
JOURNAL OF DENTISTRY AND ORAL SCIENCES
Microtomography Evaluation of the Efficacy of Reciprocating and Rotary Instruments Followed by Different Complementary Steps in the Retreatment of Curved Root Canals
| ReceivedMar 19, 2021 | RevisedMar 31, 2021 | AcceptedApr 19, 2021 | PublishedMay 17, 2021 |
Lincoln de Campos Fruchi*, Murilo Priori Alcalde, Pablo Andres Amoroso-Silva, Rodrigo Ricci Vivan, Clovis Monteiro Bramante and Marco Antonio Hungaro Duarte
Department of Dentistry, Endodontics and Dental Materials, Bauru School of Dentistry, University of São Paulo, Brazil
*Corresponding Author: Lincoln de Campos Fruchi, Department of Dentistry, Endodontics and Dental Materials, Bauru School of Dentistry, University of São Paulo, Brazil
Accepted Date: 04-19-2021; Published Date: 05-17-2021
Copyright© 2021 by de Campos Fruchi L, et al. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Objectives: The purpose of this study was to evaluate the efficacy of steps, isolated or in cumulative means, in the endodontic retreatment of curved canals.
Methodology: Forty mesial roots of mandibular molars were divided into two groups. In the group 1 the filling removal was done with NiTi reciprocating M-wire and NiTi control memory wire rotary instruments followed by a passive ultrasonic irrigation solution agitation. In the group 2, the initial filling removal was done with NiTi reciprocating M-wire and conventional NiTi wire rotary instruments followed by a rotary plastic instrument for irrigation solution agitation. The results were analyzed through micro-computed tomography.
Results: The filling material was not completely removed for both groups. All steps did not statically differ between groups regarding to the filling removal. In the intragroup analyses, the results differed in some levels, mainly in the apical level, but did not statistically differ in all the different levels after each step. A statistical significant increase (P<.05), for both groups, in the volume of filling material in the isthmus was observed.
Conclusions: None of the protocols completely removed the filling material. The better results were found for the apical level and after passive ultrasonic irrigation. Vertical warm condensation filling technique enhanced the volume of filling material in the root canal system including the isthmus.
Clinical relevance: the control memory NiTi instruments could be considered a good choice for use as an additional step in the procedure of filling removal from curved mesial root canals.
Keywords
Micro-computed Tomography; Reciprocating Motion; Root Canal Retreatment; Rotary Systems; Curved Root Canals; Solvent
Introduction
The persistence of the apical periodontitis after primary endodontic treatment is mostly caused by bacteria that remained unaffected by endodontic antimicrobial procedures [1]. In the persistence of apical periodontitis nonsurgical treatment should be considered as the primary treatment approach. Endodontic surgery has a less success rate in long term outcomes [2,3].
Nickel-titanium (NiTi) rotary and reciprocating systems have shown to be safer and more efficient in endodontic retreatments than hand files [4-7]. NiTi alloys have been made with different thermal treatments to increase flexibility [8]. Thermomechanical treatment of NiTi files provides significant benefits with regard to the efficacy and safety of endodontic instruments [8]. M-wire and CM-wire instruments are mainly in the R-phase for the first and in the martensite phase for the former. The phases are modified by heating or cooling. The CM-wire has properties that allows a great memory of the material increasing the flexibility and resistance to fatigue avoiding procedural errors during instrumentation [9]. However, the efficiency of the Hyflex CM as complementary instrument to removal of root filling material in curved canals was not investigated.
The complete or the more efficient removal of the root canal filling during retreatment should be achieved to promote the best possible disinfection [10] to achieve a successful endodontic retreatment or even for the recent use of regenerative endodontic therapy for endodontic treatments [11]. Several techniques have been used for removing root-filling materials, including hand files, burs, and rotary instruments [4-12]. The mechanical removal of material filling can be completed with additional steps like passive ultrasonic irrigation (PUI) or the activation of the irrigation solutions through mechanical rotary devices [12]. The Easy Clean is a plastic instrument to be used in reciprocal motion and in curved canals. This instrument presented better capacity to remove the smear layer in mesial curved canals in relation to the PUI [12,13]. However, its efficiency in retreatment has not been evaluated.
Although, there is no consensus about a protocol for root canal retreatments. The purpose of this study was to evaluate the filling material removal after two different retreatment protocols and after each step of them. Some studies have been shown that the hybridization of instruments is more effective in the filling removal [14,15]. Rotary and reciprocating NiTI instruments are shown to be safe and efficient in root canals retreatments [6,7,14,16,17].
The effective filling removal is necessary to allow a direct and better action of irrigant solutions and chemical substances used as dressing to reduce the bacteria and to promote the biofilm dissolution inside the canals, dentinal tubules and anatomic areas with difficult access such as the isthmus.
The aim of the present study was to evaluate two different protocols, with hybrid techniques of instrumentation in different motions and alloys with different heat treatments followed by different irrigant agitation techniques. The null hypotheses were that there were no differences between the methods in relation to the efficacy of the root canal filling removal in endodontic retreatments.
Materials and Methods
The present study was conducted under the approval of the Ethics Committee of the Bauru School of Dentistry, University of São Paulo (CAAE: 44736215.9.0000.5417). From an initial sample of 40 teeth, it was possible to select 36 teeth and shared into ttwo groups (n=18). The sample calculation was made by using the G*Power v3.1 for Mac (Heinrich Heine, Universität Düsseldorf) and selecting the Wilcoxon–Mann-Whitney test of the t-test family. The alpha-type error of 0.05, a beta power of 0.95, and a ratio N2/N1 of 1 were also stipulated. A total of 8 samples per group were indicated as the minimum size need required for noting significant differences. The teeth were digitally radiographed in the bucco-lingual and mesial-distal directions with an exposure time of 0.16 s using the Schick CDR X-ray digital system (Schick Technologies, Long Island, NY). The crowns of the teeth were flattened to a length of 16 mm with the aid of a diamond disc (FKG, Dentaire, Switzerland). The working lengths of the root canals were established by inserting the tip of a #10 K file until the apex and observing them with an operatory microscope with 8X magnification (Alliance, São Paulo, Brazil). The patency of the canals was confirmed using a #10 K-file (Dentsply Maillefer, Ballaigues, Switzerland). In Group 1, initial filling removal was performed with a Reciproc R25 instrument, followed by a #40 HyFlex instrument and passive ultrasonic irrigation (PUI). In Group RMEasy, initial filling removal was performed as in Group 2, followed by a #40 MTwo instrument and irrigant agitation with a plastic reciprocating instrument (EasyClean).
Endodontic Treatment
PathFiles #13, 16, and 19 were used to make the glide paths. The PathFiles were used with VDW electric motors (VDW, Munich, Germany), at a speed of 300 rpm and torque of 60 g•cm. Subsequently, the teeth were instrumented with R25 Reciproc files (VDW) until the working length, established at 1 mm shorter of the full canal length. The Reciproc instrument was used with the corresponding VDW electric motor as per the Reciproc program, with three in and out pecking motions using light apical pressure. During glide path formation and root canal instrumentation, 2.5% sodium hypochlorite was used as an irrigant. Final irrigation was done with 1 ml of 17% EDTA for 1 minute followed by a final rinse with 2 ml of 2.5% sodium hypochlorite with a Navitips (Ultradent) 30-gauge needle. The canals were then dried with R25 paper points and obturated with R25 single cones (VDW) and AH Plus sealer (Dentsply) using a single cone. The teeth were digitally radiographed in the bucco-lingual and mesio-distal directions with an exposure time of 0.16 s using the Schick CDR X-ray digital system (Schick Technologies, Long Island, NY) in order to evaluate the quality of canal filling. The crowns were temporarily sealed with Citodur (Dorident, Wien, Austria) and stored at 37°C and 100% humidity for 3 months.
Endodontic Retreatment
The R25 Reciproc instruments were used for an initial removal of the filling material. In the Group 1 one drop of solvent Xylen (0.8 ml) was used in the pulp chamber. The solvent was used in the early steps of instrumentation and not used in the apical third. The solvent was not used in the teeth of Group 2. The R25 Reciproc instrument was used with the same protocol as used in the endodontic treatment, although it was used with brushing motion after each three in and out pecking motion and just until its reach the working length. In Group 2, 2.5% sodium hypochlorite was used in the instrumentation steps and in the final rinse. The effective time to reach the working length was recorded.
In Group 1 the Hyflex 40 taper 0.04 instrument (Coltene-Whaledent, Allstetten, Switzerland) was used as an additional step for filling removal and reinstrumentation. In Group 2 it was used Mtwo 40, taper 0.04 instruments (VDW) for the same procedure. After reaching the working length, both instruments were used with a brushing motion for 20 seconds.
The last additional step for filling removal in Group 1 was the use of passive ultrasonic irrigation (PUI) [18], with an Irrisonic tip (Helse, São Paulo, SP, Brazil) mounted in an ultrasonic device, Jet Sonic (Gnatus, São Paulo, SP, Brazil) with 20% of the power scale. Before this procedure, a drop (0,8 ml) of xylene was put in the pulp chamber for 1 minute and dried with paper points after this time. Then, it was used passive ultrasonic irrigation (PUI) with 2.5% sodium hypochlorite [10]. In Group 2, the last step for filling removal was the activation of sodium hypochlorite 2.5% with EasyClean rotary instruments in a reciprocating motion as described for the manufacturer and analyzed in a previous study [12].
The teeth were filled again with a gutta-percha and a resin-based sealer (AHPlus) but now with warm vertical condensation rather than the single cone technique used in the first treatment filling. A single cone which matched with the size and length of the working length. It was vertically condensate with a warm tip device, Touch’N Heat (SybronEndo) until 5mm from the working length was achieved. After this procedure, the canal filling was completed with backfill using BeeFill (VDW, Munich, Germany).
Micro-CT
After the storage period, the teeth were mounted on to a custom attachment and scanned in a micro computed tomography system (micro-CT) (SkyScan 1174; Bruker-microCT, Kontich, Belgium) using the following voxel parameters: 50 kV, 800 µA, and an isotropic voxel size of 39 µm. Other parameters used were 360° rotation, 0.8° step rotation and 0.5 mm aluminum filter. The samples were reconstructed with the NRecon software version 1.6.3 and the axial cross sections were obtained with parameters of Beam Hardening Correction of 30 %, Ring Artefact Corretion of 4. Volumetric analyses of the 3D models were made with similar parameters with the CTAn v.1.12 software (Bruker-micro CT), divided into 3 segments of 3 mm each, which corresponded to the apical, middle and cervical portions. The filling material volume was calculated from the binarized area inside the region of interest, that include both root canals and isthmus, with the same parameters. The volumes were recorded and converted into percentages relative to the initial volume of the filling material.
The data were analyzed using the CTAn v.1.12 software (Bruker-micro CT). The groups were confirmed for their homogeneity of the filling material volumes, anatomy, root canal lengths and angles, Vertucci classification [19], types II and IV, and they were well balanced. The angle of root canal curvature was measured as described by Schneider [20]. The teeth with root curvature angles between 25 and 35 degrees were chosen. The volume of the initial filling material and after removal were measured with the same parameters using the same CTAn software.
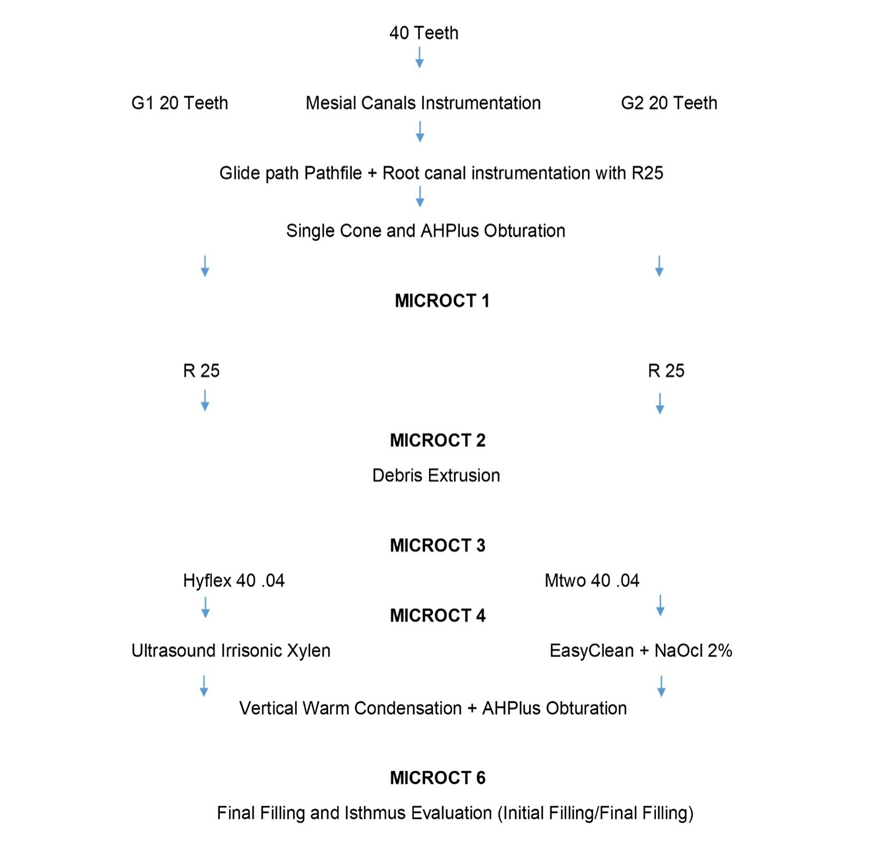
The microtomographies were made again after each step of the protocols for the groups 1 and 2, with the same parameters, as described in the summary of the experiment design (Figure 1).
Figure 1: Summary of Experimental Design.
Microtomographies were also made to evaluate the filling material extruded through the apex and the filling material in the isthmus area. The extruded material after the use of Reciproc instruments was collected in an Eppendorf half-filled with gelatin agar and adapted to the apex of each tooth during instrumentation. The space between the cervical surface of the root and the Eppendorf opening was sealed with a photoactivated resin (Top Dam, FGM, Joinville, SC, Brazil). The other microtomography was made to evaluate the initial and final filling material in the isthmus in teeth with class II Vertucci classification.
The volume of the filling material in the isthmus area were measured with Seg3D 2.2.1 software (National Institutes of Health Center for Integrative Biomedical Computing, University of Utah Scientific Computing and Imaging Institute, Salt Lake City, UT).
The dentin thickness at the medium level (6 mm from the apical foramen) of the teeth with Vertucci type II were measured in both groups after the use of Reciproc and after Hyflex and Mtwwo. The measures were made in the theCTAn v.1.12 software. It was made 3 times and the mean result selected.
Statistical analysis
Statistical analysis was performed using Prism 6.0 software (GraphPad Software Inc, L Jolla, CA, USA). The normality of the data was analyzed by the Shapiro-Wilks test, and due to the absence of normality, the Mann Whitney test was used to compare the groups in each steps of the retreatment procedure. The Wilcoxon and the Friedman and Dunn’s tests were used to compare the percentage reduction in filling material after each procedure. The significance level was established at 5%.
Results
The inclusion criteria with reference to homogeneity of the anatomy, and relative to the initial volume, and volume after each step of the filling removal, were statistically similar in both groups, which allowed for intergroup comparisons
For the both studied groups the filling material was not completely removed from inside the root canals for all levels of the root canal length (Table 1). Regarding the remaining volumes of the filling material it did not significantly differ between the two groups (P>.05).
Significant differences (P<.05) were observed in the intragroup evaluation in Group 1 (Reciproc x Hyflex x PUI) and Group 2 (Reciproc x Mtwo x EasyClean) regarding the reduction of the initial total filling material.
For the Group 1 in the apical level, there were significant differences (P<0.05) between Reciproc, Hyflex and PUI regarding the filling material removal, after each step. In the middle and cervical levels, there were significant differences (P<.05) after Hyflex; Reciproc, but not after PUI, regarding the filling material removal.
For the Group 2, in the apical and middle levels, there were significant differences (P<0.05) between Reciproc and Mtwo, but not between Mtwo and EasyClean regarding the filling material removal. In the cervical level, there were not observed significant differences between Reciproc and Mtwo (P>0.05).
Table 1: Median, minimum and maximum values of the volume percentage (%) of the filling material removal, after PUI and Easyclean and final filling material post retreatment in the different levels and total canal length of the root canal.
|
GROUP 2 |
|||||||
|
Apical |
Middle |
Cervical |
Total |
Apical |
Middle |
Cervical |
Total |
|
Reciproc |
Reciproc |
Reciproc |
Reciproc |
Reciproc |
Reciproc |
Reciproc |
Reciproc |
|
- 67% aA (35 – 97) |
- 77% aA (24 – 96) |
- 77% aA (42 – 94) |
- 78%aA (35 – 92) |
-62% aA (29 – 99) |
-73% aA (29 – 99) |
-82% aA (32 -100) |
-77% aA (41 – 91) |
|
Hyflex |
Hyflex |
Hyflex |
Hyflex |
MTwo |
MTwo |
MTwo |
MTwo |
|
- 85%aB (55 - 98) |
- 83%aB (35 - 98) |
- 80%aB (55 – 97) |
- 83%aB (54 – 96) |
-81%aB (64 -100) |
-81%aB (40 -100) |
-85%aA (34 -100) |
-84%aB (54 – 96) |
|
PUI |
PUI |
PUI |
PUI |
EasyClean |
EasyClean |
EasyClean |
EasyClean |
|
- 91 %aC (58 – 99) |
- 88 %aB (42 – 98) |
- 83 %aB (56 -100) |
- 83 %aB (56 – 96) |
-84%aB (47- 100) |
-83%aB (41– 100) |
-87%aB (56 – 99) |
-85%aC (61 – 96) |
|
Different
superscript lower-case letters in each line indicate statistical differences
between groups (P<.05). Different upper-case letters in each column
indicate statistical differences in the same group after different procedures
(P<.05). |
|||||||
However, statistical significant differences (P<.05) were observed in the comparison from EasyClean after Mtwo.
Dentin Thickness
The reduction of the dentine thickness at the medium level after the use of Mtwoinstrument was statically significant (P<.05), whereas after the use of Hyflex instrument the reduction was not statistically significant (P>.05). After M two, the reduction of dentin at the medium level was statically significant (P<.05) for the external dentin only(Table 2).
Table 2: Medium, maximum and minimum dentin thickness, in mm and percentages in the Reciproc sub-group and after the use of Hyflex instruments (G1) and in the Reciproc sub-group and after the use of Mtwo instruments (G2) in the medium level.
|
G1 |
G2 |
||||
|
IDT |
EDT |
TDT |
IDT |
EDT |
TDT |
|
Reciproc |
Reciproc |
Reciproc |
Reciproc |
Reciproc |
Reciproc |
|
0.9375a,A (0.562 - 1.64) |
1.434a,A (0.987 - 1.584) |
2.298a,A (1.737 - 3.179) |
1.039a,A (0.642 - 1.68) |
1.357a,A (1.045 - 1.592) |
2.268a,A (1.88 - 3.17) |
|
Hyflex |
Hyflex |
Hyflex |
Mtwo |
Mtwo |
Mtwo |
|
0.88a,A (0.52 - 1.38) - 8% (0 – 32) |
1.294a,A (0.899 - 1.514) - 9% (3 – 16) |
2.113a,A (1.6 - 2.891) - 9% (5 – 18) |
0.867a,A (0.615-1.525) - 12% (3 – 36) |
1.205a,B (0.823 -1.535) - 9% (1 – 31) |
2.02a,B (1.505- 3.06) - 12% (3 – 20) |
|
IDT,
Internal Dentin thickness; ED, external dentin thickness; TDT, total dentin
thickness. Different superscript lower-case letters in each line indicate
statistical differences between groups (P<.05). Different superscript
upper-case letters in each column indicate statistical differences in the
same group after different procedures (P<.05). |
|||||
Filling Material in the Retreatment
The volume of the filling material in the first treatment showed significant differences regarding the volume of the filling material after retreatment. The filling material in the endodontic retreatment compared to the filling material in the endodontic treatment was significantly enhanced in all levels evaluated(Table 3).
Table 3: Median, Maximum and Minimum values of the volume (mm³ and percentage) of the initial filling material and the filling material after retreatment.
|
|
GROUP 1 |
GROUP 2 |
||||||||
|
|
Apical |
Middle |
Cervical |
Total |
Isthmus |
Apical |
Middle |
Cervical |
Total |
Isthmus |
|
Initial Material |
1.312aA (0.590- 2.781) |
2.351aA (1.702-4.609)
|
3.968aA(3.028-8.258)
|
7.688aA
(5.860-15.648)
|
0.099aA (0.00012-0.71406)
|
1.421aA
(0.720- (2.4789) |
2.068aA
(1.768) (3.930) |
3.788aA
(2.792) (5.809) |
7.086aA
(5.673-10.743) |
0.264bA (0.02611-1.46624) |
|
Final Material |
1.877aB
(1.293-3.048) +43% (10-177)
|
3.151aB (2.657-5.578) +34% (6-85) |
4.552aB
(3.493-8.596) +15% (1-30) |
9.875aB
(7.903-17.222) +28% (8-52) |
0.196aB
(0.0000-1.02533) +45% (0-282) |
1.930aB (1.083-3.571) +36% (8-161) |
3.675aB
(2.545-4.633) +78% (18-95) |
4.581aB
(3.880-9.101) +21% (5-65) |
10.646aB (7.881-16.442) +50% (23-69) |
0.562bB (0.0769-2.24183) 86% (17-195) |
|
Different
superscript lower-case letters in the line indicate statistical differences
between groups (P<.05). Different superscript letters in each column
indicate statistical differences in the same group after different procedures
(P<.05). |
||||||||||
The evaluation of the isthmus area showed significant differences regarding the initial filling material in the first treatment relative to the filling material in the retreatment. There was an increase of volume of the filling material in the retreatment for both groups with a greater volume in Group 2 (Table 3).
The median total time for filling removal for both mesial canals of each mesial root with Reciproc were 209.40 (140.4–364.8) seconds (for Group 1) and 192.60 (188.40-381) seconds for Group 2 with no significant difference between the groups (P>.05). The amount of debris extruded were not different between groups with a mean of 0.1025 mm3 (P>.05).
Discussion
The null hypotheses were accepted since there were no differences between groups regarding the filling removal. The inclusion criteria with reference to homogeneity of the anatomy, and relative to the initial volume, and volume after the initial filling removal with reciprocating instruments were statistically similar in both groups, which allowed for intergroup comparisons.
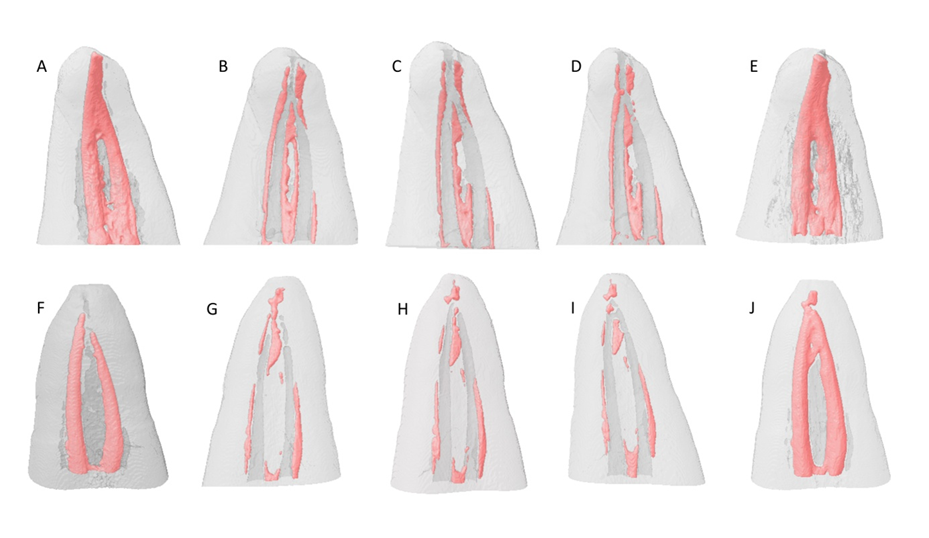
After the use of Reciproc instruments in the two protocols evaluated, it was not possible to remove completely the filling material from root canals and the less efficacy of the filling removal was observed in the apical level which is in agreement with previous studies [21-23]. In this study the amount of residual filling material in the apical third was greater than in our previous study [7]. It could be due to the methodology used in this present work. In this study, the region of interest studied (ROI) includes both canals and isthmus of the mesial roots. Therefore, all the root canal system of the mesial roots of the mandibular molars were evaluated, whereas in our previous study just the mesial-buccal canals were evaluated. The evaluation of the efficacy of the adjunctive steps in the retreatment, with the use of Hyflex, Mtwo and irrigate solution agitation were the main objectives of this study. The taper and tip of these two rotary instruments #40/.04 were chosen to increase the cleaning of the apical third. It was made due to micro-ct studies that showed a great incidence of ramifications and the presence of isthmus with an apical diameter around 0.350 mm [24,25]. Therefore, the Reciproc R25 with tip .25 is probably not efficient to clean this area. One study demonstrated that the HyFlex CM instrument preserved the original root canal shape better than the WaveOne and Reciproc reciprocating instruments, owing to its greater flexibility [26]. The incidence in vivo of Vertucci type II, two canals that merge to a single apical canal is common and can be found in 54% in vivo [24,27]. The apical area of these canals that join have usually an oval shape that difficult the filling removal (Figure 2). In our study we found 52.5% of Vertucci type II configuration in the aleatory selected teeth that were balanced shared between groups.
Figure 2: Micro-CT reconstructions of a representative sample before and after each retreatment procedure. (A and F) Initial filling, (B and G) Reciproc, (C) Hyflex, (H) Mtwo, (D) PUI, (I) EasyClean, (E and J) new filling after the retreatment.
In our study, the extruded debris through Micro – CT were evaluated. Previous studies accessed the debris with electronic balances in pre-weighted vials. This method presented viable to evaluate extrusion of material during the retreatment. In relation to the material extruded during the desobturation, the use or no of solvent did not influence in the extrusion since no differences were observed between the groups.
In one study, HyFlex CM compared with MWire instruments showed to be the most cutting efficient instrument in lateral action [28]. There were no statistic differences between Hyflex or Mtwo instruments regarding filling removal. The control memory alloy present in Hyflex have showed in some studies more flexibility than the conventional NiTi alloys present in Mtwo instruments. The lesser flexibility of Mtwoo instruments could have led to a greater reduction of the dentin thickness at the middle third of the external dentin than Hyflex instruments. Therefore, the control memory NiTi instruments could be considered a good choice for use as an additional step in the procedure of filling removal from curved mesial root canals of mandibular molars, as observed within the limits of this study.
In relation of the method of agitation of the irrigant solution, the use of passive ultrasonic irrigation (PUI) and the rotary instrument EasyClean presented similar results. In the intragroup evaluation they showed to enhance the effectiveness in the total filling material removal ability, but not for all thirds of the canal, after PUI and after the reciprocating rotary mechanical irrigant agitation step. The PUI with Irrisonic tip was statically effective in the apical third, whereas the reciprocating agitation with EasyClean was statically effective in the cervical third after Mtwo instruments. The effectiveness of PUI in root canal filling removal in curved root canals is controversial [7,10,12,29,30]. In a previous study, utilizing mesial buccal canals, the use of xylene with PUI increased the removal of filling material but it was not statically significant [7]. In the present study, the ultrasonic agitation favored a significant effective removal (p<0.05). The reason of the difference can be related with the apical diameter and the solution used in the agitation. In this study the enlargement of the apical area with instruments 40.04 maybe was responsible for the efficacy of the ultrasound in this area, whereas this was not found in our previous study with instruments 25.08 [7]. Furthermore, the PUI was made with xylene in the previous study and in this study with sodium hypochlorite 2.5% after the previous passive setting of xylene in the pulp chamber for one minute [10]. Another difference that could be responsible for this difference in the results was that in this study the two canals of the mesial canal root system including the isthmus were evaluated. The cleaning of the isthmus is a complementary and important step. One study showed that the presence of isthmus in vivo in mesial root of mandibular molars is very often (64%) and it is located in 30.3% in the cervical third, 14.8% in the middle third, and 44.3% in the apical third [31].
The cervical third can be accessed with ease and more precisely due to the better visualization with the microscope which allows a better cleaning [32]. It could also have collaborated for the better cleaning at the cervical third after EasyClean, since the isthmus in the cervical third is present very often. The better results for cleaning with PUI in the apical area, could be due to the better effectiveness of the ultrasound in the tip of the instrument and to the pre-shaping before its use [33]. The warm vertical condensation technique could also improve the filling material in the isthmus after retreatment.
In relation to the second obturation, a statistical significant increase (P<.05), for both groups, in the volume of filling material in the isthmus area was observed, with better results for G2. In this group where xylene was not used for filling removal, it could be allowed a greater volume of filling in the isthmus after re-filling in the re-treatment. It possibly happened due to the softened gutta-percha and sealer becoming a thin layer, in the presence of solvents, that can difficult their removal [34] and impair the isthmus area for cleaning as well as the presence of the new filling material.
Regarding to the time necessary to reach the working length, no statistical significant differences were found between the groups, demonstrating that the use of solvent did not favor the instrument to reach the working length. The control memory 0.4 instrument used in this study showed to be effective and safe. It is important because the medium and cervical third of the dentin thickness should be preserved from excessive enlargement [35].
Conclusion
None of the protocols completely removed the filling material. The use of rotary instruments and a complementary step with irrigant agitation after the initial filling removal with reciprocating instruments showed to be effective for a better cleaning and filling removal. The better results were found for the apical level and after passive ultrasonic irrigation. The greater flexibility of NiTi control memory instruments than that of the conventional NiTi instruments did not reduce the dentin cutting, filling removal and working time effectiveness. The two protocols evaluated followed by vertical warm condensation filling technique enhanced the volume of filling material in the root canal system including the isthmus.
Compliance with Ethical Standards
Conflict of Interest
Dr. Lincoln de Campos Fruchi declares that he has no conflict of interest. Dr. Murilo Priori Alcalde declares that he has no conflict of interest. Dr. Pablo Andres Amoroso-Silva declares that he has no conflict of interest. Dr. Rodrigo Ricci Vivan declares that he has no conflict of interest. Dr. Clovis Monteiro Bramante declares that he has no conflict of interest. Dr. Marco Antonio Hungaro Duarte declares that he has no conflict of interest.
Funding
This study was supported by State of São Paulo Research Foundation, FAPESP (2015/03829-1).
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors. All procedures performed in this study were in accordance with the ethical standards of the Committee of Bauru School of Dentistry, University of São Paulo (CAAE: 44736215.9.0000.5417) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
For this type of study, formal consent is not required.
References
1. Siqueira JF, Rôças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod. 2008;34(11):1291-1301.e1293.
2. Ng YL, Mann V, Gulabivala K. Outcome of secondary root canal treatment: a systematic review of the literature. Int Endod J. 2008;41(12):1026-1046.
3. Torabinejad M, Corr R, Handysides R, Shabahang S. Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod. 2009;35(7):930-937.
4. Betti LV, Bramante CM, de Moraes IG, Bernardineli N, Garcia RB. Efficacy of Profile .04 taper series 29 in removing filling materials during root canal retreatment--an in vitro study. Oral Surg Oral Med Oral Pathol Oral RadiolEndod. 2009;108(6):e46-50.
5. de Mello Junior JE, Cunha RS, Bueno CE, Zuolo ML. Retreatment efficacy of gutta-percha removal using a clinical microscope and ultrasonic instruments: part I--an ex vivo study. Oral Surg Oral Med Oral Pathol Oral RadiolEndod. 2009;108(1):e59-62.
6. Rödig T, Reicherts P, Konietschke F, Dullin C, Hahn W, Hülsmann M. Efficacy of reciprocating and rotary NiTi instruments for retreatment of curved root canals assessed by micro-CT. Int Endod J. 2014;47(10):942-948.
7. Fruchi LeC, Ordinola-Zapata R, Cavenago BC, Hungaro Duarte MA, Bueno CE, De Martin AS. Efficacy of reciprocating instruments for removing filling material in curved canals obturated with a single-cone technique: a micro-computed tomographic analysis. J Endod. 2014;40(7):1000-1004.
8. Shen Y, Zhou HM, Zheng YF, Peng B, Haapasalo M. Current challenges and concepts of the thermomechanical treatment of nickel-titanium instruments. J Endod. 2013;39(2):163-172.
9. Goo HJ, Kwak SW, Ha JH, Pedullà E, Kim HC. Mechanical Properties of Various Heat-treated Nickel-titanium Rotary Instruments. J Endod. 2017;43(11):1872-1877.
10. Cavenago BC, Ordinola-Zapata R, Duarte MA, del Carpio-Perochena AE, Villas-Bôas MH, Marciano MA, et al. Efficacy of xylene and passive ultrasonic irrigation on remaining root filling material during retreatment of anatomically complex teeth. Int Endod J. 2014;47(11):1078-1083.
11. Saoud TM, Huang GT, Gibbs JL, Sigurdsson A, Lin LM. Management of Teeth with Persistent Apical Periodontitis after Root Canal Treatment Using Regenerative Endodontic Therapy. J Endod. 2015;41(10):1743-1748.
12. Kato AS, Cunha RS, da Silveira Bueno CE, Pelegrine RA, Fontana CE, de Martin AS. Investigation of the Efficacy of Passive Ultrasonic Irrigation Versus Irrigation with Reciprocating Activation: An Environmental Scanning Electron Microscopic Study. J Endod. 2016;42(4):659-663.
13. Duque JA, Duarte MA, Canali LC, Zancan RF, Vivan RR, Bernardes RA, et al. Comparative Effectiveness of New Mechanical Irrigant Agitating Devices for Debris Removal from the Canal and Isthmus of Mesial Roots of Mandibular Molars. J Endod. 2017;43(2):326-331.
14. Rodrigues CT, Duarte MA, de Almeida MM, de Andrade FB, Bernardineli N. Efficacy of CM-Wire, M-Wire, and Nickel-Titanium Instruments for Removing Filling Material from Curved Root Canals: A Micro-Computed Tomography Study. J Endod. 2016;42(11):1651-1655.
15. Yürüker S, Görduysus M, Küçükkaya S, Uzunoğlu E, Ilgın C, Gülen O, et al. Efficacy of Combined Use of Different Nickel-Titanium Files on Removing Root Canal Filling Materials. J Endod. 2016;42(3):487-492.
16. Rios MeA, Villela AM, Cunha RS, Velasco RC, De Martin AS, Kato AS, et al. Efficacy of 2 reciprocating systems compared with a rotary retreatment system for gutta-percha removal. J Endod. 2014;40(4):543-546.
17. Zuolo AS, Mello JE, Cunha RS, Zuolo ML, Bueno CE. Efficacy of reciprocating and rotary techniques for removing filling material during root canal retreatment. Int Endod J. 2013;46(10):947-953.
18. van der Sluis LW, Vogels MP, Verhaagen B, Macedo R, Wesselink PR. Study on the influence of refreshment/activation cycles and irrigants on mechanical cleaning efficiency during ultrasonic activation of the irrigant. J Endod. 2010;36(4):737-740.
19. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589-599.
20. Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971;32(2):271-275.
21. Crozeta BM, Silva-Sousa YT, Leoni GB, Mazzi-Chaves JF, Fantinato T, Baratto-Filho F, et al. Micro-Computed Tomography Study of Filling Material Removal from Oval-shaped Canals by Using Rotary, Reciprocating, and Adaptive Motion Systems. J Endod. 2016;42(5):793-797.
22. Reddy N, Admala SR, Dinapadu S, Pasari S, Reddy MP, Rao MS. Comparative analysis of efficacy and cleaning ability of hand and rotary devices for gutta-percha removal in root canal retreatment: an in vitro study. J Contemp Dent Pract. 2013;14(4):635-643.
23. Romeiro K, de Almeida A, Cassimiro M, Gominho L, Dantas E, Chagas N, et al. Reciproc and Reciproc Blue in the removal of bioceramic and resin-based sealers in retreatment procedures. Clin Oral Investig. 2020;24(1):405-416.
24. Keleş A, Keskin C. Apical Root Canal Morphology of Mesial Roots of Mandibular First Molar Teeth with Vertucci Type II Configuration by Means of Micro-Computed Tomography. J Endod. 2017;43(3):481-485.
25. Villas-Bôas MH, Bernardineli N, Cavenago BC, Marciano M, Del Carpio-Perochena A, de Moraes IG, et al. Micro-computed tomography study of the internal anatomy of mesial root canals of mandibular molars. J Endod. 2011;37(12):1682-1686.
26. Marceliano-Alves MF, Sousa-Neto MD, Fidel SR, Steier L, Robinson JP, Pécora JD, et al. Shaping ability of single-file reciprocating and heat-treated multifile rotary systems: a micro-CT study. Int Endod J. 2015;48(12):1129-1136.
27. Gambarini G, Ropini P, Piasecki L, Costantini R, Carneiro E, Testarelli L, et al. A preliminary assessment of a new dedicated endodontic software for use with CBCT images to evaluate the canal complexity of mandibular molars. Int Endod J 2018;51(3):259-268.
28. Morgental RD, Vier-Pelisser FV, Kopper PM, de Figueiredo JA, Peters OA. Cutting efficiency of conventional and martensitic nickel-titanium instruments for coronal flaring. J Endod 2013;39(12):1634-1638.
29. Barreto MS, Rosa RA, Santini MF, Cavenago BC, Duarte MA, Bier CA, et al. Efficacy of ultrasonic activation of NaOCl and orange oil in removing filling material from mesial canals of mandibular molars with and without isthmus. J Appl Oral Sci 2016;24(1):37-44.
30. van der Sluis LW, Versluis M, Wu MK, Wesselink PR. Passive ultrasonic irrigation of the root canal: a review of the literature. Int Endod J. 2007;40(6):415-426.
31. Tahmasbi M, Jalali P, Nair MK, Barghan S, Nair UP. Prevalence of Middle Mesial Canals and Isthmi in the Mesial Root of Mandibular Molars: An In Vivo Cone-beam Computed Tomographic Study. J Endod. 2017;43(7):1080-1083.
32. Schirrmeister JF, Hermanns P, Meyer KM, Goetz F, Hellwig E. Detectability of residual Epiphany and gutta-percha after root canal retreatment using a dental operating microscope and radiographs--an ex vivo study. Int Endod J. 2006;39(7):558-565.
33. Ahmad M, Roy RA, Kamarudin AG. Observations of acoustic streaming fields around an oscillating ultrasonic file. Endod Dent Traumatol. 1992;8(5):189-194.
34. Gu LS, Ling JQ, Wei X, Huang XY. Efficacy of ProTaper Universal rotary retreatment system for gutta-percha removal from root canals. Int Endod J. 2008;41(4):288-295.
35. Pinto JC, Torres FFE, Santos-Junior AO, Duarte MAH, Guerreiro-Tanomaru JM, Tanomaru-Filho M. Safety and Effectiveness of Additional Apical Preparation using a Rotary Heat-treated Nickel-Titanium file with Larger Diameter and Minimum Taper in Retreatment of Curved Root Canals. Eur J Dent. 2021.