Distinct Chemokine Dynamics in Early Postoperative Period after Open and Robotic Colorectal Surgery

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Patients
2.2. Ethical Considerations
2.3. Analytical Methods
2.4. Statistical Analysis
3. Results
3.1. Chemokine Dynamics and Type of Surgery (Open vs. Robotic)
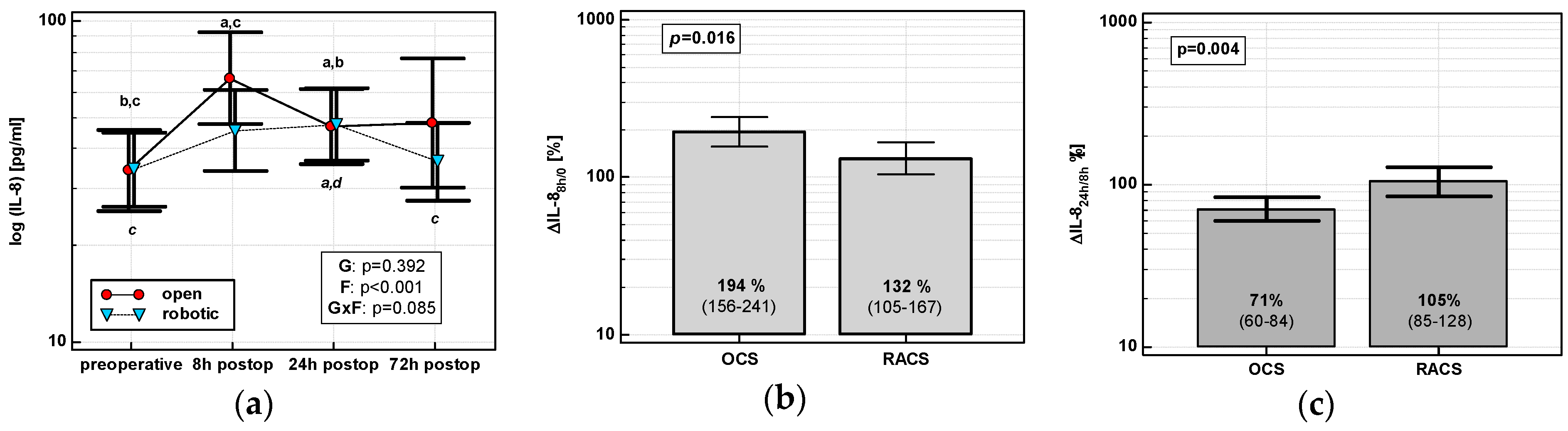
3.1.1. Interleukin-8 (IL-8/CXCL8)
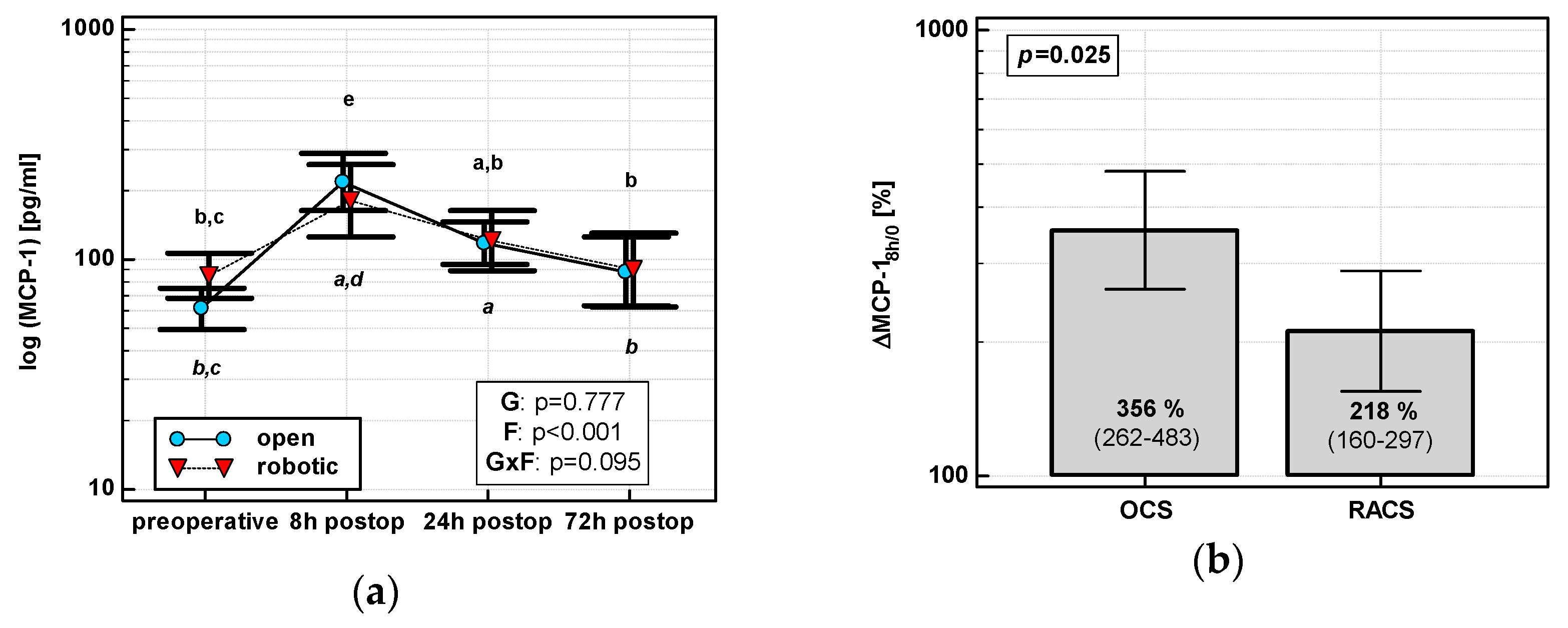
3.1.2. Monocyte Chemoattractant Protein 1 (MCP-1/CCL2)
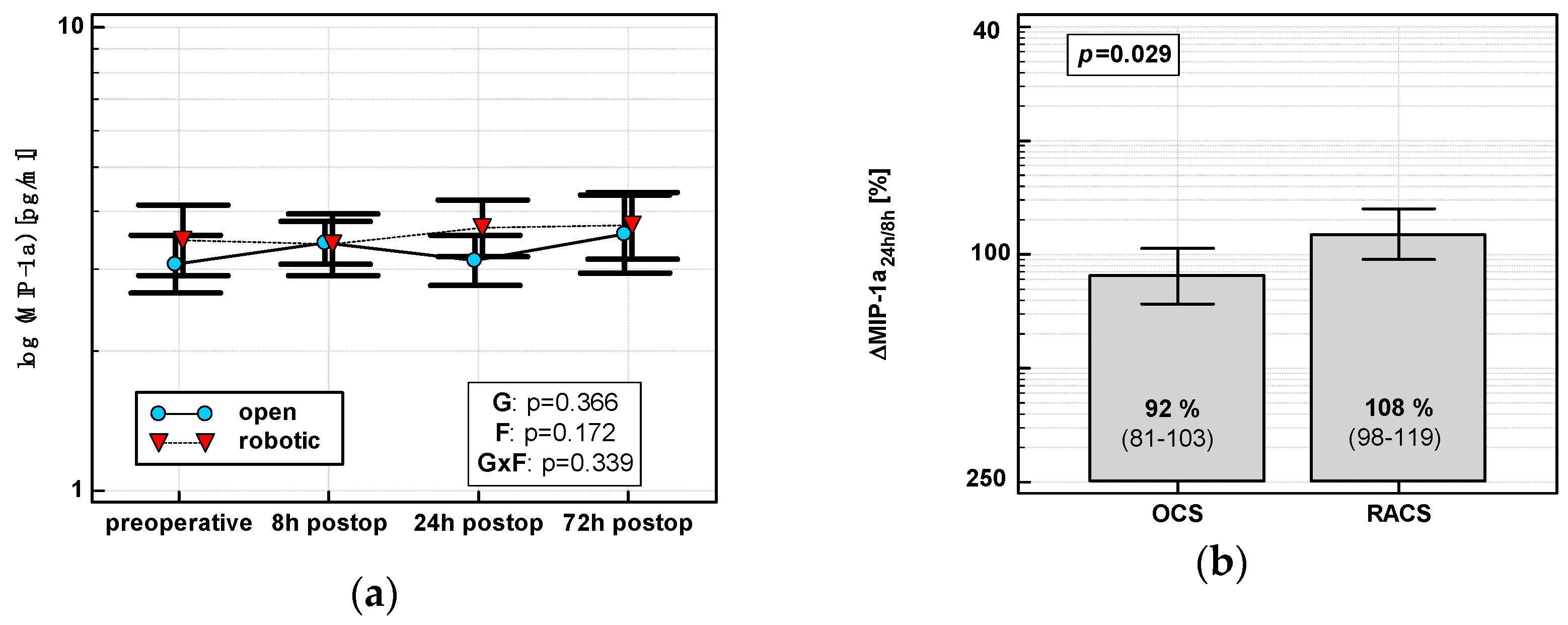
3.1.3. Macrophage Inflammatory Protein 1α (MIP-1α/CCL3)
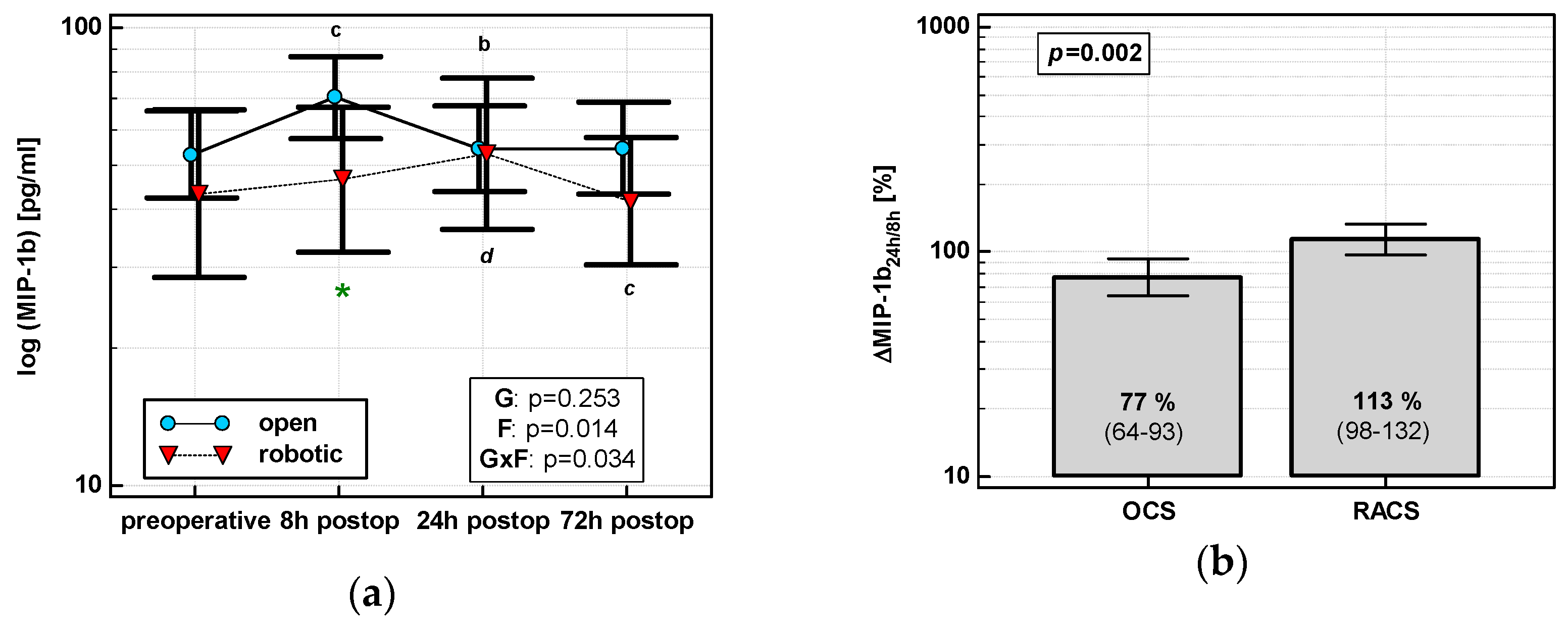
3.1.4. Macrophage Inflammatory Protein 1β (MIP-1β/CCL4)
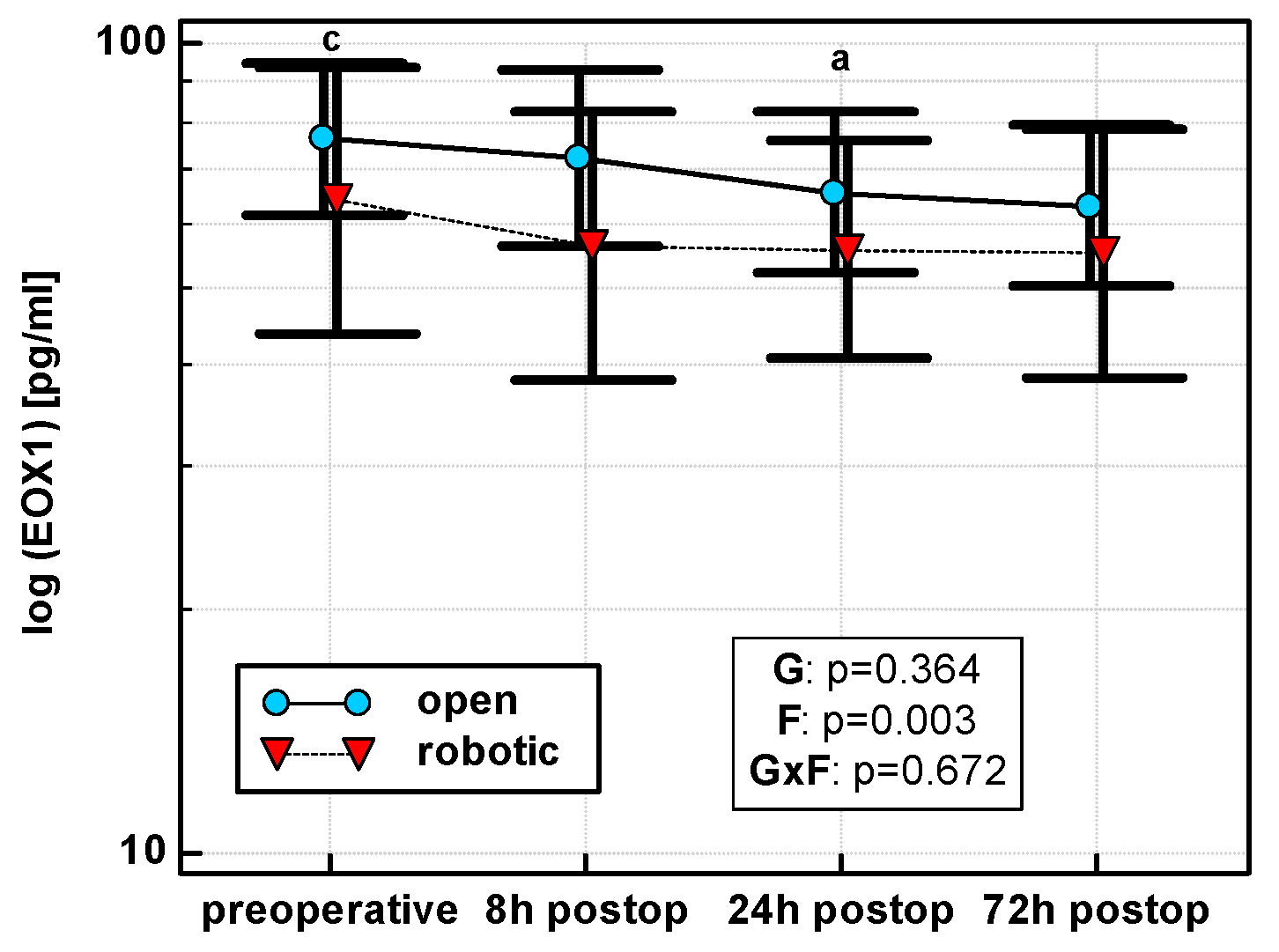
3.1.5. Eotaxin 1 (EOX1/CCL11)
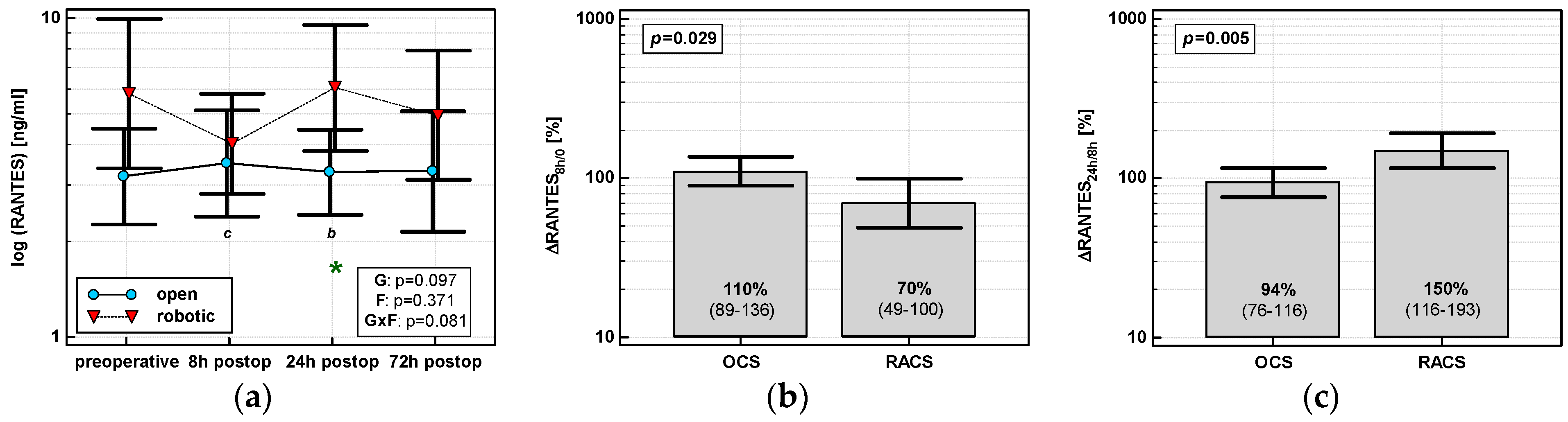
3.1.6. Regulation on Activation, Normal T Cell Expression and Secretion (RANTES/CCL5)
3.2. Impact of Other Clinical Parameters on Chemokine Dynamics
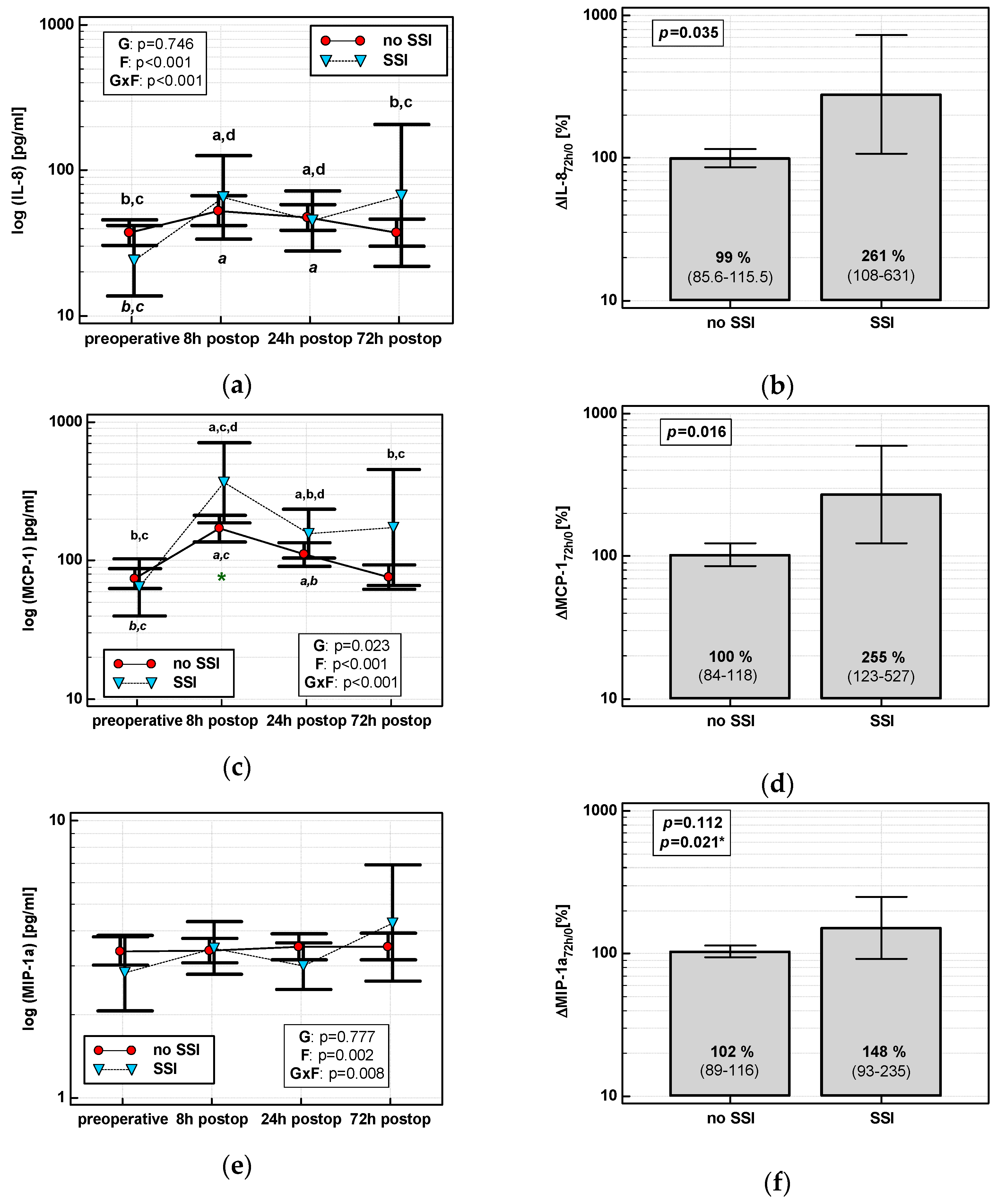
3.2.1. Interleukin-8 (IL-8/CXCL8)
3.2.2. Monocyte Chemoattractant Protein 1 (MCP-1/CCL2)
3.2.3. Macrophage Inflammatory Protein 1α (MIP-1α/CCL3)
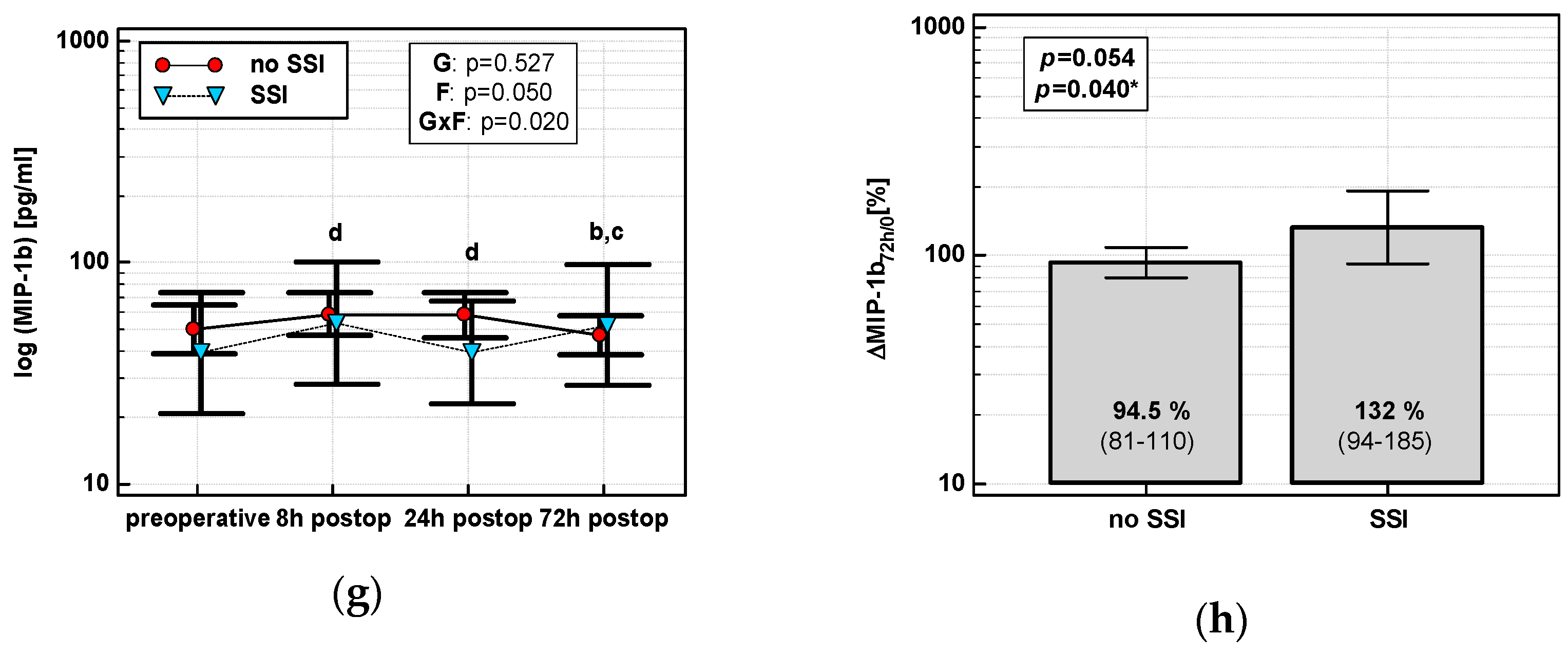
3.2.4. Macrophage Inflammatory Protein 1β (MIP-1β/CCL4)
3.2.5. Eotaxin 1 (EOX1/CCL11)
3.2.6. Regulation on Activation, Normal T Cell Expression and Secretion (RANTES/CCL5)
3.3. Predictors of Initial Chemokine Up- or Down-Regulation
3.3.1. Interleukin-8 (IL-8)
3.3.2. Monocyte Chemoattractant Protein 1 (MCP-1)
3.3.3. Macrophage Inflammatory Protein 1α (MIP-1α)
3.3.4. Macrophage Inflammatory Protein 1β (MIP-1β)
3.3.5. Eotaxin 1 (EOX1/CCL11)
3.3.6. Regulation on Activation, Normal T Cell Expression and Secretion (RANTES/CCL5)
3.4. Chemokines and Clinical Outcomes
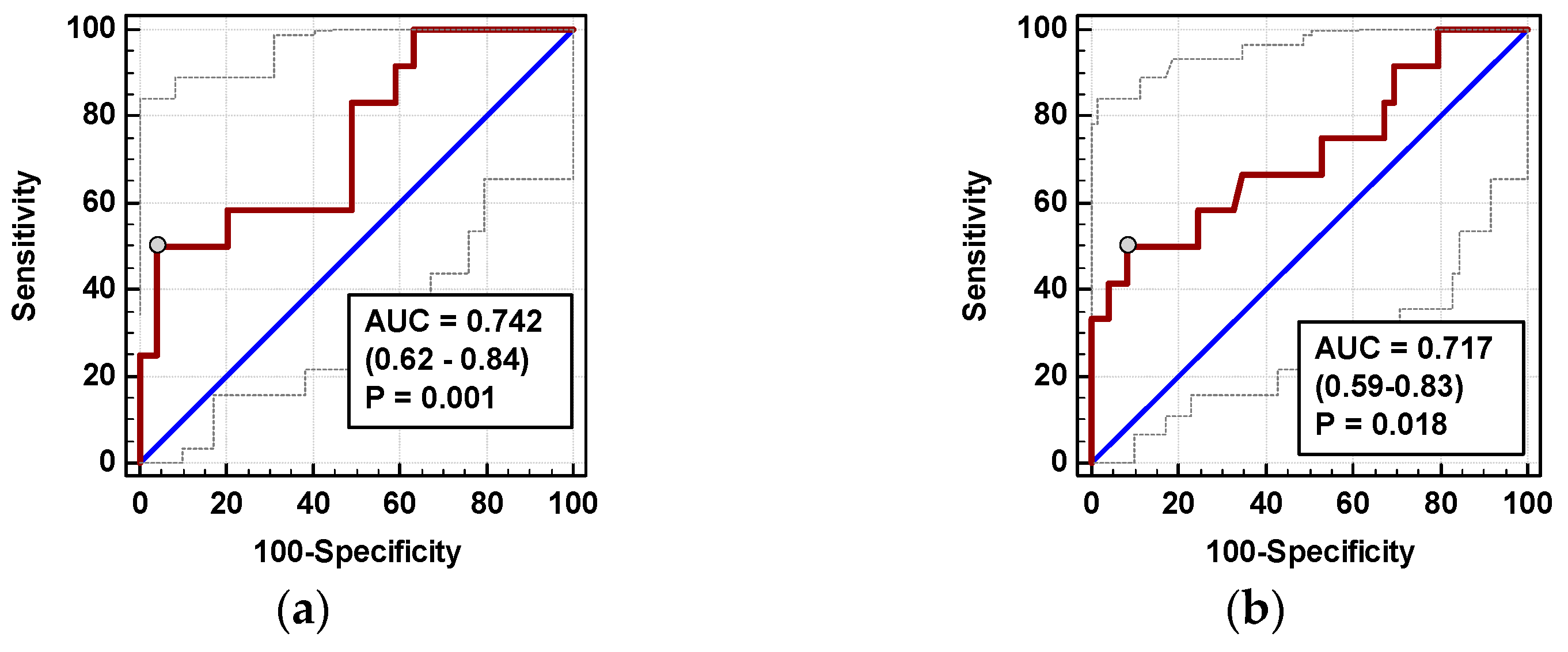
3.4.1. Surgical Site Infections (SSIs)
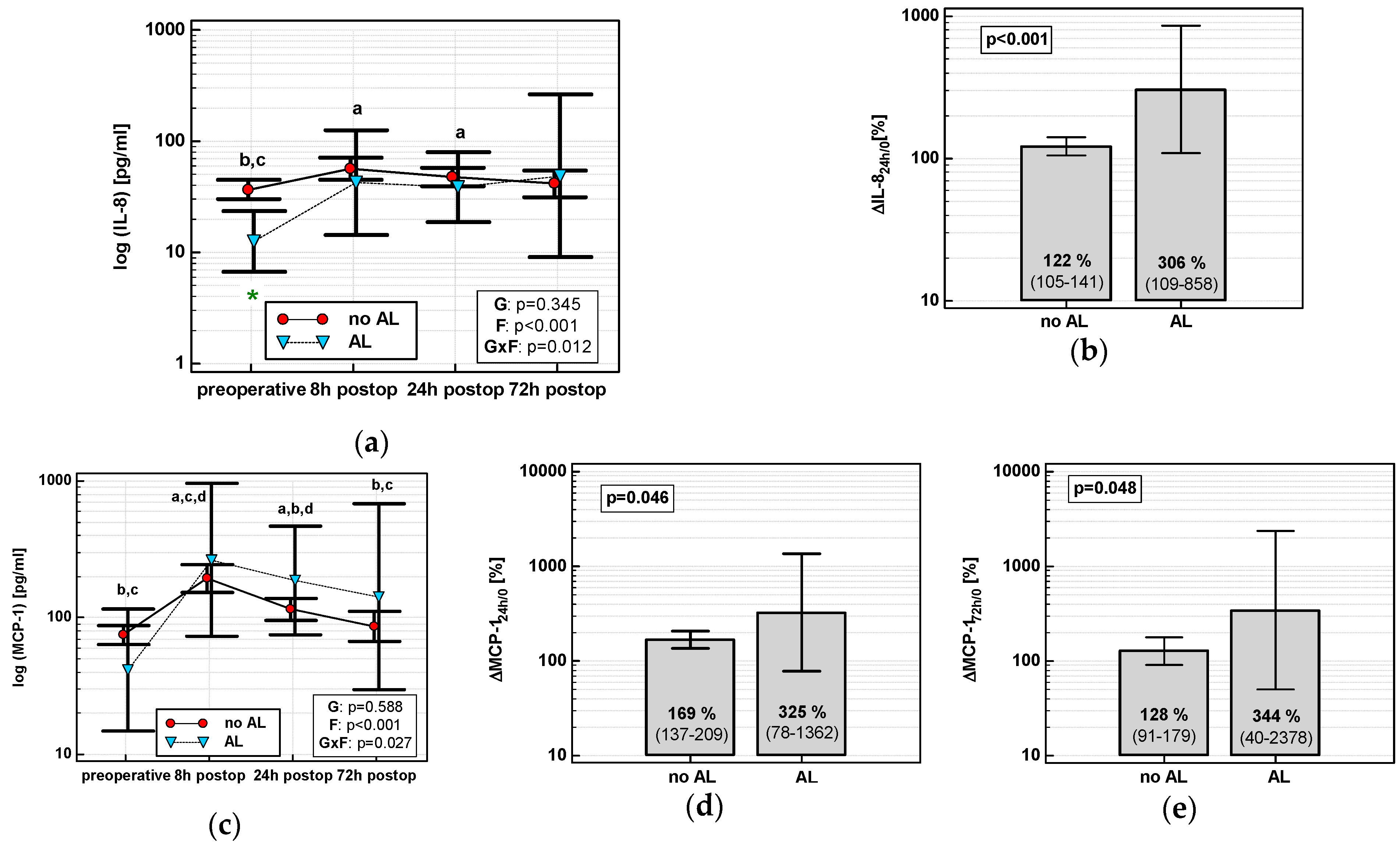
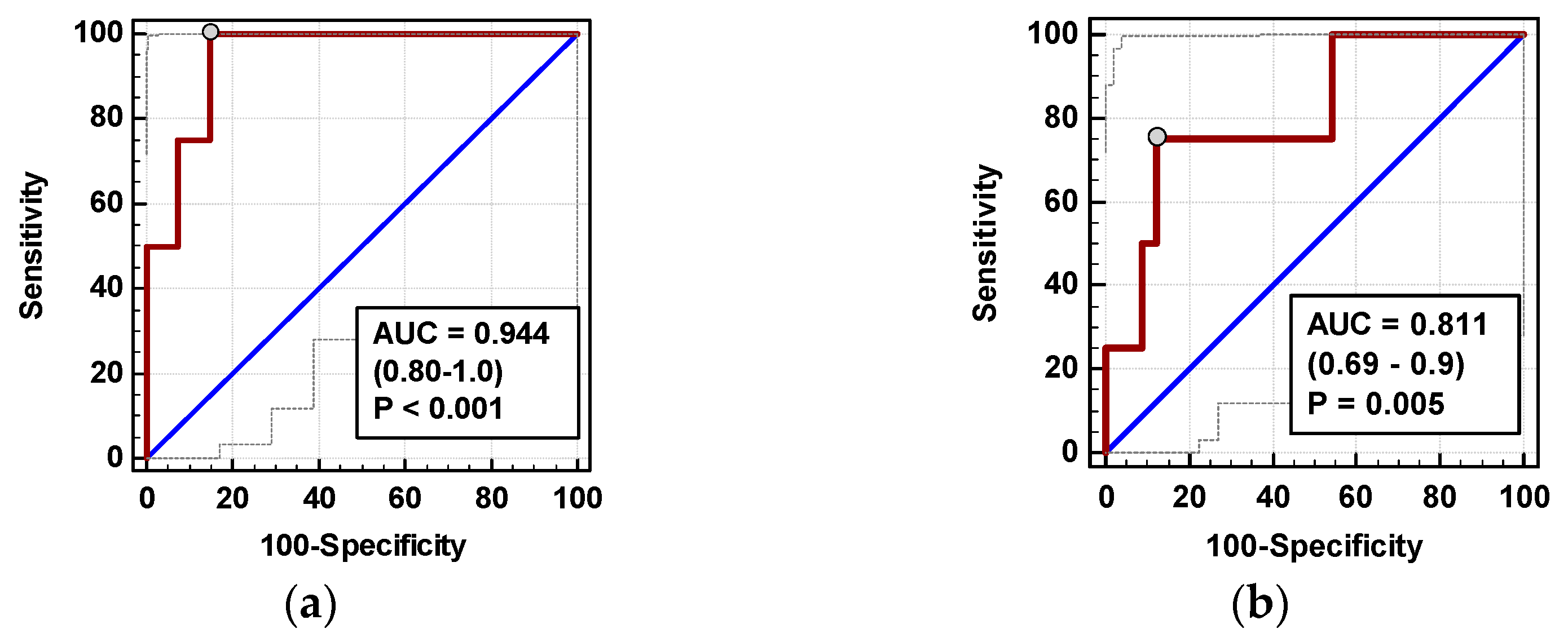
3.4.2. Anastomotic Leak (AL)
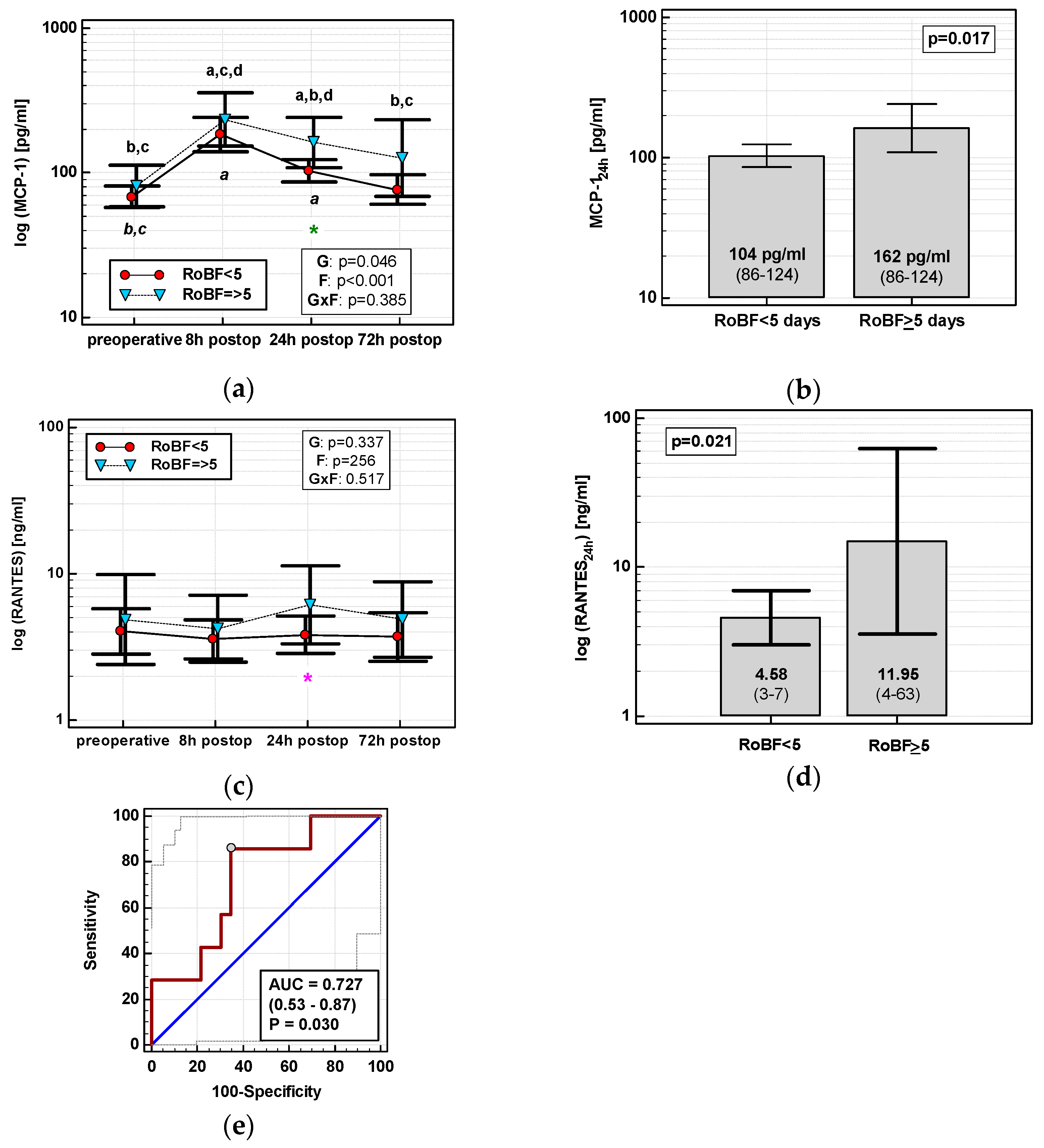
3.4.3. Restoration of Bowel Function (RoBF)
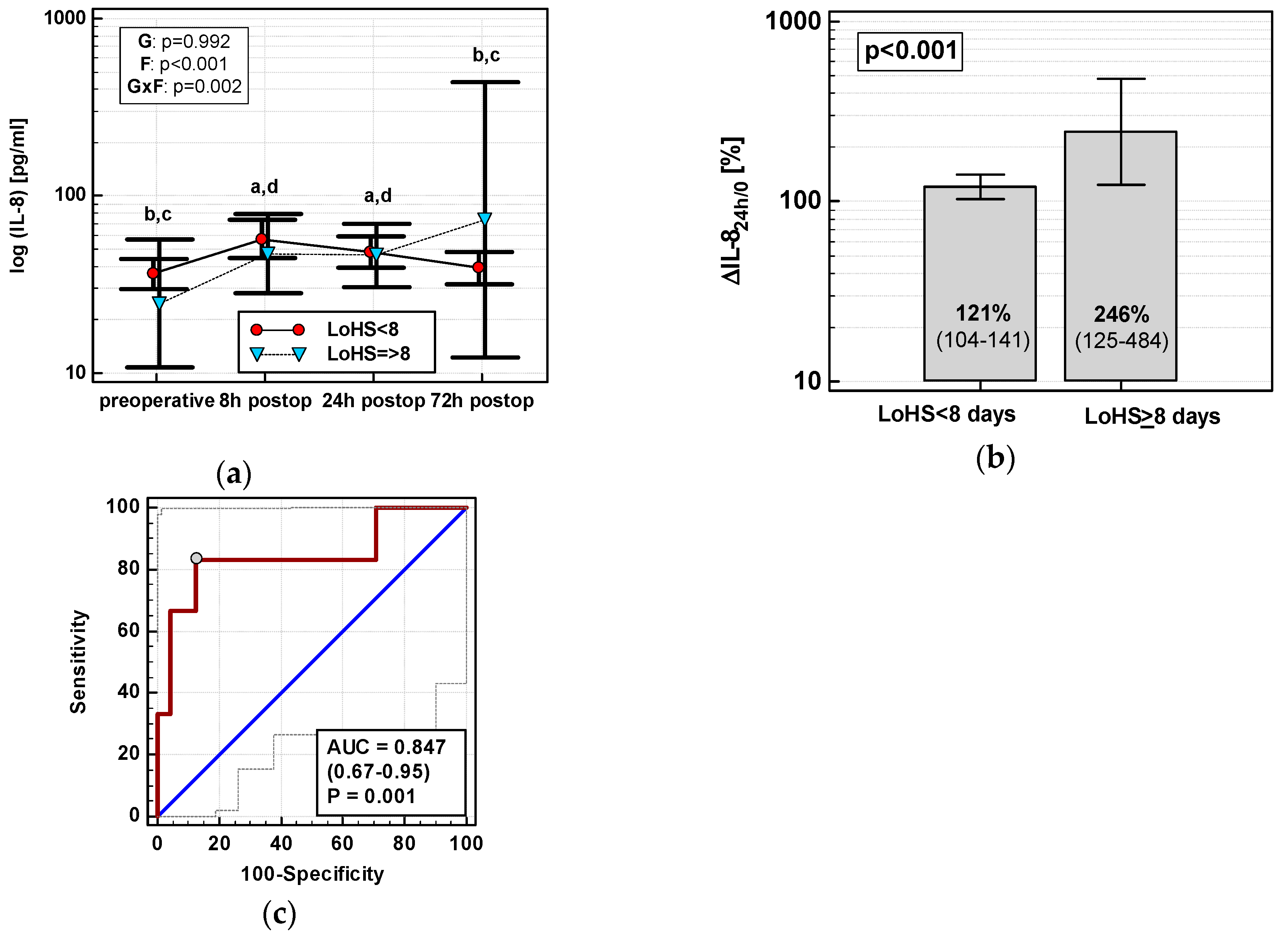
3.4.4. Length of Hospital Stay (LoHS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Scholl, R.; Bekker, A.; Babu, R. Neuroendocrine and Immune Responses to Surgery. Internet J. Anesthesiol. 2012, 30, 3. [Google Scholar]
- Forget, P.; Simonet, O.; De Kock, M. Cancer surgery induces inflammation, immunosuppression and neoangiogenesis, but is it influenced by analgesics? F1000Research 2013, 2, 102. [Google Scholar] [CrossRef] [PubMed]
- Martins-Green, M.; Petreaca, M.; Wang, L. Chemokines and their receptors are key players in the orchestra that regulates wound healing. Adv. Wound Care 2013, 2, 327–347. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications. A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Mangram, A.J.; Horan, T.C.; Pearson, M.L.; Silver, L.C.; Jarvis, W.R. Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infect. Control Hosp. Epidemiol. 1999, 20, 250–278. [Google Scholar] [CrossRef] [PubMed]
- Zawadzki, M.; Krzystek-Korpacka, M.; Gamian, A.; Witkiewicz, W. Comparison of inflammatory responses following robotic and open colorectal surgery: A prospective study. Int. J. Colorectal Dis. 2017, 32, 399–407. [Google Scholar] [CrossRef]
- Krzystek-Korpacka, M.; Zawadzki, M.; Szufnarowski, K.; Bednarz-Misa, I.; Gorska, S.; Witkiewicz, W.; Gamian, A. The perioperative dynamics of IL-7 following robot-assisted and open colorectal surgery. Sci. Rep. 2018, 8, 9126. [Google Scholar] [CrossRef]
- Biffi, R.; Luca, F.; Bianchi, P.P.; Cenciarelli, S.; Petz, W.; Monsellato, I.; Valvo, M.; Cossu, M.L.; Ghezzi, T.L.; Shmaissany, K. Dealing with robot-assisted surgery for rectal cancer: Current status and perspectives. World J. Gastroenterol. 2016, 22, 546–556. [Google Scholar] [CrossRef]
- Song, J.B.; Vemana, G.; Mobley, J.M.; Bhayani, S.B. The second “time-out”: A surgical safety checklist for lengthy robotic surgeries. Patient Saf. Surg. 2013, 7, 19. [Google Scholar] [CrossRef]
- Shibata, J.; Ishihara, S.; Tada, N.; Kawai, K.; Tsuno, N.H.; Yamaguchi, H.; Sunami, E.; Kitayama, J.; Watanabe, T. Surgical stress response after colorectal resection: A comparison of robotic, laparoscopic, and open surgery. Tech. Coloproctol. 2015, 19, 275–280. [Google Scholar] [CrossRef]
- Wang, D.; DuBois, R.N.; Richmond, A. The role of chemokines in intestinal inflammation and cancer. Curr. Opin. Pharmacol. 2009, 9, 688–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferri, M.; Rossi Del Monte, S.; Salerno, G.; Bocchetti, T.; Angeletti, S.; Malisan, F.; Cardelli, P.; Ziparo, V.; Torrisi, M.R.; Visco, V. Recovery of immunological homeostasis positively correlates both with early stages of right-colorectal cancer and laparoscopic surgery. PLoS ONE 2013, 8, e74455. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhou, X.; Huang, Z.; Zhang, H.; Zhang, L.; Shang, C.; Chen, Y. Laparoscopic surgery minimizes the release of circulating tumor cells compared to open surgery for hepatocellular carcinoma. Surg. Endosc. 2015, 29, 3146–3153. [Google Scholar] [CrossRef] [PubMed]
- Veenhof, A.A.F.A.; Sietses, C.; von Blomberg, B.M.E.; van Hoogstraten, I.M.; vd Pas, M.H.; Meijerink, W.J.; vd Peet, D.L.; vd Tol, M.P.; Bonjer, H.J.; Cuesta, M.A. The surgical stress response and postoperative immune function after laparoscopic or conventional total mesorectal excision in rectal cancer: A randomized trial. Int. J. Colorectal Dis. 2011, 26, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Allen, T.C.; Kurdowska, A. Interleukin 8 and acute lung injury. Arch. Pathol. Lab. Med. 2014, 138, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Luckey, A.; Livingston, E.; Taché, Y. Mechanisms and treatment of postoperative ileus. Arch. Surg. 2003, 138, 206–214. [Google Scholar] [CrossRef]
- Spiller, R.C. Mechanisms of postoperative intestinal motor dysfunction. Curr. Opin. Gastroenterol. 2003, 19, 103–105. [Google Scholar] [CrossRef]
- Zawadzki, M.; Krzystek-Korpacka, M.; Rząca, M.; Czarnecki, R.; Obuszko, Z.; Witkiewicz, W. Colorectal surgery in elderly population. Pol. Przegl. Chir. 2018, 90, 29–34. [Google Scholar] [CrossRef]
- Bokhari, M.B.; Patel, C.B.; Ramos-Valadez, D.I.; Ragupathi, M.; Haas, E.M. Learning curve for robotic-assisted laparoscopic colorectal surgery. Surg. Endosc. 2011, 25, 855–860. [Google Scholar] [CrossRef]
- Kim, H.J.; Choi, G.S.; Park, J.S.; Park, S.Y. Multidimensional analysis of the learning curve for robotic total mesorectal excision for rectal cancer: Lessons from a single surgeon’s experience. Dis. Colon Rectum 2014, 57, 1066–1074. [Google Scholar] [CrossRef]
- Colwell, J.C. The role of obesity in the patient undergoing colorectal surgery and fecal diversion: A review of the literature. Ostomy Wound Manag. 2014, 60, 24–28. [Google Scholar]
- Pang, Q.Y.; An, R.; Liu, H.L. Perioperative transfusion and the prognosis of colorectal cancer surgery: A systematic review and meta-analysis. World J. Surg. Oncol. 2019, 17, 7. [Google Scholar] [CrossRef] [PubMed]
- Waugh, D.J.J.; Wilson, C. The interleukin-8 pathway in cancer. Clin. Cancer Res. 2008, 14, 6735–6741. [Google Scholar] [CrossRef] [PubMed]
- Yadav, A.; Saini, V.; Arora, S. MCP-1: Chemoattractant with a role beyond immunity: A review. Clin. Chim. Acta 2010, 411, 1570–1579. [Google Scholar] [CrossRef] [PubMed]
- Arendt, B.K.; Velazquez-Dones, A.; Tschumper, R.C.; Howell, K.G.; Ansell, S.M.; Witzig, T.E.; Jelinek, D.F. Interleukin 6 induces monocyte chemoattractant protein-1 expression in myeloma cells. Leukemia 2002, 16, 2142–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okamura, S.; Fujiwara, H.; Yoneda, M.; Furutani, A.; Todo, M.; Ikai, A.; Tada, H.; Okamura, H.; Umehara, S.; Shiozaki, A.; et al. Overexpression of IL-6 by gene transfer stimulates IL-8-mediated invasiveness of KYSE170 esophageal carcinoma cells. Anticancer Res. 2013, 33, 1483–1489. [Google Scholar] [PubMed]
- Zawadzki, M.; Krzystek-Korpacka, M.; Rząca, M.; Czarnecki, R.; Obuszko, Z.; Witkiewicz, W. Introduction of robotic surgery into a community hospital setting: A prospective comparison of robotic and open colorectal resection for cancer. Dig. Surg. 2017, 34, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Krzystek-Korpacka, M.; Diakowska, D.; Kapturkiewicz, B.; Bębenek, M.; Gamian, A. Profiles of circulating inflammatory cytokines in colorectal cancer (CRC), high cancer risk conditions, and health are distinct. Possible implications for CRC screening and surveillance. Cancer Lett. 2013, 337, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Krzystek-Korpacka, M.; Zawadzki, M.; Kapturkiewicz, B.; Lewandowska, P.; Bednarz-Misa, I.; Gorska, S.; Witkiewicz, W.; Gamian, A. Subsite heterogeneity in the profiles of circulating cytokines in colorectal cancer. Cytokine 2018, 110, 435–441. [Google Scholar] [CrossRef]
- Kimura, F.; Shimizu, H.; Yoshidome, H.; Ohtsuka, M.; Kato, A.; Yoshitomi, H.; Nozawa, S.; Furukawa, K.; Mitsuhashi, N.; Sawada, S.; et al. Increased plasma levels of IL-6 and IL-8 are associated with surgical site infection after pancreaticoduodenectomy. Pancreas 2006, 32, 178–185. [Google Scholar] [CrossRef]
- Kamboj, M.; Childers, T.; Sugalski, J.; Antonelli, D.; Bingener-Casey, J.; Cannon, J.; Cluff, K.; Davis, K.A.; Dellinger, E.P.; Dowdy, S.C.; et al. Risk of surgical site infection (SSI) following colorectal resection is higher in patients with disseminated cancer: An NCCN Member Cohort Study. Infect. Control Hosp. Epidemiol. 2018, 39, 555–562. [Google Scholar] [CrossRef]
- Carvalho, R.L.R.; Campos, C.C.; Franco, L.M.C.; Rocha, A.M.; Ercole, F.F. Incidence and risk factors for surgical site infection in general surgeries. Rev. Lat. Am. Enfermagem. 2017, 25, e2848. [Google Scholar] [CrossRef]
- Park, J.S.; Huh, J.W.; Park, Y.A.; Cho, Y.B.; Yun, S.H.; Kim, H.C.; Lee, W.Y. Risk factors of anastomotic leakage and long-term survival after colorectal surgery. Medicine 2016, 95, e2890. [Google Scholar] [CrossRef] [PubMed]
- Vasiliu, E.C.; Zarnescu, N.O.; Costea, R.; Neagu, S. Review of risk factors for anastomotic leakage in colorectal surgery. Chirurgia 2015, 110, 319–326. [Google Scholar] [PubMed]
- Zawadzki, M.; Krzystek-Korpacka, M.; Gamian, A.; Witkiewicz, W. Serum cytokines in early prediction of anastomotic leakage following low anterior resection. Wideochir. Inne Tech. Maloinwazyjne 2018, 13, 33–43. [Google Scholar] [CrossRef]
- Sciuto, A.; Merola, G.; De Palma, G.D.; Sodo, M.; Pirozzi, F.; Bracale, U.M.; Bracale, U. Predictive factors for anastomotic leakage after laparoscopic colorectal surgery. World J. Gastroenterol. 2018, 24, 2247–2260. [Google Scholar] [CrossRef]
- Kelly, M.; Sharp, L.; Dwane, F.; Kelleher, T.; Comber, H. Factors predicting hospital length-of-stay and readmission after colorectal resection: A population-based study of elective and emergency admissions. BMC Health Serv. Res. 2012, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.J.; Pericleous, A.; Downey, C.; Jayne, D.G. Postoperative ileus following major colorectal surgery. Br. J. Surg. 2018, 105, 797–810. [Google Scholar] [CrossRef] [PubMed]
- Turler, A.; Schwarz, N.T.; Turler, E.; Kalff, J.C.; Bauer, A.J. MCP-1 causes leukocyte recruitment and subsequently endotoxemic ileus in rat. Am. J. Physiol. Gastrointest. Liver Physiol. 2002, 282, G145–G155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lluis, N.; Biondo, S. Prolonged postoperative ileus after colorectal surgery: Still an unresolved problem. Ann. Laparosc. Endosc. Surg. 2018, 3, 15. [Google Scholar] [CrossRef]
- Peters, E.G.; De Jonge, W.J.; Smeets, B.J.J.; Luyer, M.D.P. The contribution of mast cells to postoperative ileus in experimental and clinical studies. Neurogastroenterol. Motil. 2015, 27, 743–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattoli, S.; Ackerman, V.; Vittori, E.; Marini, M. Mast cell chemotactic activity of RANTES. Biochem. Biophys. Res. Commun. 1995, 209, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, M.F.; Huitink, J.M.; Cata, J.P. Perioperative clinical interventions that modify the immune response in cancer patients. Open J. Anesthesiol. 2013, 3, 133–139. [Google Scholar] [CrossRef]
- Deshmane, S.L.; Kremlev, S.; Amini, S.; Sawaya, B.E. Monocyte chemoattractant protein-1 (MCP-1): An overview. J. Interferon Cytokine Res. 2009, 29, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.; Dalgleish, A.G.; Kumar, D. Immune suppression and colorectal cancer. Aliment. Pharmacol. Ther. 2006, 24, 1163–1177. [Google Scholar] [CrossRef] [PubMed]
- Larrubia, J.R.; Benito-Martínez, S.; Calvino, M.; Sanz-de-Villalobos, E.; Parra-Cid, T. Role of chemokines and their receptors in viral persistence and liver damage during chronic hepatitis C virus infection. World J. Gastroenterol. 2008, 14, 7149–7159. [Google Scholar] [CrossRef] [PubMed]
- Lindell, D.M.; Standiford, T.J.; Mancuso, P.; Leshen, Z.J.; Huffnagle, G.B. Macrophage inflammatory protein 1alpha/CCL3 is required for clearance of an acute Klebsiella pneumoniae pulmonary infection. Infect. Immun. 2001, 69, 6364–6369. [Google Scholar] [CrossRef]
- Schootman, M.; Hendren, S.; Loux, T.; Ratnapradipa, K.; Eberth, J.M.; Davidson, N.O. Differences in effectiveness and use of robotic surgery in patients undergoing minimally invasive colectomy. J. Gastrointest. Surg. 2017, 21, 1296–1303. [Google Scholar] [CrossRef]
- Dolejs, S.C.; Waters, J.A.; Ceppa, E.P.; Zarzaur, B.L. Laparoscopic versus robotic colectomy: A national surgical quality improvement project analysis. Surg. Endosc. 2017, 31, 2387–2396. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Open Surgery | Robotic Surgery | p Value |
|---|---|---|---|
| Size, n | 31 | 30 | - |
| Patient-related: | |||
| Sex distribution (F/M) | 14/17 | 7/23 | 0.127 |
| Age (years), median (95% CI) | 68 (65–76) | 67 (61.5–71.8) | 0.302 |
| Patients ≥ 75 years, n | 12/19 | 8/22 | 0.416 |
| BMI 1 (kg/m 2), mean (95% CI) | 26.8 (25.1–28.5) | 26.6 (24.8–28.4) | 0.852 |
| Overweight/obese patients 1, n | 10/20 | 13/16 | 0.430 |
| ASA (1/2/3), n | 6/20/5 | 5/20/5 | 0.830 |
| Charlson Comorbidity Score, median (95% CI) | 5 (4–5) | 4.5 (4–5.8) | 0.988 |
| HGB (g/dL), mean (95% CI) | 11.9 (11.2–12.6) | 12.3 (11.6–13) | 0.456 |
| Anemia 2 (no/yes), n | 12/19 | 9/21 | 0.592 |
| WBC (×10 3/mm 3), mean (95% CI) | 7.01 (6.23–7.78) | 7.26 (6.47–8.04) | 0.645 |
| NEU (×10 3/mm 3), mean (95% CI) | 4.72 (4.1–5.34) | 4.9 (4.3–5.5) | 0.679 |
| LYM (×10 3/mm 3), mean (95% CI) | 1.5 (1.32–1.68) | 1.45 (1.19–1.72) | 0.758 |
| Cancer-related: | |||
| Stage distribution (0/I/II/III/IV), n | 2/2/15/9/3 | 2/3/11/12/2 | 0.839 |
| Stage T distribution (Tis/T1/T2/T3/T4), n | 2/1/1/20/7 | 2/0/5/16/7 | 0.393 |
| Stage N distribution (N0/N1/N2), n | 19/4/8 | 16/8/6 | 0.395 |
| Stage M distribution (M0/M1), n | 28/3 | 28/2 | 0.970 |
| Grade (G1/G2/G3/G4), n | 3/21/4/1 | 5/18/5/0 | 0.519 |
| Tumor location (LC/RC/RE), n | 11/6/14 | 7/12/11 | 0.199 |
| Surgery-related: | |||
| Surgical procedure (APR/LAR/RH/LH/SR), n | 1/13/6/1/10 | 1/10/12/3/4 | 0.203 |
| Length of surgery (min), median (95% CI) | 125 (115–150) | 205 (191–240) | <0.001 |
| Length of surgery 3 (≤165 min/>165 min), n | 26/5 | 6/24 | <0.001 |
| Total nodes resected, mean (95% CI) | 15.7 (13.5–17.9) | 14.8 (12.4–17.2) | 0.568 |
| Total nodes resected 3 (<14/≥14), n | 10/21 | 16/14 | 0.124 |
| Estimated blood loss (mL), median (95% CI) | 200 (150–200) | 50 (50–100) | <0.0001 |
| Estimated blood loss 3 (≤100 mL/>100 mL), n | 6/25 | 25/6 | <0.001 |
| Transfusions, n (%) | 5 (16.1%) | 2 (6.7%) | 0.425 |
| Frequency of stomas, n (%) | 5 (16.1%) | 5 (16.7%) | 1.0 |
| Restoration of bowel function (<5/≥5 day), n | 19/12 | 23/7 | 0.270 |
| Length of hospital stay, days (range) | 7.6 (4–20) | 5.8 (4–8) | 0.020 |
| Clavien-Dindo score (≤2/3/4/5), n | 26/3/2/0 | 29/1/0/0 | 0.207 |
| Complications 4, n (%): | 4 (12.9%) | 0 | 0.113 |
| Anastomotic leak (AL), n | 27/4 | 30/0 | 0.113 |
| Surgical site infection, n (%) | 10 (32.3%) | 2 (6.7%) | 0.013 |
| Superficial | 3 | 2 | |
| Deep | 3 | 0 | |
| Organ-space | 4 | 0 |
| Variables | Wiek | CCS | LoS | EBL | ΔIL-1β8h/0 | ΔTNFα8h/0 | ΔIL-68h/0 |
|---|---|---|---|---|---|---|---|
| ΔIL-88h/0 | ns | ns | r = 0.45, p = 0.012R | r = 0.38, p = 0.002 | r = 0.63, p < 0.001O | r = 0.54, p = 0.002O | r = 0.70, p < 0.001O r = 0.58, p < 0.001R |
| ΔMCP-18h/0 | r = 0.38, p = 0.035O | r = 0.28, p = 0.028 | ns | r = 0.35, p = 0.006 | r = 0.40, p = 0.024O | r = 0.40, p = 0.025O | r = 0.75, p < 0.001O r = 0.79, p < 0.001R |
| ΔMIP-1α8h/0 | ns | ns | ns | ns | r = 0.54, p = 0.002O r = 0.51, p = 0.002R | r = 0.49, p = 0.005O r = 0.49, p = 0.006R | ns |
| ΔMIP-1β8h/0 | ns | ns | ns | ns | r = 0.41, p = 0.026R | r = 0.39, p = 0.034R | ns |
| ΔEOX8h/0 | ns | ns | r = −0.37, p = 0.043O | ns | r = 0.36, p = 0.045O r = 0.67, p < 0.001R | r = 0.44, p = 0.014O r = 0.73, p < 0.001R | r = 0.37, p = 0.042O |
| ΔRANTES8h/0 | ns | ns | ns | ns | r = 0.42, p = 0.020R | r = 0.55, p = 0.002R | ns |
| Dependent Variable | Entered Explanatory Variables | Retained Variables Coeff. b; rp, Significance | Goodness of Fit Constant; R2; F-Ratio, Significance |
|---|---|---|---|
| ΔIL-88h/0 | surgery (OCS as 1), age1, LoS, EBL, APR2, ΔIL-1β8h/0, ΔTNFα8h/0, ΔIL-68h/0 | LoS: b = 0.001; rp = 0.43, p < 0.001 EBL: b = 0.001; rp = 0.45, p < 0.001 ΔTNFα8h/0: b = 0.397; rp = 0.38, p = 0.003 ΔIL-68h/0: b = 0.238; rp = 0.61, p < 0.0001 | 0.251; R2 = 0.623; F = 23.12, p < 0.0001; with surgery instead of EBL: 0.294; R2 = 0.584; F = 19.66, p < 0.0001 |
| ΔMCP-18h/0 | surgery, CCS, age1, LoS1, EBL, ΔIL-1β8h/0, ΔTNFα8h/0, ΔIL-68h/0 | ΔIL-68h/0: b = 0.472; rp = 0.79, p < 0.0001 | 0.942; R2 = 0.621; F = 96.65, p < 0.0001 |
| ΔMIP-1α8h/0 | APR2, ΔIL-1β8h/0 ΔTNFα8h/0 | ΔIL-1β8h/0: b = 0.359; rp = 0.51, p < 0.0001 | 1.279; R2 = 0.263; F = 21, p < 0.0001 |
| ΔMIP-1β8h/0 (in RACS) | ΔIL-1β8h/0 ΔTNFα8h/0 | ΔIL-1β8h/0: b = 0.312; rp = 0.41, p = 0.026 | 1.401; R2 = 0.165; F = 5.54, p = 0.026 |
| ΔEOX8h/0 | LoS, ΔIL-1β8h/0, ΔTNFα8h/0, ΔIL-68h/0 | ΔTNFα8h/0: b = 0.499; rp = 0.62, p < 0.0001 | 0.933; R2 = 0.378; F = 35.89, p < 0.0001 |
| ΔRANTES8h/0 | surgery, anemia, ΔIL-1β8h/0 ΔTNFα8h/0 | ΔTNFα8h/0: b = 0.769; rp = 0.42, p < 0.001 in RACS: ΔTNFα8h/0: b = 1.135; rp = 0.55, p = 0.002 | 0.358; R2 = 0.175; F = 12.54, p < 0.001 in RACS: –0.45; R2 = 0.305; F = 12.3, p = 0.002 |
| Logistic Regression: | ||||
|---|---|---|---|---|
| Dependent variable | Entered explanatory variables | Retained variables Coeff. b, p | Goodness of fit χ2, p; RN2 | Accuracy AUC (95% CI), p; sens. and spec. (%) |
| SSI | surgery (OCS encoded as 1), LoS1, ASA2, BMI1, transfusions, age, cancer dissemination3, sex, ΔIL-872h/0, ΔMCP-172h/0, ΔMIP-1α72h/0, ΔMIP-1β72h/0 | OCS: b = 1.86, p = 0.042 ΔMCP-172h/0: b = 2.69, p = 0.008; | χ2 = 15.9, p < 0.001; RN2 = 0.37 | 0.819 (0.70–0.91), p < 0.0001; 92 and 70% |
| AL (in OCS) | sex, BMI1, LoS1, transfusions, ASA2, cancer dissemination3, age, ΔIL-824h/0, ΔMCP-124h/0, ΔMCP-172h/0 | ΔIL-824h/0: b = 12, p = 0.037 | χ2 = 11.2, p < 0.001; RN2 = 0.59 | 0.938 (0.78–0.99), p < 0.0001; 100 and 83% |
| RoBF | surgery, sex, age, LoS, cancer dissemination, transfusion, stomy4, AL, TNR, BMI1,ASA2, MCP-124h, RANTES24h | LoS5: b = −1.4, p = 0.033 MCP-124: b = 2.72, p = 0.017 | χ2 = 10.4, p = 0.006; RN2 = 0.23 | 0.734 (0.60–0.84), p < 0.001; 100 and 43% |
| Multiple linear regression: | ||||
| Dependent variable | Entered explanatory variables | Retained variables Coeff. b; rp, p | Goodness of fit Constant; R2; F-ratio, p | |
| LoHS | surgery, age, ASA2, subsite6, ΔIL-824h/0, ΔMCP-124h/0, MCP-124h, ΔMIP-1α24h/0, RANTES24h | OCS: b = 2.01; rp = 0.36, p = 0.007 subsite: b = 2.01; rp = 0.37, p = 0.005 RANTES24h: b = 1.58; rp = 0.27, p = 0.045 | 3.83; R2 = 0.26; F = 6.4, p < 0.001 | |
| LoHS (open) | age, ASA2, subsite6, ΔIL-824h/0, ΔMCP-124h/0, MCP-124h, ΔMIP-1α24h/0, RANTES24h | ΔIL-824h/0: b = 8.28, rp = 0.55, p = 0.003 RANTES24h: b = 4.54; rp = 0.49, p = 0.009 | −12.4; R2 = 0.47; F = 11.5, p < 0.001 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krzystek-Korpacka, M.; Zawadzki, M.; Lewandowska, P.; Szufnarowski, K.; Bednarz-Misa, I.; Jacyna, K.; Witkiewicz, W.; Gamian, A. Distinct Chemokine Dynamics in Early Postoperative Period after Open and Robotic Colorectal Surgery. J. Clin. Med. 2019, 8, 879. https://doi.org/10.3390/jcm8060879
Krzystek-Korpacka M, Zawadzki M, Lewandowska P, Szufnarowski K, Bednarz-Misa I, Jacyna K, Witkiewicz W, Gamian A. Distinct Chemokine Dynamics in Early Postoperative Period after Open and Robotic Colorectal Surgery. Journal of Clinical Medicine. 2019; 8(6):879. https://doi.org/10.3390/jcm8060879
Chicago/Turabian StyleKrzystek-Korpacka, Malgorzata, Marek Zawadzki, Paulina Lewandowska, Krzysztof Szufnarowski, Iwona Bednarz-Misa, Krzysztof Jacyna, Wojciech Witkiewicz, and Andrzej Gamian. 2019. "Distinct Chemokine Dynamics in Early Postoperative Period after Open and Robotic Colorectal Surgery" Journal of Clinical Medicine 8, no. 6: 879. https://doi.org/10.3390/jcm8060879