
The Influence of Family Caregiver Knowledge and Behavior on Elderly Diabetic Patients’ Quality of Life in Northern Thailand

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
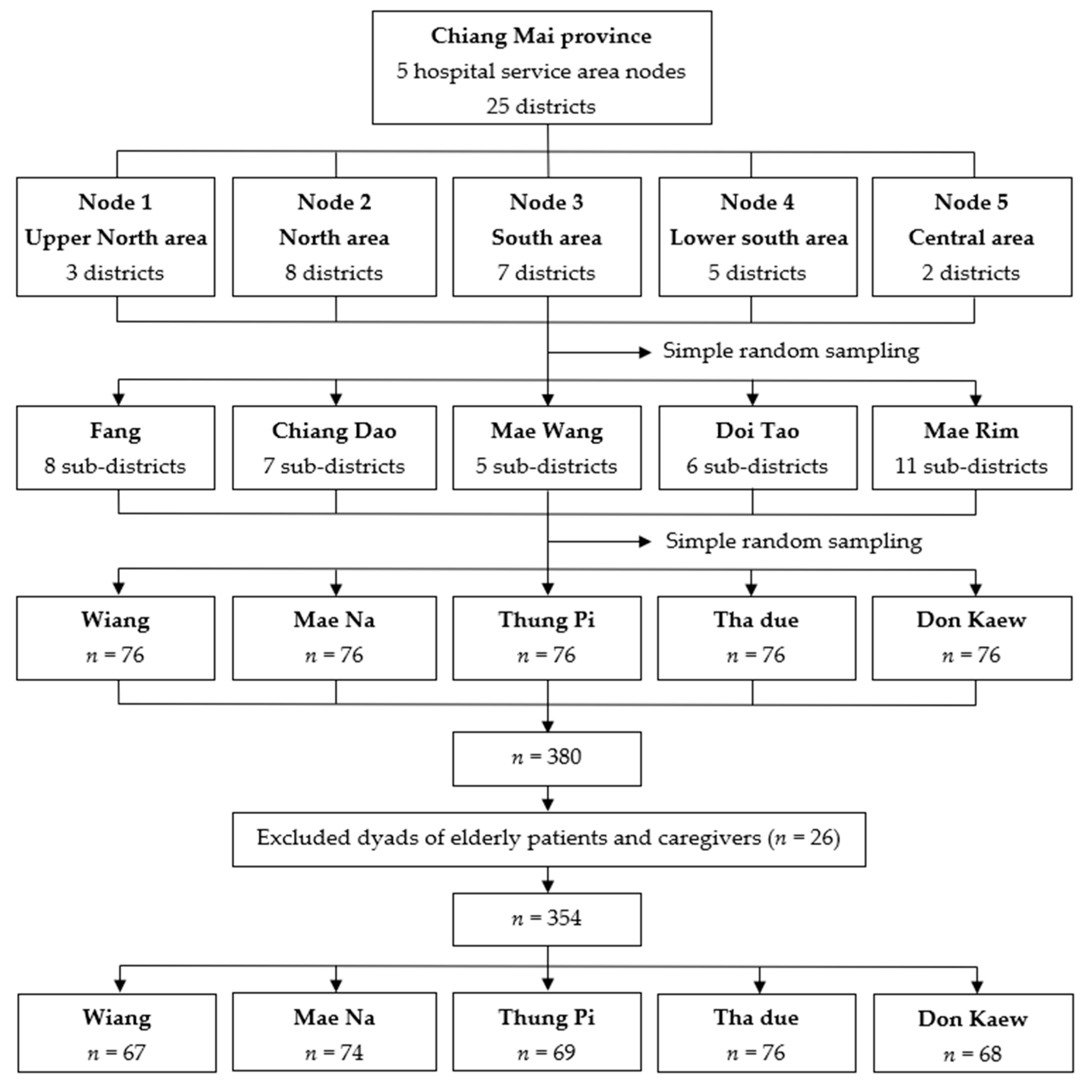
2.1. Study Design and Subjects
2.2. Data Collection
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baena-Díez, J.M.; Peñafiel, J.; Subirana, I.; Ramos, R.; Elosua, R.; Marín-Ibañez, A.; Guembe, M.J.; Rigo, F.; Tormo-Díaz, M.J.; Moreno-Iribas, C.; et al. Risk of Cause-Specific Death in Individuals With Diabetes: A Competing Risks Analysis. Diabetes Care 2016, 39, 1987–1995. [Google Scholar] [CrossRef] [PubMed]
- Spasić, A.; Catic Djordjevic, A.; Stefanovic, N.; Tatjana, C. Quality of Life in Type 2 Diabetic Patients. Acta Fac. Med. Naissensis 2014, 31, 193–200. [Google Scholar] [CrossRef]
- Ogurtsova, K.; Da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Al-Khaledi, M.; Al-Dousari, H.; Al-Dhufairi, S.; Al-Mousawi, T.; Al-Azemi, R.; Al-Azimi, F.; Hanan. Diabetes Self-Management: A Key to Better Health-Related Quality of Life in Patients with Diabetes. Med. Princ. Pract. 2018, 27, 323–331. [Google Scholar] [CrossRef] [PubMed]
- John, R.; Pise, S.; Chaudhari, L.; Deshpande, P. Evaluation of quality of life in type 2 diabetes mellitus patients using quality of life instrument for indian diabetic patients: A cross-sectional study. J. Mid-Life Health 2019, 10, 81–88. [Google Scholar] [CrossRef]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Aekplakorn, W.; Chariyalertsak, S.; Kessomboon, P.; Sangthong, R.; Inthawong, R.; Putwatana, P.; Taneepanichskul, S. The Sixth National Health Examination Survey 2020–21; The National Health Examination Survey Office, Health System Research Institute: Nonthaburi, Thailand, 2021. (In Thai) [Google Scholar]
- Bureau of Non Communicable Disease. The Number and Mortalities Rate Report of Non Communicable Disease 2016–2021; Bureau of Non Communicable Disease: Nonthaburi, Thailand, 2022. (In Thai)
- Lee, M.K.; Oh, J. Health-Related Quality of Life in Older Adults: Its Association with Health Literacy, Self-Efficacy, Social Support, and Health-Promoting Behavior. Healthcare 2020, 8, 407. [Google Scholar] [CrossRef]
- Shamshirgaran, S.M.; Stephens, C.; Alpass, F.; Aminisani, N. Longitudinal assessment of the health-related quality of life among older people with diabetes: Results of a nationwide study in New Zealand. BMC Endocr. Disord. 2020, 20, 32. [Google Scholar] [CrossRef]
- Singh, H.; Bradley, C. Quality of life in diabetes. Int. J. Diabetes Dev. Ctries. 2006, 26, 7. [Google Scholar] [CrossRef]
- Rubin, R.R.; Peyrot, M. Quality of life and diabetes. Diabetes/Metab. Res. Rev. 1999, 15, 205–218. [Google Scholar] [CrossRef]
- Totesora, D.; Ramos-Rivera, M.I.; Villegas-Florencio, M.Q.; Reyes-Sia, P.N. Association of Diabetes-related Emotional Distress with Diabetes Self-care and Glycemic Control among Adult Patients with Type 2 Diabetes at a Tertiary Hospital in Manila, Philippines. J. ASEAN Fed. Endocr. Soc. 2019, 34, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Bukhsh, A.; Khan, T.M.; Sarfraz Nawaz, M.; Sajjad Ahmed, H.; Chan, K.G.; Goh, B.-H. Association of diabetes knowledge with glycemic control and self-care practices among Pakistani people with type 2 diabetes mellitus. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1409–1417. [Google Scholar] [CrossRef] [PubMed]
- Karaoui, L.R.; Deeb, M.E.; Nasser, L.; Hallit, S. Knowledge and practice of patients with diabetes mellitus in Lebanon: A cross-sectional study. BMC Public Health 2018, 18, 525. [Google Scholar] [CrossRef] [PubMed]
- Kueh, Y.C.; Morris, T.; Borkoles, E.; Shee, H. Modelling of diabetes knowledge, attitudes, self-management, and quality of life: A cross-sectional study with an Australian sample. Health Qual. Life Outcomes 2015, 13, 129. [Google Scholar] [CrossRef]
- Sousa, M.C.d.; Dias, F.A.; Nascimento, J.S.; Tavares, D.M.D.S. Correlation of quality of life with the knowledge and attitude of diabetic elderly. Investig. Educ. Enfermería 2016, 34, 180–188. [Google Scholar] [CrossRef]
- Komaratat, C.; Auemaneekul, N.; Kittipichai, W. Quality of life for type II diabetes mellitus patients in a suburban tertiary hospital in Thailand. J. Health Res. 2020, 35, 3–14. [Google Scholar] [CrossRef]
- Babazadeh, T.; Dianatinasab, M.; Daemi, A.; Nikbakht, H.A.; Moradi, F.; Ghaffari-Fam, S. Association of Self-Care Behaviors and Quality of Life among Patients with Type 2 Diabetes Mellitus: Chaldoran County, Iran. Diabetes Metab. J. 2017, 41, 449–456. [Google Scholar] [CrossRef]
- Kristianingrum, N.D.; Wiarsih, W.; Nursasi, A.Y. Perceived family support among older persons in diabetes mellitus self-management. BMC Geriatr. 2018, 18, 304. [Google Scholar] [CrossRef]
- Bennich, B.B.; Røder, M.E.; Overgaard, D.; Egerod, I.; Munch, L.; Knop, F.K.; Vilsbøll, T.; Konradsen, H. Supportive and non-supportive interactions in families with a type 2 diabetes patient: An integrative review. Diabetol. Metab. Syndr. 2017, 9, 57. [Google Scholar] [CrossRef]
- Larocca, M.A.; Scogin, F.R. The Effect of Social Support on Quality of Life in Older Adults Receiving Cognitive Behavioral Therapy. Clin. Gerontol. 2015, 38, 131–148. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Jitapunkul, S. Disability: A problem of the elderly. Chula Med. J. 1994, 38, 67–75. [Google Scholar]
- Jitapunkul, S.; Kunanusont, C.; Phoolcharoen, W.; Suriyawongpaisal, P.; Ebrahim, S. Disability-free life expectancy of elderly people in a population undergoing demographic and epidemiologic transition. Age Ageing 2003, 32, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Mughal, S.; Barnett, A.H.; Fitzgerald, J.; Lloyd, C.E. Modification and validation of the Revised Diabetes Knowledge Scale. Diabet. Med. 2010, 28, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Khunkaew, S.; Fernandez, R.; Sim, J. Linguistic and Psychometric Validation of the Thai Version of Simplified Diabetes Knowledge Scale: A Measure of Knowledge of Diabetes in a Thai Population. SAGE Open Nurs. 2018, 4, 237796081879184. [Google Scholar] [CrossRef]
- Schmitt, A.; Gahr, A.; Hermanns, N.; Kulzer, B.; Huber, J.; Haak, T. The Diabetes Self-Management Questionnaire (DSMQ): Development and evaluation of an instrument to assess diabetes self-care activities associated with glycaemic control. Health Qual. Life Outcomes 2013, 11, 138. [Google Scholar] [CrossRef]
- Thojampa, S.; Mawn, B. Psychometric evaluation of the Thai translation of the Diabetes Self-management Questionnaire in type 2 diabetes. Int. J. Nurs. Sci. 2017, 4, 236–238. [Google Scholar] [CrossRef]
- World Health Organization. Whoqol-Old Manual; World Health Organization: Copenhagen, Denmark, 2004. [Google Scholar]
- Hongthong, D.; Somrongthong, R.; Ward, P. Factors Influencing the Quality of Life (Qol) among Thai Older People in a Rural Area of Thailand. Iran. J. Public Health 2015, 44, 479–485. [Google Scholar]
- Muchiri, J.W.; Gericke, G.J.; Rheeder, P. Effectiveness of an adapted diabetes nutrition education program on clinical status, dietary behaviors and behavior mediators in adults with type 2 diabetes: A randomized controlled trial. J. Diabetes Metab. Disord. 2021, 20, 293–306. [Google Scholar] [CrossRef]
- Brenk-Franz, K.; Strauss, B.; Tiesler, F.; Fleischhauer, C.; Ciechanowski, P.; Schneider, N.; Gensichen, J. The Influence of Adult Attachment on Patient Self-Management in Primary Care—The Need for a Personalized Approach and Patient-Centred Care. PLoS ONE 2015, 10, e0136723. [Google Scholar] [CrossRef]
- Alodhayani, A.; Almutairi, K.M.; Vinluan, J.M.; Almigbal, T.H.; Alonazi, W.B.; Ali Batais, M.; Mohammed Alnassar, M. Association between self-care management practices and glycemic control of patients with type 2 diabetes mellitus in Saud Arabia: A cross-sectional study. Saudi J. Biol. Sci. 2021, 28, 2460–2465. [Google Scholar] [CrossRef] [PubMed]
- Utli, H.; Vural Doğru, B. The effect of the COVID-19 pandemic on self-management in patients with type 2 diabetics. Prim. Care Diabetes 2021, 15, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.; Jenkins, A.J.; Quintiliani, L.M.; Truong, V.; Lasser, K.E. Resilience and diabetes self-management among African-American men receiving primary care at an urban safety-net hospital: A cross-sectional survey. Ethn. Health 2022, 27, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Tamornpark, R.; Utsaha, S.; Apidechkul, T.; Panklang, D.; Yeemard, F.; Srichan, P. Quality of life and factors associated with a good quality of life among diabetes mellitus patients in northern Thailand. Health Qual. Life Outcomes 2022, 20, 81. [Google Scholar] [CrossRef]
- Ong-Artborirak, P.; Seangpraw, K. Association Between Self-Care Behaviors and Quality of Life Among Elderly Minority Groups on the Border of Thailand. J. Multidiscip. Healthc. 2019, 12, 1049–1059. [Google Scholar] [CrossRef]
- Gondodiputro, S.; Wiwaha, G.; Lionthina, M.; Sunjaya, D.K. Reliability and validity of the Indonesian version of the World Health Organization quality of life-old (WHOQOL-OLD): A Rasch modeling. Med. J. Indones. 2021, 30, 143–151. [Google Scholar] [CrossRef]
- Wändell, P.E.; Tovi, J. The quality of life of elderly diabetic patients. J. Diabetes Its Complicat. 2000, 14, 25–30. [Google Scholar] [CrossRef]
- Van der Heide, I.; Uiters, E.; Rademakers, J.; Struijs, J.N.; Schuit, A.J.; Baan, C.A. Associations among health literacy, diabetes knowledge, and self-management behavior in adults with diabetes: Results of a dutch cross-sectional study. J. Health Commun. 2014, 19 (Suppl. 2), 115–131. [Google Scholar] [CrossRef]
- Chantriyawong, S. Developing a guide to promoting the quality of life for the elderly for families. J. Community Dev. Qual. Life 2018, 8, 16–30. (In Thai) [Google Scholar]
- Schaefer, C.; Coyne, J.C.; Lazarus, R.S. The health-related functions of social support. J. Behav. Med. 1981, 4, 381–406. [Google Scholar] [CrossRef]
- Berkman, L.F. Social support, social networks, social cohesion and health. Soc. Work Health Care 2000, 31, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Alnaim, L.; Altuwaym, R.A.; Aldehan, S.M.; Alquraishi, N.M. Assessment of knowledge among caregivers of diabetic patients in insulin dosage regimen and administration. Saudi Pharm. J. 2021, 29, 1137–1142. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | (n = 354) n (%) | Diabetes Knowledge | Self-Care Behavior | Quality of Life | |||
|---|---|---|---|---|---|---|---|
| Mean ± SD | p-Value | Mean ± SD | p-Value | Mean ± SD | p-Value | ||
| Sex | 0.017 | 0.858 | 0.961 | ||||
| Male | 105 (29.7) | 9.04 ± 4.08 | 7.16 ± 1.54 | 87.16 ± 13.50 | |||
| Female | 249 (70.3) | 7.95 ± 3.83 | 7.13 ± 1.60 | 87.24 ± 12.83 | |||
| Age | 0.277 | 0.239 | <0.001 | ||||
| 60–69 years | 210 (59.3) | 8.21 ± 4.01 | 7.24 ± 1.60 | 88.91 ± 13.05 | |||
| 70–79 years | 108 (30.5) | 8.66 ± 3.82 | 7.04 ± 1.56 | 86.87 ± 12.00 | |||
| ≥80 years | 36 (10.2) | 7.47 ± 3.79 | 6.81 ± 1.50 | 78.33 ± 12.30 | |||
| BMI | 0.554 | 0.123 | 0.006 | ||||
| <18.5 kg/m2 | 23 (6.5) | 7.96 ± 4.81 | 6.89 ± 1.67 | 80.87 ± 8.78 | |||
| 18.5–22.9 kg/ m2 | 126 (35.6) | 7.96 ± 3.94 | 7.01 ± 1.56 | 86.60 ± 12.19 | |||
| 23.0–24.9 kg/ m2 | 68 (19.2) | 8.76 ± 3.86 | 6.95 ± 1.72 | 87.38 ± 13.14 | |||
| ≥25.0 kg/ m2 | 137 (38.7) | 8.37 ± 3.82 | 7.39 ± 1.48 | 88.77 ± 14.00 | |||
| Education level | 0.348 | 0.582 | <0.001 | ||||
| None | 61 (17.3) | 7.62 ± 4.03 | 6.95 ± 1.33 | 81.61 ± 10.17 | |||
| Primary school | 233 (65.8) | 8.37 ± 3.72 | 7.19 ± 1.62 | 87.92 ± 13.21 | |||
| Secondary school or higher | 60 (16.9) | 8.55 ± 4.59 | 7.12 ± 1.65 | 90.18 ± 13.34 | |||
| Marital status | 0.467 | 0.698 | 0.961 | ||||
| Married | 210 (59.3) | 8.40 ± 4.07 | 7.17 ± 1.51 | 87.24 ± 13.03 | |||
| Unmarried | 144 (40.7) | 8.09 ± 3.72 | 7.10 ± 1.68 | 87.17 ± 13.04 | |||
| Employment | 0.253 | 0.043 | 0.715 | ||||
| Employed | 169 (47.7) | 8.02 ± 3.99 | 7.31 ± 1.58 | 87.48 ± 12.62 | |||
| Unemployed | 185 (52.3) | 8.50 ± 3.88 | 6.97 ± 1.56 | 86.97 ± 13.39 | |||
| Perceived financial status | 0.207 | 0.191 | 0.273 | ||||
| Sufficient | 169 (47.7) | 8.55 ± 4.05 | 7.02 ± 1.62 | 86.42 ± 13.50 | |||
| Insufficient | 185 (52.3) | 8.02 ± 3.82 | 7.24 ± 1.54 | 87.94 ± 12.54 | |||
| Living arrangements | 0.578 | 0.037 | <0.001 | ||||
| Multilevel family members | 194 (54.8) | 8.09 ± 3.87 | 7.26 ± 1.61 | 86.58 ± 13.69 | |||
| One spouse/son/daughter | 129 (36.4) | 8.58 ± 3.86 | 7.08 ± 1.51 | 89.50 ± 12.07 | |||
| Relatives | 31 (8.8) | 8.16 ± 4.65 | 6.60 ± 1.59 | 81.65 ± 10.44 | |||
| Duration of DM | 0.262 | 0.845 | 0.257 | ||||
| ≤5 years | 111 (31.4) | 8.77 ± 3.97 | 7.18 ± 1.74 | 88.68 ± 13.41 | |||
| 6–9 years | 71 (20.0) | 8.14 ± 3.83 | 7.20 ± 1.53 | 87.62 ± 11.83 | |||
| ≥10 years | 172 (48.6) | 8.01 ± 3.94 | 7.09 ± 1.50 | 86.10 ± 13.19 | |||
| Smoking | 0.882 | 0.191 | |||||
| Yes | 26 (7.3) | 8.38 ± 4.29 | 7.53 ± 1.51 | 90.62 ± 10.78 | |||
| No | 328 (92.7) | 8.27 ± 3.91 | 7.11 ± 1.58 | 86.95 ± 13.15 | |||
| Alcohol consumption | 0.887 | 0.924 | 0.106 | ||||
| Yes | 54 (15.3) | 8.20 ± 3.94 | 7.16 ± 1.49 | 89.85 ± 12.17 | |||
| No | 300 (84.7) | 8.29 ± 3.94 | 7.14 ± 1.60 | 86.74 ± 13.12 | |||
| Comorbidities | 0.124 | 0.041 | 0.425 | ||||
| Yes | 287 (81.1) | 8.12 ± 3.83 | 7.05 ± 1.53 | 86.95 ± 13.24 | |||
| No | 67 (18.9) | 8.94 ± 4.33 | 7.49 ± 1.75 | 88.36 ± 12.03 | |||
| Complications | 0.101 | 0.727 | 0.643 | ||||
| Yes | 93 (26.3) | 7.70 ± 3.97 | 7.19 ± 1.60 | 86.68 ± 14.43 | |||
| No | 261 (73.7) | 8.48 ± 3.91 | 7.12 ± 1.58 | 87.41 ± 12.50 | |||
| Activities in daily living | 0.887 | 0.218 | <0.001 | ||||
| Dependent (≤12) | 6 (1.7) | 8.50 ± 3.02 | 6.35 ± 1.57 | 67.67 ± 15.44 | |||
| Independent (>12) | 348 (98.3) | 8.27 ± 3.95 | 7.16 ± 1.58 | 87.56 ± 12.73 | |||
| Variable | (n = 354) n (%) | Diabetes Knowledge | Self-Care Behaviors | Quality of Life | |||
|---|---|---|---|---|---|---|---|
| Mean ± SD | p-Value | Mean ± SD | p-Value | Mean ± SD | p-Value | ||
| Sex | 0.062 | 0.059 | 0.627 | ||||
| Male | 141 (39.8) | 7.79 ± 3.90 | 7.34 ± 1.53 | 86.80 ± 12.55 | |||
| Female | 213 (60.2) | 8.59 ± 3.93 | 7.01 ± 1.60 | 87.49 ± 13.33 | |||
| Age | 0.853 | 0.332 | 0.459 | ||||
| 18–39 years | 80 (22.6) | 8.16 ± 3.32 | 7.15 ± 1.59 | 88.18 ± 11.63 | |||
| 40–59 years | 143 (40.4) | 8.20 ± 3.77 | 7.00 ± 1.51 | 86.18 ± 13.41 | |||
| ≥60 years | 131 (37.0) | 8.43 ± 4.44 | 7.29 ± 1.64 | 87.76 ± 13.39 | |||
| BMI | 0.271 | 0.577 | 0.558 | ||||
| <18.5 kg/m2 | 26 (7.3) | 7.35 ± 3.76 | 6.92 ± 1.53 | 84.81 ± 13.15 | |||
| 18.5–22.9 kg/m2 | 115 (32.5) | 7.90 ± 4.03 | 7.13 ± 1.69 | 86.41 ± 12.81 | |||
| 23.0–24.9 kg/m2 | 68 (19.2) | 8.65 ± 3.91 | 7.36 ± 1.60 | 88.30 ± 13.89 | |||
| ≥25.0 kg/m2 | 145 (41.0) | 8.57 ± 3.88 | 7.09 ± 1.50 | 87.77 ± 12.77 | |||
| Education level | 0.852 | 0.833 | 0.423 | ||||
| None | 14 (4.0) | 8.86 ± 3.25 | 7.05 ± 1.61 | 88.93 ± 17.00 | |||
| Primary school | 153 (43.2) | 8.24 ± 4.00 | 7.09 ± 1.67 | 88.09 ± 13.63 | |||
| Secondary school or higher | 187 (52.8) | 8.26 ± 3.93 | 7.19 ± 1.50 | 86.37 ± 12.15 | |||
| Marital status | 0.531 | 0.185 | 0.564 | ||||
| Married | 247 (69.8) | 8.36 ± 3.81 | 7.21 ± 1.55 | 86.95 ± 13.40 | |||
| Unmarried | 107 (30.2) | 8.07 ± 4.22 | 6.98 ± 1.63 | 87.82 ± 12.12 | |||
| Monthly family income | 0.855 | 0.419 | 0.268 | ||||
| <5000 THB | 153 (43.2) | 8.39 ± 3.97 | 7.24 ± 1.63 | 88.29 ± 13.29 | |||
| 5000-10,000 THB | 95 (26.8) | 8.26 ± 3.92 | 7.17 ± 1.54 | 85.53 ± 12.98 | |||
| ≥10,001 THB | 106 (30.0) | 8.11 ± 3.92 | 6.98 ± 1.54 | 87.18 ± 12.59 | |||
| Smoking | 0.657 | 0.195 | 0.056 | ||||
| Yes | 39 (11.0) | 8.54 ± 3.83 | 6.83 ± 1.64 | 83.46 ± 12.33 | |||
| No | 315 (89.0) | 8.24 ± 3.95 | 7.18 ± 1.56 | 87.68 ± 13.04 | |||
| Alcohol consumption | 0.989 | 0.879 | 0.234 | ||||
| Yes | 115 (32.5) | 8.28 ± 4.03 | 7.12 ± 1.50 | 86.03 ± 1267 | |||
| No | 239 (67.5) | 8.27 ± 3.89 | 7.15 ± 1.62 | 87.79 ± 13.16 | |||
| Caregiver relationship to patient | 0.703 | 0.448 | 0.858 | ||||
| Spouse | 131 (37.0) | 8.35 ± 4.48 | 7.28 ± 1.60 | 87.16 ± 13.33 | |||
| Son or daughter | 137 (38.7) | 8.39 ± 3.50 | 7.08 ± 1.48 | 87.63 ± 12.62 | |||
| Relatives | 86 (24.3) | 7.97 ± 3.70 | 7.03 ± 1.70 | 86.64 ± 13.27 | |||
| Years of caring experience | 0.695 | 0.598 | 0.435 | ||||
| <5 years | 166 (46.9) | 8.19 ± 3.90 | 7.19 ± 1.54 | 86.64 ± 11.96 | |||
| ≥5 years | 188 (53.1) | 8.35 ± 3.97 | 7.10 ± 1.61 | 87.72 ± 13.89 | |||
| Time spent caring | 0.107 | 0.855 | 0.892 | ||||
| ≤7 h/day | 164 (46.3) | 8.32 ± 4.25 | 7.10 ± 1.67 | 86.87 ± 12.37 | |||
| 8–16 h/day | 102 (28.8) | 8.79 ± 3.51 | 7.14 ± 1.41 | 87.63 ± 13.11 | |||
| ≥17 h/day | 88 (24.9) | 7.59 ± 3.71 | 7.22 ± 1.60 | 87.21 ± 14.16 | |||
| Having secondary caregiver | 0.257 | 0.786 | 0.773 | ||||
| Yes | 211 (59.6) | 8.47 ± 3.83 | 7.12 ± 1.55 | 87.38 ± 13.84 | |||
| No | 143 (40.4) | 7.99 ± 4.07 | 7.16 ± 1.62 | 86.97 ± 11.73 | |||
| Variable | n (%) | Mean ± SD | Min–Max |
|---|---|---|---|
| Patients’ diabetes knowledge | |||
| Total score | 8.27 ± 3.93 | 0–20 | |
| Percentile: | |||
| 76–100% correct | 11 (3.1) | ||
| 51–75% correct | 90 (25.4) | ||
| 26–50% correct | 160 (45.2) | ||
| 0–25% correct | 93 (26.3) | ||
| Patients’ self-care behaviors | |||
| Total DSMQ (sum-scale; SS) | 7.14 ± 1.58 | 2.50–10.00 | |
| Subscale: | |||
| Glucose management (GM) | 7.60 ± 2.15 | 0.67–10.00 | |
| Dietary control (DC) | 7.17 ± 1.82 | 1.70–10.00 | |
| Physical activity (PA) | 6.34 ± 2.51 | 0.00–10.00 | |
| Health-care use (HU) | 7.23 ± 1.98 | 1.10–10.00 | |
| Patients’ QOL | |||
| Total QOL | 87.21 ± 13.01 | 37–120 | |
| Low level (≤55) | 2 (0.6) | ||
| Moderate level (56–88) | 198 (55.9) | ||
| High level (≥89) | 154 (43.5) | ||
| Facet: | |||
| Sensory functioning (SAB) | 14.72 ± 3.33 | 5–20 | |
| Autonomy (AUT) | 13.65 ± 3.09 | 4–20 | |
| Past present and future activities (PFF) | 14.39 ± 2.64 | 6–20 | |
| Social participation (SOP) | 13.62 ± 3.04 | 4–20 | |
| Death and dying (DAD) | 16.53 ± 3.27 | 6–20 | |
| Intimacy (INT) | 14.30 ± 2.56 | 4–20 | |
| Caregivers’ diabetes knowledge | |||
| Total score | 8.42 ± 3.79 | 0–20 | |
| Percentile: | |||
| 76–100% correct | 12 (3.4) | ||
| 51–75% correct | 91 (25.7) | ||
| 26–50% correct | 168 (47.5) | ||
| 0–25% correct | 83 (23.4) | ||
| Caregivers’ patient-care behaviors | |||
| Total DSMQ (sum-scale; SS) | 7.40 ± 1.58 | 3.33–10.00 | |
| Subscale: | |||
| Glucose management (GM) | 7.34 ± 2.08 | 1.33–10.00 | |
| Dietary control (DC) | 7.84 ± 1.67 | 2.50–10.00 | |
| Physical activity (PA) | 7.27 ± 2.34 | 0.00–10.00 | |
| Health-care use (HU) | 7.22 ± 1.82 | 2.22–10.00 |
| Variable | B | SE | Beta | p-Value | R Square |
|---|---|---|---|---|---|
| Univariable | |||||
| (Constant) | 6.00 | 0.18 | <0.001 * | 11.9% | |
| Patients’ diabetes knowledge (score) | 0.14 | 0.02 | 0.344 | <0.001 * | |
| (Constant) | 5.94 | 0.19 | <0.001 * | 11.7% | |
| Caregivers’ diabetes knowledge (score) | 0.14 | 0.02 | 0.341 | <0.001 * | |
| Multivariable | |||||
| (Constant) | 6.40 | 0.41 | <0.001 * | 15.3% | |
| Employment (unemployed) | −0.36 | 0.16 | −0.114 | 0.028 * | |
| Comorbidities (no) | 0.25 | 0.21 | 0.061 | 0.233 | |
| Living arrangements: | |||||
| Multilevel family members | 0.61 | 0.29 | 0.193 | 0.033 * | |
| One spouse/son/daughter | 0.32 | 0.30 | 0.097 | 0.287 | |
| Relatives | Ref. | ||||
| Patients’ diabetes knowledge (score) | 0.14 | 0.02 | 0.351 | <0.001 * |
| Variable | B | SE | Beta | p-Value | R Square |
|---|---|---|---|---|---|
| Univariable | |||||
| (Constant) | 76.85 | 1.50 | <0.001 * | 14.3% | |
| Patients’ diabetes knowledge (score) | 1.25 | 0.16 | 0.379 | <0.001 * | |
| (Constant) | 65.84 | 2.99 | <0.001 * | 13.2% | |
| Patients’ self-care behaviors (score) | 3.00 | 0.41 | 0.363 | <0.001 * | |
| (Constant) | 79.07 | 1.62 | <0.001 * | 7.9% | |
| Caregivers’ diabetes knowledge (score) | 0.97 | 0.18 | 0.282 | <0.001 * | |
| (Constant) | 65.62 | 3.12 | <0.001 * | 12.4% | |
| Caregivers’ patient-care behaviors (score) | 2.92 | 0.41 | 0.353 | <0.001 * | |
| Multivariable | |||||
| (Constant) | 76.93 | 8.93 | <0.001 * | 27.0% | |
| Patients’ ages (years) | −0.34 | 0.09 | −0.183 | <0.001 * | |
| Patients’ BMI (kg/m2) | 0.06 | 0.15 | 0.020 | 0.680 | |
| Patients’ education level: | |||||
| None | Ref. | ||||
| Primary school | 3.35 | 1.71 | 0.122 | 0.051 | |
| Secondary school or higher | 5.84 | 2.12 | 0.169 | 0.006 | |
| Living arrangements: | |||||
| Multilevel family members | 2.00 | 2.21 | 0.077 | 0.365 | |
| One spouse/son/daughter | 4.99 | 2.28 | 0.185 | 0.030 * | |
| Relatives | Ref. | ||||
| Patients’ self-care behaviors (score) | 1.58 | 0.48 | 0.192 | 0.001 * | |
| Caregivers’ diabetes knowledge (score) | 0.58 | 0.17 | 0.169 | 0.001 * | |
| Caregivers’ patient-care behaviors (score) | 1.38 | 0.47 | 0.167 | 0.004 * |
| Variable | SS | GM | DC | PA | HU | QoL |
|---|---|---|---|---|---|---|
| Patients’ self-care behaviors and QoL | ||||||
| Sum-scale (SS) | 1 | |||||
| Glucose management (GM) | 0.772 * | 1 | ||||
| Dietary control (DC) | 0.769 * | 0.421 * | 1 | |||
| Physical activity (PA) | 0.680 * | 0.243 * | 0.489 * | 1 | ||
| Health-care use (HU) | 0.703 * | 0.452 * | 0.420 * | 0.331 * | 1 | |
| Patients’ QoL | 0.363 * | 0.266 * | 0.183 * | 0.287 * | 0.335 * | 1 |
| Caregivers’ patient-care behaviors and patients’ QoL | ||||||
| Sum-scale (SS) | 1 | |||||
| Glucose management (GM) | 0.766 * | 1 | ||||
| Dietary control (DC) | 0.819 * | 0.480 * | 1 | |||
| Physical activity (PA) | 0.812 * | 0.402 * | 0.648 * | 1 | ||
| Health-care use (HU) | 0.733 * | 0.376 * | 0.524 * | 0.553 * | 1 | |
| Patients’ QoL | 0.353 * | 0.139 * | 0.327 * | 0.350 * | 0.373 * | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongduang, K.; Boonchieng, W.; Chautrakarn, S.; Ong-Artborirak, P. The Influence of Family Caregiver Knowledge and Behavior on Elderly Diabetic Patients’ Quality of Life in Northern Thailand. Int. J. Environ. Res. Public Health 2022, 19, 10216. https://doi.org/10.3390/ijerph191610216
Thongduang K, Boonchieng W, Chautrakarn S, Ong-Artborirak P. The Influence of Family Caregiver Knowledge and Behavior on Elderly Diabetic Patients’ Quality of Life in Northern Thailand. International Journal of Environmental Research and Public Health. 2022; 19(16):10216. https://doi.org/10.3390/ijerph191610216
Chicago/Turabian StyleThongduang, Kitbordin, Waraporn Boonchieng, Sineenart Chautrakarn, and Parichat Ong-Artborirak. 2022. "The Influence of Family Caregiver Knowledge and Behavior on Elderly Diabetic Patients’ Quality of Life in Northern Thailand" International Journal of Environmental Research and Public Health 19, no. 16: 10216. https://doi.org/10.3390/ijerph191610216