
Diagnostic Accuracy of Liquid Biomarkers for the Non-Invasive Diagnosis of Endometrial Cancer: A Systematic Review and Meta-Analysis
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
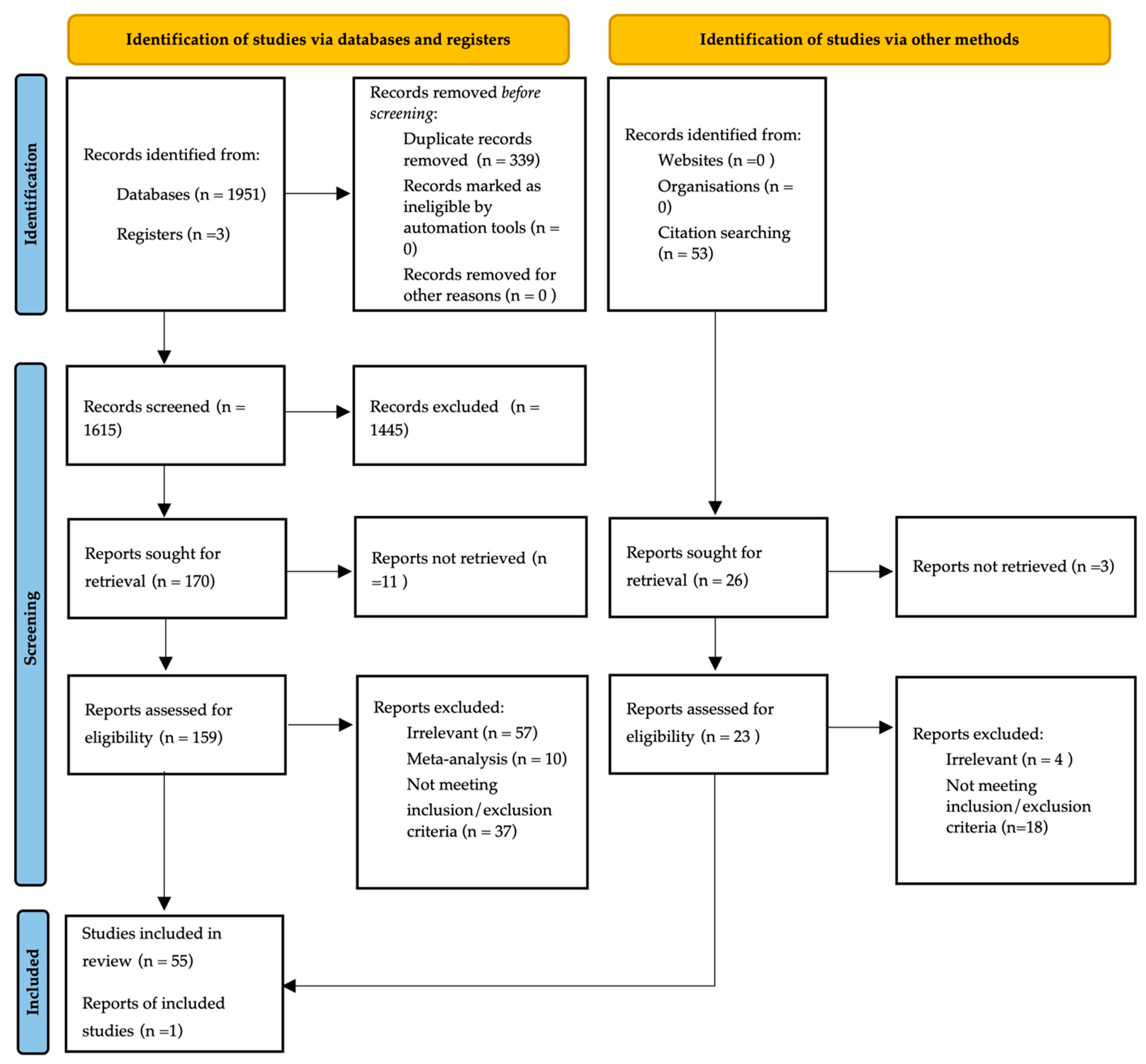
2.1. Literature Search
2.2. Data Extraction and Quality Assessment
2.3. Statistical Analysis
3. Results
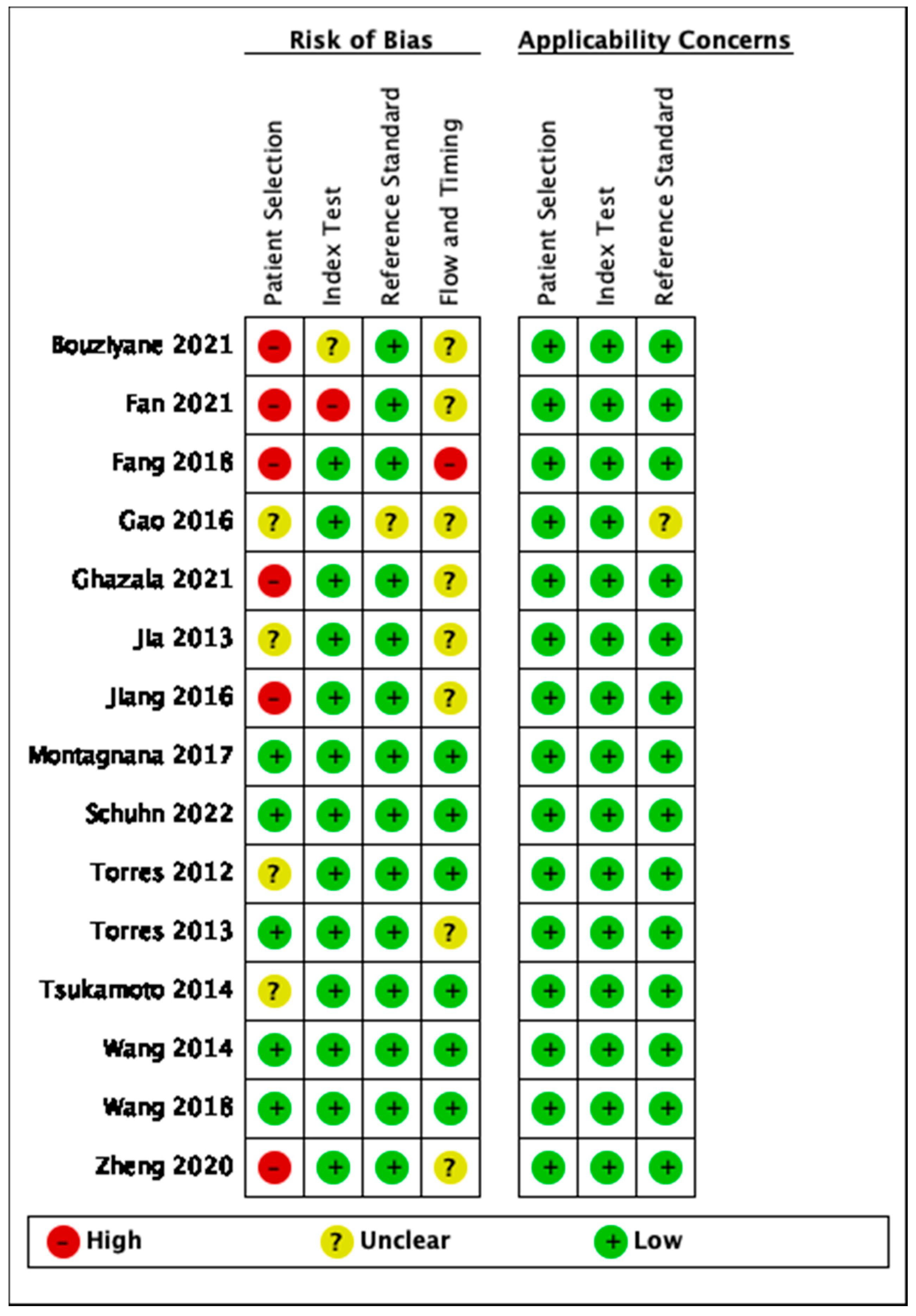
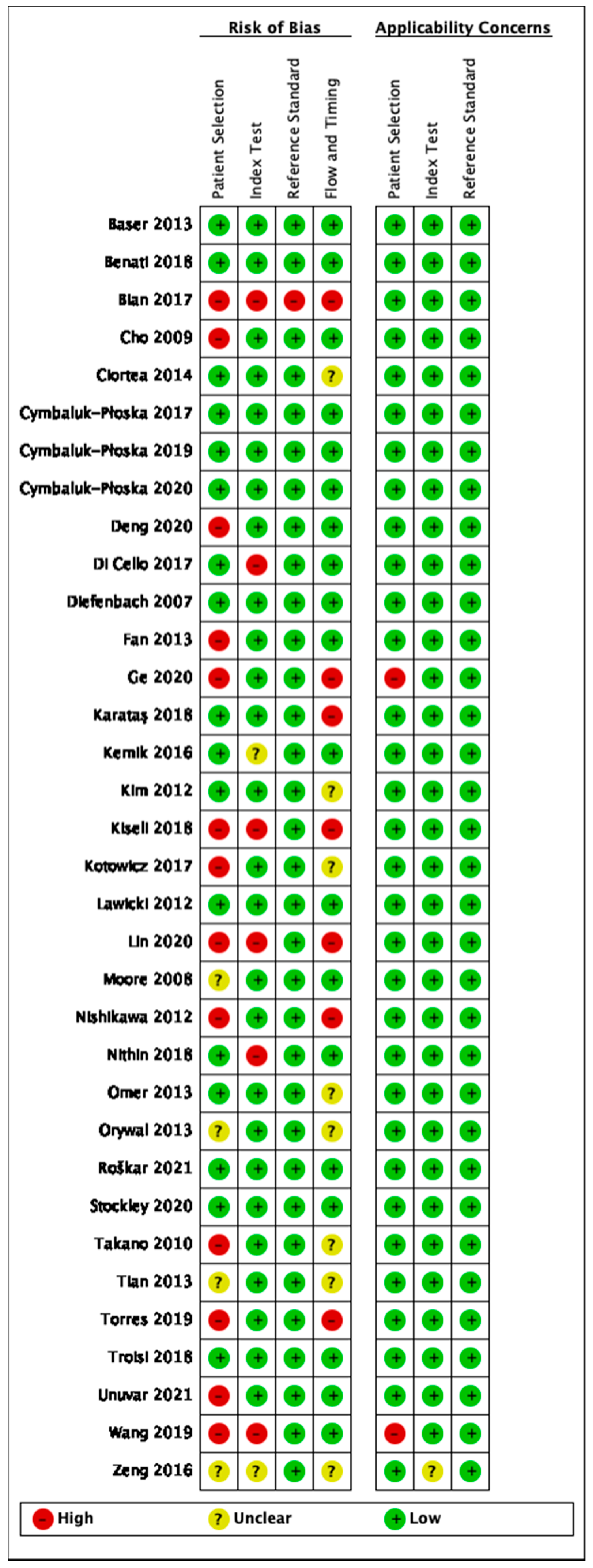
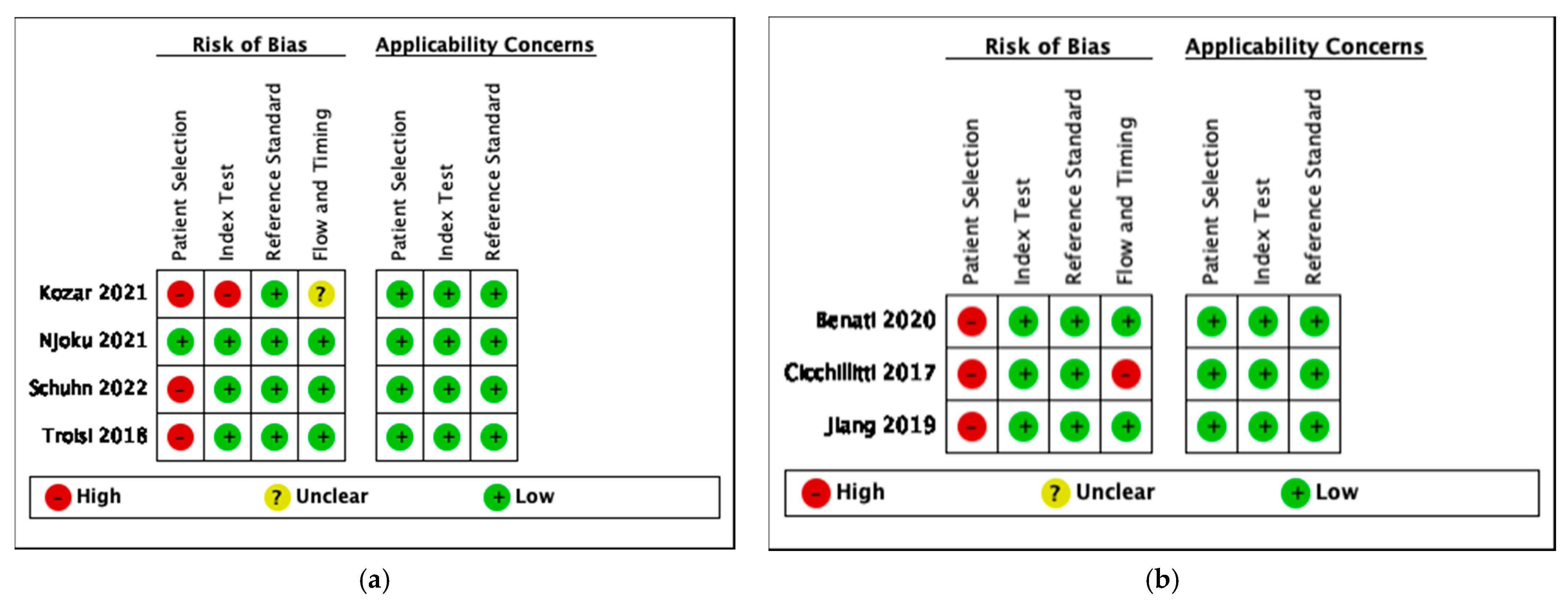
3.1. Assessment of Quality and Heterogeneity of Studies
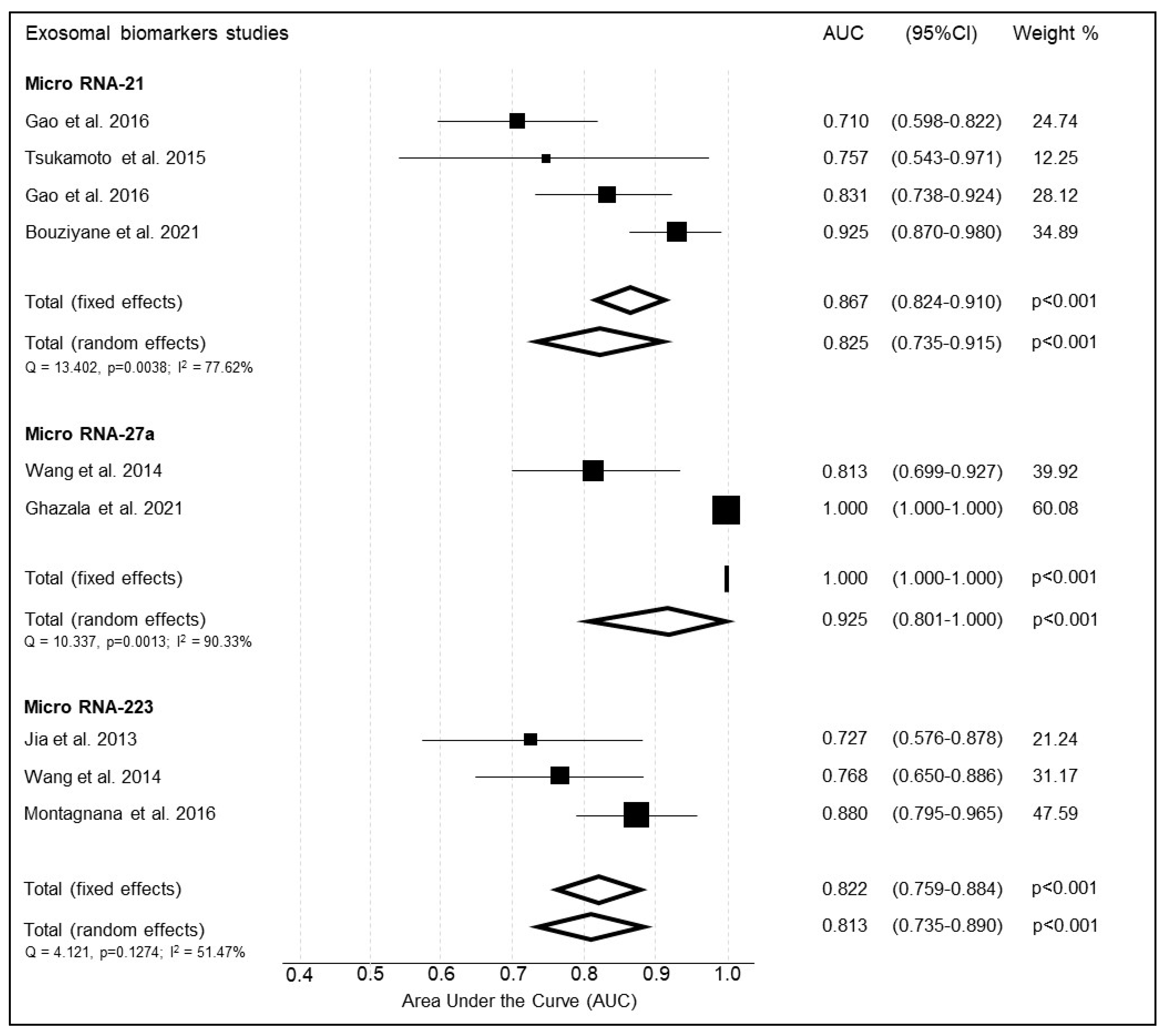
3.2. Meta-Analysis of Exosomal Biomarkers
3.2.1. Micro RNA-21
3.2.2. Micro-RNA 27a
3.2.3. Micro-RNA 223
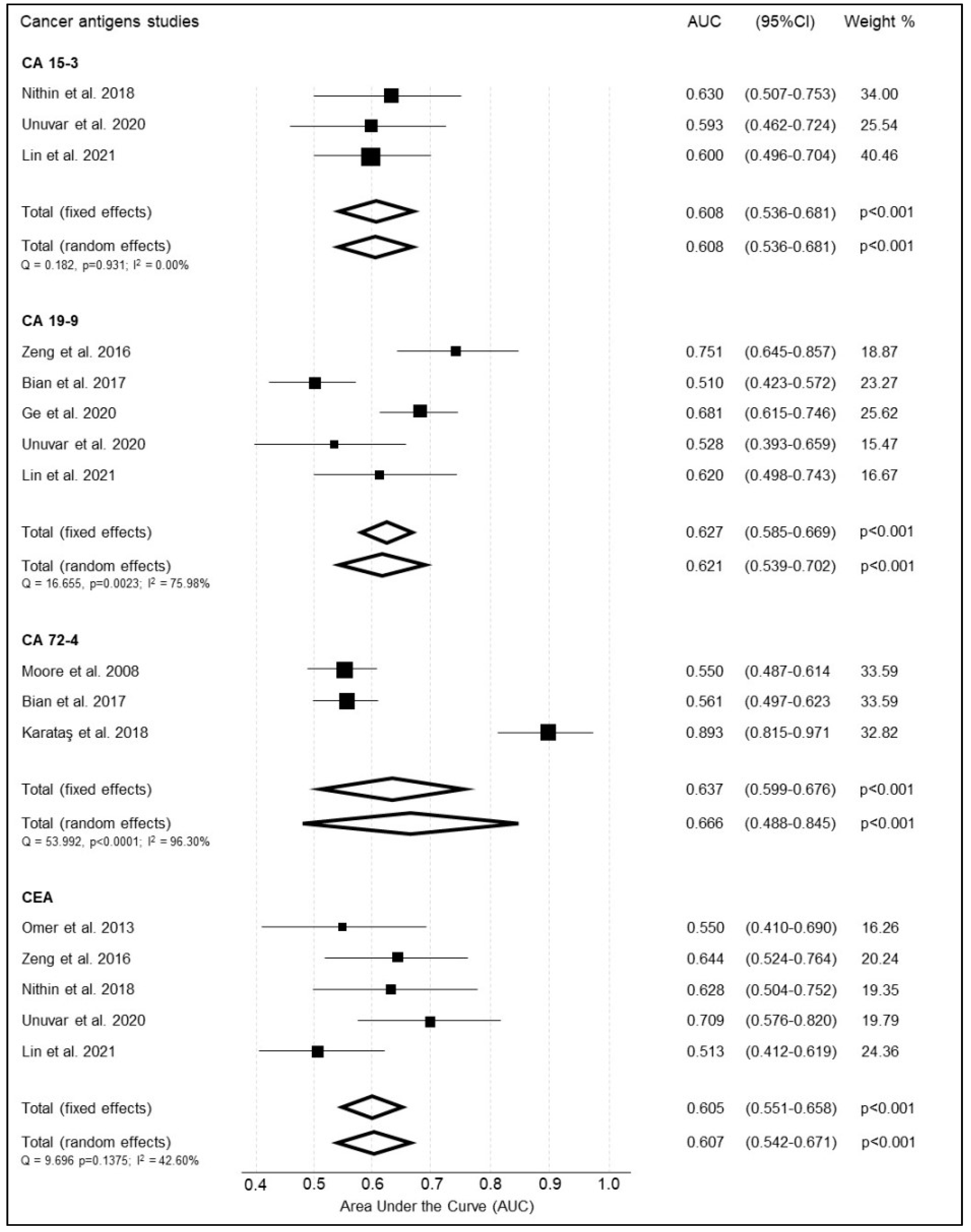
3.3. Protein Based Biomarkers
3.3.1. Cancer Antigens—CA 15-3
3.3.2. Cancer Antigen—CA 19-9
3.3.3. Cancer Antigen—CA 72-4
3.3.4. Cancer Embryonic Antigen (CEA)
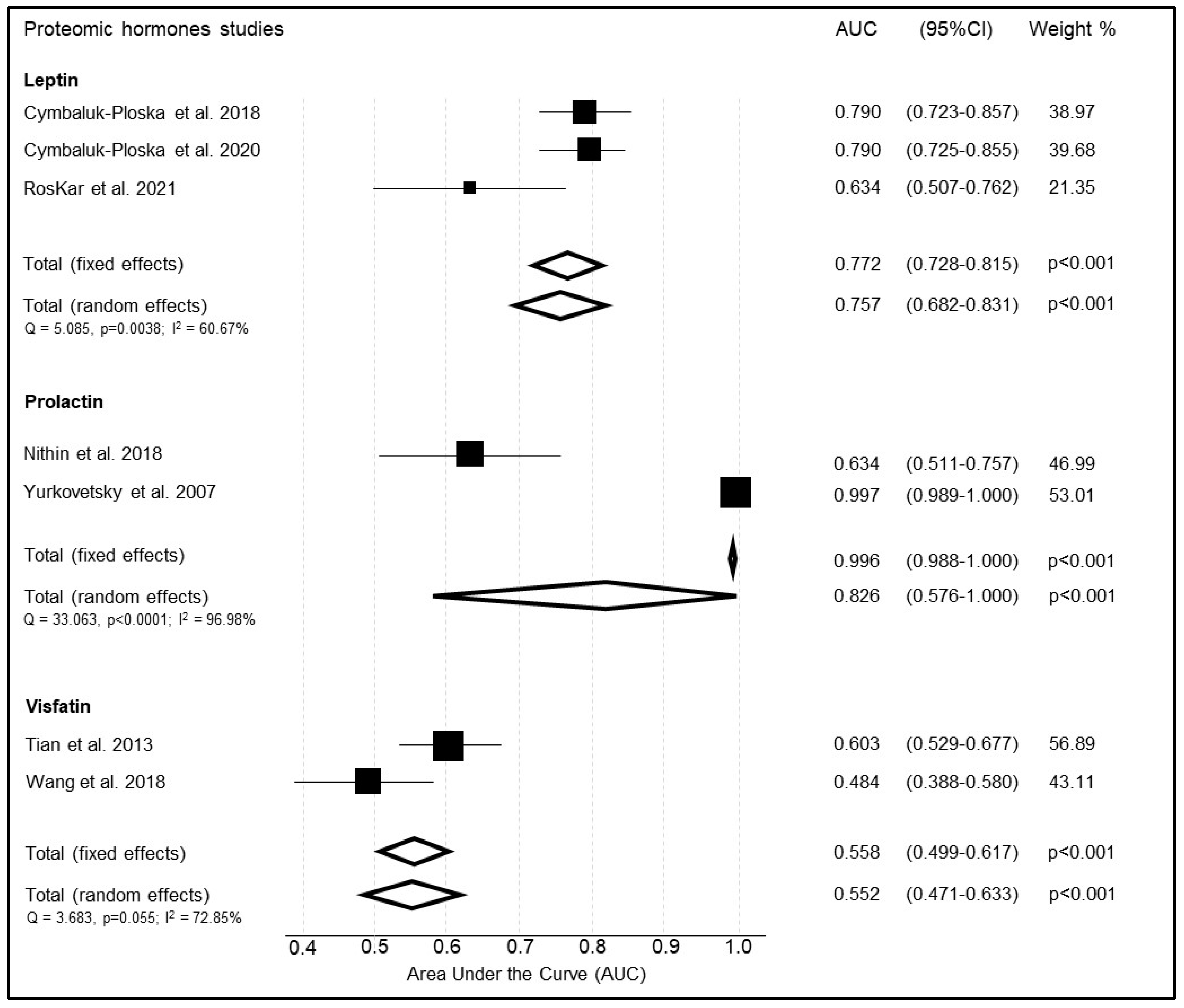
3.4. Homonal Biomarkers
3.4.1. Leptin
3.4.2. Prolactin
3.4.3. Visfatin
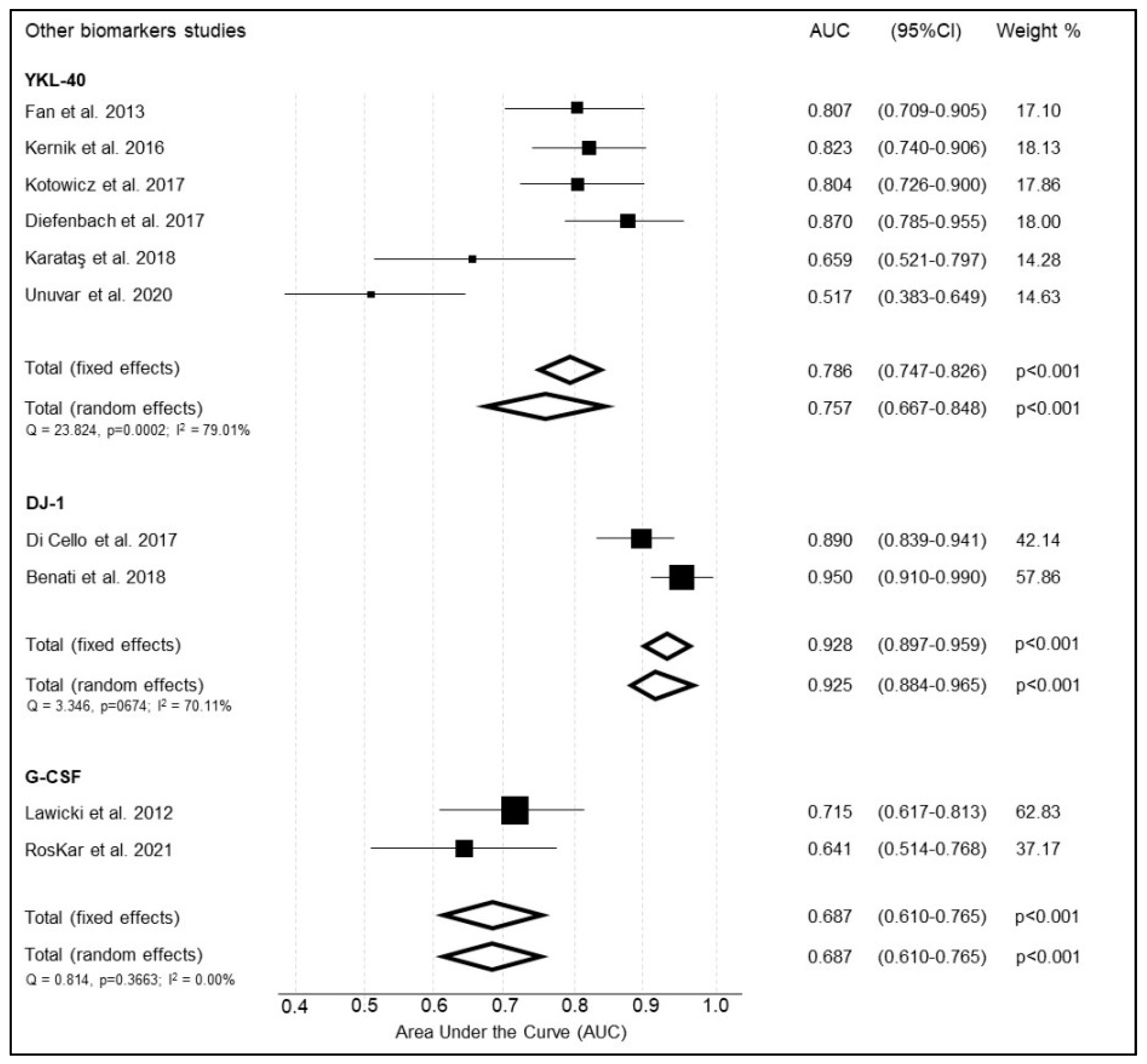
3.5. Other Proteomic Markers
3.5.1. YKL-40
3.5.2. DJ-1
3.5.3. Granulocyte-Colony Stimulating Factor (G-CSF)
3.6. Metabolomic Biomarkers
3.7. Circulating Tumor Related Material Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- CRUK. Uterine Cancer Incidence Statistics. 2020. Available online: http://www.Cancerresearchuk.Org.Last (accessed on 4 April 2022).
- Agency for Research on Cancer. Cancer Tomorrow (website). Available online: https://gco.iarc.fr/tomorrow/graphic-isotype?type=1&population=900&mode=population&sex=2&cancer=39&age_group=value&apc_male=0&apc_female=0 (accessed on 4 April 2022).
- Creasman, W.T.; Odicino, F.; Maisonneuve, P.; Quinn, M.A.; Beller, U.; Benedet, J.L.; Heintz, A.P.M.; Ngan, H.Y.S.; Pecorelli, S. Carcinoma of the Corpus Uteri. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int. J. Gynaecol. Obstet. 2006, 95 (Suppl S1), S105–S143. [Google Scholar] [CrossRef]
- Murali, R.; Soslow, R.A.; Weigelt, B. Classification of Endometrial Carcinoma: More than Two Types. Lancet Oncol. 2014, 15, e268–e278. [Google Scholar] [CrossRef]
- Sanderson, P.A.; Critchley, H.O.D.; Williams, A.R.W.; Arends, M.J.; Saunders, P.T.K. New Concepts for an Old Problem: The Diagnosis of Endometrial Hyperplasia. Hum. Reprod. Update 2017, 23, 232–254. [Google Scholar] [CrossRef]
- Morrison, J.; Balega, J.; Buckley, L.; Clamp, A.; Crosbie, E.; Drew, Y.; Durrant, L.; Forrest, J.; Fotopoulou, C.; Gajjar, K.; et al. British Gynaecological Cancer Society (BGCS) Uterine Cancer Guidelines: Recommendations for Practice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 270, 50–89. [Google Scholar] [CrossRef]
- Royal College of Obstetricians & Gynaecologists. Management of Endometrial Hyperplasia, RCOG Guideline No.67. RCOG/BSGE Jt Guidel. 2016. Available online: https://www.rcog.org.uk/media/knmjbj5c/gtg_67_endometrial_hyperplasia.pdf (accessed on 15 July 2022).
- Gupta, J.K.; Chien, P.F.W.; Voit, D.; Clark, T.J.; Khan, K.S. Ultrasonographic Endometrial Thickness for Diagnosing Endometrial Pathology in Women with Postmenopausal Bleeding: A Meta-Analysis. Acta Obstet. Gynecol. Scand. 2002, 81, 799–816. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.nice.org.uk/guidance/ng88/resources/heavy-menstrual-bleeding-assessment-and-management-pdf-1837701412549 (accessed on 15 July 2022).
- Timmermans, A.; Opmeer, B.C.; Khan, K.S.; Bachmann, L.M.; Epstein, E.; Clark, T.J.; Gupta, J.K.; Bakour, S.H.; van den Bosch, T.; van Doorn, H.C.; et al. Endometrial Thickness Measurement for Detecting Endometrial Cancer in Women with Postmenopausal Bleeding: A Systematic Review and Meta-Analysis. Obstet. Gynecol. 2010, 116, 160–167. [Google Scholar] [CrossRef]
- van Hanegem, N.; Prins, M.M.C.; Bongers, M.Y.; Opmeer, B.C.; Sahota, D.S.; Mol, B.W.J.; Timmermans, A. The Accuracy of Endometrial Sampling in Women with Postmenopausal Bleeding: A Systematic Review and Meta-Analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 197, 147–155. [Google Scholar] [CrossRef]
- Bennett, A.; Lepage, C.; Thavorn, K.; Fergusson, D.; Murnaghan, O.; Coyle, D.; Singh, S.S. Effectiveness of Outpatient Versus Operating Room Hysteroscopy for the Diagnosis and Treatment of Uterine Conditions: A Systematic Review and Meta-Analysis. J. Obstet. Gynaecol. Can. 2019, 41, 930–941. [Google Scholar] [CrossRef] [PubMed]
- Alix-Panabières, C.; Pantel, K. Liquid Biopsy: From Discovery to Clinical Application. Cancer Discov. 2021, 11, 858–873. [Google Scholar] [CrossRef]
- Zhou, X.H. Empirical Bayes Combination of Estimated Areas under ROC Curves Using Estimating Equations. Med. Decis. Mak. 1996, 16, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.D.; Zhou, X.-H.; Freeman, D.H.J.; Freeman, J.L. A Non-Parametric Method for the Comparison of Partial Areas under ROC Curves and Its Application to Large Health Care Data Sets. Stat. Med. 2002, 21, 701–715. [Google Scholar] [CrossRef] [PubMed]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L.; et al. Preferred Reporting Items for a Systematic Review and Meta-Analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Karkia, R.; Wali, S.; Karteris, E.; Chatterjee, J. Liquid Biopsy for Screening and Diagnosis of Endometrial Cancer—A Systematic Review. PROSPERO 2020 CRD42020202191. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020202191 (accessed on 15 July 2022).
- Liu, J.; Han, L.; Sun, Q.; Li, Y.; Niyazi, M. Meta-Analysis of the Diagnostic Accuracy of HE4 for Endometrial Carcinoma. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 252, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.-Q.; Xi, Y.-Y.; Zhang, C.-J.; Jiang, X. Serum Human Epididymis Protein 4 Combined with Carbohydrate Antigen 125 for Endometrial Carcinoma Diagnosis: A Meta-Analysis and Systematic Review. Genet. Test. Mol. Biomark. 2019, 23, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, X.; Qu, W.; Wang, J.; Jiang, S.-W. Comparison of Serum Human Epididymis Protein 4 and CA125 on Endometrial Cancer Detection: A Meta-Analysis. Clin. Chim. Acta 2019, 488, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Bie, Y.; Zhang, Z. Diagnostic Value of Serum HE4 in Endometrial Cancer: A Meta-Analysis. World J. Surg. Oncol. 2014, 12, 169. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Nisenblat, V.; Bossuyt, P.M.M.; Shaikh, R.; Farquhar, C.; Jordan, V.; Scheffers, C.S.; Mol, B.W.J.; Johnson, N.; Hull, M.L. Blood Biomarkers for the Non-Invasive Diagnosis of Endometriosis. Cochrane Database Syst. Rev. 2016, 2016, CD012179. [Google Scholar] [CrossRef] [PubMed]
- Rutjes, A.W.S.; Reitsma, J.B.; Vandenbroucke, J.P.; Glas, A.S.; Bossuyt, P.M.M. Case-Control and Two-Gate Designs in Diagnostic Accuracy Studies. Clin. Chem. 2005, 51, 1335–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosner, B.; Glynn, R.J.; Lee, M.-L.T. The Wilcoxon Signed Rank Test for Paired Comparisons of Clustered Data. Biometrics 2006, 62, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Dai, M.; Liu, H.; He, W.; Lin, S.; Yuan, T.; Chen, H.; Dai, S. Diagnostic Value of Circulating MiR-21: An Update Meta-Analysis in Various Cancers and Validation in Endometrial Cancer. Oncotarget 2016, 7, 68894–68908. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, O.; Miura, K.; Mishima, H.; Abe, S.; Kaneuchi, M.; Higashijima, A.; Miura, S.; Kinoshita, A.; Yoshiura, K.I.; Masuzaki, H. Identification of Endometrioid Endometrial Carcinoma-Associated MicroRNAs in Tissue and Plasma. Gynecol. Oncol. 2014, 132, 715–721. [Google Scholar] [CrossRef]
- Bouziyane, A. Diagnostic Value of MicroRNA 21 in Endometrial Cancer and Benign Lesions and Its Differential Expression with Clinicopathological Parameters. Microrna 2021, 10, 146–152. [Google Scholar] [CrossRef]
- Wang, L.; Chen, Y.J.; Xu, K.; Xu, H.; Shen, X.Z.; Tu, R.Q. Circulating MicroRNAs as a Fingerprint for Endometrial Endometrioid Adenocarcinoma. PLoS ONE 2014, 9, 1–7. [Google Scholar] [CrossRef]
- Ghazala, R.A.; El-Attar, E.A.; Abouzeid, Z.S. Circulating MiRNA 27a and MiRNA150-5p; a Noninvasive Approach to Endometrial Carcinoma. Mol. Biol. Rep. 2021, 48, 4351–4360. [Google Scholar] [CrossRef]
- Jia, W.; Wu, Y.; Zhang, Q.; Gao, G.; Zhang, C.; Xiang, Y. Identification of Four Serum MicroRNAs from a Genome-Wide Serum MicroRNA Expression Profile as Potential Non-Invasive Biomarkers for Endometrioid Endometrial Cancer. Oncol. Lett. 2013, 6, 261–267. [Google Scholar] [CrossRef]
- Montagnana, M.; Benati, M.; Danese, E.; Giudici, S.; Perfranceschi, M.; Ruzzenenete, O.; Salvagno, G.L.; Bassi, A.; Gelati, M.; Paviati, E.; et al. Aberrant MicroRNA Expression in Patients With Endometrial Cancer. Int. J. Gynecol. Cancer 2017, 27, 459–466. [Google Scholar] [CrossRef]
- Fan, X.; Zou, X.; Liu, C.; Cheng, W.; Zhang, S.; Geng, X.; Zhu, W. MicroRNA Expression Profile in Serum Reveals Novel Diagnostic Biomarkers for Endometrial Cancer. Biosci. Rep. 2021, 41, BSR2021011. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Wang, N.; Yin, D.; Li, Y.K.; Guo, L.; Shi, L.P.; Huang, X. Changes in the Expression of Serum MiR-887-5p in Patients with Endometrial Cancer. Int. J. Gynecol. Cancer 2016, 26, 1143–1147. [Google Scholar] [CrossRef] [PubMed]
- Schuhn, A.; Tobar, T.W.; Gahlawat, A.W.; Hauke, J.; Baumann, L.; Okun, J.G.; Nees, J. Potential of Blood-Based Biomarker Approaches in Endometrium and Breast Cancer: A Case-Control Comparison Study. Arch. Gynecol. Obstet. 2022, No. 0123456789. [Google Scholar] [CrossRef]
- Torres, A.; Torres, K.; Pesci, A.; Ceccaroni, M.; Paszkowski, T.; Cassandrini, P.; Zamboni, G.; Maciejewski, R. Deregulation of MiR-100, MiR-99a and MiR-199b in Tissues and Plasma Coexists with Increased Expression of MTOR Kinase in Endometrioid Endometrial Carcinoma. BMC Cancer 2012, 12. [Google Scholar] [CrossRef]
- Fang, S.; Gao, M.; Xiong, S.; Chen, Q.; Zhang, H. Expression of Serum Hsa-MiR-93 in Uterine Cancer and Its Clinical Significance. Oncol. Lett. 2018, 15, 9896–9900. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Torres, K.; Pesci, A.; Ceccaroni, M.; Paszkowski, T.; Cassandrini, P.; Zamboni, G.; MacIejewski, R. Diagnostic and Prognostic Significance of MiRNA Signatures in Tissues and Plasma of Endometrioid Endometrial Carcinoma Patients. Int. J. Cancer 2013, 132, 1633–1645. [Google Scholar] [CrossRef]
- Wang, H.; Wang, T.T.; Lv, X.P. Expression and Prognostic Value of MiRNA-29b in Peripheral Blood for Endometrial Cancer. Future Oncol. 2018, 14, 1365–1376. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Yang, J.; Wang, Y.; Liu, X. Exosomal MiRNA-93 and MiRNA-205 Expression in Endometrial Cancer. J. King Saud Univ. —Sci. 2020, 32, 1111–1115. [Google Scholar] [CrossRef]
- Lin, D.; Zhao, L.; Zhu, Y.; Huang, Y.; Yuan, K.; Liu, W.; Li, S.; Guo, X.; Hao, Y. Combination IETA Ultrasonographic Characteristics Simple Scoring Method With Tumor Biomarkers Effectively Improves the Differentiation Ability of Benign and Malignant Lesions in Endometrium and Uterine Cavity. Front. Oncol. 2021, 11, 605847. [Google Scholar] [CrossRef]
- Moore, R.G.; Brown, A.K.; Miller, M.C.; Badgwell, D.; Lu, Z.; Allard, W.J.; Granai, C.O.; Bast, R.C.J.; Lu, K. Utility of a Novel Serum Tumor Biomarker HE4 in Patients with Endometrioid Adenocarcinoma of the Uterus. Gynecol. Oncol. 2008, 110, 196–201. [Google Scholar] [CrossRef] [Green Version]
- Lawicki, S.; Będkowska, G.E.; Gacuta-Szumarska, E.; Szmitkowski, M. Hematopoietic Cytokines as Tumor Markers in Gynecological Malignancies: A Multivariate Analysis with ROC Curve in Endometrial Cancer Patients. Growth Factors 2012, 30, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.W.; Jeon, Y.E.; Cho, H.; Nam, E.J.; Kim, S.W.; Kim, S.; Kim, Y.T.; Kim, J.-H. Pre-Treatment Diagnosis of Endometrial Cancer through a Combination of CA125 and Multiplication of Neutrophil and Monocyte. J. Obstet. Gynaecol. Res. 2012, 38, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Unuvar, S.; Melekoglu, R.; Turkmen, N.B.; Yilmaz, E.; Yasar, S.; Yuce, H. Comparison of Preoperative Serum Neopterin, Periostin, Indoleamine 2,3-Dioxygenase, YKL-40, and Tenascin-C Levels with Current Tumor Markers for Early-Stage Endometrial Cancer. Int. J. Gynaecol. Obstet. 2021, 155, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Orywal, K.; Jelski, W.; Zdrodowski, M.; Szmitkowski, M. The Diagnostic Value of Alcohol Dehydrogenase Isoenzymes and Aldehyde Dehydrogenase Measurement in the Sera of Patients with Endometrial Cancer. Anticancer Res. 2013, 33, 3725–3730. [Google Scholar]
- Roškar, L.; Klančič, T.; Knific, T.; Rižner, T.L.; Smrkolj, Š. Tie-2, G-CSF, and Leptin as Promising Diagnostic Biomarkers for Endometrial Cancer: A Pilot Study. J. Clin. Med. 2021, 10. [Google Scholar] [CrossRef]
- Cymbaluk-Płoska, A.; Gargulińska, P.; Chudecka-Głaz, A.; Kwiatkowski, S.; Pius-Sadowska, E.; Machaliński, B. The Suitability of FGF21 and FGF23 as New Biomarkers in Endometrial Cancer Patients. Diagnostics 2020, 10, 414. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Pac-Sosińska, M.; Wiktor, K.; Paszkowski, T.; Maciejewski, R.; Torres, K. CD44, TGM2 and EpCAM as Novel Plasma Markers in Endometrial Cancer Diagnosis. BMC Cancer 2019, 19, 401. [Google Scholar] [CrossRef]
- Cymbaluk-Płoska, A.; Chudecka-Głaz, A.; Jagodzińska, A.; Pius-Sadowska, E.; Sompolska-Rzechuła, A.; Machaliński, B.; Menkiszak, J. Evaluation of Biologically Active Substances Promoting the Development of or Protecting against Endometrial Cancer. OncoTargets Ther. 2018, 11, 1363–1372. [Google Scholar] [CrossRef] [PubMed]
- Ge, L.; Liu, G.; Hu, K.; Huang, K.; Zhang, M.; Zhou, J.; Teng, F.; Cao, J.; Dai, C.; Jia, X. A New Risk Index Combining D-Dimer, Fibrinogen, HE4, and CA199 Differentiates Suspecting Endometrial Cancer From Patients With Abnormal Vaginal Bleeding or Discharge. Technol. Cancer Res. Treat. 2020, 19, 1533033819901117. [Google Scholar] [CrossRef]
- Lin, S.; Wang, Y.; Wang, X.; Yan, B.; Lou, W.; Di, W. Serum Immunoglobulin G N-Glycome: A Potential Biomarker in Endometrial Cancer. Ann. Transl. Med. 2020, 8, 748. [Google Scholar] [CrossRef]
- Cho, H.; Kang, E.S.; Kim, Y.T.; Kim, J.-H. Diagnostic and Prognostic Impact of Osteopontin Expression in Endometrial Cancer. Cancer Investig. 2009, 27, 313–323. [Google Scholar] [CrossRef]
- Cymbaluk-Płoska, A.; Chudecka-Głaz, A.; Pius-Sadowska, E.; Machaliński, B.; Sompolska-Rzechuła, A.; Kwiatkowski, S.; Menkiszak, J. The Role of Lipocalin-2 Serum Levels in the Diagnostics of Endometrial Cancer. Cancer Biomark. 2019, 24, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Kiseli, M.; Caglar, G.S.; Yarci Gursoy, A.; Tasci, T.; Candar, T.; Akincioglu, E.; Pabuccu, E.G.; Boran, N.; Tulunay, G.; Umudum, H. Pro-Gastrin Releasing Peptide: A New Serum Marker for Endometrioid Adenocarcinoma. Gynecol. Obstet. Investig. 2018, 83, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Cymbaluk-Płoska, A.; Chudecka-Głaz, A.; Pius-Sadowska, E.; Sompolska-Rzechuła, A.; Machaliński, B.; Surowiec, A.; Menkiszak, J. Clinical Importance of Serum HE4 and MMP2 Levels in Endometrial Cancer Patients. OncoTargets Ther. 2017, 10, 3169–3175. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, R.; Suzumori, N.; Nishiyama, T.; Nishikawa, H.; Arakawa, A.; Sugiura-Ogasawara, M. Clinical Significance of Serum Growth-Regulated Oncogene Alpha (GROalpha) in Patients with Gynecological Cancer. Eur. J. Gynaecol. Oncol. 2012, 33, 138–141. [Google Scholar]
- Wang, Z.; Gao, S.; Sun, C.; Li, J.; Gao, W.; Yu, L. Clinical Significance of Serum Adiponectin and Visfatin Levels in Endometrial Cancer. Int. J. Gynaecol. Obstet. 2019, 145, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Baser, E.; Togrul, C.; Ozgu, E.; Ayhan, S.; Caglar, M.; Erkaya, S.; Gungor, T. Sperm-Associated Antigen 9 Is a Promising Marker for Early Diagnosis of Endometrial Cancer. Asian Pac. J. Cancer Prev. 2013, 14, 7635–7638. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.-H.; Yao, Z.-Y.; He, X.; Zhang, J.-B.; Xie, K.; Chen, J.; Cao, M.; Zhang, J.; Yie, S.-M. Clinical Significance of Plasma Anti-TOPO48 Autoantibody and Blood Survivin-Expressing Circulating Cancer Cells in Patients with Early Stage Endometrial Carcinoma. Arch. Gynecol. Obstet. 2019, 299, 229–237. [Google Scholar] [CrossRef]
- Stockley, J.; Akhand, R.; Kennedy, A.; Nyberg, C.; Crosbie, E.J.; Edmondson, R.J. Detection of MCM5 as a Novel Non-Invasive Aid for the Diagnosis of Endometrial and Ovarian Tumours. BMC Cancer 2020, 20, 1000. [Google Scholar] [CrossRef] [PubMed]
- Takano, M.; Kikuchi, Y.; Asakawa, T.; Goto, T.; Kita, T.; Kudoh, K.; Kigawa, J.; Sakuragi, N.; Sakamoto, M.; Sugiyama, T.; et al. Identification of Potential Serum Markers for Endometrial Cancer Using Protein Expression Profiling. J. Cancer Res. Clin. Oncol. 2010, 136, 475–481. [Google Scholar] [CrossRef]
- Deng, L.; Liang, H.; Han, Y. Cyclooxygenase-2 and β-Catenin as Potential Diagnostic and Prognostic Markers in Endometrial Cancer. Front. Oncol. 2020, 10, 56. [Google Scholar] [CrossRef]
- Zeng, X.; Zhang, Z.; Gao, Q.-Q.; Wang, Y.-Y.; Yu, X.-Z.; Zhou, B.; Xi, M.-R. Clinical Significance of Serum Interleukin-31 and Interleukin-33 Levels in Patients of Endometrial Cancer: A Case Control Study. Dis. Markers 2016, 2016, 9262919. [Google Scholar] [CrossRef] [Green Version]
- Ciortea, R.; Mihu, D.; Mihu, C.M. Association between Visceral Fat, IL-8 and Endometrial Cancer. Anticancer. Res. 2014, 34, 379–383. [Google Scholar] [PubMed]
- Troisi, J.; Sarno, L.; Landolfi, A.; Scala, G.; Martinelli, P.; Venturella, R.; Di Cello, A.; Zullo, F.; Guida, M. Metabolomic Signature of Endometrial Cancer. J. Proteome Res. 2018, 17, 804–812. [Google Scholar] [CrossRef]
- Nithin, K.U.; Sridhar, M.G.; Srilatha, K.; Habebullah, S. CA 125 Is a Better Marker to Differentiate Endometrial Cancer and Abnormal Uterine Bleeding. Afr. Health Sci. 2018, 18, 972–978. [Google Scholar] [CrossRef]
- Bian, J.; Sun, X.; Li, B.; Ming, L. Clinical Significance of Serum HE4, CA125, CA724, and CA19-9 in Patients With Endometrial Cancer. Technol. Cancer Res. Treat. 2017, 16, 435–439. [Google Scholar] [CrossRef]
- Karataş, S.; Şal, V.; Kahramanoğlu, İ.; Demirkıran, F.; Beşe, T.; Arvas, M.; Sofiyeva, N.; Güralp, O.; Uzun, H. Ykl-40 and Cancer Antigen 72-4 as New and Promising Diagnostic and Prognostic Markers for Endometrial Cancer. Turk. J. Obstet. Gynecol. 2018, 15, 235–242. [Google Scholar] [CrossRef]
- Omer, B.; Genc, S.; Takmaz, O.; Dirican, A.; Kusku-Kiraz, Z.; Berkman, S.; Gurdol, F. The Diagnostic Role of Human Epididymis Protein 4 and Serum Amyloid-A in Early-Stage Endometrial Cancer Patients. Tumour. Biol. 2013, 34, 2645–2650. [Google Scholar] [CrossRef]
- Yurkovetsky, Z.; Ta’asan, S.; Skates, S.; Rand, A.; Lomakin, A.; Linkov, F.; Marrangoni, A.; Velikokhatnaya, L.; Winans, M.; Gorelik, E.; et al. Development of Multimarker Panel for Early Detection of Endometrial Cancer. High Diagnostic Power of Prolactin. Gynecol. Oncol. 2007, 107, 58–65. [Google Scholar] [CrossRef]
- Tian, W.; Zhu, Y.; Wang, Y.; Teng, F.; Zhang, H.; Liu, G.; Ma, X.; Sun, D.; Rohan, T.; Xue, F. Visfatin, a Potential Biomarker and Prognostic Factor for Endometrial Cancer. Gynecol. Oncol. 2013, 129, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Si, X.; Liao, Y.; Shen, P. The Diagnostic and Prognostic Value of Serum YKL-40 in Endometrial Cancer. Arch. Gynecol. Obstet. 2013, 287, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Kemik, P.; Saatli, B.; Yıldırım, N.; Kemik, V.D.; Deveci, B.; Terek, M.C.; Koçtürk, S.; Koyuncuoğlu, M.; Saygılı, U. Diagnostic and Prognostic Values of Preoperative Serum Levels of YKL-40, HE-4 and DKK-3 in Endometrial Cancer. Gynecol. Oncol. 2016, 140, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Kotowicz, B.; Fuksiewicz, M.; Jonska-Gmyrek, J.; Wagrodzki, M.; Kowalska, M. Preoperative Serum Levels of YKL 40 and CA125 as a Prognostic Indicators in Patients with Endometrial Cancer. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 215, 141–147. [Google Scholar] [CrossRef]
- Diefenbach, C.S.M.; Shah, Z.; Iasonos, A.; Barakat, R.R.; Levine, D.A.; Aghajanian, C.; Sabbatini, P.; Hensley, M.L.; Konner, J.; Tew, W.; et al. Preoperative Serum YKL-40 Is a Marker for Detection and Prognosis of Endometrial Cancer. Gynecol. Oncol. 2007, 104, 435–442. [Google Scholar] [CrossRef]
- Di Cello, A.; Di Sanzo, M.; Perrone, F.M.; Santamaria, G.; Rania, E.; Angotti, E.; Venturella, R.; Mancuso, S.; Zullo, F.; Cuda, G.; et al. DJ-1 Is a Reliable Serum Biomarker for Discriminating High-Risk Endometrial Cancer. Tumour. Biol. 2017, 39, 1010428317705746. [Google Scholar] [CrossRef]
- Benati, M.; Montagnana, M.; Danese, E.; Paviati, E.; Giudici, S.; Ruzzenente, O.; Franchi, M.; Lippi, G. The Clinical Significance of DJ-1 and HE4 in Patients with Endometrial Cancer. J. Clin. Lab. Anal. 2018, 32. [Google Scholar] [CrossRef]
- Kozar, N.; Kruusmaa, K.; Dovnik, A.; Bitenc, M.; Argamasilla, R.; Adsuar, A.; Goswami, N.; Takač, I.; Arko, D. Identification of Novel Diagnostic Biomarkers in Endometrial Cancer Using Targeted Metabolomic Profiling. Advances in Medical Sciences 2021, 66, 46–51. [Google Scholar] [CrossRef]
- Njoku, K.; Campbell, A.E.; Geary, B.; MacKintosh, M.L.; Derbyshire, A.E.; Kitson, S.J.; Sivalingam, V.N.; Pierce, A.; Whetton, A.D.; Crosbie, E.J. Metabolomic Biomarkers for the Detection of Obesity-Driven Endometrial Cancer. Cancers 2021, 13, 718. [Google Scholar] [CrossRef]
- Cicchillitti, L.; Corrado, G.; De Angeli, M.; Mancini, E.; Baiocco, E.; Patrizi, L.; Zampa, A.; Merola, R.; Martayan, A.; Conti, L.; et al. Circulating Cell-Free DNA Content as Blood Based Biomarker in Endometrial Cancer. Oncotarget 2017, 8, 115230–115243. [Google Scholar] [CrossRef]
- Benati, M.; Montagnana, M.; Danese, E.; Mazzon, M.; Paviati, E.; Garzon, S.; Laganà, A.S.; Casarin, J.; Giudici, S.; Raffaelli, R.; et al. Aberrant Telomere Length in Circulating Cell-Free DNA as Possible Blood Biomarker with High Diagnostic Performance in Endometrial Cancer. Pathol. Oncol. Res. 2020, 26, 2281–2289. [Google Scholar] [CrossRef]
- Li, L.-M.; Zhu, Y.-X.; Zhong, Y.; Su, T.; Fan, X.-M.; Xi, Q.; Li, M.-Y.; Fu, J.; Tan, H.; Liu, S. Human Epididymis Protein 4 in Endometrial Cancer: A Meta-Analysis. Clin. Chim. Acta 2018, 482, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Behrouzi, R.; Barr, C.E.; Crosbie, E.J. HE4 as a Biomarker for Endometrial Cancer. Cancers 2021, 13, 4764. [Google Scholar] [CrossRef] [PubMed]
- Paraskevaidi, M.; Morais, C.L.M.; Ashton, K.M.; Stringfellow, H.F.; McVey, R.J.; Ryan, N.A.J.; O’Flynn, H.; Sivalingam, V.N.; Kitson, S.J.; Mackintosh, M.L.; et al. Detecting Endometrial Cancer by Blood Spectroscopy: A Diagnostic Cross-Sectional Study. Cancers 2020, 12, 1256. [Google Scholar] [CrossRef] [PubMed]
- Ihata, Y.; Miyagi, E.; Numazaki, R.; Muramatsu, T.; Imaizumi, A.; Yamamoto, H.; Yamakado, M.; Okamoto, N.; Hirahara, F. Amino acid profile index for early detection of endometrial cancer: Verification as a novel diagnostic marker. Int. J. Clin. Oncol. 2014, 19, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Dimou, N.L.; Papadimitriou, N.; Mariosa, D.; Johansson, M.; Brennan, P.; Peters, U.; Chanock, S.J.; Purdue, M.; Bishop, D.T.; Gago-Dominquez, M.; et al. Circulating Adipokine Concentrations and Risk of Five Obesity-Related Cancers: A Mendelian Randomization Study. Int. J. Cancer 2021, 148, 1625–1636. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | m-RNA | Cases (n) | Controls (n) | AUC | 95% AUC | Sensitivity | Specificity |
|---|---|---|---|---|---|---|---|
| Acceptable performance | |||||||
| Fan et al., 2021 1 [36] | 484 | 92 | 102 | 0.644 | 0.566 to 0.722 | - | - |
| Fan et al., 2021 1 [36] | 204-5p | 92 | 102 | 0.668 | 0.592 to 0.743 | - | - |
| Fan par. 2021 1 [36] | 195-5p | 92 | 102 | 0.669 | 0.593 to 0.745 | - | - |
| Fan et al., 2021 1 [36] | 143-3p | 92 | 102 | 0.677 | 0.602 to 0.751 | - | - |
| Fan et al., 2021 1 [36] | 423-3p | 92 | 102 | 0.689 | 0.611 to 0.767 | - | - |
| Montagnana et al., 2016 1 [35] | 186 | 46 | 28 | 0.700 | 0.580 to 0.830 | - | - |
| Good performance | |||||||
| Montagnana et al., 2016 1 [35] | 222 | 46 | 28 | 0.720 | 0.590 to 0.850 | - | - |
| Jiang et al., 2016 1 [37] | 887-5p | 20 | 20 | 0.728 | 0.563 to 0.892 | 0.950 | 0.600 |
| Jia et al., 2013 1 [34] | 204 | 26 | 22 | 0.740 | 0.594 to 0.885 | - | - |
| Schuhn et al., 2022 1 [38] | 200c | 20 | 157 | 0.740 | 0.666 to 0.815 | 1.000 | 0.573 |
| Torres et al., 2012 1 [39] | 100 | 34 | 14 | 0.740 | 0.592 to 0.897 | 0.640 | 0.790 |
| Fan et al., 2021 1 [36] | 20b-5p | 92 | 102 | 0.756 | 0.689 to 0.823 | - | - |
| Wang et al., 2014 1,2 [32] | 15b | 31 | 33 | 0.767 | 0.653 to 0.882 | 0.740 | 0.697 |
| Schuhn et al., 2022 1 [38] | 320b | 20 | 157 | 0.774 | 0.702 to 0.845 | 0.950 | 0.659 |
| Schuhn et al., 2022 1 [38] | 652 | 20 | 157 | 0.775 | 0.651 to 0.859 | 0.900 | 0.598 |
| Fang et al., 2018 1 [40] | 93 | 176 | 100 | 0.781 | 0.724 to 0.842 | - | - |
| Torres et al., 2012 1 [39] | 199b | 34 | 14 | 0.786 | 0.642 to 0.892 | 0.790 | 0.710 |
| Schuhn et al., 2022 1 [38] | 375 | 20 | 157 | 0.796 | 0.712 to 0.880 | 0.850 | 68.700 |
| Excellent performance | |||||||
| Torres et al., 2012 1 [39] | 99a | 34 | 14 | 0.810 | 0.669 to 0.909 | 0.760 | 0.790 |
| Tsukamoto et al., 2015 1 [30] | 30a-3p | 28 | 28 | 0.813 | 0.638 to 0.987 | - | - |
| Jia et al., 2013 1 [34] | 222 | 26 | 22 | 0.837 | 0.726 to 0.948 | - | - |
| Jia et al., 2013 1 [34] | 186 | 26 | 22 | 0.865 | 0.755 to 0.974 | - | - |
| Torres et al., 2013 1 [41] | 449a | 34 | 14 | 0.879 | 0.814 to 0.943 | - | - |
| Torres et al., 2013 1 [41] | 1228 | 34 | 14 | 0.890 | 0.829 to 0.951 | - | - |
| Outstanding performance | |||||||
| Tsukamoto et al., 2015 1 [30] | 135b | 28 | 28 | 0.972 | 0.913 to 1.00 | - | - |
| Wang et al., 2018 2 [42] | 29-b | 356 | 149 | 0.976 | 0.951 to 1.00 | 0.960 | 0.979 |
| Ghazala et al., 2021 1 [21] | 150-5p | 36 | 36 | 0.982 | 0.955 to 1.00 | 0.890 | 1.000 |
| Zheng et al., 2019 1,2 [43] | 93 | 100 | 100 | 0.990 | 0.976 to 1.00 | 0.930 | 0.970 |
| Montagnana et al., 2016 1 [35] | 204 | 46 | 28 | 1.000 | - | - | - |
| Tsukamoto et al., 2015 1 [30] | 205 | 28 | 28 | 1.000 | - | - | - |
| Author | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Gao et al., 2016 [29] | 50 | 50 | 0.710 | 0.598 to 0.822 | 0.640 | 0.760 | - | - |
| Tsukamoto et al., 2015 [30] | 12 | 12 | 0.757 | 0.543 to 0.971 | - | - | - | - |
| Gao et al., 2016 [29] | 50 | 50 | 0.831 | 0.738 to 0.924 | 0.700 | 0.920 | - | - |
| Bouziyane et al., 2021 [31] | 71 | 54 | 0.925 | 0.870 to 0.980 | 0.850 | 0.868 | - | - |
| Author | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Wang et al., 2014 [32] | 31 | 33 | 0.813 | 0.699 to 0.927 | 0.770 | 0.818 | - | - |
| Ghazala et al., 2021 [33] | 36 | 36 | 1.000 | 1.000 to 1.000 | 1.000 | 1.000 | - | - |
| Author | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Jia et al., 2013 [34] | 26 | 22 | 0.727 | 0.576–0.878 | 0.084 | - | - | - |
| Wang et al., 2014 [32] | 31 | 33 | 0.768 | 0.650–0.886 | 0.065 | 0.650 | 0.818 | - |
| Montagnana et al., 2016 [35] | 74 | 28 | 0.880 | 0.795–0.965 | 0.043 | - | - | - |
| Author | Biomarker | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|---|
| Poor performance | |||||||||
| Lin et al., 2021 [44] | AFP | 101 | 475 | 0.490 | 0.385–0.594 | 0.710 | 0.345 | - | - |
| Moore et al., 2008 1 [45] | SMRP | 156 | 171 | 0.505 | 0.443–0.568 | - | - | - | - |
| Lin et al., 2021 [44] | SCC-Ag | 101 | 475 | 0.512 | 0.407–0.617 | 0.903 | 0.208 | - | - |
| Lawicki et al., 2012 1,2 [46] | IL-3 | 65 | 40 | 0.527 | 0.413–0.641 | 0.800 | 0.980 | 0.830 | 0.430 |
| Kim et al., 2012 1 [47] | NLR | 238 | 596 | 0.539 | 0.495–0.583 | - | 0.512 | 0.591 | - |
| Lawicki et al., 2012 1,2 [46] | GM-CSF | 65 | 40 | 0.557 | 0.445–0.669 | 0.140 | 0.930 | 0.750 | 0.430 |
| Unuvar et al., 2020 [48] | TNC | 38 | 21 | 0.575 | 0.440–0.703 | 0.605 | 0.619 | 0.742 | 0.464 |
| Acceptable performance | |||||||||
| Orywal et al., 2013 [49] | Total ADH | 40 | 52 | 0.623 | 0.507–0.739 | 0.690 | 0.770 | 0.620 | 0.610 |
| Unuvar et al., 2020 [48] | Neopterin | 38 | 21 | 0.633 | 0.498–0.755 | 0.447 | 0.857 | 0.850 | 0.462 |
| Kim et al., 2012 1 [47] | Neutrophil | 238 | 596 | 0.641 | 0.598–0.684 | - | 0.794 | 0.237 | - |
| RosKar et al., 2021 [50] | Tie-2 | 36 | 36 | 0.652 | 0.525–0.779 | - | - | - | - |
| Cymbaluk-Ploska et al., 2020 [51] | FGF23 | 98 | 84 | 0.660 | 0.582–0.738 | - | - | - | - |
| Torres et al., 2019 [52] | EpCAM | 45 | 20 | 0.667 | 0.540–0.780 | 0.420 | 0.950 | 0.021 | 0.998 |
| Unuvar et al., 2020 [48] | Periostin | 38 | 21 | 0.668 | 0.533–0.785 | 0.526 | 0.857 | 0.870 | 0.500 |
| Cymbaluk-Ploska et al., 2018 [53] | Galectin-3 | 92 | 76 | 0.680 | 0.600–0.760 | 0.670 | 0.700 | - | - |
| Orywal et al., 2013 1,2 [49] | ADH1 | 40 | 52 | 0.682 | 0.570–0.793 | 0.600 | 0.630 | - | - |
| Kim et al., 2012 1 [47] | MNM | 238 | 596 | 0.696 | 0.655–0.737 | - | 0.629 | 0.691 | - |
| Ge et al., 2020 [54] | Fibrinogen | 127 | 96 | 0.690 | 0.625–0.724 | 0.925 | 0.244 | - | - |
| Good performance | |||||||||
| Lin et al., 2020 [44] | GP6 | 94 | 112 | 0.700 | 0.630–0.770 | - | - | - | - |
| Kim et al., 20121 [47] | Monocyte | 238 | 596 | 0.706 | 0.665–0.747 | - | 0.550 | 0.773 | - |
| Ge et al., 2020 [54] | Fibrinogen | 127 | 96 | 0.717 | 0.654–0.779 | 0.945 | 0.346 | - | - |
| Lin et al., 2020 [44] | GP4 | 94 | 112 | 0.720 | 0.650–0.790 | - | - | - | - |
| Lin et al., 2020 [44] | GP12 | 94 | 112 | 0.730 | 0.660–0.800 | - | - | - | - |
| Omer et al., 2013 [49] | SAA | 64 | 34 | 0.730 | 0.600–0.860 | 0.687 | 0.586 | 0.786 | 0.459 |
| Unuvar et al., 2020 [48] | IDO | 38 | 21 | 0.733 | 0.602–0.840 | 0.868 | 0.571 | 0.786 | 0.706 |
| Lin et al., 2020 [55] | GP14 | 94 | 112 | 0.740 | 0.680–0.810 | - | - | - | - |
| Lawicki et al., 2012 1,2 [46] | SCF | 65 | 40 | 0.751 | 0.659–0.843 | 0.430 | 0.930 | 0.900 | 0.530 |
| Cho et al., 20091 [56] | Osteopontin | 56 | 154 | 0.758 | 0.678–0.838 | 0.627 | 0.779 | - | - |
| Cymbaluk-Ploska et al., 2019 [57] | Lipocalin-2 | 52 | 67 | 0.760 | 0.660–0.850 | 0.840 | 0.780 | - | - |
| Kiseli et al., 2018 [58] | pro-GRP | 37 | 32 | 0.775 | 0.667–0.882 | 0.607 | 0.814 | 0.680 | 0.761 |
| Cymbaluk-Ploska et al., 2017 [59] | MMP2 | 62 | 50 | 0.790 | 0.707–0.873 | 0.680 | 0.860 | - | - |
| Lawicki et al., 2012 1,2 [46] | M-CSF | 65 | 40 | 0.794 | 0.710–0.878 | 0.690 | 0.930 | 0.940 | 0.680 |
| Nishikawa et al., 2012 1 [60] | GRO alpha | 39 | 38 | 0.799 | 0.699–0.899 | - | - | - | - |
| Excellent performance | |||||||||
| Cymbaluk-Ploska et al., 2020 [51] | FGF21 | 98 | 84 | 0.810 | 0.748–0.872 | - | - | - | - |
| Wang et al., 2019 [61] | Adiponectin | 53 | 98 | 0.814 | 0.747–0.881 | 0.857 | 0.726 | - | - |
| Cymbaluk-Ploska et al., 2018 [53] | Omentin-1 | 92 | 76 | 0.820 | 0.678–0.838 | 0.850 | 0.790 | - | - |
| Baser et al., 2013 2 [62] | SPAG9 | 63 | 37 | 0.820 | 0.739–0.901 | 0.740 | 0.830 | 0.880 | 0.645 |
| Jiang et al., 2019 [63] | TOPO48 | 80 | 80 | 0.826 | 0.743–0.913 | - | - | - | - |
| Stockley et al., 2020 [64] | MCM5 * | 41 | 58 | 0.830 | 0.740–0.920 | 0.878 | 0.759 | - | - |
| Torres et al., 2019 [52] | CD44 | 45 | 20 | 0.834 | 0.710–0.920 | 0.490 | 1.000 | 1.000 | 0.998 |
| Takano et al., 2010 1 [65] | m/z 28000 | 40 | 40 | 0.860 | 0.777–0.943 | 0.943 | - | - | - |
| Cymbaluk-Ploska et al., 2018 [53] | Vaspin | 92 | 76 | 0.860 | 0.804–0.916 | 0.890 | 0.830 | - | - |
| Takano et al., 2010 1 [65] | m/z 6680 | 40 | 40 | 0.880 | 0.803–0.957 | - | - | - | - |
| Takano et al., 2010 1 [65] | m/z 9300 | 40 | 40 | 0.880 | 0.039–0.803 | 0.957 | - | - | - |
| Deng et al., 2020 [66] | COX2 | 61 | 32 | 0.887 | 0.822–0.952 | 0.951 | 0.719 | - | - |
| Outstanding performance | |||||||||
| Torres et al., 2019 [52] | TGM2 | 45 | 20 | 0.901 | 0.790–0.970 | 0.780 | 1.000 | 1.000 | 0.999 |
| Takano et al., 2010 1 [65] | m/z 3340 | 40 | 40 | 0.920 | 0.032–0.857 | 0.983 | - | - | - |
| Zeng et al., 2016 [67] | IL-33 | 160 | 160 | 0.929 | 0.860–0.998 | - | - | - | - |
| Deng et al., 2020 [66] | wnt3a | 61 | 32 | 0.931 | 0.881–0.981 | 0.967 | 0.812 | - | - |
| Ciortea et al., 2014 1 [68] | IL-8 | 44 | 44 | 0.940 | 0.888–0.992 | - | - | - | - |
| Troisi et al., 2017 1 [69] | Progesterone | 88 | 80 | 0.965 | 0.925–1.000 | - | - | - | - |
| Zeng et al., 2016 1 [67] | IL-31 | 160 | 160 | 0.973 | 0.945–0.998 | - | - | - | - |
| Troisi et al., 2017 1 [69] | Lactic Acid | 88 | 80 | 1.000 | - | - | - | - | - |
| Author | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Nithin et al., 2018 [70] | 38 | 40 | 0.630 | 0.506–0.754 | 0.447 | 0.825 | 0.708 | 0.611 |
| Unuvar et al., 2020 [48] | 38 | 21 | 0.593 | 0.457–0.719 | 0.526 | 0.714 | 0.769 | 0.455 |
| Lin et al., 2020 [55] | 101 | 475 | 0.600 | 0.496–0.705 | 0.613 | 0.593 | - | - |
| Author | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Zeng et al., 2016 [67] | 160 | 160 | 0.751 | 0.645–0.857 | 0.813 | 0.479 | - | - |
| Bian et al., 2017 1 [71] | 105 | 87 | 0.510 | 0.423–0.572 | 0.163 | - | 0.510 | 0.590 |
| Ge et al., 2020 [54] | 96 | 31 | 0.681 | 0.615–0.746 | 0.945 | 0.047 | - | - |
| Unuvar et al., 2020 [48] | 38 | 21 | 0.528 | 0.393–0.659 | 0.290 | 1.000 | 1.000 | 0.438 |
| Lin et al., 2020 [55] | 101 | 475 | 0.620 | 0.498–0.743 | 0.548 | 0.747 | - | - |
| Author | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Moore et al., 2008 [45] | 156 | 171 | 0.550 | 0.487–0.614 | - | - | - | - |
| Bian et al., 2017 [71] | 105 | 87 | 0.561 | 0.497–0.623 | 0.113 | - | 0.500 | 0.650 |
| Karataş et al., 2018 [72] | 41 | 21 | 0.893 | 0.815–0.971 | 0.976 | 0.714 | - | - |
| Author | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Omer et al., 2013 [73] | 64 | 34 | 0.550 | 0.410–0.690 | 0.587 | 0.427 | 0.698 | 0.316 |
| Zeng et al., 2016 [67] | 160 | 160 | 0.644 | 0.524–0.764 | 0.800 | 0.457 | - | - |
| Nithin et al., 2018 [70] | 38 | 40 | 0.628 | 0.504–0.752 | 0.342 | 0.950 | 0.867 | 0.603 |
| Unuvar et al., 2020 [48] | 38 | 21 | 0.709 | 0.576–0.820 | 0.474 | 0.905 | 0.900 | 0.487 |
| Lin et al., 2021 [55] | 101 | 475 | 0.513 | 0.412–0.619 | 0.882 | 0.236 | - | - |
| Author | Cases (N) | Controls (N) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Cymbaluk-Ploska et al., 2018 [53] | 92 | 76 | 0.790 | 0.723–0.857 | 0.840 | 0.720 | - | - |
| Cymbaluk-Ploska et al., 2020 [51] | 98 | 84 | 0.790 | 0.725–0.855 | 0.820 | 0.710 | - | - |
| RosKar et al., 2021 [50] | 36 | 36 | 0.634 | 0.506–0.762 | - | - | - | - |
| Author | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Nithin et al., 2018 [70] | 38 | 40 | 0.634 | 0.510–0.758 | 0.386 | 0.875 | 0.737 | 0.593 |
| Yurkovetsky et al., 2007 [74] | 115 | 135 | 0.997 | 0.990–1.004 | 0.983 | 0.980 | - | - |
| Author | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Tian et al., 2013 [75] | 120 | 70 | 0.603 | 0.528–0.677 | 0.758 | 0.567 | - | 0.542 |
| Wang et al., 2018 [61] | 53 | 98 | 0.484 | 0.388–0.579 | - | - | - | - |
| Author | Cases (N) | Controls (N) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Fan et al., 2013 [76] | 50 | 50 | 0.807 | 0.709–0.905 | 0.735 | 0.816 | 0.694 | 0.844 |
| Kemik et al., 2016 [77] | 34 | 60 | 0.823 | 0.740–0.906 | 0.940 | 0.480 | - | - |
| Kotowicz et al., 2017 [78] | 41 | 21 | 0.804 | 0.726–0.900 | 0.689 | 0.800 | - | - |
| Diefenbach et al., 2017 [79] | 34 | 44 | 0.870 | 0.785–0.955 | 0.760 | 0.930 | - | - |
| Karataş et al., 2018 [72] | 74 | 25 | 0.659 | 0.521–0.797 | 0.366 | 0.952 | 0.938 | 0.435 |
| Unuvar et al., 2020 [48] | 38 | 21 | 0.517 | 0.383–0.649 | 0.605 | 0.571 | 0.719 | 0.444 |
| Author | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Di Cello et al., 2017 [80] | 101 | 44 | 0.890 | 0.839–0.941 | 0.753 | 0.796 | 0.583 | 0.894 |
| Benati et al., 2018 [81] | 45 | 29 | 0.950 | 0.910–0.990 | 0.890 | 0.900 | - | - |
| Author | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| Lawicki et al., 2012 [46] | 65 | 40 | 0.715 | 0.618–0.812 | 0.210 | 0.930 | 0.820 | 0.450 |
| RosKar et al., 2021 [50] | 36 | 36 | 0.641 | 0.513–0.769 | - | - | - | - |
| Author | Metabolite | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|---|
| Good performance | |||||||||
| Kozar et al., 2020 4 [82] | 1-Methyladenosine | 15 | 21 | 0.746 | 0.576–0.916 | 0.670 | 0.810 | - | - |
| Schuhn et al., 2022 1 [38] | One CpG site at at S100P, | 20 | 157 | 0.750 | 0.641–0.858 | 0.895 | 0.545 | - | - |
| Schuhn et al., 2022 1 [38] | Tetrade-Cenoylcarnitine | 20 | 157 | 0.751 | 0.647–0.856 | 0.800 | 0.690 | - | - |
| Kozar et al., 2020 4 [82] | AC 16:1-OH | 15 | 21 | 0.759 | 0.577–0.941 | 0.600 | 0.950 | - | - |
| Kozar et al., 2020 4 [82] | Cer 40:1; 2 | 15 | 21 | 0.768 | 0.610–0.927 | 0.670 | 0.810 | - | - |
| Schuhn et al., 2022 1 [38] | One CpG site at RAPSN | 20 | 157 | 0.772 | 0.665–0.889 | 0.737 | 0.752 | - | - |
| Schuhn et al., 2022 1 [38] | Carnitine | 20 | 157 | 0.792 | 0.710–0.873 | 0.950 | 0.579 | - | - |
| Schuhn et al., 2022 1 [38] | Acetylcarnitine | 20 | 157 | 0.800 | 0.715–0.884 | 0.950 | 0.608 | - | - |
| Excellent performance | |||||||||
| Njoku et al., 2021 2 [83] | 3-Hydroxybutyrate | 67 | 69 | 0.817 | 0.737–0.884 | - | - | - | - |
| Schuhn et al., 2022 1 [83] | Malonylcarnitine | 20 | 157 | 0.819 | 0.721–0.918 | 0.800 | 0.731 | - | - |
| Njoku et al., 2021 2 [83] | 1-1- Enyl-Stearoyl-2 Oleoyl GPE | 67 | 69 | 0.825 | 0.750–0.888 | - | - | - | - |
| Njoku et al., 2021 2 [83] | 3-Hydroxy-Butyrlcarnitine | 67 | 69 | 0.826 | 0.752–0.853 | - | - | - | - |
| Kozar et al., 2020 4 [82] | Cer 34:1; 2 | 15 | 21 | 0.835 | 0.705–0.965 | 0.730 | 0.810 | - | - |
| Njoku et al., 2021 2 [83] | 1-1- Enyl-Stearoyl-GPE | 67 | 69 | 0.841 | 0.767–0.900 | - | - | - | - |
| Njoku et al., 2021 2 [83] | 1-linolenoyl-GPC | 67 | 69 | 0.844 | 0.776–0.909 | - | - | - | - |
| Njoku et al., 2021 2 [83] | 1-(1-enyl-stearoyl)-2-linoleoyl-GPE | 67 | 69 | 0.853 | 0.780–0.910 | - | - | - | - |
| Outstanding performance | |||||||||
| Njoku et al., 2021 2 [83] | 1-Lignoceroyl GPC | 67 | 69 | 0.910 | 0.860–0.950 | - | - | - | - |
| Troisi et al., 2018 3 [69] | Stearic Acid | 88 | 80 | 0.943 | 0.893–0.979 | - | - | - | - |
| Troisi et al., 2018 3 [69] | Homocysteine | 88 | 80 | 0.952 | 0.906–0.989 | - | - | - | - |
| Troisi et al., 2018 3 [69] | Threonine | 88 | 80 | 0.979 | 0.933–1.000 | - | - | - | - |
| Troisi et al., 2018 3 [69] | Valine | 88 | 80 | 0.999 | 0.995–1.000 | - | - | - | - |
| Troisi et al., 2008 3 [69] | Myristic Acid | 88 | 80 | 1.000 | 0.996–1.000 | - | - | - | - |
| Author | Biomarker | Cases (n) | Controls (n) | AUC | AUC 95%CI | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|---|
| Cicchillitti et al., 2017 [84] | cCFDNA | 59 | 21 | 0.704 | 0.632–0.777 | 0.521 | 0.839 | - | - |
| Jiang et al., 2019 [63] | cCFDNA | 80 | 80 | 0.791 | 0.657–0.887 | - | - | - | - |
| Benati et al., 2020 [85] | Survivin-expressing CTC | 40 | 31 | 0.870 | 0.790–0.950 | 0.800 | 0.807 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karkia, R.; Wali, S.; Payne, A.; Karteris, E.; Chatterjee, J. Diagnostic Accuracy of Liquid Biomarkers for the Non-Invasive Diagnosis of Endometrial Cancer: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 4666. https://doi.org/10.3390/cancers14194666
Karkia R, Wali S, Payne A, Karteris E, Chatterjee J. Diagnostic Accuracy of Liquid Biomarkers for the Non-Invasive Diagnosis of Endometrial Cancer: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(19):4666. https://doi.org/10.3390/cancers14194666
Chicago/Turabian StyleKarkia, Rebecca, Sarah Wali, Annette Payne, Emmanouil Karteris, and Jayanta Chatterjee. 2022. "Diagnostic Accuracy of Liquid Biomarkers for the Non-Invasive Diagnosis of Endometrial Cancer: A Systematic Review and Meta-Analysis" Cancers 14, no. 19: 4666. https://doi.org/10.3390/cancers14194666