
JOURNAL OF ANESTHESIA AND SURGICAL RESEARCH
The Normal Tendon and Ligament Anatomy of the Lateral Elbow: Implications for Tennis Elbow Syndrome
Stuart G Kirkham1* and Michael J Millar1
1Department of Orthopaedic Surgery, The SAN Hospital, Sydney NSW, Australia.
*Corresponding Author: Stuart G Kirkham, The SAN Hospital, Suite 508, 185 Fox Valley Road, Wahroonga, Sydney, NSW 2076, Australia.
| ReceivedJun 5, 2023 | RevisedJun 15, 2023 | AcceptedJun 20, 2023 | PublishedJul 5, 2023 |
Abstract
Introduction: Numerous authors have studied the role that ligaments play in various elbow instability syndromes. There is no published article that has studied the role of ligaments in tennis elbow pathology. Tennis elbow patients exhibit increased pain during elbow extension. Lateral ligaments become taut in extension. Therefore, researchers decided to investigate the possibility of an anatomical link between the tendon and ligament anatomy, and how this might help to understand tennis elbow.
Methods: Four fresh cadaveric elbows were dissected. Researchers examined the four tendons which comprise the common extensor origin (CEO). Researchers documented the exact footprint created by each tendon origin creates on the Humerus. Researchers also studied the exact attachments of the various named lateral ligaments both macroscopically and histologically using H and E staining.
Results: Four tendons contribute to the CEO: Extensor Carpi Radialis Brevis (ECRB), Extensor Digitorum Communis (EDC), Supinator and Anconeus. All four tendons are inseparably blended together, when viewed under 2.5 x power loupe magnification. The deep fibers of the CEO are inseparably blended with the lateral collateral ligament (LCL). This was confirmed with macroscopic inspection, under 2.5 x loupe magnification, and at histological assessment.
Discussion/conclusion-clinical relevance: Researchers already know that the LCL becomes taught in extension, and that the ECRB tendon becomes taut in forearm pronation. These two actions produce two shear forces at the CEO which pull in opposite directions. Researchers have found that these tendons and ligaments are inseparably blended together over a distance of 10 mm-between the lateral epicondyle and the radio capitellar joint line-researchers propose that this unique anatomy creates a specific vulnerable location whereby there exists shear forces between those two layers of collagenous tissue. Researchers propose that this explains the initiation and the perpetuation of tennis elbow lesions. It also explains the clinically observed pain during elbow extension in tennis elbow.
Keywords
Tennis elbow; Ligaments; Common extensor origin; Lateral epicondylitis; Tendinosis; Tendinitis
Introduction
Tennis elbow is a very common clinical condition seen by surgeons, family doctors, and allied health practitioners, estimating to affect 1-3% of the general population [1], and 4-30% of manual laborers per annum [2]. The pain and disability caused by tennis elbow is a common reason for decreased productivity in the workforce today, with an average of 9.3 weeks-time off work per year [3] and medical expenses and lost work time associated to cost more than $22 billion per year in the US alone [2].
Tennis elbow has been described as a tendinosis [4] resulting from overuse of the extensor radialis brevis (ECRB) muscle by repetitive micro trauma [4]. The ECRB tendon inserts into the base of the 3rd metacarpal, becoming more taught when the forearm is in pronation. Therefore, forearm pronation places the ECRB tendon under relatively greater tension and load and forearm pronation is thought to be one factor which contributes in the initiation of tears of the common extensor origin CEO (tennis elbow tears) [5,6]. While there is common agreement that tennis elbow results from a lesion of the deep fibers of the (CEO) [4], there is still a relatively large gap in the understanding of this common disease. It is not clear from the anatomical literature exactly where the CEO tendon footprint blends into which part of the bone of the lateral epicondyle and if there is blending of the tendon footprint into the lateral collateral ligament [7,8].
If the CEO tendon and ligament do in fact blend together then it follows that the lateral collateral ligament is capable of producing a force that acts upon the CEO tendon, contributing to the initiation and perpetuation of a tear. Such patho-anatomy would explain why sufferers of tennis elbow commonly have both pain and or difficulty performing elbow extension, irrespective of the degree of forearm rotation; the lateral ligament tightens in extension, playing a role in symptomatology rather than only the torn fibers of the CEO tendon.
The purpose of this study was to define the normal anatomy at the lateral side of the elbow. Specifically, researchers aimed to analyze (a) the macroscopic and histological bony footprints of ligaments and tendons and (b) whether or not any of these tendon fibers actually blend into the ligament fibers. Most previous authors who have studied the ligamentous anatomy of the lateral elbow have been primarily concerned with elbow instability, including the posterolateral rotatory instability (PLRI) syndrome [9]. Researchers aim to investigate the anatomical relationship of the CEO and lateral collateral ligament in context of the relevance to tennis elbow, not instability.
Methods
Researchers studied four [1] fresh frozen cadaveric elbows. Dissection was carried out by an experienced upper limb consultant specialist orthopaedic surgeon, using 2.5 x loupe magnification. Researchers identified the following tendons (EDC, ECRB, Supinator, and Anconeus) and dissected them back to the place of origin at the lateral aspect of the elbow. Researchers also identified and followed the lateral ligament complex (lateral collateral ligament and LUCL) to its points of bony origin on the Humerus. The ligament and tendon footprints were pinned, and then photographed as macroscopic specimens. Specimens were sectioned so as to maintain the soft tissue attachments to the lateral epicondyle and Capitellum regions of the distal Humerus. Macroscopic specimens were placed into containers of 70% ethanol, awaiting histological preparation. Specimens were then decalcified where necessary before being set in paraffin. Sections were made at 2mm in both the coronal and sagittal planes. Specimens were then stained with Hematoxylin and Eosin. Researchers then hired a medical illustrator to recreate and clarify the findings.
Results
1. In all four elbows researchers found the following:
a. Four tendons contribute to the common extensor origin (CEO)-namely extensor Carpi Radials Bevis (ECRB), Extensor Digitorum Communis (EDC), Supinator and Anconeus.
b. All 4 tendons are inseparably blended together at the most proximal 10 mm before they blend into the periosteum of the lateral epicondyle. Effectively these 4 tendons behave and perform as one combined tendon unit- commonly known as the Common Extensor Origin (CEO).
c. The 4 tendons cannot be individually identified in their most proximal 10 mm. After 10mm researchers reach the radio capitellar joint line. Distal to this point they start to be discernible as 4 separate tendons.
d. ECRB and supinator attach more anteriorly on the LE.
e. EDC and anconeus attach more posteriorly on the LE.
f. The ECRB portion of the CEO appears to be the tendon most in contact with the capsular ligaments in between the RCJL and the LE.
g. The 4 tendons attach to and cover the entire bony projection known as the lateral epicondyle. (The lateral epicondyle derives its shape from the load and function afforded to it by these Musculo-tendinous attachments. It is significantly smaller than the Medial epicondyle which provides attachment to the more powerful flexor forearm muscles).
h. The deep fibers of the CEO tendon blend inseparably with the superficial fibers of the lateral collateral ligament.
i. The blending of tendon and ligament is inseparable over 10 mm which starts at the lateral epicondyle and extends distally to reach the radio-capitellar joint line.
j. The lateral ligament attaches to the inferior cortex (not the lateral cortex) of the lateral epicondyle.
k. There is a continuous sheet of capsular ligaments that start at the posterior edge of the inferior cortex of the LE and continues anteriorly as far as the anterior edge of the LE.
l. Within this continuous sheet of capsular ligaments there are discernible thickenings which are already named and known as the Lateral collateral ligament LCL and the lateral ulnar collateral ligament LUCL.
m. The superficial forearm fascia is a strong investing layer that encompasses not only the CEO but also the muscles of ECU and Brachioradialis. It appears to be capable of playing a role in transmitting loads across these structures. It is analogous to the fascia lata of the thigh which is also believed to play a role in force transmission.
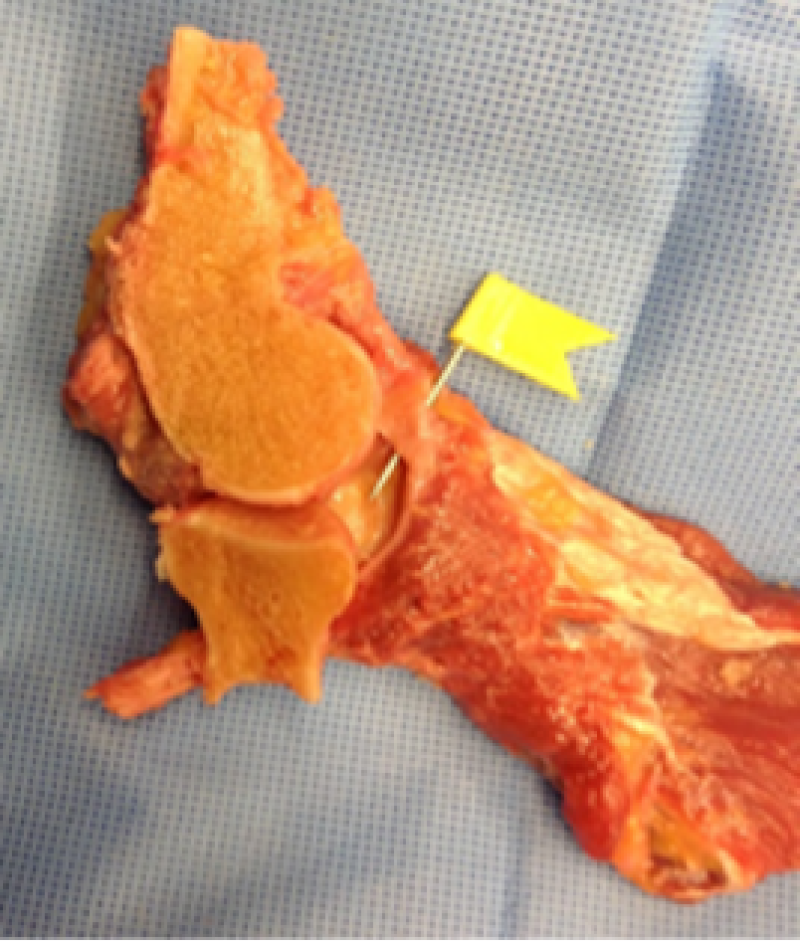
Figure 1: This macroscopic dissection of the lateral elbow structures demonstrates that the joint capsule is inseparably blended with CEO tendon.

Figure 2: The 4 tendons of the CEO are inseparably blended as they all contribute to the footprint of the CEO at the Lateral epicondyle.

Figure 3: The histology whereby tendon and ligament are inseparably blended over the terminal 10 mm before both insert into the periosteum of the lateral epicondylar bone.
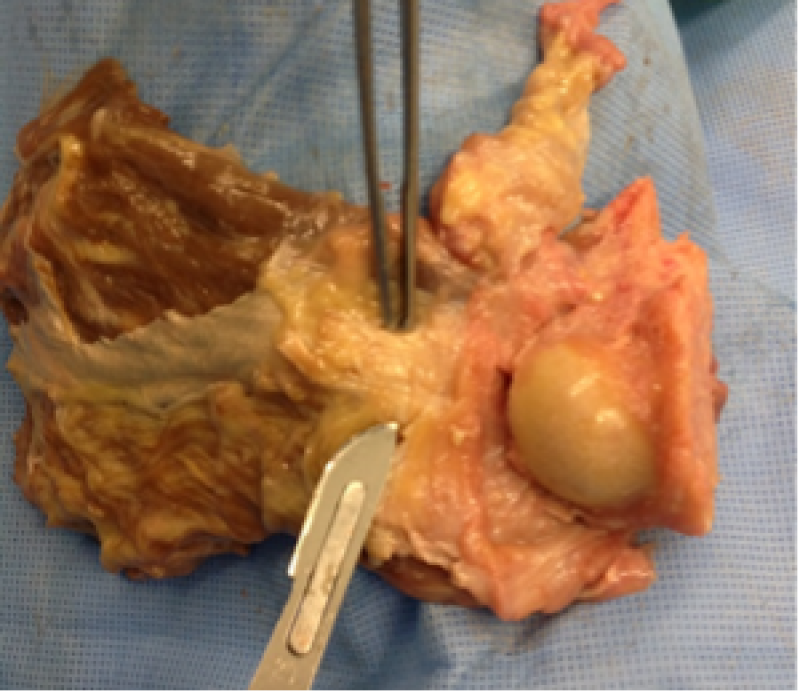
Figure 4: The CEO tendon between the 2 surgical instruments. Again, it is inseparable from the ligamentous joint capsule.

Figure 5: The sectioned capitellum together with adjacent lateral soft tissues. Importantly, the tendon and ligament tissues are inseparably blended as they take origin from the lateral epicondyle (covered by tissue in this photograph).
Discussion
The human elbow anatomy is unique. Only the forearm is capable of pronating and supinating through a range of almost 180 degrees; whereas in the only other two bone system (tibia and fibula) this range of rotation is not afforded by the vastly different ligament and joint anatomies. The need for human forearm rotation and hand positioning has in the opinion made it essential that human elbow ligaments have evolved in this unique way.
Only at the lateral elbow do researchers observe a system of ligaments whereby none of these ligaments attach to the radius. Uniquely, the radius pivots within the annular ligament, which attaches only to the ulna. The other ligaments-LCL and LUCL-blend into the annular ligament and the ulna, but none attach to the radius. This is why researchers have illustrated the radius as invisible-the soft tissues are uniquely suspended around it; but are not attached.
The human elbow lateral ligaments are made even more extraordinary by also giving attachment to the CEO tendons which are already known to be implicated in tennis elbow syndrome.
When the elbow is extended (actively or passively) the lateral ligament tightens. Researchers have frequently observed that patients with tennis elbow syndrome often exhibit marked and reproducible pain when attempting maximal elbow extension, irrespective of the position of the forearm and/or wrist. This led to the hypothesis that it was not only the well-known CEO tendon lesion but also very likely that the lateral ligament complex was contributing to the above observed symptoms.
In most anatomical texts, the ligaments are described as being separate to the tendons 10. Most previous authors who have studied the lateral ligaments have concentrated primarily on its relevance to elbow instability [10], including posterolateral rotatory instability (PLRI) [6,7]. There are however a few authors, as in the study, who have already commented that the ligaments and tendons appear to be blended. [11-13]. Researchers find this highly interesting as it might explain the very commonly observed pain during elbow extension, which is seen in the majority of tennis elbow patients.
In this cadaveric study, researchers have found that the ligament and tendon fibers are definitely blended together. Researchers would like to highlight the relevance of these findings with respect to tennis elbow syndrome, rather than to re-visit the relevance to elbow instability.
Researchers note that several authors have advocated an arthroscopic type of treatment for tennis elbow [11,12]. Those authors claimed that authors could identify and locate the tendon lesion using an intra-articular view and then also advocate debriding the tendon lesion from inside the joint. This must involve excising some of the normal, uninjured joint capsule (or ligamentous fibers) before reaching tendon. So called “safe zones” have been described for this arthroscopic procedure, to minimize the risks of iatrogenic damage to the important lateral ulnar collateral ligament (LUCL) which can result in posterolateral rotatory instability (PLRI) [14]. Whilst researchers agree that the lesion can be reached and even debrided arthroscopically, do not advocate violating the normal uninjured capsule if it can be avoided.
Nirschl [4] described that the lesion is extra-articular and is most often located in the deep fibers of the CEO tendon. On that basis, researchers believe it is logical to approach this extra articular lesion without a more elaborate, expensive and potentially time consuming intra articular arthroscopic procedure and deliberately violating the intact joint capsule. Researchers advocate open surgery, not arthroscopic, as the preferred method when surgery is indicated. Previous authors have admitted that during open extra articular surgical procedure that an inadvertent arthrotomy sometimes can occur and that furthermore this usually did not lead to any appreciable complications. This is in keeping with the findings that the typical location of the lesion is in the deep fibers of the CEO immediately adjacent to the LCL which is typically the only tissue intact between the lesion and the joint cavity at the time of surgery.
Wang et al [15] have published on both the tension found in various parts of the CEO and the detention that can be achieved by sectioning the superficial fascia-a procedure called fractional lengthening. the study supports the concept of fractional lengthening. Researchers believe that division of the superficial fascia (being a robust sheet and similar to fascia lata of the lower limb) could conceivably detention of CEO. Given the visible and palpable strength of the superficial forearm fascia researchers assume that the superficial fascia contributes to distribution of loads both in normal forearms and in tennis-elbow-forearms.
Researchers know from previous authors and from MRI observations that the true “tennis elbow lesion” lies within the CEO tendon tissue [16]. However, researchers now contend from the findings that it is reasonable to believe that the ligament plays a role by at least exerting traction (tension) upon the lesion which is in deep fibers of the CEO tendon. The wrist extensors and finger extensors are relatively weak when compared to the wrist flexors and the finger flexors. Anatomists often recite that “form follows function and function follows form”. The medial epicondyle is very much larger than the lateral epicondyle reflecting the huge difference in power of these opposing two muscle groups. The human grip is a flexor function; and extension is used mainly for the release and not the retention of objects. Accordingly, these relatively weak extensor tendons on the lateral side are probably subject to injury at lower load levels than the more powerful flexor group. Finger extensor are used in typing and computer keyboard work. Supinator is used for opening jars and using screwdrivers. Human life expectancy has increased in the last 50-100 years. The lateral elbow has probably not evolved fast enough to allow for modern human endeavors that place it at loads which exceed its strength. Tendons are composed of collagen which is largely extracellular. Tendons transmit load and have a finite capacity for withstanding forces. Tendons will tear once their load threshold of load is reached. Researchers propose that in tennis elbow that the tendon is at maximal vulnerability or risk for exceeding its unique load threshold when the elbow is in extension and the forearm is in pronation.
Figures 6 and 7 illustrate the concepts that:
1. 4 tendons contribute to the CEO. These 4 tendons entirely cover the lateral epicondyle, leaving nil bare areas of bone on the lateral cortex.
2. Those 4 tendons are inseparably blended; there is a cuff-like blending of 4 muscular units into a common tendon.
3. The deep fibers of the CEO tendon and the superficial fibers of the lateral collateral ligament are also blended over 10 mm in between the LE and the RCJL.
4. Uniquely, the radius does not attach to any of these soft tissues. There is a unique suspensory arrangement whereby all soft tissues are indirectly attached to the ulna via the annular ligament. This creates a unique set of forces which researchers believe is the cause of tennis elbow.
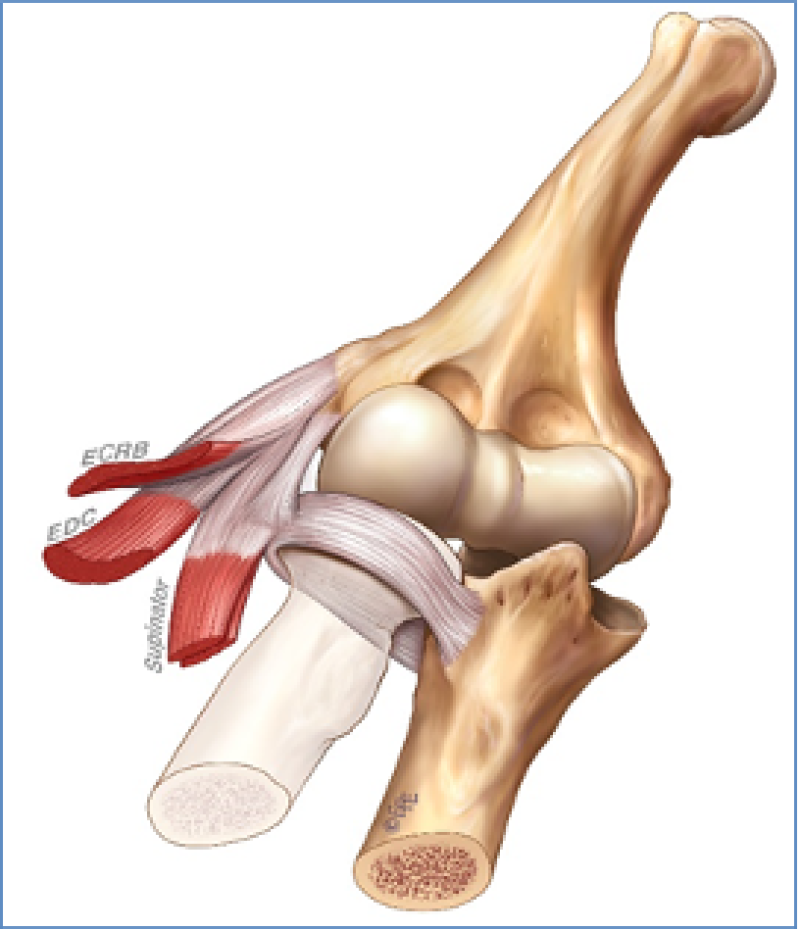
Figure 6: Lateral sided tendons and ligaments, anterior view (note the radius is rendered invisible as it has nil ligamentous or tendons attachments).
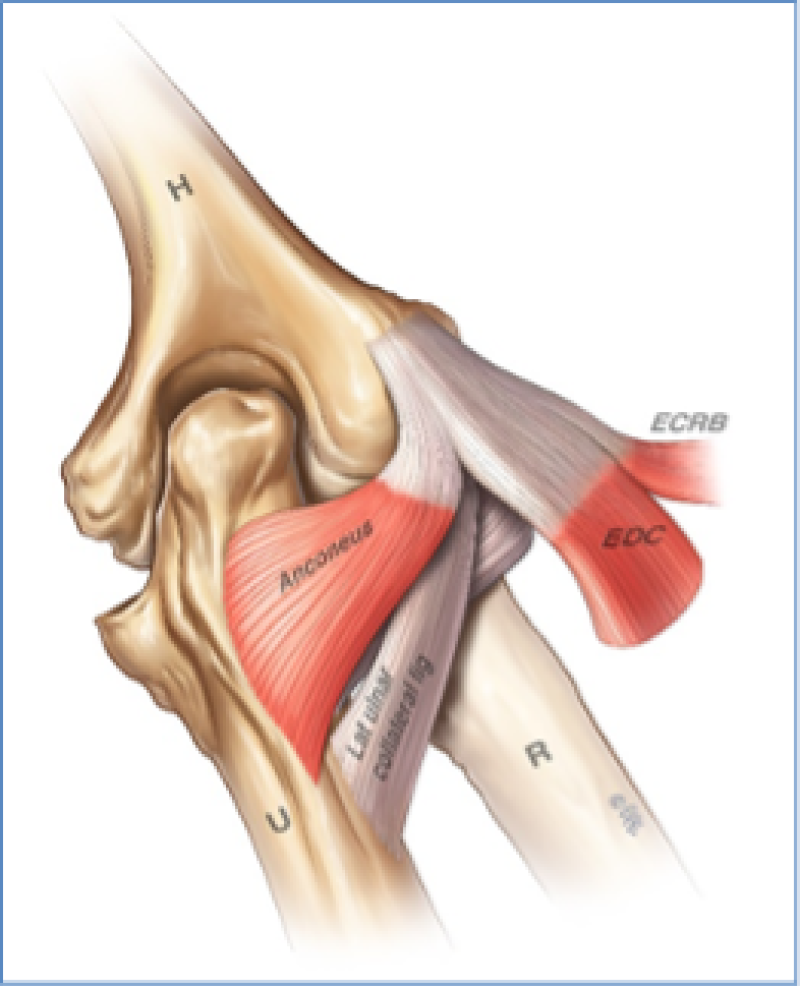
Figure 7: Lateral sided tendons and ligaments, posterior view (note that the radius is rendered invisible here because it has nil direct ligamentous or tendons attachments).
Researchers also note the unique soft tissue arrangement at the lateral elbow, whereby none of the lateral ligaments or tendons attach to the Radius bone. The ligaments and tendons (which researchers now know are blended) are in fact indirectly attached to the Ulna bone, via the annular ligament-as shown in Figure6. This illustration shows the radius as invisible to highlight the concept that the radius actually plays no role in bony attachment of soft tissue at the lateral elbow–a truly unique anatomical relationship that is not seen in the lower limb.
Researchers believe that Anconeus and supinator are only weak contributors to forces at the CEO. One weakness of this study is that researchers only studied four elbows. It would have been preferable to study more elbows but without sponsorship the cost was prohibitive. Researchers are grateful to Exactech Pty Ltd and to Global Pty Ltd to have sponsor some of the costs of these 4 cadavers.
Conclusions and Clinical Relevance
In this study researchers have found:
1. The 4 tendons of the CEO (ECRB, EDC, Supinator and Anconeus) are inseparably blended to each other over their most proximal 10mm-in between the lateral epicondyle and the radio capitellar joint line. Through a limited skin incision at the elbow, it is not possible to distinguish the fibers of any individual tendon. It is a cuff-like arrangement, whereby the tendons are blended at their origins.
2. Using scalpel dissections and histology researchers found that the deep fibers of the CEO tendon are inseparably blended with and are attached to the superficial fibers of the lateral collateral ligament.
3. The deep forearm fascia is a significantly strong structure capable of taking some load.
From these anatomical findings, researchers believe that the relevance to clinical practice is as follows:
1. Researchers believe that the unique suspensory style of indirect ligament attachments of the lateral human elbow (see figures 6 and 7) combined with the inseparable blending of tendons and ligaments creates a uniquely vulnerable specific location at which there is a unique risk for tears occurring in what is a structurally relatively weak tendon tissue. This tendon is expected to withstand the forces of pronation and supination, whilst also withstanding the forces of elbow extension. The shear forces between these layers explains why the tears are observed in the same location.
2. This understanding of anatomy and associated forces explains.
a. The initiation of tears (most vulnerable when extension is combined with forearm pronation)
b. The perpetuation of tears after it is initiated or torn. This helps explain chronic lesions.
c. The symptom of pain during elbow extension.
3. The lesion typically seen on MRI is a complete tear of the CEO deep tendon fibers. The underlying ligament tissue does not tear as part of the tennis elbow lesion. The remaining intact tissue commonly seen on MRI is the lateral collateral ligament. The tears often extend only as far as the RC joint line.
As researchers improve the understanding of the normal anatomy and the patho-anatomy including the tear mechanism researchers are better able to come up with improved treatment options that will address the true problem. Anatomy is the foundation of the understanding. This more detailed knowledge will hopefully help us to find better treatment options for the patients.
References
1. De Smedt T, De Jong A, Van Leemput W, Lieven D, Van Glabbeek F. Lateral Epicondylitis in Tennis: Update on Aetiology, Biomechanics and Treatment. Br J Sports Med. 2007;41(11):816-9. PubMed | CrossRef
2. Werner RA, Franzblau A, Gell N, Hartigan A, Ebersole M, Armstrong TJ. Predictors of Persistent Elbow Tendonitis Among Auto Assembly Workers. J Occup Rehabil. 2005:393-400. PubMed | CrossRef
3. Struijs PA, Korthals-de Bos IB, van Tulder MW, Van Dijk CN, Bouter LM, Assendelft WJ. Cost effectiveness of Brace, Physiotherapy, or Both for Treatment of Tennis Elbow. Br J Sports Med. 2006;40(7):637-43. PubMed | CrossRef
4. Kraushaar BS, Nirschl RP. Tendinosis of the Elbow (tennis elbow): Clinical Features and Findings of Histological, Immunohistochemical, and Electron Microscopy Studies. J Bone Joint Surg Am. 1999;81(2):259. PubMed
5. Briggs CA, Elliott BG. Epicondylitis: Relationship Between Anatomical Structures and Tennis Elbow: A Review of Structures Associated with Tennis Elbow. Anatomia Clinica. 1985;7(3):149-53. PubMed | CrossRef
6. Cohen MS, Hill Hastings II. Rotatory Instability of the Elbow. The Anatomy and Role of the Lateral Stabilizers. JBJS. 1997;79(2):225-33. PubMed
7. Reichel LM, Morales OA. Gross Anatomy of the Elbow Capsule: A Cadaveric Study. J Hand Surg Am. 2013;38(1):110-6. PubMed | CrossRef
8. Sinnatamby CS, Last RJ. Last's Anatomy: Regional and Applied. 11th ed. Edinburgh; New York: Elsevier/Churchill Livingstone. 2006:65-6, 77-8.
9. Molinier F, Laffosse JM, Bouali O, Tricoire JL, Moscovici J. The anconeus, an Active Lateral Ligament of the Elbow: New Anatomical Arguments. Surg Radiol Anat. 2011:617-21. PubMed | CrossRef
10. Reichel LM, Milam GS, Sitton SE, Curry MC, Mehlhoff TL. Elbow Lateral Collateral Ligament Injuries. J Hand Surg Am. 2013;38(1):184-201. PubMed | CrossRef
11. Ando R, Arai T, Beppu M, Hirata K, Takagi M. Anatomical Study of Arthroscopic Surgery for Lateral Epicondylitis. Hand Surg. 2008;13(02):85-91. PubMed | CrossRef
12. Tsuji H, Wada T, Oda T, Iba K, Aoki M, Murakami G, Yamashita T. Arthroscopic, Macroscopic, and Microscopic Anatomy of the Synovial Fold of the Elbow Joint in Correlation with the Common Extensor Origin. Arthroscopy. J Arthrosc Relat. 2008;24(1):34-8. PubMed | CrossRef
13. Zoner CS, Buck FM, Cardoso FN, Gheno R, Trudell DJ, Randall TD, et al. Detailed MRI-Anatomic Study of the Lateral Epicondyle of the Elbow and its Tendinous and Ligamentous Attachments in Cadavers. AJR Am J Roentgenol. 2010;195(3):629-36. PubMed | CrossRef
14. Smith AM, Castle JA, Ruch DS. Arthroscopic Resection of the Common Extensor Origin: Anatomic Considerations. J Shoulder Elbow Surg. 2003;12(4):375-9. PubMed | CrossRef
15. Wang AW, Erak S. Fractional Lengthening of Forearm Extensors for Resistant Lateral Epicondylitis. ANZ J Surg. 2007;77(11):981-4. PubMed | CrossRef
16. Mackay D, Rangan A, Hide G, Hughes T, Latimer J. The objective Diagnosis of Early Tennis Elbow by Magnetic Resonance Imaging. Occup Med (Lond).2003;53(5):309-12. PubMed
Stuart G Kirkham1* and Michael J Millar1
1Department of Orthopaedic Surgery, The SAN Hospital, Sydney NSW, Australia.
*Corresponding Author: Stuart G Kirkham, The SAN Hospital, Suite 508, 185 Fox Valley Road, Wahroonga, Sydney, NSW 2076, Australia.
Copyright© 2023 by Kirkham SG, et al. All rights reserved. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Kirkham SG, Millar MJ. The Normal Tendon and Ligament Anatomy of the Lateral Elbow: Implications for Tennis Elbow Syndrome-Conceptual Review. J Anaesth Surg Res. 2023;3(2):160-70. DOI: https://doi.org/10.37191/Mapsci-JASR-3(2)-027