Direct estimation of central aortic pressure from measured or quantified mean and diastolic brachial blood pressure: agreement with invasive records
 Daniel Bia1*
Daniel Bia1*  Federico Salazar2
Federico Salazar2  Luis Cinca2 Marcos Gutierrez2 Alvaro Facta2
Luis Cinca2 Marcos Gutierrez2 Alvaro Facta2  Yanina Zócalo1
Yanina Zócalo1  Alejandro Diaz3
Alejandro Diaz3
- 1Departamento de Fisiología, Centro Universitario de Investigación, Innovación y Diagnóstico Arterial (CUiiDARTE), Facultad de Medicina, Universidad de la República, Montevideo, Uruguay
- 2Sección Hipertensión Arterial, Departamento de Cardiología, Hospital Privado de Comunidad, Mar del Plata, Argentina
- 3Instituto de Investigación en Ciencias de la Salud, UNICEN-CCT CONICET, Tandil, Argentina
Background: Recently it has been proposed a new approach to estimate aortic systolic blood pressure (aoSBP) without the need for specific devices, operator-dependent techniques and/or complex wave propagation models/algorithms. The approach proposes aoSBP can be quantified from brachial diastolic and mean blood pressure (bDBP, bMBP) as: aoSBP = bMBP2/bDBP. It remains to be assessed to what extent the method and/or equation used to obtain the bMBP levels considered in aoSBP calculation may affect the estimated aoSBP, and consequently the agreement with aoSBP invasively recorded.
Methods: Brachial and aortic pressure were simultaneously obtained invasively (catheterization) and non-invasively (brachial oscillometry) in 89 subjects. aoSBP was quantified in seven different ways, using measured (oscillometry-derived) and calculated (six equations) mean blood pressure (MBP) levels. The agreement between invasive and estimated aoSBP was analyzed (Concordance correlation coefficient; Bland-Altman Test).
Conclusions: The ability of the equation “aoSBP = MBP2/DBP” to (accurately) estimate (error <5 mmHg) invasive aoSBP depends on the method and equation considered to determine bMBP, and on the aoSBP levels (proportional error). Oscillometric bMBP and/or approaches that consider adjustments for heart rate or a form factor ∼40% (instead of the usual 33%) would be the best way to obtain the bMBP levels to be used to calculate aoSBP.
1. Introduction
Several approaches and devices are used to non-invasively estimate aortic systolic blood pressure (aoSBP). They differ in the technology (e.g., ultrasound, applanation tonometry), recording-site (e.g., carotid, radial, brachial) and/or in the mathematical analysis (e.g., direct vs. general transfer function-derived estimation) considered (1–4). This could result in differences in the aoSBP levels obtained (1, 2) and in the agreement with invasive aoSBP data. This, in turn, could depend on the “calibration scheme” considered (1, 2, 5–9). However, at present there is no consensus and it is still discussed on which (if any) would be the best approach to estimate aoSBP (1, 2). The above could have contributed to the fact that aoSBP estimation has not become widespread in clinical practice, despite the recognized value of knowing central haemodynamics in different situations (10).
Recently, Chemla et al. proposed a simple approach [“direct central blood pressure estimation (DCBP)”] that could “facilitate” aoSBP estimation (and may help to expand its use in clinical practice). According to the authors, from brachial diastolic (bDBP) and mean (bMBP) blood pressure (BP), aoSBP could be determined as: aoSBP = bMBP2/bDBP (11). It should be noted that prior to becoming “accepted and generalized”, the proposed method must be further evaluated by contrasting the aoSBP values it estimates with those obtained invasively (catheterization). On the other hand, and related with the above, it should be evaluated to what extent the way in which bMBP is quantified could impact on the aoSBP levels estimated. In this regard, mean blood pressure (MBP), could correspond to MBP (or bMBP) measured by oscillometry (lowest cuff pressure value measured during the maximum oscillations' plateau), or calculated from bDBP and bSBP (1, 2, 12). About this, bMBP has been calculated from equations that differ in the use of predefined empirical adjustments (e.g., adding 5 mmHg to pre-calculated values), corrections by heart rate (HR) and/or in the form factor (FF) considered (e.g., 33%, 42%) (12–14). bMBP levels obtained with different approaches can differ significantly and it should be noted that while some authors have stated that a given approach would be superior to the others when estimating bMBP, others suggested that ´the best´ way to quantify bMBP may differ depending on the situation and/or the aim pursued (12, 15–17).
The objective of the present study was to assess the level of association and agreement between aoSBP obtained invasively (catheterization) and estimated (DCBP), considering different approaches to quantify bMBP. It is worth noting that in this work we are not validating a calculated parameter, but providing information on what margins of deviation and error could be expected if the aortic pressure quantification approach (“DCBP”) proposed by Chemla et al. is used in clinical settings.
2. Methods
2.1. Subjects
Eighty-nine subjects undergoing coordinated coronary angiogram (Department of Cardiology of the Hospital Privado de Comunidad, Mar del Plata, Argentina) were included. Aortic valve disease, left ventricular (LV) outflow tract obstruction and/or arrhythmia were exclusion criteria. Prior to the study, a clinical evaluation enabled assessing the exposure to cardiovascular risk factors (18–23). All the included subjects gave their written informed consent. Data included in this work were not considered in prior publications. The protocol was approved by the Institutional Ethic Committee. The procedures agreed with the Declaration of Helsinki.
The following data were obtained: (1) invasive aortic BP (aoBP) and bBP (catheterization), (2) non-invasive bBP and aoBP, levels and waveforms assessed from oscillometric/plethysmographic brachial artery data (Mobil-O-Graph device, Model PWA, IEM GmbH, Stolberg, Germany).
2.2. Invasive measurement of aoBP and bBP
Intra-arterial aoBP and bBP levels and waveforms were obtained with the subjects lying in supine position. Asepsis of the area, followed by cutaneous/subcutaneous injection of lidocaine was performed prior to the arterial (radial) access. Then, a 5 or 6 French introducer sheath was positioned in the arterial lumen and heparin was administered. After that, a 0.035-inch guide wire was placed in the ascending aorta and finally a 5 French pig tail catheter (Cordis, Miami, USA) was introduced. The catheter tip was always placed ∼4 cm away from the aortic valve. Once the correct positioning of the catheter was verified (fluoroscopy), the guide was removed and the catheter was washed with saline solution. Soft sedation was administered during the catheterization to minimize pain and discomfort.
To obtain intravascular (proximal ascending aorta or brachial) pressure, the fluid-filled catheter was connected to an external transducer (TruWave, PX260, Edwards, Dominican Republic), associated to a Mindray Mec 2012 system (Shenzhen Mindray Bio-Medical Electronics Co., China) which was synchronized with a x-ray device (Allura CV-20, Philips Healthcare, Netherlands). The external transducer was always kept at the heart level (mid-axillary line) and was calibrated in agreement with the system's inbuilt two-point calibration technique. The Allura CV-20 monitor allowed a display of the registered BP waves. Prior to any record or measurement the system was flushed with saline solution and the quality of the pressure signals was visually checked.
After obtaining aoBP data, the catheter was placed in the brachial artery (opposite to that of the limb of the vascular access), at the level in which the cuff for bBP measurement was positioned. Then, invasive intra-arterial bBP was measured and non-invasive (oscillometry-derived) bBP values were obtained immediately before or after the invasive recordings. After each bBP recording, the catheter was placed in the ascending aorta to check hemodynamic stability.
From invasive BP data, the processing systems enabled HR, systolic and diastolic BP values to be obtained.
After data collection, the catheter was withdrawn and the patient was sent to the recovery area.
2.3. Non-invasive measurement of bBP and MBP estimation
Immediately before and/or after each invasive aortic or brachial record, bBP was non-invasively determined from a pneumatic cuff positioned in the arm opposite to that of the vascular access (oscillometry/plethysmography, Mobil-O-Graph device) (20, 24, 25). The system obtains bMBP (and HR) and after applying internal algorithms (manufactureŕs property) it gives systolic (bSBP) and bDBP (but not the bMBP), from which pulse pressure can be calculated (bPP, bPP = bSBP-bDBP).
From the data obtained, bMBP was quantified as follows (1, 15, 26, 27):
(i) bMBP0.42 = 0.42*bSBPosc + 0.58*bDBPosc
(ii) bMBP0.412 = bDBPosc + [0.412*(bSBPosc-bDBPosc)]
(iii) bMBP0.33 = bDBPosc + 0.33*(bSBPosc-bDBPosc).
(iv) bMBP0.33 + 5 = bDBPosc + [0.33*(bSBPosc-bDBPosc) + 5].
(v) bMBP0.33HR = bDBPosc + [0.33 + (0.0012*HRosc)]*(bSBPosc-bDBPosc)
(vi) bMBPSBP*DBP0.5 = (bSBPosc*bDBPosc)0.5
The suffix osc was used to name the variables obtained from oscillometry (bMBPosc, bSBPosc, bDBPosc, bPPosc and HRosc). The bMBP values obtained as described were considered to calculate the aoSBP using Chemla et al. approach (DCBP) (11).
2.4. Estimation of aoSBP
Using the equation proposed by Chemla et al. (11), and considering the different methods used to calculate MBP, aoSBP levels were obtained from invasive aoBP, invasive bBP and non-invasive bBP recordings. The non-invasive bBP data used to calculate aoBP were obtained simultaneously with the invasive aortic recordings. Then, as an example, aoSBP obtained from non-invasive bBP was named according to the approach used to quantify bMBP: (i) aoSBP_0.42, (ii) aoSBP_0.412, (iii) aoSBP_0.33, (iv) aoSBP_033 + 5, (v) aoSBP_0.33HR, (vi) aoSBP_SBP*DBP0.5 and (vii) aoSBP_Osc.
2.5. Data analysis
2.5.1. Association and agreement between measured and estimated aoSBP
After analyzing the subjectś characteristics (Table 1; Supplementary File S1, Supplementary Table S1), we evaluated the association and agreement between aoSBP data invasively measured and estimated. To this end, Lin's Concordance Correlation Coefficient (CCC) and Bland-Altman analyses (Table 2; Supplementary File S1, Supplementary Tables S2–S4; Supplementary File S2, Supplementary Figures S1–S3) were considered. Measured (invasive) aoSBP was always the ´reference method´. The analyses were performed for aoSBP levels (DCBP), calculated from systolic and diastolic BP values: (i) measured at the aorta (Supplementary Figure S1), (ii) measured at the brachial artery (Supplementary Figure S2), and (iii) estimated from non-invasive bBP records (Mobil-O-Graph) (Supplementary Figure S3). Bland-Altman tests were used to assess the presence of mean (systematic) and proportional errors between aoSBP data obtained with the reference (invasive) and the ´tested´ method (DCBP). The analyses correspond to reference data (measured aoSBP; x-axis) plotted against the difference between measured and estimated aoSBP (y-axis). The regression equations were obtained.
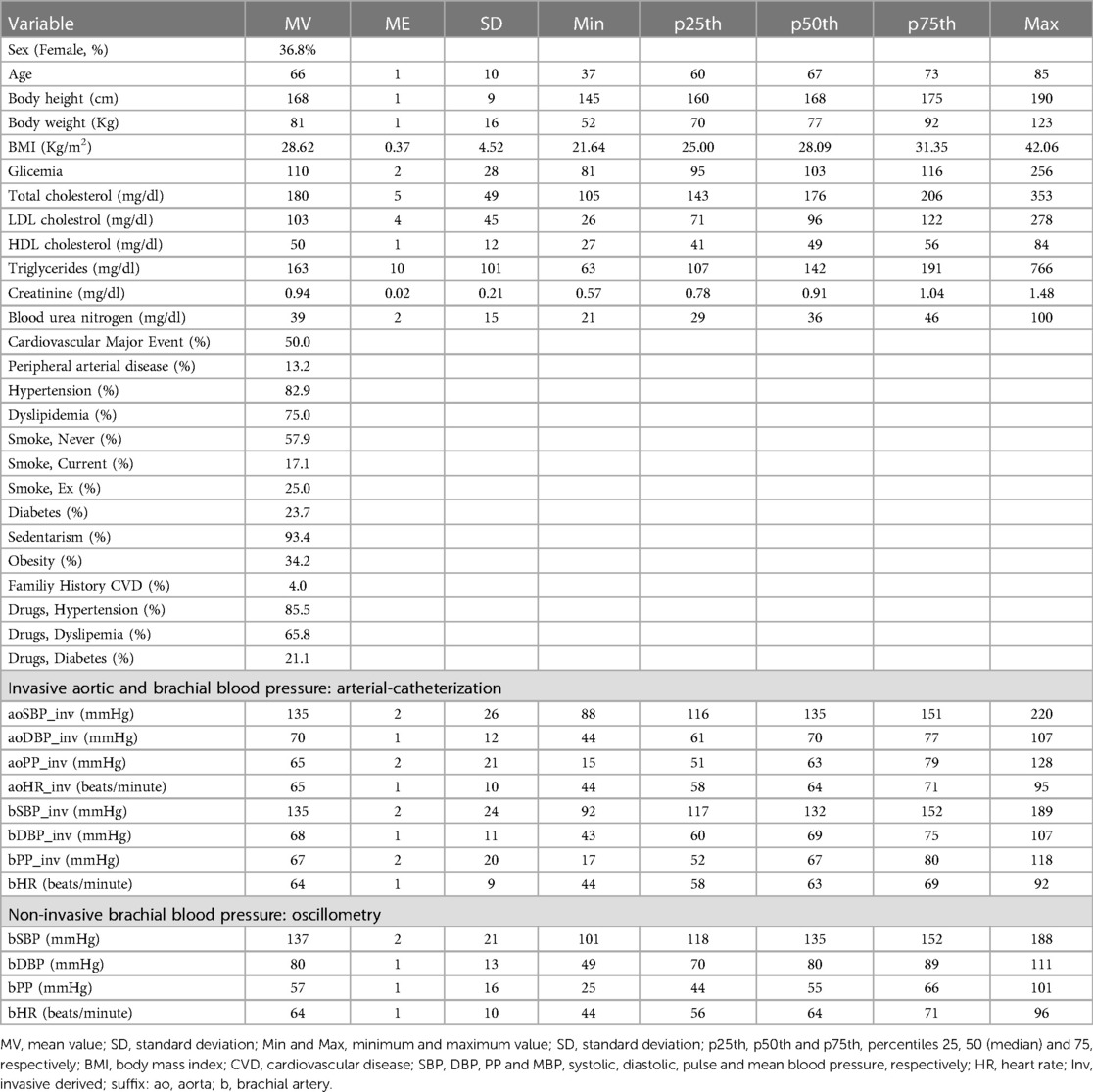
Table 1. Demographic, anthropometric and clinical characteristics of the study population.
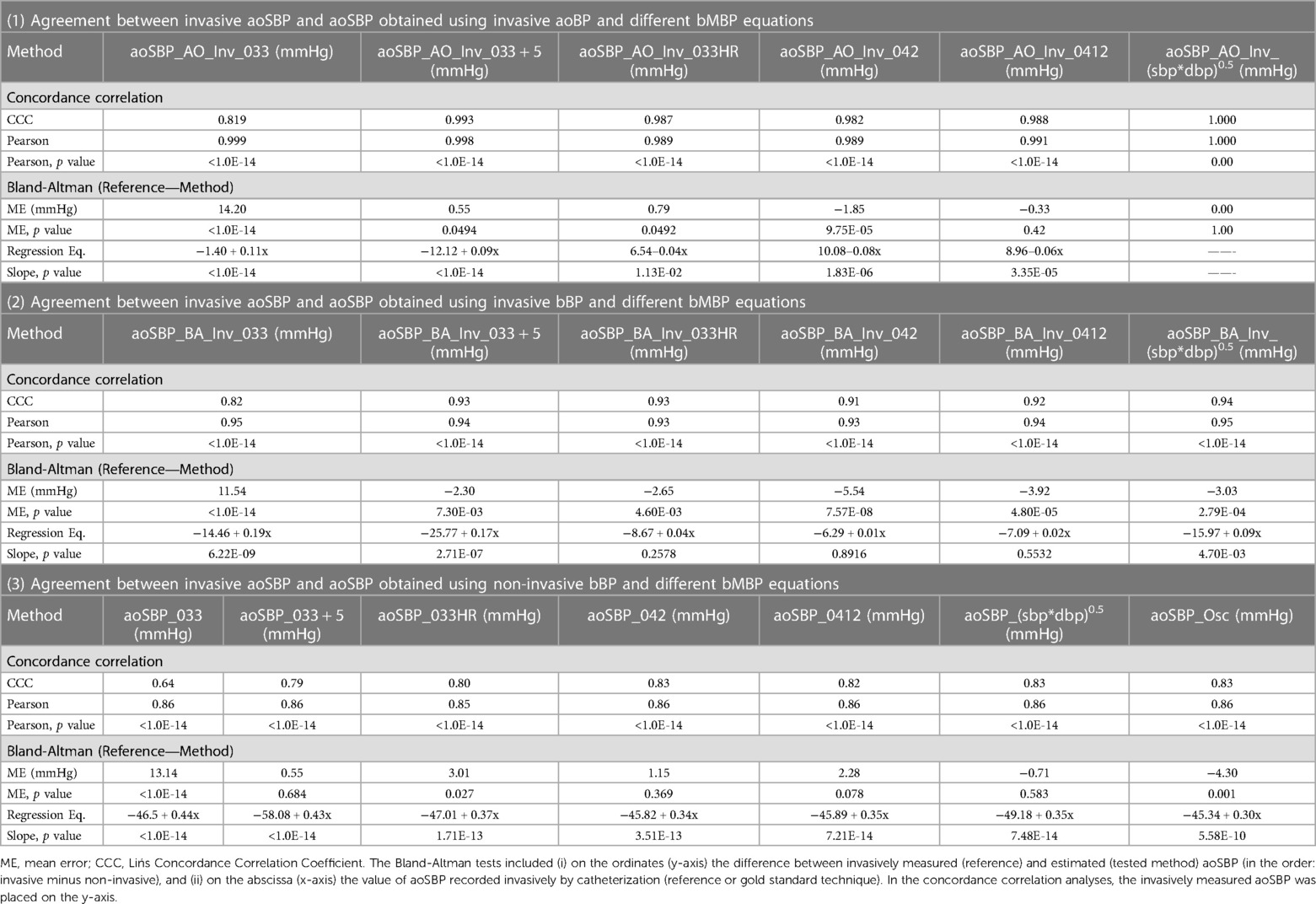
Table 2. Correlation and agreement between invasive aoSBP (reference) and estimated aoSBP (considering invasive aoBP and invasive and non-invasive bBP levels, and different bMBP equations).
2.5.2. Level of agreement between invasive and estimated aoSBP
The measurements were divided into four categories (ranges) according to Bland-Altman mean errors (rounded absolute value): (i) 0–5 mmHg, measurements considered “very accurate” (errors without clinical relevance; green), (ii) 6–10 mmHg, measurements “slightly inaccurate” (yellow), (iii) 11–15 mmHg, measurements “moderately inaccuraté (orange), and (iv) >15 mmHg, “very inaccurate” measurements (red) (Table 3) (11, 28). Taking into account these bands and the regression equation obtained in the Bland-Altman analysis, the bias (in mmHg) for each of the methods used to quantify aoSBP was determined considering the minimum, the maximum and the percentiles 25th, 50th and 75th of the invasive aoSBP data. (Table 3, Top). In addition, the ranges of measured aoSBP levels for which the different estimation methods would yield “very accurate” (−5 to 5 mmHg), “slightly inaccurate” (−10 to 10 mmHg) or “moderately inaccurate” (−15 to 15 mmHg) estimates were identified (Table 3, Bottom). Finally, the “average” aoSBP levels for which the different estimation methods would achieve the described errors were calculated.
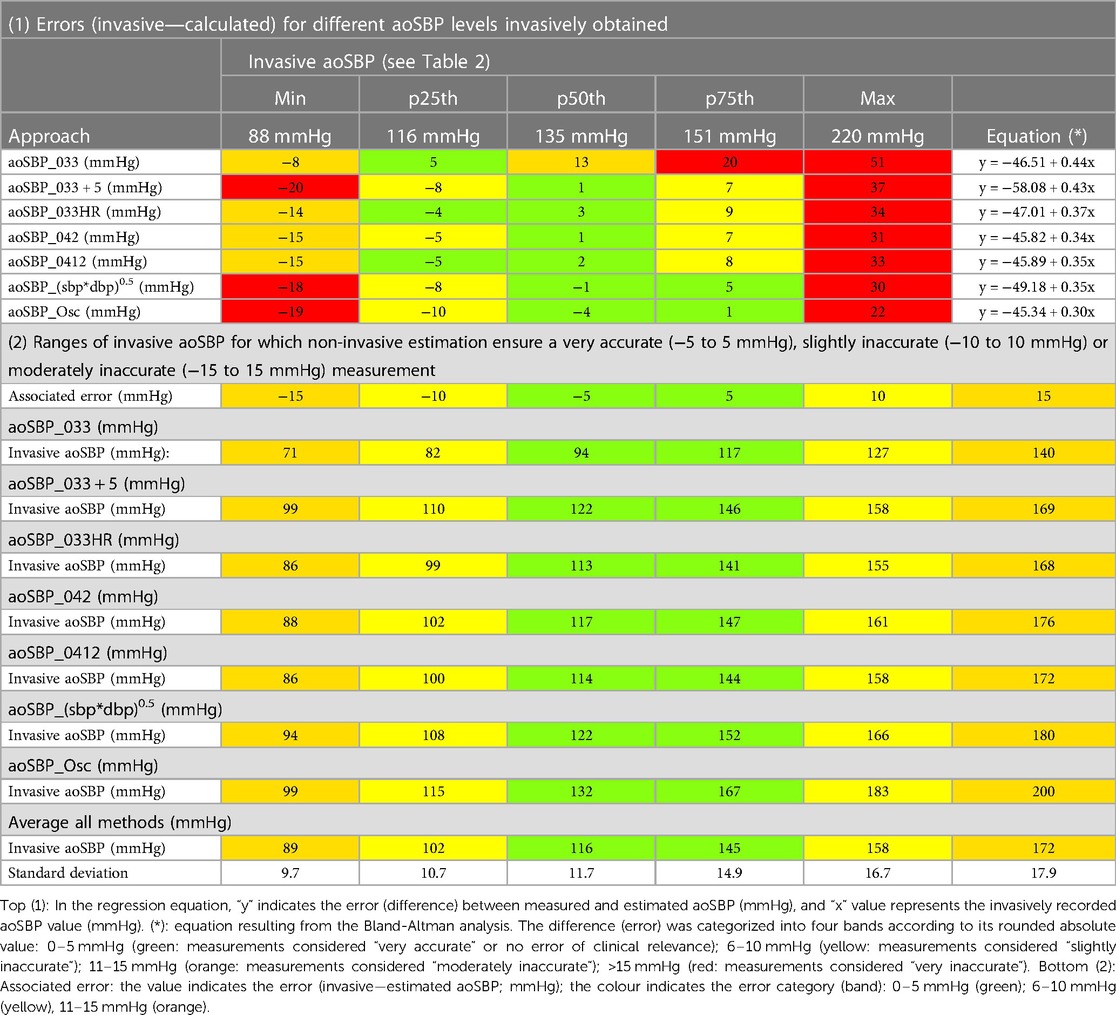
Table 3. Non-invasive approach error levels related to invasive blood pressure values.
Evans's Empirical Classification (“correlation strength”) was used to interpret r values: <0.20: very weak; 0.20–0.39: weak; 0.40–0.59: moderate; 0.60–0.79: strong; ≥0.80: very strong (29). According to the central limit theorem, taking into account Kurtosis and Skewness coefficients distribution and the number of subjects (sample size > 30) a normal distribution was considered (30). The sample size exceeds the minimum (n = 85) recommended for studies in which analyses of agreement between invasive and non-invasive BP measurements are performed (17). MedCalc (v.14.8.1, MedCalc Inc., Ostend, Belgium) and IBM-SPSS Statistical Software (v.26, SPSS Inc., Illinois, USA) were used. A p < 0.05 was considered as the statistical significance threshold.
3. Results
3.1. Population and hemodynamic characteristics
The studied subjects were distributed over a wide range of ages (37–85 y) (Table 1; Supplementary File S1, Supplementary Table S1). Invasive aoSBP and bSBP values were also distributed across a broad range: 7.8% and 4.5% were <100 mmHg, 53.9% and 48.4% were between 100 and 139 mmHg, 21.3% and 30.3% were between 140 and 159 mmHg, and 16.9% and 15.7% of the values were ≥160 mmHg. In turn, invasive aoDBP and bDBP values were <60 mmHg in 21.3% and 25.8% of cases; they were between 60 and 84 mmHg in 68.5% and 64.0%, and in 10.1% and 8.9% of cases the values were >85 mmHg. HR values were always within the expected (normal) range.
3.2. Agreement between measured and estimated aoSBP
3.2.1. Aortic invasive records
When considering invasive aoDBP and aoMBP calculated from invasive aoSBP and aoDBP (Table 2; Supplementary File S1, Supplementary Table S2, Supplementary File S2, Supplementary Figure S1: (i) calculated and measured (invasive) aoSBP data showed ´very stronǵ association, (ii) the equation using a FF = 33% showed a large mean error (14.2 mmHg), whereas (iii) the equations using a FF = 33% with HR correction, a FF = 42% or a FF = 41.2% achieved very low mean errors (0.3 to 1.85 mmHg). The equation aoMBP = (aoSBP*aoDBP)0.5 allowed full agreement with invasive aoSBP. With the only exception of the latter, all the methods showed proportional errors. The largest was observed when using FF = 33%.
3.2.2. Brachial invasive records
Similarly, when analyzing invasive bDBP and bMBP calculated from invasive bSBP and bDBP records (Table 2; Supplementary File S1, Supplementary Table S3, Supplementary File S2, Supplementary Figure S2): (i) calculated and invasive aoSBP showed “very strong” association, (ii) using a FF = 33% resulted in large mean error (11.5 mmHg), and (iii) equations using FF = 33% and HR correction, FFs = 42% and FF = 41.2%, achieved very low mean bias (<5 mmHg), and showed no proportional errors.
3.2.3. Brachial non-invasive (oscillometric) records
Invasive and non-invasive aoSBP data showed “strong” and “very strong” degrees of concordance (CCC between 0.64 and 0.83). The lowest CCC (yet statistically significant) was observed when analyzing invasive aoSBP and DCBP quantified using bMBP_033 (FF = 33% without HR correction) (Table 2; Supplementary File S1, Supplementary Table S4, Supplementary File S2, Supplementary Figure S3).
The mean error values obtained with the different methods were distributed over a wide range (−4.30 to 13.14 mmHg). However, most (6 out of 7) approaches showed mean bias between −5 and 5 mmHg and several (4 out of 7) showed mean errors without statistical significance (Table 2). The highest mean error was observed for aoSBP quantified using bMBP_033 (FF = 33% uncorrected for HR).
The “slopes” (proportional errors) of the linear adjustments showed that regardless of the equation used to quantify bMBP, aoSBP data obtained from bMBP2/bDBP showed variations in the error levels related to inter-individual differences in invasive aoSBP (Table 2).
3.3. Agreement between measured and estimated aoSBP
Related with the above, when analyzing the errors observed when considering different aoSBP levels it was found that (Table 3, Top): (i) all approaches underestimated aoSBP (error range: 22–51 mmHg) at high aoSBP levels (e.g., close to 220 mmHg, the maximum measured). The highest bias was obtained when using FF = 33% without correction for HR; (ii) at low invasive aoSBP levels (e.g., close to 88 mmHg, the lowest value measured) all approaches overestimated aoSBP (error range: 8–20 mmHg); (iii) for aoSBP values within 25th and 75th percentiles (116–151 mmHg), non-invasive approaches allowed reaching errors <10 mmHg (except for the method using a FF = 33%). The calculation of aoSBP using bMBPosc would enable to minimize errors when considering high invasive aoSBP levels (Table 3, Top); but the use of bMBP calculated using FF = 33% corrected for HR, FF = 42% or 41.2%, would result in acceptable bias.
Table 3 (Bottom), shows that different non-invasive approaches had different aoSBP ranges in which they “ensured” errors between (i) −5 and 5 mmHg (green), (ii) −10 and 10 mmHg (yellow) and/or (iii) −15 and 15 mmHg (orange). For instance, estimating aoSBP from bDBP and bMBPosc, allowed ensuring errors <10 mmHg when invasive aoSBP levels were between 115 and 183 mmHg, while the calculus of bMBP using an FF = 33%, would ensure reduced errors within an aoSBP range between 82 and 127 mmHg. In general terms, the remaining methods (FF = 33% corrected for HR, FF = 42% or 41.2%) resulted in errors <10 mmHg, within a pressure range of 100–110 (lower limit) and 155–165 mmHg (upper limit). In summary, the different approaches used to calculate aoSBP: (i) showed differences in “global” mean bias, (ii) over- and under-estimated aoSBP at low and high BP levels, respectively, and (iii) showed differences in the aoSBP range in which they would perform best as aoSBP estimators.
4. Discussion
4.1. Clinical and physiological relevance
Chemla et al. developed their equation by comparing invasive (cathetersm) measurements in the ascending aorta with invasive measurements in the radial and brachial arteries. The validation of the Chemla et al. equation for cuff-based oscillometrically measured bBP values is still pending. Additionally, it remains to be assessed to what extent the method or equation used to obtain the bMBP levels has an influence on the validity of the Chemla et al. equation. In this work we applied, for the first time using invasive and non-invasive records, the method proposed by Chemla et al. and analyzed the obtained data with the aim of contributing to define to what extent the approach considered to determine the bMBP values to be used to calculate the aoSBP according to the method would impact on the accuracy and validity of the estimated data. The main contribution of this manuscript is the demonstration that the usefulness of the method recently proposed by Chemla et al. would be (i) highly dependent on the approach used to quantify bMBP, and (ii) on the aoBP levels considered. Our work highlights four issues.
First, the ability of Chemla et al. (11) approach to obtain aoSBP values close to those measured invasively depends on the way in which bMBP is obtained (measured or quantified) and on the actual aoSBP levels in the specific subject. Then, trying to generalize and define dichotomously whether the approach is “good or bad” without taking into account the above would be a mistake (and an over-simplification). The different approaches used to calculate aoSBP: (i) showed differences in “global” mean bias, (ii) over- and under-estimated aoSBP at low and high BP levels, respectively, and (iii) showed differences in the aoSBP range in which they would perform best as aoSBP estimators.
Second, calculating bMBP using a FF = 33% without HR adjustment (the most widespread way of calculating the MBP), would result in aoSBP values far from the invasive ones. Furthermore, that approach gave the highest mean error levels. Additionally, compared to other approaches, its best performance (lowest error) was observed at low aoSBP levels (Table 3, Bottom) which would be mainly observed in haemodynamic states or clinical situations in which assessing central haemodynamics could not be considered decisive (e.g., in terms of clinical decisions). On the other hand, and in the same line, at least in theory, aoSBP_033 could be considered useful to assess aoSBP in children and adolescents who have low aoSBP. However, it would not be useful in children/adolescents exposed to clinical conditions and/or risk factors (e.g., sedentary, overweight-obesity) in which aoSBP levels have been shown to be elevated (25, 31–33). This should be evaluated in future studies.
Third, the other methods used to calculate bMBP and/or bMBPosc, showed (quite) similarity in their ability to estimate aoSBP. Unfortunately, most brachial cuff-based methods (oscillometric devices) do not give bMBPosc, even though it is quantified as a prior step to the obtaining of bSBP and bDBP (the values actually given). In fact, most of the oscillometric devices do not show the researcher or clinician the bMBPosc (e.g., Mobil-O-Graph, Omron semi-automatic BP devices). These devices show on the display the HR and bSBP and bDBP values (calculated with the manufacturer's own internal algorithms). Then, the researcher and/or clinician can only quantify bMBP using equations such as those used in our manuscript. In other words, the systems “measure” the bMBPosc (as is widely known), but then use it to calculate bSBP and bDBP values, which are the values shown, and do not display the measured data. Therefore, the bMBPosc related approach while accurate would be difficult to apply and generalize in clinical practice.
Fourth, methods using a FF = 33% with HR correction and/or a FF close to 40% (42% or 41.2%) may be one step ahead of the rest when jointly considering three factors: (i) agreement with invasive aoSBP, (ii) aoSBP range within which they ensure the lowest errors (100–110 to 155–165 mmHg), and (iii) feasibility to be applied in clinical practice.
4.2. Strengths and limitations
First, healthy subjects were not included in this work. This is a common feature of this kind of studies given the conditions required for the indication of invasive evaluations (e.g., suspected or known cardiovascular disease) (2). However, and in line with the above, the studied subjects would be representative of those whose accurate hemodynamic and/or cardiovascular assessment would be considered critical in clinical practice.
Second, the sample size (n = 89) exceeded the minimum recommended for studies aimed at analyzing the agreement (e.g., Blant-Altman test) between invasive and non-invasive BP measurements (17). In addition, despite, the sample size could be considered moderate, it enabled to detect statistical differences, thus achieving suitable statistical power (minimizing type 2 errors). Measurements in the brachial artery opposite to that of the vascular access limb and the need for additional recordings in the aorta considered in the study protocol, increased catheterization-time, which restricted the number of patients considered elective and/or who agreed to participate.
Third, although we are aware that differences between measured and estimated aoSBP could vary depending on covariates (34, 35) neither the sample size, nor its heterogeneity allowed to define subgroups (e.g., defined by age, sex and/or exposure to risk factors) and perform adequate statistical analyses. Further multicentre studies would be necessary to analyze the impact of covariates on the results.
Fourth, we used “fluid column” transducers instead of solid-state pressure sensors, which characteristically provide accurate BP waveforms (mainly due to their ability to detect the high-frequency components of the wave). In any case, fluid column transducers are not only the sensors used in our Hospital but they are widely used to measure aoSBP in clinical practice. Furthermore, in the ARTERY Society task force consensus statement on protocol standardization, Sharman et al. stated that while micromanometer-tipped catheters would be the sensors of choice, if carefully handled, fluid column catheters could be used to measure intra-arterial BP (17). Additionally, recently, in a systematic review and meta-analysis, fluid-filled and catheter-tipped transducers have shown similar mean bias in non-invasive aoSBP estimation (2). Taking into account the natural frequency and damping coefficient of our recording (catheter-tubing-external transducer) system, and although the methods and devices used are widely validated, the systolic and diastolic BP values obtained invasively could entail a small over- and under-estimation, respectively.
Fifth, an issue to consider is that regardless of the method used, non-invasively assessed bBP always has “inherent errors” (e.g., under- and over-estimation of bSBP and bDBP, respectively) (36). Then, the ability of bBP to accurately quantify aoBP (using the method of Chemla et al.) may depend (among other factors) on the approach and device used. Additionally, taking into account the inter-individual differences in BP amplification and in the brachial pulse waveform, the form factor that should be used to properly calculate bMBP may vary (37). In this regard, Schultz et al. showed that no universal form factor would achieve an accurate estimation of bMBP in all individuals (37). Thus, our results regarding the best approach to quantify bMBP to be used to estimate aoSBP must be analyzed in the context of the overall scenario, as there may be differences among individuals.
5. Conclusions
The ability of “aoSBP = MBP2/DBP” equation to accurately estimate (error <5 mmHg) invasive aoSBP levels depends on the bMBP method/equation employed, and on the actual aoSBP levels (proportional error).
The best way to obtain bMBP to be used to calculate aoSBP would be bMBPosc and/or approaches that include adjustments for HR or FF ∼40% (bMBP042, bMBP0.412, bMBP033HR), instead of the usual FF = 33%.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Comité de Ética del Hospital Privado de Comunidad, Argentina, Mar del Plata, Provincia de Buenos Aires, Argentina. The patients/participants provided their written informed consent to participate in this study.
Author contributions
DB and YZ: contributed to conception and design of the study. FS, LC, MG, and AF: performed the invasive and non-invasive recordings. DB, FS, and AD: constructed and organized the database. DB and YZ: performed the statistical analysis. DB, YZ, and AD wrote the work's first draft and final version. All authors contributed to the article and approved the submitted version.
Funding
This research was funded by the Departamento de Cardiología, Hospital Privado de Comunidad, Argentina, Mar del Plata, Provincia de Buenos Aires (Argentina), Agencia Nacional de Investigación e Innovación (ANII; grant number PRSCT–008–020; Uruguay), Programa de Desarrollo de las Ciencias Básicas (PEDECIBA-Biología; Uruguay), and extra budgetary funds provided by DB and YZ and CUiiDARTE.
Acknowledgments
We thank the participants for their contribution to the study and the colleagues who helped during the studies.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1207069/full#supplementary-material
References
1. Bia D, Zócalo Y, Sánchez R, Lev G, Mendiz O, Pessana F, et al. Aortic systolic and pulse pressure invasively and non-invasively obtained: comparative analysis of recording techniques, arterial sites of measurement, waveform analysis algorithms and calibration methods. Front Physiol. (2023) 14:1113972. doi: 10.3389/fphys.2023.1113972
2. Papaioannou TG, Karageorgopoulou TD, Sergentanis TN, Protogerou AD, Psaltopoulou T, Sharman JE, et al. Accuracy of commercial devices and methods for noninvasive estimation of aortic systolic blood pressure a systematic review and meta-analysis of invasive validation studies. J Hypertens. (2016) 34(7):1237–48. doi: 10.1097/HJH.0000000000000921
3. Chi C, Lu Y, Zhou Y, Li J, Xu Y, Zhang Y. Factors that may impact the noninvasive measurement of central blood pressure compared to invasive measurement: the MATCHY study. J Pers Med. (2022) 12(9):1482. doi: 10.3390/jpm12091482
4. Jedrzejewski D, McFarlane E, Lacy PS, Williams B. Pulse wave calibration and implications for blood pressure measurement: systematic review and meta-analysis. Hypertension. (2021) 78(2):360–71. doi: 10.1161/HYPERTENSIONAHA.120.16817
5. Díaz A, Bia D. Association between central-peripheral blood pressure amplification and structural and functional cardiac properties in children, adolescents, and adults: impact of the amplification parameter, recording system and calibration scheme. High Blood Press Cardiovas Prev. (2021) 28(2):185–249. doi: 10.1007/s40292-021-00440-2
6. Papaioannou TG, Lekakis JP, Karatzis EN, Papamichael CM, Stamatelopoulos KS, Protogerou AD, et al. Transmission of calibration errors (input) by generalized transfer functions to the aortic pressures (output) at different hemodynamic states. Int J Cardiol. (2006) 110(1):46–52. doi: 10.1016/j.ijcard.2005.07.014
7. Nakagomi A, Okada S, Shoji T, Kobayashi Y. Comparison of invasive and brachial cuff-based noninvasive measurements for the assessment of blood pressure amplification. Hypertens Res. (2017) 40(3):237–42. doi: 10.1038/hr.2016.132
8. Weber T, Wassertheurer S, Rammer M, Maurer E, Hametner B, Mayer CC, et al. Validation of a brachial cuff-based method for estimating central systolic blood pressure. Hypertension. (2011) 58(5):825–32. doi: 10.1161/HYPERTENSIONAHA.111.176313
9. Wassertheurer S, Hametner B, Mayer CC, Hafez A, Negishi K, Papaioannou TG, et al. Aortic systolic pressure derived with different calibration methods: associations to brachial systolic pressure in the general population. Blood Press Monit. (2018) 23(3):134–40. doi: 10.1097/MBP.0000000000000319
10. Diaz A, Zócalo Y, Salazar F, Bia D. Non-invasive central aortic pressure measurement: what limits its application in clinical practice? Front Cardiovasc Med. (2023) 10:1159433. doi: 10.3389/fcvm.2023.1159433
11. Chemla D, Millasseau S, Hamzaoui O, Teboul JL, Monnet X, Michard F, et al. New method to estimate central systolic blood pressure from peripheral pressure: a proof of concept and validation study. Front Cardiovasc Med. (2021) 8:772613. doi: 10.3389/fcvm.2021.772613
12. Bia D, Zócalo Y, Sánchez R, Torrado JF, Lev G, Mendiz O, et al. Brachial blood pressure invasively and non-invasively obtained using oscillometry and applanation tonometry: impact of mean blood pressure equations and calibration schemes on agreement levels. J Cardiovasc Dev Dis. (2023) 10(2):45. doi: 10.3390/jcdd10020045
13. Laugesen E, Rossen NB, Peters CD, Mæng M, Ebbehøj E, Knudsen ST, et al. Assessment of central blood pressure in patients with type 2 diabetes: a comparison between SphygmoCor and invasively measured values. Am J Hypertens. (2014) 27(2):169–76. doi: 10.1093/ajh/hpt195
14. Mahieu D, Kips J, Rietzschel ER, De Buyzere ML, Verbeke F, Gillebert TC, et al. Noninvasive assessment of central and peripheral arterial pressure (waveforms): implications of calibration methods. J Hypertens. (2010) 28(2):300–5. doi: 10.1097/HJH.0b013e3283340a1a
15. Papaioannou TG, Protogerou AD, Vrachatis D, Konstantonis G, Aissopou E, Argyris A, et al. Mean arterial pressure values calculated using seven different methods and their associations with target organ deterioration in a single-center study of 1878 individuals. Hypertens Res. (2016) 39(9):640–7. doi: 10.1038/hr.2016.41
16. Díaz A, Bia D, Zócalo Y. Impact of methodological and calibration approach on the association of central and peripheral systolic blood pressure with cardiac structure and function in children, adolescents and adults. High Blood Press Cardiovasc Prev. (2019) 26(6):509–34. doi: 10.1007/s40292-019-00346-0
17. Sharman JE, Avolio AP, Baulmann J, Benetos A, Blacher J, Blizzard CL, et al. Validation of non-invasive central blood pressure devices: aRTERY society task force consensus statement on protocol standardization. Eur Heart J. (2017) 38(37):2805–12. doi: 10.1093/eurheartj/ehw632
18. Zócalo Y, Bia D. Sex- and age-related physiological profiles for brachial, vertebral, carotid, and femoral arteries blood flow velocity parameters during growth and aging (4–76 years): comparison with clinical cut-off levels. Front Physiol. (2021) 12:729309. doi: 10.3389/fphys.2021.729309
19. Zócalo Y, Bia D. Age- and sex-related profiles for macro, macro/micro and microvascular reactivity indexes: association between indexes and normative data from 2609 healthy subjects (3–85 years). PLoS One. (2021) 16(7):e0254869. doi: 10.1371/journal.pone.0254869
20. Zócalo Y, Bia D. Central pressure waveform-derived indexes obtained from carotid and radial tonometry and brachial oscillometry in healthy subjects (2–84 y): age-, height-, and sex-related profiles and analysis of indexes agreement. Front Physiol. (2022) 12:774390. doi: 10.3389/fphys.2021.774390
21. Zócalo Y, García-Espinosa V, Castro JM, Zinoveev A, Marin M, Chiesa P, et al. Stroke volume and cardiac output non-invasive monitoring based on brachial oscillometry-derived pulse contour analysis: explanatory variables and reference intervals throughout life (3–88 years). Cardiol J. (2021) 6:864–78. doi: 10.5603/CJ.a2020.0031
22. Bia D, Zócalo Y. Physiological age- and sex-related profiles for local (aortic) and regional (carotid-femoral, carotid-radial) pulse wave velocity and center-to-periphery stiffness gradient, with and without blood pressure adjustments: reference intervals and greement between methods in healthy subjects (3–84 years). J Cardiovasc Dev Dis. (2021) 8(1):3. doi: 10.3390/jcdd8010003
23. Diaz A, Zócalo Y, Bia D, Wray S, Fischer EC. Reference intervals and percentiles for carotid-femoral pulse wave velocity in a healthy population aged between 9 and 87 years. J Clin Hypertens. (2018) 20(4):659–71. doi: 10.1111/jch.13251
24. Zinoveev A, Castro JM, García-Espinosa V, Marin M, Chiesa P, Bia D, et al. Aortic pressure and forward and backward wave components in children, adolescents and young-adults: agreement between brachial oscillometry, radial and carotid tonometry data and analysis of factors associated with their differences. PLoS One. (2019) 14(12):e0226709. doi: 10.1371/journal.pone.0226709
25. García-Espinosa V, Curcio S, Marotta M, Castro JM, Arana M, Peluso G, et al. Changes in central aortic pressure levels, wave components and determinants associated with high peripheral blood pressure states in childhood: analysis of hypertensive phenotype. Pediatr Cardiol. (2016) 37(7):1340–50. doi: 10.1007/s00246-016-1440-5
26. Agnoletti D, Zhang Y, Salvi P, Borghi C, Topouchian J, Safar ME, et al. Pulse pressure amplification, pressure waveform calibration and clinical applications. Atherosclerosis. (2012) 224(1):108–12. doi: 10.1016/j.atherosclerosis.2012.06.055
27. Chemla D, Antony I, Zamani K, Nitenberg A. Mean aortic pressure is the geometric mean of systolic and diastolic aortic pressure in resting humans. J Appl Physiol (1985). (2005) 99(6):2278–84. doi: 10.1152/japplphysiol.00713.2005
28. O'Brien E, Pickering T, Asmar R, Myers M, Parati G, Staessen J, et al. Working group on blood pressure monitoring of the European society of hypertension international protocol for validation of blood pressure measuring devices in adults. Blood Press Monit. (2002) 7(1):3–17. doi: 10.1097/00126097-200202000-00002
29. Evans JD. Straightforward statistics for the behavioral sciences. Pacific Grove, CA: Brooks-Cole Publishing (1996).
30. Lumley T, Diehr P, Emerson S, Chen L. The importance of the normality assumption in large public health data sets. Annu Rev Public Health. (2002) 23:151–69. doi: 10.1146/annurev.publhealth.23.100901.140546
31. Castro JM, García-Espinosa V, Curcio S, Arana M, Chiesa P, Giachetto G, et al. Childhood obesity associates haemodynamic and vascular changes that result in increased central aortic pressure with augmented incident and reflected wave components, without changes in peripheral amplification. Int J Vasc Med. (2016) 2016:3129304. doi: 10.1155/2016/3129304
32. Garcia-Espinosa V, Bia D, Castro J, Zinoveev A, Marin M, Giachetto G, et al. Peripheral and central aortic pressure, wave-derived reflection parameters, local and regional arterial stiffness and structural parameters in children and adolescents: impact of body mass index variations. High Blood Press Cardiovasc Prev. (2018) 25(3):267–80. doi: 10.1007/s40292-018-0264-1
33. Peluso G, García-Espinosa V, Curcio S, Marota M, Castro J, Chiesa P, et al. High central aortic rather than brachial blood pressure is associated with carotid wall remodeling and increased arterial stiffness in childhood. High Blood Press Cardiovasc Prev. (2017) 24(1):49–60. doi: 10.1007/s40292-017-0179-2
34. Bia D, Zócalo Y, Armentano R, Camus J, Forteza E, Cabrera-Fischer E. Increased reversal and oscillatory shear stress cause smooth muscle contraction-dependent changes in sheep aortic dynamics: role in aortic balloon pump circulatory support. Acta Physiol. (2008) 192(4):487–503. doi: 10.1111/j.1748-1716.2007.01765.x
35. Curcio S, García-Espinosa V, Arana M, Farro I, Chiesa P, Giachetto G, et al. Growing-related changes in arterial properties of healthy children, adolescents, and young adults nonexposed to cardiovascular risk factors: analysis of gender-related differences. Int J Hypertens. (2016) 2016:4982676. doi: 10.1155/2016/4982676
36. Picone DS, Schultz MG, Hughes AD, Sharman JE. Cuff under pressure for greater accuracy. Curr Hypertens Rep. (2020) 22(11):93. doi: 10.1007/s11906-020-01103-8
Keywords: aortic pressure, brachial blood pressure, catheterism, invasive records, non-invasive records, oscillometry, physiological measurements, human physiology
Citation: Bia D, Salazar F, Cinca L, Gutierrez M, Facta A, Zócalo Y and Diaz A (2023) Direct estimation of central aortic pressure from measured or quantified mean and diastolic brachial blood pressure: agreement with invasive records. Front. Cardiovasc. Med. 10:1207069. doi: 10.3389/fcvm.2023.1207069
Received: 17 April 2023; Accepted: 3 July 2023;
Published: 25 July 2023.
Edited by:
Gregor Theilmeier, University of Oldenburg, GermanyReviewed by:
Audrey Adji, Victor Chang Cardiac Research Institute, AustraliaGiuliano Tocci, Sapienza University of Rome, Italy
© 2023 Bia, Salazar, Cinca, Gutierrez, Facta, Zócalo and Diaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel Bia dbia.santana@gmail.com dbia@fmed.edu.uy
Abbreviations aoBP, central aortic blood pressure; aoSBP, central aortic systolic blood pressure; bBP, brachial artery blood pressure; bDBP, brachial artery diastolic blood pressure; bDBPosc, brachial artery diastolic blood pressure obtained with the oscillometric system; bMBP, brachial artery mean blood pressure; bMBPosc, brachial artery mean blood pressure obtained with the oscillometric system; BP, blood pressure; bPP, brachial artery pulse pressure; bPPosc, brachial artery pulse pressure obtained with the oscillometric system; bSBP, brachial artery systolic blood pressure; bSBPosc, brachial artery systolic blood pressure obtained with the oscillometric system; CCC, Lin's concordance correlation coefficient; DCBP, direct central blood pressure; FF, form factor; HR, heart rate; MBP, mean blood pressure; MOG, Mobil-O-Graph: oscillometry/plethysmography.