
Management of Patients with Newly Diagnosed Desmoid Tumors in a First-Line Setting

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Active Surveillance and Treatment
2.3. Assessment of Adverse Events and Complications
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Patient Characteristics
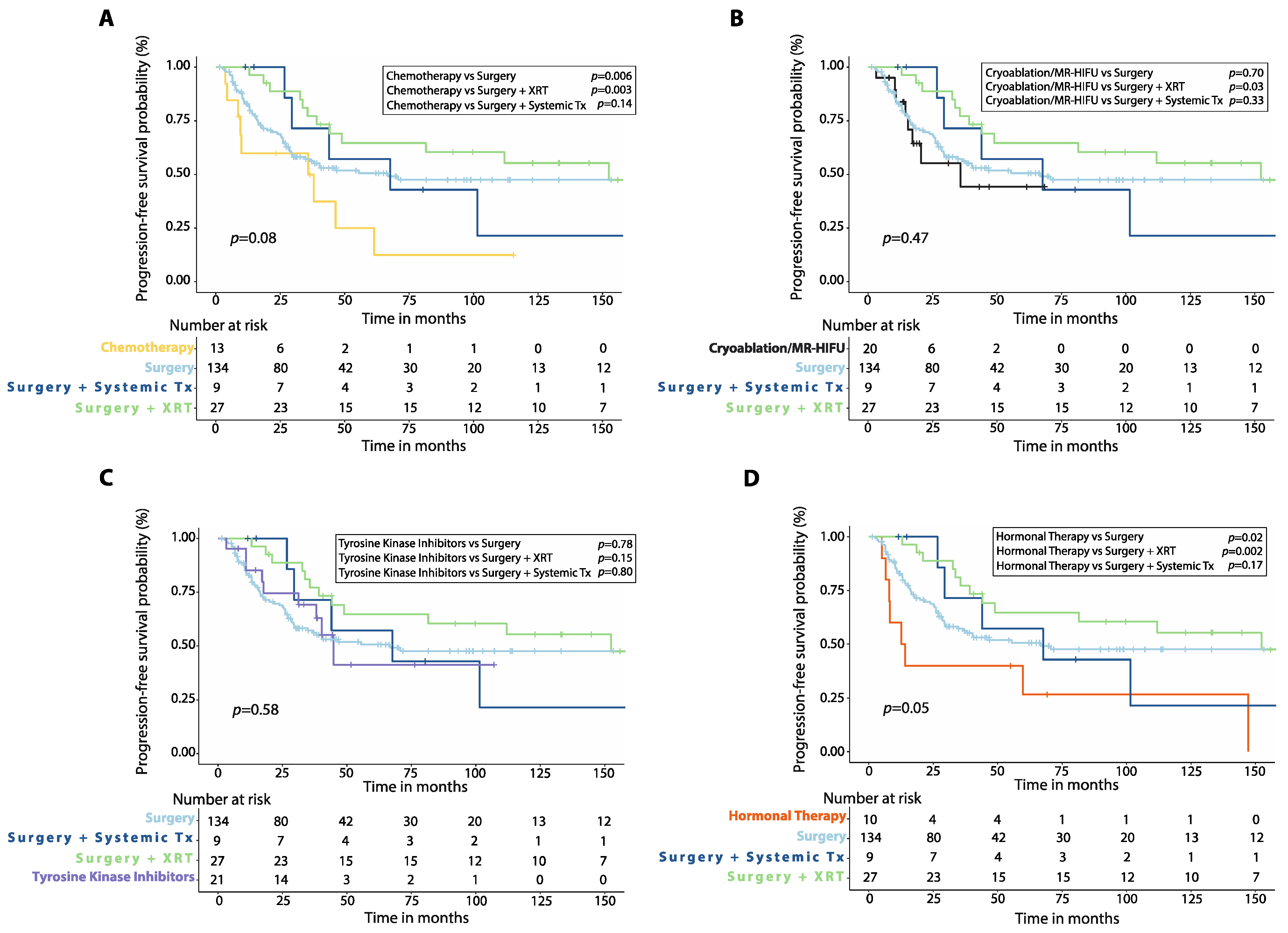
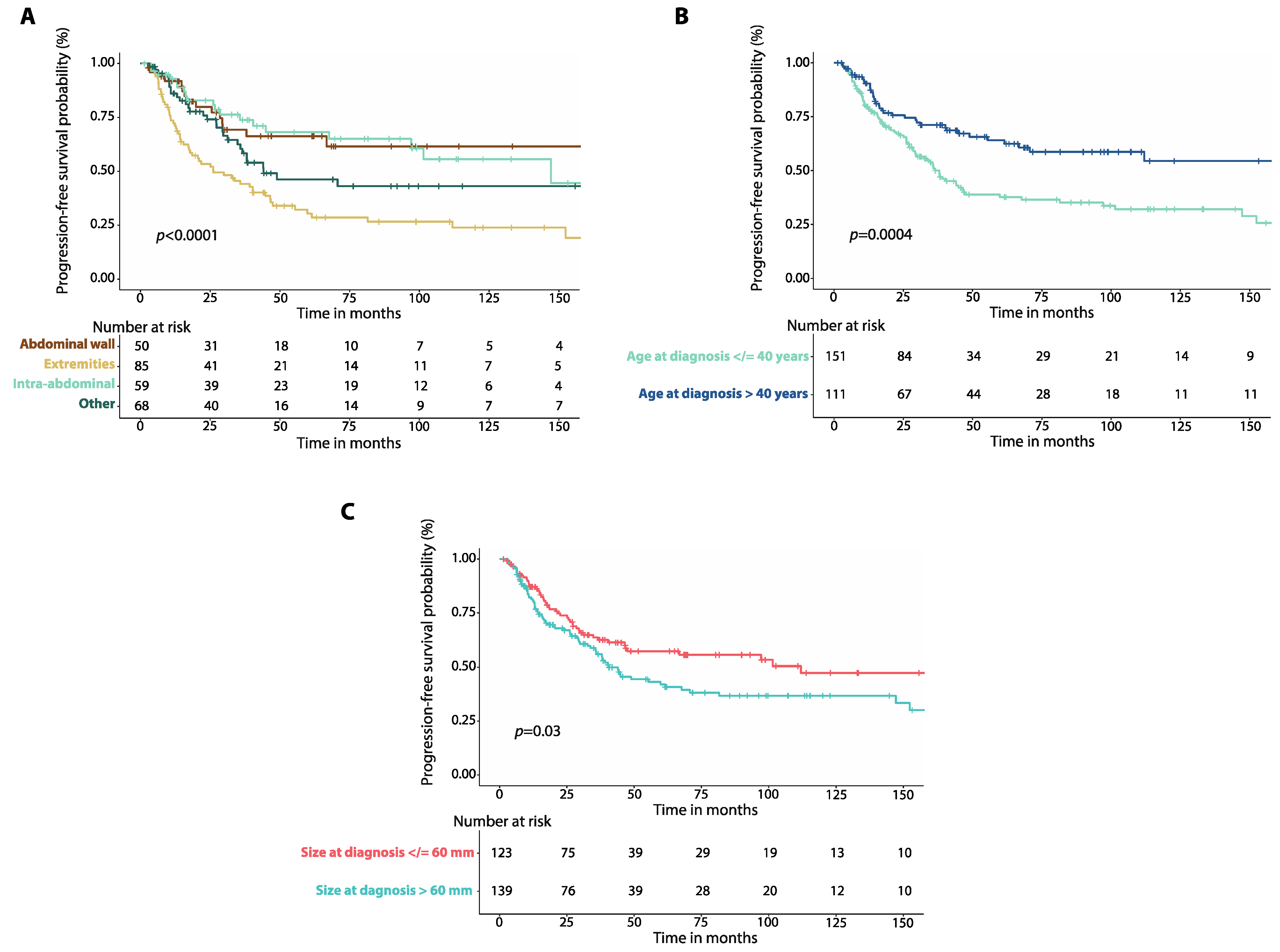
3.2. Progression-Free Survival
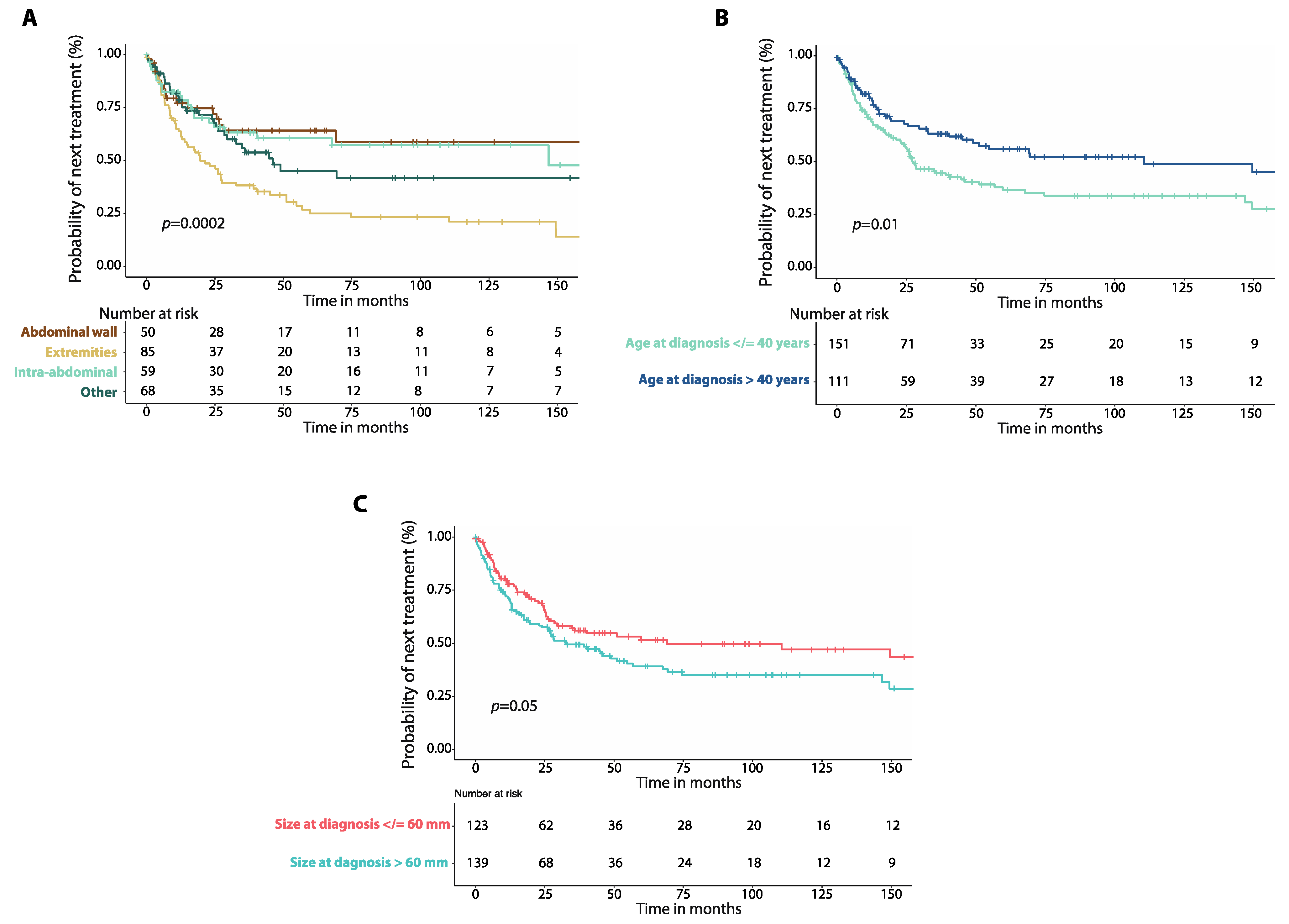
3.3. Time to Next Treatment
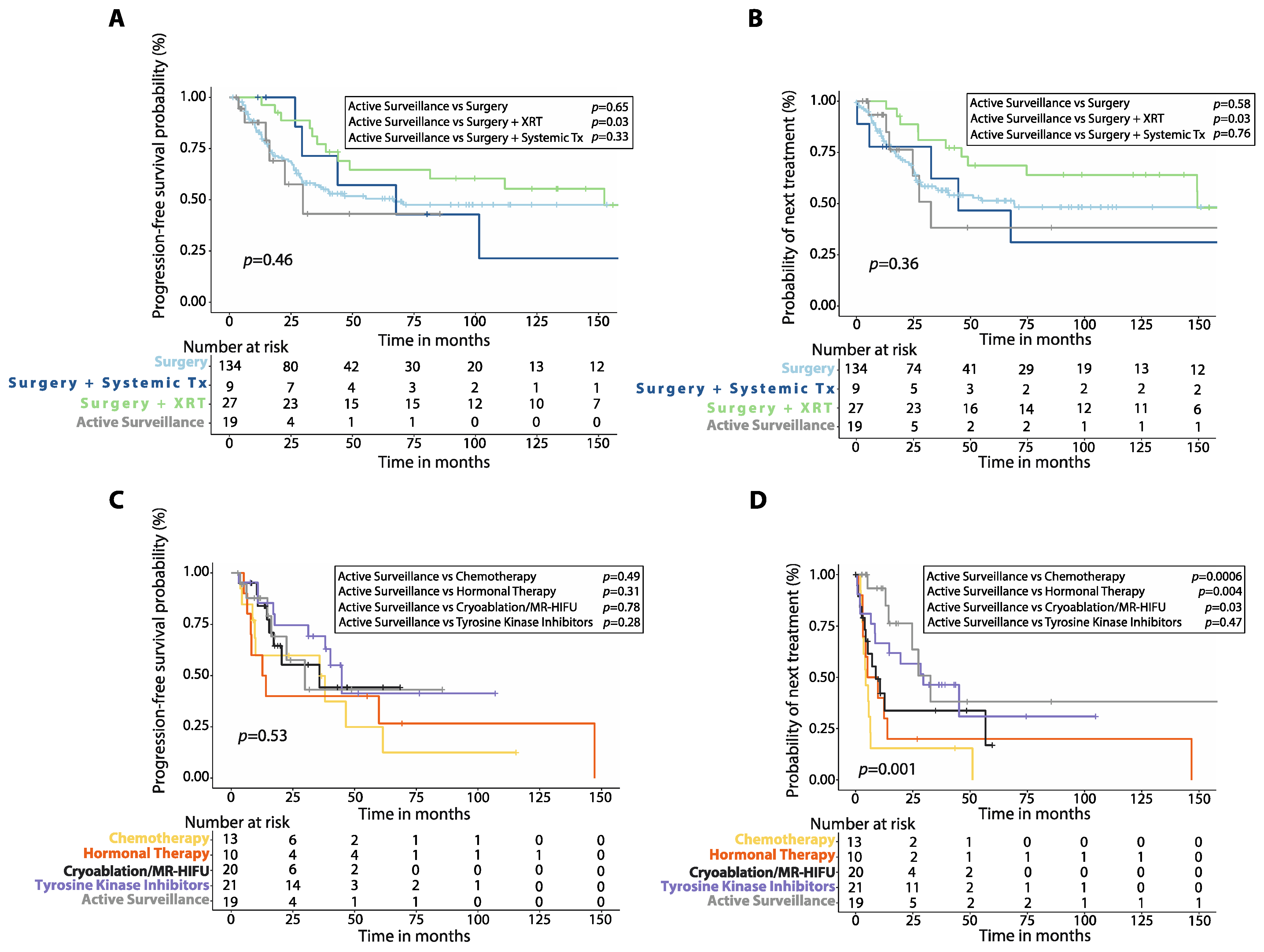
3.4. Active Surveillance vs. Upfront Treatment
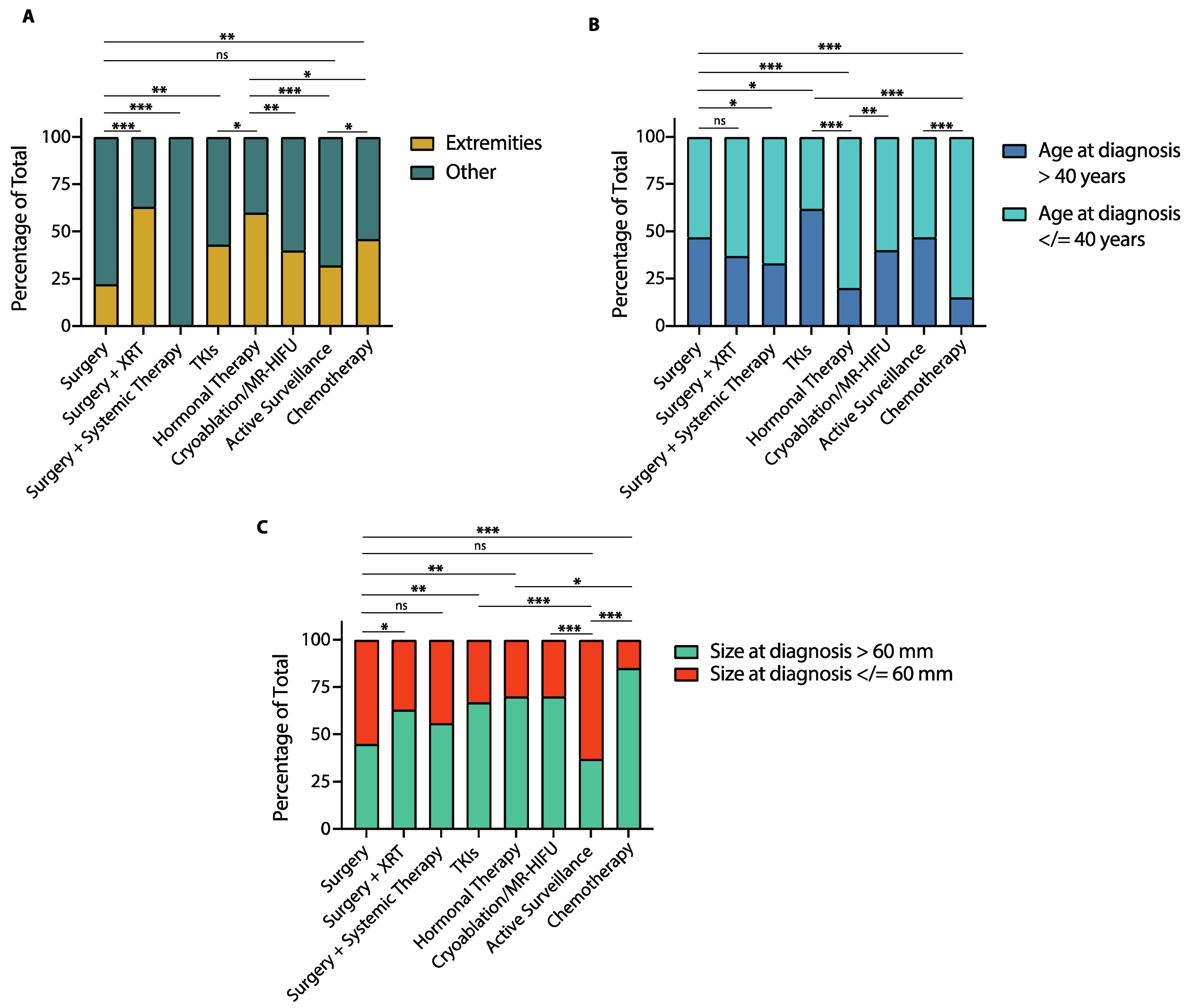
3.5. Baseline Characteristics and Treatment Modality
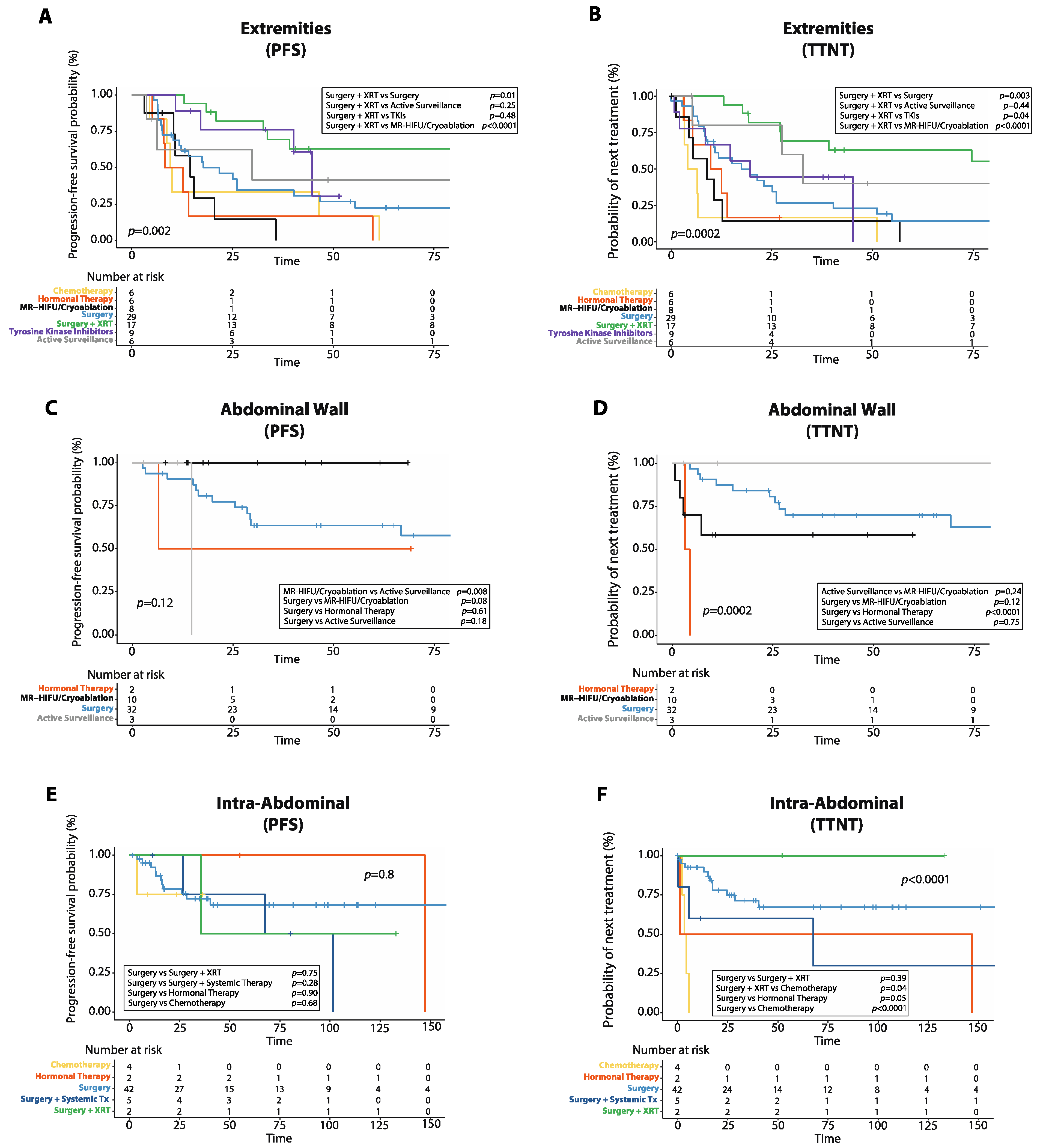
3.6. Progression-Free Survival and Time to Next Treatment by Tumor Location
3.7. Adverse Events and Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reitamo, M.J.J.; Häyry, M.P.; Nykyri, M.E.; Saxen, M.E. The Desmoid Tumor. I.: Incidence, Sex-, Age- and Anatomical Distribution in the Finnish Population. Am. J. Clin. Pathol. 1982, 77, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Van Broekhoven, D.L.M.; Grünhagen, D.J.; Bakker, M.A.D.; Van Dalen, T.; Verhoef, C. Time Trends in the Incidence and Treatment of Extra-Abdominal and Abdominal Aggressive Fibromatosis: A Population-Based Study. Ann. Surg. Oncol. 2015, 22, 2817–2823. [Google Scholar] [CrossRef]
- Koskenvuo, L.; Ristimäki, A.; Lepistö, A.H. Comparison of sporadic and FAP-associated desmoid-type fibromatoses. J. Surg. Oncol. 2017, 116, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Crago, A.M.; Chmielecki, J.; Rosenberg, M.; O’Connor, R.; Byrne, C.; Wilder, F.G.; Thorn, K.; Agius, P.; Kuk, D.; Socci, N.D.; et al. Near universal detection of alterations in CTNNB1 and Wnt pathway regulators in desmoid-type fibromatosis by whole-exome sequencing and genomic analysis. Genes Chromosom. Cancer 2015, 54, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Salas, S.; Chibon, F.; Noguchi, T.; Terrier, P.; Ranchere-Vince, D.; Lagarde, P.; Benard, J.; Forget, S.; Blanchard, C.; Dômont, J.; et al. Molecular characterization by array comparative genomic hybridization and DNA sequencing of 194 desmoid tumors. Genes Chromosom. Cancer 2010, 49, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Devata, S.; Chugh, R. Desmoid Tumors: A comprehensive review of the evolving biology, unpredictable behavior, and myriad of management options. Hematol. Clin. N. Am. 2013, 27, 989–1005. [Google Scholar] [CrossRef]
- Bonvalot, S.; Ternès, N.; Fiore, M.; Bitsakou, G.; Colombo, C.; Honoré, C.; Marrari, A.; Le Cesne, A.; Perrone, F.; Dunant, A.; et al. Spontaneous Regression of Primary Abdominal Wall Desmoid Tumors: More Common than Previously Thought. Ann. Surg. Oncol. 2013, 20, 4096–4102. [Google Scholar] [CrossRef] [PubMed]
- Ballo, M.T.; Zagars, G.K.; Pollack, A.; Pisters, P.W.; Pollock, R.A. Desmoid Tumor: Prognostic Factors and Outcome After Surgery, Radiation Therapy, or Combined Surgery and Radiation Therapy. J. Clin. Oncol. 1999, 17, 158–167. [Google Scholar] [CrossRef]
- Mullen, J.T.; Delaney, T.F.; Kobayashi, W.K.; Szymonifka, J.; Yeap, B.Y.; Chen, Y.-L.; Rosenberg, A.E.; Harmon, D.C.; Choy, E.; Yoon, S.S.; et al. Desmoid Tumor: Analysis of Prognostic Factors and Outcomes in a Surgical Series. Ann. Surg. Oncol. 2012, 19, 4028–4035. [Google Scholar] [CrossRef]
- Al-Jazrawe, M.; Au, M.; Alman, B. Optimal therapy for desmoid tumors: Current options and challenges for the future. Expert Rev. Anticancer Ther. 2015, 15, 1443–1458. [Google Scholar] [CrossRef] [PubMed]
- Colombo, C.; Miceli, R.; Le Péchoux, C.; Palassini, E.; Honoré, C.; Stacchiotti, S.; Mir, O.; Casali, P.; Dômont, J.; Fiore, M.; et al. Sporadic extra abdominal wall desmoid-type fibromatosis: Surgical resection can be safely limited to a minority of patients. Eur. J. Cancer 2015, 51, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Alman, B.; Attia, S.; Baumgarten, C.; Benson, C.; Blay, J.-Y.; Bonvalot, S.; Breuing, J.; Cardona, K.; Casali, P.G.; van Coevorden, F.; et al. The management of desmoid tumours: A joint global consensus-based guideline approach for adult and paediatric patients. Eur. J. Cancer 2020, 127, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Batalni, J.P.; Belloir, C.; Mazabraud, A.; Pilleron, J.P.; Cartigny, A.; Jaulerry, C.; Ghossein, N.A. Desmoid tumors in adults: The role of radiotherapy in their management. Am. J. Surg. 1988, 155, 754–760. [Google Scholar] [CrossRef]
- Bishop, A.J.; Zarzour, M.A.; Ratan, R.; Torres, E.K.; Feig, B.W.; Wang, W.-L.; Lazar, A.; Moon, B.S.; Roland, C.L.; Guadagnolo, B.A. Long-Term Outcomes for Patients with Desmoid Fibromatosis Treated With Radiation Therapy: A 10-Year Update and Re-evaluation of the Role of Radiation Therapy for Younger Patients. Int. J. Radiat. Oncol. 2019, 103, 1167–1174. [Google Scholar] [CrossRef]
- Zhang, R.; Chen, J.-Y.; Zhang, L.; Li, K.-Q.; Xiao, Z.-B.; Mo, S.-J.; Chen, L.; Chen, W.-Z. The safety and ablation efficacy of ultrasound-guided high-intensity focused ultrasound ablation for desmoid tumors. Int. J. Hyperth. 2021, 38, 89–95. [Google Scholar] [CrossRef]
- Kurtz, J.-E.; Buy, X.; Deschamps, F.; Sauleau, E.; Bouhamama, A.; Toulmonde, M.; Honoré, C.; Bertucci, F.; Brahmi, M.; Chevreau, C.; et al. CRYODESMO-O1: A prospective, open phase II study of cryoablation in desmoid tumour patients progressing after medical treatment. Eur. J. Cancer 2021, 143, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Freites-Martinez, A.; Santana, N.; Arias-Santiago, S.; Viera, A. Using the Common Terminology Criteria for Adverse Events (CTCAE—Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies. Actas Dermo-Sifiliográficas 2020, 112, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Kassambara, A.; Kosinski, M.; Biecek, P. Survminer: Drawing Survival Curves Using ‘ggplot2’. 2019. Available online: https://CRAN.R-project.org/package=survminer (accessed on 1 March 2022).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Choudhary, S.; McLeod, M.; Torchia, D.; Romanelli, P. Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syn-drome. J. Clin. Aesthet. Dermatol. 2013, 6, 31–37. [Google Scholar]
- Baumert, B.G.; Spahr, O.M.; Von Hochstetter, A.; Beauvois, S.; Landmann, C.; Fridrich, K.; Villà, S.; Kirschner, M.J.; Storme, G.; Thum, P.; et al. The impact of radiotherapy in the treatment of desmoid tumours. An international survey of 110 patients. A study of the Rare Cancer Network. Radiat. Oncol. 2007, 2, 12. [Google Scholar] [CrossRef]
- Skapek, S.X.; Anderson, J.R.; Hill, D.A.; Henry, D.; Spunt, S.L.; Meyer, W.; Kao, S.; Hoffer, F.A.; Grier, H.E.; Hawkins, D.S.; et al. Safety and efficacy of high-dose tamoxifen and sulindac for desmoid tumor in children: Results of a Children’s Oncology Group (COG) Phase II Study. Pediatr. Blood Cancer 2013, 60, 1108–1112. [Google Scholar] [CrossRef]
- Libertini, M.; Mitra, I.; Van Der Graaf, W.T.A.; Miah, A.B.; Judson, I.; Jones, R.L.; Thomas, K.; Moskovic, E.; Szucs, Z.; Benson, C.; et al. Aggressive fibromatosis response to tamoxifen: Lack of correlation between MRI and symptomatic response. Clin. Sarcoma Res. 2018, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- Palassini, E.; Frezza, A.M.; Mariani, L.; Lalli, L.; Colombo, C.; Fiore, M.; Messina, A.; Casale, A.; Morosi, C.; Collini, P.; et al. Long-term Efficacy of Methotrexate Plus Vinblastine/Vinorelbine in a Large Series of Patients Affected by Desmoid-Type Fibromatosis. Cancer J. 2017, 23, 86–91. [Google Scholar] [CrossRef]
- Moding, E.J.; Million, L.; Avedian, R.; Ghanouni, P.; Kunder, C.; Ganjoo, K.N. Concurrent Imatinib and Radiation Therapy for Unresectable and Symptomatic Desmoid Tumors. Sarcoma 2017, 2017, 2316839. [Google Scholar] [CrossRef] [PubMed]
- Penel, N.; Le Cesne, A.; Bui, B.N.; Perol, D.; Brain, E.G.; Ray-Coquard, I.; Guillemet, C.; Chevreau, C.; Cupissol, D.; Chabaud, S.; et al. Imatinib for progressive and recurrent aggressive fibromatosis (desmoid tumors): An FNCLCC/French Sarcoma Group phase II trial with a long-term follow-up. Ann. Oncol. 2011, 22, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Chugh, R.; Wathen, J.K.; Patel, S.R.; Maki, R.G.; Meyers, P.A.; Schuetze, S.M.; Priebat, D.A.; Thomas, D.G.; Jacobson, J.A.; Samuels, B.L.; et al. Efficacy of Imatinib in Aggressive Fibromatosis: Results of a Phase II Multicenter Sarcoma Alliance for Research through Collaboration (SARC) Trial. Clin. Cancer Res. 2010, 16, 4884–4891. [Google Scholar] [CrossRef] [PubMed]
- Gounder, M.M.; Mahoney, M.R.; Van Tine, B.A.; Ravi, V.; Attia, S.; Deshpande, H.A.; Gupta, A.A.; Milhem, M.; Conry, R.M.; Movva, S.; et al. Sorafenib for Advanced and Refractory Desmoid Tumors. N. Engl. J. Med. 2018, 379, 2417–2428. [Google Scholar] [CrossRef]
- Bouhamama, A.; Lame, F.; Mastier, C.; Cuinet, M.; Thibaut, A.; Beji, H.; Ricoeur, A.; Blay, J.-Y.; Pilleul, F. Local Control and Analgesic Efficacy of Percutaneous Cryoablation for Desmoid Tumors. Cardiovasc. Interv. Radiol. 2020, 43, 110–119. [Google Scholar] [CrossRef]
- Ghanouni, P.; Dobrotwir, A.; Bazzocchi, A.; Bucknor, M.; Bitton, R.; Rosenberg, J.; Telischak, K.; Busacca, M.; Ferrari, S.; Albisinni, U.; et al. Magnetic resonance-guided focused ultrasound treatment of extra-abdominal desmoid tumors: A retrospective multicenter study. Eur. Radiol. 2017, 27, 732–740. [Google Scholar] [CrossRef]
- Testa, S.; Bui, N.Q.; Wang, D.S.; Louie, J.D.; Sze, D.Y.; Ganjoo, K.N. Efficacy and Safety of Trans-Arterial Yttrium-90 Radioembolization in Patients with Unresectable Liver-Dominant Metastatic or Primary Hepatic Soft Tissue Sarcomas. Cancers 2022, 14, 324. [Google Scholar] [CrossRef]
- Vora, B.M.K.; Munk, P.L.; Somasundaram, N.; Ouellette, H.A.; Mallinson, P.I.; Sheikh, A.; Kadir, H.A.; Tan, T.J.; Yan, Y.Y. Cryotherapy in extra-abdominal desmoid tumors: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0261657. [Google Scholar] [CrossRef]
- Penel, N.; Le Cesne, A.; Bonvalot, S.; Giraud, A.; Bompas, E.; Rios, M.; Salas, S.; Isambert, N.; Boudou-Rouquette, P.; Honore, C.; et al. Surgical versus non-surgical approach in primary desmoid-type fibromatosis patients: A nationwide prospective cohort from the French Sarcoma Group. Eur. J. Cancer 2017, 83, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Timbergen, M.J.; Schut, A.-R.W.; Grünhagen, D.J.; Sleijfer, S.; Verhoef, C. Active surveillance in desmoid-type fibromatosis: A systematic literature review. Eur. J. Cancer 2020, 137, 18–29. [Google Scholar] [CrossRef] [PubMed]
- de Bénazé, G.D.; Vigan, M.; Corradini, N.; Minard-Colin, V.; Marie-Cardine, A.; Verite, C.; Defachelles, A.-S.; Thebaud, E.; Castex, M.; Sirvent, N.; et al. Functional analysis of young patients with desmoid-type fibromatosis: Initial surveillance does not jeopardize long term quality of life. Eur. J. Surg. Oncol. 2020, 46, 1294–1300. [Google Scholar] [CrossRef]
- Salas, S.; Dufresne, A.; Bui, B.; Blay, J.-Y.; Terrier, P.; Ranchere-Vince, D.; Bonvalot, S.; Stoeckle, E.; Guillou, L.; Le Cesne, A.; et al. Prognostic Factors Influencing Progression-Free Survival Determined From a Series of Sporadic Desmoid Tumors: A Wait-and-See Policy According to Tumor Presentation. J. Clin. Oncol. 2011, 29, 3553–3558. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age at Diagnosis | |
| Median in years (range) | 36.5 (0–87) |
| Site | |
| Extremities | 85 (32.4%) |
| Intra-abdominal | 59 (22.5%) |
| Abdominal wall | 50 (19.0%) |
| Other a | 68 (25.9%) |
| Size at diagnosis (cm) | |
| Median (range) | 6.6 (1–30.0) |
| Sex | |
| Male (n, %) | 77 (29.4%) |
| Female (n, %) | 185 (70.6%) |
| Treatment (First-line) | |
| Surgery (n, %) | 134 (51.1%) |
| Surgery + XRT (n, %) | 27 (10.3%) |
| Surgery + Systemic Treatment (n, %) | 9 (3.4%) |
| Chemotherapy (n, %) | 13 (4.9%) |
| Hormonal Therapy (n, %) | 10 (3.8%) |
| TKIs (n, %) | 21 (8.0%) |
| Cryoablation/MR-HIFU (n, %) | 20 (7.6%) |
| Active surveillance (n, %) | 19 (7.2%) |
| Other b (n, %) | 9 (3.4%) |
| Follow-up (months) | |
| Median (range) | 63 (1–286) |
| FAP | |
| Yes (n, %) | 14 (5.3%) |
| No (n, %) | 248 (94.7%) |
| Mutation | |
| CTNNB1 p.T41A (n, %) | 20 (7.6%) |
| CTNNB1 p.S45F (n, %) | 8 (3.0%) |
| APC (n, %) | 14 (5.3%) |
| Other c (n, %) | 3 (1.1%) |
| Not available (n, %) | 228 (87.0%) |
| Status at last follow-up | |
| Deceased (n, %) | 4 (1.6%) |
| Alive WD (n, %) | 118 (45.0%) |
| Alive NED (n, %) | 140 (53.4%) |
| PFS | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|
| Variables | Patients (Events) | 1-Year (95% CI) | 5-Year (95% CI) | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| First-line Treatment | |||||||
| Surgery | 134 (58) | 82.2% (74.4–87.8%) | 50.6% (41.0–59.5%) | 0.9 (0.6–1.3) | 0.66 | 1.5 (0.7–3.1) | 0.26 |
| Surgery plus XRT | 27 (10) | 100% (N/A) | 64.9% (43.2–80%) | 0.4 (0.2–0.9) | 0.02 | 0.4 (0.1–0.9) | 0.04 |
| Surgery plus Systemic Therapy | 9 (5) | 100% (N/A) | 57.1% (17.2–83.7%) | 1.1 (0.4–2.5) | 0.98 | 1.5 (0.5–5.0) | 0.45 |
| Chemotherapy | 13 (9) | 59.8% (28.5–80.0%) | 24.9% (4.3–54.2%) | 1.9 (1.0–3.9) | 0.05 | 1.3 (0.5–3.4) | 0.59 |
| Hormonal Therapy | 10 (8) | 60.0% (25.3–82.7%) | 26.7% (4.7–56.3%) | 2.2 (1.1–4.5) | 0.03 | 1.7 (0.7–4.7) | 0.25 |
| TKIs | 21 (9) | 85.2% (60.8–95%) | 41.3% (13.7–67.4%) | 0.9 (0.5–1.8) | 0.83 | 0.9 (0.3–2.4) | 0.83 |
| Cryoablation/MR-HIFU | 20 (8) | 83.8% (57.7–94.4%) | 44.4% (16.8–69.1%) | 1.2 (0.6–2.5) | 0.59 | 1.3 (0.5–3.5) | 0.60 |
| Active Surveillance | 19 (6) | 87.7% (58.8–96.8%) | 43.1% (12.2–71.4%) | 1.3 (0.5–2.8) | 0.57 | 1.1 (0.4–3.1) | 0.88 |
| Other a | 9 (5) | 88.8% (43.2–98.3%) | 55.5% (20.4–80.4%) | 0.9 (0.4–2.2) | 0.79 | – | – |
| Age (years) | |||||||
| >40 | 111 (37) | 90.4% (82.9–94.7%) | 64.1% (53.1–73.2%) | 0.5 (0.4–0.7) | <0.001 | – | – |
| ≤40 | 151 (85) | 79.7% (72.3–85.4%) | 37.7% (28.8–46.5%) | 1.9 (1.3–2.9) | <0.001 | 1.9 (1.3–2.9) | 0.002 |
| Sex | |||||||
| Male | 77 (38) | 86.4% (76.3–92.4%) | 53.3% (40.4–64.7%) | 1.0 (0.7–1.5) | 0.86 | – | – |
| Female | 185 (84) | 83.1% (76.8–87.8%) | 46.9% (38.4–54.9%) | 0.9 (0.7–1.4) | 0.86 | 0.7 (0.5–1.1) | 0.18 |
| Tumor site | |||||||
| Intra-abdominal | 59 (19) | 92.8% (82.0–97.2%) | 68.1% (52.2–79.7%) | 0.5 (0.3–0.9) | 0.01 | 0.4 (0.2–0.7) | 0.004 |
| Abdominal Wall | 50 (15) | 91.8% (79.6–96.8%) | 66.2% (49.4–78.6%) | 0.5 (0.3–0.9) | 0.03 | 0.5 (0.3–0.9) | 0.04 |
| Extremities | 85 (58) | 72.3% (61.4–80.6%) | 30.4% (20.2–41.2%) | 2.2 (1.6–3.2) | <0.001 | 2.0 (1.2–3.2) | 0.003 |
| Other b | 68 (30) | 86.0% (74.9–92.4%) | 46.2% (31.8–59.4%) | 0.9 (0.6–1.4) | 0.72 | – | – |
| Tumor size | |||||||
| >60 mm | 139 (74) | 84.3% (76.9–89.5%) | 42.1% (32.6–51.3%) | 1.5 (1.0–2.1) | 0.04 | 1.4 (0.9–2.1) | 0.06 |
| ≤60 mm | 123 (48) | 83.8% (75.8–89.3%) | 57.2% (46.7–66.4%) | 0.7 (0.5–0.9) | 0.04 | – | – |
| Mutation | |||||||
| CTNNB1 p.T41A | 20 (9) | 89.5% (65.1–97.3%) | 65.4% (38.3–82.9%) | 1.4 (0.7–2.8) | 0.28 | 1.8 (0.9–3.7) | 0.11 |
| CTNNB1 p.S45F | 8 (4) | 85.7% (33.4–97.8%) | 85.7% (33.4–97.8%) | 1.8 (0.7–4.9) | 0.24 | 1.5 (0.5–4.5) | 0.41 |
| APC | 14 (9) | 92.9% (59.1–99.0%) | 50.6% (21.2–74.1%) | 1.2 (0.6–2.3) | 0.62 | 1.7 (0.7–3.7) | 0.20 |
| Other c | 3 (3) | 66.7% (5.4–94.5%) | 33.3% (0.9–77.4%) | 1.8 (0.6–5.6) | 0.32 | 2.2 (0.6–8.0) | 0.21 |
| TTNT | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|
| Variables | Patients (Events) | Median (Months) | (95% CI) | HR (95% CI) | p Value | HR (95% CI) | p Value |
| First-line Treatment | |||||||
| Surgery | 134 (58) | 69.1 | Not reached | 0.6 (0.4–0.9) | 0.008 | 0.8 (0.4–1.6) | 0.54 |
| Surgery plus XRT | 27 (11) | 149.5 | Not reached | 0.4 (0.2–0.7) | 0.005 | 0.3 (0.1–0.7) | 0.004 |
| Surgery plus Systemic Therapy | 9 (5) | 44.7 | 2.9–86.4 | 1.0 (0.4–2.5) | 0.95 | 0.9 (0.3–3.0) | 0.97 |
| Chemotherapy | 13 (12) | 4.4 | 2.0–6.7 | 4.9 (2.8–9.2) | <0.001 | 4.0 (1.7–9.6) | 0.002 |
| Hormonal Therapy | 10 (9) | 5.3 | 0.0–13.6 | 3.3 (1.7–6.6) | <0.001 | 1.8 (0.7–4.5) | 0.21 |
| TKIs | 21 (12) | 29.6 | 8.0–51.1 | 1.3 (0.7–2.3) | 0.39 | 0.9 (0.4–2.3) | 0.98 |
| Cryoablation/MR-HIFU | 20 (12) | 8.9 | 2.7–15.1 | 2.4 (1.3–4.4) | 0.004 | 2.2 (0.9–5.4) | 0.07 |
| Active Surveillance | 19 (7) | 32.7 | 22.4–42.9 | 0.9 (0.4–1.9) | 0.81 | 0.6 (0.2–1.7) | 0.40 |
| Other a | 9 (7) | 45.1 | 25.8–64.5 | 0.8 (0.5–1.2) | 0.38 | – | – |
| Age (years) | |||||||
| 40 | 111 (46) | 110.5 | 25.3–195.6 | 0.6 (0.4–0.9) | 0.01 | – | – |
| 40 | 151 (87) | 27.5 | 19.2–35.7 | 1.6 (1.1–2.2) | 0.01 | 1.5 (0.9–2.2) | 0.05 |
| Sex | |||||||
| Male | 77 (38) | 67.6 | 40.4–94.8 | 0.9 (0.6–1.2) | 0.48 | – | – |
| Female | 185 (95) | 34.8 | 17.9–51.7 | 1.1 (0.8–1.7) | 0.48 | 1.1 (0.7–1.7) | 0.61 |
| Tumor site | |||||||
| Intra-abdominal | 59 (22) | 146.7 | Not reached | 0.6 (0.4–1.0) | 0.06 | 0.6 (0.3–1.2) | 0.16 |
| Abdominal Wall | 50 (18) | 170.1 | Not reached | 0.6 (0.4–1.0) | 0.05 | 0.6 (0.3–1.1) | 0.10 |
| Extremities | 85 (62) | 19.6 | 10.4–28.8 | 2.1 (1.5–2.9) | <0.001 | 1.6 (0.9–2.6) | 0.05 |
| Other b | 68 (31) | 46.1 | 11.7–80.5 | 0.8 (0.6–1.2) | 0.38 | – | – |
| Tumor size | |||||||
| 60 mm | 139 (79) | 32.7 | 17.7–47.8 | 1.4 (0.9–1.9) | 0.06 | 1.1 (0.7–1.5) | 0.74 |
| 60 mm | 123 (54) | 69.1 | 0.0–163.8 | 0.7 (0.5–1.0) | 0.06 | – | – |
| Mutation | |||||||
| CTNNB1 p.T41A | 20 (11) | 17.4 | 4.0–30.8 | 1.6 (0.9–3.0) | 0.12 | 1.6 (0.8–3.2) | 0.14 |
| CTNNB1 p.S45F | 8 (6) | 11.8 | 0.0–23.8 | 2.5 (1.1–5.8) | 0.02 | 2.1 (0.9–5.0) | 0.09 |
| APC | 14 (9) | 35.8 | 15.3–56.3 | 1.2 (0.6–2.4) | 0.55 | 1.6 (0.8–3.5) | 0.20 |
| Other c | 3 (2) | 24.6 | 21.7–27.5 | 1.2 (0.3–5.0) | 0.75 | 0.5 (0.1–2.1) | 0.32 |
| Treatment Modality | Adverse Effect and Complications (n, %) | n Grade 1 Toxicities | n Grade 2 Toxicities | n Grade 3 Toxicities |
|---|---|---|---|---|
| Imatinib (n = 5) | ||||
| Diarrhea (2, 40%) | 1 | 1 | 0 | |
| fatigue (1, 20%) | 0 | 1 | 0 | |
| Lower extremity edema (1, 20%) | 1 | 0 | 0 | |
| Imatinib + XRT (n = 9) | ||||
| Diarrhea (2, 22%) | 1 | 1 | 0 | |
| Nausea (2, 22%) | 1 | 1 | 0 | |
| Lower extremity edema (1, 11%) | 1 | 0 | 0 | |
| Dermatitis (1, 11%) | 0 | 1 | 0 | |
| Sorafenib (n = 6) | ||||
| Dermatitis (1, 17%) | 0 | 1 | 0 | |
| DRESS (2, 33%) | ||||
| Pazopanib (n = 1) | ||||
| Hypertension (1, 100%) | 0 | 1 | 0 | |
| Hormonal Therapy | ||||
| Hot flashes (3, 30%) | 2 | 1 | 0 | |
| Methotrexate-Vinblastine (n = 6) | ||||
| Vomiting (3, 50%) | 0 | 2 | 0 | |
| Doxorubicin (n = 4) | ||||
| Hair loss (1, 25%) | 0 | 1 | 0 | |
| Doxorubicin-Dacarbazine (n = 1) | ||||
| Neutropenic fever (1, 100%) | 0 | 0 | 1 | |
| MR-HIFU (n = 10) | ||||
| Pain at the ablation site (4, 40%) | 3 | 1 | 0 | |
| Cryoablation (n = 10) | ||||
| Pain at the ablation site (2, 20%) | 2 | 0 | 0 | |
| Active Surveillance (n = 19) | ||||
| Tumor pain (6, 32%) | 0 | 3 | 0 | |
| Tumor growth (6, 32%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Testa, S.; Bui, N.Q.; Charville, G.W.; Avedian, R.S.; Steffner, R.; Ghanouni, P.; Mohler, D.G.; Ganjoo, K.N. Management of Patients with Newly Diagnosed Desmoid Tumors in a First-Line Setting. Cancers 2022, 14, 3907. https://doi.org/10.3390/cancers14163907
Testa S, Bui NQ, Charville GW, Avedian RS, Steffner R, Ghanouni P, Mohler DG, Ganjoo KN. Management of Patients with Newly Diagnosed Desmoid Tumors in a First-Line Setting. Cancers. 2022; 14(16):3907. https://doi.org/10.3390/cancers14163907
Chicago/Turabian StyleTesta, Stefano, Nam Q. Bui, Gregory W. Charville, Raffi S. Avedian, Robert Steffner, Pejman Ghanouni, David G. Mohler, and Kristen N. Ganjoo. 2022. "Management of Patients with Newly Diagnosed Desmoid Tumors in a First-Line Setting" Cancers 14, no. 16: 3907. https://doi.org/10.3390/cancers14163907