Less Typical Courses of Rhodococcus equi Infections in Foals
by
 , and
, and
Alicja Rakowska
1,* ,
,
Agnieszka Marciniak-Karcz
2,
Andrzej Bereznowski
1,
Anna Cywińska
3,
Monika Żychska
1 and
Lucjan Witkowski
1 1
Division of Veterinary Epidemiology and Economics, Institute of Veterinary Medicine, Warsaw University of Life Sciences, 02-787 Warsaw, Poland
2
Private Veterinary Practice, 13-400 Aubagne, France
3
Faculty of Biological and Veterinary Sciences, Nicolaus Copernicus University, 87-100 Toruń, Poland
*
Author to whom correspondence should be addressed.
Vet. Sci. 2022, 9(11), 605; https://doi.org/10.3390/vetsci9110605
Submission received: 22 September 2022
/
Revised: 18 October 2022
/
Accepted: 27 October 2022
/
Published: 31 October 2022
(This article belongs to the Section Veterinary Internal Medicine)
Abstract
:Simple Summary
For decades, Rhodococcus equi infections remain one of the most common causes of death in foals before weaning, coming from endemic studs. The pathogen can create many problems other than its classical form—pneumonia. Such issues are described in the clinical cases presented in this paper. The first case concerns the potential contribution of rhodococcal infection to a grave outcome in a prematurely born foal lost as a yearling. Another presents so-called “extrapulmonary disorders” (EPD) and a theory of inherited immunodeficiency in a breeding dam line from one stud. The third case is connected with a suspected atypical location of the pulmonary abscess. The last example is associated with drug-induced anhidrosis. These clinical pictures may be considered rare or interesting and worth presenting in a scientific report.
Abstract
This article aims to present several interesting and less typical courses of Rhodococcus equi infections in foals, collected during the 2019–2021 foaling seasons in some Polish studs. The study was conducted by the Division of Veterinary Epidemiology and Economics, Warsaw University of Life Sciences—SGGW, and concentrated on ultrasonographic contribution to diagnostics and treatment of the disease. Among many standard cases of rhodococcal pneumonia, some rare ones occurred. The aforementioned issues include the potential contribution of rhodococcal infection to a grave outcome in a prematurely born filly, lost as a yearling, so-called “extrapulmonary disorders” (EPD), a hypothesis of inherited immunodeficiency with grave outcome in a breeding dam line from one stud, and macrolide-induced anhidrosis. The main benefit of this report would be to supplement the general picture of clinical rhodococcosis.
1. Introduction
For many decades, Rhodococcus equi remains one of the main problems in foals before weaning worldwide. Despite being thoroughly described, this ubiquitous, opportunistic, intracellular, Gram + pathogen creates a severe risk of significant health problems and loss of foals in certain endemic studs. Its impact in a particular season and stud varies [1,2,3,4,5].
Commonly, rhodococcal infections are classified as pyogranulomatous pneumonia; however, the latest clinical papers identify many different forms of the disease, affecting tissues and organs other than the respiratory system. Increasing numbers of so-called “extrapulmonary changes” are being reported [4,6,7,8,9]. Additionally, many problems arise from the management of the disease. Lack of satisfying immunoprophylaxis, different approaches to diagnosis, no validated treatment alternatives, and problems with antimicrobial resistance creates a constant challenge for both researchers and field veterinarians [1,3,4,10,11,12,13,14].
This clinical report presents some less typical cases that have been presented for clinical and ultrasound evaluation during the studies on equine rhodococcosis provided in central and eastern Poland by the Division of Veterinary Epidemiology and Economics, Warsaw University of Life Sciences (SGGW), during 2019–2021 breeding seasons.
2. Clinical Cases: History and Examination Results
2.1. Clinical Approach
The monitoring program of rhodococcosis in foals including lung ultrasound was established in 5 horse studs in cooperation with SGGW. The participating studs are considered endemic based on the history of multiple Rhodococcus equi infections confirmed by post-mortem examinations and positive microbiological culture on blood agar, CAZ-NB and API Coryne tests from the samples collected in previous breeding seasons. A total of 192 foals were examined during the program. The screening aimed to improve and promote non-invasive and widely available field management of rhodococcosis in equine breeding centres. Considering the prior history of multiple foal loss due to Rhodococcus equi and scientific reports which claimed a higher probability of such infections in pneumonic foals of 2–3 months of age than any other pathogens [15,16,17,18,19], the diagnosis was based on the clinical picture and ultrasonographic evaluation of the lungs and pleural cavity (Draminski 4Vet Slim, linear transducer 8–10 MHz) [6,20,21]. Imaging diagnostics were performed roughly in two-week intervals, between the 3rd week and 4th month of life or later in case of clinical problems in older foals. The alluded approach emerged from a constant need to improve clinical diagnostics and treatment protocols which vary significantly in different seasons, counties, and studs [1,17,22,23].
2.1.1. Case 1—Premature Foal
A one-month-old Anglo-Arabian filly, born nearly a month prematurely was appointed for a clinical and ultrasound examination in early June 2019. At the delivery, apparent signs of immaturity were observed, such as small size, domed forehead, silky hair, tendon laxity, and general weakness. Because of the presence of the suckling reflex, the owner decided to introduce the treatment. She received colostrum within the first 12 h of her life from the local high-quality colostrum reserves (>30% of sugar, digital Colostrum Refractometer, KRUUSE, Langeskov, Denmark). Supportive treatment with dexamethasone (0.05 mg/kg IV) and butafosfan with B12 vitamin (0.05 mg/kg IV) was also administered. During her first weeks of life, she was bottle-fed with a milk replacer and received supportive therapies including physiotherapy and assistance with standing up and learning to nurse whenever it became possible. The foal was isolated from other horses for a prolonged time due to its weakness and significantly smaller size.
Her first examination took place at 5 weeks of age. This stud participated in a lung ultrasound screening program; however, the inclusion of the filly was primarily delayed due to her isolation and specific maintenance. Physical examination revealed pyrexia (rectal temperature of 39.6 °C) with a mildly elevated respiratory rate (56 breaths/min), tachycardia (108 beats/min), capillary refill time (CRT) of 2 s, pink and moist mucus membranes and mandibular lymph nodes within a normal range. She had no audible abnormalities on the thoracic auscultation. During the ultrasound examination, multiple B- lines were detected bilaterally. A multifocal abscess of significant size was detected on the left side at the 12th intercostal space (ICS). Furthermore, a 10 mm abscess occurred at the 14th ICS on the right side, and an irregular abscessation was visible cranially from the 9th ICS (Figure 1). Antimicrobial treatment with clarithromycin (7.5 mg/kg 2/daily PO) and rifampicin (5 mg/kg 2/daily PO) was implemented on the same day and continued for the following ten weeks, according to the changes in the filly’s weight [1].
During the treatment, she presented both recurrent fever and lesions of variable size and number. In her third month of life, the filly developed clinical signs of retrobulbar abscess. It progressed to partial blindness and left-sided microphthalmia over the next month, despite the additionally implemented treatment of topical tropicamide and gentamicin.
The filly was monitored until she was nearly 5 months old. Neither clinical findings nor major ultrasound abnormalities were present at that time. She had a small number of B-lines of variable width, present mostly in the cranial parts of the lungs and suggestive of post-inflammatory fibrous changes.
The case came back in July 2020, when she was 14 months old. This yearling was appointed for an ultrasound examination due to her quickly deteriorating condition and significant dyspnoea. Noticeable underweight and left-side microphthalmia were observed. On physical examination, a rectal temperature of 37.9 °C with a mildly elevated respiratory effort (28 breaths/min) and heart rate (HR; 76 beats/min), CRT of 2 s, pink and moist mucus membranes and mandibular lymph nodes within a normal range were noted. Apparent and loud wheezes were detected during thoracic auscultation. No other clinical abnormalities were reported. Ultrasound examination revealed a significant amount of free fluid in the pleural cavity bilaterally, with multiple hyperechoic shadows suggestive of fibrin clots. A few days later the yearling died. A shortened field necropsy was performed on the same day. A significant amount of fibrotic, turbid pleural fluid was confirmed in the thoracic cavity. Moreover, the size of the lungs was severely decreased and macroscopically presented major post-inflammatory and fibrotic changes. A small amount of turbid, fibrotic fluid was also present in the abdominal cavity, with chronic inflammatory changes in intestinal mucosa and mildly enlarged mesenteric lymph nodes. The owner decided not to pursue further post-mortem diagnostics. Bacteriological examination of the lung parenchyma revealed the presence of Rhodococcus equi and Streptococcus sp. β-haemolytic type.
2.1.2. Case 2—Problematic Bloodline
Two foals from the same Anglo-Arabian dam breeding line were undergoing a clinical and ultrasound examination as a part of a monitoring program aiming to recognize early signs of rhodococcosis in foals. Both mares, mother (Dam 1) and daughter (Dam 2) from this line had been successfully inseminated with two different, unrelated sires and were expecting foals in the 2020 breeding season. Both dams had a history of abortions or losses of foals in prior years; however, due to breeder change, it was not yet investigated.
2.1.3. Case 2.1
Dam 2 Gave Birth to a Healthy Colt at the End of January 2020
This foal underwent his first monitoring examination at the 3 weeks of age. He had no history of previous health issues. On physical examination, a rectal temperature of 38.7 °C with a respiratory rate within normal and tachycardia (100 beats/min), CRT < 2 s, pale pink and moist mucus membranes and mandibular lymph nodes within a normal range were noted. No auscultation abnormalities were detected. Ultrasound examination revealed a small number of B-lines, which might be considered acceptable for a foal at his age. The monitoring was performed in two weeks intervals, with no significant exacerbations detected until 8 weeks of age.
The foal was reported pyrectic at 10 weeks. On physical examination, a rectal temperature of 40.1 °C with a mildly elevated respiratory rate and HR of 76 beats/min, CRT of 2 s, pale pink and moist mucus membranes, and mandibular lymph nodes within normal were noted. No auscultation abnormalities were detected. A small number of B-lines and a few small consolidations in the right cranial lobe were recognized during the ultrasound examination. Since then, the colt was treated with tulathromycin (2.5 mg/kg 1/week IM) and rifampicin (5 mg/kg 2/daily PO) according to the changes in the foal’s weight [1,13]. He was euthanized a month later, at 14 weeks old, due to progressive deterioration.
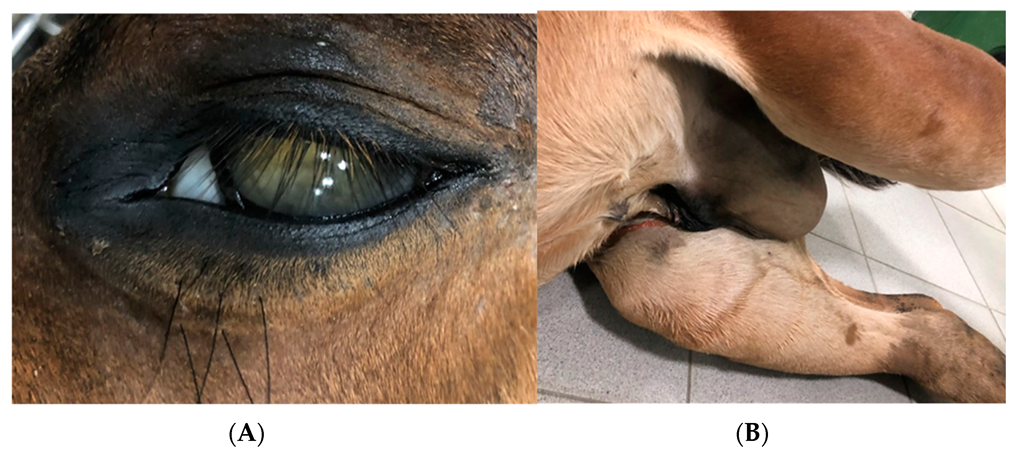
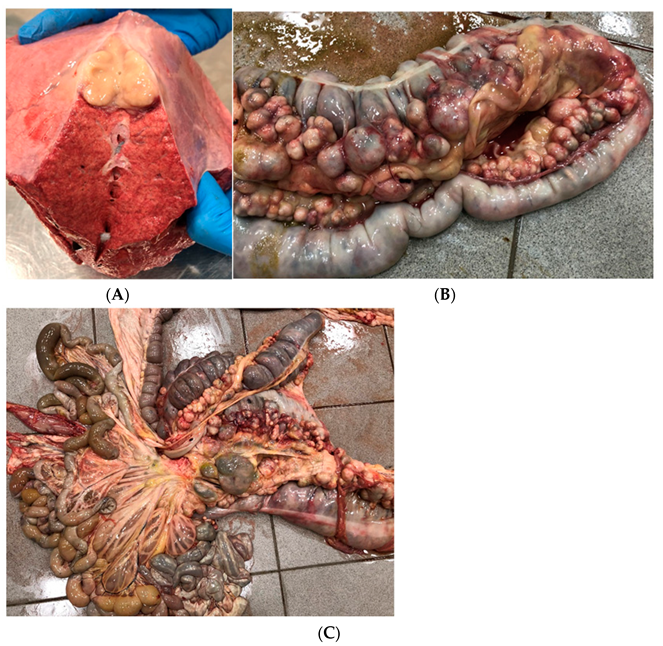
A necropsy was performed on the following day. The external evaluation showed significant underweight, bilateral uveitis (Figure 2a), and arthritis with a significant amount of synovial fluid, especially in the tarsal joints. Additionally, excessive overgrowth of the synovia was recognized. Internal evaluation of the thorax revealed fibrotic pleural fluid, inflammatory foci, and a few abscesses of 10–15 mm in diameter in the lung parenchyma (Figure 3a), particularly in the cranial and dorsal parts. Mediastinal lymph nodes were severely enlarged and purulent, which is rarely described [19]. Internal evaluation of the abdomen showed fibrotic, turbid fluid in the peritoneum, multiple abscesses along the large intestine with mesenteric lymph nodes abscessation (Figure 3b,c), and advanced inflammatory changes in the intestinal mucosa. Moreover, scrotal oedema (Figure 2b) with fibrotic, turbid fluid inside the tunica vaginalis, bilateral testicle atrophy, and inguinal hernia with omentum partially inside the scrotum were present. A bacteriological examination of the samples from the lung tissue and mesenteric lymph nodes confirmed the presence of Rhodococcus equi. The inflammatory changes in tarsal joints seemed to be immune-mediated aseptic polysynovitis since no microbiological culture from the synovial membrane samples was confirmed.
2.1.4. Case 2.2
Dam 1 Gave Birth to a Healthy Filly at the Beginning of June 2020
This foal also underwent her first screening at 3 weeks old. She had no history of prior health issues. On physical examination, a rectal temperature of 38.6 °C with a respiratory rate within a normal range and HR of 104 beats/min, CRT < 2 s, pink and moist mucus membranes and mandibular lymph nodes within a normal range were detected. She had no abnormalities audible on thoracic auscultation. Ultrasound examination revealed a small number of B-lines, which might be considered acceptable for a foal of this age. During the next ultrasound examination (5 weeks old) clinical parameters of the filly stayed within a normal range; however, a significant number of B-lines up to 5 mm was recognized with a few small consolidations in cranial lobes.
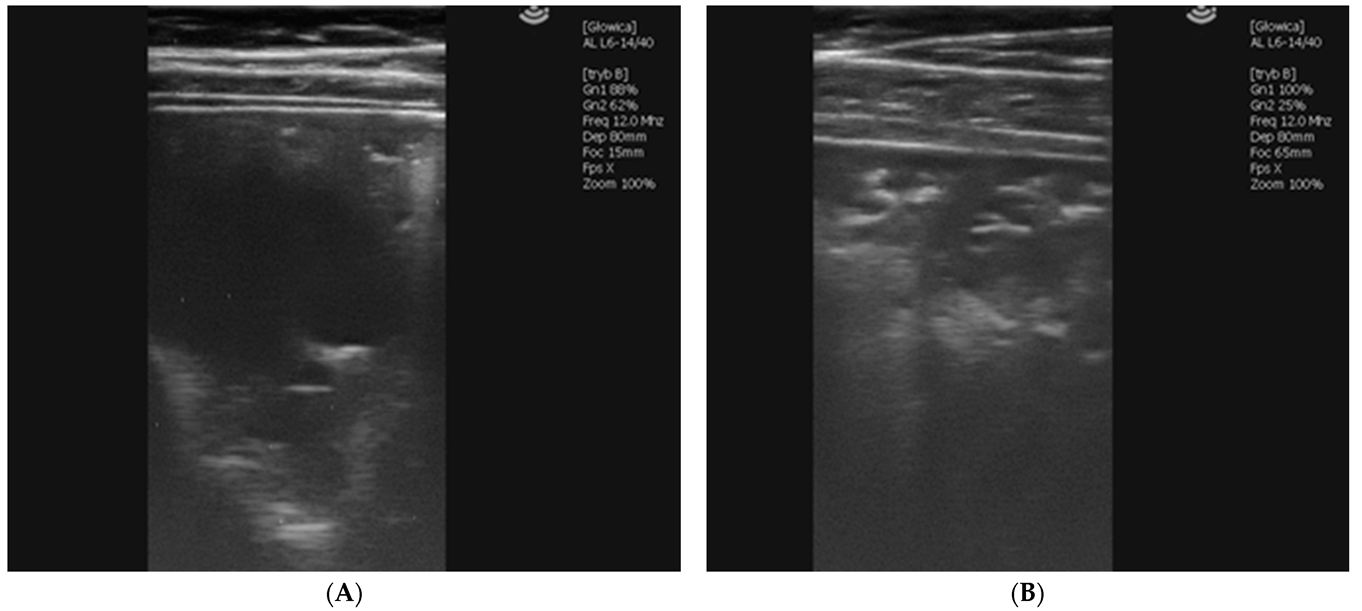
The filly was reported pyrectic with 39.9 °C being 7 weeks old. She also had a mildly elevated respiratory rate and tachycardia (96 beats/min), CRT of 2 s, pink mucus membranes, and mandibular lymph nodes within a normal range were detected. She had audible wheezes on thoracic auscultation. Ultrasound examination revealed two significant abscesses of 25 and 40 mm in diameter localized in 12 and 11 intercostal spaces, respectively on the left side (Figure 4a) and two abscesses on the right side, one of 43 mm in 11 ICS and another one, multifocal and irregular of significant size in 10–8 ICS (Figure 4b). The treatment was started on the same day (tulathromycin 2.5 mg/kg 1/week IM and rifampicin 5 mg/kg 2/daily PO) and conducted according to the changes in the filly’s weight [1,13]. The foal was examined for the last time at 12 weeks, with poor improvement and persistent recurrent fever, and died three days later.
A necropsy was performed on the following day. The foal was in moderate body condition. The examination revealed multiple variable sizes of abscesses and inflammatory changes in lung parenchyma and a moderate amount of turbid pleural fluid. No extrapulmonary changes were detected. Bacteriological examination of the lung parenchyma revealed the presence of Rhodococcus equi and Streptococcus sp. β-haemolytic type.
Due to significant health issues and deaths of the previous foals and suspicions of the breeder about congenital predispositions, it was decided to perform a laboratory test to determine the Immunoglobulin levels of the family. Accordingly, the mother’s (Dam 1), daughter’s (Dam 2), and grandson’s Ig levels were investigated in the laboratory at the beginning of May. The second examination took place in August and included Dam 1 and her filly. The results of the examinations are presented in Table 1.
The results indicated that none of the horses had IgM levels within a normal range, and all of the offspring showed significant IgM deficiency. Thus, it might be suspected that Dam 1 might pass some congenital immunological defect affecting the foals’ losses. No apparent clinical signs that might indicate infection were detected in both mares during the blood sampling. As a result, the breeder decided to withdraw both mares from reproduction without further investigation.
2.1.5. Case 3—Suspicion of Extrapulmonary Disorders
A 6-week-old Arabian filly was appointed for a clinical and ultrasound examination due to weakness, mild diarrhoea, reduced appetite, no weight gain, and apathy for a few days. She was not included in an ultrasound screening program. Her daily rectal temperature measurements had stayed within a normal range and there have been no other health complaints about her since birth.
During the first physical examination, a rectal temperature of 38.3 °C with a respiratory rate within a normal range and HR of 64 beats/min, CRT of 2 s, pink and moist mucus membranes and mandibular lymph nodes within normal were detected. She had mild auscultation wheezes present on the left side of the thorax. A small number of B- lines were detected bilaterally during the ultrasound examination, which may be considered normal for a foal at this age. However, on the left side at the 16th intercostal space, an abscess of 45 mm was detected. This location is considered less common for a single pulmonary consolidation since most of the lesions are usually detected in the cranial and medial parts of the lungs [20]. Moreover, her clinical appearance described above implied the possibility of extrapulmonary disorders connected with abdominal abscessation; however, no such changes were available to visualize during the ultrasound examination. Due to the significant size of the abscess and the poor general condition of the filly, antimicrobial treatment was recommended and implemented on the following day. She was treated with tulathromycin (2.5 mg/kg 1/week IM) according to the changes in the filly’s weight [13]. The antimicrobial treatment was conducted until she reached 11 weeks when no signs of abscessation were detected during the ultrasound examination.
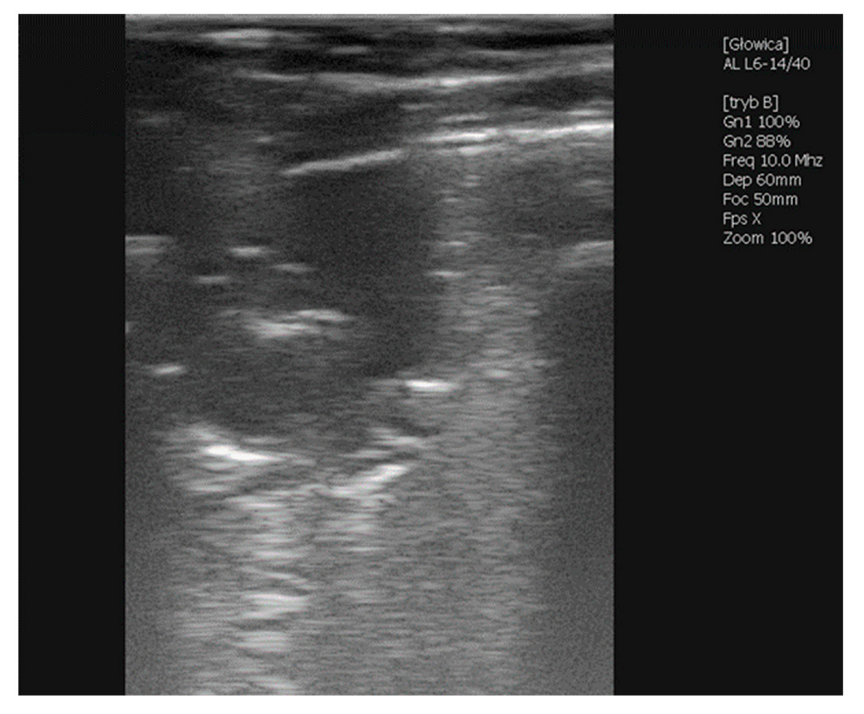
Clinical parameters stayed within a normal range during the treatment, and no fever incidents were detected. It took approximately two weeks for the foal to regain the expected condition and the abscess to reduce in size (26.4 mm). On the following examination, the abscess became irregular due to fibrotic tissue appearing in the lung parenchyma and the exact abscess’ size was not available to be measured. During the last examination, there were no remains of the abscess detected.
2.1.6. Case 4—Drug-Induced Hyperthermia
A 5-week-old Angloarabian filly, was appointed for a clinical and ultrasound examination due to pyrexia and dyspnoea. The haematologic results from the day of pyrexia onset presented in Table 2 indicate acute inflammation and dehydration. Her daily rectal temperature measurements stayed within a normal range until two days before the ultrasound examination, when it reached 39.2 °C. She was given benzylpenicillin (8 mg/kg, IM) with streptomycin (10 mg/kg, IM) and metamizole (22 mg/kg, IV) for three days which reduced the fever.
During the first examination two days later, she presented dyspnea. Her rectal temperature was 38.6 °C HR 64 beats/min, CRT 2 s, pink mucus membranes, mandibular lymph nodes within a normal range, and she had no other apparent health issues. She had no audible auscultation abnormalities on any side of the thorax. A moderate number of B- lines were detected bilaterally during the ultrasound examination, which might be considered acceptable for a foal at this age for a short period. An irregular abscess of significant diameter was detected on the left side at the 8–6th intercostal space. On the right side of the thorax, another irregular abscess occurred at the 11–8th intercostal space. Antimicrobial treatment was recommended and implemented on the same day. The filly was treated with clarithromycin (7.5 mg/kg 2/daily PO) and rifampicin (5 mg/kg 2/daily PO) according to the changes in the filly’s weight [1]. The antimicrobial treatment was conducted until the filly reached 14 weeks when no abnormalities were detected during an ultrasound examination.
The second examination of the filly happened to occur at the beginning of June (7 weeks of age). The outdoor temperatures were reaching 30 °C during the daytime and the foal presented rectal temperatures from 39.5 °C up to 41.0 °C for a few days, with little response to antipyretic drugs. However, an ultrasound examination revealed a significant reduction in the abscesses’ size (Figure 5). Since macrolides are known to have an anhidrosis potential in some horses, such a case was suspected. Therefore, the stable staff was asked to wet the filly with cold water regularly and to carefully monitor the rectal temperatures for a few days. Hyperthermia secondary to macrolide-induced anhidrosis seemed to be the proper diagnosis and owing to regularly wetting the filly and careful temperature checks, no other antipyretic drugs were needed. The procedure was implemented throughout the treatment, which took nearly two months in total. Wetting was conducted whenever the outdoor temperature was high and the stable staff reported increased rectal temperature (above 39 °C) during the morning examination.
3. Discussion
Rhodococcus equi is commonly associated with respiratory signs in foals from endemic studs. However, attaining reports about extrapulmonary findings and persisting impact of Rhodococcus on the health of endemic areas may indicate underlying issues. Extrapulmonary findings are often bound with more severe cases and worse prognoses [6,8,25,26,27]. This approach may be very accurate, but our ability to diagnose some of them, especially those connected with abdominal abscessations, is limited due to the most common locations of the changes, often superimposed by gaseous loops of the intestines. Moreover, clinical findings of abdominal abscessation are usually very unspecific and often restricted to diarrhoea and underweight. Those cases can also be difficult to differentiate from macrolide-induced problems. Many extrapulmonary incidents are confirmed and reported only based on post-mortem examination [25,27], or, in the case of skeletal abscesses during the radiological examination due to different reasons. Both types of changes may be significantly underdiagnosed. In the aforementioned Case 2.2, abdominal signs were suspected due to cachexia, persisting diarrhoea and slow response to antimicrobial treatment.
Ophthalmic changes are barely reported and generally worsen prognoses [6,26]. What is more, the papers describe cases of rhodococcal infections referred for hospital treatment, which are usually more severe [6]. In the alluded cases, ophthalmic changes terminated in the loss of foals. Filly described in Case 1 seemed to have the retrobulbar abscess at least partially cured. The eye bulb became microphthalmic, but the filly reacted properly to rapid movements and light changes on the affected side.
One of the most important problems while managing rhodococcosis is undoubtedly an extremely limited number of therapeutics effective in vivo [1,4,12,13,14,25,28]. Additionally, increasing antimicrobial resistance presents a serious threat to both human and veterinary medicine [29,30,31]. Unfortunately, in many countries, we lack such data, or, as in Poland, they are limited only to some regions [28,31]. In all of the aforementioned fatal cases, antimicrobial resistance against antibiotics selected for treatments was not detected.
Antimicrobial resistance does not end the list of disadvantages. Digestive issues and dysbiosis resulting from the use of certain drugs, especially macrolides, may create a serious risk for both mares and foals [32]. What is more, macrolide-induced anhidrosis may present even greater peril. These reactions in certain foals are connected with ion channels and β2-adrenergic receptors, but the proceedings and prognosis in such incidents are still not settled [33,34]. Up to date, in case of such antimicrobial adverse effects, the only solution implemented in cooperating studs relies on careful monitoring of the foals by appropriately qualified and responsible stable staff and their minute fulfilment of the recommendations.
Genetic susceptibility for rhodococcal infections in foals was not established and scientific reports on that matter are also extremely limited [2,35]. Some genes were suspected to possibly influence the development and course of clinical rhodococcosis but were not yet extended for more biological samples and results. Other papers claim no strict reliance on genetic factors in the development of clinical rhodococcosis [35]. It might be possible that some mares deliver foals that are of higher risk due to lower colostrum quality. Some foals may also be more prone to the disease due to increased exposure to pathogens caused by environmental factors or higher periodic faecal shedding among the group [3,4,36,37,38] but not for any strictly genetic problem. Thus some epigenetic and environmental factors may become crucial for further investigation.
Another suspicion arises around recurrent problems in certain bloodlines, frequently reported by field practitioners but not mentioned in scientific reports. In such cases, stud veterinarians often briefly investigate the matter in local laboratories; however, it usually ends with no clear answer. The key to resolving the problem may stay beyond genetic profile. For instance, some authors report a correlation between early Equine Herpes Virus type 1 or 2 (EHV1 and 2) infections and an increased risk of developing clinical rhodococcosis [39,40]. This hypothesis may be at least partially true for many reasons. The possibility of post-viral immunosuppression after early herpes infection being connected with increased susceptibility to clinical rhodococcosis is worth considering. Other species, including humans, significantly less affected by environmental Rhodococcus, suffer from the disease mostly when immunologically deficient [4,10,41,42,43,44,45]. What is more, susceptibility often occurs simultaneously with the highest exposure to a significant number of clinical and subclinical foals confirmed to have increased faecal shedding [36]. This hypothesis can also be supported considering that clinical signs usually develop during the immunological gap in foals. Nevertheless, these matters are still to be investigated.
The deficiency in immunoglobulins type M (IgM) of possibly inherited background suspected above partially binds earlier hypotheses. Reports about deficient IgM in horses are extremely rare. Primary selective IgM deficiency is usually mentioned in the manuals with a grave prognosis due to the foals being highly prone to multiple and recurrent bacterial and viral infections, especially pneumonia. The issue typically occurs in Arabians or AQH breeds [24,46]. The IgM deficiency was also described in a colt with a confirmed impaired B-cell response. IgMs are known to take part in initial antigen recognition and humoral activation, so this may partially explain the primary inability to fight infection in such foals and the following deterioration [47]. Secondary selective IgM deficiency is associated with lymphoma in adult horses; however, despite high sensitivity, it failed to be its only marker during diagnostic trials [48,49]. Although IgG seems to play a major role in clearing rhodococcal infections, IgM levels were also found elevated in the bronchoalveolar lavage (BAL) of foals affected with rhodococcosis [49]. These immunologic patterns remain yet undetermined; however, congenital immunological deficiencies could be considered in some recurrent problems of certain bloodlines.
The study presents certain limitations. The monitoring program was introduced as an additional tool to improve diagnostic procedures and treatment outcomes in endemic studs, thus the veterinarian performing lung ultrasound diagnosis was only an advisor to the stud veterinarians, who held full responsibility for the decisions regarding diagnosis and treatment. Moreover, the article gathers a few retrospective clinical cases, which unfortunately made most of the additional diagnostic procedures no longer available to perform.
4. Conclusions
Regardless of being an old and common dilemma, Rhodococcus equi and its clinical presentation remain a very challenging problem in endemic horse studs. What is particularly important is to preserve both scientific and clinical points of view to critically assess the ideas and implement proper solutions in managing the disease in field conditions, which remains an ultimate goal in solving clinical problems.
Author Contributions
A.R. and A.M.-K. performed diagnostic and veterinary procedures or sampling; A.R., A.B., M.Ż. and L.W. performed necropsies; A.R., A.B. and A.C. analysed and selected data; M.Ż. was responsible for photographic documentation and laboratory data curation; A.R. prepared and wrote the manuscript; A.B., A.C. and L.W. supervised the work. All authors have read and agreed to the published version of the manuscript.
Funding
This research was partially funded by grants from the Ministry of Science and Higher Education of Poland, decision no. 9506/E-385/R/2018 and Ministry of Education and Science of Poland, decision no. 16/491568/SPUB/SP/2021.
Institutional Review Board Statement
The study was carried out following the standards recommended by The Act of the Polish Parliament of 15 January 2015 on the Protection of Animals Used for Scientific or Educational Purposes (Journal of Laws 2015, item 266). According to Polish legal regulations (The Act of the Polish Parliament of 15 January 2015 on the Protection of Animals Used for Scientific or Educational Purposes, Journal of Laws 2015, item 266) no formal ethics consent was required for this study except for the informed consent for participation in the study, which was obtained from the owner of the studs.
Informed Consent Statement
Informed consent was obtained in advance from all of the representatives responsible for animals involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Giguère, S.; Cohen, N.D.; Keith Chaffin, M.; Slovis, N.M.; Hondalus, M.K.; Hines, S.A.; Prescott, J.F. Diagnosis, Treatment, Control, and Prevention of Infections Caused by Rhodococcus equi in Foals. J. Vet. Intern. Med. 2011, 25, 1209–1220. [Google Scholar] [CrossRef] [PubMed]
- Heller, M.C.; Jackson, K.A.; Watson, J.L. Identification of Immunologically Relevant Genes in Mare and Foal Dendritic Cells Responding to Infection by Rhodococcus equi. Vet. Immunol. Immunopathol. 2010, 136, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Dawson, T.R.M.Y.; Horohov, D.W.; Meijer, W.G.; Muscatello, G. Current Understanding of the Equine Immune Response to Rhodococcus equi. An Immunological Review of R. equi Pneumonia. Vet. Immunol. Immunopathol. 2010, 135, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Muscatello, G.; Leadon, D.P.; Klay, M.; Ocampo-Sosa, A.; Lewis, D.A.; Fogarty, U.; Buckley, T.; Gilkerson, J.R.; Meijer, W.G.; Vazquez-Boland, J.A. Rhodococcus equi Infection in Foals: The Science of “Rattles”. Equine Vet. J. 2007, 39, 470–478. [Google Scholar] [CrossRef]
- Witkowski, L.; Kaba, J.; Rzewuska, M.; Nowicki, M.; Szaluś-Jordanow, O.; Kita, J. Development of ELISA Test for Determination of the Level of Antibodies against Rhodococcus equi in Equine Serum and Colostrum. Vet. Immunol. Immunopathol. 2012, 149, 280–285. [Google Scholar] [CrossRef]
- Tarancón, I.; Leiva, M.; Jose-Cunilleras, E.; Ríos, J.; Peña, T. Ophthalmologic Findings Associated with Rhodococcus equi Bronchopneumonia in Foals. Vet. Ophthalmol. 2019, 22, 660–665. [Google Scholar] [CrossRef]
- Reuss, S.M.; Chaffin, M.K.; Schmitz, D.G.; Norman, T.E. Sonographic Characteristics of Intraabdominal Abscessation and Lymphadenopathy Attributable to Rhodococcus equi Infections in Foals. Vet. Radiol. Ultrasound 2011, 52, 462–465. [Google Scholar] [CrossRef]
- Reuss, S.M. Rhodococcus equi, Extrapulmonary Disorders and Lack of Response to Therapy. Equine Vet. Educ. 2021, 34, 399–400. [Google Scholar] [CrossRef]
- Morresey, P.R.; Garrett, K.S.; Carter, D. Rhodococcus equi Occipital Bone Osteomyelitis, Septic Arthritis and Meningitis in a Neurological Foal. Equine Vet. Educ. 2011, 23, 398–402. [Google Scholar] [CrossRef]
- Lin, W.V.; Kruse, R.L.; Yang, K.; Musher, D.M. Diagnosis and Management of Pulmonary Infection Due to Rhodococcus equi. Clin. Microbiol. Infect. 2019, 25, 310–315. [Google Scholar] [CrossRef]
- Giguére, S.; Jacks, S.; Roberts, G.D.; Hernandez, J.; Long, M.T.; Ellis, C. Retrospective Comparison of Azithromycin, Clarithromycin, and Erythromycin for the Treatment of Foals with Rhodococcus equi Pneumonia. J. Vet. Intern. Med. 2004, 18, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Wetzig, M.; Venner, M.; Giguère, S. Efficacy of the Combination of Doxycycline and Azithromycin for the Treatment of Foals with Mild to Moderate Bronchopneumonia. Equine Vet. J. 2019, 52, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Rutenberg, D.; Venner, M.; Giguère, S. Efficacy of Tulathromycin for the Treatment of Foals with Mild to Moderate Bronchopneumonia. J. Vet. Intern. Med. 2017, 31, 901–906. [Google Scholar] [CrossRef]
- Hildebrand, F.; Venner, M.; Giguère, S. Efficacy of Gamithromycin for the Treatment of Foals with Mild to Moderate Bronchopneumonia. J. Vet. Intern. Med. 2015, 29, 333–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leclere, M.; Magdesian, K.G.; Kass, P.H.; Pusterla, N.; Rhodes, D.M. Comparison of the Clinical, Microbiological, Radiological and Haematological Features of Foals with Pneumonia Caused by Rhodococcus equi and Other Bacteria. Vet. J. 2011, 187, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, M.V.; Mello, L.S.; Ribeiro, P.R.; Wentz, M.F.; Stolf, A.S.; Lopes, B.C.; de Andrade, C.P.; Snel, G.G.M.; Sonne, L.; Driemeier, D.; et al. Causes and Pathology of Equine Pneumonia and Pleuritis in Southern Brazil. J. Comp. Pathol. 2020, 179, 65–73. [Google Scholar] [CrossRef]
- McCracken, J.L.; Slovis, N.M. Use of Thoracic Ultrasound for the Prevention of Rhodococcus equi Pneumonia on Endemic Farms. Proc. Am. Assoc. Equine Pract. 2009, 55, 38–44. [Google Scholar]
- Huber, L.; Gressler, L.T.; Sanz, M.G.; Garbade, P.; Vargas, Á.; Silveira, B.P. Monitoring Foals by Thoracic Ultrasonography, Bacterial Culture, and PCR: Diagnostic of Rhodococcus equi Subclinical Pneumonia in South of Brazil. J. Equine Vet. Sci. 2018, 60, 104–108.e1. [Google Scholar] [CrossRef]
- Giguère, S.; Roberts, G.D. Association between Radiographic Pattern and Outcome in Foals with Pneumonia Caused by Rhodococcus equi. Vet. Radiol. Ultrasound 2012, 53, 601–604. [Google Scholar] [CrossRef]
- Venner, M.; Walther, S.M.; Münzer, B.; Stadler, P. Diagnostic of Pulmonary Abscesses in Foals-Comparison of Sonographic and Radiographic Examination. Pferdeheilkunde 2014, 30, 561–566. [Google Scholar] [CrossRef] [Green Version]
- Łobaczewski, A.; Czopowicz, M.; Moroz, A.; Mickiewicz, M.; Stabińska, M.; Petelicka, H.; Frymus, T.; Szaluś-Jordanow, O. Lung Ultrasound for Imaging of B-Lines in Dogs and Cats—A Prospective Study Investigating Agreement between Three Types of Transducers and the Accuracy in Diagnosing Cardiogenic Pulmonary Edema, Pneumonia and Lung Neoplasia. Animals 2021, 11, 3279. [Google Scholar] [CrossRef] [PubMed]
- Arnold-Lehna, D.; Venner, M.; Berghaus, L.J.; Berghaus, R.; Giguère, S. Changing Policy to Treat Foals with Rhodococcus equi Pneumonia in the Later Course of Disease Decreases Antimicrobial Usage without Increasing Mortality Rate. Equine Vet. J. 2020, 52, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Cauchard, S.; Giguère, S.; Venner, M.; Muscatello, G.; Cauchard, J.; Cohen, N.D.; Haas, A.; Hines, S.A.; Hondalus, M.K.; Horohov, D.W.; et al. Rhodococcus equi Research 2008-2012: Report of the Fifth International Havemeyer Workshop. Equine Vet. J. 2013, 45, 523–526. [Google Scholar] [CrossRef]
- Slovis, N.M.; McAuliffe, S.B. Color Atlas of Diseases and Disorders of the Foal; Elsevier: Amsterdam, The Netherlands, 2008; ISBN 9780702028106. [Google Scholar]
- Reuss, S.M.; Chaffin, M.K.; Cohen, N.D. Extrapulmonary Disorders Associated with Rhodococcus equi Infection in Foals: 150 Cases (1987–2007). J. Am. Vet. Med. Assoc. 2009, 235, 855–863. [Google Scholar] [CrossRef]
- Wilkes, E.J.A.; Hughes, K.J.; Kessell, A.E.; Raidal, S.L. Successful Management of Multiple Extrapulmonary Complications Associated with Rhodococcus equi Pneumonia in a Foal. Equine Vet. Educ. 2016, 28, 186–192. [Google Scholar] [CrossRef]
- le Corre, S.; Janes, J.; Slovis, N.M. Multiple Extra-Pulmonary Disorders Associated with Rhodococcus equi Infection in a 2-Month-Old Foal. Equine Vet. Educ. 2021, 33, 396. [Google Scholar] [CrossRef]
- Kalinowski, M.; Jarosz, Ł.; Grądzki, Z. Assessment of Antimicrobial Susceptibility of Virulent Strains of Rhodococcus equi Isolated From Foals and Soil of Horse Breeding Farms With and Without Endemic Infections. J. Equine Vet. Sci. 2020, 91, 103114. [Google Scholar] [CrossRef] [PubMed]
- Huber, L.; Giguère, S.; Slovis, N.M.; Carter, C.N.; Barr, B.S.; Cohen, N.D.; Elam, J.; Erol, E.; Locke, S.J.; Phillips, E.D.; et al. Emergence of Resistance to Macrolides and Rifampin in Clinical Isolates of Rhodococcus equi from Foals in Central Kentucky, 1995 to 2017. Antimicrob. Agents Chemother. 2018, 63. [Google Scholar] [CrossRef] [Green Version]
- Huber, L.; Giguère, S.; Cohen, N.D.; Slovis, N.M.; Hanafi, A.; Schuckert, A.; Berghaus, L.; Greiter, M.; Hart, K.A. Prevalence and Risk Factors Associated with Emergence of Rhodococcus equi Resistance to Macrolides and Rifampicin in Horse-Breeding Farms in Kentucky, USA. Vet. Microbiol. 2019, 235, 243–247. [Google Scholar] [CrossRef]
- Burton, A.J.; Giguère, S.; Sturgill, T.L.; Berghaus, L.J.; Slovis, N.M.; Whitman, J.L.; Levering, C.; Kuskie, K.R.; Cohen, N.D. Macrolide- and Rifampin-Resistant Rhodococcus equi on a Horse Breeding Farm, Kentucky, USA. Emerg. Infect. Dis. 2013, 19, 282–285. [Google Scholar] [CrossRef]
- Noah Cohen, B.D. Rhodococcus equi Pneumonia in Foals: An Update on Epidemiology, Diagnosis, Treatment, and Prevention. AAEP 2021. Available online: https://aaep.org/horsehealth/rhodococcus-equi-pneumonia-foals-update-epidemiology-diagnosis-treatment-and-prevention (accessed on 10 September 2022).
- Stieler, A.L.; Sanchez, L.C.; Mallicote, M.F.; Martabano, B.B.; Burrow, J.A.; MacKay, R.J. Macrolide-Induced Hyperthermia in Foals: Role of Impaired Sweat Responses. Equine Vet. J. 2016, 48, 590–594. [Google Scholar] [CrossRef] [PubMed]
- Patterson Rosa, L.; Mallicote, M.F.; MacKay, R.J.; Brooks, S.A. Ion Channel and Ubiquitin Differential Expression during Erythromycin-Induced Anhidrosis in Foals. Animals 2021, 11, 3379. [Google Scholar] [CrossRef] [PubMed]
- Mcqueen, C.M.; Dindot, S.V.; Foster, M.J.; Cohen, N.D. Genetic Susceptibility to Rhodococcus equi. J. Vet. Intern. Med. 2015, 29, 1648–1659. [Google Scholar] [CrossRef] [PubMed]
- Huber, L.; Giguère, S.; Berghaus, L.J.; Hanafi, A.; Ryan, C. Fecal Shedding of Rhodococcus equi in Mares and Foals after Experimental Infection of Foals and Effect of Composting on Concentrations of R. equi in Contaminated Bedding. Vet. Microbiol. 2018, 223, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Cohen, N.D.; Chaffin, M.K.; Kuskie, K.R.; Syndergaard, M.K.; Blodgett, G.P.; Takai, S. Association of Perinatal Exposure to Airborne Rhodococcus equi with Risk of Pneumonia Caused by R Equi in Foals. Am. J. Vet. Res. 2013, 74, 102–109. [Google Scholar] [CrossRef]
- Madrigal, R.G.; Shaw, S.D.; Witkowski, L.A.; Sisson, B.E.; Blodgett, G.P.; Chaffin, M.K.; Cohen, N.D. Use of Serial Quantitative PCR of the VapA Gene of Rhodococcus equi in Feces for Early Detection of R. equi Pneumonia in Foals. J. Vet. Intern. Med. 2016, 30, 664–670. [Google Scholar] [CrossRef]
- Nordengrahn, A.; Rusvai, M.; Merza, M.; Ekstrijm, J.; Morein, B.; Bela, S. Equine Herpesvirus Type 2 (EHV-2) as a Predisposing Factor for Rhodococcus equi Pneumonia in Foals: Prevention of the Bifactorial Disease with EHV-2 Immunostimulating Complexes. Vet. Microbiol. 1996, 51, 55–68. [Google Scholar] [CrossRef]
- Perez-Ecija, A.; Mendoza, F.J.; Estepa, J.C.; Bautista, M.J.; Pérez, J. Equid Herpesvirus 1 and Rhodococcus equi Coinfection in a Foal with Bronchointerstitial Pneumonia. J. Vet. Med. Sci. 2016, 78, 1511–1513. [Google Scholar] [CrossRef] [Green Version]
- Stewart, A.; Sowden, D.; Caffery, M.; Bint, M.; Broom, J. Rhodococcus equi Infection: A Diverse Spectrum of Disease. IDCases 2019, 15, e00487. [Google Scholar] [CrossRef]
- Zychska, M.; Witkowski, L.; Klementowska, A.; Rzewuska, M.; Kwiecien, E.; Stefanska, I.; Czopowicz, M.; Szalus-Jordanow, O.; Mickiewicz, M.; Moroz, A.; et al. Rhodococcus equi—Occurrence in Goats and Clinical Case Report. Pathogens 2021, 10, 1141. [Google Scholar] [CrossRef]
- Bordin, A.I.; Gressler, L.T.; Alexander, E.R.C.; Sule, P.; Cirillo, J.D.; Edwards, J.F.; Cohen, N.D. Guinea Pig Infection with the Intracellular Pathogen Rhodococcus equi. Vet. Microbiol. 2018, 215, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Kubota, H.; Madarame, H.; Takase, F.; Takahashi, K.; Sasaki, Y.; Kakuda, T.; Takai, S. Pathogenicity and Genomic Features of VapN-Harboring Rhodococcus equi Isolated from Human Patients. Int. J. Med. Microbiol. 2021, 311, 151519. [Google Scholar] [CrossRef] [PubMed]
- Salmuna, Z.N.; Azim, W.A.W.A.; Harun, A. Rhodococcus equi Pulmonary Infection in an Immunocompromised Patient: Case Report and Literature Review. Clin. Microbiol. Newsl. 2018, 40, 128–130. [Google Scholar] [CrossRef]
- Boy, M.G.; Zhang, C.; Antczak, D.F.; Hamir, A.N.; Whitlock, R.H.; Baker, J.A. Unusual Selective Immunoglobulin Deficiency in an Arabian-Foal. J. Vet. Intern. Med. 1992, 6, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Weldon, A.D.; Zhang, C.; Antczak, D.F.; Rebhun, W.C. Selective IgM Deficiency and Abnormal B-Cell Response in a Foal. J. Am. Vet. Med. Assoc. 1992, 201, 1396–1398. [Google Scholar] [PubMed]
- Taintor, J.; Schleis, S. Equine Lymphoma. Equine Vet. Educ. 2011, 23, 205–213. [Google Scholar] [CrossRef]
- Perkins, G.A.; Nydam, D.V.; Flaminio, M.J.B.F.; Ainsworth, D.M. Serum IgM Concentrations in Normal, Fit Horses and Horses with Lymphoma or Other Medical Conditions. J. Vet. Intern. Med. 2003, 17, 337–342. [Google Scholar] [CrossRef]
Figure 1.
Ultrasonographic picture of an irregular abscessation observed in the right lobe from 9th ICS cranially during the first examination of Case 1. Visible parts of the abscess are 35.6 mm in width and 21.7 mm in depth.
Figure 1.
Ultrasonographic picture of an irregular abscessation observed in the right lobe from 9th ICS cranially during the first examination of Case 1. Visible parts of the abscess are 35.6 mm in width and 21.7 mm in depth.

Figure 2.
Anatomopathological findings concerning Case 2.1. Uveitis (A), scrotal edema and hernia (B).
Figure 2.
Anatomopathological findings concerning Case 2.1. Uveitis (A), scrotal edema and hernia (B).

Figure 3.
Anatomopathological findings concerning Case 2.1. Dissection of a pulmonary abscess (A), large intestine and mesenteric abscessation (B,C).
Figure 3.
Anatomopathological findings concerning Case 2.1. Dissection of a pulmonary abscess (A), large intestine and mesenteric abscessation (B,C).

Figure 4.
Ultrasonographic picture of an irregular abscessation with hypoechoic fluid in the left lobe in 11th ICS (A) and a multifocal abscessation in the right lobe from 11th ICS cranially in the right lobe (B) observed during the first examination of Case 2.2.
Figure 4.
Ultrasonographic picture of an irregular abscessation with hypoechoic fluid in the left lobe in 11th ICS (A) and a multifocal abscessation in the right lobe from 11th ICS cranially in the right lobe (B) observed during the first examination of Case 2.2.

Figure 5.
Ultrasonographic picture of a circular abscessation observed in the left lung, 16th ICS during the second examination of Case 3. Visible parts of the abscess are 26.4 mm in depth and 23.3 mm in width.
Figure 5.
Ultrasonographic picture of a circular abscessation observed in the left lung, 16th ICS during the second examination of Case 3. Visible parts of the abscess are 26.4 mm in depth and 23.3 mm in width.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Results of immunoglobulin levels investigation. The Ig reference values for foals above 60 days of life are the same as for adult horses.
Table 1.
Results of immunoglobulin levels investigation. The Ig reference values for foals above 60 days of life are the same as for adult horses.
| Horse | Results from the Beginning of May 2020 | Results from the End of August 2020 | |||
|---|---|---|---|---|---|
| IgG (Ref. Value 500–2000) | IgM (Ref. Value 90–150) | IgG (Ref. Value 500–2000) | IgM (Ref. Value 90–150) | IgA (Ref. Value 60–130) | |
| Dam 1 | 1480 mg/dL | 340.1 mg/dL | 2190 mg/dL | 272.3 mg/dL | 55.4 mg/dL |
| Filly from Dam 1 | 630 mg/dL | 4.5 mg/dL | 101.9 mg/dL | ||
| Dam 2 * | 1310 mg/dL | 34.8 mg/dL | |||
| Colt from Dam 2 | 1390 mg/dL | 14.2 mg/dL | |||
* Daughter of Dam 1.
Table 2.
Haematological results of Case 4 from the day of pyrexia onset with reference values [24].
Table 2.
Haematological results of Case 4 from the day of pyrexia onset with reference values [24].
| RBC | MCV | HCT | PLT | MPV | WBC | HGB | MCH | MCHC | LYMF | GRAN | MID | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref. value | 6.5–9.99 | 38–53 | 33–48 | 115–450 | - | 5.0–12.6 | 11–16 | 12–16 | 31–37 | 1.4–2.3 | 2.75–8.19 | - |
| Case 4 | 9.96 | 32 | 31.9 | 360 | 7.3 | 29.7 | 20.7 | 20.8 | 64.8 | 4.6 | 23.5 | 1.5 |
RBC—red blood cell count; MCV—mean cell volume; HCT—haematocrit; PLT—platelet count; MPV—mean platelet volume; WBC—white blood cell count; HGB—haemoglobin; MCH—mean cell haemoglobin; MCHC—mean corpuscular haemoglobin concentration; LYMF—lymphocytes; GRAN—granulocytes; MID—mid-range absolute cell count.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Rakowska, A.; Marciniak-Karcz, A.; Bereznowski, A.; Cywińska, A.; Żychska, M.; Witkowski, L. Less Typical Courses of Rhodococcus equi Infections in Foals. Vet. Sci. 2022, 9, 605. https://doi.org/10.3390/vetsci9110605
AMA Style
Rakowska A, Marciniak-Karcz A, Bereznowski A, Cywińska A, Żychska M, Witkowski L. Less Typical Courses of Rhodococcus equi Infections in Foals. Veterinary Sciences. 2022; 9(11):605. https://doi.org/10.3390/vetsci9110605
Chicago/Turabian StyleRakowska, Alicja, Agnieszka Marciniak-Karcz, Andrzej Bereznowski, Anna Cywińska, Monika Żychska, and Lucjan Witkowski. 2022. "Less Typical Courses of Rhodococcus equi Infections in Foals" Veterinary Sciences 9, no. 11: 605. https://doi.org/10.3390/vetsci9110605
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.