Daytime Changes in Tear Film Parameters and Visual Acuity with New-Generation Daily Disposable Silicone Hydrogel Contact Lenses—A Double-Masked Study in Symptomatic Subjects

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Subjects
2.2. Contact Lenses
2.3. Clinical Examination Routine
2.4. Comfort Assessment
2.5. Visual Acuity
2.6. Noninvasive Tear Break-Up Time (NIBUT)
2.7. Dynamic Topography
2.8. Statistical Analysis
3. Results
3.1. Sample Characteristics—Baseline Results
3.2. Visual Acuity
3.3. Pre-Lens NIBUT
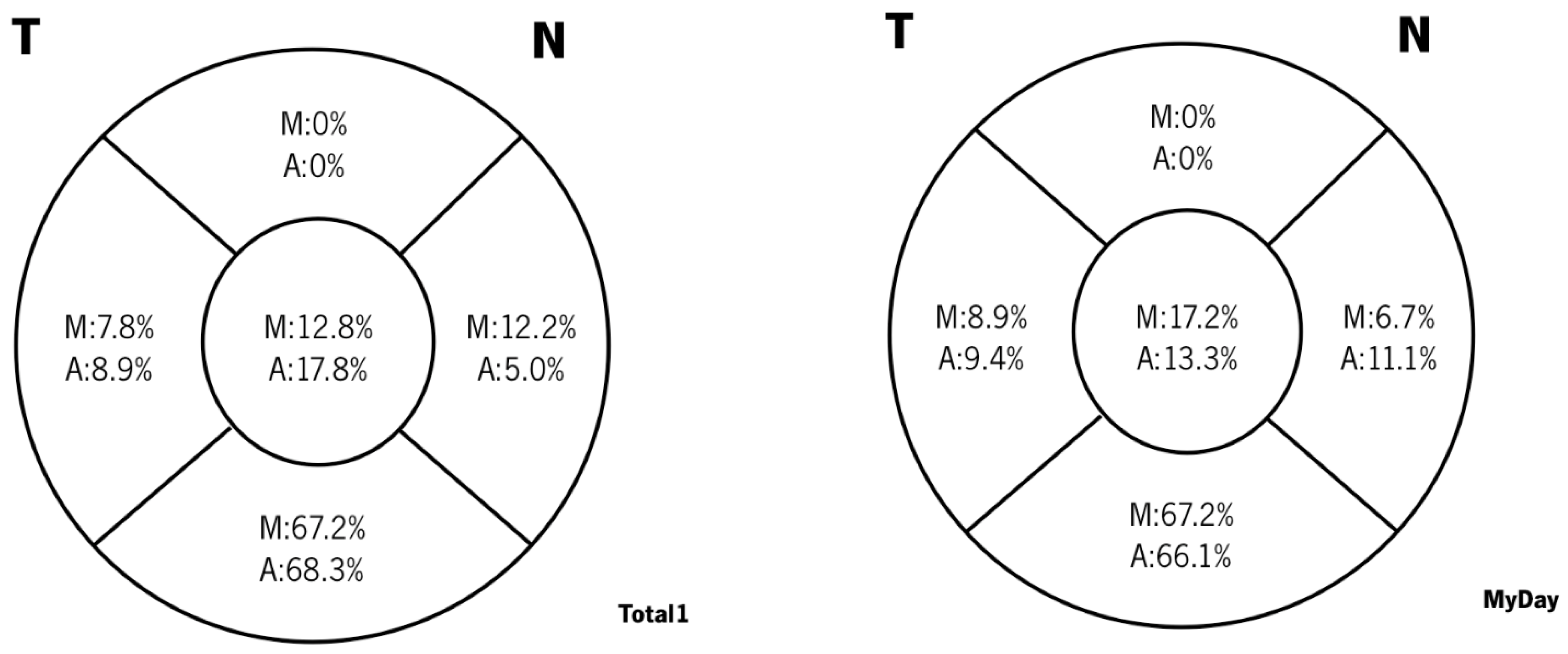
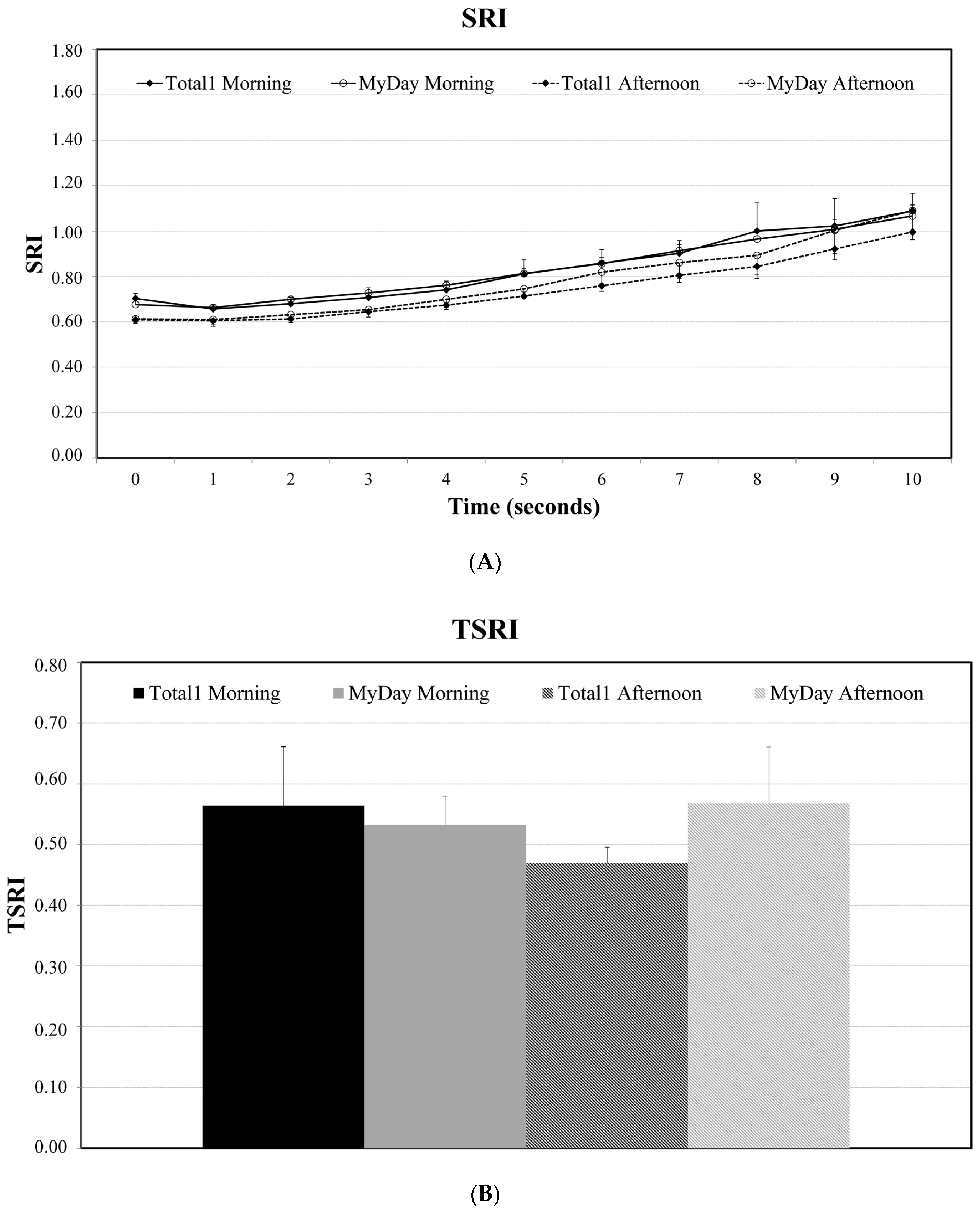
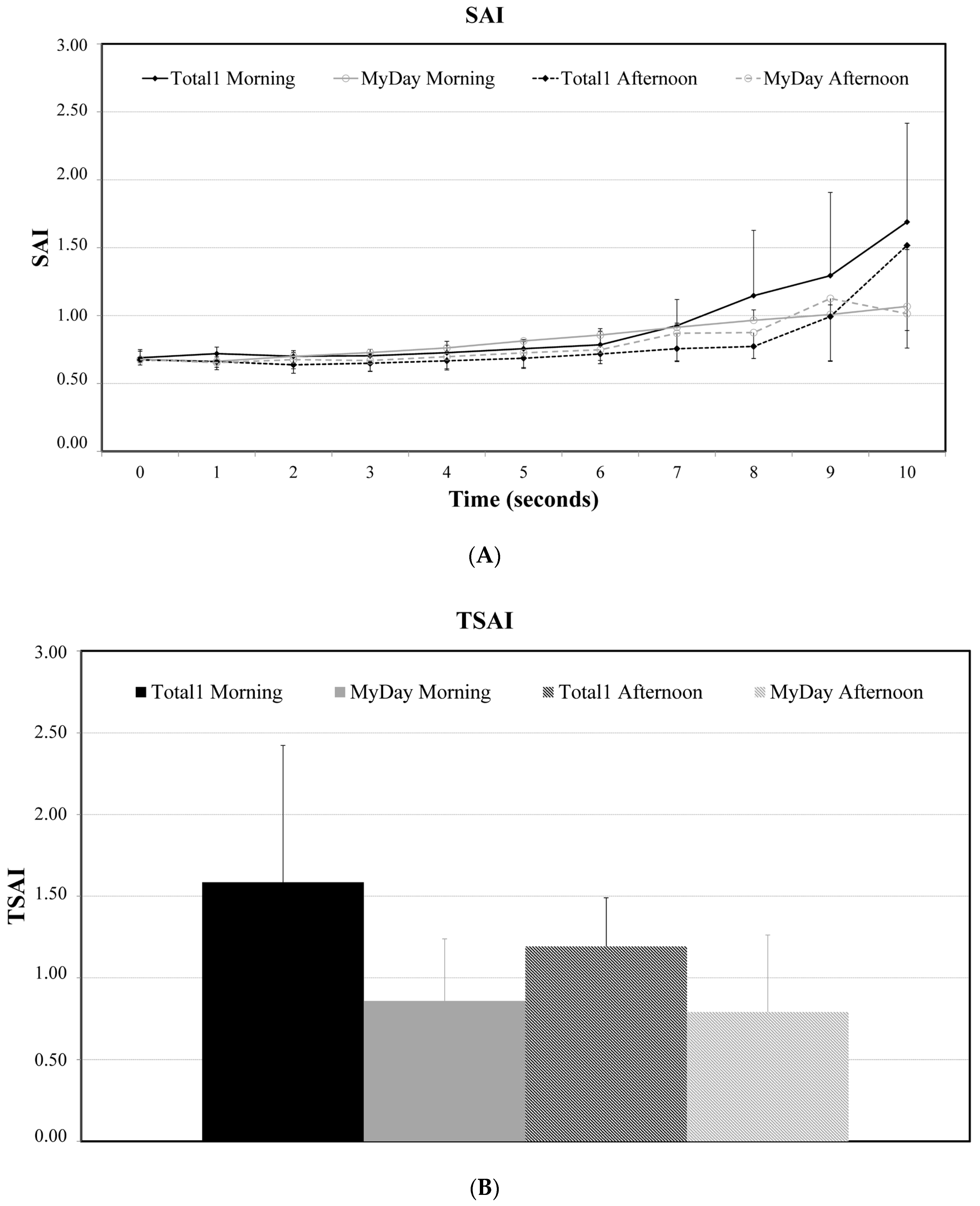
3.4. Dynamic Topography
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Koh, S.; Tung, C.I.; Inoue, Y.; Jhanji, V. Effects of tear film dynamics on quality of vision. Br. J. Ophthalmol. 2018, 102, 1615–1620. [Google Scholar] [CrossRef] [PubMed]
- Montés-Micó, R.; Alió, J.L.; MuñOz, G.; Charman, W.N. Temporal Changes in Optical Quality of Air–Tear Film Interface at Anterior Cornea after Blink. Investig. Opthalmol. Vis. Sci. 2004, 45, 1752–1757. [Google Scholar] [CrossRef] [PubMed]
- Albarrán, C.; Pons, A.; Lorente, A.; Montés, R.; Artigas, J. Influence of the tear film on optical quality of the eye. Contact Lens Anterior Eye 1997, 20, 129–135. [Google Scholar] [CrossRef]
- Tutt, R.; Bradley, A.; Begley, C.; Thibos, L.N. Optical and visual impact of tear break-up in human eyes. Investig. Ophthalmol. Vis. Sci. 2000, 41, 4117–4123. [Google Scholar]
- Montés-Micó, R.; Cervino, A.; Ferrer-Blasco, T.; García-Lázaro, S.; Madrid-Costa, D. The Tear Film and the optical Quality of the Eye. Ocul. Surf. 2010, 8, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Montés-Micó, R. Role of the tear film in the optical quality of the human eye. J. Cataract Refract. Surg. 2007, 33, 1631–1635. [Google Scholar] [CrossRef] [PubMed]
- Nagahara, Y.; Koh, S.; Maeda, N.; Nishida, K.; Watanabe, H. Prominent Decrease of Tear Meniscus Height With Contact Lens Wear and Efficacy of Eye Drop Instillation. Eye Contact Lens Sci. Clin. Pract. 2015, 41, 318–322. [Google Scholar] [CrossRef]
- Yokoi, N.; Eftimov, P.; Georgiev, G.A. Dynamic Aspects of Pre-Soft Contact Lens Tear Film and Their Relation to Dry Eye: Basic Science and Clinical Relevance. Life 2023, 13, 859. [Google Scholar] [CrossRef]
- Nichols, K.K.; Redfern, R.L.; Jacob, J.T.; Nelson, J.D.; Fonn, D.; Forstot, S.L.; Huang, J.-F.; Holden, B.A.; Nichols, J.J. The TFOS International Workshop on Contact Lens Discomfort: Report of the Definition and Classification Subcommittee. Investig. Opthalmology Vis. Sci. 2013, 54, TFOS14. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef]
- Kojima, T. Contact Lens-Associated Dry Eye Disease: Recent Advances Worldwide and in Japan. Investig. Opthalmology Vis. Sci. 2018, 59, DES102. [Google Scholar] [CrossRef] [PubMed]
- McMonnies, C.W. Why are soft contact lens wear discontinuation rates still too high? Expert Rev. Ophthalmol. 2023, 18, 11–18. [Google Scholar] [CrossRef]
- Pucker, A.D.; Tichenor, A.A. A Review of Contact Lens Dropout. Clin. Optom. 2020, 12, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Foulks, G.; Chalmers, R.; Keir, N.; Woods, C.A.; Simpson, T.; Lippman, R.; Gleason, W.; Schaumberg, D.A.; Willcox, M.D.P.; Jalbert, I. The TFOS International Workshop on Contact Lens Discomfort: Report of the Subcommittee on Clinical Trial Design and Outcomes. Investig. Opthalmol. Vis. Sci. 2013, 54, TFOS157. [Google Scholar] [CrossRef] [PubMed]
- García-Marqués, J.V.; Macedo-De-Araújo, R.J.; McAlinden, C.; Faria-Ribeiro, M.; Cerviño, A.; González-Méijome, J.M. Short-term tear film stability, optical quality and visual performance in two dual-focus contact lenses for myopia control with different optical designs. Ophthalmic Physiol. Opt. 2022, 42, 1062–1073. [Google Scholar] [CrossRef] [PubMed]
- García-Marqués, J.V.; Macedo-De-Araújo, R.; Lopes-Ferreira, D.; Cerviño, A.; García-Lázaro, S.; González-Méijome, J.M. Tear film stability over a myopia control contact lens compared to a monofocal design. Clin. Exp. Optom. 2022, 105, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Lafosse, E.; Martínez-Albert, N.; Wolffsohn, J.S.W.; Cerviño, A.; García-Lázaro, S. Response of the Aging Eye to First Day of Modern Material Contact Lens Wear. Eye Contact Lens Sci. Clin. Pract. 2019, 45, 40–45. [Google Scholar] [CrossRef]
- Szczesna-Iskander, D.H. Comparison of Tear Film Surface Quality Measured In Vivo on Water Gradient Silicone Hydrogel and Hydrogel Contact Lenses. Eye Contact Lens Sci. Clin. Pract. 2014, 40, 23–27. [Google Scholar] [CrossRef]
- García-Montero, M.; Rico-Del-Viejo, L.; Martínez-Alberquilla, I.; Hernández-Verdejo, J.L.; Lorente-Velázquez, A.; Madrid-Costa, D. Effects of Blink Rate on Tear Film Optical Quality Dynamics with Different Soft Contact Lenses. J. Ophthalmol. 2019, 2019, 4921538. [Google Scholar] [CrossRef]
- García-Montero, M.; Rico-Del-Viejo, L.; Llorens-Quintana, C.; Lorente-Velázquez, A.; Hernández-Verdejo, J.L.; Madrid-Costa, D. Randomized crossover trial of silicone hydrogel contact lenses. Contact Lens Anterior Eye 2019, 42, 475–481. [Google Scholar] [CrossRef]
- Patel, S.; Bevan, R.; Farrell, J.C. Diurnal Variation in Precorneal Tear Film Stability. Optom. Vis. Sci. 1988, 65, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Lira, M.; Oliveira, M.E.C.R.; Franco, S. Comparison of the tear film clinical parameters at two different times of the day. Clin. Exp. Optom. 2011, 94, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Bitton, E.; Keech, A.; Jones, L.; Simpson, T. Subjective and Objective Variation of the Tear Film Pre- and Post-Sleep. Optom. Vis. Sci. 2008, 85, 740–749. [Google Scholar] [CrossRef] [PubMed]
- Pena-Verdeal, H.; García-Resúa, C.; Ramos, L.; Yebra-Pimentel, E.; Giráldez, M.J. Diurnal variations in tear film break-up time determined in healthy subjects by software-assisted interpretation of tear film video recordings. Clin. Exp. Optom. 2016, 99, 142–148. [Google Scholar] [CrossRef] [PubMed]
- DU Toit, R.; Situ, P.; Simpson, T.; Fonn, D. The Effects of Six Months of Contact Lens Wear on the Tear Film, Ocular Surfaces, and Symptoms of Presbyopes. Optom. Vis. Sci. 2001, 78, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Cho, P.B.O.; Yap, M.O. Age, Gender, and Tear Break-Up Time. Optom. Vis. Sci. 1993, 70, 828–831. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Boyd, K.E.; Burns, J. Age, stability of the precorneal tear film and the refractive index of tears. Contact Lens Anterior Eye 2000, 23, 44–47. [Google Scholar] [CrossRef]
- Maïssa, C.; Guillon, M. Tear film dynamics and lipid layer characteristics—Effect of age and gender. Contact Lens Anterior Eye 2010, 33, 176–182. [Google Scholar] [CrossRef]
- Sweeney, D.F.; Millar, T.J.; Raju, S.R. Tear film stability: A review. Exp. Eye Res. 2013, 117, 28–38. [Google Scholar] [CrossRef]
- Özcura, F.; Aydin, S.; Helvaci, M.R. Ocular Surface Disease Index for the Diagnosis of Dry Eye Syndrome. Ocul. Immunol. Inflamm. 2007, 15, 389–393. [Google Scholar] [CrossRef]
- Pastor-Zaplana, J.; Borrás, F.; Gallar, J.; Acosta, M.C. OSDI Questions on Daily Life Activities Allow to Detect Subclinical Dry Eye in Young Contact Lens Users. J. Clin. Med. 2022, 11, 2626. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and Validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Németh, J.; Erdélyi, B.; Csákány, B.; Gaspar, P.; Soumelidis, A.; Kahlesz, F.; Lang, Z. High-speed videotopographic measurement of tear film build-up time. Investig. Ophthalmol. Vis. Sci. 2002, 43, 1783–1790. [Google Scholar]
- Wilson, S.E.; Klyce, S.D. Advances in the analysis of corneal topography. Surv. Ophthalmol. 1991, 35, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Burns, D.M.; Johnston, F.M.; Frazer, D.G.; Patterson, C.; Jackson, A.J. Keratoconus: An analysis of corneal asymmetry. Br. J. Ophthalmol. 2004, 88, 1252–1255. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.E.; Lin, D.T.; Klyce, S.D. Corneal topography of keratoconus. Cornea 1991, 10, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Kojima, T.; Ishida, R.; Dogru, M.; Goto, E.; Takano, Y.; Matsumoto, Y.; Kaido, M.; Ohashi, Y.; Tsubota, K. A New Noninvasive Tear Stability Analysis System for the Assessment of Dry Eyes. Investig. Opthalmology Vis. Sci. 2004, 45, 1369–1374. [Google Scholar] [CrossRef]
- Belda-Salmerón, L.; Ferrer-Blasco, T.; Albarrán-Diego, C.; Madrid-Costa, D.; Montés-Micó, R. Diurnal Variations in Visual Performance for Disposable Contact Lenses. Optom. Vis. Sci. 2013, 90, 682–690. [Google Scholar] [CrossRef]
- Pettersson, A.L.; Mårtensson, L.; Salkic, J.; Unsbo, P.; Brautaset, R. Spherical aberration in relation to visual performance in contact lens wear. Contact Lens Anterior Eye 2011, 34, 12–16. [Google Scholar] [CrossRef]
- Mengher, L.S.; Bron, A.J.; Tonge, S.R.; Gilbert, D.J. A non-invasive instrument for clinical assessment of the pre-corneal tear film stability. Curr. Eye Res. 1985, 4, 1–7. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Mroczkowska, S.; Hunt, O.A.; Bilkhu, P.; Drew, T.; Sheppard, A. Crossover Evaluation of Silicone Hydrogel Daily Disposable Contact Lenses. Optom. Vis. Sci. 2015, 92, 1063–1068. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, G.S.; Sujakhu, D.; Shrestha, J.B.; Shrestha, J.K. Tear Film Evaluation in Contact Lens Wearers and Non-Wearers. J. Inst. Med. 2012, 34, 14–20. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Hunt, O.A.; Chowdhury, A. Objective clinical performance of ‘comfort-enhanced’ daily disposable soft contact lenses. Contact Lens Anterior Eye 2010, 33, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Glasson, M.J.; Stapleton, F.; Keay, L.; Willcox, M. The effect of short term contact lens wear on the tear film and ocular surface characteristics of tolerant and intolerant wearers. Contact Lens Anterior Eye 2006, 29, 41–47. [Google Scholar] [CrossRef] [PubMed]
- de Paiva, C.S.; Lindsey, J.L.; Pflugfelder, S.C. Assessing the severity of keratitis sicca with videokeratoscopic indices. Ophthalmology 2003, 110, 1102–1109. [Google Scholar] [CrossRef] [PubMed]
- Kopf, M.; Yi, F.; Iskander, D.R.; Collins, M.J.; Shaw, A.J.; Straker, B. Tear Film Surface Quality with Soft Contact Lenses Using Dynamic Videokeratoscopy. J. Optom. 2008, 1, 14–21. [Google Scholar] [CrossRef]
- Iskander, D.R.; Collins, M.J. Applications of high-speed videokeratoscopy. Clin. Exp. Optom. 2005, 88, 223–231. [Google Scholar] [CrossRef]
- Németh, J.; Erdélyi, B.; Csákány, B. Corneal topography changes after a 15 s pause in blinking. J. Cataract Refract. Surg. 2001, 27, 589–592. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Lens | Material | Diameter (mm) | Base Curve (mm) | Centre Thickness (mm) | Water Content (%) | DK/t | Modulus (MPa) |
|---|---|---|---|---|---|---|---|
| Total1 | Delefilcon A | 14.1 | 8.5 | 0.09 | >80% at surface 33% at core | 156 | 0.7 |
| MyDay | Stenfilcon A | 14.2 | 8.4 | 0.08 | 54% | 100 | 0.4 |
| Parameter | Description |
|---|---|
| N | 20 |
| Gender | 13 F (65%) |
| 7 M (35%) | |
| Age (years) | 26.75 ± 6.28 |
| 26.92 ± 6.4 F | |
| 26.42 ± 6.6 Ma | |
| Habitual refraction (D) Mean ± SD | Pre-Delefilcon A Eye |
| −1.97 ± 1.14 DS | |
| −0.11 ± 0.27 DC | |
| Pre-Stenfilcon A Eye | |
| −1.88 ± 1.15 DS | |
| −0.16 ± 0.33 DC | |
| Keratometry Mean ± SD | Pre-Delefilcon A Eye: 7.71 ± 0.26 (D) |
| Pre-Stenfilcon A Eye: 7.79 ± 0.26 (D) | |
| Habitual correction | Glasses and sporadic CL wear: 5 |
| Sporadic CL wear only: 2 | |
| Daily disposable CL wear: 5 | |
| Monthly CL (daily wear): 8 | |
| NIBUT (seconds) Mean ± SD | Pre-Delefilcon A Eye: 7.73 ± 2.2 s |
| Pre-Stenfilcon A Eye: 8.3 ± 2.9 s | |
| OSDI Mean ± SD | 32.95 ± 9.82 (range: 16.67 to 56.25) |
| 33.36 ± 9.7 F | |
| 32.70 ± 10.9 Ma |
| HCVA | LCVA | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Day 1 | Day 2 | Day 3 | Mean p (a) | Day 1 | Day 2 | Day 3 | Mean p (a) | ||
| Delefilcon A | Morning | −0.05 ± 0.07 | −0.05 ± 0.10 | −0.07 ± 0.11 | −0.06 ± 0.08 0.821 * | 0.17 ± 0.10 | 0.16 ± 0.11 | 0.13 ± 0.12 | 0.16 ± 0.10 0.081 + |
| Afternoon | −0.03 ± 0.10 | −0.05 ± 0.10 | −0.08 ± 0.10 | −0.05 ± 0.09 0.021 + | 0.17 ± 0.12 | 0.14 ± 0.10 | 0.13 ± 0.12 | 0.15 ± 0.10 0.043 + | |
| Difference p (b) | −0.02 ± 0.06, 0.144 º | 0.00 ± 0.07, 0.984 × | 0.01 ± 0.06, 0.425 º | 0.00 ± 0.07 0.950 º | 0.02 ± 0.06, 0.079 º | 0.00 ± 0.06, 0.801 º | |||
| Stenfilcon A | Morning | −0.04 ± 0.09 | −0.04 ± 0.11 | −0.06 ± 0.11 | −0.04 ± 0.09 0.771 * | 0.17 ± 0.09 | 0.15 ± 0.12 | 0.12 ± 0.09 | 0.15 ± 0.08 0.196 * |
| Afternoon | −0.05 ± 0.10 | −0.05 ± 0.10 | −0.06 ± 0.09 | −0.05 ± 0.09 0.877 * | 0.14 ± 0.11 | 0.12 ± 0.08 | 0.12 ± 0.11 | 0.13 ± 0.09 0.766 * | |
| Difference p (b) | 0.01 ± 0.06 0.468 º | 0.01 ± 0.08 0.484 º | 0.00 ± 0.08 0.769 º | 0.04 ± 0.06 0.024 º | 0.04 ± 0.12 0.304 × | 0.00 ± 0.05 0.729 º | |||
| BINOCULAR | Morning | −0.15 ± 0.17 | −0.12 ± 0.07 | −0.14 ± 0.08 | −0.14 ± 0.09 0.513 + | 0.09 ± 0.06 | 0.06 ± 0.07 | 0.04 ± 0.05 | 0.06 ± 0.05 0.068 * |
| Afternoon | −0.12 ± 0.08 | −0.13 ± 0.06 | −0.12 ± 0.08 | −0.13 ± 0.07 0.921 * | 0.06 ± 0.06 | 0.05 ± 0.05 | 0.05 ± 0.06 | 0.05 ± 0.05 0.461 + | |
| Difference p (b) | −0.02 ± 0.16, 0.636 × | 0.01 ± 0.04, 0.280 º | −0.01 ± 0.07, 0.452 × | 0.03 ± 0.05, 0.029 º | 0.01 ± 0.05, 0.267 º | −0.01 ± 0.04, 0.391 º | |||
| Day 1 | Day 2 | Day 3 | Mean (s) p (a) | ||
|---|---|---|---|---|---|
| Delefilcon A | Morning | 5.94 ± 1.58 | 5.27 ± 1.33 | 5.57 ± 1.31 | 5.59 ± 1.05 0.387 + |
| Afternoon | 5.21 ± 0.82 | 4.80 ± 0.86 | 4.83 ± 1.17 | 4.95 ± 0.63 0.326 * | |
| Difference p (b) | 0.73 ± 1.63 0.102 × | 0.47 ± 1.22 0.101 º | 0.74 ± 1.58 0.048 × | ||
| Stenfilcon A | Morning | 5.97 ± 1.58 | 5.45 ± 1.15 | 5.66 ± 1.43 | 5.69 ± 1.21 0.165 + |
| Afternoon | 5.07 ± 0.79 | 4.87 ± 1.32 | 4.93 ± 1.95 | 4.96 ± 0.93 0.200 + | |
| Difference p (b) | 0.89 ± 1.29 0.006 º | 0.58 ± 0.99 0.017 º | 0.74 ± 1.90 0.007 × |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macedo-de-Araújo, R.J.; Rico-del-Viejo, L.; Martin-Montañez, V.; Queirós, A.; González-Méijome, J.M. Daytime Changes in Tear Film Parameters and Visual Acuity with New-Generation Daily Disposable Silicone Hydrogel Contact Lenses—A Double-Masked Study in Symptomatic Subjects. Vision 2024, 8, 11. https://doi.org/10.3390/vision8010011
Macedo-de-Araújo RJ, Rico-del-Viejo L, Martin-Montañez V, Queirós A, González-Méijome JM. Daytime Changes in Tear Film Parameters and Visual Acuity with New-Generation Daily Disposable Silicone Hydrogel Contact Lenses—A Double-Masked Study in Symptomatic Subjects. Vision. 2024; 8(1):11. https://doi.org/10.3390/vision8010011
Chicago/Turabian StyleMacedo-de-Araújo, Rute J., Laura Rico-del-Viejo, Vicente Martin-Montañez, António Queirós, and José M. González-Méijome. 2024. "Daytime Changes in Tear Film Parameters and Visual Acuity with New-Generation Daily Disposable Silicone Hydrogel Contact Lenses—A Double-Masked Study in Symptomatic Subjects" Vision 8, no. 1: 11. https://doi.org/10.3390/vision8010011