 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Brian Monaisa1, Sibusiso Phiri1, Elias Ndobe1
1University of the Witwatersrand, Johannesburg, South Africa
Correspondence to: Brian Monaisa, University of the Witwatersrand, Johannesburg, South Africa;
E-mail: brian@livereality.co.za
Received date: July 27, 2020; Accepted date: August 7, 2020; Published date: August 14, 2020
Citation: Monaisa B, Phiri S, Ndobe E (2020) Paediatric Elbow Flexion Reconstruction with the Latissimus Dorsi Muscle Flap, Case Report and Literature Review. J
Med Res Surg. 1(4): pp. 1-3.
Copyright: ©2020 Monaisa B, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
We have conducted two latissimus dorsi transfers for elbow function reconstruction in paediatric patients at Chris Hani Baragwanath Academic Hospital. The first patient was a four-year-old girl with distal, asymmetric arthrogryposis, involving the shoulder, elbow, and wrist. The second patient was a five-year-old boy with paediatric brachial plexus injury, with C5 and C6 root avulsions with an inability to flex the elbow, as well as a glenohumeral contracture. He presented following a rotational humerus osteotomy. We performed a unipolar latissimus dorsi transfer in both patients with good results. We also performed a literature review to compare the available methods of elbow flexion reconstruction, especially in paediatric cases. We believe that the latissimus dorsi transfer is the preferred muscle transfer for reconstructing elbow function and the literature review supports this assertion.
Latissimus dorsi, Elbow, Nerve, Muscle, Elbow flexion
The elbow joint is essential for carrying out activities of daily living. As a hinge joint, it is essential for positioning the hand in space to reach the face, torso, and perineum. Eating, bathing, and getting dressed all become difficult to achieve without a functional elbow [1]. Inability to flex the elbow results in severe loss of function and learning of maladaptive behaviors. Restoration of elbow flexion is therefore a priority and the timing of surgery depends on the cause of the defect. Loss of elbow function in paediatric cases may be congenital, secondary to birth trauma to the Brachial Plexus (BPI), or due to neuromuscular degeneration, as seen in poliomyelitis. The commonest congenital cause of the inability to flex the elbow is arthrogryposis. BPI should be addressed early, with nerve transfers between 6 to 9 months. Failure to address the BPI early results in a progressive deformity of the shoulder joint. Missed cases may present later, at a time when the possibility of nerve transfers have been lost due to motor endplate degeneration. Regardless of the etiology, it is best to address the defect before the child starts school, at around 4 to 5 years of age
Arthrogryposis is derived from the Greek words Arthro=Joints and Grypos=Stiff. It refers to joint contractures that are present at birth. Multiple forms of arthrogryposis vary in clinical features, severity, and the number of involved joints. The joint contractures are secondary to a lack of motion during fetal life. Multiple processes can lead to a lack of fetal limb movement, including muscle abnormalities, nerve anomalies, restricted intrauterine space, vascular insufficiency, and maternal illness. The elbow is frequently the most problematic joint in children with arthrogryposis. Lack of flexion is the common impairment, and it prohibits hand-to-mouth function and many daily tasks. The first goal is the restoration of passive motion. Adequate passive flexion allows the hand to be placed near the face with the use of tabletop or adaptive equipment. Passive flexion is a prerequisite for active motion. Treatment goals and principles include the release of joint contractures; increase relative tendon length, and provide appropriate motors for the joints by judicious tendon transfers (Figure 1).
 Figure 1:Good passive range of motion in the left elbow of TM
(arthrogryposis).
Figure 1:Good passive range of motion in the left elbow of TM
(arthrogryposis).TM presents with atypical, distal arthrogryposis, which is also asymmetrical. She can flex her right elbow and has developed more strength on the right side of her body. Her left elbow has good passive elbow flexion but no active flexion. Often the latissimus dorsi is also affected in arthrogryposis and unavailable for use. If available, the latissimus dorsi is the first choice for the restoration of active flexion of the elbow [2]. Examination of the latissimus in our patient showed that it was weaker than the contralateral latissimus, but was able to act against resistance (M4), and chosen as the donor’s muscle (Figure 2 and 3)
 Figure 2: Good passive range of motion in the left elbow of TM
(arthrogryposis).
Figure 2: Good passive range of motion in the left elbow of TM
(arthrogryposis). Figure 3: Results 12 weeks post-op, showing good active elbow flexion.
Figure 3: Results 12 weeks post-op, showing good active elbow flexion.Brachial plexus birth palsy has an incidence of 0.5 to 2 per 1000 live births. Perinatal risk factors for brachial plexus palsy include large-for-gestational-age infants, multiparous pregnancies, prolonged labour, assisted (vacuum or forceps), and cephalopelvic disproportion. Most commonly, brachial plexus birth palsy involves the upper trunk (C5 and C6), potentially in combination with an injury to C7; or, less often, the entire plexus (C5 to T1) is injured. Management of these depends on adequate diagnosis and timeous intervention [3].
The commonest defect is a C5, C6 injury, presenting with a flail shoulder, and inability to flex the elbow. The child, who tires of having to use the other hand to position the affected limb, also neglects the affected arm. If diagnosed early, BPI is reliably treated with nerve transfers at around 6 to 9 months of age. Missed/untreated BPI develops a progressive contracture of the glenohumeral joint, with shoulder and flexor muscle atrophy. Delayed presentation is treated with muscle transfers (Figure 4 and 5).
 Figure 4: Position and markings of the resting muscle length, with the
shoulder abducted to 110 degrees, markings are made 2 cm apart on the
muscle, and replicated with the elbow at 110 degrees at inset.
Figure 4: Position and markings of the resting muscle length, with the
shoulder abducted to 110 degrees, markings are made 2 cm apart on the
muscle, and replicated with the elbow at 110 degrees at inset.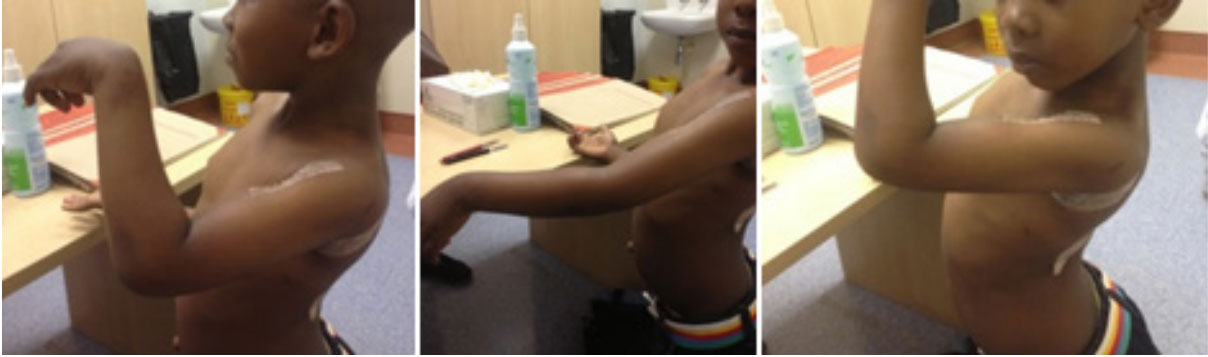 Figure 5: Early (8 weeks) exercises with gravity eliminated.
Figure 5: Early (8 weeks) exercises with gravity eliminated.
The selection of the donor muscle in BPI is dependent on examining the child and choosing between pedicled transfer of the pectoralis major or latissimus dorsi, Steindler flexorplasty, or a free muscle transfer. Because of the innervation of the pectoralis major and the latissimus dorsi, it is important to make sure the donor muscles have adequate power [4].
The goals of treatment are to restore elbow flexion with a range of motion that will allow the hand to reach the face. Grade M3 or M4 power should be attainable, so ideally the donor muscle should have at least M4 power before transfer [4] The gain in function from the transfer should outweigh any deficits caused by muscle transfer. There should be a reasonable time to recovery useful functions. Recovery is a time-consuming process and involves extensive rehabilitation, with intense involvement of occupational therapists. For this reason, muscle transfers are best undertaken in patients that are cognitive and motivated to participate in the process. In paediatric cases, it means waiting until the child is at least four years old.
TThe choice of pedicled muscle transfer is between pectoralis major, pectoralis minor, triceps transfer, Steindler flexorplasty, and the latissimus dorsi. The number of available transfers points to the variable results seen, and the lack of a perfect donor. A review of the literature points to the many advantages of the latissimus dorsi and is the first choice if available. The pectoralis muscle is a reliable transfer but often needs the addition of a fascial graft to reach the biceps tendon. Transferring the pectoralis major involves surgery to the chest, with risk of injury to the breast bud. A stable shoulder is a prerequisite, and the ability to hold objects against the body may be lost. The pectoralis minor is associated with le
Transfer of the triceps is popular in treating arthrogryposis, due to its dual effect of releasing extension contracture and providing flexor motors. Drawbacks include a high risk of flexion contracture and loss of elbow extension [4]. Steindler flexorplasty is the transfer of the common flexor tendon from the medial epicondyle to a point more proximal on the humerus. This results in flexion of the elbow at the same time as flexion of the digits, and Brunelli modified it by excluding flexor digitorum superficialis to avoid this. Other drawbacks include the limited strength gains, as well as the resultant elbow flexion contracture. Eggers et al place the Steindler flexorplasty as their backup option, should the latissimus be unavailable for transfer [5].
The latissimus dorsi muscle is the largest in the body and can provide adequate power for elbow flexion. It may be transferred as either a unipolar or a bipolar transfer [6]. The unipolar transfer involves transferring the muscle origins to the biceps tendon while leaving the insertion in situ, while bipolar transfer involves transferring the insertion onto the coracoid, to more accurately imitate the biceps excursion. Bipolar transfer does result in greater degree of flexion at the elbow but with a significant loss of power. The unipolar transfer is reliable, simple, and effective in returning power to the elbow joint [5].
Several authors have compared the various donor muscles, with the latissimus dorsi proving to be most reliable. Chuang compared Steindler flexorplasty, latissimus dorsi and free gracilis transfer and found that all three reliably gave at least M3 power [4]. Eggers et al [5], and Berger and Brenner (4) independentlyflexion. Marshall et al, showed good reliability of the latissimus transfer, with all of the patients in their stud achieving good or fair results [4].y
we would like to reiterate that the latissimus dorsi is a reliable muscle transfer for restoring elbow flexion in paediatric patients. Restoration of elbow flexion has a good impact on the quality of life and should be performed before the child starts school.

