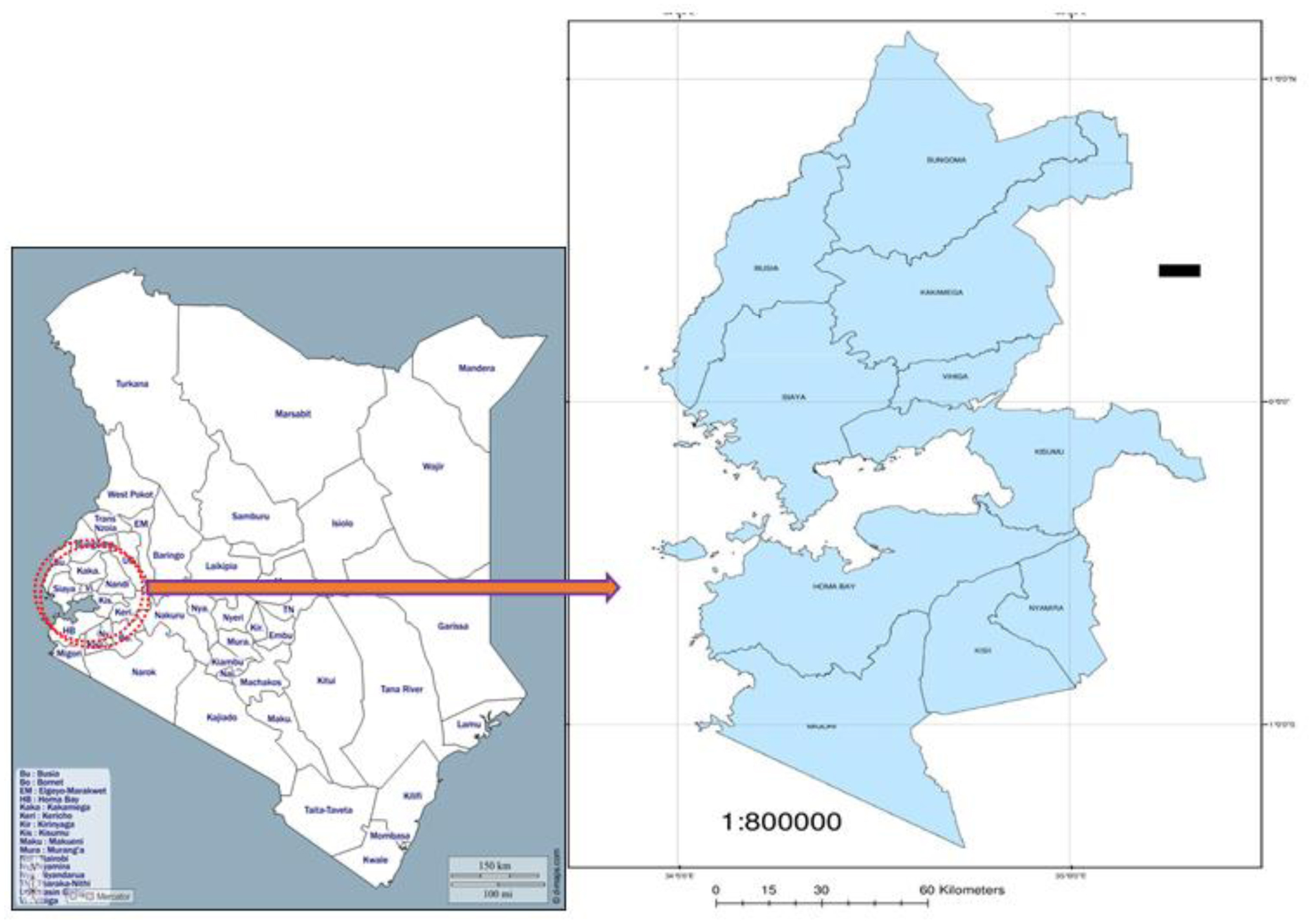
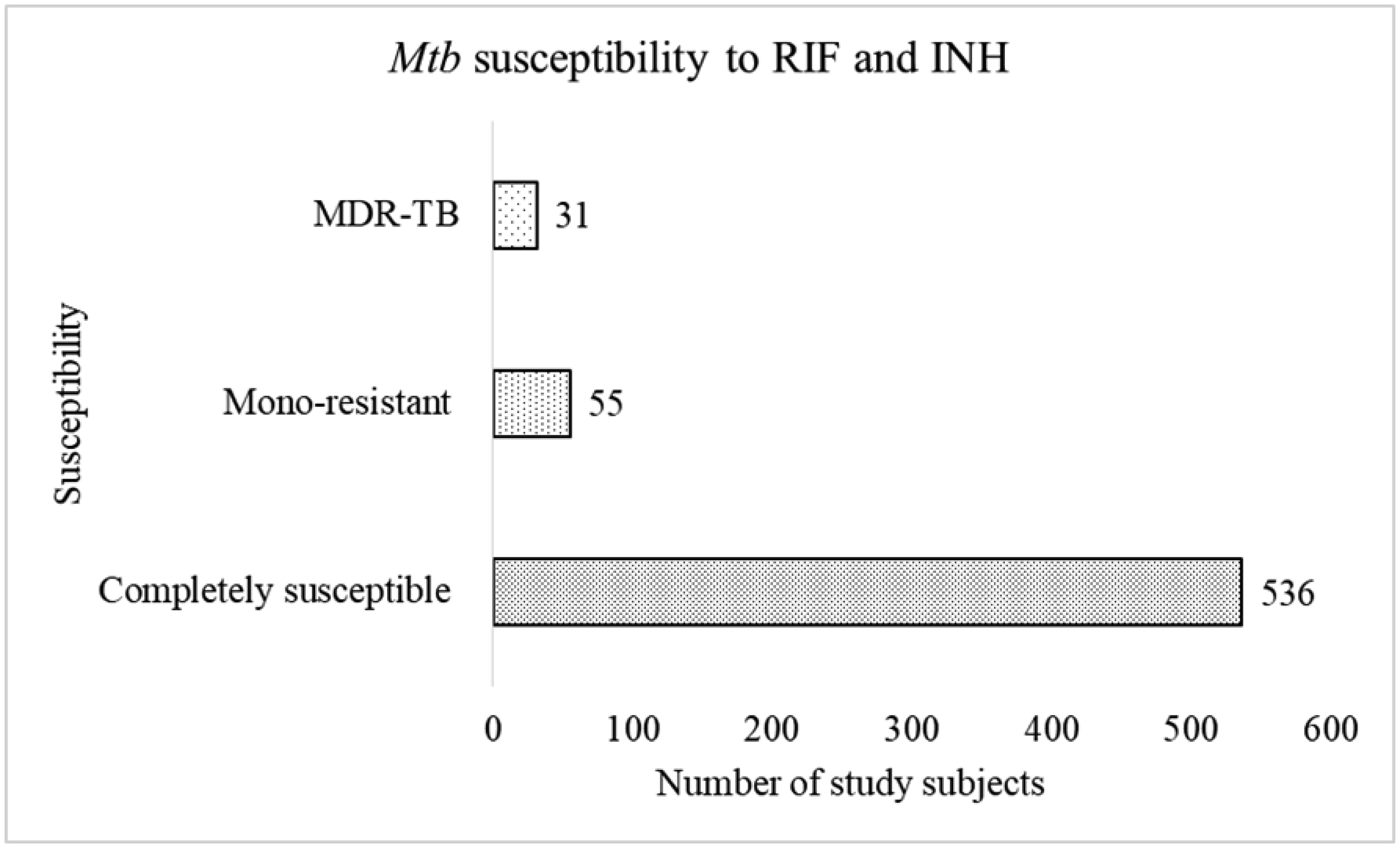
Multidrug-resistant tuberculosis (TB) (MDR-TB), or TB that is simultaneously resistant to both isoniazid (INH) and rifampicin (RIF), is a barrier to successful TB control and treatment. Stratified data on MDR-TB, particularly in the high-burden western Kenya region, remain unknown. This data is important to monitor the efficacy of TB control and treatment efforts. Herein, we determined the molecular epidemiology of drug-resistant TB and associated risk factors in western Kenya. This was a non-experimental, population-based, cross-sectional study conducted between January and August 2018. Morning sputum samples of individuals suspected of pulmonary TB were collected, processed, and screened for Mycobacterium tuberculosis (Mtb) and drug resistance using line probe assay (LPA) and Mycobacterium growth indicator tubes (MGIT) culture. MGIT-positive samples were cultured on brain heart infusion (BHII) agar media, and the presence of Mtb was validated using Immunochromatographic assay (ICA). Drug sensitivity was performed on MGIT and ICA-positive but BHI-negative samples. Statistical significance was set at P < 0.05. Of the 622 Mtb isolates, 536 (86.2%) were susceptible to RIF and INH. The rest, 86 (13.83%), were resistant to either drugs or both. A two-sample proportional equality test revealed that the MDR-TB prevalence in western Kenya (5%) did not vary significantly from the global MDR-TB estimate (3.9%) (P = 0.196). Men comprised the majority of susceptible and resistant TB (75.9% and 77.4%%, respectively). Also, compared with healthy individuals, the prevalence of HIV was significantly higher in MDR-TB patients (35.9% vs 5.6%). Finally, TB prevalence was highest in individuals aged 25–44 years, who accounted for 58.4% of the total TB cases. Evidently, the prevalence of MDRTB in western Kenya is high. Particular attention should be paid to men, young adults, and those with HIV, who bear the greatest burden of resistant TB. Overall, there is a need to refine TB control and treatment programs in the region to yield better outcomes.
Citation: George O Lugonzo, Ezekiel M. Njeru, William Songock, Albert A. Okumu, Eric M. Ndombi. Epidemiology of multi-drug resistant Tuberculosis in the western region of Kenya[J]. AIMS Microbiology, 2024, 10(2): 273-287. doi: 10.3934/microbiol.2024014
Multidrug-resistant tuberculosis (TB) (MDR-TB), or TB that is simultaneously resistant to both isoniazid (INH) and rifampicin (RIF), is a barrier to successful TB control and treatment. Stratified data on MDR-TB, particularly in the high-burden western Kenya region, remain unknown. This data is important to monitor the efficacy of TB control and treatment efforts. Herein, we determined the molecular epidemiology of drug-resistant TB and associated risk factors in western Kenya. This was a non-experimental, population-based, cross-sectional study conducted between January and August 2018. Morning sputum samples of individuals suspected of pulmonary TB were collected, processed, and screened for

| [1] | (2019) World Health OrganizationGlobal tuberculosis report 2019. Geneva, Swizerland: WHO press: 284. Available from: https://www.who.int/publications/i/item/9789241565714. |
| [2] | National AIDS and STI Control Programme (NASCOP)Kenya AIDS indicator survey 2012: final report (2014). |
| [3] | (2018) World Health OrganizationGlobal tuberculosis report 2018. Geneva, Swizerland: WHO press: 266. Available from: https://www.who.int/publications/i/item/9789241565646. |
| [4] | Kenya Ministry of HealthKenya tuberculosis prevalence survey 2016 (2016). |
| [5] |
Ding P, Li X, Jia Z, et al. (2017) Multidrug-resistant tuberculosis (MDR-TB) disease burden in China: A systematic review and spatio-temporal analysis. BMC Infect Dis 17: 1-29. https://doi.org/10.1186/s12879-016-2151-5 
|
| [6] | (2010) World Health OrganizationGlobal tuberculosis control 2010. Geneva, Swizerland: WHO press: 218. Available from: https://www.who.int/publications/i/item/9789241564069. |
| [7] |
Baffoe-Bonnie A, Houpt ER, Turner L, et al. (2019) Drug-susceptible and multidrug-resistant mycobacterium tuberculosis in a single patient. Emerg Infect Dis 25: 2120-2121. https://doi.org/10.3201/eid2511.180638
|
| [8] | Walley J (1997) DOTS for TB: It's not easy. Afr Health 20: 21-22. |
| [9] |
Zignol M, van Gemert W, Falzon D, et al. (2012) Surveillance of anti-tuberculosis drug resistance in the world: an updated analysis, 2007–2010. Bull World Health Organ 90: 111-119. https://doi.org/10.2471/BLT.11.092585
|
| [10] | (2017) World Health OrganisationGlobal tuberculosis report 2017. Geneva, Swizerland: WHO press: 251. Available from: https://www.who.int/publications/i/item/9789241565516. |
| [11] |
Lange C, Chesov D, Heyckendorf J, et al. (2018) Drug-resistant tuberculosis: an update on disease burden, diagnosis and treatment. Respirology 23: 656-673. https://doi.org/10.1111/resp.13304
|
| [12] | (2016) World Health OrganizationGlobal ruberculosis report 2016. Geneva, Swizerland: WHO press: 214. Available from: https://www.who.int/publications/i/item/9789241565394. |
| [13] | Ministry of Health KenyaNTLD-Program annual report 2008 (2008). |
| [14] |
Ombura IP, Onyango N, Odera S, et al. (2016) Prevalence of drug resistance Mycobacterium tuberculosis among patients seen in coast provincial general hospital, Mombasa, Kenya. PLoS ONE 11: e0163994. https://doi.org/10.1371/journal.pone.0163994
|
| [15] |
Ogari CO, Nyamache AK, Nonoh J, et al. (2019) Prevalence and detection of drug resistant mutations in Mycobacterium tuberculosis among drug naïve patients in Nairobi, Kenya. BMC Infect Dis 19. https://doi.org/10.1186/s12879-019-3911-9
|
| [16] |
Ogwang MO, Imbuga M, Ngugi C, et al. (2021) Distribution patterns of drug resistance Mycobacterium tuberculosis among HIV negative and positive tuberculosis patients in Western Kenya. BMC Infect Dis 21. https://doi.org/10.1186/s12879-021-06887-x
|
| [17] |
Nema V (2012) Tuberculosis diagnostics: challenges and opportunities. Lung India 29: 259-66. https://doi.org/10.4103/0970-2113.99112
|
| [18] | Pepper T, Joseph P, Mwenya C (2018) Normal chest radiography in pulmonary tuberculosis: implications for obtaining respiratory specimen cultures. Int J Tuberc Lung Dis 12: 397-403. |
| [19] | Naveen G, PeeraPur B (2012) Comparison of the lowenstein-jensen medium, the Middlebrook 7H10 medium and MB/BacT for the isolation of Mycobacterium tuberculosis (MTB) from clinical specimens. J Clin Diagn Res 6: 1704-1709. https://doi.org/10.7860/JCDR/2012/4603.2635 |
| [20] | Ministry of Health KenyaThe first Kenya tuberculosis patient cost survey 2017 (2017). |
| [21] | (2022) World Health OrganizationImplementing the end tb strategy: the essentials 2022. Geneva, Swizerland: WHO press: 62. Available from: https://www.who.int/publications/i/item/9789240065093. |
| [22] |
Sitienei J, Nyambati V (2013) The epidemiology of smear positive tuberculosis in three TB/HIV high burden provinces of Kenya (2003–2009). Epidemiol Res Int 2013: 1-7. https://doi.org/10.1155/2013/417038
|
| [23] |
Narasimhan P, Wood J, Macintyre CR, et al. (2013) Risk factors for tuberculosis. Pulm Med 2013. https://doi.org/10.1155/2013/828939
|
| [24] |
Chopra KK, Arora VK (2019) End TB–Strategy–A dream to achieve. Indian J Tuberc 66: 163-164. https://doi.org/10.1016/j.ijtb.2019.02.001
|
| [25] | National Bureau of StatisticsKenya population and housing census 2019 (2019). |
| [26] | Kubica GP, Dye WE, Cohn ML, et al. (1963) Sputum digestion and decontamination with N-acetyl-l-cysteine-sodium hydroxide for culture of mycobacteria. Am Rev Respir Dis 87: 775-779. |
| [27] |
Martin A, Bombeeck D, Fissette K, et al. (2011) Evaluation of the BD MGIT TBc identification test (TBc ID), a rapid chromatographic immunoassay for the detection of Mycobacterium tuberculosis complex from liquid culture. J Microbiol Methods 84: 255-257. https://doi.org/10.1016/j.mimet.2010.12.003
|
| [28] |
Ardito F, Posteraro B, Sanguinetti M, et al. (2001) Evaluation of BACTEC ycobacteria growth indicator tube (MGIT 960) automated system for drug susceptibility testing of Mycobacterium tuberculosis. J Clin Microbiol 39: 4440-4444. https://doi.org/10.1128/JCM.39.12.4440-4444.2001
|
| [29] |
Baliza M, Bach A, Queiroz G, et al. (2008) High frequency of resistance to the drugs isoniazid and rifampicin among tuberculosis cases in the city of Cabo de Santo Agostinho, an urban area in northeastern Brazil. Rev Soc Bras Med Trop 41: 11-16. https://doi.org/10.1590/S0037-86822008000100003
|
| [30] |
Kidenya B, Mshana S, Fitzgerald D (2018) Genotypic drug resistance using whole-genome sequencing of Mycobacterium tuberculosis clinical isolates from North-western Tanzania. Tuberculosis (Edinb) 109: 97-101. https://doi.org/10.1016/j.tube.2018.02.004
|
| [31] |
Balcells M, Thomas S (2006) Isoniazid preventive therapy and risk for resistant tuberculosis. Emerg Infect Dis 12: 7447-7451. https://doi.org/10.3201/eid1205.050681
|
| [32] | Snow K, Yadav R, Denholm J, et al. (2018) Tuberculosis among children, adolescents and young adults in the Philippines: a surveillance report. West Pac J 9: 16-20. https://doi.org/10.5365/wpsar.2017.8.4.011 |
| [33] |
Snow K, Hesseling A, Naidoo P (2017) Tuberculosis in adolescents and young adults: epidemiology and treatment outcomes in the Western Cape. Int J Tuberc Lung Dis 21: 651-657. https://doi.org/10.5588/ijtld.16.0866
|
| [34] |
Ojiezeh T, Ogundipe O, Adefosoyo V (2015) A retrospective study on incidence of pulmonary tuberculosis and human immunodeficiency virus co-infection among patients attending National Tuberculosis and Leprosy Control Programme, Owo centre. Pan Afr Med J 20: 345. https://doi.org/10.11604/pamj.2015.20.345.5643
|
| [35] |
Budgell E, Evans D, Leuner R, et al. (2018) The costs and outcomes of paediatric tuberculosis treatment at primary healthcare clinics in Johannesburg, South Africa. S Afr Med J 108: 423-431. https://doi.org/10.7196/SAMJ.2018.v108i5.12802
|
| [36] |
Coffman J, Chanda-Kapata P, Marais BJ, et al. (2017) Tuberculosis among older adults in Zambia: burden and characteristics among a neglected group. BMC Public Health 17: 1-6. https://doi.org/10.1186/s12889-017-4836-0
|
| [37] |
Ogwang MO, Imbuga M, Ngugi C, et al. (2021) Distribution patterns of drug resistance Mycobacterium tuberculosis among HIV negative and positive tuberculosis patients in Western Kenya. BMC Infect Dis 21. https://doi.org/10.1186/s12879-021-06887-x
|
| [38] | Borgdorff M, Nagelkerke N, Dye C, et al. (2000) Gender and tuberculosis: A comparison of prevalence surveys with notification data to explore sex differences in case detection. Int J Tuberc Lung Dis 4: 123-132. |
| [39] |
Gaude GS, Hattiholli J, Kumar P (2014) Risk factors and drug-resistance patterns among pulmonary tuberculosis patients in northern Karnataka region. Niger Med J J Niger Med Assoc 55: 327-332. https://doi.org/10.4103/0300-1652.137194
|
| [40] |
Adane K, Ameni G, Bekele S, et al. (2015) Prevalence and drug resistance profile of Mycobacterium tuberculosis isolated from pulmonary tuberculosis patients attending two public hospitals in East Gojjam zone, northwest Ethiopia. BMC Public Health 15: 1-8. https://doi.org/10.1186/s12889-015-1933-9
|
| [41] |
Lönnroth K, Jaramillo E, Williams BG, et al. (2009) Drivers of tuberculosis epidemics: the role of risk factors and social determinants. Soc Sci Med 68: 2240-2246. https://doi.org/10.1016/j.socscimed.2009.03.041
|
| [42] | Rajeswari R, Chandrasekaran V, Suhadev M, et al. (2002) Factors associated with patient and health system delays in the diagnosis of tuberculosis in South India. Int J Tuberc Lung Dis 6: 789-795. |
| [43] |
Baya B, Achenbach CJ, Kone B, et al. (2019) Clinical risk factors associated with multidrug-resistant tuberculosis (MDR-TB) in Mali. Int J Infect Dis 81: 149-155. https://doi.org/10.1016/j.ijid.2019.02.004
|
| [44] | National Aids Control CouncilKenya AIDS response progress report 2016 (2016). |
| [45] |
Ramaswamy S, Musser JM (1998) Molecular genetic basis of antimicrobial agent resistance in Mycobacterium tuberculosis: 1998 update. Tuber Lung Dis 79: 3-29. https://doi.org/10.1054/tuld.1998.0002
|
| [46] |
Van Halsema CL, Fielding KL, Chihota VN, et al. (2012) Trends in drug-resistant tuberculosis in a gold-mining workforce in South Africa, 2002–2008. Int J Tuberc Lung Dis 16: 967-973. https://doi.org/10.5588/ijtld.11.0122
|
| [47] | Affolabi D, Adjagba OABG, Tanimaomo-Kledjo B, et al. (2007) Anti-tuberculosis drug resistance among new and previously treated pulmonary tuberculosis patients in Cotonou, Benin. Int J Tuberc Lung Dis 11: 1221-1224. |
| [48] | Sangaré L, Diandé S, Badoum G, et al. (2010) Anti-Tuberculosis drug resistance in new and previously treated pulmonary tuberculosis cases in Burkina Faso. Int J Tuberc Lung Dis 14: 1424-429. |
| [49] |
Diarra B, Goita D, Tounkara S, et al. (2016) Tuberculosis drug resistance in Bamako, Mali, from 2006 to 2014. BMC Infect Dis 16: 1-8. https://doi.org/10.1186/s12879-016-2060-7
|
| [50] | (2023) World Helath OrganizationGlobal tuberculosis report 2023. Geneva, Swizerland: WHO press. Available from: https://www.who.int/publications/i/item/9789240083851. |
| [51] |
Kwan CK, Ernst JD (2011) HIV and tuberculosis: a deadly human syndemic. Clin Microbiol Rev 24: 351-376. https://doi.org/10.1128/CMR.00042-10
|
| [52] |
Moir S, Chun TW, Fauci AS (2011) Pathogenic mechanisms of HIV disease. Annu Rev Pathol Mech Dis 6: 223-248. https://doi.org/10.1146/annurev-pathol-011110-130254
|
| [53] |
Sonnenberg P, Glynn J, Katherine F, et al. (2005) How soon after infection with HIV does the risk of tuberculosis start to increase? a retrospective cohort study in South African gold miners. J Infect Dis 191: 150-158. https://doi.org/10.1086/426827
|
| [54] |
Mesfin YM, Hailemariam D, Biadglign S, et al. (2014) Association between HIV/AIDS and multi-drug resistance tuberculosis: A systematic review and meta-analysis. PLoS ONE 9: e82235. https://doi.org/10.1371/journal.pone.0082235
|
| [55] |
Sultana ZZ, Hoque FU, Beyene J, et al. (2021) HIV infection and multidrug resistant tuberculosis: a systematic review and meta-analysis. BMC Infect Dis 21: 1-13. https://doi.org/10.1186/s12879-020-05749-2
|
| [56] | Ogunleye O, Owolabi O, Mubarak, M (2018) Population growth and economic growth in Nigeria: An Appraisal. Int j manag account econ 5: 282-299. https://doi.org/10.33987/vsed.2(73).2020.27-45 |
| [57] |
Duan Q, Chen Z, Chen C, et al. (2016) The Prevalence of drug resistant tuberculosis in mainland China:an updated systematic review and meta-analysis. PLoS ONE 11: e0148041. https://doi.org/10.1371/journal.pone.0148041
|
| [58] | Marais B, Gie R, Schaaf H (2004) The clinical epidemiology of childhood pulmonary tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis 8: 278-285. |
| [59] | Daniel O, Osman E, Oladimeji O (2013) Pre-extensive drug resistant tuberculosis (Pre-XDR-TB) among MDR-TB patents in Nigeria. Glob Adv Res J Microbiol 2: 22-25. https://doi.org/10.4236/jtr.2018.63018 |
| [60] |
Utpat KV, Rajpurohit R, Desai U (2023) Prevalence of pre-extensively drug-resistant tuberculosis (Pre XDR-TB) and extensively drug-resistant tuberculosis (XDR-TB) among extra pulmonary (EP) multidrug resistant tuberculosis (MDR-TB) at a tertiary care center in Mumbai in pre Bedaquiline (BDQ) era. Lung India 40: 19-23. https://doi.org/10.4103/lungindia.lungindia_182_22
|
| [61] |
Shibabaw A, Gelaw B, Gebreyes W, et al. (2020) The burden of pre-extensively and extensively drug-resistant tuberculosis among MDR-TB patients in the Amhara region, Ethiopia. PLoS ONE 15: e0229040. https://doi.org/10.1371/journal.pone.0229040
|
Figures(2) / Tables(3)

George O Lugonzo, Ezekiel M. Njeru, William Songock, Albert A. Okumu, Eric M. Ndombi. Epidemiology of multi-drug resistant Tuberculosis in the western region of Kenya[J]. AIMS Microbiology, 2024, 10(2): 273-287. doi: 10.3934/microbiol.2024014







 DownLoad:
DownLoad: