
Serum and Erythrocyte Antioxidant Defense in Colorectal Cancer Patients during Early Postoperative Period: Potential Modifiers and Impact on Clinical Outcomes

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Analysis of Antioxidant Defenses
2.2.1. Serum Antioxidants
Total Antioxidant Capacity (TAC)
Ferric Reducing Antioxidant Power (FRAP)
2.2.2. Erythrocyte Antioxidants
Glutathione Peroxidase (GPx) (EC 1.11.1.9)
Superoxide Dismutase (SOD) (EC 1.15.1.1)
2.3. Laboratory Paramaters and Inflammatory Cytokines
2.4. Statistical Methods
3. Results
3.1. Impact of Patient- and Disease-Related Factors on Preoperative Serum and Erythrocyte Antioxidant Capacity
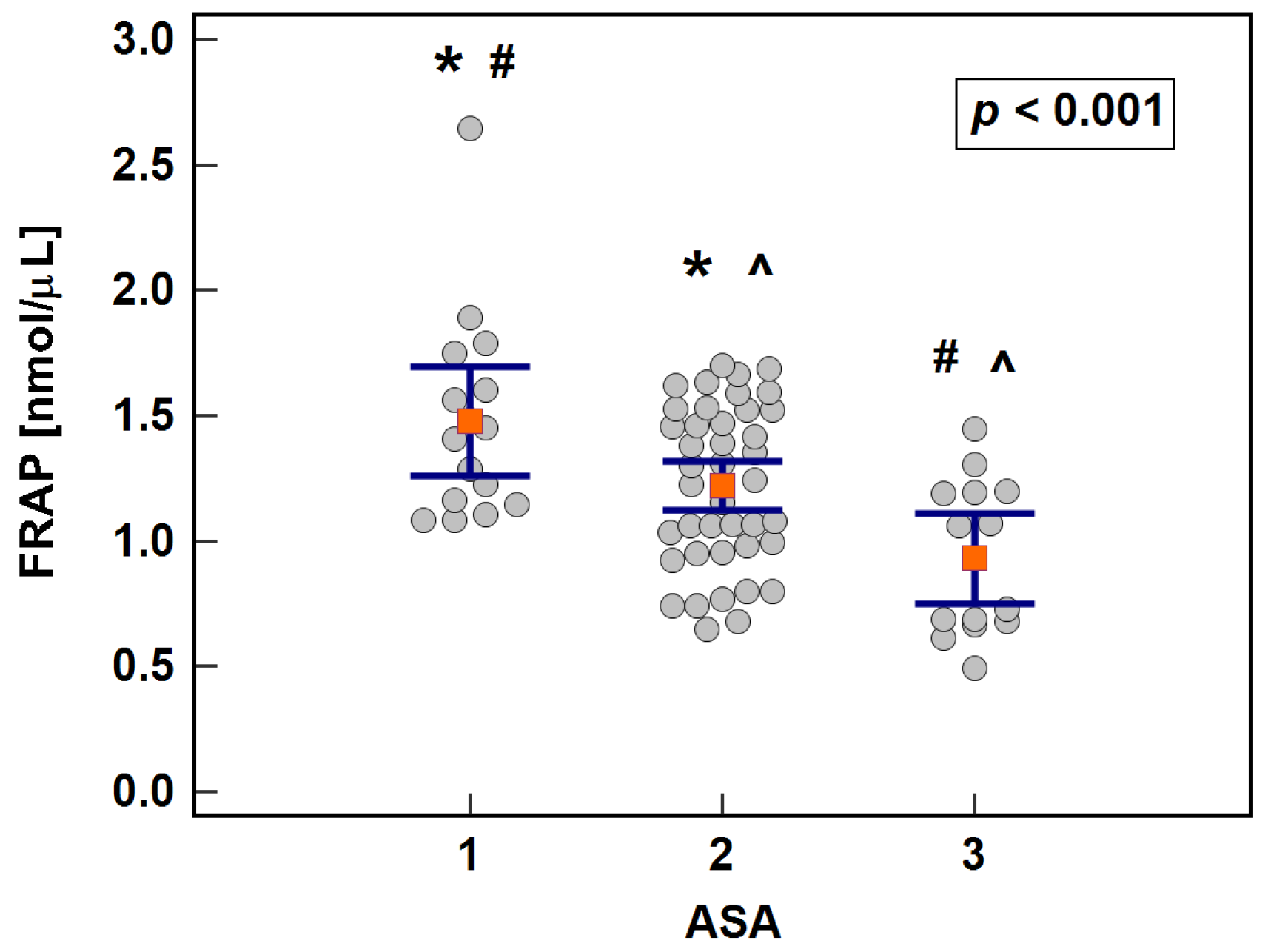
3.1.1. Serum Antioxidant Capacity: FRAP and TAC
3.1.2. Erythrocyte Antioxidants: SOD1 and GPx1
3.2. Impact of Patient- and Disease-Related Factors on Serum Antioxidant Capacity and Erythrocyte Antioxidant Enzymes during Early Postoperative Period
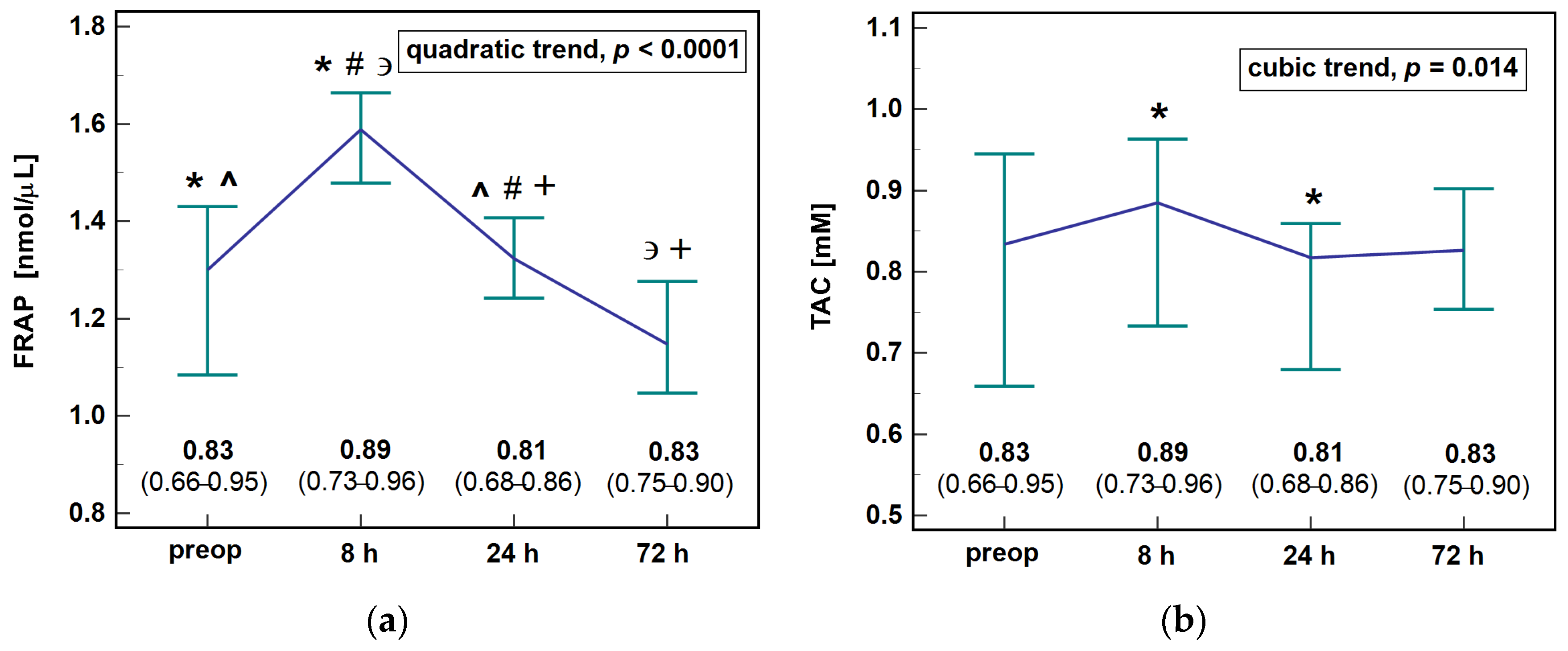
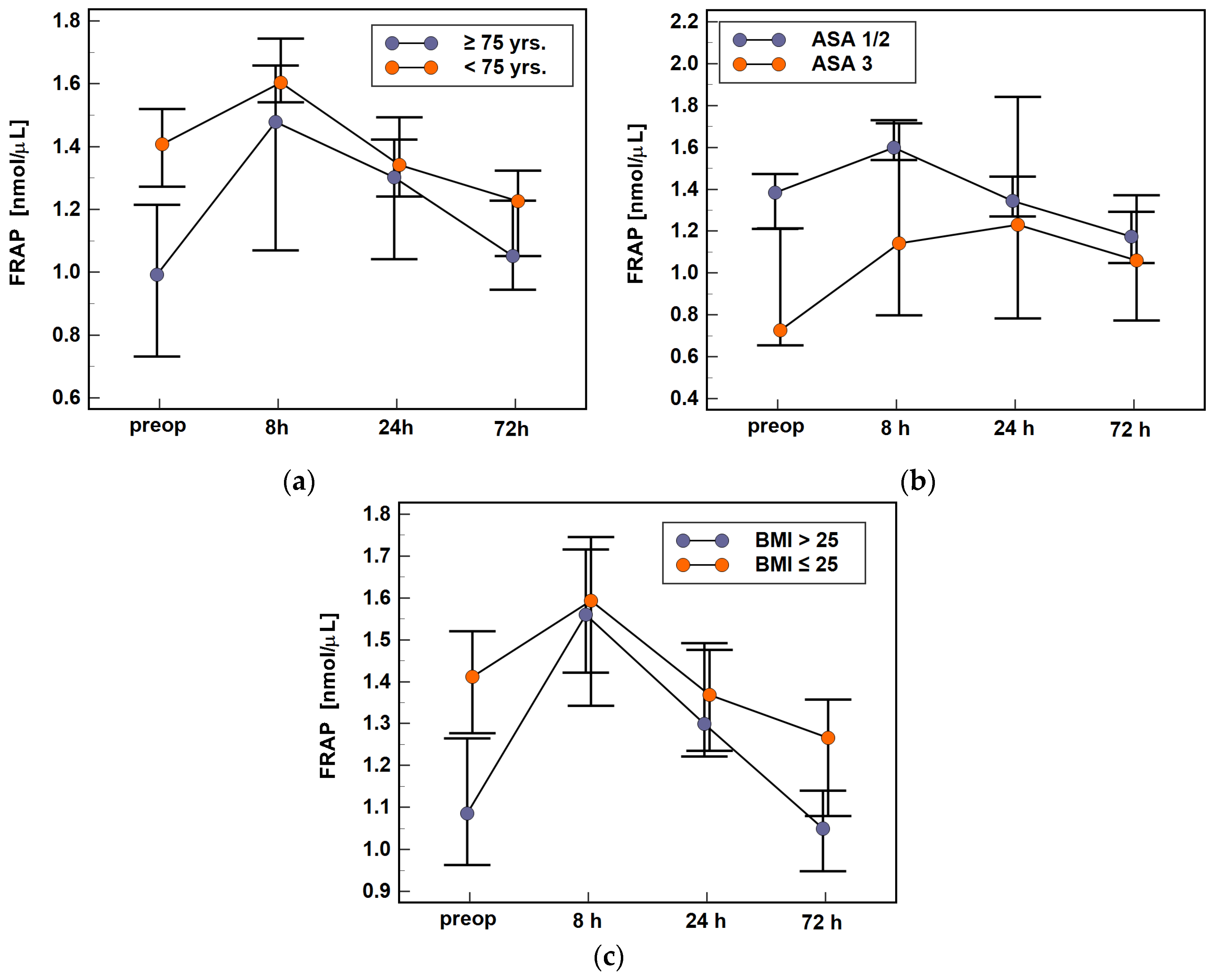
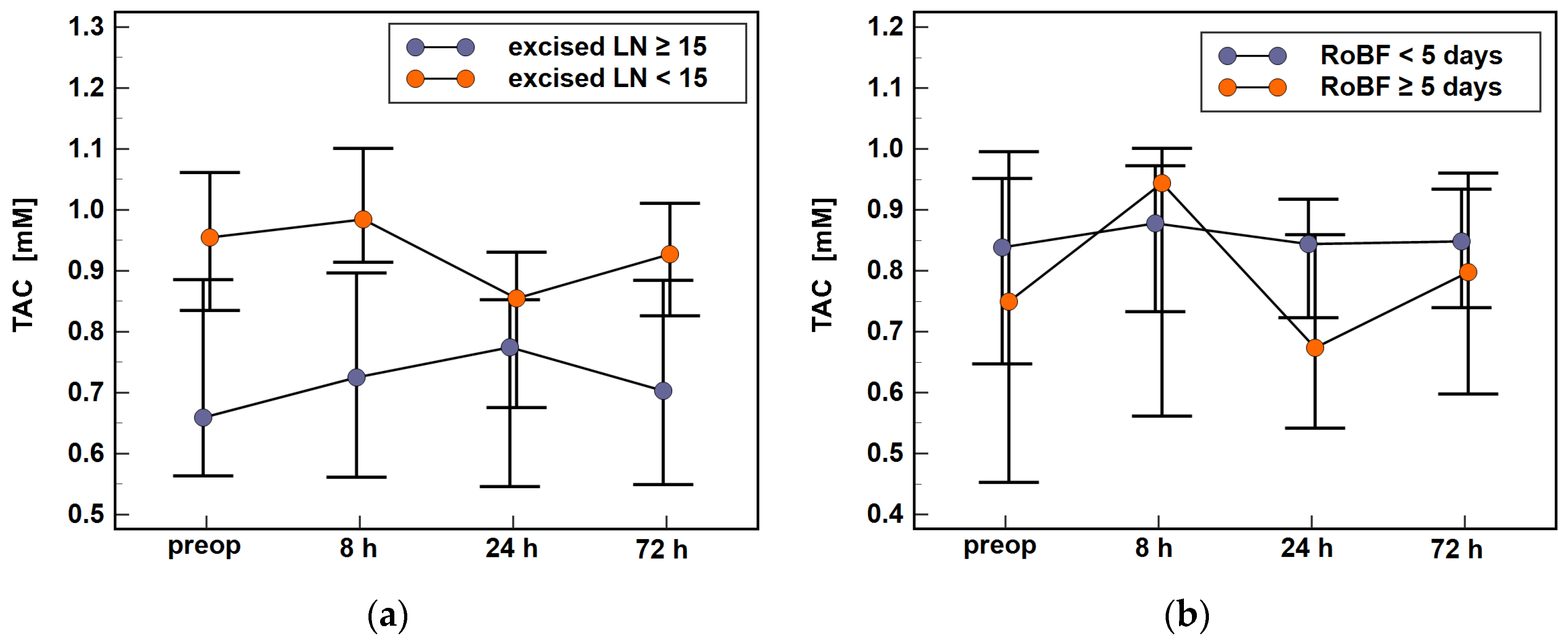
3.2.1. Serum Antioxidant Capacity: FRAP and TAC

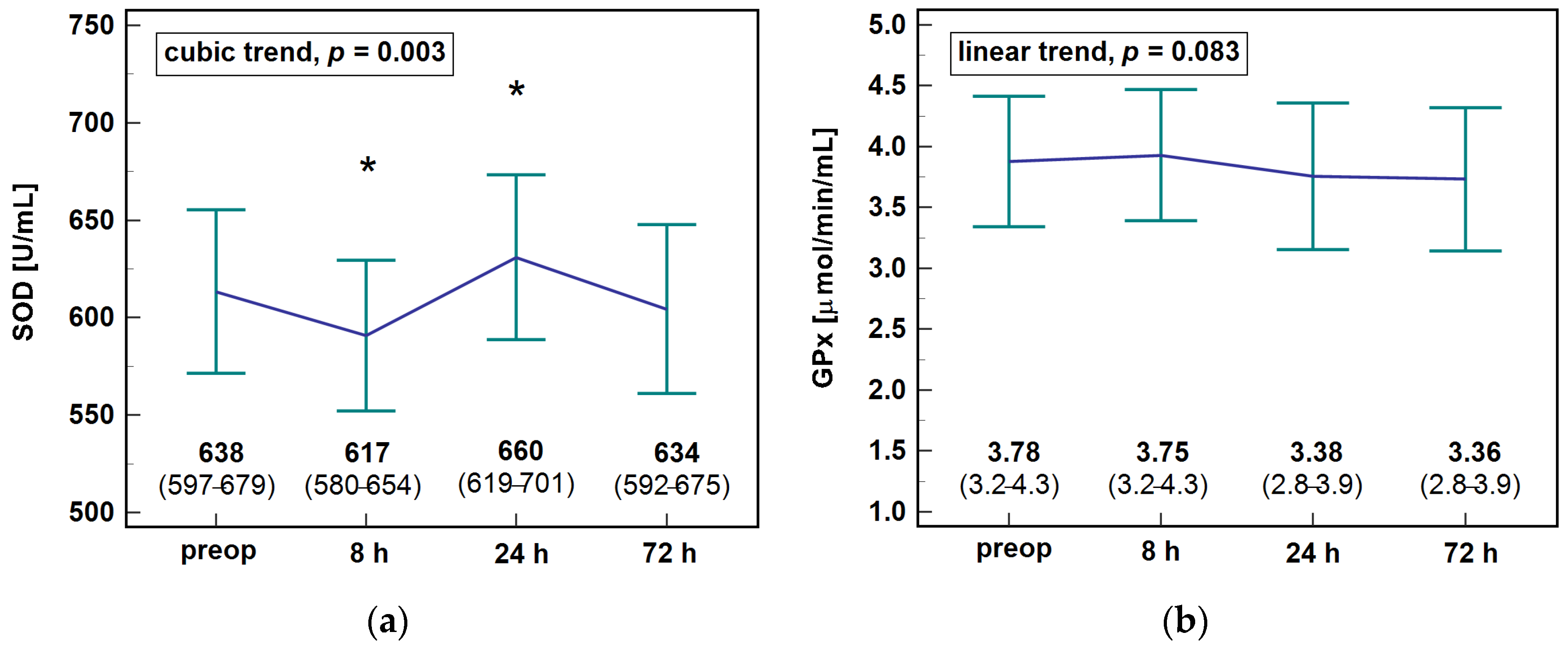
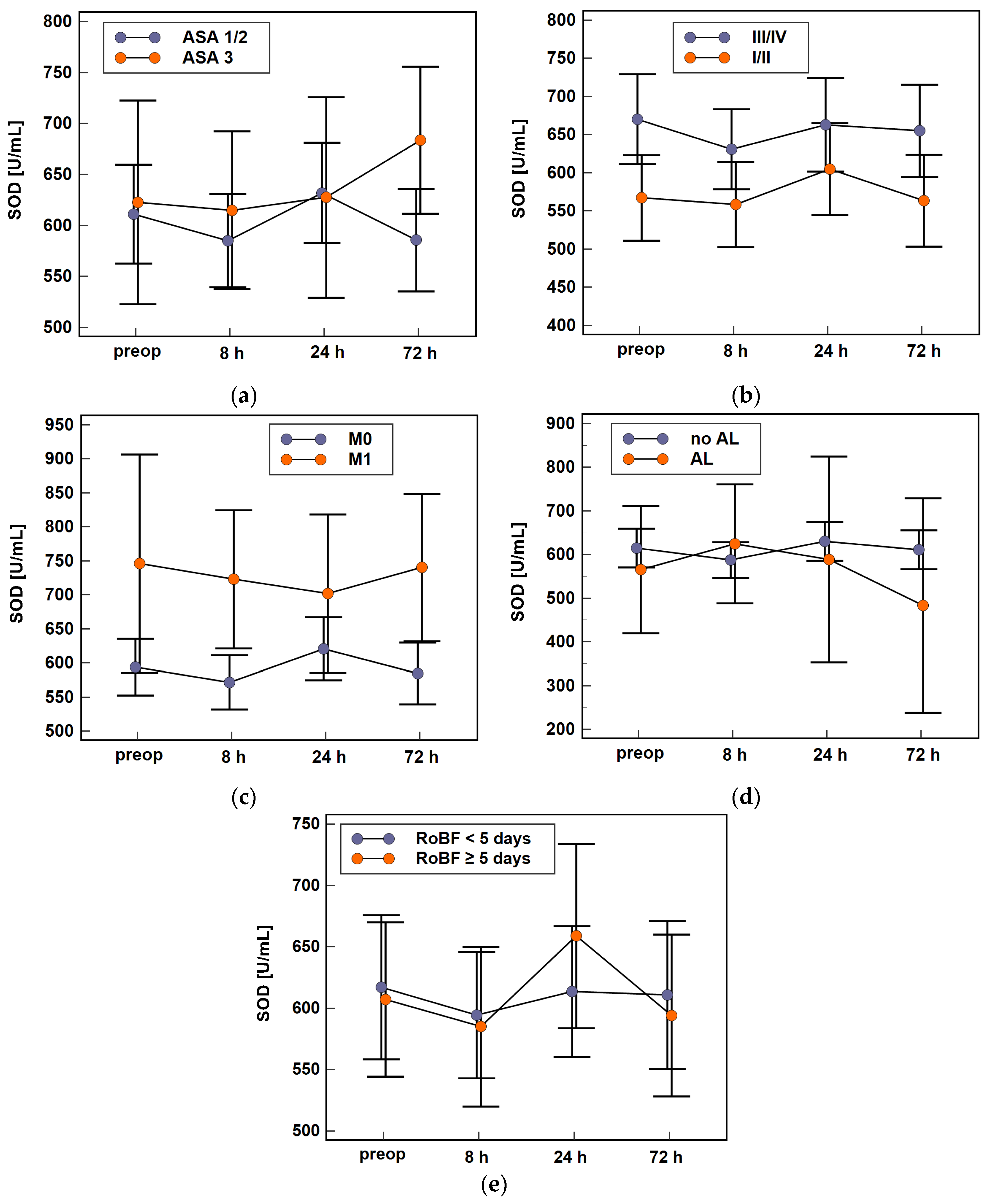
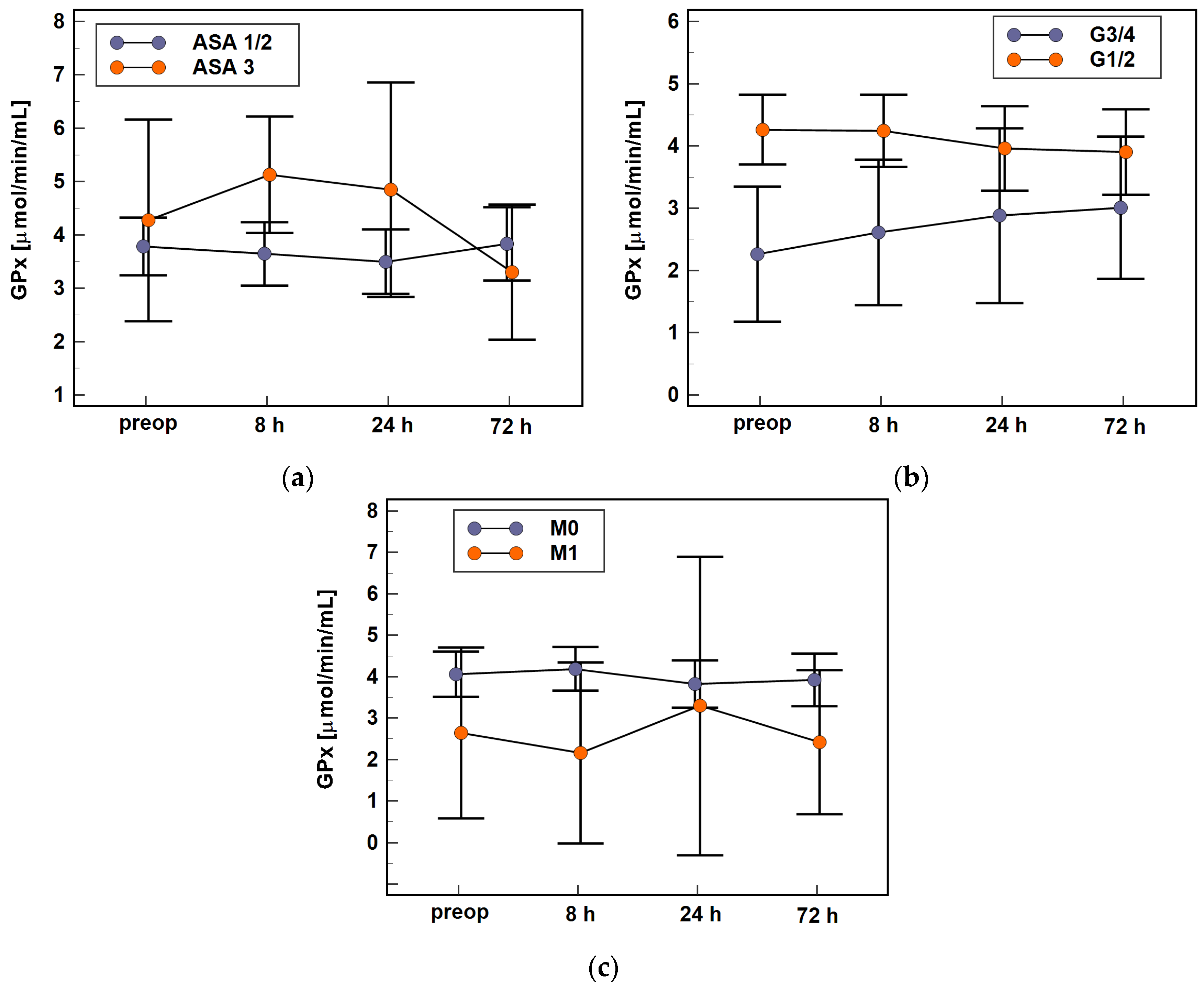
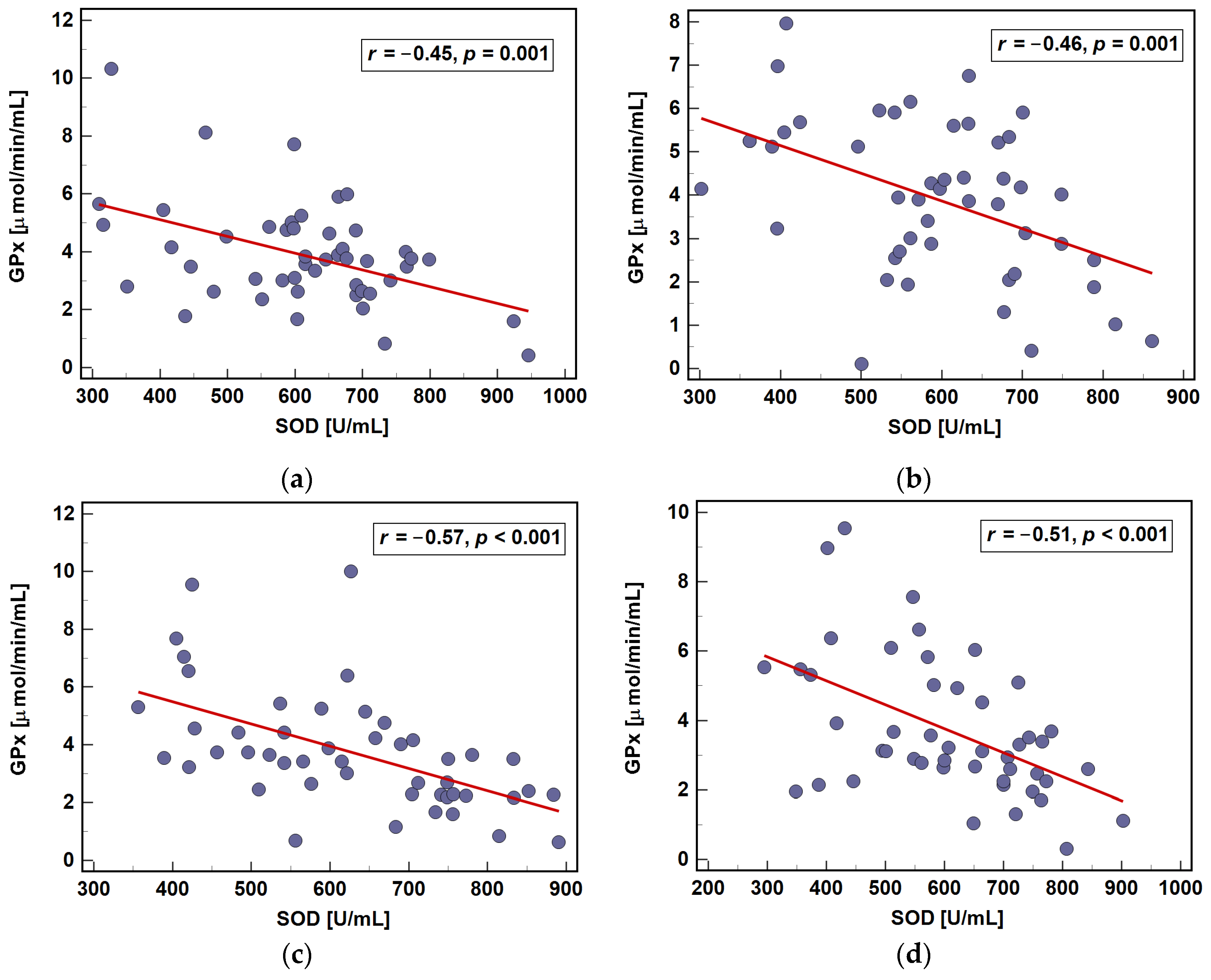
3.2.2. Erythrocyte Antioxidants: SOD and GPx
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Pellino, G.; Gallo, G.; Pallante, P.; Capasso, R.; De Stefano, A.; Maretto, I.; Malapelle, U.; Qiu, S.; Nikolaou, S.; Barina, A.; et al. Noninvasive Biomarkers of Colorectal Cancer: Role in Diagnosis and Personalised Treatment Perspectives. Gastroenterol. Res. Pract. 2018, 2018, 2397863. [Google Scholar] [CrossRef] [PubMed]
- Gothai, S.; Muniandy, K.; Gnanaraj, C.; Ibrahim, I.A.A.; Shahzad, N.; Al-Ghamdi, S.S.; Ayoub, N.; Veeraraghavan, V.P.; Kumar, S.S.; Esa, N.M.; et al. Pharmacological insights into antioxidants against colorectal cancer: A detailed review of the possible mechanisms. Biomed. Pharmacother. 2018, 107, 1514–1522. [Google Scholar] [CrossRef] [PubMed]
- Harris, I.S.; DeNicola, G.M. The complex interplay between antioxidants and ROS in cancer. Trends Cell Biol. 2020, 30, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Tian, T.; Wang, Z.; Zhang, J. Pathomechanisms of oxidative stress in inflammatory bowel disease and potential antioxidant therapies. Oxid. Med. Cell. Longev. 2017, 2017, 4535194. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, A.; Costa, M. Nutritionally mediated oxidative stress and inflammation. Oxid. Med. Cell. Longev. 2013, 2013, 610950. [Google Scholar] [CrossRef] [Green Version]
- Stevens, J.L.; Feelisch, M.; Martin, D.S. Perioperative oxidative stress: The unseen enemy. Anesth. Analg. 2019, 129, 1749–1760. [Google Scholar] [CrossRef]
- O’Leary, D.P.; Wang, J.H.; Cotter, T.G.; Redmond, H.P. Less stress, more success? Oncological implications of surgery-induced oxidative stress. Gut 2013, 62, 461–470. [Google Scholar] [CrossRef]
- Van Stijn, M.F.; Ligthart-Melis, G.C.; Boelens, P.G.; Scheffer, P.G.; Teerlink, T.; Twisk, J.W.; Houdijk, A.P.; van Leeuwen, P.A. Antioxidant enriched enteral nutrition and oxidative stress after major gastrointestinal tract surgery. World J. Gastroenterol. 2008, 14, 6960–6969. [Google Scholar] [CrossRef]
- Rosenfeldt, F.; Wilson, M.; Lee, G.; Kure, C.; Ou, R.; Braun, L.; de Haan, J. Oxidative stress in surgery in an ageing population: Pathophysiology and therapy. Exp. Gerontol. 2013, 48, 45–54. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [Green Version]
- Clinical Consensus Update in General Surgery. 2006. Available online: http://www.clinicalwebcasts.com/pdfs/GenSurg_WEB.pdf (accessed on 8 June 2021).
- Zawadzki, M.; Krzystek-Korpacka, M.; Gamian, A.; Witkiewicz, W. Comparison of inflammatory responses following robotic and open colorectal surgery: A prospective study. Int. J. Colorectal Dis. 2017, 32, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Mills, K.; le Cessie, S.; Noordam, R.; van Heemst, D. Ageing, age-related diseases and oxidative stress: What to do next? Ageing Res. Rev. 2020, 57, 100982. [Google Scholar] [CrossRef] [PubMed]
- Pisoschi, A.M.; Pop, A.; Iordache, F.; Stanca, L.; Predoi, G.; Serban, A.I. Oxidative stress mitigation by antioxidants—An overview on their chemistry and influences on health status. Eur. J. Med. Chem. 2021, 209, 112891. [Google Scholar] [CrossRef]
- Lopez-Candales, A.; Hernández Burgos, P.M.; Hernandez-Suarez, D.F.; Harris, D. Linking chronic inflammation with cardiovascular disease: From normal aging to the metabolic syndrome. J. Nat. Sci. 2017, 3, e341. [Google Scholar] [PubMed]
- Panis, C.; Herrera, A.C.; Victorino, V.J.; Campos, F.C.; Freitas, L.F.; De Rossi, T.; Colado Simão, A.N.; Cecchini, A.L.; Cecchini, R. Oxidative stress and hematological profiles of advanced breast cancer patients subjected to paclitaxel or doxorubicin chemotherapy. Breast Cancer Res. Treat. 2012, 133, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Macciò, A.; Madeddu, C.; Gramignano, G.; Mulas, C.; Tanca, L.; Cherchi, M.C.; Floris, C.; Omoto, I.; Barracca, A.; Ganz, T. The role of inflammation, iron, and nutritional status in cancer-related anemia: Results of a large, prospective, observational study. Haematologica 2015, 100, 124–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imam, M.U.; Zhang, S.; Ma, J.; Wang, H.; Wang, F. Antioxidants mediate both iron homeostasis and oxidative stress. Nutrients 2017, 9, 671. [Google Scholar] [CrossRef]
- Krzystek-Korpacka, M.; Matusiewicz, M.; Diakowska, D.; Grabowski, K.; Blachut, K.; Kustrzeba-Wojcicka, I.; Gamian, A. Even a mild anemia is related to tumor aggressiveness mediated by angiogenic factors. Exp. Oncol. 2009, 31, 52–56. [Google Scholar]
- Wiciński, M.; Liczner, G.; Cadelski, K.; Kołnierzak, T.; Nowaczewska, M.; Malinowski, B. Anemia of chronic diseases: Wider diagnostics-better treatment? Nutrients 2020, 12, 1784. [Google Scholar] [CrossRef]
- Zhang, M.L.; Wu, H.T.; Chen, W.J.; Xu, Y.; Ye, Q.Q.; Shen, J.X.; Liu, J. Involvement of glutathione peroxidases in the occurrence and development of breast cancers. J. Transl. Med. 2020, 18, 247. [Google Scholar] [CrossRef]
- Metta, S.; Basalingappa, D.R.; Uppala, S.; Mitta, G. Erythrocyte antioxidant defenses against cigarette smoking in ischemic heart disease. J. Clin. Diagn. Res. 2015, 9, BC08–BC11. [Google Scholar] [CrossRef] [PubMed]
- Gundu, H.R. Cardiometabolic diseases: A global perspective. J. Cardiol. Cardiovasc. Ther. 2018, 12, 555834. [Google Scholar] [CrossRef]
- Serra-Rexach, J.A.; Jimenez, A.B.; García-Alhambra, M.A.; Pla, R.; Vidán, M.; Rodríguez, P.; Ortiz, J.; García-Alfonso, P.; Martín, M. Differences in the therapeutic approach to colorectal cancer in young and elderly patients. Oncologist 2012, 17, 1277–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zawadzki, M.; Krzystek-Korpacka, M.; Rzaca, M.; Czarnecki, R.; Obuszko, Z.; Witkiewicz, W. Colorectal surgery in elderly population. Pol. J. Surg. 2018, 90, 17–22. [Google Scholar] [CrossRef]
- Kundović, S.A.; Rašić, D.; Popović, L.; Peraica, M.; Črnjar, K. Oxidative stress under general intravenous and inhalation anaesthesia. Arh. Hig. Rada Toksikol. 2020, 71, 169–177. [Google Scholar] [CrossRef]
- Braz, M.G.; Braz, L.G.; Braz, J.R.; Pierine, D.T.; Correa, C.R.; Ferreira, A.L.; Carvalho, L.R.; Yeum, K.J.; Salvadori, D.M. Comparison of oxidative stress in ASA physical status I patients scheduled for minimally invasive surgery under balanced or intravenous anesthesia. Minerva Anestesiol. 2013, 79, 1030–1038. [Google Scholar] [PubMed]
- Abdel-Salam, O.M.; Youness, E.R.; Mohammed, N.A.; Ibrahim, A.M. Effect of propofol and fentanyl on brain oxidative stress after systemic lipopolysaccharide injection in rats. React. Oxyg. Species 2021, 11, r1–r13. [Google Scholar] [CrossRef]
- Braz, M.G.; Braz, L.G.; Freire, C.M.M.; Lucio, L.M.C.; Braz, J.R.C.; Tang, G.; Salvadori, D.M.F.; Yeum, K.J.; Amornyotin, S. Isoflurane and propofol contribute to increasing the antioxidant status of patients during minor elective surgery a randomized clinical study. Medicine 2015, 94, e1266. [Google Scholar] [CrossRef]
- Tsuchiya, M.; Shiomoto, K.; Mizutani, K.; Fujioka, K.; Suehiro, K.; Yamada, T.; Sato, E.F.; Nishikawa, K. Reduction of oxidative stress a key for enhanced postoperative recovery with fewer complications in esophageal surgery patients: Randomized control trial to investigate therapeutic impact of anesthesia management and usefulness of simple blood test for prediction of high-risk patients. Medicine 2018, 97, e12845. [Google Scholar] [CrossRef]
- Zhang, X.; Li, J.; Yang, J.; Huang, Z. Fentanyl combined with butorphanol protects myocardial ischemia/reperfusion injury via κ-opioid receptor-mediated Nrf2-ARE signaling. Int. J. Clin. Exp. Med. 2016, 9, 2500–2506. [Google Scholar]
- Lee, Y.M.; Song, B.C.; Yeum, K.J. Impact of volatile anesthetics on oxidative stress and inflammation. BioMed Res. Int. 2015, 2015, 242709. [Google Scholar] [CrossRef]
- Jeong, J.S.; Suh, J.K.; Cho, E.S.; Kim, D.W.; Jeong, M.A. Antioxidant effect of muscle relaxants (vecuronium, rocuronium) on the rabbit abdominal aortic endothelial damage induced by reactive oxygen species. Korean J. Anesthesiol. 2013, 65, 552–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.J.; Ko, J.S.; Lee, S.H.; Kim, J.-Y.; Ok, S.H.; Bae, S.I.; Hwang, Y.; Park, K.-E.; Kim, J.W.; Sohn, J.-T. Sugammadex reverses vecuronium-mediated inhibition of reactive oxygen species production in endothelial cells and vascular smooth muscle cells. Int. J. Clin. Exp. Med. 2020, 13, 3483–3488. [Google Scholar]
- Erstad, B.L.; Barletta, J.F. Drug dosing in the critically ill obese patient—A focus on sedation, analgesia, and delirium. Crit. Care 2020, 24, 315. [Google Scholar] [CrossRef]
- Dinis-Oliveira, R.J. Metabolic profiles of propofol and fospropofol: Clinical and forensic interpretative aspects. BioMed Res. Int. 2018, 2018, 6852857. [Google Scholar] [CrossRef] [Green Version]
- Xu, S.F.; Hu, A.L.; Xie, L.; Liu, J.J.; Wu, Q.; Liu, J. Age-associated changes of cytochrome P450 and related phase-2 gene/proteins in livers of rats. Peer J. 2019, 7, e7429. [Google Scholar] [CrossRef]
- Tilstra, J.S.; Clauson, C.L.; Niedernhofer, L.J.; Robbins, P.D. NF-κB in aging and disease. Aging Dis. 2011, 2, 449–465. [Google Scholar] [PubMed]
- Ponce-Ruiz, N.; Murillo-González, F.E.; Rojas-García, A.E.; Mackness, M.; Bernal-Hernández, Y.Y.; Barrón-Vivanco, B.S.; González-Arias, C.A.; Medina-Díaz, I.M. Transcriptional regulation of human paraoxonase 1 by nuclear receptors. Chem. Biol. Interact. 2017, 268, 77–84. [Google Scholar] [CrossRef]
- Morgan, M.J.; Liu, Z.G. Crosstalk of reactive oxygen species and NF-κB signaling. Cell Res. 2011, 21, 103–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surinenaite, B.; Prasmickiene, G.; Milasiene, V.; Stratilatovas, E.; Didziapetriene, J. The influence of surgical treatment and red blood cell transfusion on changes in antioxidative and immune system parameters in colorectal cancer patients. Medicina 2009, 45, 785–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krzystek-Korpacka, M.; Zawadzki, M.; Lewandowska, P.; Szufnarowski, K.; Bednarz-Misa, I.; Jacyna, K.; Witkiewicz, W.; Gamian, A. Distinct chemokine dynamics in early postoperative period after open and robotic colorectal surgery. J. Clin. Med. 2019, 8, 879. [Google Scholar] [CrossRef] [Green Version]
- Krzystek-Korpacka, M.; Zawadzki, M.; Szufnarowski, K.; Bednarz-Misa, I.; Gorska, S.; Witkiewicz, W.; Gamian, A. The perioperative dynamics of IL-7 following robot-assisted and open colorectal surgery. Sci. Rep. 2018, 8, 9126. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Yu, W.; Lin, Z.; Chen, Q.; Shi, J.; Dong, Y.; Duan, K.; Bai, X.; Xu, L.; Li, J.; et al. Peritoneal air exposure elicits an intestinal inflammation resulting in postoperative ileus. Mediat. Inflamm. 2014, 2014, 924296. [Google Scholar] [CrossRef] [Green Version]
- Janaszewska, A.; Bartosz, G. Assay of total antioxidant capacity: Comparison of four methods as applied to human blood plasma. Scand. J. Clin. Lab. Investig. 2002, 62, 231–236. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Serum AOXs | Erythrocyte AOXs |
|---|---|---|
| N | 72 | 58 |
| Demographics and anthropometrics: | ||
| Sex, F/M (n) | 28/44 | 22/36 |
| Age (y), mean (95% CI) | 67.2 (64.7–69.7) | 65.8 (62.9–68.8) |
| BMI (kg/m2), mean (95% CI) | 26.15 (24.8–27.6) | 27.04 (25.8–28.3) |
| Health status: | ||
| ASA, 1/2/3 (n) | 15/46/11 | 12/36/10 |
| CCS, median (range) | 5 (2–8) | 4 (2–7) |
| WBC (×109/L), mean (95% CI) | 7.02 (6.51–7.52) | 6.88 (6.37–7.38) |
| HGB (g/dL), mean (95% CI) | 12.06 (11.59–12.53) | 12.27 (11.77–12.78) |
| IL-1β (pg/mL), mean (95% CI) | 1.96 (1.72–2.24) | 1.79 (1.52–2.1) |
| IL-6 (pg/mL), mean (95% CI) | 14.2 (12.06–16.72) | 14.3 (11.72–17.45) |
| TNFα (pg/mL), mean (95% CI) | 32.64 (29.01–36.71) | 30.5 (26.49–35.11) |
| Oncological features: | ||
| TNM, 0-I/II/III/IV (n) | 11/29/27/5 | 10/21/21/6 |
| T, Tis/1/2/3/4 (n) | 5/1/8/43/15 | 4/2/6/37/9 |
| N, 0/1/2 (n) | 38/18/16 | 31/13/14 |
| M, 0/1 (n) | 67/5 | 52/6 |
| G, 1/2/3/4/x (n) | 12/48/10/1/1 | 9/39/7/3 |
| Characteristics | Serum AOXs | Erythrocyte AOXs |
|---|---|---|
| N | 59 | 47 |
| Demographics: | ||
| Sex, F/M (n) | 20/39 | 16/31 |
| Age (y), mean (95% CI) | 67.1 (64.2–70.1) | 65.0 (61.7–68.2) |
| BMI [kg/m2], mean (95% CI) | 26.0 (24.7–27.37) | 26.74 (25.42–28.06) |
| ASA, 1/2/3 (n) | 11/39/9 | 13/29/5 |
| CCS, median (range) | 5 (2–8) | 4 (2–7) |
| Oncological features: | ||
| TNM, 0-I/II/III/IV (n) | 9/26/19/5 | 8/18/15/6 |
| T, Tis/1/2/3/4 (n) | 4/1/6/35/13 | 3/1/6/29/8 |
| N, 0/1/2 (n) | 33/13/13 | 26/10/11 |
| M, 0/1 (n) | 54/5 | 41/6 |
| G, 1/2/3/4/x (n) | 11/37/9/1/1 | 6/32/6/3 |
| Surgical features: | ||
| Type, open/robotic (n) | 29/30 | 25/22 |
| Procedure, APR/LH/LAR/RH/SR (n) | 2/4/22/18/13 | 1/3/21/11/11 |
| Length of surgery (min), median (range) | 165 (50–360) | 165 (150–203) |
| EBL (mL), median (range) | 100 (30–300) | 125 (100–200) |
| Harvested LN, median (range) | 14 (3–43) | 14 (3–43) |
| CDC (≥3), no/yes (n) | 56/3 | 44/3 |
| SSI, no/yes (n) | 47/12 | 38/9 |
| RoBF (≥5 days), no/yes (n) | 38/21 | 29/18 |
| LoHS (days), median (range) | 6 (4–20) | 6 (3–20) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krzystek-Korpacka, M.; Mierzchała-Pasierb, M.; Zawadzki, M.; Diakowska, D.; Witkiewicz, W. Serum and Erythrocyte Antioxidant Defense in Colorectal Cancer Patients during Early Postoperative Period: Potential Modifiers and Impact on Clinical Outcomes. Antioxidants 2021, 10, 999. https://doi.org/10.3390/antiox10070999
Krzystek-Korpacka M, Mierzchała-Pasierb M, Zawadzki M, Diakowska D, Witkiewicz W. Serum and Erythrocyte Antioxidant Defense in Colorectal Cancer Patients during Early Postoperative Period: Potential Modifiers and Impact on Clinical Outcomes. Antioxidants. 2021; 10(7):999. https://doi.org/10.3390/antiox10070999
Chicago/Turabian StyleKrzystek-Korpacka, Małgorzata, Magdalena Mierzchała-Pasierb, Marek Zawadzki, Dorota Diakowska, and Wojciech Witkiewicz. 2021. "Serum and Erythrocyte Antioxidant Defense in Colorectal Cancer Patients during Early Postoperative Period: Potential Modifiers and Impact on Clinical Outcomes" Antioxidants 10, no. 7: 999. https://doi.org/10.3390/antiox10070999