 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Maitham Ali Kadhem 1* , Mohammed Alfardan2, Maryam Fadhel Hammad3
, Mohammed Alfardan2, Maryam Fadhel Hammad3
1Department of Ophthalmology, Government Hospitals, Salmaniya Medical Complex, Manama, Kingdom of Bahrain.
2Department of Surgery, Government Hospitals, Salmaniya Medical Complex, Manama, Kingdom of Bahrain.
3Department of Pathology, Government Hospitals, Salmaniya Medical Complex, Kingdom of Bahrain.
Correspondence to: Maitham Ali Kadhem, Department of Ophthalmology, Government Hospitals, Salmaniya Medical Complex, Manama, Kingdom of Bahrain.
Received date: February 11, 2023; Accepted date: February 26, 2023; Published date: March 06, 2023
Citation: Kadhem MA, Alfardan M, Hammad MF. Patterns of Corneal Disorders in Corneal Button Specimens: Descriptive Study in a Tertiary Referral Hospital in Bahrain. J Med Res Surg. 2023;4(1):17-21. doi: 10.52916/jmrs234100
Copyright: ©2023 Kadhem MA, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Introduction: Corneal injuries and disorders are among the commonest clinical scenarios that are encountered in the ophthalmology clinical practice. Penetrating Keratoplasty (PKP) surgeries count for the most frequent efficient surgical management of diseased corneas. The latter are usually sent as button specimens for histopathology examination for further describing the pattern of the corneal disorders. Aims and Objectives: The aims of this study are to discuss the rate of Penetrating Keratoplasty (PKP) surgeries in SMC in 6 years interval (2016-2022) along with to determine the most common histopathological and microbiological diagnosis of corneal specimens from Penetrating Keratoplasty (PKP) and to study the clinical spectrum with age and sex distribution of corneal disorders in Bahrain alongside correlation with the comorbidities and the pathological diagnosis. Patients and Methods: It is a retrospective analysis of one-hundred and one histopathology reports of corneal button specimens at Salmaniya medical complex during the last 6 years (1-1-2016 till 31-3-2022). Medical records, surgical notes and histopathology reports of patients were retrieved from ISEHA system. Statistical analysis was done using Microsoft Excel 2019. Results: Corneal scarring (44%) was the most common pathological diagnosis, followed by Keratoconus (KC) (15%), acute keratitis (14%), degeneration (9%), chronic keratitis with fibrosis (5%), decompensated cornea and failed graft (5%), pseudophakic bullous keratopathy (3%) and herpetic keratitis (3%). There was Bahraini nationality (98%) and male preponderance (66%). The most common age group affected was 70–79 years with the median age of 51.5 year. Conclusion: Our study shows the importance of determining the most common histological diagnoses of corneal button specimens along with the correlation of the latter with the age, gender, surgical complications and systemic comorbidities. Knowing the exact pathology of the diseased cornea would assist in providing the proper post-operative management and to avoid possible elements that could promote complications.
Keratoconus, Bullous keratopathies, Corneal graft, Keratitis, Cornea transplant, Keratoplasty
Globally, at least 2.2 billion people have a near or distance vision impairment. In at least 1 billion–or almost half–of these cases, vision impairment could have been prevented or has yet to be addressed. According to WHO, Corneal diseases (4.2 million) leading to corneal blindness is the fourth common cause of blindness in the world, after uncorrected refractive errors, cataract and glaucoma [1]. Corneal transplantation is considered the most common transplant surgery in the world. However, its success depends on the health of the ocular surface and the intact immune privilege of the eye. In the absence of these two conditions, corneal transplants have an increased failure rate and result in corneal blindness. Corneal injuries and disorders vary with different age groups, previous corneal insults and systemic co-morbidities. These corneal injuries are among the commonest clinical scenarios that are encountered in the ophthalmology clinical practice. Penetrating Keratoplasty (PKP) surgeries count for the most frequent efficient surgical management of diseased corneas. The latter is usually sent as button specimens for histopathology examination for further describing the pattern of the corneal disorders. Corneal button specimens are the most common ophthalmic tissue specimens sent for histopathology lab for evaluation of the pattern of the disorder, confirm a possible infection or further sub-classify the type of its injury.
This is a retrospective analysis of all histopathology reports of corneal button specimens at the main tertiary governmental hospital in the Kingdom of Bahrain-Salmaniya. Medical complex during the last 6 years (1-1-2016 till 31-3-2022). Medical records of patients, surgical notes and histopathology reports were all retrieved from ISEHA system. The latter were assessed with respect to demographic information, surgical indication of PKP, and histopathology reports of the diseased cornea. Statistical analysis was done using mean, proportion, and percentage with the assistance of Microsoft Excel 2019.
One hundred and one patients were included in the study. There was Bahraini nationality (98%) and male preponderance (66%). The most common age group affected was 70–79 years with the median age of 51.5 year. Most surgical specimen type was received as corneal button from the right eye (55%) while the left eye corneas accounted for( 45%) of the specimens received. In our study, Corneal scarring (44%) was the most common pathological diagnosis, followed by Keratoconus (KC) (15%), acute keratitis (14%), degeneration (9%), chronic keratitis with fibrosis (5%), decompensated cornea and failed graft (6%), Pseudophakic Bullous Keratopathy (3%) and herpetic keratitis (3%) (Table 1) and (Figure1).
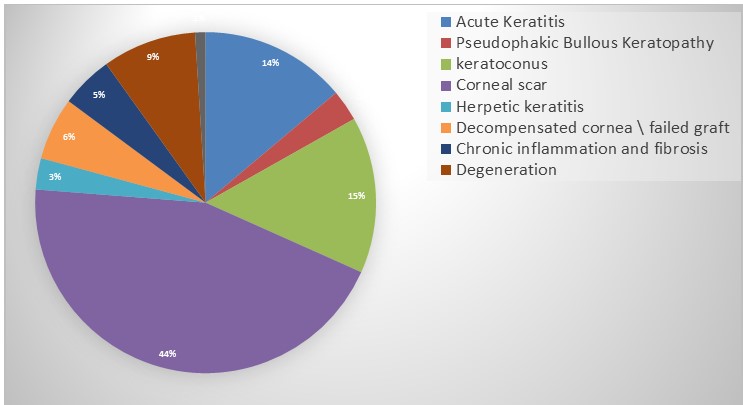 Figure 1: Distribution of the number of patients according to pathological diagnosis done on the cornea button specimens.
Figure 1: Distribution of the number of patients according to pathological diagnosis done on the cornea button specimens.|
Corneal Pathology |
Number of cases |
|
Acute Keratitis |
14 |
|
Pseudophakic bullous keratopathy |
3 |
|
Keratoconus |
15 |
|
Corneal scar |
45 |
|
Herpetic keratitis |
3 |
|
Decompensated cornea \ failed graft |
6 |
|
Chronic inflammation and fibrosis |
5 |
|
Degeneration |
9 |
|
Inadequate |
1 |
|
Total |
101 |
In our study, when comparing the most common corneal pathology in certain age group, we found that in the younger age groups, keratoconus was the most common pathology diagnosed in patients 40 years and younger. It accounted for 11 cases (73.3%). On the other hand, in the other extreme of age, corneal scarring was the most common pathology diagnosed. It accounts for the majority of corneal pathology diagnosis in patients above 50 years. The percentage of corneal scarring in these patients reached 84.4% of total cases diagnosed with corneal scars (Figure 2).
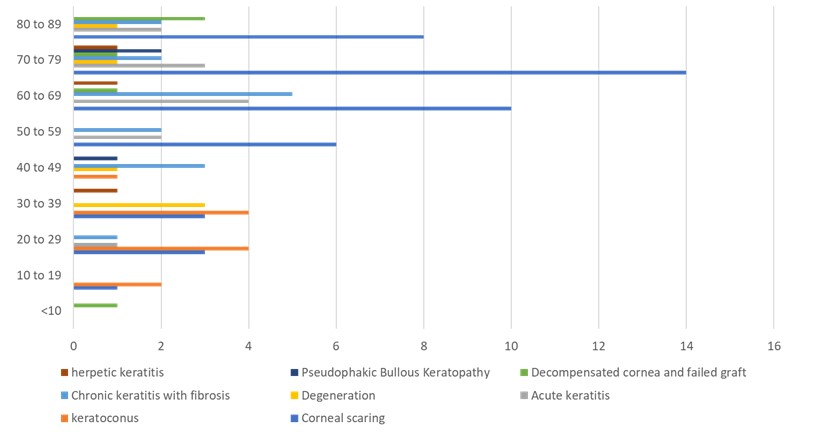 Figure 2: Distribution of the number of patients according to age group.
Figure 2: Distribution of the number of patients according to age group.Other pathologies of the cornea which were included in our study such as acute and chronic keratitis, Pseudophakic bullous keratopathy, decompensated cornea associated with failed pathological diagnosis, followed by Keratoconus (KC) (15%), acute keratitis (14%), degeneration (9%), chronic keratitis with fibrosis (5%), decompensated cornea and failed graft (6%), Pseudophakic Bullous Keratopathy (3%) and herpetic keratitis (3%) (Table 1) and (Figure1). graft, corneal degeneration and infective keratitis with herpes virus did not show any age group or sex predilection. When correlating the corneal pathologies with the systemic co-morbidities that most of the patients suffered from, we found that the majority of our subjects were diabetics and hypertensives. These co-morbidities were the highest in the patients with advanced age.
The cornea is resilient and can typically heal from minor abrasions. However, major corneal damage can result in a corneal scar [1,2]. These can be caused by improper use of contact lenses, deep lacerations, burns, and some diseases like trachoma, shingles and syphilis. After major damage, clear corneal tissue may be replaced by scar tissue or become occluded by new blood vessels (neovascularization). These corneal scars can severely impair the vision [2]. Our study highlights the most common patterns of corneal pathology encountered at our hospital following Penetrating Keratoplasty (PKP) surgeries. Which also reflects the indications of the latter. In a previous study assessing the most common indications of Penetrating Keratoplasty (PKP) surgeries among Bahraini population old trachoma with corneal scaring was the second most indication. In our study, corneal scarring was by far the most common pathological pattern of corneal diseases included in the study [1,2]. Interestingly, studies in Asia and Africa also showed similar results [2]. Histologically, corneal scar is evident as a focal absence of keratocytes and an obliteration of corneal lamellae. Granulation tissue can be seen in early scars. However, stromal fibrosis is the most common pathological feature in chronic, well-organized scar tissue. There are other conditions that can give the same histological picture of corneal scar under the microscope. These conditions include Corneal decompensation arising from a non-functional graft or from endothelial diseases such as Fuchs endothelial dystrophy [3] and pseudophakic bullous keratopathy (Figure 3) [4]. The latter which is also known as Pseudophakic Corneal Edema (PCE) traditionally refers to the development of irreversible corneal edema after cataract surgery and Intraocular Lens (IOL) implantation [4,5]. Initially, there is endothelial trauma, which is followed by progressive stromal and epithelial edema. The epithelial edema results in the formation of bullae. If severe or chronic enough, pseudophakic bullous keratopathy may lead to anterior corneal fibrosis and scarring. In these conditions, the clinical and the surgical history of the patient is very important to correlate with the histopathology findings seen in the corneal button specimens [5,6]. Pseudophakic bullous keratopathy was forming 13% of the indicated PKP cases in the era prior to our study according to a previous study ( 1999-2016 ) which was proposed due to learning curve of phacoemulsification, as phacoemulsification was first introduced in Salmaniya medical complex in 1996. Moreover during covid pandemic elective cataract extraction procedures were stopped, leading to significantly reduced number of aphakic or Pseudophakic bullous keratopathy. The second most common pathological diagnosis of the resected corneas in our study was keratoconus. Keratoconus (KC) is a disorder of the eye that results in progressive thinning of the cornea. This may result in blurry vision, double vision, nearsightedness, irregular astigmatism, and light sensitivity leading to poor quality-of-life. Usually both eyes are affected [6]. This condition occurs in most instances in the first two decades of life. This is apparent from our results that shows a rise in keratoconus pathological pattern in patients 20-30 years old and younger. In comparison to a previous study held in Bahrain, it was showing keratoconus as the leading indication, with 33%, while our data showing 15% of the total number, which could be due to early detection of corneal changes with the wildly use of pentacam and corneal collagen cross linking to stop progression to advanced disease requiring surgical intervention. In 2016, the US Food and Drug Administration approved riboflavin ophthalmic solution cross-linking based on three 12-month clinical trials.
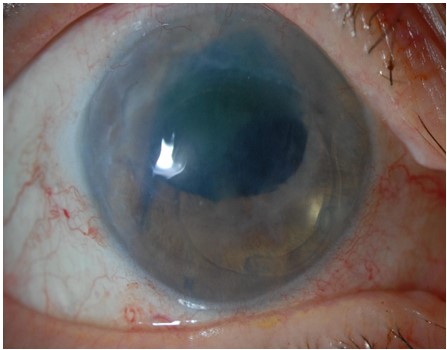 Figure 3: Pseudophakic bullous keratopathy secondary to anterior chamber intraocular lens. Image courtesy of Dr. Hall Chew, MD[4].
Figure 3: Pseudophakic bullous keratopathy secondary to anterior chamber intraocular lens. Image courtesy of Dr. Hall Chew, MD[4].In our study, acute and chronic keratitis including herpetic keratitis cumulatively accounted for around 22% of the corneal pathologies included in the study. Which shows discrepancy with the published international studies found in the literature [7-9]. In general, keratitis could be infective and non-infective. Differentiating between them is crucial in managing both. Careful clinical examination, aided by laboratory investigations, could help in correct diagnosis and proper management [10,11]. Even-though both conditions may involve all age groups, infective keratitis occurs more frequently in children and adults [12,13]. Infective and non-infective keratitis may overlap each other. Non-infective keratitis may become infective by pathogenic or nonpathogenic microbes and may result in sight-threatening complications [14,15]. Infective keratitis could also be suppurative and non-suppurative. Suppurative keratitis is frequently caused by bacteria and fungi. Non-suppurative infective keratitis could be viral, spirochaetal or parasitic [16,17]. Among the infective keratitis corneal buttons, we found the commonest organism to be : Herptic keratitis. Herpetic keratitis were diagnosed in 3 patients in our study. This form of infective keratitis is a form of keratitis caused by recurrent Herpes Simplex Virus (HSV) infection in the cornea [18,19]. It begins with infection of epithelial cells on the surface of the eye and retrograde infection of nerves serving the cornea [20]. Primary infection typically presents as swelling of the conjunctiva and eyelids (blepharoconjunctivitis), accompanied by small white itchy lesions on the corneal surface. The effect of the lesions varies, from minor damage to the epithelium (superficial punctate keratitis), to more serious consequences such as the formation of dendritic ulcers [21,22]. To get a definite diagnosis, Corneal smears or impression cytology specimens can be analyzed by culture, antigen detection, or fluorescent antibody testing. Tzanck smear, i.e.Papanicolaou staining of corneal smears. This will show multi-nucleated giant cells and intranuclear inclusion bodies, however, the test is low in sensitivity and specificity [23,24].
Our study shows the importance of determining the most common histological diagnoses of corneal button specimens along with the correlation of the latter with the age group, gender and systemic co-morbidities. We concluded that there was male preponderance among our patients. According to age-grouped distribution we had two main age-group related pathologies. Corneal scarring was the most common corneal pathology diagnosed in the older age group. While keratoconus was the second most common pathological pattern overall and it was more frequently diagnosed in the younger age groups. Knowing the exact pathology of the diseased cornea would assist in providing the proper post-operative management and to avoid possible elements that could promote complications.
All data collection and analysis in the study were in accordance with the ethical standards of the national research committee.
Research data supporting this publication are available from I-SEHA system–Government hospitals–Salmaniya Medical Complex–Kingdom of Bahrain.
The authors declare that they have NO affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript.
The consent was taken from the patient.
The study was not supported by grant from any foundation. Authors supported themselves personally
Dr. Maitham Ali Kadhem contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript. Dr. Mohammad Al Fardan and Dr. Maryam Hammad contributed to the data collection and analysis of the research.

