
Revisiting the Role of Knee External Rotation in Non-Contact ACL Mechanism of Injury
 , ,
, ,
Abstract
:1. Introduction
2. Methods
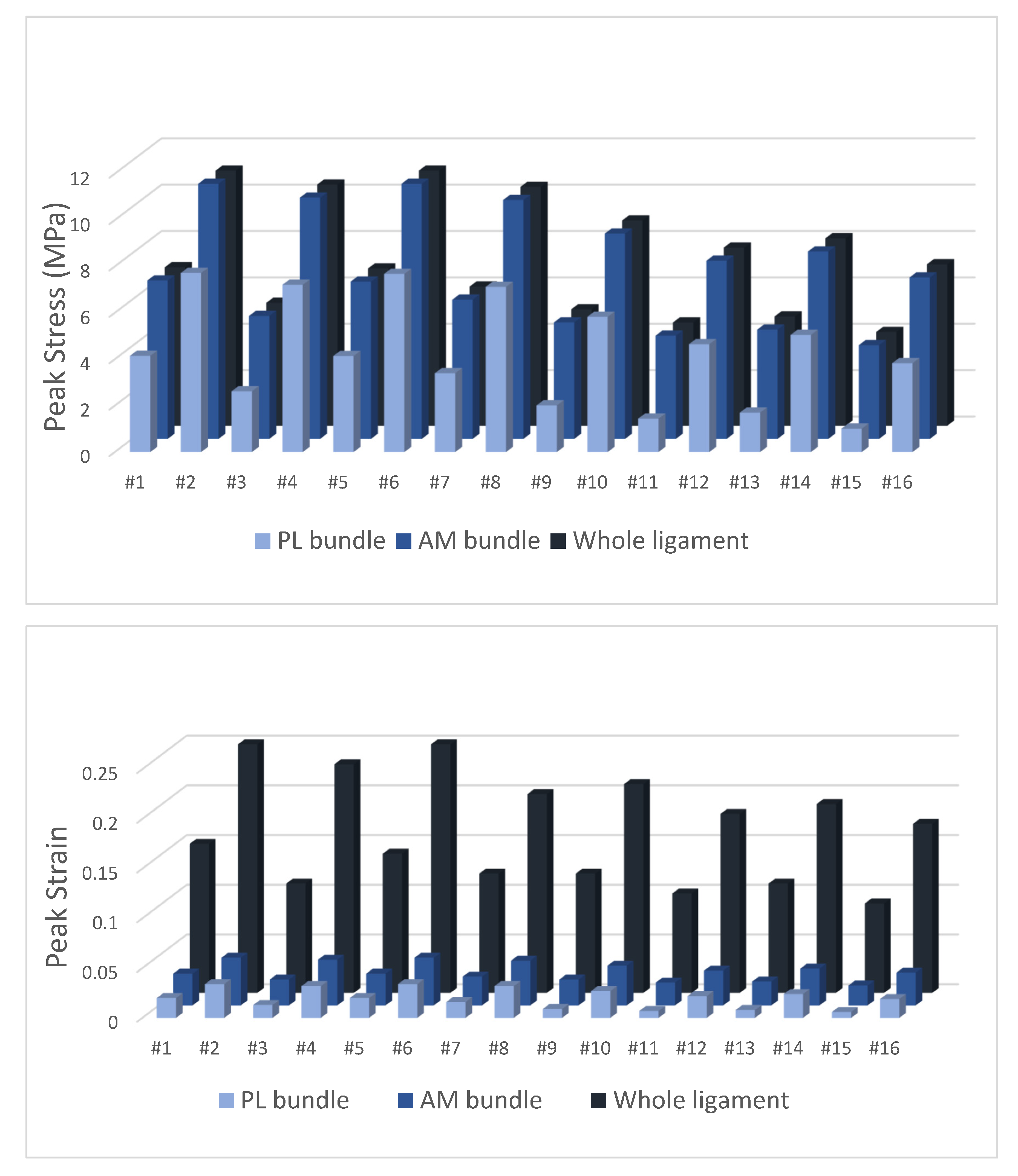
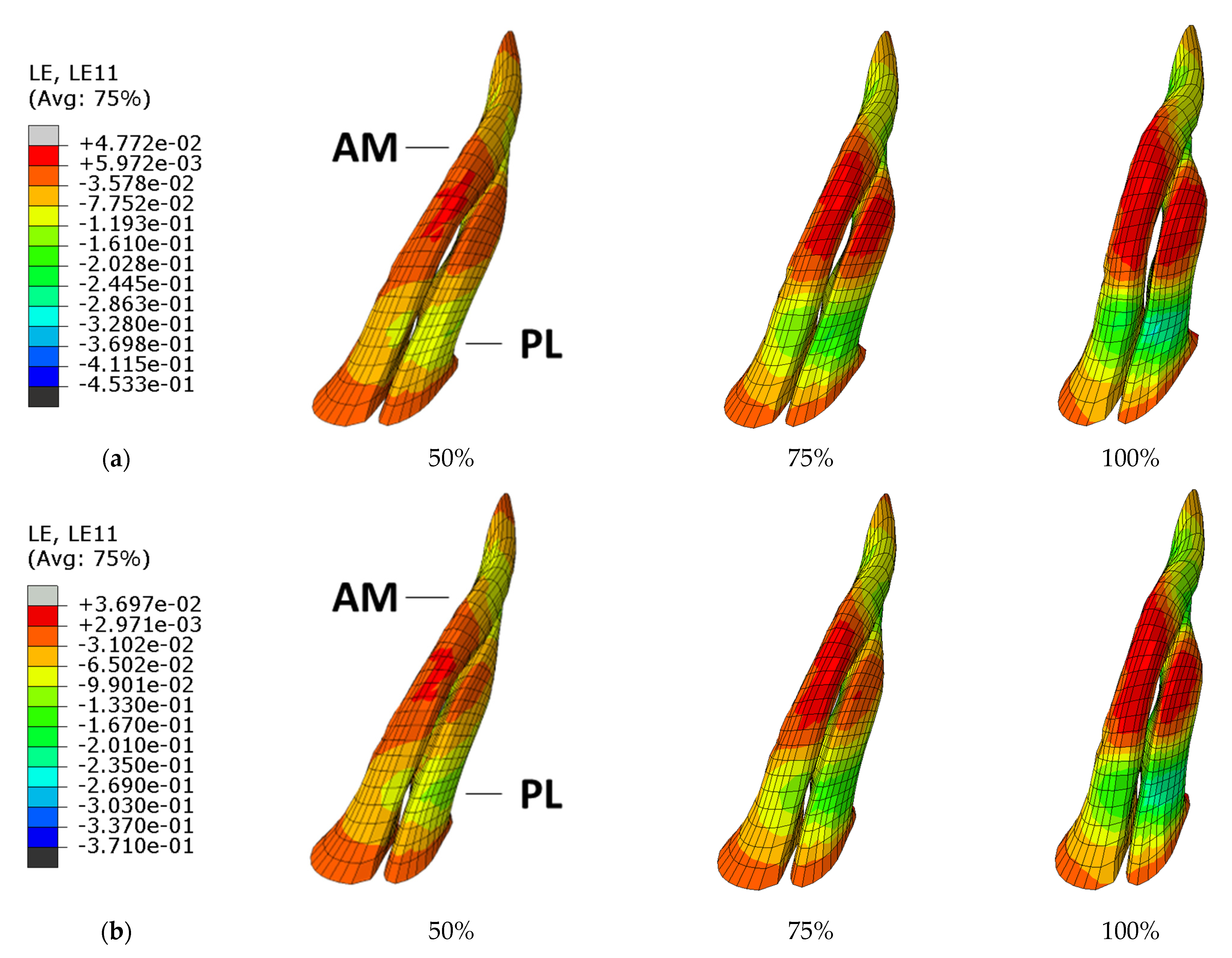
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McLean, S.G.; Mallett, K.F.; Arruda, E.M. Deconstructing the anterior cruciate ligament: What we know and do not know about function, material properties, and injury mechanics. J. Biomech. Eng. 2015, 137, 020906. [Google Scholar] [CrossRef] [PubMed]
- Horvath, A.; Meredith, S.J.; Nishida, K.; Hoshino, Y.; Musahl, V. Objectifying the Pivot Shift Test. Sports Med. Arthrosc. Rev. 2020, 28, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Noyes, F.R.; Jetter, A.W.; Grood, E.S.; Harms, S.P.; Gardner, E.J.; Levy, M.S. Anterior cruciate ligament function in providing rotational stability assessed by medial and lateral tibiofemoral compartment translations and subluxations. Am. J. Sports Med. 2015, 43, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Spritzer, C.E.; Utturkar, G.M.; Toth, A.P.; Garrett, W.E.; DeFrate, L.E. Knee Kinematics During Noncontact Anterior Cruciate Ligament Injury as Determined From Bone Bruise Location. Am. J. Sports Med. 2015, 43, 2515–2521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amis, A.A.; Dawkins, G.P. Functional anatomy of the anterior cruciate ligament. Fibre bundle actions related to ligament replacements and injuries. J. Bone Jt. Surg. Br. Vol. 1991, 73, 260–267. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Han, K.; Su, W.; Jiang, J.; Yan, X.; Yu, J.; Dong, S.; Zhao, J. A Secondary Injury of the Anterolateral Structure Plays a Minor Role in Anterior and Anterolateral Instability of ACL-Deficient Knees in the Case of Functional Iliotibial Band. Arthroscopy 2020, 37, 1182–1191. [Google Scholar] [CrossRef]
- Lee, J.K.; Seo, Y.J.; Jeong, S.Y.; Yang, J.H. Biomechanical function of the anterolateral ligament of the knee: A systematic review. Knee Surg. Relat. Res. 2020, 32, 6. [Google Scholar] [CrossRef]
- Smith, P.A.; Thomas, D.M.; Pomajzl, R.J.; Bley, J.A.; Pfeiffer, F.M.; Cook, J.L. A Biomechanical Study of the Role of the Anterolateral Ligament and the Deep Iliotibial Band for Control of a Simulated Pivot Shift With Comparison of Minimally Invasive Extra-articular Anterolateral Tendon Graft Reconstruction Versus Modified Lemaire Reconstruction After Anterior Cruciate Ligament Reconstruction. Arthroscopy 2019, 35, 1473–1483. [Google Scholar]
- Delaloye, J.R.; Hartog, C.; Blatter, S.; Schläppi, M.; Müller, D.; Denzler, D.; Murar, J.; Koch, P.P. Anterolateral Ligament Reconstruction and Modified Lemaire Lateral Extra-Articular Tenodesis Similarly Improve Knee Stability After Anterior Cruciate Ligament Reconstruction: A Biomechanical Study. Arthroscopy 2020, 36, 1942–1950. [Google Scholar] [CrossRef]
- Kittl, C.; El-Daou, H.; Athwal, K.K.; Gupte, C.M.; Weiler, A.; Williams, A.; Amis, A.A. The Role of the Anterolateral Structures and the ACL in Controlling Laxity of the Intact and ACL-Deficient Knee. Am. J. Sports Med. 2016, 44, 345–354. [Google Scholar] [CrossRef]
- Spencer, L.; Burkhart, T.A.; Tran, M.N.; Rezansoff, A.J.; Deo, S.; Caterine, S.; Getgood, A.M. Biomechanical analysis of simulated clinical testing and reconstruction of the anterolateral ligament of the knee. Am. J. Sports Med. 2015, 43, 2189–2197. [Google Scholar] [CrossRef]
- Inderhaug, E.; Stephen, J.M.; Williams, A.; Amis, A.A. Biomechanical Comparison of Anterolateral Procedures Combined With Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2017, 45, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Marom, N.; Ouanezar, H.; Jahandar, H.; Zayyad, Z.A.; Fraychineaud, T.; Hurwit, D.; Imhauser, C.W.; Wickiewicz, T.L.; Pearle, A.D.; Nawabi, D.H. Lateral Extra-articular Tenodesis Reduces Anterior Cruciate Ligament Graft Force and Anterior Tibial Translation in Response to Applied Pivoting and Anterior Drawer Loads. Am. J. Sports Med. 2020, 48, 3183–3193. [Google Scholar] [CrossRef] [PubMed]
- Csintalan, R.P.; Ehsan, A.; McGarry, M.H.; Fithian, D.F.; Lee, T.Q. Biomechanical and Anatomical Effects of an External Rotational Torque Applied to the Knee: A Cadaveric Study. Am. J. Sports Med. 2006, 34, 1623–1629. [Google Scholar] [CrossRef] [PubMed]
- Lorbach, O.; Pape, D.; Maas, S.; Zerbe, T.; Busch, L.; Kohn, D.; Seil, R. Influence of the anteromedial and posterolateral bundles of the anterior cruciate ligament on external and internal tibiofemoral rotation. Am. J. Sports Med. 2010, 38, 721–727. [Google Scholar] [CrossRef]
- Bull, A.M.; Andersen, H.N.; Basso, O.; Targett, J.; Amis, A.A. Incidence and mechanism of the pivot shift. An in vitro study. Clin. Orthop. Relat. Res. 1999, 363, 219–231. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, H.; Suda, Y.; Otani, T.; Niki, Y.; Seedhom, B.B.; Fujikawa, K. Roles of the anterior cruciate ligament and the medial collateral ligament in preventing valgus instability. J. Orthop. Sci. 2001, 6, 28–32. [Google Scholar] [CrossRef]
- Bach, B.R., Jr.; Warren, R.F.; Wickiewicz, T.L. The pivot shift phenomenon: Results and description of a modified clinical test for anterior cruciate ligament insufficiency. Am. J. Sports Med. 1988, 16, 571–576. [Google Scholar] [CrossRef]
- Jakob, R.P.; Stäubli, H.U.; Deland, J.T. Grading the pivot shift. Objective tests with implications for treatment. J. Bone Jt. Surg. Br. Vol. 1987, 69, 294–299. [Google Scholar] [CrossRef]
- Noyes, F.R.; Grood, E.S.; Cummings, J.F.; Wroble, R.R. An analysis of the pivot shift phenomenon. The knee motions and subluxations induced by different examiners. Am. J. Sports Med. 1991, 19, 148–155. [Google Scholar] [CrossRef]
- Meyer, E.G.; Baumer, T.G.; Slade, J.M.; Smith, W.E.; Haut, R.C. Tibiofemoral contact pressures and osteochondral microtrauma during anterior cruciate ligament rupture due to excessive compressive loading and internal torque of the human knee. Am. J. Sports Med. 2008, 36, 1966–1977. [Google Scholar] [CrossRef] [PubMed]
- Bates, N.A.; Schilaty, N.D.; Nagelli, C.V.; Krych, A.J.; Hewett, T.E. Multiplanar Loading of the Knee and Its Influence on Anterior Cruciate Ligament and Medial Collateral Ligament Strain During Simulated Landings and Noncontact Tears. Am. J. Sports Med. 2019, 47, 1844–1853. [Google Scholar] [CrossRef] [PubMed]
- Lo, J.; Müller, O.; Wünschel, M.; Bauer, S.; Wülker, N. Forces in anterior cruciate ligament during simulated weight-bearing flexion with anterior and internal rotational tibial load. J. Biomech. 2008, 41, 1855–1861. [Google Scholar] [CrossRef] [PubMed]
- Kiapour, A.M.; Demetropoulos, C.K.; Kiapour, A.; Quatman, C.E.; Wordeman, S.C.; Goel, V.K.; Hewett, T.E. Strain Response of the Anterior Cruciate Ligament to Uniplanar and Multiplanar Loads During Simulated Landings: Implications for Injury Mechanism. Am. J. Sports Med. 2016, 44, 2087–2096. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.W.; Kiapour, A.M.; Quatman, C.E.; Wordeman, S.C.; Goel, V.K.; Hewett, T.E.; Demetropoulos, C.K. Clinically relevant injury patterns after an anterior cruciate ligament injury provide insight into injury mechanisms. Am. J. Sports Med. 2013, 41, 385–395. [Google Scholar] [CrossRef] [Green Version]
- Kiapour, A.; Kiapour, A.M.; Kaul, V.; Quatman, C.E.; Wordeman, S.C.; Hewett, T.E.; Demetropoulos, C.K.; Goel, V.K. Finite element model of the knee for investigation of injury mechanisms: Development and validation. J. Biomech. Eng. 2014, 136, 011002. [Google Scholar] [CrossRef] [Green Version]
- Sága, M.; Vaško, M.; Ságová, Z.; Kuric, I.; Kopas, P.; Handrik, M. FEM Simulation of Non-proportional Multiaxial Fatigue Damage. In Proceedings of the MATEC Web of Conferences, Curtin, Malaysia, 12–13 December 2022; p. 02006. [Google Scholar]
- Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; Wibowo, D.B.; Kurdi, O.; Tauviqirrahman, M.; Jamari, J. Minimizing risk of failure from ceramic-on-ceramic total hip prosthesis by selecting ceramic materials based on tresca stress. Sustainability 2022, 14, 13413. [Google Scholar] [CrossRef]
- Stanev, D.; Moustakas, K.; Gliatis, J.; Koutsojannis, C. ACL Reconstruction Decision Support. Personalized Simulation of the Lachman Test and Custom Activities. Methods Inf. Med. 2016, 55, 98–105. [Google Scholar] [CrossRef]
- Weiss, J.A.; Maker, B.N.; Govindjee, S. Finite element implementation of incompressible, transversely isotropic hyperelasticity. Comput. Methods Appl. Mech. Eng. 1996, 135, 107–128. [Google Scholar] [CrossRef]
- Benos, L.; Stanev, D.; Spyrou, L.; Moustakas, K.; Tsaopoulos, D.E. A Review on Finite Element Modeling and Simulation of the Anterior Cruciate Ligament Reconstruction. Front. Bioeng. Biotechnol. 2020, 8, 967. [Google Scholar] [CrossRef]
- Naghibi Beidokhti, H.; Janssen, D.; van de Groes, S.; Hazrati, J.; Van den Boogaard, T.; Verdonschot, N. The influence of ligament modelling strategies on the predictive capability of finite element models of the human knee joint. J. Biomech. 2017, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Homyk, A.; Orsi, A.; Wibby, S.; Yang, N.; Nayeb-Hashemi, H.; Canavan, P.K. Failure locus of the anterior cruciate ligament: 3D finite element analysis. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Shi, H.; Liu, Z.; Zhang, J.; Li, H.; Huang, H.; Ao, Y. Finite Element Analysis and Experimental Validation of the Anterior Cruciate Ligament and Implications for the Injury Mechanism. Bioengineering 2022, 9, 590. [Google Scholar] [CrossRef] [PubMed]
- Amis, A.A. The functions of the fibre bundles of the anterior cruciate ligament in anterior drawer, rotational laxity and the pivot shift. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Erdemir, A. Open Knee: Open Source Modeling and Simulation in Knee Biomechanics. J. Knee Surg. 2016, 29, 107–116. [Google Scholar] [CrossRef] [Green Version]
- Iriuchishima, T.; Ryu, K.; Aizawa, S.; Fu, F.H. Size correlation between the tibial anterior cruciate ligament footprint and the tibia plateau. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1147–1152. [Google Scholar] [CrossRef]
- Cohen, S.B.; VanBeek, C.; Starman, J.S.; Armfield, D.; Irrgang, J.J.; Fu, F.H. MRI measurement of the 2 bundles of the normal anterior cruciate ligament. Orthopedics 2009, 32, 687. [Google Scholar]
- Siebold, R.; Dejour, D.; Zaffagnini, S. Anterior Cruciate Ligament Reconstruction: A Practical Surgical Guide; Springer Science & Business: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Sohn, K.M.; Lee, M.J.; Hong, H.; Yoon, Y.C.; Park, C.D.; Wang, J.H. The Bow Tie Shape of the Anterior Cruciate Ligament as Visualized by High-Resolution Magnetic Resonance Imaging. Am. J. Sports Med. 2017, 45, 1881–1887. [Google Scholar] [CrossRef]
- Kubıcek, M.; Florian, Z. Stress strain analysis of knee joint. Eng. Mech. 2009, 16, 315–322. [Google Scholar]
- Li, L.; Yang, X.; Yang, L.; Zhang, K.; Shi, J.; Zhu, L.; Liang, H.; Wang, X.; Jiang, Q. Biomechanical analysis of the effect of medial meniscus degenerative and traumatic lesions on the knee joint. Am. J. Transl. Res. 2019, 11, 542–556. [Google Scholar]
- Kiapour, A. Non-Contact ACL Injuries During Landing: Risk Factors and Mechanisms. Ph.D. Thesis, University of Toledo, Toledo, OH, USA, 2013. [Google Scholar]
- Galbusera, F.; Freutel, M.; Dürselen, L.; D’Aiuto, M.; Croce, D.; Villa, T.; Sansone, V.; Innocenti, B. Material models and properties in the finite element analysis of knee ligaments: A literature review. Front. Bioeng. Biotechnol. 2014, 2, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, R.J.; Wilcox, R.K.; Jones, A.C. Finite element models of the tibiofemoral joint: A review of validation approaches and modelling challenges. Med. Eng. Phys. 2019, 74, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Vedi, V.; Williams, A.; Tennant, S.J.; Spouse, E.; Hunt, D.M.; Gedroyc, W.M. Meniscal movement. An in-vivo study using dynamic MRI. J. Bone Jt. Surg. Br. Vol. 1999, 81, 37–41. [Google Scholar] [CrossRef]
- Johnston, J.T.; Mandelbaum, B.R.; Schub, D.; Rodeo, S.A.; Matava, M.J.; Silvers-Granelli, H.J.; Cole, B.J.; ElAttrache, N.S.; McAdams, T.R.; Brophy, R.H. Video Analysis of Anterior Cruciate Ligament Tears in Professional American Football Athletes. Am. J. Sports Med. 2018, 46, 862–868. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, C.; Blackburn, J.; Withers, D.; Tierney, G.; Moran, C.; Simms, C. Mechanisms of ACL injury in professional rugby union: A systematic video analysis of 36 cases. Br. J. Sports Med. 2018, 52, 994–1001. [Google Scholar] [CrossRef]
- Olsen, O.E.; Myklebust, G.; Engebretsen, L.; Bahr, R. Injury mechanisms for anterior cruciate ligament injuries in team handball: A systematic video analysis. Am. J. Sports Med. 2004, 32, 1002–1012. [Google Scholar] [CrossRef] [PubMed]
- Carlson, V.R.; Sheehan, F.T.; Boden, B.P. Video Analysis of Anterior Cruciate Ligament (ACL) Injuries: A Systematic Review. JBJS Rev. 2016, 4, e5. [Google Scholar] [CrossRef] [Green Version]
- Krosshaug, T.; Nakamae, A.; Boden, B.P.; Engebretsen, L.; Smith, G.; Slauterbeck, J.R.; Hewett, T.E.; Bahr, R. Mechanisms of anterior cruciate ligament injury in basketball: Video analysis of 39 cases. Am. J. Sports Med. 2007, 35, 359–367. [Google Scholar] [CrossRef]
- Della Villa, F.; Buckthorpe, M.; Grassi, A.; Nabiuzzi, A.; Tosarelli, F.; Zaffagnini, S.; Della Villa, S. Systematic video analysis of ACL injuries in professional male football (soccer): Injury mechanisms, situational patterns and biomechanics study on 134 consecutive cases. Br. J. Sports Med. 2020, 54, 1423–1432. [Google Scholar] [CrossRef]
- Waldén, M.; Krosshaug, T.; Bjørneboe, J.; Andersen, T.E.; Faul, O.; Hägglund, M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: A systematic video analysis of 39 cases. Br. J. Sports Med. 2015, 49, 1452–1460. [Google Scholar] [CrossRef] [Green Version]
- Kimura, Y.; Ishibashi, Y.; Tsuda, E.; Yamamoto, Y.; Tsukada, H.; Toh, S. Mechanisms for anterior cruciate ligament injuries in badminton. Br. J. Sports Med. 2010, 44, 1124–1127. [Google Scholar] [CrossRef] [PubMed]
- Kiapour, A.M.; Wordeman, S.C.; Paterno, M.V.; Quatman, C.E.; Levine, J.W.; Goel, V.K.; Demetropoulos, C.K.; Hewett, T.E. Diagnostic value of knee arthrometry in the prediction of anterior cruciate ligament strain during landing. Am. J. Sports Med. 2014, 42, 312–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Chen, J. A comparative study on different walking load models. Struct. Eng. Mech. 2017, 63, 847–856. [Google Scholar]
- Järvinen, M.; Natri, A.; Laurila, S.; Kannus, P. Mechanisms of anterior cruciate ligament ruptures in skiing. Knee Surg. Sports Traumatol. Arthrosc. 1994, 2, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Bastos, R.; Andrade, R.; Vasta, S.; Pereira, R.; Papalia, R.; van der Merwe, W.; Rodeo, S.; Espregueira-Mendes, J. Tibiofemoral bone bruise volume is not associated with meniscal injury and knee laxity in patients with anterior cruciate ligament rupture. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 3318–3326. [Google Scholar] [CrossRef] [PubMed]
- Kim-Wang, S.Y.; Scribani, M.B.; Whiteside, M.B.; DeFrate, L.E.; Lassiter, T.E.; Wittstein, J.R. Distribution of Bone Contusion Patterns in Acute Noncontact Anterior Cruciate Ligament-Torn Knees. Am. J. Sports Med. 2021, 49, 404–409. [Google Scholar] [CrossRef]
- Zhang, L.; Hacke, J.D.; Garrett, W.E.; Liu, H.; Yu, B. Bone Bruises Associated with Anterior Cruciate Ligament Injury as Indicators of Injury Mechanism: A Systematic Review. Sports Med. 2019, 49, 453–462. [Google Scholar] [CrossRef]
- Grassi, A.; Agostinone, P.; Di Paolo, S.; Lucidi, G.A.; Macchiarola, L.; Bontempi, M.; Marchiori, G.; Bragonzoni, L.; Zaffagnini, S. Knee position at the moment of bone bruise could reflect the late phase of non-contact anterior cruciate ligament injury rather than the mechanisms leading to ligament failure. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 4138–4145. [Google Scholar] [CrossRef]
- Park, H.S.; Wilson, N.A.; Zhang, L.Q. Gender differences in passive knee biomechanical properties in tibial rotation. J. Orthop. Res. 2008, 26, 937–944. [Google Scholar] [CrossRef]
- LaPrade, R.F.; Burnett, Q.M. Femoral intercondylar notch stenosis and correlation to anterior cruciate ligament injuries. A prospective study. Am. J. Sports Med. 1994, 22, 198–202. [Google Scholar] [CrossRef]
- Fu, Y.; Wang, X.; Yu, T. Simulation Analysis of Knee Ligaments in the Landing Phase of Freestyle Skiing Aerial. Appl. Sci. 2019, 9, 3713. [Google Scholar] [CrossRef] [Green Version]
- Xu, D.; Jiang, X.; Cen, X.; Baker, J.S.; Gu, Y. Single-Leg Landings Following a Volleyball Spike May Increase the Risk of Anterior Cruciate Ligament Injury More Than Landing on Both-Legs. Appl. Sci. 2021, 11, 130. [Google Scholar] [CrossRef]
- Takahashi, S.; Nagano, Y.; Ito, W.; Kido, Y.; Okuwaki, T. A retrospective study of mechanisms of anterior cruciate ligament injuries in high school basketball, handball, judo, soccer, and volleyball. Medicine 2019, 98, e16030. [Google Scholar] [CrossRef] [PubMed]
- Koga, H.; Nakamae, A.; Shima, Y.; Iwasa, J.; Myklebust, G.; Engebretsen, L.; Bahr, R.; Krosshaug, T. Mechanisms for noncontact anterior cruciate ligament injuries: Knee joint kinematics in 10 injury situations from female team handball and basketball. Am. J. Sports Med. 2010, 38, 2218–2225. [Google Scholar] [CrossRef] [PubMed]
- van der List, J.P.; Mintz, D.N.; DiFelice, G.S. The Location of Anterior Cruciate Ligament Tears: A Prevalence Study Using Magnetic Resonance Imaging. Orthop. J. Sports Med. 2017, 5, 2325967117709966. [Google Scholar] [CrossRef] [Green Version]
- Henle, P.; Röder, C.; Perler, G.; Heitkemper, S.; Eggli, S. Dynamic Intraligamentary Stabilization (DIS) for treatment of acute anterior cruciate ligament ruptures: Case series experience of the first three years. BMC Musculoskelet. Disord. 2015, 16, 27. [Google Scholar] [CrossRef] [Green Version]
- van der List, J.P.; DiFelice, G.S. Role of tear location on outcomes of open primary repair of the anterior cruciate ligament: A systematic review of historical studies. Knee 2017, 24, 898–908. [Google Scholar] [CrossRef]
- Paschos, N.K.; Gartzonikas, D.; Barkoula, N.M.; Moraiti, C.; Paipetis, A.; Matikas, T.E.; Georgoulis, A.D. Cadaveric study of anterior cruciate ligament failure patterns under uniaxial tension along the ligament. Arthroscopy 2010, 26, 957–967. [Google Scholar] [CrossRef]
- Woo, S.L.; Hollis, J.M.; Adams, D.J.; Lyon, R.M.; Takai, S. Tensile properties of the human femur-anterior cruciate ligament-tibia complex. The effects of specimen age and orientation. Am. J. Sports Med. 1991, 19, 217–225. [Google Scholar] [CrossRef]
- Butler, D.L.; Guan, Y.; Kay, M.D.; Cummings, J.F.; Feder, S.M.; Levy, M.S. Location-dependent variations in the material properties of the anterior cruciate ligament. J. Biomech. 1992, 25, 511–518. [Google Scholar] [CrossRef]
- Zantop, T.; Herbort, M.; Raschke, M.J.; Fu, F.H.; Petersen, W. The role of the anteromedial and posterolateral bundles of the anterior cruciate ligament in anterior tibial translation and internal rotation. Am. J. Sports Med. 2007, 35, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Limbert, G.; Middleton, J.; Taylor, M. Finite element analysis of the human ACL subjected to passive anterior tibial loads. Comput. Methods Biomech. Biomed. Eng. 2004, 7, 1–8. [Google Scholar] [CrossRef]
- Hodel, S.; Postolka, B.; Flury, A.; Schütz, P.; Taylor, W.R.; Vlachopoulos, L.; Fucentese, S.F. Influence of Bone Morphology on In Vivo Tibio-Femoral Kinematics in Healthy Knees during Gait Activities. J. Clin. Med. 2022, 11, 5082. [Google Scholar] [CrossRef]
- Knapp, A.; Williams, L.N. Predicting the Effect of Localized ACL Damage on Neighbor Ligament Mechanics via Finite Element Modeling. Bioengineering 2022, 9, 54. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, B.; Cheng, C.-K. Stiffness and shape of the ACL graft affects tunnel enlargement and graft wear. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 2184–2193. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.G.; Kang, K.T.; Wang, J.H. Biomechanical Difference between Conventional Transtibial Single-Bundle and Anatomical Transportal Double-Bundle Anterior Cruciate Ligament Reconstruction Using Three-Dimensional Finite Element Model Analysis. J. Clin. Med. 2021, 10, 1625. [Google Scholar] [CrossRef]
- Wang, H.; Tao, M.; Shi, Q.; He, K.; Cheng, C.-K. Graft Diameter Should Reflect the Size of the Native Anterior Cruciate Ligament (ACL) to Improve the Outcome of ACL Reconstruction: A Finite Element Analysis. Bioengineering 2022, 9, 507. [Google Scholar] [CrossRef]
- Bartolin, P.B.; Boixadera, R.; Hudetz, D. Experimental testing and finite element method analysis of the anterior cruciate ligament primary repair with internal brace augmentation. Med. Eng. Phys. 2021, 95, 76–83. [Google Scholar] [CrossRef]
- Bittencourt, N.F.N.; Meeuwisse, W.H.; Mendonça, L.D.; Nettel-Aguirre, A.; Ocarino, J.M.; Fonseca, S.T. Complex systems approach for sports injuries: Moving from risk factor identification to injury pattern recognition—Narrative review and new concept. Br. J. Sports Med. 2016, 50, 1309. [Google Scholar] [CrossRef] [Green Version]
- Dhaher, Y.Y.; Kwon, T.-H.; Barry, M. The effect of connective tissue material uncertainties on knee joint mechanics under isolated loading conditions. J. Biomech. 2010, 43, 3118–3125. [Google Scholar] [CrossRef] [Green Version]
- Chokhandre, S.; Schwartz, A.; Klonowski, E.; Landis, B.; Erdemir, A. Open Knee(s): A Free and Open Source Library of Specimen-Specific Models and Related Digital Assets for Finite Element Analysis of the Knee Joint. Ann. Biomed. Eng. 2023, 51, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Andrade, R.; Vasta, S.; Sevivas, N.; Pereira, R.; Leal, A.; Papalia, R.; Pereira, H.; Espregueira-Mendes, J. Notch morphology is a risk factor for ACL injury: A systematic review and meta-analysis. J. ISAKOS 2016, 1, 70–81. [Google Scholar] [CrossRef]
- Bayer, S.; Meredith, S.J.; Wilson, K.; de Sa, D.; Pauyo, T.; Byrne, K.; McDonough, C.M.; Musahl, V. Knee Morphological Risk Factors for Anterior Cruciate Ligament Injury: A Systematic Review. J. Bone Jt. Surg. Am. 2020, 102, 703–718. [Google Scholar] [CrossRef]
- Nelitz, M.; Seitz, A.M.; Bauer, J.; Reichel, H.; Ignatius, A.; Dürselen, L. Increasing posterior tibial slope does not raise anterior cruciate ligament strain but decreases tibial rotation ability. Clin. Biomech. (Bristol Avon) 2013, 28, 285–290. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Young’s Modulus (MPa) | Poisson’s Ratio | Parameters | Elements | Nodes | |
|---|---|---|---|---|---|---|
| Femur/Tibia [41] | Elastic | 17400. | 0.3 | - | S4 13860/11360 | 13,862/11,362 |
| Articular cartilage [41] | Elastic | 80. | 0.475 | - | C3D8H 25721 | 35,712 |
| Menisci [42] | Elastic | 120. | 0.45 | - | C3D8H 9100 | 11,616 |
| ACL Connective tissue [32] | Hyperelastic (Neo–Hookean) | - | - | C10 = 1.0 D1 = 1 × 10−5 | C3D4H 3875 | 1288 |
| Anterior Cruciate Ligament [32] | Anisotropic Hyperelastic (HGO) | - | - | K1 = 52.52 K2 = 5.86 K = 0.0 | C3D8H 3000 | 3796 |
| Posterior Cruciate Ligament [32] | Anisotropic Hyperelastic (HGO) | - | - | K1 = 46.42 K2 = 2.73 K = 0.0 | C3D8H 5248 | 5922 |
| Lateral Collateral Ligament [32] | Anisotropic Hyperelastic (HGO) | - | - | K1 = 41.21 K2 = 5.26 K = 0.0 | C3D8H 6656 | 7425 |
| Medial Collateral Ligament [32] | Anisotropic Hyperelastic (HGO) | - | - | K1 = 41.01 K2 = 5.07 K = 0.0 | C3D8H 5120 | 5781 |
| # Simulation | Knee Flexion | Axial Force | Anterior Tibial Load | External Rotation | Internal Rotation | Valgus (Abduction Moment) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| 20° | 700 N | 4000 N | 0 N | 134 N | 15 Nm | 20 Nm | 15 Nm | 20 Nm | 50 Nm | |
| #1 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #2 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #3 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #4 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #5 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #6 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #7 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #8 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #9 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #10 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #11 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #12 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #13 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #14 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #15 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| #16 | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, C.F.; Bastos, R.; Andrade, R.; Pereira, R.; Parente, M.P.L.; Jorge, R.N.; Espregueira-Mendes, J. Revisiting the Role of Knee External Rotation in Non-Contact ACL Mechanism of Injury. Appl. Sci. 2023, 13, 3802. https://doi.org/10.3390/app13063802
Santos CF, Bastos R, Andrade R, Pereira R, Parente MPL, Jorge RN, Espregueira-Mendes J. Revisiting the Role of Knee External Rotation in Non-Contact ACL Mechanism of Injury. Applied Sciences. 2023; 13(6):3802. https://doi.org/10.3390/app13063802
Chicago/Turabian StyleSantos, Carla F., Ricardo Bastos, Renato Andrade, Rogério Pereira, Marco P. L. Parente, Renato Natal Jorge, and João Espregueira-Mendes. 2023. "Revisiting the Role of Knee External Rotation in Non-Contact ACL Mechanism of Injury" Applied Sciences 13, no. 6: 3802. https://doi.org/10.3390/app13063802