
Comparative Effectiveness of Western and Eastern Manual Therapies for Chronic Obstructive Pulmonary Disease: A Systematic Review and Network Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Analysis and Synthesis
2.6.1. Conventional Pair-Wise Meta-Analysis
2.6.2. Network Meta-Analysis
2.7. Dealing with Missing Data
3. Results
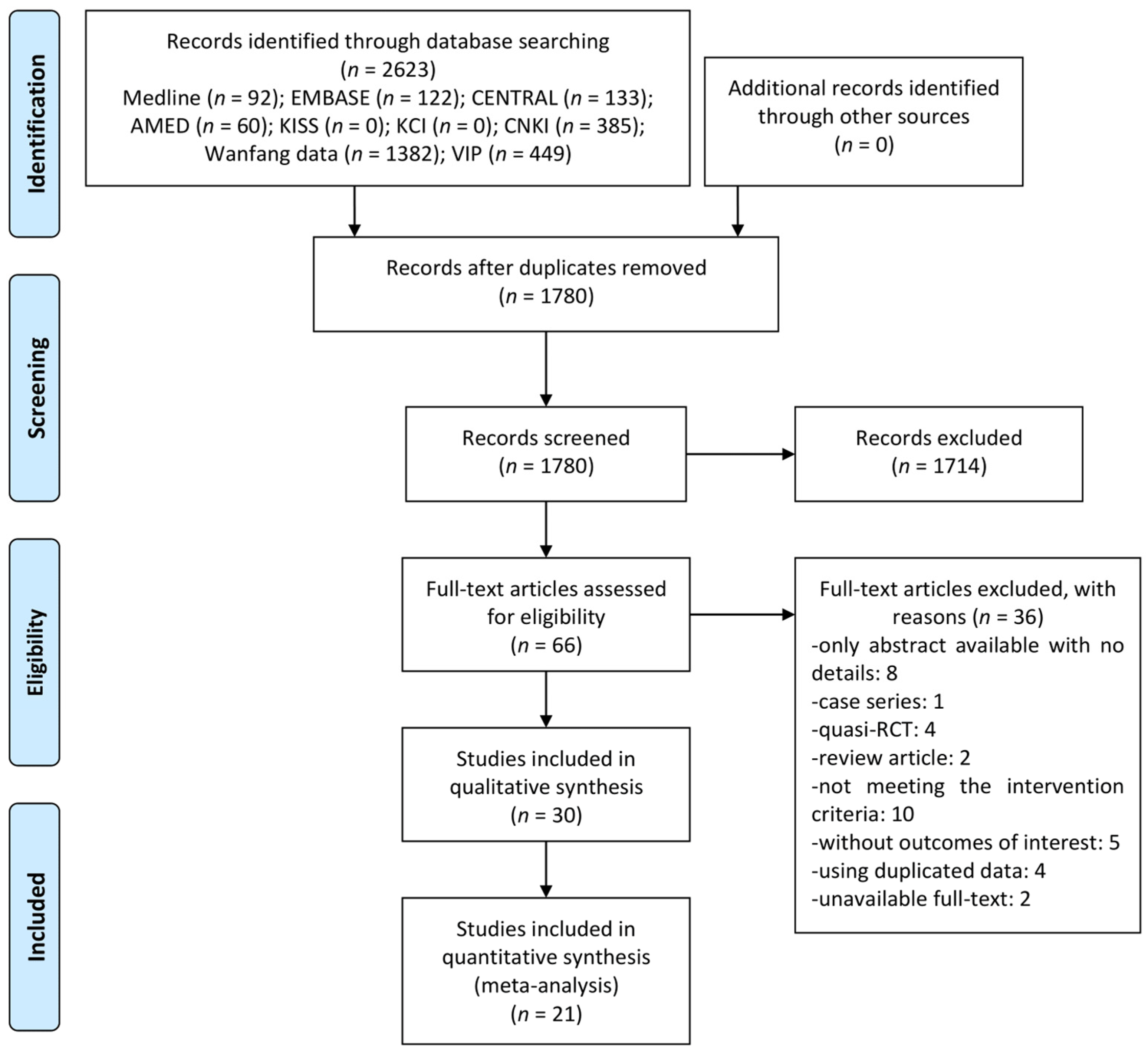
3.1. Study Selection
3.2. Study Characteristics
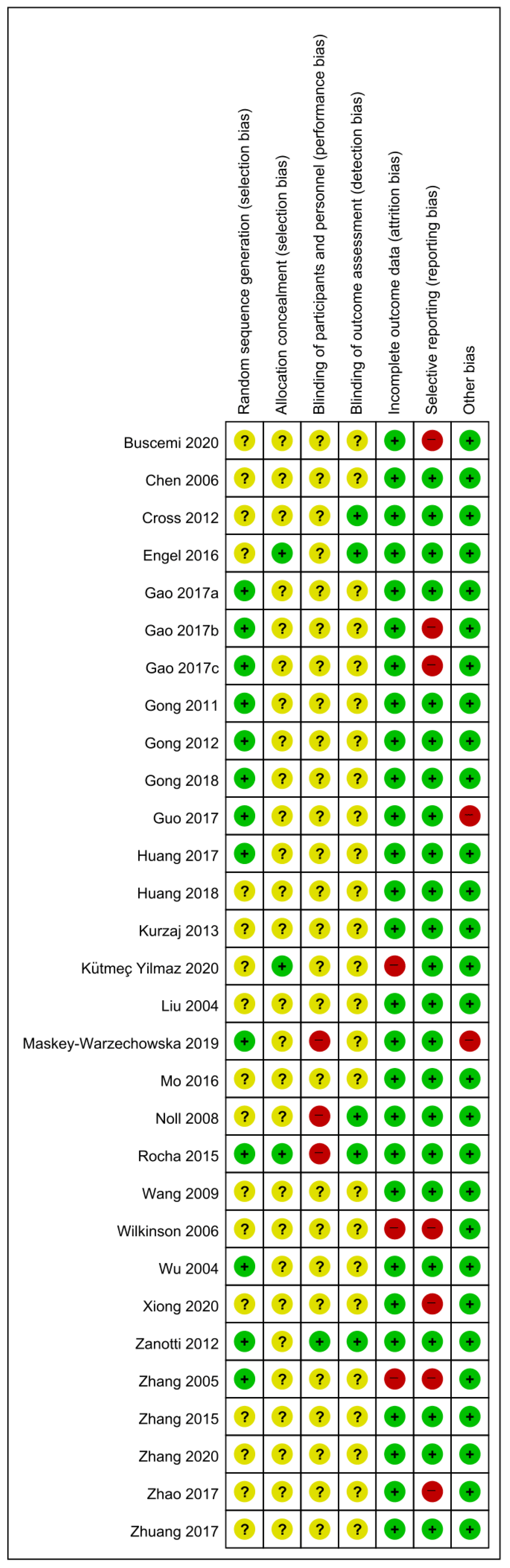
3.3. Risk of Bias Assessment
3.4. Effectiveness and Safety of Manual Therapies Using Pair-Wise Meta-Analysis
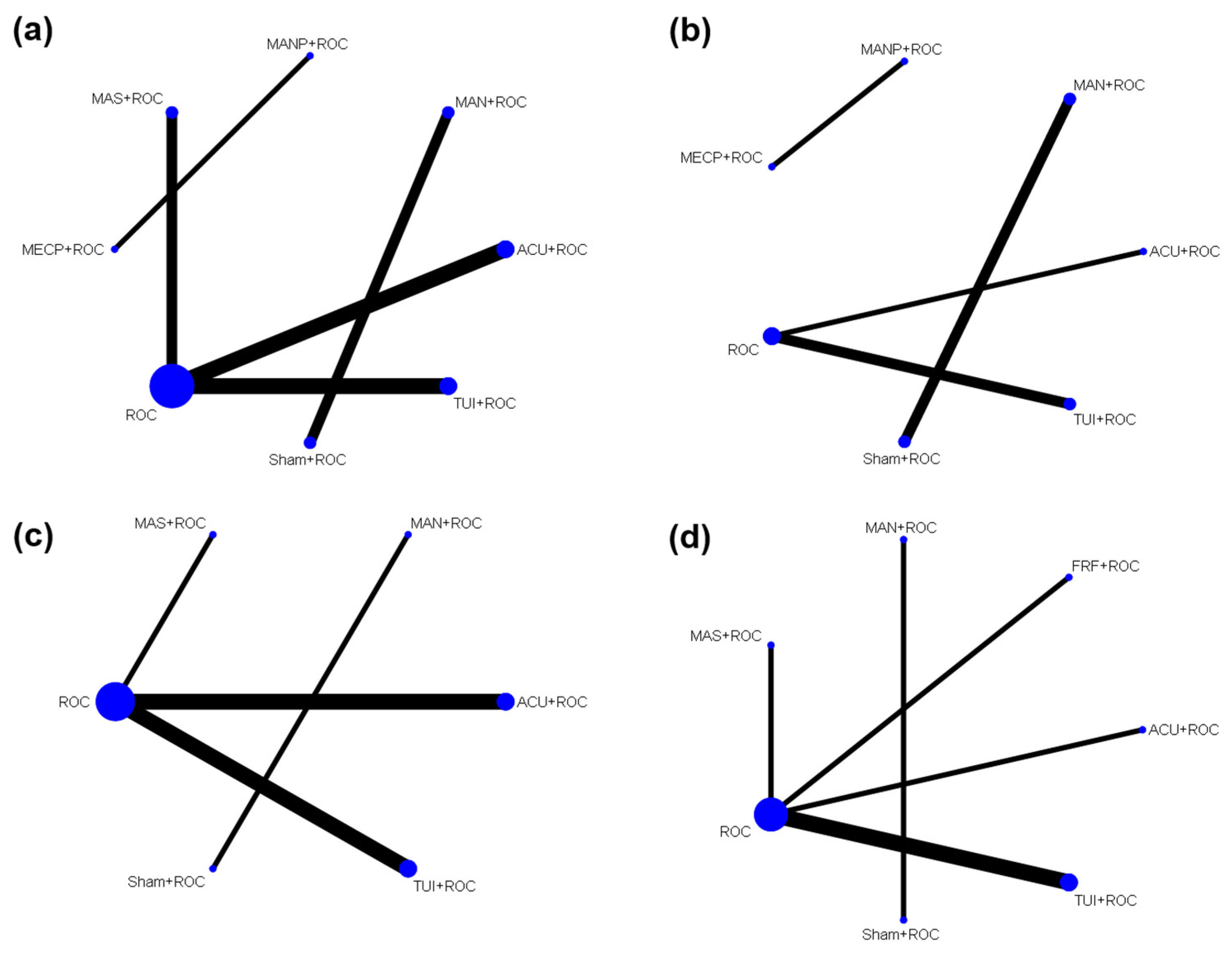
3.5. Comparative Effectiveness of Manual Therapies Using NMA
3.5.1. Lung Function
3.5.2. Exercise Capacity
4. Discussion
4.1. Summary of Evidence
4.2. Clinical Implications
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vestbo, J. COPD: Definition and phenotypes. Clin. Chest Med. 2014, 35, 1–6. [Google Scholar] [CrossRef]
- Diaz-Guzman, E.; Mannino, D.M. Epidemiology and prevalence of chronic obstructive pulmonary disease. Clin. Chest Med. 2014, 35, 7–16. [Google Scholar] [CrossRef]
- Iheanacho, I.; Zhang, S.; King, D.; Rizzo, M.; Ismaila, A.S. Economic burden of chronic obstructive pulmonary disease (COPD): A systematic literature review. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 439–460. [Google Scholar] [CrossRef]
- Nici, L.; Mammen, M.J.; Charbek, E.; Alexander, P.E.; Au, D.H.; Boyd, C.M.; Criner, G.J.; Donaldson, G.C.; Dreher, M.; Fan, V.S.; et al. Pharmacologic management of chronic obstructive pulmonary disease. An official American thoracic society clinical practice guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e56–e69. [Google Scholar] [CrossRef]
- Clarke, S.; Munro, P.E.; Lee, A.L. The role of manual therapy in patients with COPD. Healthcare 2019, 7, 21. [Google Scholar] [CrossRef]
- Simonelli, C.; Vitacca, M.; Vignoni, M.; Ambrosino, N.; Paneroni, M. Effectiveness of manual therapy in COPD: A systematic review of randomised controlled trials. Pulmonology 2019, 25, 236–247. [Google Scholar] [CrossRef]
- Wearing, J.; Beaumont, S.; Forbes, D.; Brown, B.; Engel, R. The use of spinal manipulative therapy in the management of chronic obstructive pulmonary disease: A systematic review. J. Altern. Complement. Med. 2016, 22, 108–114. [Google Scholar] [CrossRef]
- Chan, C.; Ho, P.S.; Chow, E. A body-mind-spirit model in health: An Eastern approach. Soc. Work. Health Care 2001, 34, 261–282. [Google Scholar] [CrossRef]
- Shim, J.M.; Kim, J. Cross-national differences in the holistic use of traditional East Asian medicine in East Asia. Health Promot. Int. 2018, 33, 536–544. [Google Scholar] [CrossRef]
- Park, T.Y.; Moon, T.W.; Cho, D.C.; Lee, J.H.; Ko, Y.S.; Hwang, E.H.; Heo, K.H.; Choi, T.Y.; Shin, B.C. An introduction to Chuna manual medicine in Korea: History, insurance coverage, education, and clinical research in Korean literature. Integr. Med. Res. 2014, 3, 49–59. [Google Scholar] [CrossRef]
- Singh, D.; Miravitlles, M.; Vogelmeier, C. Chronic Obstructive Pulmonary Disease Individualized Therapy: Tailored Approach to Symptom Management. Adv. Ther. 2017, 34, 281–299. [Google Scholar] [CrossRef] [PubMed]
- Tonin, F.S.; Rotta, I.; Mendes, A.M.; Pontarolo, R. Network meta-analysis: A technique to gather evidence from direct and indirect comparisons. Pharm. Pract. 2017, 15, 943. [Google Scholar] [CrossRef]
- Rouse, B.; Cipriani, A.; Shi, Q.; Coleman, A.L.; Dickersin, K.; Li, T. Network meta-analysis for clinical practice guidelines: A case study on first-line medical therapies for primary open-angle glaucoma. Ann. Intern. Med. 2016, 164, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ (Clin. Res. Ed.) 2021, 372, n160. [Google Scholar] [CrossRef]
- Higgins, J. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [Updated March 2011]. The Cochrane Collaboration. Available online: https://handbook-5-1.cochrane.org/ (accessed on 11 March 2021).
- Spineli, L.M.; Pandis, N. The importance of careful selection between fixed-effect and random-effects models. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 432–433. [Google Scholar] [CrossRef]
- Shim, S.; Yoon, B.H.; Shin, I.S.; Bae, J.M. Network meta-analysis: Application and practice using Stata. Epidemiol. Health 2017, 39, e2017047. [Google Scholar] [CrossRef]
- Buscemi, A.; Pennisi, V.; Rapisarda, A.; Pennisi, A.; Coco, M. Efficacy of osteopathic treatment in patients with stable moderate-to-severe chronic obstructive pulmonary disease: A randomized controlled pilot study. J. Complement. Integr. Med. 2020, 17, 20180128. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Zhong, L.W.; Liu, H.B.; Zhang, J.F.; Xie, G.G.; Jin, X.Q.; Zhou, X. Massage therapy for chronic obstructive pulmonary disease. Chin. J. Clin. Rehabil. 2006, 10, 10–12. [Google Scholar]
- Cross, J.L.; Elender, F.; Barton, G.; Clark, A.; Shepstone, L.; Blyth, A.; Bachmann, M.O.; Harvey, I. Evaluation of the effectiveness of manual chest physiotherapy techniques on quality of life at six months post exacerbation of COPD (MATREX): A randomised controlled equivalence trial. BMC Pulm. Med. 2012, 12, 33. [Google Scholar] [CrossRef] [PubMed]
- Engel, R.M.; Gonski, P.; Beath, K.; Vemulpad, S. Medium term effects of including manual therapy in a pulmonary rehabilitation program for chronic obstructive pulmonary disease (COPD): A randomized controlled pilot trial. J. Man. Manip. Ther. 2016, 24, 80–89. [Google Scholar] [CrossRef]
- Gao, L. Application effect of midnight-noon ebb-flow of acupoint massage timing in COPD patients with accumulation of phlegm-heat in lung. J. Nurs. Sci. 2017, 32, 41–43. [Google Scholar]
- Gao, L.; Sheng, H.; Zhu, Y. Application of mechanical-assisted expectoration combined with acupoint massage in nursing care of phlegm obstructing lung type of chronic obstructive pulmonary disease patients. Chin. Nurs. Res. 2017, 31, 182–185. [Google Scholar]
- Gao, L.; Tang, Y. Observation of effect of treating acute exacerbation of chronic obstructive pulmonary disease by applying midnight-midday ebb-flow acupoint massage. Chin. J. Pract. Nurs. 2017, 33, 689–692. [Google Scholar]
- Gong, H.; Chen, J. Effects of foot’s reflection area therapy on quality of life and pulmonary function of patients with stable COPD. J. Fujian Univ. TCM 2011, 21, 10–12. [Google Scholar]
- Gong, H.; Huang, M. The intervention effect of foot reflex zone massage for patients with stable COPD. J. Shenyang Med. Coll. 2018, 20, 407–409. [Google Scholar]
- Gong, H.R.; Zhuang, H.L.; Liu, Z.H. The impact of foot reflex zone therapy on exercise tolerance and dyspnea of stable COPD patients. J. Clin. Exp. Med. 2012, 11, 12–13, 15. [Google Scholar] [CrossRef]
- Guo, X.T.; Zhan, X.P.; Jin, X.Z.; Huang, Q.H.; Jin, C.C.; Hu, L.D.; Yu, N.N.; Qi, X. Effect of acupoint massage and respiratory function exercise on pulmonary function and quality of life of patients with chronic obstructive pulmonary disease in stable stage. Chin. Gen. Pract. 2017, 20, 345–347. [Google Scholar]
- Huang, M.C.; Gong, H.R.; Deng, Y.C. Rehabilitation effect of foot reflex zone massage on 60 patients with stable COPD with lung and spleen qi deficiency. Fujian Med. J. 2017, 39, 43–45. [Google Scholar]
- Huang, Y.L.; Feng, L.Y.; Lin, D.Y. Clinical observation on the effect of acupoint massage on pulmonary rehabilitation of COPD patients with lung-spleen-qi deficiency in the stable period. J. Front. Med. 2018, 8, 344–345. [Google Scholar] [CrossRef]
- Kurzaj, M.; Wierzejski, W.; Dor, A.; Stawska, J.; Rozek, K. The impact of specialized physiotherapy methods on BODE index in COPD patients during hospitalization. Adv. Clin. Exp. Med. 2013, 22, 721–730. [Google Scholar]
- Kütmeç Yilmaz, C.; Duru Aşiret, G.; Çetinkaya, F. The effect of back massage on physiological parameters, dyspnoea, and anxiety in patients with chronic obstructive pulmonary disease in the intensive care unit: A randomised clinical trial. Intensive Crit. Care Nurs. 2021, 63, 102962. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhou, Y.; Chen, Y.F. Study on effect of point massage on promoting sputum exclude in treatment of chronic obstructive pulmonary disease (COPD) during acute episode. Mod. Prev. Med. 2004, 31, 588–589. [Google Scholar]
- Maskey-Warzechowska, M.; Mierzejewski, M.; Gorska, K.; Golowicz, R.; Jesien, L.; Krenke, R. Effects of osteopathic manual therapy on hyperinflation in patients with chronic obstructive pulmonary disease: A randomized cross-over study. Adv. Exp. Med. Biol. 2019, 1222, 17–25. [Google Scholar] [CrossRef]
- Mo, F. Observation of Clinical Efficacy on Stable COPD (Lung and Kidney Qi Deficiency) by Replenishing Kidney Holding Qi Down. Master’s Thesis, Changchun University of Chinese Medicine, Changchun, China, 2016. [Google Scholar]
- Noll, D.R.; Degenhardt, B.F.; Johnson, J.C.; Burt, S.A. Immediate effects of osteopathic manipulative treatment in elderly patients with chronic obstructive pulmonary disease. J. Am. Osteopath. Assoc. 2008, 108, 251–259. [Google Scholar]
- Rocha, T.; Souza, H.; Brandão, D.C.; Rattes, C.; Ribeiro, L.; Campos, S.L.; Aliverti, A.; de Andrade, A.D. The manual diaphragm release technique improves diaphragmatic mobility, inspiratory capacity and exercise capacity in people with chronic obstructive pulmonary disease: A randomised trial. J. Physiother. 2015, 61, 182–189. [Google Scholar] [CrossRef]
- Wang, X.Y.; Wu, X.H.; Cao, C.F.; Liu, X.H. A comparative study on the effect of different sputum excretion methods on patients with COPD and pulmonary infection. World Health Dig. Med. Period. 2009, 6, 39–40. [Google Scholar] [CrossRef]
- Wilkinson, I.S.A.; Prigmore, S.; Rayner, C.F. A randomised-controlled trail examining the effects of reflexology of patients with chronic obstructive pulmonary disease (COPD). Complement. Ther. Clin. Pract. 2006, 12, 141–147. [Google Scholar] [CrossRef]
- Wu, H.S.; Wu, S.C.; Lin, J.G.; Lin, L.C. Effectiveness of acupressure in improving dyspnoea in chronic obstructive pulmonary disease. J. Adv. Nurs. 2004, 45, 252–259. [Google Scholar] [CrossRef]
- Xiong, Y.; Yang, F. Study on the application of mechanical sputum drainage combined with acupoint massage in the nursing of patients with phlegm turbid and dammed lung type chronic obstructive pulmonary disease. Chin. Foreign Med. Res. 2020, 18, 90–92. [Google Scholar]
- Zanotti, E.; Berardinelli, P.; Bizzarri, C.; Civardi, A.; Manstretta, A.; Rossetti, S.; Fracchia, C. Osteopathic manipulative treatment effectiveness in severe chronic obstructive pulmonary disease: A pilot study. Complement. Ther. Med. 2012, 20, 16–22. [Google Scholar] [CrossRef]
- Zhang, J.F.; Zong, L.W.; Liu, H.B.; Chen, Q. Treatment of chronic obstructive pulmonary disease in remission stage by tuina. J. Acupunct. Tuina Sci. 2005, 3, 44–47. [Google Scholar]
- Zhang, W. Study on the effect of massage therapy on chronic obstructive pulmonary disease. Guide China Med. 2015, 13, 195. [Google Scholar]
- Zhang, X.; Huang, Y.; Zhang, D. The application of acupoint massage combined with respiratory function exercise in patients with stable chronic obstructive pulmonary disease. Guangming J. Chin. Med. 2020, 35, 557–559. [Google Scholar]
- Zhao, L. Application of mechanical assisted expectoration combined with acupoint massage in the nursing of patients with chronic obstructive pulmonary disease. J. Aerosp. Med. 2017, 28, 1410–1411. [Google Scholar]
- Zhuang, Y. Observation on the effect of comprehensive rehabilitation nursing in improving lung function of elderly patients with chronic obstructive pulmonary disease. J. Contemp. Clin. Med. 2017, 30, 2788–2790. [Google Scholar] [CrossRef]
- Vu, G.V.; Ha, G.H.; Nguyen, C.T.; Vu, G.T.; Pham, H.Q.; Latkin, C.A.; Tran, B.X.; Ho, R.C.M.; Ho, C.S.H. Interventions to Improve the Quality of Life of Patients with Chronic Obstructive Pulmonary Disease: A Global Mapping During 1990–2018. Int. J. Environ. Res. Public Health 2020, 17, 3089. [Google Scholar] [CrossRef]
- Li, T.; Li, X.; Huang, F.; Tian, Q.; Fan, Z.Y.; Wu, S. Clinical Efficacy and Safety of Acupressure on Low Back Pain: A Systematic Review and Meta-Analysis. Evidence-Based Complement. Altern. Med. eCAM 2021, 2021, 8862399. [Google Scholar] [CrossRef]
- Lee, E.J.; Frazier, S.K. The efficacy of acupressure for symptom management: A systematic review. J. Pain Symptom Manag. 2011, 42, 589–603. [Google Scholar] [CrossRef]
- Feng, G.; Han, M.; Li, X.; Geng, L.; Miao, Y. Clinical effectiveness of Tui Na for insomnia compared with estazolam: A systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med. 2019, 47, 102186. [Google Scholar] [CrossRef]
- Sterne, J.A.; Gavaghan, D.; Egger, M. Publication and related bias in meta-analysis: Power of statistical tests and prevalence in the literature. J. Clin. Epidemiol. 2000, 53, 1119–1129. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| First Author (Year), Country | Sample Size (Included →Analyzed) | Mean Age (Year) | Diagnosis | (A) Treatment Intervention | (B) Control Intervention | Duration of Treatment/Follow-Up | Outcome of Interest |
|---|---|---|---|---|---|---|---|
| Stable COPD | |||||||
| Noll (2008), USA | 35(18:17)→35(18:17) | (A) 69.6 ± 6.6 (B) 72.2 ± 7.1 | Known COPD history, FEV1/FVC < 70% | Osteopathic manipulative treatment | Sham (light touch) | 20 min one session/none | 1. FEV1 (L); 2. FVC (L); 3. FEV1/FVC (%); 4. Adverse events |
| Zanotti (2012), Italy | 20(10:10)→20(10:10) | (A) 63.5 ± 4.7 (B) 64.2 ± 5.5 | GOLD | Osteopathic manipulative treatment | Sham (light touch) | 45 min once a week for 4 weeks/none | 1. VC (L); 2. FEV1 (L); 3. FVC (L); 4. 6MWD (m); 5. Adverse events |
| Maskey-Warzechowska (2019), Poland | 38(19:19)→38(19:19) | 68 | Severe-very severe (FEV1 < 50%), GOLD 2016 | Osteopathic manipulative treatment | Sham | 25 min one session/none | Note. Only median (IQR) value was reported. 1. FEV1 (L, %pv); 2. FVC (L, %pv); 3. FEV1/FVC (%); 4. VAS (dyspnea); 5. Adverse events |
| Buscemi (2020), Italy | 32→32 | 71 | Moderate-severe COPD | Osteopathic manipulative treatment + (B) | Conventional pharmacotherapy | once a week for 8 weeks/15 days | Note. Raw data were not reported except adverse events. 1. FVC (L); 2. FEV1 (L); 3. CAT; 4. 6MWD (m); 5. Adverse events |
| Rocha (2015), Brazil | 20(11:9)→19(10:9) | (A) 71 ± 5 (B) 71 ± 6 | GOLD 2011 | Manual diaphragm release technique | Sham (light touch) | 6 times on non-consecutive days within 2 weeks/none | Note. Only change value was reported. 1. 6MWD (m) |
| AECOPD | |||||||
| Kurzaj (2013), Poland | 30(20:10)→30(20:10) | (A) 57 (B) 55 | NR | Massage + (B) | Basic physiotherapy (Respirometric training) | 30 min daily for 6 days/none | 1. FEV1 (L, %pv); 2. 6MWD (m); 3. MRC; 4. BODE index |
| Cross (2012), UK | 522(258:264)→372(186:186) | (A) 69.08 ± 9.85 (B) 69.58 ± 9.51 | NR | Manual chest technique + (B) | Breathing technique | 1–41 min, total 1–21 sessions/6 mon | Note. Raw data of sputum volume and SpO2 were not reported. 1. SGRQ; 2. Breathlessness Cough and Sputum Scale; 3. EQ-5D; 4. EQ-VAS; 5. Sputum volume (mL); 6. SpO2; 7. Hospitalization period; 8. Adverse events |
| Wang (2009), China | 120(60:60)→120(60:60) | NR | NR | Manual percussion | Mechanical percussion | twice a day for 7 days/none | 1. Sputum excretion (mL); 2. SpO2; 3. Hospitalization period; 4. Time to improvement/disappearance of cough, dyspnea, and sputum sound in lungs; 5. FVC (L); 6. FEV1 (L) |
| Unclear COPD | |||||||
| Engel (2016), Australia | 33(9:9:15)→31(8:8:15) | (A1) 67.6 ± 3.5 (A2) 65.0 ± 4.1 (B) 64.5 ± 4.1 | NR | (A1) Massage + (B) (A2) Massage + Spinal manipulation + (B) | Pulmonary rehabilitation | twice a week for 8 weeks/none | Note. Only change value was reported. 1. FEV1 (L); 2. FVC (L); 3. SGRQ; 4. 6MWD (m); 5. Adverse events |
| Zhuang (2017), China | 70(35:35)→70(35:35) | (A) 64.98 ± 4.98 (B) 65.23 ± 5.25 | NR | Massage + (B) | Routine care (medication, exercise education, diet education, etc.) | NR/none | 1. FEV1 (L); 2. FEV1/FVC (%); 3. TER (respiratory symptom) |
| Kütmeç Yilmaz (2020), Turkey | 91(49:42)→58(28:30) | 70.6 | NR | Back massage + (B) | Routine care | 15 min, daily for 4 days/none | Note. Only median (IQR) value was reported. 1. SpO2 |
| First Author (Year), Country | Sample Size (Included→Analyzed) | Mean Age (Year) | Diagnosis | (A) Treatment Intervention | (B) Control Intervention | Duration of Treatment/Follow-Up | Outcome of Interest |
|---|---|---|---|---|---|---|---|
| Stable COPD | |||||||
| Guo (2017), China | 200(100:100)→200(100:100) | NR | Criteria used by associations or guidelines in China | Acupressure + (B) | Basic physiotherapy (Respirometric training) | 2–3 min per acupoint, once a day for 6 mon/none | 1. FEV1 (L); 2. FEV1/FVC (%); 3. SGRQ |
| Huang (2018), China | 68(34:34)→68(34:34) | (A) 52.43 ± 3.96 (B) 54.43 ± 1.27 | COPD | Acupressure + (B) | Basic physiotherapy (Respirometric training) | 2 min per acupoint twice a day for 3 mon/none | 1. FEV1 (L, %pv); 2. FEV1/FVC (%); 3. 6MWD (m); 4. CAT |
| Zhang (2020), China | 90(45:45)→90(45:45) | (A) 67.46 ± 5.23 (B) 67.85 ± 5.62 | Criteria used by associations or guidelines in China | Acupressure + (B) | Basic physiotherapy (Respirometric training) | 2–3 min per acupoint once a day for 6 mon/none | 1. FVC (L); 2. FEV1 (L); 3. FEV1/FVC (%) |
| Wilkinson (2006), UK | 14(7:7)→14(7:7) | (A) 77 (B) 75 | Moderate–severe COPD | Foot reflexology | No intervention | 50 min once a week for 4 weeks/none | Note. Raw data were not reported. 1. Quality of life (questionnaire); 2. SpO2 |
| Gong (2011), China | 60(30:30)→60(30:30) | (A) 67.03 ± 9.48 (B) 69.93 ± 8.18 | Criteria used by associations or guidelines in China | Foot reflexology + (B) | Health education | 30 min once a day for 3 mon/none | Note. Only change value was reported. 1. SGRQ; 2. FEV1 (L, %pv); 3. FEV1/FVC (%) |
| Gong (2012), China | 60(30:30)→60(30:30) | (A) 67.03 ± 9.48 (B) 69.93 ± 8.18 | Criteria used by associations or guidelines in China | Foot reflexology + (B) | Health education | 30 min once a day for 3 mon/none | Note. On 6MWD and MRC, only change values were reported. 1. 6MWD (m); 2. MRC; 3. TER (respiratory symptom) |
| Huang (2017), China | 60(30:30)→59(29:30) | (A) 69.52 ± 4.31 (B) 69.37 ± 4.56 | Criteria used by associations or guidelines in China | Foot reflexology + (B) | Health education | 30 min once a day for 6 mon/none | 1. 6MWD (m) |
| Gong (2018), China | 60(30:30)→59(29:30) | (A) 69.52 ± 4.31 (B) 69.37 ± 4.56 | Criteria used by associations or guidelines in China | Foot reflexology + (B) | Health education | 30 min once a day for 6 mon/none | Note. Only change value was reported. 1. BODE index; 2. 6MWD (m); 3. modified MRC; 4. FEV1 (%) |
| Zhang (2005), China | 66(33:33)→63(31:32) | (A) 68.3 ± 6.79 (B) 67.7 ± 7.92 | Criteria used by associations or guidelines in China | Tuina | Basic physiotherapy (Respirometric training) | 20 min 3 times a week for 3 mon/none | 1. FVC (%); 2. FEV1 (L); 3. FEV1/FVC (%); 4. 6MWD (m); 5. TER (SGRQ); 6. Quality of life (questionnaire) |
| Chen (2006), China | 30(15:15)→30(15:15) | (A) 69.12 ± 6.21 (B) 67.63 ± 7.01 | Criteria used by associations or guidelines in China | Tuina + (B) | Conventional pharmacotherapy | 20 min 5 times a week for 8 weeks/none | 1. TER (dyspnea); 2. FEV1/FVC (%); 3. FEV1 (L); 4. FVC (L); 5. 6MWD (m) |
| Mo (2016), China | 60(30:30)→57(29:28) | (A) 56.5 ± 6.2 (B) 58.4 ± 5.6 | Criteria used by associations or guidelines in China | Tuina + (B) | Conventional pharmacotherapy | 6 times a week for 4 weeks/none | 1. CAT; 2. 6MWD (m); 3. Adverse events |
| AECOPD | |||||||
| Liu (2004), China | 127(64:63) | (A) 65.33 ± 4.44 (B) 64.49 ± 5.63 | Criteria used by associations or guidelines in China | Acupressure + (B) | Routine care | 1hr once a day for 7 days/none | 1. TER (respiratory symptom); 2. Time to improve cough, sputum, and dyspnea; 3. PaO2; 4. PaCO2 |
| Gao (2017a), China | 60(30:30)→60(30:30) | (A) 66.65 ± 3.70 (B) 68.77 ± 4.28 | Criteria used by associations or guidelines in China | Acupressure + (B) | Routine care | 1 min per acupoint for 10 min twice a day for 7 days/none | 1. TER (respiratory symptom); 2. Symptom score (cough, sputum, wheezing, shortness of breath); 3. PaO2; 4. PaCO2; 5. SaO2 |
| Gao (2017b), China | 60(30:30)→60(30:30) | (A) 70.5 ± 4. (B) 68.5 ± 4.7 | Criteria used by associations or guidelines in China | Acupressure + (B) | Routine care | 20 min twice a day for 7 days/none | 1. Sputum excretion (mL); 2. SpO2; 3. PaO2; 4. PaCO2 |
| Gao (2017c), China | 60(30:30)→60(30:30) | (A) 69.36 ± 5.65 (B) 70.84 ± 4.76 | Criteria used by associations or guidelines in China | Acupressure + (B) | Routine care | 15 min twice a day for 7 days/none | 1. Symptom score (cough, sputum, asthma, dyspnea); 2. PaO2; 3. PaCO2; 4. SaO2; 5. TER (respiratory symptom); 6. Hospitalization period |
| Zhao (2017), China | 58(29:29)→58(29:29) | (A) 67.5 ± 3.6 (B) 68.5 ± 4.1 | NR | Acupressure + (B) | Routine care | 10 min twice a day for 7 days/none | 1. Sputum excretion (mL); 2. SpO2; 3. PaO2; 4. PaCO2 |
| Unclear COPD | |||||||
| Wu (2004), Taiwan | 44(22:22)→44(22:22) | 73 ± 9.7 | NR | Acupressure | Sham (unrelated acupoint) | 16 min five times a week for 4 weeks/none | Note. Only change value was reported. 1. 6MWD (m); 2. SpO2 |
| Xiong (2020), China | 120(60:60)→120(60:60) | (A) 50.89 ± 4.58 (B) 55.72 ± 4.54 | NR | Acupressure + (B) | Routine care | 30 min twice a day for 1 mon/none | 1. TER (respiratory symptom); 2. Sputum excretion (mL) |
| Zhang (2015), China | 80(40:40)→80(40:40) | (A) 45 ± 2.5 (B) 43 ± 3.4 | Criteria used by associations or guidelines in China | Tuina + (B) | Routine care (medication) | ~25 min five times a week for 7 weeks/none | 1. TER (respiratory symptom); 2. FEV1/FVC (%); 3. FEV1 (L); 4. FVC (L) |
| ROC | 0.04 (−0.48, 0.55) | 0.74 (0.08, 1.40) | 0.09 (−0.46, 0.65) |
| 0.33 (0.17, 0.49) | ACU + ROC | 0.70 (−0.13, 1.54) | 0.05 (−0.70, 0.81) |
| MAS + ROC | −0.65 (−1.51, 0.21) | ||
| 0.26 (−0.05, 0.58) | −0.07 (−0.42, 0.28) | TUI + ROC |
| ROC | 0.82 (−3.50, 5.14) | 20.00 (12.16, 27.84) | 3.01 (−1.68, 7.69) | |
| 14.38 (−12.74, 41.50) | ACU + ROC | 19.18 (10.23, 28.13) | 2.19 (−4.18, 8.56) | |
| 36.08 (−1.14, 73.30) | 21.70 (−24.35, 67.75) | FRF + ROC | ||
| 56.20 (−12.84, 125.24) | 41.82 (−32.36, 116.00) | 20.12 (−58.31, 98.55) | MAS + ROC | −16.99 (−26.13, −7.86) |
| 49.49 (25.60, 73.38) | 35.11 (−1.03, 71.26) | 13.41 (−30.81, 57.64) | −6.71 (−79.77, 66.35) | TUI + ROC |
| Interventions | FEV1 (L) | FVC (L) | FEV1/FVC (%) | 6MWD (m) |
|---|---|---|---|---|
| ROC | 27.9 | 2.5 | 15.4 | 6 |
| ACU + ROC | 35.1 | 82.4 | 29.9 | 30 |
| FRF + ROC | 59.5 | |||
| MAS + ROC | 95.6 | 100 | 76.5 | |
| TUI + ROC | 41.4 | 65.1 | 54.7 | 78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, C.-Y.; Lee, B.; Lee, B.-J.; Kim, K.-I.; Jung, H.-J. Comparative Effectiveness of Western and Eastern Manual Therapies for Chronic Obstructive Pulmonary Disease: A Systematic Review and Network Meta-Analysis. Healthcare 2021, 9, 1127. https://doi.org/10.3390/healthcare9091127
Kwon C-Y, Lee B, Lee B-J, Kim K-I, Jung H-J. Comparative Effectiveness of Western and Eastern Manual Therapies for Chronic Obstructive Pulmonary Disease: A Systematic Review and Network Meta-Analysis. Healthcare. 2021; 9(9):1127. https://doi.org/10.3390/healthcare9091127
Chicago/Turabian StyleKwon, Chan-Young, Boram Lee, Beom-Joon Lee, Kwan-Il Kim, and Hee-Jae Jung. 2021. "Comparative Effectiveness of Western and Eastern Manual Therapies for Chronic Obstructive Pulmonary Disease: A Systematic Review and Network Meta-Analysis" Healthcare 9, no. 9: 1127. https://doi.org/10.3390/healthcare9091127