community and the medical health measurement technology. More abundant and high-quality data will be needed to measure rural households’ health levels more accurately and scientifically.
Second, because social capital is a broad concept, there are other ways to categorize it, including a taxonomy of individual and group social capital, bonded and linked social capital, and more. Further research is necessary to fully understand the various impacts of various social capital on the health of rural populations. However, family care is simply one of the variables that affect rural households’ social capital and multidimensional poverty. Future research should look at how these and other aspects of poverty affect health in order to fully understand the effects of multidimensional poverty on the self-rated health of rural households.
Third, as a limitation of expanding the research, it is also necessary to account for cultural aspects as social care may not be typical in some countries. Additionally, the social care is a wide concept, which has many other dimensions, such as the social care structure and age makeup. In order to fully capture the impacts of social care on the rural household’s health, it is worthwhile for future research to further explore the impact of the elements of cultural aspects on the rural household’s behavior.
This study aimed to address how the multidimensional poverty affected the self-rated health of rural households. Social capital was used as a mediating variable and family care was used as a moderating variable. We conducted the model and used the survey data including 382 out-of-poverty sample rural households from 2020 in Jiangxi Province, enabling us to take advantage of the moderated mediation model in exploring the relationship between multidimensional poverty and the self-rated health. It was revealed that multidimensional poverty affected rural households’ self-rated health primarily through social capital (β = 3.240 and t = 13.482) and that family care moderated the mediating pathway. Family care exacerbated the negative effect of multidimensional poverty on rural households’ self-rated health (β = 0.558 and t = −5.221) and weakened the beneficial effect of social capital on rural households’ self-rated health (β = −2.100, t = −3.304). The lower the level of family care, the more significant the positive effect of social capital on rural households’ health (simple slope = 1.742, t = 9.093, and p = 0.001).
To strengthen the viability of rural households in response to the fundamental needs of rural areas in the research region, targeted policies for reducing poverty should be developed. China should rely on the current information system for poverty alleviation and development, consider elements such as medical care, education, income, and living conditions, summarize the experience and failures of the period of eradicating poverty, and establish reasonable income baseline and vulnerability line monitoring standards in light of the current situation. Firstly, concentrate on boosting infrastructure building and medical and healthcare investment in rural areas. To stop and slow the spread of diseases, improve the medical and health infrastructure in rural areas. Secondly, in addition to strengthening the fight against adult illiteracy, literature that is tailored to farmers’ requirements should be published, and cultural events should be planned to raise the literacy levels of farm households. The development of social capital in rural households, leveraging social capital’s contribution to eradicating multifaceted poverty, and assisting farmers in deepening and broadening their interpersonal connections should then be the focus of attention. Finally, in order to lighten the pressure on family care and lessen the burden on family carers, the long-term care insurance system should be reinforced to encourage and support social care as well as the development of care offered by social institutions and community services. The government must consistently encourage the growth of socialized care services to fill the gap in family care so that social care can be used as a complementary or alternative resource to family care.







{kind=link}
{kind=link}
{kind=link}