
Utilization of Engineering Advances for Detailed Biomechanical Characterization of the Mitral–Ventricular Relationship to Optimize Repair Strategies: A Comprehensive Review

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Biomechanical Foundations of Mitral-Ventricular Interaction
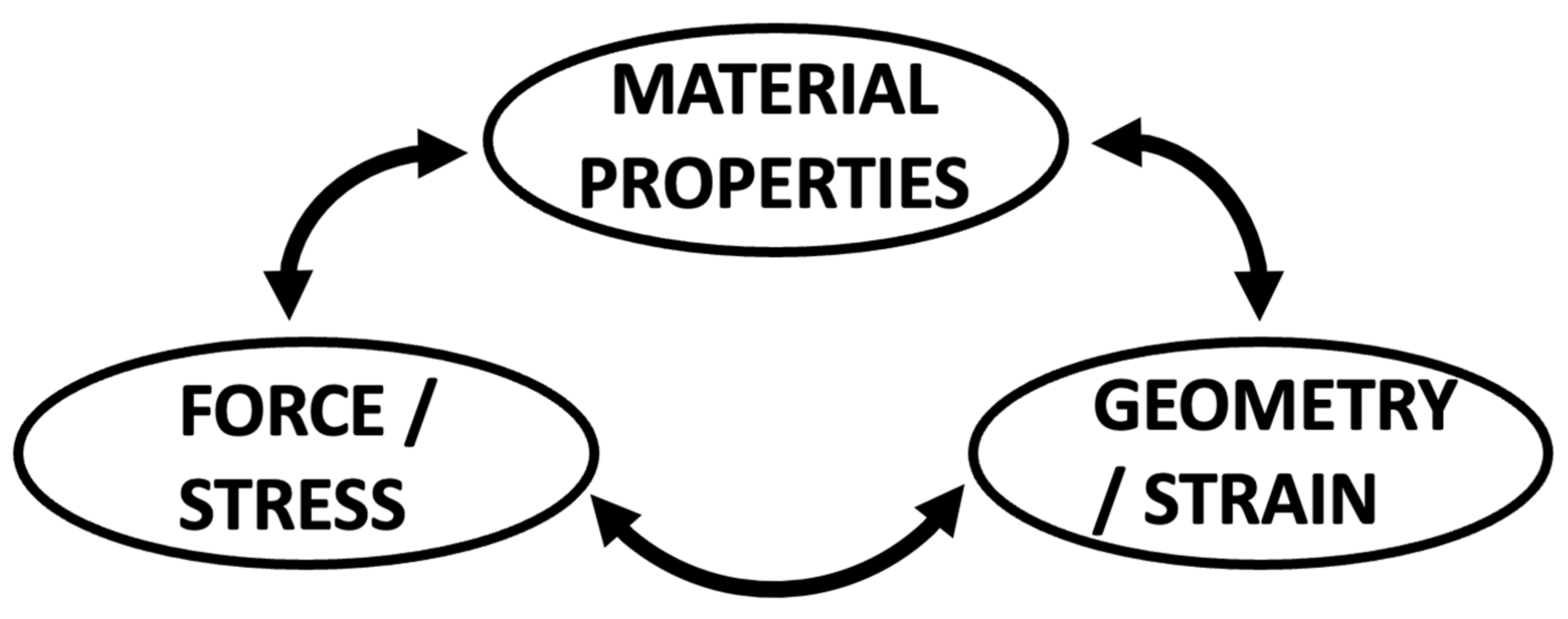
2.1. Mitral Valve Modelling
2.2. The Physiologic Mitral–Ventricular Relationship
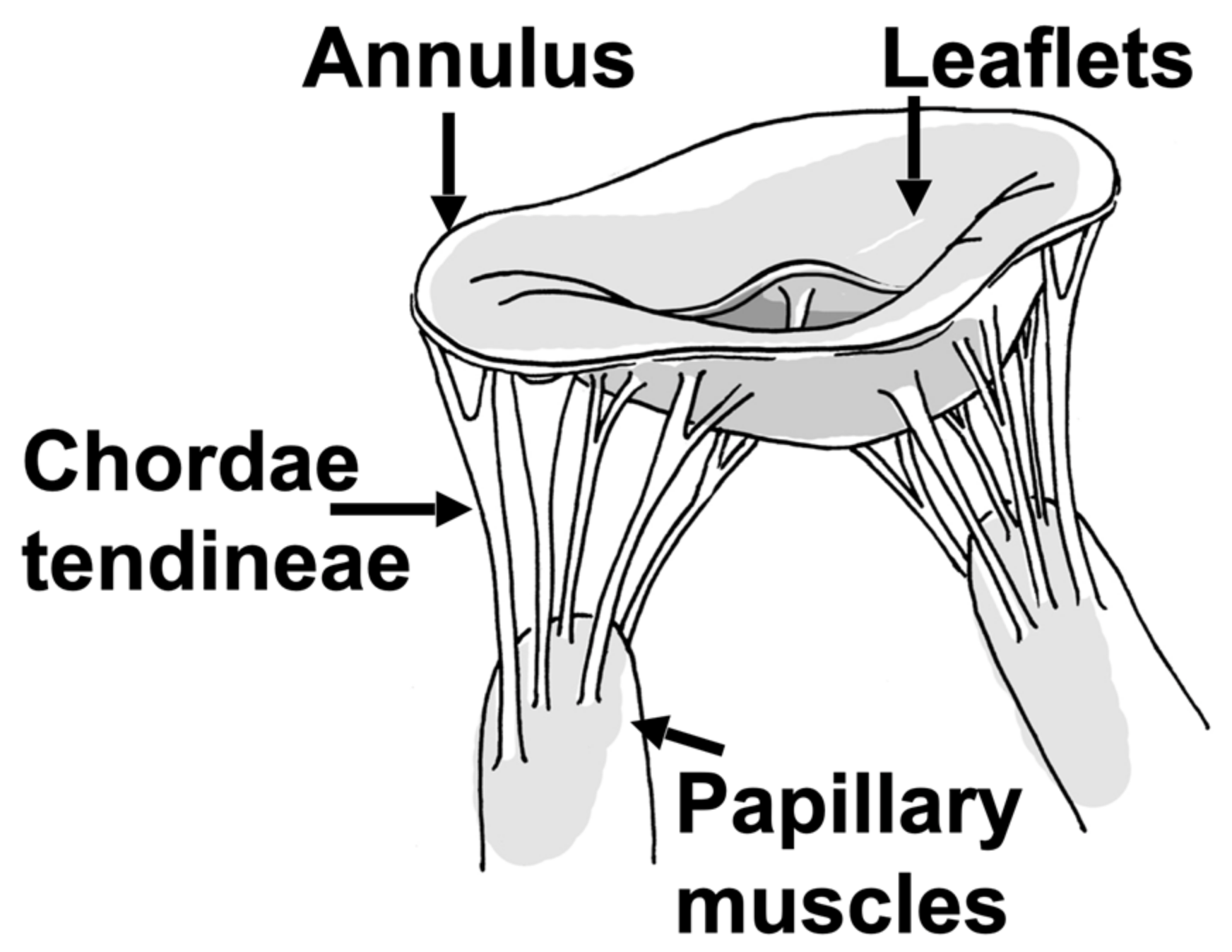
2.2.1. Mitral Valve Leaflets
2.2.2. Mitral Valve Annulus
2.2.3. Chordae Tendineae
2.2.4. Papillary Muscles and Adjacent Myocardium
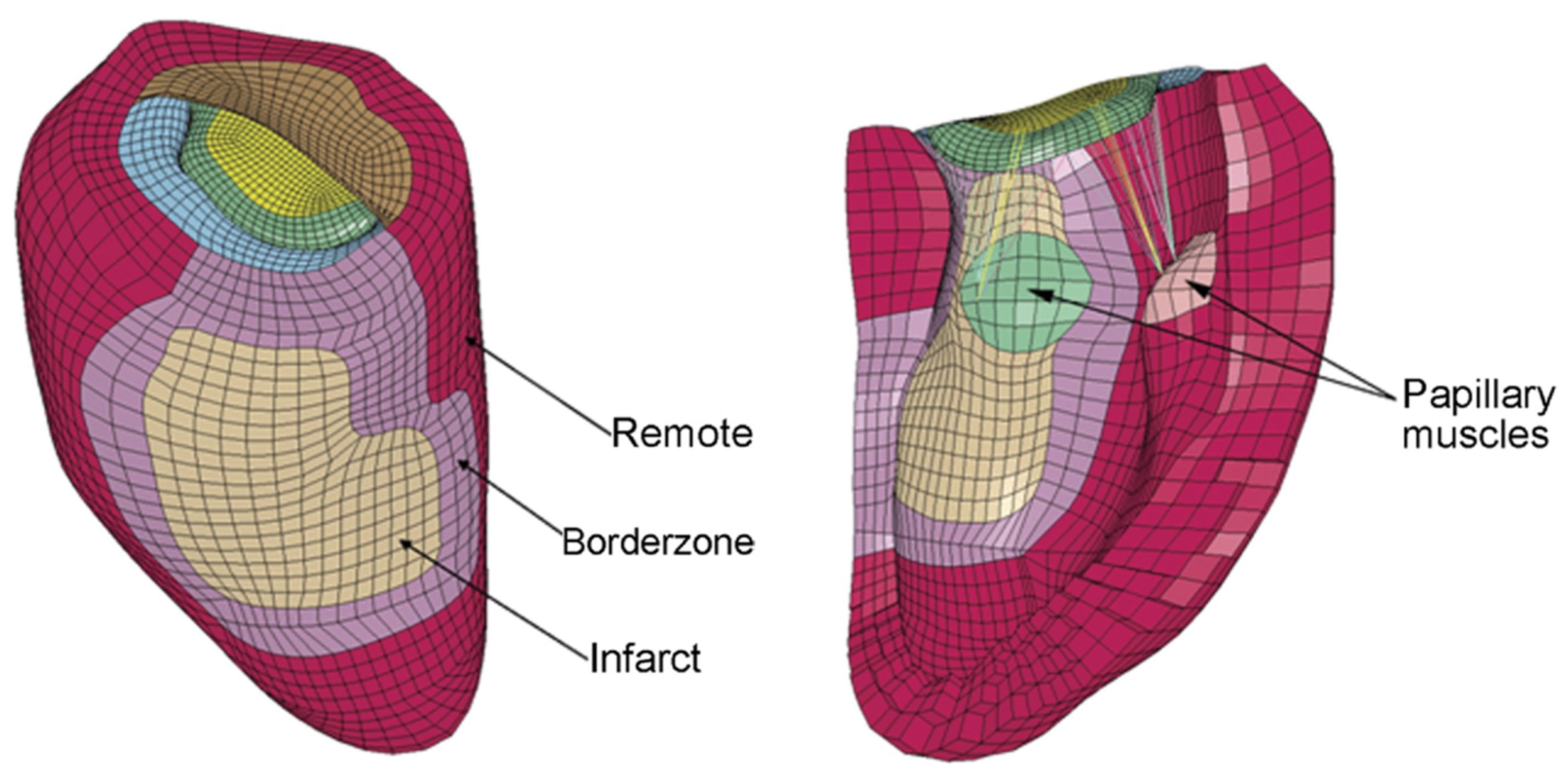
3. Chronic Ischemic Mitral Regurgitation
3.1. The Ventricle Tethers the Valve
3.2. Annular Mechanics and Remodeling
3.3. Implications for Existing and Future Surgical and Interventional Approaches
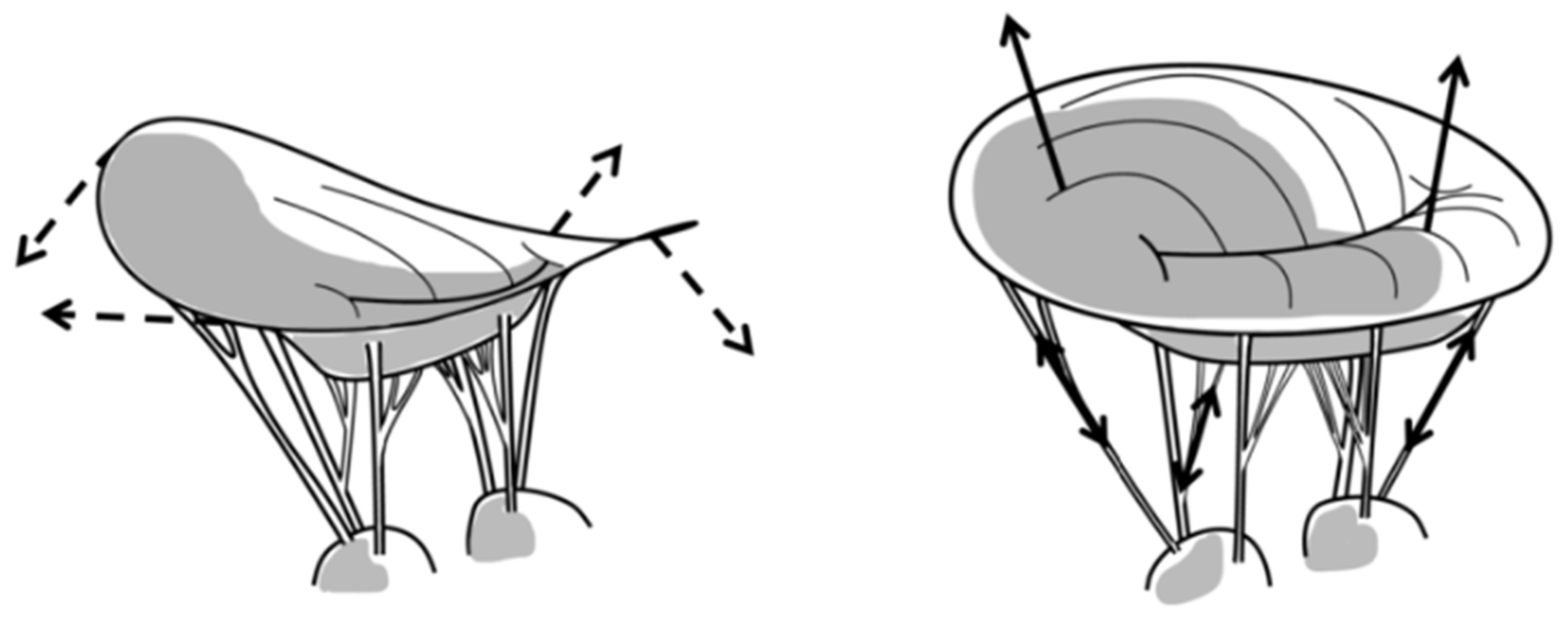
4. Mitral Valve Prolapse
4.1. The Valve Pulls on the Ventricle
4.2. Surgical Repair Techniques
5. Knowledge Gaps
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levine, R.A.; Hagége, A.A.; Judge, D.P.; Padala, M.; Dal-Bianco, J.P.; Aikawa, E.; Beaudoin, J.; Bischoff, J.; Bouatia-Naji, N.; Bruneval, P.; et al. Mitral valve disease--morphology and mechanisms. Nat. Rev. Cardiol. 2015, 12, 689–710. [Google Scholar] [CrossRef] [PubMed]
- Sarris, G.E.; Miller, D.C. Valvular-ventricular interaction: The importance of the mitral chordae tendineae in terms of global left ventricular systolic function. J. Card. Surg. 1988, 3, 215–234. [Google Scholar] [CrossRef] [PubMed]
- Lillehei, C.W.; Levy, M.J.; Bonnabeau, R.C., Jr. Mitral Valve Replacement with Preservation of Papillary Muscles and Chordae Tendineae. J. Thorac. Cardiovasc. Surg. 1964, 47, 532–543. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.O.; Hagege, A.A.; Otsuji, Y.; Levine, R.A.; Leducq Transatlantic, M.N. The unsaddled annulus: Biomechanical culprit in mitral valve prolapse? Circulation 2013, 127, 766–768. [Google Scholar] [CrossRef] [PubMed]
- Silverman, M.E.; Hurst, J.W. The mitral complex. Interaction of the anatomy, physiology, and pathology of the mitral annulus, mitral valve leaflets, chordae tendineae, and papillary muscles. Am. Heart J. 1968, 76, 399–418. [Google Scholar] [CrossRef]
- Park, M.H.; Zhu, Y.; Imbrie-Moore, A.M.; Wang, H.; Marin-Cuartas, M.; Paulsen, M.J.; Woo, Y.J. Heart Valve Biomechanics: The Frontiers of Modeling Modalities and the Expansive Capabilities of Ex Vivo Heart Simulation. Front. Cardiovasc. Med. 2021, 8, 673689. [Google Scholar] [CrossRef]
- Wang, H.; Paulsen, M.J.; Imbrie-Moore, A.M.; Tada, Y.; Bergamasco, H.; Baker, S.W.; Shudo, Y.; Ma, M.; Woo, Y.J. In Vivo Validation of Restored Chordal Biomechanics after Mitral Ring Annuloplasty in a Rare Ovine Case of Natural Chronic Functional Mitral Regurgitation. J. Cardiovasc. Dev. Dis. 2020, 7, 17. [Google Scholar] [CrossRef]
- Askov, J.B.; Honge, J.L.; Jensen, M.O.; Nygaard, H.; Hasenkam, J.M.; Nielsen, S.L. Significance of force transfer in mitral valve-left ventricular interaction: In vivo assessment. J. Thorac. Cardiovasc. Surg. 2013, 145, 1635–1641.e1. [Google Scholar] [CrossRef]
- Ostli, B.; Vester-Petersen, J.; Askov, J.B.; Honge, J.L.; Levine, R.A.; Hagege, A.; Nielsen, S.L.; Hasenkam, J.M.; Nygaard, H.; Jensen, M.O. In Vitro System for Measuring Chordal Force Changes Following Mitral Valve Patch Repair. Cardiovasc. Eng. Technol. 2012, 3, 263–268. [Google Scholar] [CrossRef]
- Nielsen, S.L.; Soerensen, D.D.; Libergren, P.; Yoganathan, A.P.; Nygaard, H. Miniature C-shaped transducers for chordae tendineae force measurements. Ann. Biomed. Eng. 2004, 32, 1050–1057. [Google Scholar] [CrossRef]
- Skov, S.N.; Ropcke, D.M.; Ilkjaer, C.; Rasmussen, J.; Tjornild, M.J.; Jimenez, J.H.; Yoganathan, A.P.; Nygaard, H.; Nielsen, S.L.; Jensen, M.O. New mitral annular force transducer optimized to distinguish annular segments and multi-plane forces. J. Biomech. 2016, 49, 742–748. [Google Scholar] [CrossRef]
- Pierce, E.L.; Siefert, A.W.; Paul, D.M.; Wells, S.K.; Bloodworth, C.H.t.; Takebayashi, S.; Aoki, C.; Jensen, M.O.; Gillespie, M.J.; Gorman, R.C.; et al. How Local Annular Force and Collagen Density Govern Mitral Annuloplasty Ring Dehiscence Risk. Ann. Thorac. Surg. 2016, 102, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Bloodworth, C.H.t.; Pierce, E.L.; Easley, T.F.; Drach, A.; Khalighi, A.H.; Toma, M.; Jensen, M.O.; Sacks, M.S.; Yoganathan, A.P. Ex Vivo Methods for Informing Computational Models of the Mitral Valve. Ann. Biomed. Eng. 2017, 45, 496–507. [Google Scholar] [CrossRef] [PubMed]
- Toma, M.; Jensen, M.O.; Einstein, D.R.; Yoganathan, A.P.; Cochran, R.P.; Kunzelman, K.S. Fluid-Structure Interaction Analysis of Papillary Muscle Forces Using a Comprehensive Mitral Valve Model with 3D Chordal Structure. Ann. Biomed. Eng. 2016, 44, 942–953. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.D.; Diaz-Zuccarini, V.; Scambler, P.; Burriesci, G. Fluid-structure interaction study of the edge-to-edge repair technique on the mitral valve. J. Biomech. 2011, 44, 2409–2417. [Google Scholar] [CrossRef]
- Wenk, J.F.; Zhang, Z.; Cheng, G.; Malhotra, D.; Acevedo-Bolton, G.; Burger, M.; Suzuki, T.; Saloner, D.A.; Wallace, A.W.; Guccione, J.M.; et al. First finite element model of the left ventricle with mitral valve: Insights into ischemic mitral regurgitation. Ann. Thorac. Surg. 2010, 89, 1546–1553. [Google Scholar] [CrossRef]
- Bouma, W.; Lai, E.K.; Levack, M.M.; Shang, E.K.; Pouch, A.M.; Eperjesi, T.J.; Plappert, T.J.; Yushkevich, P.A.; Mariani, M.A.; Khabbaz, K.R.; et al. Preoperative Three-Dimensional Valve Analysis Predicts Recurrent Ischemic Mitral Regurgitation after Mitral Annuloplasty. Ann. Thorac. Surg. 2016, 101, 567–575, discussion 575. [Google Scholar] [CrossRef]
- Levack, M.M.; Jassar, A.S.; Shang, E.K.; Vergnat, M.; Woo, Y.J.; Acker, M.A.; Jackson, B.M.; Gorman, J.H., 3rd; Gorman, R.C. Three-dimensional echocardiographic analysis of mitral annular dynamics: Implication for annuloplasty selection. Circulation 2012, 126, S183–S188. [Google Scholar] [CrossRef]
- Wijdh-den Hamer, I.J.; Bouma, W.; Lai, E.K.; Levack, M.M.; Shang, E.K.; Pouch, A.M.; Eperjesi, T.J.; Plappert, T.J.; Yushkevich, P.A.; Hung, J.; et al. The value of preoperative 3-dimensional over 2-dimensional valve analysis in predicting recurrent ischemic mitral regurgitation after mitral annuloplasty. J. Thorac. Cardiovasc. Surg. 2016, 152, 847–859. [Google Scholar] [CrossRef]
- Noack, T.; Janietz, M.; Lurz, P.; Kiefer, P.; Sieg, F.; Marin-Cuartas, M.; Spampinato, R.; Besler, C.; Rommel, K.P.; Holzhey, D.; et al. Dynamic mitral valve geometry in patients with primary and secondary mitral regurgitation: Implications for mitral valve repair. Eur. J. Cardiothorac. Surg. 2019, 56, 983–992. [Google Scholar] [CrossRef]
- Grbic, S.; Easley, T.F.; Mansi, T.; Bloodworth, C.H.; Pierce, E.L.; Voigt, I.; Neumann, D.; Krebs, J.; Yuh, D.D.; Jensen, M.O.; et al. Personalized mitral valve closure computation and uncertainty analysis from 3D echocardiography. Med. Image Anal. 2017, 35, 238–249. [Google Scholar] [CrossRef]
- Einstein, D.R.; Del Pin, F.; Jiao, X.; Kuprat, A.P.; Carson, J.P.; Kunzelman, K.S.; Cochran, R.P.; Guccione, J.M.; Ratcliffe, M.B. Fluid-Structure Interactions of the Mitral Valve and Left Heart: Comprehensive Strategies, Past, Present and Future. Int. J. Numer. Methods Eng. 2010, 26, 348–380. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Adams, J.; Wang, V.Y.; Horwitz, L.; Tartibi, M.; Morgan, A.E.; Kim, J.; Wallace, A.W.; Weinsaft, J.W.; Ge, L.; et al. A finite element model of the cardiac ventricles with coupled circulation: Biventricular mesh generation with hexahedral elements, airbags and a functional mockup interface to the circulation. Comput. Biol. Med. 2021, 137, 104840. [Google Scholar] [CrossRef] [PubMed]
- Gaidulis, G.; Suresh, K.S.; Xu, D.; Padala, M. Patient-Specific Three-Dimensional Ultrasound Derived Computational Modeling of the Mitral Valve. Ann. Biomed. Eng. 2022, 50, 847–859. [Google Scholar] [CrossRef] [PubMed]
- Yoganathan, A.P.; Lemmon, J.D., Jr.; Kim, Y.H.; Walker, P.G.; Levine, R.A.; Vesier, C.C. A computational study of a thin-walled three-dimensional left ventricle during early systole. J. Biomech. Eng. 1994, 116, 307–314. [Google Scholar] [CrossRef]
- Yoganathan, A.P.; Lemmon, J.D., Jr.; Kim, Y.H.; Levine, R.A.; Vesier, C.C. A three-dimensional computational investigation of intraventricular fluid dynamics: Examination into the initiation of systolic anterior motion of the mitral valve leaflets. J. Biomech. Eng. 1995, 117, 94–102. [Google Scholar] [CrossRef]
- Stephens, S.E.; Kammien, A.J.; Paris, J.C.; Applequist, A.P.; Ingels, N.B.; Jensen, H.K.; Rodgers, D.E.; Cole, C.R.; Wenk, J.F.; Jensen, M.O. In Vitro Mitral Valve Model with Unrestricted Ventricular Access: Using Vacuum to Close the Valve and Enable Static Trans-Mitral Pressure. J. Cardiovasc. Transl. Res. 2022, 15, 845–854. [Google Scholar] [CrossRef]
- Jimenez, J.H.; Soerensen, D.D.; He, Z.; Ritchie, J.; Yoganathan, A.P. Mitral valve function and chordal force distribution using a flexible annulus model: An in vitro study. Ann. Biomed. Eng. 2005, 33, 557–566. [Google Scholar] [CrossRef]
- Jensen, M.O.; Fontaine, A.A.; Yoganathan, A.P. Improved in vitro quantification of the force exerted by the papillary muscle on the left ventricular wall: Three-dimensional force vector measurement system. Ann. Biomed. Eng. 2001, 29, 406–413. [Google Scholar] [CrossRef]
- He, S.; Weston, M.W.; Lemmon, J.; Jensen, M.; Levine, R.A.; Yoganathan, A.P. Geometric distribution of chordae tendineae: An important anatomic feature in mitral valve function. J. Heart Valve Dis. 2000, 9, 495–501, discussion 502–493. [Google Scholar]
- Bajona, P.; Zehr, K.J.; Liao, J.; Speziali, G. Tension measurement of artificial chordae tendinae implanted between the anterior mitral valve leaflet and the left ventricular apex: An in vitro study. Innovations 2008, 3, 33–37. [Google Scholar] [CrossRef]
- Imbrie-Moore, A.M.; Park, M.H.; Paulsen, M.J.; Sellke, M.; Kulkami, R.; Wang, H.; Zhu, Y.; Farry, J.M.; Bourdillon, A.T.; Callinan, C.; et al. Biomimetic six-axis robots replicate human cardiac papillary muscle motion: Pioneering the next generation of biomechanical heart simulator technology. J. R. Soc. Interface 2020, 17, 20200614. [Google Scholar] [CrossRef]
- Rahmani, A.; Rasmussen, A.Q.; Honge, J.L.; Ostli, B.; Levine, R.A.; Hagege, A.A.; Nygaard, H.; Nielsen, S.L.; Jensen, M.O. Mitral Valve Mechanics Following Posterior Leaflet Patch Augmentation. J. Heart Valve Dis. 2013, 22, 28–35. [Google Scholar]
- He, S.; Fontaine, A.A.; Schwammenthal, E.; Yoganathan, A.P.; Levine, R.A. Integrated mechanism for functional mitral regurgitation: Leaflet restriction versus coapting force: In vitro studies. Circulation 1997, 96, 1826–1834. [Google Scholar] [CrossRef]
- He, S.; Lemmon, J.D., Jr.; Weston, M.W.; Jensen, M.O.; Levine, R.A.; Yoganathan, A.P. Mitral valve compensation for annular dilatation: In vitro study into the mechanisms of functional mitral regurgitation with an adjustable annulus model. J. Heart Valve Dis. 1999, 8, 294–302. [Google Scholar]
- Siefert, A.W.; Rabbah, J.P.; Saikrishnan, N.; Kunzelman, K.S.; Yoganathan, A.P. Isolated effect of geometry on mitral valve function for in silico model development. Comput. Methods Biomech. Biomed. Eng. 2015, 18, 618–627. [Google Scholar] [CrossRef]
- Pasrija, C.; Quinn, R.; Ghoreishi, M.; Eperjesi, T.; Lai, E.; Gorman, R.C.; Gorman, J.H.; Gorman, R.C.; Pouch, A.; Cortez, F.V.; et al. A Novel Quantitative Ex Vivo Model of Functional Mitral Regurgitation. Innovations 2020, 15, 329–337. [Google Scholar] [CrossRef]
- Paulsen, M.J.; Imbrie-Moore, A.M.; Wang, H.; Bae, J.H.; Hironaka, C.E.; Farry, J.M.; Lucian, H.J.; Thakore, A.D.; MacArthur, J.W.; Cutkosky, M.R.; et al. Mitral chordae tendineae force profile characterization using a posterior ventricular anchoring neochordal repair model for mitral regurgitation in a three-dimensional-printed ex vivo left heart simulator. Eur. J. Cardiothorac. Surg. 2020, 57, 535–544. [Google Scholar] [CrossRef]
- Bozkurt, S.; Preston-Maher, G.L.; Torii, R.; Burriesci, G. Design, Analysis and Testing of a Novel Mitral Valve for Transcatheter Implantation. Ann. Biomed. Eng. 2017, 45, 1852–1864. [Google Scholar] [CrossRef]
- Jimenez, J.H.; Liou, S.W.; Padala, M.; He, Z.; Sacks, M.; Gorman, R.C.; Gorman, J.H., 3rd; Yoganathan, A.P. A saddle-shaped annulus reduces systolic strain on the central region of the mitral valve anterior leaflet. J. Thorac. Cardiovasc. Surg. 2007, 134, 1562–1568. [Google Scholar] [CrossRef]
- Padala, M.; Hutchison, R.A.; Croft, L.R.; Jimenez, J.H.; Gorman, R.C.; Gorman, J.H., 3rd; Sacks, M.S.; Yoganathan, A.P. Saddle shape of the mitral annulus reduces systolic strains on the P2 segment of the posterior mitral leaflet. Ann. Thorac. Surg. 2009, 88, 1499–1504. [Google Scholar] [CrossRef] [PubMed]
- Paulsen, M.J.; Bae, J.H.; Imbrie-Moore, A.M.; Wang, H.; Hironaka, C.E.; Farry, J.M.; Lucian, H.; Thakore, A.D.; Cutkosky, M.R.; Joseph Woo, Y. Development and Ex Vivo Validation of Novel Force-Sensing Neochordae for Measuring Chordae Tendineae Tension in the Mitral Valve Apparatus Using Optical Fibers With Embedded Bragg Gratings. J. Biomech. Eng. 2020, 142, 145011–145019. [Google Scholar] [CrossRef] [PubMed]
- Lomholt, M.; Nielsen, S.L.; Hansen, S.B.; Andersen, N.T.; Hasenkam, J.M. Differential tension between secondary and primary mitral chordae in an acute in-vivo porcine model. J. Heart Valve Dis. 2002, 11, 337–345. [Google Scholar] [PubMed]
- Park, M.H.; van Kampen, A.; Melnitchouk, S.; Wilkerson, R.J.; Nagata, Y.; Zhu, Y.; Wang, H.; Pandya, P.K.; Morningstar, J.E.; Borger, M.A.; et al. Native and Post-Repair Residual Mitral Valve Prolapse Increases Forces Exerted on the Papillary Muscles: A Possible Mechanism for Localized Fibrosis? Circ. Cardiovasc. Interv. 2022, 15, e011928. [Google Scholar] [CrossRef]
- Hatle, L.; Brubakk, A.; Tromsdal, A.; Angelsen, B. Noninvasive assessment of pressure drop in mitral stenosis by Doppler ultrasound. Br. Heart J. 1978, 40, 131–140. [Google Scholar] [CrossRef]
- Hatle, L.; Angelsen, B.A.; Tromsdal, A. Non-invasive assessment of aortic stenosis by Doppler ultrasound. Br. Heart J. 1980, 43, 284–292. [Google Scholar] [CrossRef]
- Hatle, L.; Angelsen, B.A.; Tromsdal, A. Non-invasive estimation of pulmonary artery systolic pressure with Doppler ultrasound. Br. Heart J. 1981, 45, 157–165. [Google Scholar] [CrossRef]
- Cape, E.G.; Skoufis, E.G.; Weyman, A.E.; Yoganathan, A.P.; Levine, R.A. A new method for noninvasive quantification of valvular regurgitation based on conservation of momentum. In vitro validation. Circulation 1989, 79, 1343–1353. [Google Scholar] [CrossRef]
- Cape, E.G.; Yoganathan, A.P.; Levine, R.A. A new theoretical model for noninvasive quantification of mitral regurgitation. J. Biomech. 1990, 23, 27–33. [Google Scholar] [CrossRef]
- Buck, T.; Mucci, R.A.; Guerrero, J.L.; Holmvang, G.; Handschumacher, M.D.; Levine, R.A. The power-velocity integral at the vena contracta: A new method for direct quantification of regurgitant volume flow. Circulation 2000, 102, 1053–1061. [Google Scholar] [CrossRef]
- Buck, T.; Plicht, B.; Hunold, P.; Mucci, R.A.; Erbel, R.; Levine, R.A. Broad-beam spectral Doppler sonification of the vena contracta using matrix-array technology: A new solution for semi-automated quantification of mitral regurgitant flow volume and orifice area. J. Am. Coll. Cardiol. 2005, 45, 770–779. [Google Scholar] [CrossRef]
- Blumlein, S.; Bouchard, A.; Schiller, N.B.; Dae, M.; Byrd, B.F., 3rd; Ports, T.; Botvinick, E.H. Quantitation of mitral regurgitation by Doppler echocardiography. Circulation 1986, 74, 306–314. [Google Scholar] [CrossRef]
- Pierce, E.L.; Rabbah, J.P.; Thiele, K.; Wei, Q.; Vidakovic, B.; Jensen, M.O.; Hung, J.; Yoganathan, A.P. Three-Dimensional Field Optimization Method: Gold-Standard Validation of a Novel Color Doppler Method for Quantifying Mitral Regurgitation. J. Am. Soc. Echocardiogr. 2016, 29, 917–925. [Google Scholar] [CrossRef]
- Cape, E.G.; Yoganathan, A.P.; Weyman, A.E.; Levine, R.A. Adjacent solid boundaries alter the size of regurgitant jets on Doppler color flow maps. J. Am. Coll. Cardiol. 1991, 17, 1094–1102. [Google Scholar] [CrossRef]
- Chen, C.G.; Thomas, J.D.; Anconina, J.; Harrigan, P.; Mueller, L.; Picard, M.H.; Levine, R.A.; Weyman, A.E. Impact of impinging wall jet on color Doppler quantification of mitral regurgitation. Circulation 1991, 84, 712–720. [Google Scholar] [CrossRef]
- Rabbah, J.P.; Saikrishnan, N.; Siefert, A.W.; Santhanakrishnan, A.; Yoganathan, A.P. Mechanics of healthy and functionally diseased mitral valves: A critical review. J. Biomech. Eng. 2013, 135, 021007. [Google Scholar] [CrossRef]
- Yoganathan, A.P.; He, Z.; Casey Jones, S. Fluid mechanics of heart valves. Annu. Rev. Biomed. Eng. 2004, 6, 331–362. [Google Scholar] [CrossRef]
- Krishnamurthy, G.; Ennis, D.B.; Itoh, A.; Bothe, W.; Swanson, J.C.; Karlsson, M.; Kuhl, E.; Miller, D.C.; Ingels, N.B., Jr. Material properties of the ovine mitral valve anterior leaflet in vivo from inverse finite element analysis. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H1141–H1149. [Google Scholar] [CrossRef]
- Cochran, R.P.; Kunzelman, K.S.; Chuong, C.J.; Sacks, M.S.; Eberhart, R.C. Nondestructive analysis of mitral valve collagen fiber orientation. ASAIO Trans. 1991, 37, M447–M448. [Google Scholar]
- Kunzelman, K.S.; Cochran, R.P. Stress/strain characteristics of porcine mitral valve tissue: Parallel versus perpendicular collagen orientation. J. Card. Surg. 1992, 7, 71–78. [Google Scholar] [CrossRef]
- Levine, R.A.; Triulzi, M.O.; Harrigan, P.; Weyman, A.E. The relationship of mitral annular shape to the diagnosis of mitral valve prolapse. Circulation 1987, 75, 756–767. [Google Scholar] [CrossRef] [PubMed]
- Flachskampf, F.A.; Chandra, S.; Gaddipatti, A.; Levine, R.A.; Weyman, A.E.; Ameling, W.; Hanrath, P.; Thomas, J.D. Analysis of shape and motion of the mitral annulus in subjects with and without cardiomyopathy by echocardiographic 3-dimensional reconstruction. J. Am. Soc. Echocardiogr. 2000, 13, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, J.H.; Soerensen, D.D.; He, Z.; He, S.; Yoganathan, A.P. Effects of a saddle shaped annulus on mitral valve function and chordal force distribution: An in vitro study. Ann. Biomed. Eng. 2003, 31, 1171–1181. [Google Scholar] [CrossRef] [PubMed]
- Salgo, I.S.; Gorman, J.H., 3rd; Gorman, R.C.; Jackson, B.M.; Bowen, F.W.; Plappert, T.; St John Sutton, M.G.; Edmunds, L.H., Jr. Effect of annular shape on leaflet curvature in reducing mitral leaflet stress. Circulation 2002, 106, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Skov, S.N.; Ropcke, D.M.; Tjornild, M.J.; Ilkjaer, C.; Rasmussen, J.; Nygaard, H.; Jensen, M.O.; Nielsen, S.L. The effect of different mitral annuloplasty rings on valve geometry and annular stress distributiondagger. Interact. Cardiovasc. Thorac. Surg. 2017, 24, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.O.; Jensen, H.; Smerup, M.; Levine, R.A.; Yoganathan, A.P.; Nygaard, H.; Hasenkam, J.M.; Nielsen, S.L. Saddle-shaped mitral valve annuloplasty rings experience lower forces compared with flat rings. Circulation 2008, 118, S250–S255. [Google Scholar] [CrossRef]
- Jensen, M.O.; Jensen, H.; Levine, R.A.; Yoganathan, A.P.; Andersen, N.T.; Nygaard, H.; Hasenkam, J.M.; Nielsen, S.L. Saddle-shaped mitral valve annuloplasty rings improve leaflet coaptation geometry. J. Thorac. Cardiovasc. Surg. 2011, 142, 697–703. [Google Scholar] [CrossRef]
- Ross, C.J.; Zheng, J.; Ma, L.; Wu, Y.; Lee, C.H. Mechanics and Microstructure of the Atrioventricular Heart Valve Chordae Tendineae: A Review. Bioengineering 2020, 7, 25. [Google Scholar] [CrossRef]
- Gunnal, S.A.; Wabale, R.N.; Farooqui, M.S. Morphological study of chordae tendinae in human cadaveric hearts. Heart Views 2015, 16, 209–220. [Google Scholar] [CrossRef]
- Prot, V.; Haaverstad, R.; Skallerud, B. Finite element analysis of the mitral apparatus: Annulus shape effect and chordal force distribution. Biomech. Model. Mechanobiol. 2009, 8, 43–55. [Google Scholar] [CrossRef]
- Sarris, G.E.; Cahill, P.D.; Hansen, D.E.; Derby, G.C.; Miller, D.C. Restoration of left ventricular systolic performance after reattachment of the mitral chordae tendineae. The importance of valvular-ventricular interaction. J. Thorac. Cardiovasc. Surg. 1988, 95, 969–979. [Google Scholar] [CrossRef]
- Lam, J.H.; Ranganathan, N.; Wigle, E.D.; Silver, M.D. Morphology of the human mitral valve. I. Chordae tendineae: A new classification. Circulation 1970, 41, 449–458. [Google Scholar] [CrossRef]
- Ranganathan, N.; Lam, J.H.; Wigle, E.D.; Silver, M.D. Morphology of the human mitral valve. II. The value leaflets. Circulation 1970, 41, 459–467. [Google Scholar] [CrossRef]
- Ingels, N.B.; Karlsson, M. Mitral Valve Mechanics; Linköping University Electronic Press: Linköping, Sweden, 2015. [Google Scholar] [CrossRef]
- Yacoub, M.H. Anatomy of the Mitral Valve. A Pluridisciplinary Approach; Edward Arnold: London, UK, 1977. [Google Scholar]
- Ritchie, J.; Jimenez, J.; He, Z.; Sacks, M.S.; Yoganathan, A.P. The material properties of the native porcine mitral valve chordae tendineae: An in vitro investigation. J. Biomech. 2006, 39, 1129–1135. [Google Scholar] [CrossRef]
- He, Z.; Jowers, C. A novel method to measure mitral valve chordal tension. J. Biomech. Eng. 2009, 131, 14501. [Google Scholar] [CrossRef]
- Sedransk, K.L.; Grande-Allen, K.J.; Vesely, I. Failure mechanics of mitral valve chordae tendineae. J. Heart Valve Dis. 2002, 11, 644–650. [Google Scholar]
- Dagum, P.; Timek, T.A.; Green, G.R.; Lai, D.; Daughters, G.T.; Liang, D.H.; Hayase, M.; Ingels, N.B., Jr.; Miller, D.C. Coordinate-free analysis of mitral valve dynamics in normal and ischemic hearts. Circulation 2000, 102, III62–III69. [Google Scholar] [CrossRef]
- Joudinaud, T.M.; Kegel, C.L.; Flecher, E.M.; Weber, P.A.; Lansac, E.; Hvass, U.; Duran, C.M. The papillary muscles as shock absorbers of the mitral valve complex. An experimental study. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2007, 32, 96–101. [Google Scholar] [CrossRef]
- Kalra, K.; Wang, Q.; McIver, B.V.; Shi, W.; Guyton, R.A.; Sun, W.; Sarin, E.L.; Thourani, V.H.; Padala, M. Temporal changes in interpapillary muscle dynamics as an active indicator of mitral valve and left ventricular interaction in ischemic mitral regurgitation. J. Am. Coll. Cardiol. 2014, 64, 1867–1879. [Google Scholar] [CrossRef]
- Askov, J.B.; Honge, J.L.; Nygaard, H.; Hasenkam, J.M.; Nielsen, S.L.; Jensen, M.O. Papillary Muscle Force Transducer for Measurement In Vivo. Cardiovasc. Eng. Technol. 2011, 2, 196–202. [Google Scholar] [CrossRef]
- Liel-cohen, N.; Guerrero, J.L.; Otsuji, Y.; Handschumacher, M.D.; Rudski, L.G.; Hunziker, P.; Tanabe, H.; Scherrer-Crosbie, M.; Sullivan, S.; Levine, R.A. Design of a new surgical approach for ventricular remodeling to relieve ischemic mitral regurgitation: Insights from 3-dimensional echocardiography. Circulation 2000, 101, 2756–2763. [Google Scholar] [CrossRef]
- Levine, R.A.; Schwammenthal, E. Ischemic mitral regurgitation on the threshold of a solution: From paradoxes to unifying concepts. Circulation 2005, 112, 745–758. [Google Scholar] [CrossRef] [PubMed]
- Bothe, W.; Timek, T.A.; Tibayan, F.A.; Walther, M.; Daughters, G.T.; Ingels, N.B.; Miller, D.C. Characterization of 3-dimensional papillary muscle displacement in in vivo ovine models of ischemic/functional mitral regurgitation. J. Thorac. Cardiovasc. Surg. 2019, 157, 1444–1449. [Google Scholar] [CrossRef] [PubMed]
- Tibayan, F.A.; Rodriguez, F.; Zasio, M.K.; Bailey, L.; Liang, D.; Daughters, G.T.; Langer, F.; Ingels, N.B., Jr.; Miller, D.C. Geometric distortions of the mitral valvular-ventricular complex in chronic ischemic mitral regurgitation. Circulation 2003, 108 (Suppl. S1), II116–II121. [Google Scholar] [CrossRef] [PubMed]
- Kunzelman, K.S.; Reimink, M.S.; Cochran, R.P. Annular dilatation increases stress in the mitral valve and delays coaptation: A finite element computer model. Cardiovasc. Surg. 1997, 5, 427–434. [Google Scholar] [CrossRef]
- Dal-Bianco, J.P.; Aikawa, E.; Bischoff, J.; Guerrero, J.L.; Handschumacher, M.D.; Sullivan, S.; Johnson, B.; Titus, J.S.; Iwamoto, Y.; Wylie-Sears, J.; et al. Active adaptation of the tethered mitral valve: Insights into a compensatory mechanism for functional mitral regurgitation. Circulation 2009, 120, 334–342. [Google Scholar] [CrossRef]
- Beaudoin, J.; Dal-Bianco, J.P.; Aikawa, E.; Bischoff, J.; Guerrero, J.L.; Sullivan, S.; Bartko, P.E.; Handschumacher, M.D.; Kim, D.H.; Wylie-Sears, J.; et al. Mitral Leaflet Changes Following Myocardial Infarction: Clinical Evidence for Maladaptive Valvular Remodeling. Circ. Cardiovasc. Imaging 2017, 10, e006512. [Google Scholar] [CrossRef]
- Marsit, O.; Clavel, M.A.; Cote-Laroche, C.; Hadjadj, S.; Bouchard, M.A.; Handschumacher, M.D.; Clisson, M.; Drolet, M.C.; Boulanger, M.C.; Kim, D.H.; et al. Attenuated Mitral Leaflet Enlargement Contributes to Functional Mitral Regurgitation after Myocardial Infarction. J. Am. Coll. Cardiol. 2020, 75, 395–405. [Google Scholar] [CrossRef]
- Balachandran, K.; Alford, P.W.; Wylie-Sears, J.; Goss, J.A.; Grosberg, A.; Bischoff, J.; Aikawa, E.; Levine, R.A.; Parker, K.K. Cyclic strain induces dual-mode endothelial-mesenchymal transformation of the cardiac valve. Proc. Natl. Acad. Sci. USA 2011, 108, 19943–19948. [Google Scholar] [CrossRef]
- Kunzelman, K.S.; Quick, D.W.; Cochran, R.P. Altered collagen concentration in mitral valve leaflets: Biochemical and finite element analysis. Ann. Thorac. Surg. 1998, 66, S198–S205. [Google Scholar] [CrossRef]
- Kunzelman, K.S.; Einstein, D.R.; Cochran, R.P. Fluid-structure interaction models of the mitral valve: Function in normal and pathological states. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2007, 362, 1393–1406. [Google Scholar] [CrossRef]
- Ben Zekry, S.; Freeman, J.; Jajoo, A.; He, J.; Little, S.H.; Lawrie, G.M.; Azencott, R.; Zoghbi, W.A. Patient-Specific Quantitation of Mitral Valve Strain by Computer Analysis of Three-Dimensional Echocardiography: A Pilot Study. Circ. Cardiovasc. Imaging 2016, 9, e003254. [Google Scholar] [CrossRef]
- El-Tallawi, K.C.; Zhang, P.; Azencott, R.; He, J.; Xu, J.; Herrera, E.L.; Jacob, J.; Chamsi-Pasha, M.; Lawrie, G.M.; Zoghbi, W.A. Mitral Valve Remodeling and Strain in Secondary Mitral Regurgitation: Comparison With Primary Regurgitation and Normal Valves. JACC Cardiovasc. Imaging 2021, 14, 782–793. [Google Scholar] [CrossRef]
- Bischoff, J.; Casanovas, G.; Wylie-Sears, J.; Kim, D.H.; Bartko, P.E.; Guerrero, J.L.; Dal-Bianco, J.P.; Beaudoin, J.; Garcia, M.L.; Sullivan, S.M.; et al. CD45 Expression in Mitral Valve Endothelial Cells after Myocardial Infarction. Circ. Res. 2016, 119, 1215–1225. [Google Scholar] [CrossRef]
- Ayoub, S.; Tsai, K.C.; Khalighi, A.H.; Sacks, M.S. The Three-Dimensional Microenvironment of the Mitral Valve: Insights into the Effects of Physiological Loads. Cell. Mol. Bioeng. 2018, 11, 291–306. [Google Scholar] [CrossRef]
- Rego, B.V.; Khalighi, A.H.; Gorman, J.H., 3rd; Gorman, R.C.; Sacks, M.S. Simulation of Mitral Valve Plasticity in Response to Myocardial Infarction. Ann. Biomed. Eng. 2023, 51, 71–87. [Google Scholar] [CrossRef]
- Sacks, M.; Drach, A.; Lee, C.H.; Khalighi, A.; Rego, B.; Zhang, W.; Ayoub, S.; Yoganathan, A.; Gorman, R.C.; Gorman Iii, J.H. On the simulation of mitral valve function in health, disease, and treatment. J. Biomech. Eng. 2019, 141, 708041–7080422. [Google Scholar] [CrossRef]
- Simonian, N.T.; Liu, H.; Pouch, A.M.; Gorman, J.H., 3rd; Gorman, R.C.; Sacks, M.S. Quantitative in vivo assessment of human mitral valve coaptation area after undersized ring annuloplasty repair for ischemic mitral regurgitation. JTCVS Tech. 2022, 16, 49–59. [Google Scholar] [CrossRef]
- Rausch, M.K.; Tibayan, F.A.; Ingels, N.B., Jr.; Miller, D.C.; Kuhl, E. Mechanics of the mitral annulus in chronic ischemic cardiomyopathy. Ann. Biomed. Eng. 2013, 41, 2171–2180. [Google Scholar] [CrossRef]
- Timek, T.A.; Lai, D.T.; Tibayan, F.; Liang, D.; Daughters, G.T.; Dagum, P.; Ingels, N.B., Jr.; Miller, D.C. Septal-lateral annular cinching abolishes acute ischemic mitral regurgitation. J. Thorac. Cardiovasc. Surg. 2002, 123, 881–888. [Google Scholar] [CrossRef]
- Pedersen, W.R.; Block, P.; Leon, M.; Kramer, P.; Kapadia, S.; Babaliaros, V.; Kodali, S.; Tuzcu, E.M.; Feldman, T. iCoapsys mitral valve repair system: Percutaneous implantation in an animal model. Catheter. Cardiovasc. Interv. 2008, 72, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Bouma, W.; van der Horst, I.C.; Wijdh-den Hamer, I.J.; Erasmus, M.E.; Zijlstra, F.; Mariani, M.A.; Ebels, T. Chronic ischaemic mitral regurgitation. Current treatment results and new mechanism-based surgical approaches. Eur. J. Cardiothorac. Surg. 2010, 37, 170–185. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.O.; Honge, J.L.; Benediktsson, J.A.; Siefert, A.W.; Jensen, H.; Yoganathan, A.P.; Snow, T.K.; Hasenkam, J.M.; Nygaard, H.; Nielsen, S.L. Mitral valve annular downsizing forces: Implications for annuloplasty device development. J. Thorac. Cardiovasc. Surg. 2014, 148, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Imbrie-Moore, A.M.; Zhu, Y.; Bandy-Vizcaino, T.; Park, M.H.; Wilkerson, R.J.; Woo, Y.J. Ex Vivo Model of Ischemic Mitral Regurgitation and Analysis of Adjunctive Papillary Muscle Repair. Ann. Biomed. Eng. 2021, 49, 3412–3424. [Google Scholar] [CrossRef] [PubMed]
- Acker, M.A.; Parides, M.K.; Perrault, L.P.; Moskowitz, A.J.; Gelijns, A.C.; Voisine, P.; Smith, P.K.; Hung, J.W.; Blackstone, E.H.; Puskas, J.D.; et al. Mitral-valve repair versus replacement for severe ischemic mitral regurgitation. N. Engl. J. Med. 2014, 370, 23–32. [Google Scholar] [CrossRef]
- Wong, V.M.; Wenk, J.F.; Zhang, Z.; Cheng, G.; Acevedo-Bolton, G.; Burger, M.; Saloner, D.A.; Wallace, A.W.; Guccione, J.M.; Ratcliffe, M.B.; et al. The effect of mitral annuloplasty shape in ischemic mitral regurgitation: A finite element simulation. Ann. Thorac. Surg. 2012, 93, 776–782. [Google Scholar] [CrossRef]
- Siefert, A.W.; Rabbah, J.P.; Pierce, E.L.; Kunzelman, K.S.; Yoganathan, A.P. Quantitative Evaluation of Annuloplasty on Mitral Valve Chordae Tendineae Forces to Supplement Surgical Planning Model Development. Cardiovasc. Eng. Technol. 2014, 5, 35–43. [Google Scholar] [CrossRef]
- Green, G.R.; Dagum, P.; Glasson, J.R.; Nistal, J.F.; Daughters, G.T., 2nd; Ingels, N.B., Jr.; Miller, D.C. Restricted posterior leaflet motion after mitral ring annuloplasty. Ann Thorac. Surg. 1999, 68, 2100–2106. [Google Scholar] [CrossRef]
- Hung, J.; Chaput, M.; Guerrero, J.L.; Handschumacher, M.D.; Papakostas, L.; Sullivan, S.; Solis, J.; Levine, R.A. Persistent reduction of ischemic mitral regurgitation by papillary muscle repositioning: Structural stabilization of the papillary muscle-ventricular wall complex. Circulation 2007, 116, I259–I263. [Google Scholar] [CrossRef]
- Hung, J.; Guerrero, J.L.; Handschumacher, M.D.; Supple, G.; Sullivan, S.; Levine, R.A. Reverse ventricular remodeling reduces ischemic mitral regurgitation: Echo-guided device application in the beating heart. Circulation 2002, 106, 2594–2600. [Google Scholar] [CrossRef]
- Hung, J.; Solis, J.; Handschumacher, M.D.; Guerrero, J.L.; Levine, R.A. Persistence of mitral regurgitation following ring annuloplasty: Is the papillary muscle outside or inside the ring? J. Heart Valve Dis. 2012, 21, 218–224. [Google Scholar]
- Levine, R.A.; Hung, J.; Otsuji, Y.; Messas, E.; Liel-Cohen, N.; Nathan, N.; Handschumacher, M.D.; Guerrero, J.L.; He, S.; Yoganathan, A.P.; et al. Mechanistic insights into functional mitral regurgitation. Curr. Cardiol. Rep. 2002, 4, 125–129. [Google Scholar] [CrossRef]
- Hung, J.; Papakostas, L.; Tahta, S.A.; Hardy, B.G.; Bollen, B.A.; Duran, C.M.; Levine, R.A. Mechanism of recurrent ischemic mitral regurgitation after annuloplasty: Continued LV remodeling as a moving target. Circulation 2004, 110, II85–II90. [Google Scholar] [CrossRef]
- Zhan-Moodie, S.; Xu, D.; Suresh, K.S.; He, Q.; Onohara, D.; Kalra, K.; Guyton, R.A.; Sarin, E.L.; Padala, M. Papillary Muscle Approximation Reduces Systolic Tethering Forces and Improves Mitral Valve Closure in the Repair of Functional Mitral Regurgitation. JTCVS Open 2021, 7, 91–104. [Google Scholar] [CrossRef]
- Rabbah, J.P.; Chism, B.; Siefert, A.; Saikrishnan, N.; Veledar, E.; Thourani, V.H.; Yoganathan, A.P. Effects of targeted papillary muscle relocation on mitral leaflet tenting and coaptation. Ann. Thorac. Surg. 2013, 95, 621–628. [Google Scholar] [CrossRef]
- Pausch, J.; Girdauskas, E.; Conradi, L.; Reichenspurner, H. Secondary mitral regurgitation repair techniques and outcomes: Subannular repair techniques in secondary mitral regurgitation type IIIb. JTCVS Tech. 2021, 10, 92–97. [Google Scholar] [CrossRef]
- Enomoto, Y.; Gorman, J.H., 3rd; Moainie, S.L.; Jackson, B.M.; Parish, L.M.; Plappert, T.; Zeeshan, A.; St John-Sutton, M.G.; Gorman, R.C. Early ventricular restraint after myocardial infarction: Extent of the wrap determines the outcome of remodeling. Ann. Thorac. Surg. 2005, 79, 881–887. [Google Scholar] [CrossRef]
- Kataoka, A.; Zeng, X.; Guerrero, J.L.; Kozak, A.; Braithwaite, G.; Levine, R.A.; Vlahakes, G.J.; Hung, J. Application of polymer-mesh device to remodel left ventricular-mitral valve apparatus in ischemic mitral regurgitation. J. Thorac. Cardiovasc. Surg. 2018, 155, 1485–1493. [Google Scholar] [CrossRef]
- Blom, A.S.; Mukherjee, R.; Pilla, J.J.; Lowry, A.S.; Yarbrough, W.M.; Mingoia, J.T.; Hendrick, J.W.; Stroud, R.E.; McLean, J.E.; Affuso, J.; et al. Cardiac support device modifies left ventricular geometry and myocardial structure after myocardial infarction. Circulation 2005, 112, 1274–1283. [Google Scholar] [CrossRef]
- Blom, A.S.; Pilla, J.J.; Gorman, R.C., 3rd; Gorman, J.H.; Mukherjee, R.; Spinale, F.G.; Acker, M.A. Infarct size reduction and attenuation of global left ventricular remodeling with the CorCap cardiac support device following acute myocardial infarction in sheep. Heart Fail. Rev. 2005, 10, 125–139. [Google Scholar] [CrossRef]
- Varela, C.E.; Fan, Y.; Roche, E.T. Optimizing Epicardial Restraint and Reinforcement Following Myocardial Infarction: Moving Towards Localized, Biomimetic, and Multitherapeutic Options. Biomimetics 2019, 4, 7. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Akita, T.; Mizuno, F.; Nakayama, A.; Morioka, K. Beneficial effects of a cardiac support device on left ventricular remodeling after posterior myocardial infarction: An evaluation by echocardiography, pressure-volume curves and ventricular histology. Surg. Today 2016, 46, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef] [PubMed]
- Szymanski, C.; Bel, A.; Cohen, I.; Touchot, B.; Handschumacher, M.D.; Desnos, M.; Carpentier, A.; Menasche, P.; Hagege, A.A.; Levine, R.A.; et al. Comprehensive annular and subvalvular repair of chronic ischemic mitral regurgitation improves long-term results with the least ventricular remodeling. Circulation 2012, 126, 2720–2727. [Google Scholar] [CrossRef]
- Messas, E.; Pouzet, B.; Touchot, B.; Guerrero, J.L.; Vlahakes, G.J.; Desnos, M.; Menasche, P.; Hagege, A.; Levine, R.A. Efficacy of chordal cutting to relieve chronic persistent ischemic mitral regurgitation. Circulation 2003, 108 (Suppl. S1), II111–II115. [Google Scholar] [CrossRef]
- Messas, E.; Bel, A.; Szymanski, C.; Cohen, I.; Touchot, B.; Handschumacher, M.D.; Desnos, M.; Carpentier, A.; Menasche, P.; Hagege, A.A.; et al. Relief of mitral leaflet tethering following chronic myocardial infarction by chordal cutting diminishes left ventricular remodeling. Circ. Cardiovasc. Imaging 2010, 3, 679–686. [Google Scholar] [CrossRef]
- Hata, M.; Fujita, B.; Hakim-Meibodi, K.; Gummert, J.F. Papillary Muscle Heads Focalization for Functional Mitral Valve Regurgitation. Ann. Thorac. Surg. 2020, 110, e59–e61. [Google Scholar] [CrossRef]
- Namazi, F.; Delgado, V.; Pio, S.M.; Ajmone Marsan, N.; Asch, F.M.; Medvedofsky, D.; Weissman, N.J.; Zhou, Z.; Redfors, B.; Lindenfeld, J.; et al. Prognostic implications of mitral valve geometry in patients with secondary mitral regurgitation: The COAPT trial. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 1540–1551. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, V.Y.; Morgan, A.E.; Kim, J.; Handschumacher, M.D.; Moskowitz, C.S.; Levine, R.A.; Ge, L.; Guccione, J.M.; Weinsaft, J.W.; et al. Mechanical effects of MitraClip on leaflet stress and myocardial strain in functional mitral regurgitation—A finite element modeling study. PLoS ONE 2019, 14, e0223472. [Google Scholar] [CrossRef]
- Kong, F.; Caballero, A.; McKay, R.; Sun, W. Finite element analysis of MitraClip procedure on a patient-specific model with functional mitral regurgitation. J. Biomech. 2020, 104, 109730. [Google Scholar] [CrossRef]
- Caballero, A.; Mao, W.; McKay, R.; Hahn, R.T.; Sun, W. A Comprehensive Engineering Analysis of Left Heart Dynamics after MitraClip in a Functional Mitral Regurgitation Patient. Front. Physiol. 2020, 11, 432. [Google Scholar] [CrossRef]
- Errthum, R.; Caballero, A.; McKay, R.; Sun, W. Comparative computational analysis of PASCAL and MitraClip implantation in a patient-specific functional mitral regurgitation model. Comput. Biol. Med. 2021, 136, 104767. [Google Scholar] [CrossRef]
- Pantoja, J.L.; Morgan, A.E.; Grossi, E.A.; Jensen, M.O.; Weinsaft, J.W.; Levine, R.A.; Ge, L.; Ratcliffe, M.B. Undersized Mitral Annuloplasty Increases Strain in the Proximal Lateral Left Ventricular Wall. Ann. Thorac. Surg. 2017, 103, 820–827. [Google Scholar] [CrossRef]
- Freed, L.A.; Levy, D.; Levine, R.A.; Larson, M.G.; Evans, J.C.; Fuller, D.L.; Lehman, B.; Benjamin, E.J. Prevalence and clinical outcome of mitral-valve prolapse. N. Engl. J. Med. 1999, 341, 1–7. [Google Scholar] [CrossRef]
- Morningstar, J.E.; Nieman, A.; Wang, C.; Beck, T.; Harvey, A.; Norris, R.A. Mitral Valve Prolapse and Its Motley Crew-Syndromic Prevalence, Pathophysiology, and Progression of a Common Heart Condition. J. Am. Heart Assoc. 2021, 10, e020919. [Google Scholar] [CrossRef]
- Toomer, K.A.; Yu, M.; Fulmer, D.; Guo, L.; Moore, K.S.; Moore, R.; Drayton, K.D.; Glover, J.; Peterson, N.; Ramos-Ortiz, S.; et al. Primary cilia defects causing mitral valve prolapse. Sci. Transl. Med. 2019, 11, eaax0290. [Google Scholar] [CrossRef]
- Connell, P.S.; Azimuddin, A.F.; Kim, S.E.; Ramirez, F.; Jackson, M.S.; Little, S.H.; Grande-Allen, K.J. Regurgitation Hemodynamics Alone Cause Mitral Valve Remodeling Characteristic of Clinical Disease States In Vitro. Ann. Biomed. Eng. 2016, 44, 954–967. [Google Scholar] [CrossRef]
- Roselli, C.; Yu, M.; Nauffal, V.; Georges, A.; Yang, Q.; Love, K.; Weng, L.C.; Delling, F.N.; Maurya, S.R.; Schrolkamp, M.; et al. Genome-wide association study reveals novel genetic loci: A new polygenic risk score for mitral valve prolapse. Eur. Heart J. 2022, 43, 1668–1680. [Google Scholar] [CrossRef]
- Juang, J.J.; Ke, S.R.; Lin, J.L.; Hwang, J.J.; Hsu, K.L.; Chiang, F.T.; Tseng, C.D.; Tseng, Y.Z.; Chen, J.J.; Hu, F.C.; et al. Rupture of mitral chordae tendineae: Adding to the list of hypertension complications. Heart 2009, 95, 976–979. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.H.; Su, H.M.; Voon, W.C.; Lai, H.M.; Yen, H.W.; Lai, W.T.; Sheu, S.H. Association between hypertension and primary mitral chordae tendinae rupture. Am. J. Hypertens. 2006, 19, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Jassar, A.S.; Vergnat, M.; Jackson, B.M.; McGarvey, J.R.; Cheung, A.T.; Ferrari, G.; Woo, Y.J.; Acker, M.A.; Gorman, R.C.; Gorman, J.H., 3rd. Regional annular geometry in patients with mitral regurgitation: Implications for annuloplasty ring selection. Ann. Thorac. Surg. 2014, 97, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Caiani, E.G.; Fusini, L.; Veronesi, F.; Tamborini, G.; Maffessanti, F.; Gripari, P.; Corsi, C.; Naliato, M.; Zanobini, M.; Alamanni, F.; et al. Quantification of mitral annulus dynamic morphology in patients with mitral valve prolapse undergoing repair and annuloplasty during a 6-month follow-up. Eur. J. Echocardiogr. 2011, 12, 375–383. [Google Scholar] [CrossRef]
- Imbrie-Moore, A.M.; Paulsen, M.J.; Thakore, A.D.; Wang, H.; Hironaka, C.E.; Lucian, H.J.; Farry, J.M.; Edwards, B.B.; Bae, J.H.; Cutkosky, M.R.; et al. Ex Vivo Biomechanical Study of Apical Versus Papillary Neochord Anchoring for Mitral Regurgitation. Ann. Thorac. Surg. 2019, 108, 90–97. [Google Scholar] [CrossRef]
- Paulsen, M.J.; Cuartas, M.M.; Imbrie-Moore, A.; Wang, H.; Wilkerson, R.; Farry, J.; Zhu, Y.; Ma, M.; MacArthur, J.W.; Woo, Y.J. Biomechanical engineering comparison of four leaflet repair techniques for mitral regurgitation using a novel 3-dimensional-printed left heart simulator. JTCVS Tech. 2021, 10, 244–251. [Google Scholar] [CrossRef]
- Granier, M.; Jensen, M.O.; Honge, J.L.; Bel, A.; Menasche, P.; Nielsen, S.L.; Carpentier, A.; Levine, R.A.; Hagege, A.A. Consequences of mitral valve prolapse on chordal tension: Ex vivo and in vivo studies in large animal models. J. Thorac. Cardiovasc. Surg. 2011, 142, 1585–1587. [Google Scholar] [CrossRef]
- Imbrie-Moore, A.M.; Paulsen, M.J.; Zhu, Y.; Wang, H.; Lucian, H.J.; Farry, J.M.; MacArthur, J.W.; Ma, M.; Woo, Y.J. A novel cross-species model of Barlow’s disease to biomechanically analyze repair techniques in an ex vivo left heart simulator. J. Thorac. Cardiovasc. Surg. 2021, 161, 1776–1783. [Google Scholar] [CrossRef]
- Kitkungvan, D.; Nabi, F.; Kim, R.J.; Bonow, R.O.; Khan, M.A.; Xu, J.; Little, S.H.; Quinones, M.A.; Lawrie, G.M.; Zoghbi, W.A.; et al. Myocardial Fibrosis in Patients With Primary Mitral Regurgitation With and Without Prolapse. J. Am. Coll. Cardiol. 2018, 72, 823–834. [Google Scholar] [CrossRef]
- Constant Dit Beaufils, A.L.; Huttin, O.; Jobbe-Duval, A.; Senage, T.; Filippetti, L.; Piriou, N.; Cueff, C.; Venner, C.; Mandry, D.; Sellal, J.M.; et al. Replacement Myocardial Fibrosis in Patients With Mitral Valve Prolapse: Relation to Mitral Regurgitation, Ventricular Remodeling, and Arrhythmia. Circulation 2021, 143, 1763–1774. [Google Scholar] [CrossRef]
- Basso, C.; Perazzolo Marra, M.; Rizzo, S.; De Lazzari, M.; Giorgi, B.; Cipriani, A.; Frigo, A.C.; Rigato, I.; Migliore, F.; Pilichou, K.; et al. Arrhythmic Mitral Valve Prolapse and Sudden Cardiac Death. Circulation 2015, 132, 556–566. [Google Scholar] [CrossRef]
- Morningstar, J.E.; Gensemer, C.; Moore, R.; Fulmer, D.; Beck, T.C.; Wang, C.; Moore, K.; Guo, L.; Sieg, F.; Nagata, Y.; et al. Mitral Valve Prolapse Induces Regionalized Myocardial Fibrosis. J. Am. Heart Assoc. 2021. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, A.J.; Harrigan, P.; Popovic, A.D.; Weyman, A.E.; Levine, R.A. Papillary muscle traction in mitral valve prolapse: Quantitation by two-dimensional echocardiography. J. Am. Coll. Cardiol. 1992, 19, 564–571. [Google Scholar] [CrossRef]
- Nagata, Y.; Bertrand, P.B.; Melnitchouk, S.; Borger, M.A.; Delling, F.N.; Hung, J.; Norris, R.A.; Weinsaft, J.W.; Levine, R.A. Abnormal Mechanics Relate to Myocardial Fibrosis and Ventricular Arrhythmias in Patients with Mitral Valve Prolapse. Circ. Cardiovasc. Imaging 2023, 16, e014963. [Google Scholar] [CrossRef]
- Romero Daza, A.; Chokshi, A.; Pardo, P.; Maneiro, N.; Guijarro Contreras, A.; Larranaga-Moreira, J.M.; Ibanez, B.; Fuster, V.; Fernandez Friera, L.; Solis, J.; et al. Mitral valve prolapse morphofunctional features by cardiovascular magnetic resonance: More than just a valvular disease. J. Cardiovasc. Magn. Reson. 2021, 23, 107. [Google Scholar] [CrossRef]
- Padala, M.; Powell, S.N.; Croft, L.R.; Thourani, V.H.; Yoganathan, A.P.; Adams, D.H. Mitral valve hemodynamics after repair of acute posterior leaflet prolapse: Quadrangular resection versus triangular resection versus neochordoplasty. J. Thorac. Cardiovasc. Surg. 2009, 138, 309–315. [Google Scholar] [CrossRef]
- Park, M.H.; van Kampen, A.; Zhu, Y.; Melnitchouk, S.; Levine, R.A.; Borger, M.A.; Woo, Y.J. Neochordal Goldilocks: Analyzing the Biomechanics of Neochord Length on Papillary Muscle Forces Suggests Higher Tolerance to Shorter Neochordae. J. Thorac. Cardiovasc. Surg. 2023. [Google Scholar] [CrossRef]
- Pandya, P.K.; Wilkerson, R.J.; Imbrie-Moore, A.M.; Zhu, Y.; Marin-Cuartas, M.; Park, M.H.; Woo, Y.J. Quantitative biomechanical optimization of neochordal implantation location on mitral leaflets during valve repair. JTCVS Tech. 2022, 14, 89–93. [Google Scholar] [CrossRef]
- Fernandez, L.; Monzonis, A.M.; El-Diasty, M.M.; Alvarez-Lorenzo, C.; Concheiro, A.; Fernandez, A.L. Biomechanical characteristics of different methods of neo-chordal fixation to the papillary muscles. J. Card. Surg. 2022, 37, 4408–4415. [Google Scholar] [CrossRef]
- Grinberg, D.; Cottinet, P.J.; Thivolet, S.; Audigier, D.; Capsal, J.F.; Le, M.Q.; Obadia, J.F. Measuring chordae tension during transapical neochordae implantation: Toward understanding objective consequences of mitral valve repair. J. Thorac. Cardiovasc. Surg. 2019, 158, 746–755. [Google Scholar] [CrossRef]
- Jensen, H.; Jensen, M.O.; Waziri, F.; Honge, J.L.; Sloth, E.; Fenger-Gron, M.; Nielsen, S.L. Transapical neochord implantation: Is tension of artificial chordae tendineae dependent on the insertion site? J. Thorac. Cardiovasc. Surg. 2014, 148, 138–143. [Google Scholar] [CrossRef]
- Colli, A.; Manzan, E.; Rucinskas, K.; Janusauskas, V.; Zucchetta, F.; Zakarkaite, D.; Aidietis, A.; Gerosa, G. Acute safety and efficacy of the NeoChord proceduredagger. Interact. Cardiovasc. Thorac. Surg. 2015, 20, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Colli, A.; Bagozzi, L.; Banchelli, F.; Besola, L.; Bizzotto, E.; Pradegan, N.; Fiocco, A.; Manzan, E.; Zucchetta, F.; Bellu, R.; et al. Learning curve analysis of transapical NeoChord mitral valve repair. Eur. J. Cardiothorac. Surg. 2018, 54, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Imbrie-Moore, A.M.; Zhu, Y.; Park, M.H.; Paulsen, M.J.; Wang, H.; Woo, Y.J. Artificial papillary muscle device for off-pump transapical mitral valve repair. J. Thorac. Cardiovasc. Surg. 2022, 164, e133–e141. [Google Scholar] [CrossRef]
- Schulte, L.J.; Melby, S.J. Mitral annuloplasty ring design and selection: Flexible bands are (mostly) all you need. J. Thorac. Cardiovasc. Surg. 2022. [Google Scholar] [CrossRef]
- Zhu, Y.; Imbrie-Moore, A.M.; Wilkerson, R.J.; Paulsen, M.J.; Park, M.H.; Woo, Y.J. Ex vivo biomechanical analysis of flexible versus rigid annuloplasty rings in mitral valves using a novel annular dilation system. BMC Cardiovasc. Disord. 2022, 22, 73. [Google Scholar] [CrossRef]
- Sharony, R.; Saunders, P.C.; Nayar, A.; McAleer, E.; Galloway, A.C.; Delianides, J.; Schwartz, C.F.; Applebaum, R.M.; Kronzon, I.; Colvin, S.B.; et al. Semirigid partial annuloplasty band allows dynamic mitral annular motion and minimizes valvular gradients: An echocardiographic study. Ann. Thorac. Surg. 2004, 77, 518–522. [Google Scholar] [CrossRef]
- Witschey, W.R.; Zhang, D.; Contijoch, F.; McGarvey, J.R.; Lee, M.; Takebayashi, S.; Aoki, C.; Han, Y.; Han, J.; Barker, A.J.; et al. The Influence of Mitral Annuloplasty on Left Ventricular Flow Dynamics. Ann. Thorac. Surg. 2015, 100, 114–121. [Google Scholar] [CrossRef]
- Morichi, H.; Itatani, K.; Yamazaki, S.; Numata, S.; Nakaji, K.; Tamaki, N.; Yaku, H. Influences of mitral annuloplasty on left ventricular flow dynamics assessed with 3-dimensional cine phase-contrast flow magnetic resonance imaging. J. Thorac. Cardiovasc. Surg. 2022, 163, 947–959. [Google Scholar] [CrossRef]
- Hiraoka, A.; Hayashida, A.; Toki, M.; Chikazawa, G.; Yoshitaka, H.; Yoshida, K.; Sakaguchi, T. Impact of type and size of annuloplasty prosthesis on hemodynamic status after mitral valve repair for degenerative disease. Int. J. Cardiol. Heart Vasc. 2020, 28, 100517. [Google Scholar] [CrossRef]
- Alfieri, O.; Maisano, F.; De Bonis, M.; Stefano, P.L.; Torracca, L.; Oppizzi, M.; La Canna, G. The double-orifice technique in mitral valve repair: A simple solution for complex problems. J. Thorac. Cardiovasc. Surg. 2001, 122, 674–681. [Google Scholar] [CrossRef]
- Bhattacharya, S.; He, Z. Annulus tension of the prolapsed mitral valve corrected by edge-to-edge repair. J. Biomech. 2012, 45, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Park, M.H.; Van Kampen, A.; Nagata, Y.; Zhu, Y.; Pandya, P.; Borger, M.A.; Woo, Y.J. Abstract 15014: Aberrant, Elevated Papillary Muscle and Left Ventricular Wall Forces Associated With Mitral Valve Prolapse Are Normalized by Surgical Neochordal Repair but Not by Transcatheter Edge-to-Edge Repair. Circulation 2022, 146, A15014. [Google Scholar]
- Delling, F.N.; Noseworthy, P.A.; Adams, D.H.; Basso, C.; Borger, M.A.; Bouatia-Naij, N.; Elmariah, S.; Evans, F.; Gerstenfeld, E.; Hung, J.; et al. Research Opportunities in the Treatment of Mitral Valve Prolapse: JACC Expert Panel. J. Am. Coll. Cardiol. 2022, 80, 2331–2347. [Google Scholar] [CrossRef]














Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Kampen, A.; Morningstar, J.E.; Goudot, G.; Ingels, N.; Wenk, J.F.; Nagata, Y.; Yaghoubian, K.M.; Norris, R.A.; Borger, M.A.; Melnitchouk, S.; et al. Utilization of Engineering Advances for Detailed Biomechanical Characterization of the Mitral–Ventricular Relationship to Optimize Repair Strategies: A Comprehensive Review. Bioengineering 2023, 10, 601. https://doi.org/10.3390/bioengineering10050601
van Kampen A, Morningstar JE, Goudot G, Ingels N, Wenk JF, Nagata Y, Yaghoubian KM, Norris RA, Borger MA, Melnitchouk S, et al. Utilization of Engineering Advances for Detailed Biomechanical Characterization of the Mitral–Ventricular Relationship to Optimize Repair Strategies: A Comprehensive Review. Bioengineering. 2023; 10(5):601. https://doi.org/10.3390/bioengineering10050601
Chicago/Turabian Stylevan Kampen, Antonia, Jordan E. Morningstar, Guillaume Goudot, Neil Ingels, Jonathan F. Wenk, Yasufumi Nagata, Koushiar M. Yaghoubian, Russell A. Norris, Michael A. Borger, Serguei Melnitchouk, and et al. 2023. "Utilization of Engineering Advances for Detailed Biomechanical Characterization of the Mitral–Ventricular Relationship to Optimize Repair Strategies: A Comprehensive Review" Bioengineering 10, no. 5: 601. https://doi.org/10.3390/bioengineering10050601