
Does the Mediterranean Dietary Pattern Promote Lower Sodium Urinary Excretion in Children?

 ,
,  , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Methods & Materials
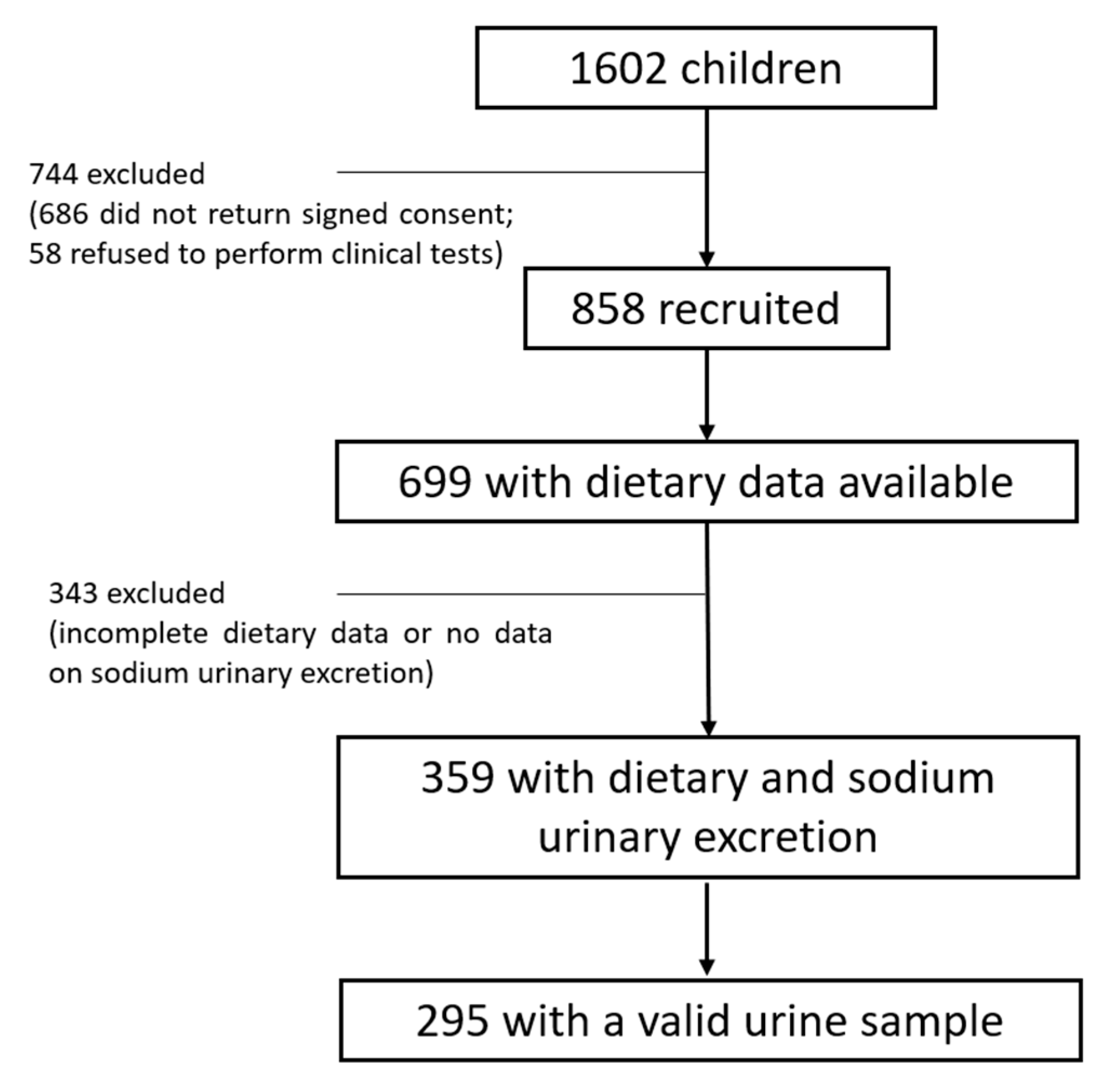
2.1. Participants and Study Design
2.2. Participants Assessment
2.2.1. Diet Quality and Dietary Evaluation
2.2.2. Urine Collection—24 h
2.2.3. Covariates
2.2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wójcik, M.; Kozioł-Kozakowska, A. Obesity, Sodium Homeostasis, and Arterial Hypertension in Children and Adolescents. Nutrients 2021, 13, 4032. [Google Scholar] [CrossRef]
- Appel, L.J.; Lichtenstein, A.H.; Callahan, E.A.; Sinaiko, A.; Van Horn, L.; Whitsel, L. Reducing Sodium Intake in Children: A Public Health Investment. J. Clin. Hypertens. 2015, 17, 657–662. [Google Scholar] [CrossRef]
- Song, P.; Zhang, Y.; Yu, J.; Zha, M.; Zhu, Y.; Rahimi, K.; Rudan, I. Global Prevalence of Hypertension in Children: A Systematic Review and Meta-analysis. JAMA Pediatr. 2019, 173, 1154–1163. [Google Scholar] [CrossRef]
- World Health Organization. Guideline: Sodium Intake for Adults and Children; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- EFSA Panel on Nutrition; Novel Foods and Food Allergens (NDA); Turck, D.; Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.-I.; Kearney, J.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; et al. Dietary reference values for sodium. EFSA J. 2019, 17, e05778. [Google Scholar]
- Ozemek, C.; Laddu, D.R.; Arena, R.; Lavie, C.J. The role of diet for prevention and management of hypertension. Curr. Opin. Cardiol. 2018, 33, 388–393. [Google Scholar] [CrossRef]
- De Pergola, G.; D’Alessandro, A. Influence of Mediterranean Diet on Blood Pressure. Nutrients 2018, 10, 1700. [Google Scholar] [CrossRef]
- Russo, G.L.; Siani, A.; Fogliano, V.; Geleijnse, J.M.; Giacco, R.; Giampaoli, S.; Iacoviello, L.; Kromhout, D.; Lionetti, L.; Naska, A.; et al. The Mediterranean diet from past to future: Key concepts from the second “Ancel Keys” International Seminar. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 717–732. [Google Scholar] [CrossRef]
- Hidalgo-Mora, J.J.; García-Vigara, A.; Sánchez-Sánchez, M.L.; García-Pérez, M.; Tarín, J.; Cano, A. The Mediterranean diet: A historical perspective on food for health. Maturitas 2020, 132, 65–69. [Google Scholar] [CrossRef]
- Koumpagioti, D.; Boutopoulou, B.; Moriki, D.; Priftis, K.N.; Douros, K. Does Adherence to the Mediterranean Diet Have a Protective Effect against Asthma and Allergies in Children? A Systematic Review. Nutrients 2022, 14, 1618. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet: A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- Finicelli, M.; Di Salle, A.; Galderisi, U.; Peluso, G. The Mediterranean Diet: An Update of the Clinical Trials. Nutrients 2022, 14, 2956. [Google Scholar] [CrossRef] [PubMed]
- Katidi, A.; Vlassopoulos, A.; Noutsos, S.; Kapsokefalou, M. Ultra-Processed Foods in the Mediterranean Diet according to the NOVA Classification System: A Food Level Analysis of Branded Foods in Greece. Foods 2023, 12, 1520. [Google Scholar] [CrossRef]
- Mirmiran, P.; Gaeini, Z.; Bahadoran, Z.; Ghasemi, A.; Norouzirad, R.; Tohidi, M.; Azizi, F. Urinary sodium-to-potassium ratio: A simple and useful indicator of diet quality in population-based studies. Eur. J. Med. Res. 2021, 26, 3. [Google Scholar] [CrossRef]
- Vasara, E.; Marakis, G.; Breda, J.; Skepastianos, P.; Hassapidou, M.; Kafatos, A.; Rodopaios, N.; Koulouri, A.A.; Cappuccio, F.P. Sodium and Potassium Intake in Healthy Adults in Thessaloniki Greater Metropolitan Area-The Salt Intake in Northern Greece (SING) Study. Nutrients 2017, 9, 417. [Google Scholar] [CrossRef]
- Magriplis, E.; Farajian, P.; Pounis, G.D.; Risvas, G.; Panagiotakos, D.B.; Zampelas, A. High sodium intake of children through ‘hidden’ food sources and its association with the Mediterranean diet: The GRECO study. J. Hypertens. 2011, 29, 1069–1076. [Google Scholar] [CrossRef]
- Kanauchi, M.; Kanauchi, K. Development of a Mediterranean diet score adapted to Japan and its relation to obesity risk. Food Nutr. Res. 2016, 60, 32172. [Google Scholar] [CrossRef]
- La Verde, M.; Mulè, S.; Zappalà, G.; Privitera, G.; Maugeri, G.; Pecora, F.; Marranzano, M. Higher adherence to the Mediterranean diet is inversely associated with having hypertension: Is low salt intake a mediating factor? Int. J. Food Sci. Nutr. 2018, 69, 235–244. [Google Scholar] [CrossRef]
- Mendes, F.C.; Paciência, I.; Cavaleiro Rufo, J.; Farraia, M.; Silva, D.; Padrão, P.; Delgado, L.; Garcia-Larsen, V.; Moreira, A.; Moreira, P. Higher diversity of vegetable consumption is associated with less airway inflammation and prevalence of asthma in school-aged children. Pediatr. Allergy Immunol. 2021, 32, 925–936. [Google Scholar] [CrossRef]
- Walker, J.L.; Ardouin, S.; Burrows, T. The validity of dietary assessment methods to accurately measure energy intake in children and adolescents who are overweight or obese: A systematic review. Eur. J. Clin. Nutr. 2018, 72, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Barros, R.; Moreira, A.; Fonseca, J.; de Oliveira, J.F.; Delgado, L.; Castel-Branco, M.G.; Haahtela, T.; Lopes, C.; Moreira, P. Adherence to the Mediterranean diet and fresh fruit intake are associated with improved asthma control. Allergy 2008, 63, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.M.; Willett, W.C. Trends in 24-h urinary sodium excretion in the United States, 1957–2003: A systematic review. Am. J. Clin. Nutr. 2010, 92, 1172–1180. [Google Scholar] [CrossRef] [PubMed]
- Remer, T.; Neubert, A.; Maser-Gluth, C. Anthropometry-based reference values for 24-h urinary creatinine excretion during growth and their use in endocrine and nutritional research. Am. J. Clin. Nutr. 2002, 75, 561–569. [Google Scholar] [CrossRef]
- Chen, S.L.; Dahl, C.; Meyer, H.E.; Madar, A.A. Estimation of Salt Intake Assessed by 24-Hour Urinary Sodium Excretion among Somali Adults in Oslo, Norway. Nutrients 2018, 10, 900. [Google Scholar] [CrossRef]
- Kuczmarski, R.J.; Ogden, C.L.; Grummer-Strawn, L.M.; Flegal, K.M.; Guo, S.S.; Wei, R.; Mei, Z.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. CDC Growth Charts: United States; Department of Health and Human Services: Washington, DC, USA, 2000; pp. 1–27. [Google Scholar]
- Elsenburg, L.K.; Rieckmann, A.; Nguyen, T.-L.; Bengtsson, J.; Andersen, A.-M.N.; Taylor-Robinson, D.; Lange, T.; Rod, N.H. Mediation of the parental education gradient in early adult mortality by childhood adversity: A population-based cohort study of more than 1 million children. Lancet Public Health 2022, 7, e146–e155. [Google Scholar] [CrossRef]
- Viroli, G.; Gonçalves, C.; Pinho, O.; Silva-Santos, T.; Padrão, P.; Moreira, P. High Adherence to Mediterranean Diet Is Not Associated with an Improved Sodium and Potassium Intake. Nutrients 2021, 13, 4151. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Bes-Rastrollo, M.; Román-Viñas, B.; Pfrimer, K.; Sánchez-Villegas, A.; Martínez-González, M.A. Dietary patterns and nutritional adequacy in a Mediterranean country. Br. J. Nutr. 2009, 101 (Suppl. S2), S21–S28. [Google Scholar] [CrossRef]
- Charlton, K.; Ware, L.J.; Chidumwa, G.; Cockeran, M.; Schutte, A.E.; Naidoo, N.; Kowal, P. Prediction of 24-hour sodium excretion from spot urine samples in South African adults: A comparison of four equations. J. Human. Hypertens. 2020, 34, 24–33. [Google Scholar] [CrossRef]
- Schröder, H.; Schmelz, E.; Marrugat, J. Relationship between diet and blood pressure in a representative Mediterranean population. Eur. J. Nutr. 2002, 41, 161–167. [Google Scholar] [CrossRef]
- Psaltopoulou, T.; Naska, A.; Orfanos, P.; Trichopoulos, D.; Mountokalakis, T.; Trichopoulou, A. Olive oil, the Mediterranean diet, and arterial blood pressure: The Greek European Prospective Investigation into Cancer and Nutrition (EPIC) study. Am. J. Clin. Nutr. 2004, 80, 1012–1018. [Google Scholar] [CrossRef] [PubMed]
- Gowrishankar, M.; Blair, B.; Rieder, M.J. Dietary intake of sodium by children: Why it matters. Paediatr. Child Health 2020, 25, 47–61. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; He, F.J.; MacGregor, G.A. High salt intake: Independent risk factor for obesity? Hypertension 2015, 66, 843–849. [Google Scholar] [CrossRef]
- Zuccarelli, M.T.; Faraj, L. Sodium and potassium content of some fresh, frozen and canned vegetables. Arch. Latinoam. Nutr. 1986, 36, 477–482. [Google Scholar]
- Aboul-Enein, B.H.; Puddy, W.C.; Bernstein, J. Ancel Benjamin Keys (1904–2004): His early works and the legacy of the modern Mediterranean diet. J. Med. Biogr. 2020, 28, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Zaragoza-Martí, A.; Cabañero-Martínez, M.J.; Hurtado-Sánchez, J.A.; Laguna-Pérez, A.; Ferrer-Cascales, R. Evaluation of Mediterranean diet adherence scores: A systematic review. BMJ Open 2018, 8, e019033. [Google Scholar] [CrossRef]
- Francesco, P.C.; Chen, J.; Chiara, D.; Luigi, P.; Renato, I.; Diego, V.; Simona, G.; Pasquale, S. Geographic and socioeconomic variation of sodium and potassium intake in Italy: Results from the MINISAL-GIRCSI programme. BMJ Open 2015, 5, e007467. [Google Scholar]
- Moreira, S.; Moreira, P.; Sousa, A.S.; Guerra, R.S.; Afonso, C.; Santos, A.; Borges, N.; Amaral, T.F.; Padrão, P. Urinary Sodium Excretion and Adherence to the Mediterranean Diet in Older Adults. Nutrients 2021, 14, 61. [Google Scholar] [CrossRef]
- Ginos, B.N.R.; Engberink, R. Estimation of Sodium and Potassium Intake: Current Limitations and Future Perspectives. Nutrients 2020, 12, 3275. [Google Scholar] [CrossRef]
- Shim, J.S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef]
- Ortega, R.M.; Pérez-Rodrigo, C.; López-Sobaler, A.M. Dietary assessment methods: Dietary records. Nutr. Hosp. 2015, 31 (Suppl. S3), 38–45. [Google Scholar] [PubMed]
- Foster, E.; Bradley, J. Methodological considerations and future insights for 24-hour dietary recall assessment in children. Nutr. Res. 2018, 51, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wolper, C.H.S.; Heymsfield, S.B. Measuring Food Intake: An Overview. In Handbook of Assessment Methods for Eating Behaviors and Weight-Related Problems: Measures, Theory, and Research; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1995. [Google Scholar]
- Cicero, A.F.G.; Veronesi, M.; Fogacci, F. Dietary Intervention to Improve Blood Pressure Control: Beyond Salt Restriction. High Blood Press. Cardiovasc. Prev. 2021, 28, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.; de Castro Mendes, F.; Padrão, P.; Delgado, L.; Paciência, I.; Barros, R.; Rufo, J.C.; Silva, D.; Moreira, A.; Moreira, P. Mediterranean Diet and Airway Inflammation in School-Aged Children. Children 2023, 10, 1305. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total, n = 295 (100%) | Sodium (≤2484 mg) | Sodium (>2484 mg) | p-Value | |
|---|---|---|---|---|
| Age (years), mean ± SD | 8.53 ± 0.73 | 8.45 ± 0.63 | 8.63 ± 0.82 | 0.043 * |
| Sex, n (%) | 0.004 * | |||
| Female | 138 (46.8%) | 82 (55.0%) | 56 (38.4%) | |
| Male | 157 (53.2%) | 67 (42.7%) | 90 (57.3%) | |
| BMI | 0.015 * | |||
| Non-overweight/obese (p < 85th) | 226 (76.6%) | 123 (82.6%) | 103 (70.5%) | |
| Overweight/obese (p ≥ 85th) | 69 (23.4%) | 26 (17.4%) | 43 (29.5%) | |
| aMED score, mean ± SD | 2.66 ± 1.54 | 2.62 ± 1.52 | 2.69 ± 1.50 | 0.596 |
| Vegetables, g, median (25th–75th) | 107.02 ± 92.08 | 111.59 ± 96.60 | 102.37 ± 87.31 | 0.390 |
| Fruits, g, mean ± SD | 194.43 ± 168.61 | 203.76 ± 166.14 | 184.91 ± 171.14 | 0.338 |
| Ratio MUFA to SFA | 1.18 (0.91–1.47) | 1.22 (0.91–1.52) | 1.14 (0.89–1.40) | 0.130 |
| Fish (g), median (25th–75th) | 0.00 (0.00–100.00) | 0.00 (0.00–100.00) | 0.00 (0.00–80.00) | 0.553 |
| Nuts(g), median (25th–75th) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 0.436 |
| Whole grains, (g), median (25th–75th) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 0.510 |
| Legumes, (g), median (25th–75th) | 0.00 (0.00–14.52) | 0.00 (0.00–0.00) | 0.00 (0.00–33.38) | 0.035 * |
| Red and processed meat, (g), median (25th–75th) | 90.70 (30.0–159.9) | 90.00 (34.85–154.15) | 92.32 (20.00–161.53) | 0.719 |
| Total energy intake (kcal), median (25th–75th) | 2223.72 (1889.76–2482.90) | 2154.17 (1817.75–2410.48) | 2224.12 (1923.87–2559.93) | 0.043 * |
| Physical activity a, n (%) | 0.162 | |||
| <2 timesx/week | 128 (47.2%) | 72 (56.3%) | 56 (42.1%) | |
| 2–3 times/week | 105 (38.7%) | 48 (34.8%) | 57 (42.9%) | |
| ≥4 times/week | 38 (14.0%) | 18 (13.0%) | 20 (15.0%) | |
| Parental education b, n (%) | 0.233 | |||
| <9 years | 87 (35.1%) | 39 (29.3%) | 48 (41.7%) | |
| 10–12 years | 63 (25.4%) | 41 (30.8%) | 22 (19.1%) | |
| >12 years | 98 (39.5%) | 53 (54.1%) | 45 (39.1%) | |
| aMED Score Crude Model, OR (95% CI) | p-Value | aMED Score Adjusted Model, OR (95% CI) | p-Value | |
|---|---|---|---|---|
| Increased levels of excreted urinary sodium (>2484 mg) | ||||
| All participants | 0.96 (0.83–1.12) | 0.595 | 1.08 (0.91–1.28) | 0.393 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, M.; Castro Mendes, F.d.; Padrão, P.; Delgado, L.; Barros, R.; Rufo, J.C.; Silva, D.; Moreira, A.; Moreira, P. Does the Mediterranean Dietary Pattern Promote Lower Sodium Urinary Excretion in Children? Children 2023, 10, 1478. https://doi.org/10.3390/children10091478
Rodrigues M, Castro Mendes Fd, Padrão P, Delgado L, Barros R, Rufo JC, Silva D, Moreira A, Moreira P. Does the Mediterranean Dietary Pattern Promote Lower Sodium Urinary Excretion in Children? Children. 2023; 10(9):1478. https://doi.org/10.3390/children10091478
Chicago/Turabian StyleRodrigues, Mónica, Francisca de Castro Mendes, Patrícia Padrão, Luís Delgado, Renata Barros, João Cavaleiro Rufo, Diana Silva, André Moreira, and Pedro Moreira. 2023. "Does the Mediterranean Dietary Pattern Promote Lower Sodium Urinary Excretion in Children?" Children 10, no. 9: 1478. https://doi.org/10.3390/children10091478