
The Effectiveness and Safety of Chuna Manual Therapy Adjuvant to Western Medicine in Patients with Chronic Obstructive Pulmonary Disease: A Randomized, Single-Blind, Investigator-Initiated, Pilot Trial

Abstract
:1. Introduction
2. Materials and Methods
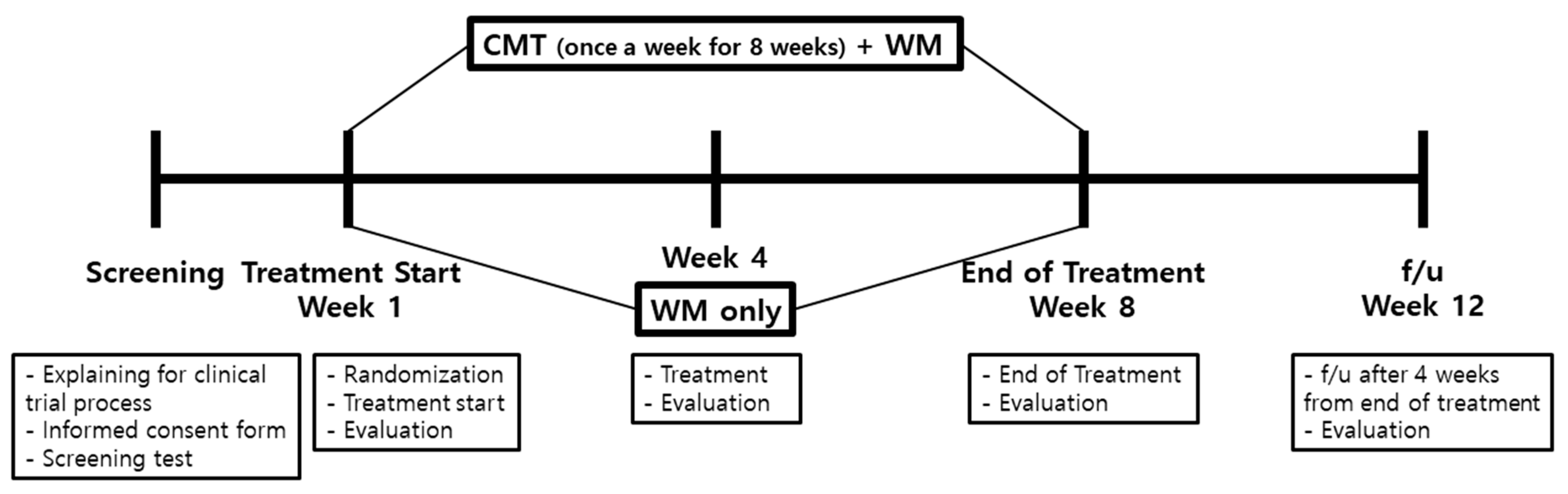
2.1. Study Protocol
2.2. Study Design
2.3. Participants
2.3.1. Inclusion Criteria
- Patients aged ≥40 years and ≤80 years
- Meeting the diagnostic criteria for COPD: Patients with a spirometry test result showing a forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio of <0.70 [4] and currently undergoing standard drug therapy
- Patients who willingly provided informed consent to participate in the clinical trial
2.3.2. Exclusion Criteria
- Individuals with moderate-to-severe respiratory symptoms due to diseases other than COPD (cystic fibrosis, pneumonia, interstitial lung disease, and lung cancer)
- Individuals with a history of alcohol or other substance abuse or dependency
- Individuals diagnosed with a clinically significant disease or condition of the liver or heart, or cardiovascular, respiratory, endocrine, or central nervous system based on clinical testing, or having a history of malignant tumors or mental disorder. (However, patients were considered as eligible for participation if their conditions had not recurred for at least five years after surgery)
- Individuals showing a change in drug use within the past three months prior to the present study
- Patients who cannot walk without assistance
- Patients who received exercise therapy, physiotherapy, or MT related to respiratory rehabilitation in the last month
- Patients under oxygen therapy
- Individuals contraindicated for Chuna MT
- Pregnant or planning for pregnancy
- Patients deemed unsuitable for participation in this study by the principal investigator
2.4. Randomization and Blinding
2.5. Interventions
- Cervical relaxation: The therapist assumed a position in which both the hands were wrapped around the patient’s neck while the patient was in the supine position. Using the second and third fingers, strong pressure was applied to the C1-7 spinous process and splenic muscles while rotating the neck.
- Occipitocervical junction relaxation: The patient’s head was positioned outside the bed and firm pressure was applied on the occipitocervical junction using the second, third, and fourth fingers.
- Trapezius muscle relaxation: Using the thumb and index finger, both trapezius muscles were grasped in a manner similar to when using forceps. Firm pressure was applied with the thumbs to promote muscle relaxation.
- Clavicle relaxation: The upper and lower parts of the clavicle were pressed with the thumb with a rubbing motion.
- Pectoralis major and latissimus dorsi muscle relaxation: With hands extended and the fingers stretched out, the therapist relaxed the patient’s pectoralis major muscle by applying force to the thumbs. Subsequently, the insertion point of the serratus anterior muscle was pressed vertically below the armpit using the thumb.
- Rectus abdominal muscle relaxation (via the upper limbs): The therapist held both hands of the patient and extended the arms upward. Patients were instructed to fully extend their feet while exhaling (Set 1) and bring their toes toward the body while exhaling (Set 2), and the process was repeated.
- Quadratus lumborum and intercostal muscle relaxation (via the upper limbs): The patient’s arms were stretched to the left while assuming the position from Step 6. Simultaneously, the direction of the patient’s feet was guided toward the left (Set 1). Subsequently, the patient’s arm was stretched to the right (Set 2). Simultaneously, the direction of the patient’s feet was guided toward the right (Set 2). The processes under Sets 1 and 2 were repeated.
- Thoracic breathing relaxation (via pressure on the humeral head): The therapist placed their palms on both humeral heads and applied pressure while the patient inhaled. The pressure was released while the patient exhaled.
- Breathing relaxation (via pressure on the pectoralis major muscle): The palms were placed on both the pectoralis major muscles, and pressure was applied to the muscles when the patient inhaled and released when the patient exhaled.
- Abdominal trapezius and thoracolumbar paraspinal muscle relaxation: Pressure was continuously applied and released using both palms along the thoracolumbar paraspinal muscles, starting from the Dazhui point and progressing toward the waist. This step mainly focused on relaxing the abdominal trapezius and thoracolumbar paraspinal muscles.
2.6. Outcome Measures
2.7. Sample Size Calculation
2.8. Adverse Events
2.9. Statistical Analysis
3. Results
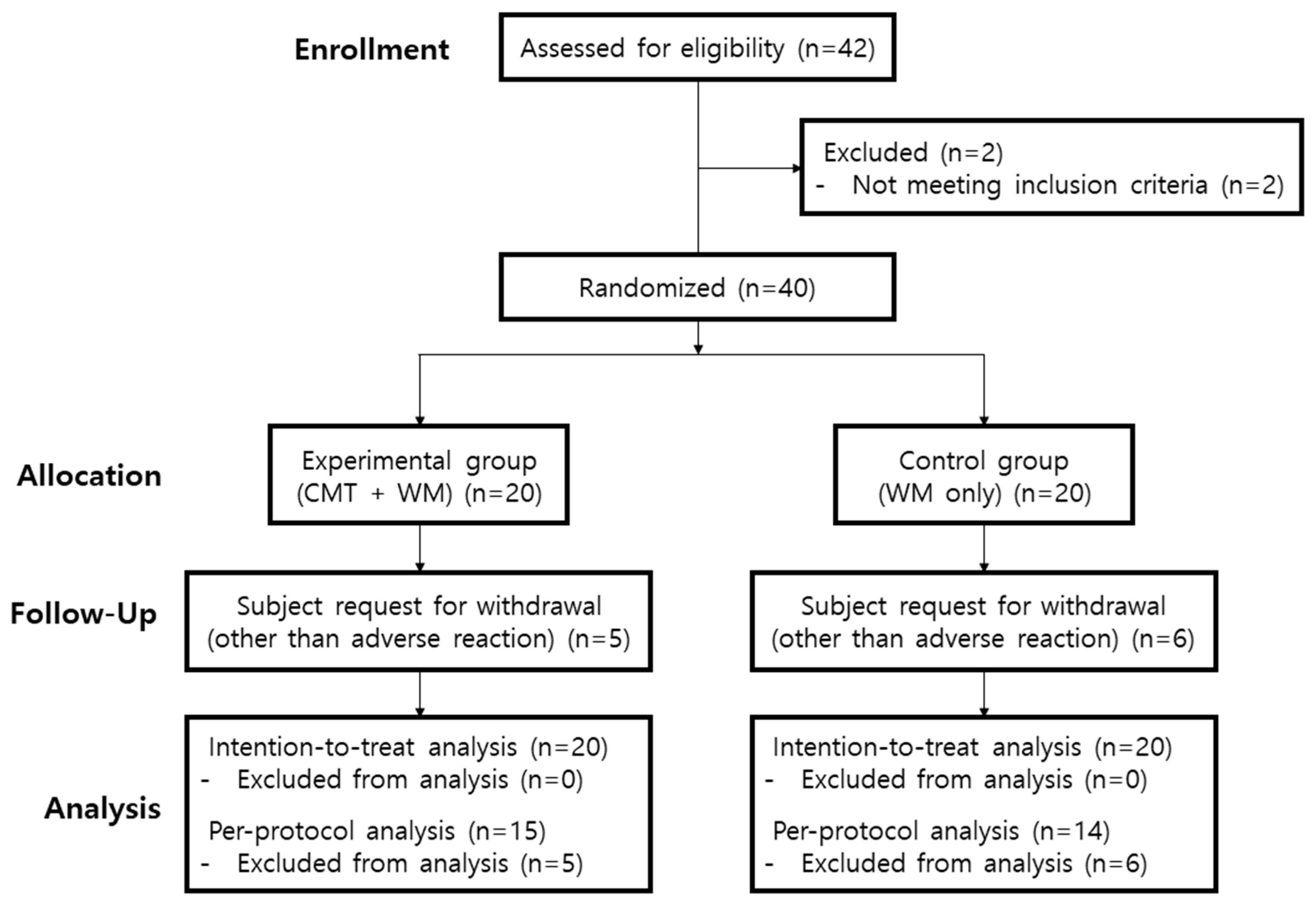
3.1. Participants
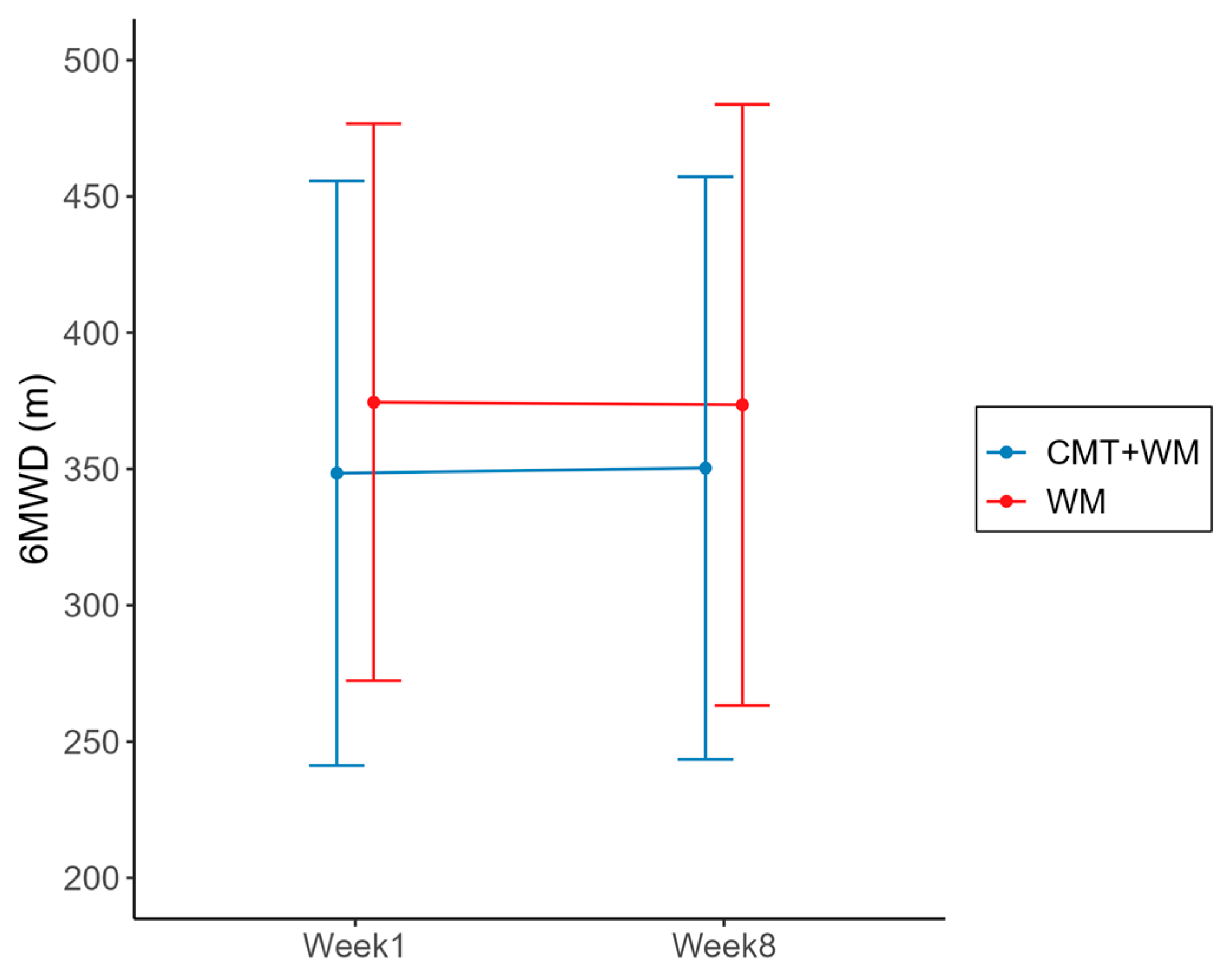
3.2. Primary Outcome
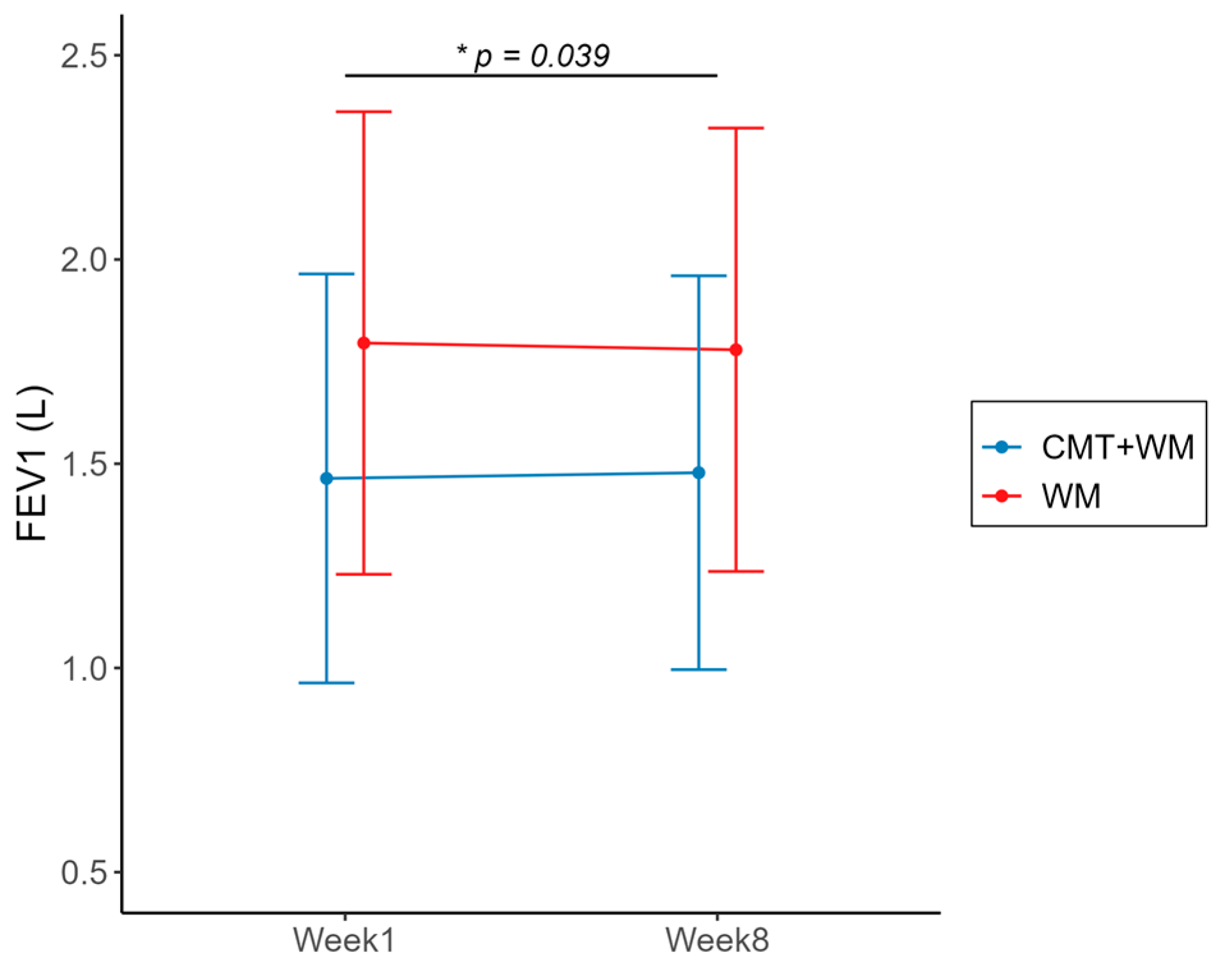
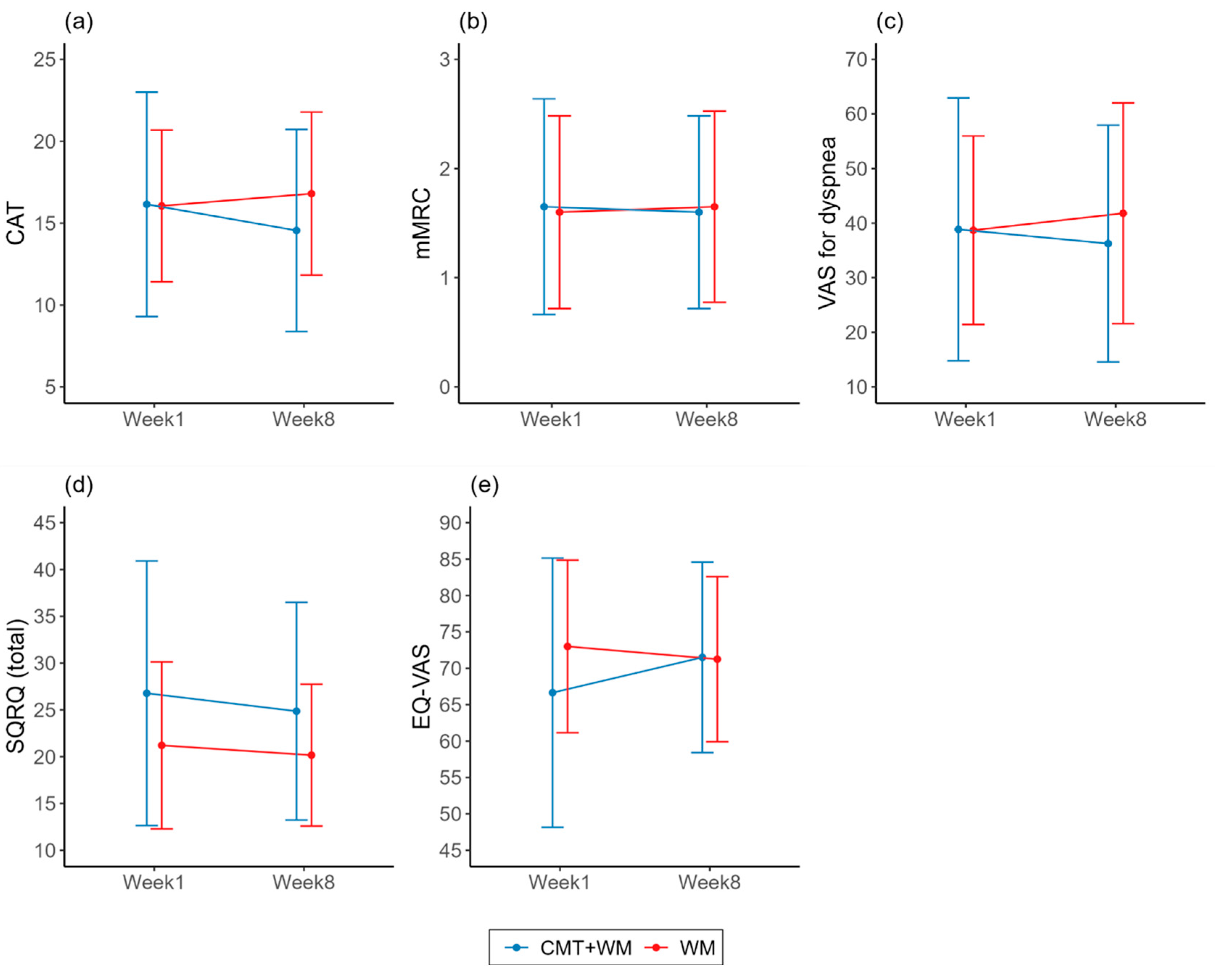
3.3. Secondary Outcomes
3.4. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Celli, B.; Fabbri, L.; Criner, G.; Martinez, F.J.; Mannino, D.; Vogelmeier, C.; Montes de Oca, M.; Papi, A.; Sin, D.D.; Han, M.K. Definition and nomenclature of chronic obstructive pulmonary disease: Time for its revision. Am. J. Respir. Crit. Care Med. 2022, 206, 1317–1325. [Google Scholar] [CrossRef]
- Adeloye, D.; Song, P.; Zhu, Y.; Campbell, H.; Sheikh, A.; Rudan, I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: A systematic review and modelling analysis. Lancet Respir. Med. 2022, 10, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Adeloye, D.; Chua, S.; Lee, C.; Basquill, C.; Papana, A.; Theodoratou, E.; Nair, H.; Gasevic, D.; Sridhar, D.; Campbell, H. Global and regional estimates of COPD prevalence: Systematic review and meta–analysis. J. Glob. Health 2015, 5, 020415. [Google Scholar] [CrossRef] [PubMed]
- GOLD. Global Strategy for Prevention, Diagnosis and Management of COPD: 2023 Report. 2023. Available online: https://goldcopd.org/2023-gold-report-2/ (accessed on 12 March 2023).
- Nici, L.; Mammen, M.J.; Charbek, E.; Alexander, P.E.; Au, D.H.; Boyd, C.M.; Criner, G.J.; Donaldson, G.C.; Dreher, M.; Fan, V.S. Pharmacologic management of chronic obstructive pulmonary disease. An official American Thoracic Society clinical practice guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e56–e69. [Google Scholar] [CrossRef]
- Kew, K.M.; Mavergames, C.; Walters, J.A. Long-acting beta 2-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- Karner, C.; Chong, J.; Poole, P. Tiotropium versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Papi, A.; Vestbo, J.; Fabbri, L.; Corradi, M.; Prunier, H.; Cohuet, G.; Guasconi, A.; Montagna, I.; Vezzoli, S.; Petruzzelli, S. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): A double-blind, parallel group, randomised controlled trial. Lancet 2018, 391, 1076–1084. [Google Scholar] [CrossRef]
- Chrystyn, H.; Small, M.; Milligan, G.; Higgins, V.; Gil, E.G.; Estruch, J. Impact of patients’ satisfaction with their inhalers on treatment compliance and health status in COPD. Respir. Med. 2014, 108, 358–365. [Google Scholar] [CrossRef]
- Miravitlles, M.; Auladell-Rispau, A.; Monteagudo, M.; Vázquez-Niebla, J.C.; Mohammed, J.; Nuñez, A.; Urrútia, G. Systematic review on long-term adverse effects of inhaled corticosteroids in the treatment of COPD. Eur. Respir. Rev. 2021, 30, 210075. [Google Scholar] [CrossRef]
- Engel, R.; Vemulpad, S. The role of spinal manipulation, soft-tissue therapy, and exercise in chronic obstructive pulmonary disease: A review of the literature and proposal of an anatomical explanation. J. Altern. Complement. Med. 2011, 17, 797–801. [Google Scholar] [CrossRef]
- Tsimouris, D.; Arvanitidis, M.; Moutzouri, M.; Koumantakis, G.A.; Gioftsos, G.; Papandreou, M.; Grammatopoulou, E. Is manual therapy of the diaphragm effective for people with Obstructive Lung Diseases? A Systematic Review. Respir. Med. Res. 2023, 83, 101002. [Google Scholar] [CrossRef]
- Heneghan, N.R.; Adab, P.; Balanos, G.M.; Jordan, R.E. Manual therapy for chronic obstructive airways disease: A systematic review of current evidence. Man. Ther. 2012, 17, 507–518. [Google Scholar] [CrossRef]
- Roh, J.-A.; Kim, K.-I.; Jung, H.-J. The efficacy of manual therapy for chronic obstructive pulmonary disease: A systematic review. PLoS ONE 2021, 16, e0251291. [Google Scholar] [CrossRef]
- Kwon, C.-Y.; Lee, B.; Lee, B.-J.; Kim, K.-I.; Jung, H.-J. Comparative Effectiveness of Western and Eastern Manual Therapies for Chronic Obstructive Pulmonary Disease: A Systematic Review and Network Meta-Analysis. Healthcare 2021, 9, 1127. [Google Scholar] [CrossRef]
- Lee, N.-W.; Kim, G.-H.; Heo, I.; Kim, K.-W.; Ha, I.-H.; Lee, J.-H.; Hwang, E.-H.; Shin, B.-C. Chuna (or Tuina) manual therapy for musculoskeletal disorders: A systematic review and meta-analysis of randomized controlled trials. Evid.-Based Complement. Altern. Med. 2017, 2017, 8218139. [Google Scholar] [CrossRef]
- Chung, I.-C.; Cha, Y.-Y.; Heo, I. Chuna Manual Therapy for Tinnitus: A Systematic Review and meta-analysis. J. Korea CHUNA Man. Med. Spine Nerves 2019, 14, 13–23. [Google Scholar] [CrossRef]
- Heo, I.; Shin, B.-C.; Hwang, E.-H.; Hwang, M.-S.; Kim, B.-J.; Kim, S.-Y.; Heo, K.-H. Chuna manual therapy for functional dyspepsia: A systematic review and meta-analysis. J. Korea CHUNA Man. Med. Spine Nerves 2015, 10, 1–14. [Google Scholar]
- Park, H.-J.; Kim, H.-T.; Lee, S.-H.; Hwang, M.-S.; Hwang, E.-H.; Shin, B.-C.; Heo, I. Chuna Manual Therapy for Pediatric Cough: A Systematic Review and Meta-analysis. J. Korea CHUNA Man. Med. Spine Nerves 2021, 16, 25–34. [Google Scholar] [CrossRef]
- Cho, J.-c.; Park, I.-h.; Heo, I. Chuna Manual Therapy for Rhinitis: Systematic Review and Meta Analysis. J. Korea CHUNA Man. Med. Spine Nerves 2021, 16, 35–42. [Google Scholar] [CrossRef]
- Kim, K.-I.; Lee, B.-J.; Jung, H.-J. The effectiveness and safety of Chuna manual therapy adjuvant to Western medicine in patients with chronic obstructive pulmonary disease: Study protocol for a randomized, single-blind, investigator-initiated, pilot trial. Medicine 2021, 100, e27217. [Google Scholar] [CrossRef]
- Sundh, J.; Janson, C.; Lisspers, K.; Ställberg, B.; Montgomery, S. The Dyspnoea, Obstruction, Smoking, Exacerbation (DOSE) index is predictive of mortality in COPD. Prim. Care Respir. J. 2012, 21, 295–301. [Google Scholar] [CrossRef]
- Jones, P.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.; Leidy, N.K. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M.; Littlejohns, P. A self-complete measure of health status for chronic airflow limitation. Am. Rev. Respir. Dis. 1992, 145, 1321–1327. [Google Scholar] [CrossRef]
- Kim, S.-H.; Ahn, J.; Ock, M.; Shin, S.; Park, J.; Luo, N.; Jo, M.-W. The EQ-5D-5L valuation study in Korea. Qual. Life Res. 2016, 25, 1845–1852. [Google Scholar] [CrossRef]
- Julious, S.A. Sample size of 12 per group rule of thumb for a pilot study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Hertzog, M.A. Considerations in determining sample size for pilot studies. Res. Nurs. Health 2008, 31, 180–191. [Google Scholar] [CrossRef]
- Aarts, S.; Van Den Akker, M.; Winkens, B. The importance of effect sizes. Eur. J. Gen. Pract. 2014, 20, 61–64. [Google Scholar] [CrossRef]
- Jacob, C. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Kakavas, S.; Kotsiou, O.S.; Perlikos, F.; Mermiri, M.; Mavrovounis, G.; Gourgoulianis, K.; Pantazopoulos, I. Pulmonary function testing in COPD: Looking beyond the curtain of FEV1. Npj Prim. Care Respir. Med. 2021, 31, 23. [Google Scholar] [CrossRef]
- Yohannes, A.M.; Dryden, S.; Casaburi, R.; Hanania, N.A. Long-term benefits of pulmonary rehabilitation in patients with COPD: A 2-year follow-up study. Chest 2021, 159, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Casal, A.; Toubes, M.; Sanz, L.; Rodríguez, C.; Rábade, C.; Riveiro, V.; Lourido, T.; Abelleira, R.; Ferreiro, L.; Lama, A. Multidimensional Assessment of Pulmonary Rehabilitation Programs in COPD Patients. Eur. Respir. J. 2022, 60, 1890. [Google Scholar]
- Kon, S.S.; Canavan, J.L.; Jones, S.E.; Nolan, C.M.; Clark, A.L.; Dickson, M.J.; Haselden, B.M.; Polkey, M.I.; Man, W.D. Minimum clinically important difference for the COPD Assessment Test: A prospective analysis. Lancet Respir. Med. 2014, 2, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Zanini, A.; Aiello, M.; Adamo, D.; Casale, S.; Cherubino, F.; Della Patrona, S.; Raimondi, E.; Zampogna, E.; Chetta, A.; Spanevello, A. Estimation of minimal clinically important difference in EQ-5D visual analog scale score after pulmonary rehabilitation in subjects with COPD. Respir. Care 2015, 60, 88–95. [Google Scholar] [CrossRef]
- Jones, P.W. St. George’s respiratory questionnaire: MCID. COPD 2005, 2, 75–79. [Google Scholar] [CrossRef]
- Ozarda, Y.; Ichihara, K.; Barth, J.H.; Klee, G.; on behalf of the Committee on Reference Intervals and Decision Limits (C-RIDL). Protocol and standard operating procedures for common use in a worldwide multicenter study on reference values. Clin. Chem. Lab. Med. 2013, 51, 1027–1040. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | CMT + WM (n = 20) | WM (n = 20) | p-Value |
|---|---|---|---|
| Age (years) | 70.4 ± 7.11 | 70.9 ± 5.40 | 0.9675 * |
| Sex (male) | 15 (75.0) | 20 (100.0) | 0.0471 * |
| Height (cm) | 161.7 ± 7.1 | 165.5 ± 5.5 | 0.0619 * |
| Weight (kg) | 62.8 ± 14.3 | 68.5 ± 14.3 | 0.2615 * |
| BMI (kg/m2) | 23.8 ± 3.9 | 24.8 ± 4.35 | 0.6847 * |
| Smoking | |||
| No | 15 (75.0) | 15 (75.0) | 1 † |
| Yes | 5 (25.0) | 5 (25.0) | |
| Alcohol consumption | |||
| No | 20 (100.0) | 19 (95.0) | 1 ‡ |
| Yes | 0 (0.0) | 1 (5.0) | |
| CRP | |||
| normal (<0.5) | 20 (100.00) | 17 (85.00) | 0.2308 ‡ |
| NCS | 0 (0.00) | 3 (15.00) | |
| Primary outcome | |||
| 6MWD (m) | 348.45 ± 107.23 | 374.50 ± 102.18 | 0.3866 * |
| Secondary outcomes | |||
| CAT | 16.15 ± 6.85 | 16.05 ± 4.63 | 0.839 * |
| mMRC | 1.65 ± 0.99 | 1.60 ± 0.88 | 0.7899 * |
| VAS for dyspnea (mm) | 38.85 ± 24.07 | 38.70 ± 17.27 | 0.8181 * |
| FEV1 (L) | 1.46 ± 0.50 | 1.80 ± 0.57 | 0.1231 * |
| FEV1 (%) | 55.1 ± 15.26 | 60.7 ± 16.35 | 0.2974 * |
| FVC (L) | 2.70 ± 0.75 | 3.34 ± 0.75 | 0.0231 * |
| FVC (%) | 71.40 ± 14.77 | 78.40 ± 14.59 | 0.213 * |
| FEV1/FVC (%) | 54.50 ± 12.07 | 53.50 ± 10.72 | 0.7763 * |
| SGRQ (total) | 26.77 ± 14.14 | 21.21 ± 8.92 | 0.2648 * |
| SGRQ (sysptoms component) | 30.89 ± 12.77 | 30.32 ± 11.35 | 1 * |
| SGRQ (activity component) | 45.69 ± 22.10 | 33.37 ± 13.48 | 0.0541 * |
| SGRQ (impacts component) | 14.19 ± 13.05 | 11.01 ± 11.35 | 0.4043 * |
| EQ-5D (mobility) | 2.45 ± 0.83 | 2.25 ± 0.55 | 0.4211 * |
| EQ-5D (self-care) | 1.20 ± 0.52 | 1.05 ± 0.22 | 0.2985 * |
| EQ-5D (usual activities) | 1.80 ± 0.89 | 1.60 ± 0.60 | 0.7144 * |
| EQ-5D (pain/discomfort) | 1.60 ± 0.60 | 1.50 ± 0.51 | 0.6245 * |
| EQ-5D (anxiety/depression) | 1.25 ± 0.72 | 1.10 ± 0.31 | 0.6206 * |
| EQ-VAS | 66.65 ± 18.50 | 73.00 ± 11.85 | 0.2695 * |
| CMT + WM (n = 20) | WM (n = 20) | p-Value † | Effect Size | |||||
|---|---|---|---|---|---|---|---|---|
| Week 1 | Week 8 | Mean Difference | Week 1 | Week 8 | Mean Difference | |||
| 6MWD (m) | 348.45 ± 107.23 | 350.35 ± 106.90 | 1.90 (−20.00, 23.80) | 374.50 ± 102.18 | 373.55 ± 110.25 | −0.95 (−1.76, 39.86) | 0.7548 | 0.0407 |
| FEV1 (L) | 1.46 ± 0.50 | 1.48 ± 0.48 | 0.01 (−0.02, 0.05) | 1.80 ± 0.57 | 1.78 ± 0.54 | −0.02 (−0.07, 0.03) | 0.039 * | 0.3416 |
| FEV1 (%) | 55.1 ± 15.26 | 55.7 ± 14.77 | 0.60 (−0.83, 2.03 | 60.7 ± 16.35 | 60.4 ± 16.22 | −0.30 (−1.74, 1.14) | 0.1234 | 0.2936 |
| FVC (L) | 2.70 ± 0.75 | 2.70 ± 0.69 | 0.00 (−0.06, 0.06) | 3.34 ± 0.75 | 3.34 ± 0.71 | 0.00 (−0.06, 0.06) | 0.231 | 0.012 |
| FVC (%) | 71.40 ± 14.77 | 71.55 ± 13.75 | 0.15 (−1.28, 1.58) | 78.40 ± 14.59 | 78.60 ± 14.39 | 0.20 (−1.32, 1.72) | 0.3168 | 0.0159 |
| FEV1/FVC (%) | 54.50 ± 12.07 | 54.85 ± 12.56 | 0.35 (−0.35, 1.05) | 53.50 ± 10.72 | 53.10 ± 10.96 | −0.40 (−1.21, 0.41) | 0.5257 | 0.4638 |
| CAT | 16.15 ± 6.85 | 14.55 ± 6.17 | −1.60 (−4.17, 0.97) | 16.05 ± 4.63 | 16.80 ± 4.98 | 0.75 (−0.78, 2.28) | 0.6289 | 0.5198 |
| mMRC | 1.65 ± 0.99 | 1.60 ± 0.88 | 0.05 (−0.23, 0.13) | 1.60 ± 0.88 | 1.65 ± 0.88 | 0.05 (−0.23, 0.33) | 0.7129 | 0.1959 |
| VAS for dyspnea (mm) | 38.85 ± 24.07 | 36.25 ± 21.69 | 2.60 (−14.53, 9.33) | 38.70 ± 17.27 | 41.80 ± 20.21 | 3.10 (−4.11, 10.31) | 0.524 | |
| SGRQ (total) | 26.77 ± 14.14 | 24.86 ± 11.63 | −1.91 (−4.26, 0.43) | 21.21 ± 8.92 | 20.16 ± 7.57 | −1.05 (−3.81, 1.71) | 0.0603 | 0.1586 |
| SGRQ (symptoms component) | 30.89 ± 12.77 | 31.14 ± 11.74 | 0.24 (−2.08, 2.57) | 30.32 ± 11.35 | 30.30 ± 8.43 | −0.02 (−2.92, 2.89) | 1 | 0.0464 |
| SGRQ (activity component) | 45.69 ± 22.10 | 41.97 ± 18.56 | −3.72 (−8.02, 0.59) | 33.37 ± 13.48 | 34.03 ± 12.94 | 0.67 (−1.14, 2.47) | 0.0583 | 0.6207 |
| SGRQ (impacts component) | 14.19 ± 13.05 | 12.64 ± 9.96 | −1.55 (−4.27, 1.18 | 11.01 ± 11.35 | 8.61 ± 7.06 | −2.40 (−7.37, 2.57) | 0.5237 | 0.0996 |
| EQ-5D (mobility) | 2.45 ± 0.83 | 2.20 ± 0.52 | −0.25 (−0.62, 0.12) | 2.25 ± 0.55 | 2.15 ± 0.37 | −0.10 (−0.31, 0.11) | 0.654 | 0.2345 |
| EQ-5D (self-care) | 1.20 ± 0.52 | 1.10 ± 0.31 | −0.10 (−0.31, 0.11) | 1.05 ± 0.22 | 1.15 ± 0.37 | 0.10 (−0.04, 0.24) | 0.1117 | 0.521 |
| EQ-5D (usual activities) | 1.80 ± 0.89 | 1.60 ± 0.60 | −0.20 (−0.56, 0.16) | 1.60 ± 0.60 | 1.65 ± 0.59 | 0.05 (−0.27, 0.37) | 0.3301 | 0.3433 |
| EQ-5D (pain/discomfort) | 1.60 ± 0.60 | 1.60 ± 0.50 | 0.00 (−0.26, 0.26) | 1.50 ± 0.51 | 1.45 ± 0.51 | −0.05 (−0.29, 0.19) | 0.7824 | 0.0931 |
| EQ-5D (anxiety/depression) | 1.25 ± 0.72 | 1.10 ± 0.31 | −0.15 (−0.50, 0.20) | 1.10 ± 0.31 | 1.05 ± 0.22 | −0.05 (−0.15, 0.05) | 0.9793 | 0.1818 |
| EQ-VAS | 66.65 ± 18.50 | 71.50 ± 13.09 | 4.85 (−1.79, 11.49) | 73.00 ± 11.85 | 71.25 ± 11.34 | −1.75 (−5.86, 2.36) | 0.1254 | 0.5595 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Kwon, M.; Lee, B.-J.; Kim, K.-I.; Jung, H.-J. The Effectiveness and Safety of Chuna Manual Therapy Adjuvant to Western Medicine in Patients with Chronic Obstructive Pulmonary Disease: A Randomized, Single-Blind, Investigator-Initiated, Pilot Trial. Healthcare 2024, 12, 152. https://doi.org/10.3390/healthcare12020152
Park J, Kwon M, Lee B-J, Kim K-I, Jung H-J. The Effectiveness and Safety of Chuna Manual Therapy Adjuvant to Western Medicine in Patients with Chronic Obstructive Pulmonary Disease: A Randomized, Single-Blind, Investigator-Initiated, Pilot Trial. Healthcare. 2024; 12(2):152. https://doi.org/10.3390/healthcare12020152
Chicago/Turabian StylePark, Jiwon, Minji Kwon, Beom-Joon Lee, Kwan-Il Kim, and Hee-Jae Jung. 2024. "The Effectiveness and Safety of Chuna Manual Therapy Adjuvant to Western Medicine in Patients with Chronic Obstructive Pulmonary Disease: A Randomized, Single-Blind, Investigator-Initiated, Pilot Trial" Healthcare 12, no. 2: 152. https://doi.org/10.3390/healthcare12020152