
Comparison of Three Cellular Assays to Predict the Course of CMV Infection in Liver Transplant Recipients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. ELISpot and QuantiFERON Assays
2.3. CMV Status and Viral Load
2.4. Statistics
3. Results
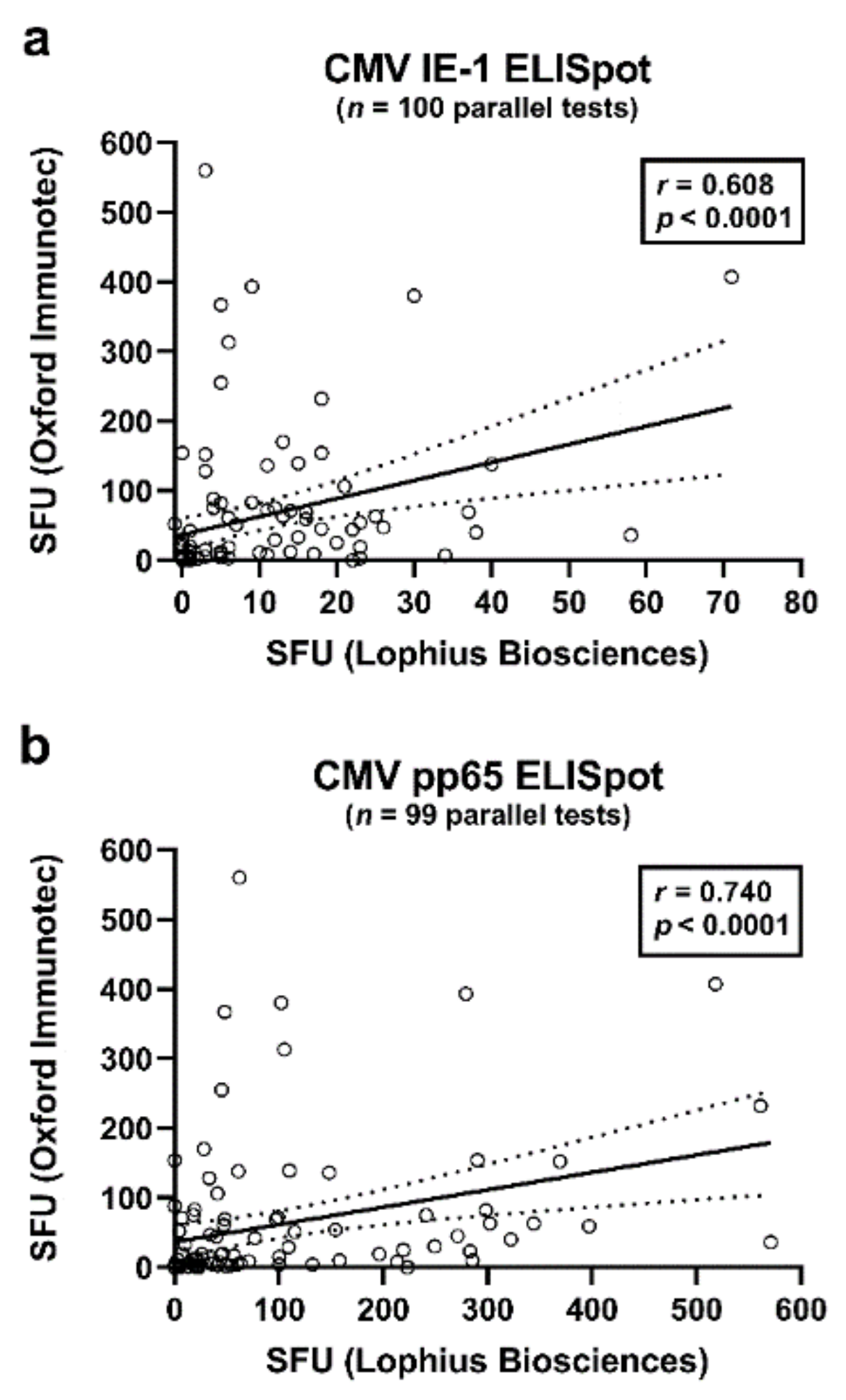
3.1. Correlation of Three CMV-Specific Interferon-Gamma-Release Assays
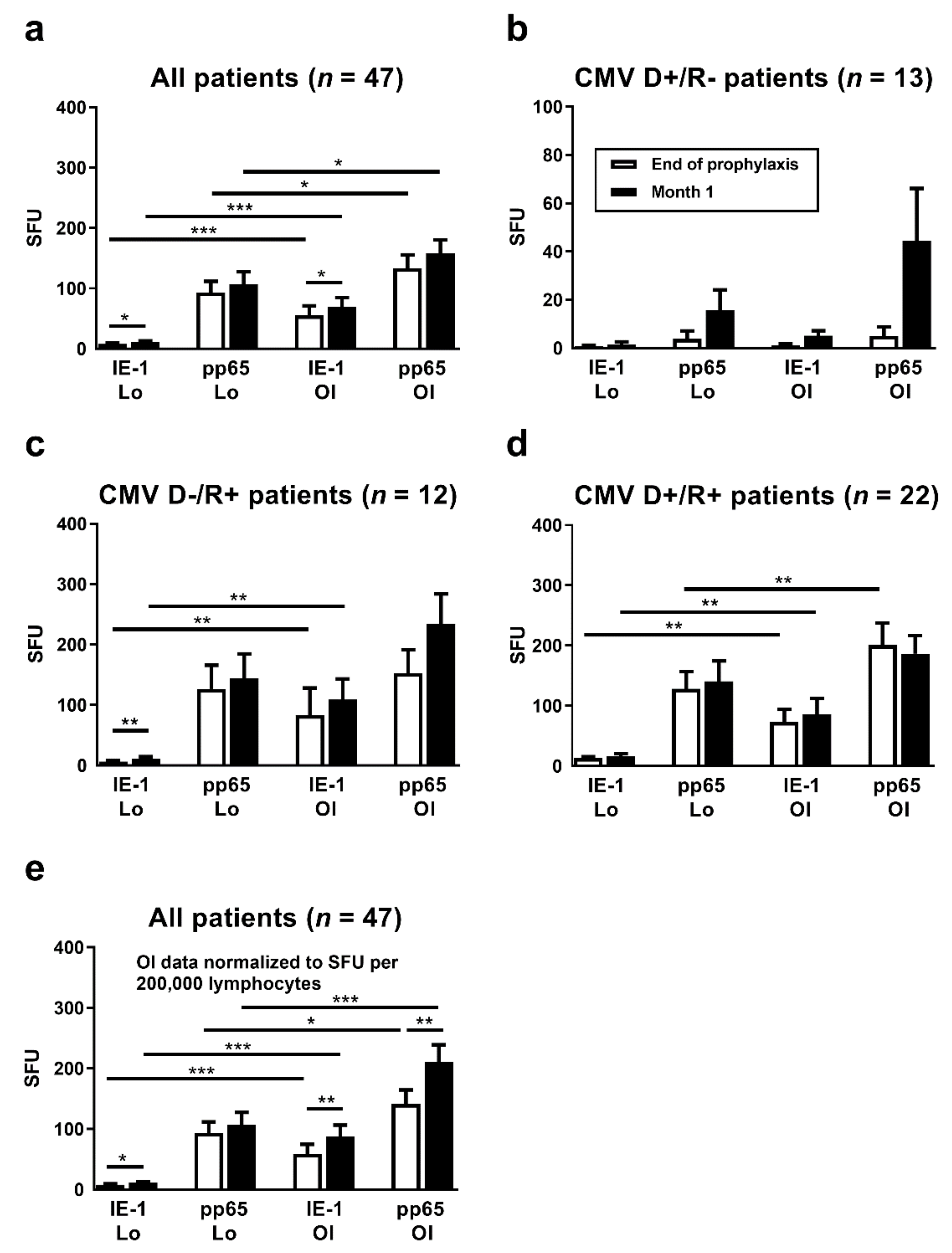
3.2. Comparison of Cellular Responses at the End of Antiviral Prophylaxis with Results One Month Thereafter
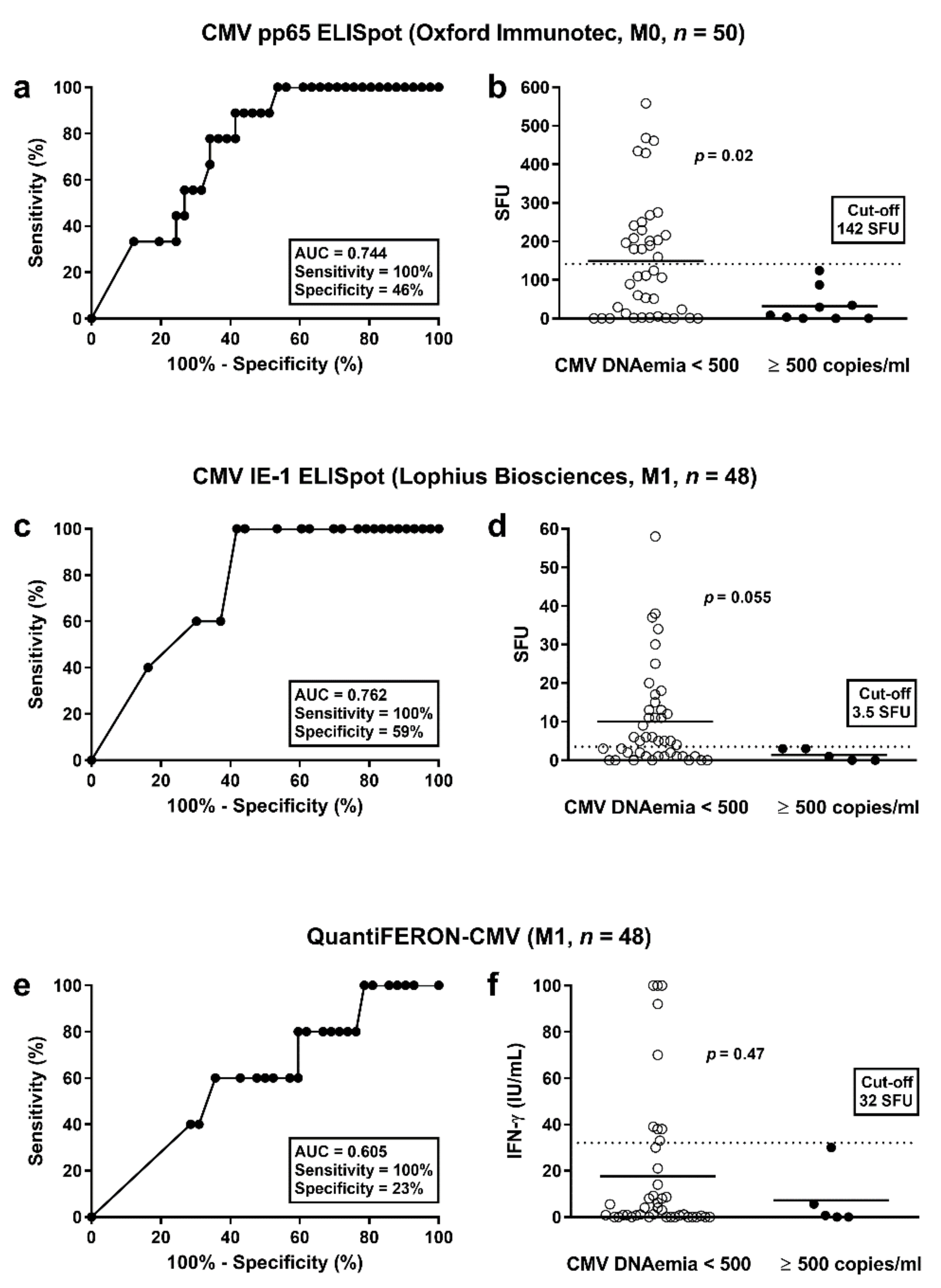
3.3. Determination of Cut-off Values for Protective T Cell Responses
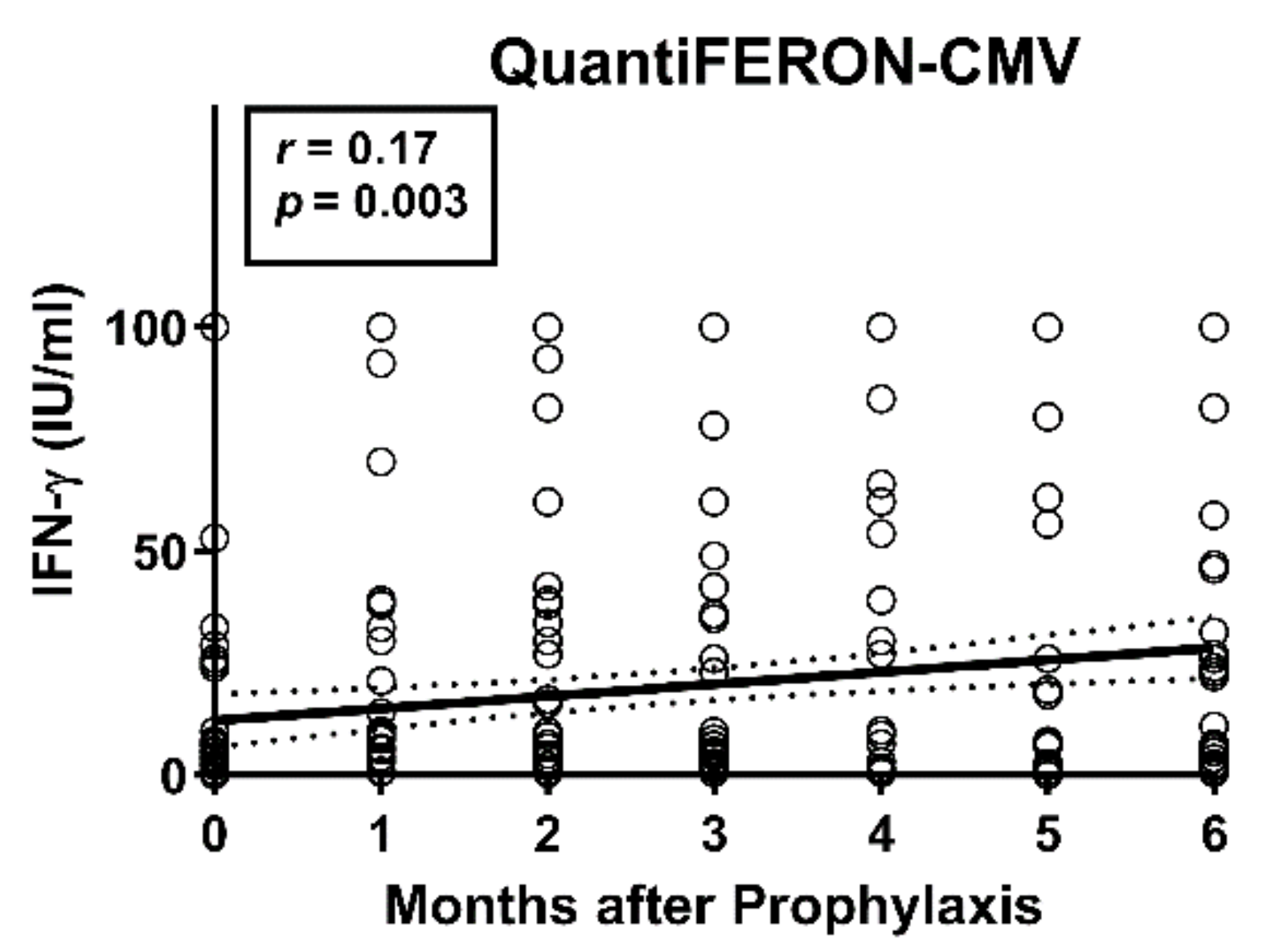
3.4. Correlation of CMV-Specific Cellular Immunity with Additonal Clinical Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cannon, M.J.; Schmid, D.S.; Hyde, T.B. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev. Med. Virol. 2010, 20, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Marcelin, J.R.; Beam, E.; Razonable, R.R. Cytomegalovirus infection in liver transplant recipients: Updates on clinical management. World J. Gastroenterol. 2014, 20, 10658–10667. [Google Scholar] [CrossRef] [PubMed]
- Varani, S.; Landini, M.P. Cytomegalovirus-induced immunopathology and its clinical consequences. Herpesviridae 2011, 2, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azevedo, L.S.; Pierrotti, L.C.; Abdala, E.; Costa, S.F.; Strabelli, T.M.; Campos, S.V.; Ramos, J.F.; Latif, A.Z.; Litvinov, N.; Maluf, N.Z.; et al. Cytomegalovirus infection in transplant recipients. Clinics 2015, 70, 515–523. [Google Scholar] [CrossRef]
- Martin-Gandul, C.; Mueller, N.J.; Pascual, M.; Manuel, O. The Impact of Infection on Chronic Allograft Dysfunction and Allograft Survival After Solid Organ Transplantation. Am. J. Transplant. 2015, 15, 3024–3040. [Google Scholar] [CrossRef] [Green Version]
- Halme, L.; Hockerstedt, K.; Lautenschlager, I. Cytomegalovirus infection and development of biliary complications after liver transplantation. Transplantation 2003, 75, 1853–1858. [Google Scholar] [CrossRef]
- Kotton, C.N.; Kumar, D.; Caliendo, A.M.; Huprikar, S.; Chou, S.; Danziger-Isakov, L.; Humar, A.; The Transplantation Society International, C.M.V.C.G. The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-organ Transplantation. Transplantation 2018, 102, 900–931. [Google Scholar] [CrossRef] [Green Version]
- Fishman, J.A.; Emery, V.; Freeman, R.; Pascual, M.; Rostaing, L.; Schlitt, H.J.; Sgarabotto, D.; Torre-Cisneros, J.; Uknis, M.E. Cytomegalovirus in transplantation—Challenging the status quo. Clin. Transplant. 2007, 21, 149–158. [Google Scholar] [CrossRef]
- Bruminhent, J.; Razonable, R.R. Management of cytomegalovirus infection and disease in liver transplant recipients. World J. Hepatol. 2014, 6, 370–383. [Google Scholar] [CrossRef]
- Egli, A.; Humar, A.; Kumar, D. State-of-the-art monitoring of cytomegalovirus-specific cell-mediated immunity after organ transplant: A primer for the clinician. Clin. Infect. Dis. 2012, 55, 1678–1689. [Google Scholar] [CrossRef] [Green Version]
- Ruan, Y.; Guo, W.; Liang, S.; Xu, Z.; Niu, T. Diagnostic performance of cytomegalovirus (CMV) immune monitoring with ELISPOT and QuantiFERON-CMV assay in kidney transplantation: A PRISMA-compliant article. Medicine 2019, 98, e15228. [Google Scholar] [CrossRef] [PubMed]
- Banas, B.; Steubl, D.; Renders, L.; Chittka, D.; Banas, M.C.; Wekerle, T.; Koch, M.; Witzke, O.; Muhlfeld, A.; Sommerer, C.; et al. Clinical validation of a novel enzyme-linked immunosorbent spot assay-based in vitro diagnostic assay to monitor cytomegalovirus-specific cell-mediated immunity in kidney transplant recipients: A multicenter, longitudinal, prospective, observational study. Transpl. Int. 2018, 31, 436–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gliga, S.; Korth, J.; Krawczyk, A.; Wilde, B.; Horn, P.A.; Witzke, O.; Lindemann, M.; Fiedler, M. T-Track-CMV and QuantiFERON-CMV assays for prediction of protection from CMV reactivation in kidney transplant recipients. J. Clin. Virol. 2018, 105, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Sester, U.; Gartner, B.C.; Wilkens, H.; Schwaab, B.; Wossner, R.; Kindermann, I.; Girndt, M.; Meyerhans, A.; Mueller-Lantzsch, N.; Schafers, H.J.; et al. Differences in CMV-specific T-cell levels and long-term susceptibility to CMV infection after kidney, heart and lung transplantation. Am. J. Transplant. 2005, 5, 1483–1489. [Google Scholar] [CrossRef]
- Chanouzas, D.; Small, A.; Borrows, R.; Ball, S. Assessment of the T-SPOT.CMV interferon-gamma release assay in renal transplant recipients: A single center cohort study. PLoS ONE 2018, 13, e0193968. [Google Scholar] [CrossRef] [Green Version]
- Barabas, S.; Spindler, T.; Kiener, R.; Tonar, C.; Lugner, T.; Batzilla, J.; Bendfeldt, H.; Rascle, A.; Asbach, B.; Wagner, R.; et al. An optimized IFN-gamma ELISpot assay for the sensitive and standardized monitoring of CMV protein-reactive effector cells of cell-mediated immunity. BMC Immunol. 2017, 18, 14. [Google Scholar] [CrossRef] [Green Version]
- Shin, K.H.; Lee, H.J.; Chang, C.L.; Kim, E.J.; Lim, S.; Lee, S.J.; Ryu, J.H.; Yang, K.; Choi, B.H.; Lee, T.B.; et al. CMV specific T cell immunity predicts early viremia after liver transplantation. Transpl. Immunol. 2018, 51, 62–65. [Google Scholar] [CrossRef]
- Rogers, R.; Saharia, K.; Chandorkar, A.; Weiss, Z.F.; Vieira, K.; Koo, S.; Farmakiotis, D. Clinical experience with a novel assay measuring cytomegalovirus (CMV)-specific CD4+ and CD8+ T-cell immunity by flow cytometry and intracellular cytokine staining to predict clinically significant CMV events. BMC Infect. Dis. 2020, 20, 58. [Google Scholar] [CrossRef]
- Thompson, G.; Boan, P.; Baumwol, J.; Chakera, A.; MacQuillan, G.; Swaminathan, S.; Lavender, M.; Flexman, J.; James, I.; John, M. Analysis of the QuantiFERON-CMV assay, CMV viraemia and antiviral treatment following solid organ transplantation in Western Australia. Pathology 2018, 50, 554–561. [Google Scholar] [CrossRef]
- Kumar, D.; Mian, M.; Singer, L.; Humar, A. An Interventional Study Using Cell-Mediated Immunity to Personalize Therapy for Cytomegalovirus Infection after Transplantation. Am. J. Transplant. 2017, 17, 2468–2473. [Google Scholar] [CrossRef]
- Manuel, O.; Husain, S.; Kumar, D.; Zayas, C.; Mawhorter, S.; Levi, M.E.; Kalpoe, J.; Lisboa, L.; Ely, L.; Kaul, D.R.; et al. Assessment of cytomegalovirus-specific cell-mediated immunity for the prediction of cytomegalovirus disease in high-risk solid-organ transplant recipients: A multicenter cohort study. Clin. Infect. Dis. 2013, 56, 817–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, D.; Chin-Hong, P.; Kayler, L.; Wojciechowski, D.; Limaye, A.P.; Osama Gaber, A.; Ball, S.; Mehta, A.K.; Cooper, M.; Blanchard, T.; et al. A prospective multicenter observational study of cell-mediated immunity as a predictor for cytomegalovirus infection in kidney transplant recipients. Am. J. Transplant. 2019, 19, 2505–2516. [Google Scholar] [CrossRef] [PubMed]
- Lisboa, L.F.; Kumar, D.; Wilson, L.E.; Humar, A. Clinical utility of cytomegalovirus cell-mediated immunity in transplant recipients with cytomegalovirus viremia. Transplantation 2012, 93, 195–200. [Google Scholar] [CrossRef]
- Chiereghin, A.; Potena, L.; Borgese, L.; Gibertoni, D.; Squarzoni, D.; Turello, G.; Petrisli, E.; Piccirilli, G.; Gabrielli, L.; Grigioni, F.; et al. Monitoring of Cytomegalovirus (CMV)-Specific Cell-Mediated Immunity in Heart Transplant Recipients: Clinical Utility of the QuantiFERON-CMV Assay for Management of Posttransplant CMV Infection. J. Clin. Microbiol. 2018, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czerkinsky, C.; Andersson, G.; Ekre, H.P.; Nilsson, L.A.; Klareskog, L.; Ouchterlony, O. Reverse ELISPOT assay for clonal analysis of cytokine production. I. Enumeration of gamma-interferon-secreting cells. J. Immunol. Methods 1988, 110, 29–36. [Google Scholar] [CrossRef]
- Barabas, S.; Gary, R.; Bauer, T.; Lindner, J.; Lindner, P.; Weinberger, B.; Jilg, W.; Wolf, H.; Deml, L. Urea-mediated cross-presentation of soluble Epstein-Barr virus BZLF1 protein. PLoS Pathog. 2008, 4, e1000198. [Google Scholar] [CrossRef]
- Giulieri, S.; Manuel, O. QuantiFERON(R)-CMV assay for the assessment of cytomegalovirus cell-mediated immunity. Expert Rev. Mol. Diagn. 2011, 11, 17–25. [Google Scholar] [CrossRef]
- Redeker, A.; Remmerswaal, E.B.M.; van der Gracht, E.T.I.; Welten, S.P.M.; Hollt, T.; Koning, F.; Cicin-Sain, L.; Nikolich-Zugich, J.; Ten Berge, I.J.M.; van Lier, R.A.W.; et al. The Contribution of Cytomegalovirus Infection to Immune Senescence Is Set by the Infectious Dose. Front. Immunol. 2017, 8, 1953. [Google Scholar] [CrossRef]
- Fletcher, J.M.; Vukmanovic-Stejic, M.; Dunne, P.J.; Birch, K.E.; Cook, J.E.; Jackson, S.E.; Salmon, M.; Rustin, M.H.; Akbar, A.N. Cytomegalovirus-specific CD4+ T cells in healthy carriers are continuously driven to replicative exhaustion. J. Immunol. 2005, 175, 8218–8225. [Google Scholar] [CrossRef] [Green Version]
- Pourgheysari, B.; Khan, N.; Best, D.; Bruton, R.; Nayak, L.; Moss, P.A. The cytomegalovirus-specific CD4+ T-cell response expands with age and markedly alters the CD4+ T-cell repertoire. J. Virol. 2007, 81, 7759–7765. [Google Scholar] [CrossRef] [Green Version]
- Khan, N.; Shariff, N.; Cobbold, M.; Bruton, R.; Ainsworth, J.A.; Sinclair, A.J.; Nayak, L.; Moss, P.A. Cytomegalovirus seropositivity drives the CD8 T cell repertoire toward greater clonality in healthy elderly individuals. J. Immunol. 2002, 169, 1984–1992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindemann, M.; Korth, J.; Sun, M.; Xu, S.; Struve, C.; Werner, K.; Dornieden, T.; Horn, P.A.; Witzke, O.; Wilde, B. The Cytomegalovirus-Specific IL-21 ELISpot Correlates with Allograft Function of Kidney Transplant Recipients. Int. J. Mol. Sci. 2018, 19, 3945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, S.E.; Sedikides, G.X.; Mason, G.M.; Okecha, G.; Wills, M.R. Human Cytomegalovirus (HCMV)-Specific CD4(+) T Cells Are Polyfunctional and Can Respond to HCMV-Infected Dendritic Cells In Vitro. J. Virol. 2017, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swain, S.L.; McKinstry, K.K.; Strutt, T.M. Expanding roles for CD4(+) T cells in immunity to viruses. Nat. Rev. Immunol. 2012, 12, 136–148. [Google Scholar] [CrossRef] [PubMed]
- Banas, B.; Boger, C.A.; Luckhoff, G.; Kruger, B.; Barabas, S.; Batzilla, J.; Schemmerer, M.; Kostler, J.; Bendfeldt, H.; Rascle, A.; et al. Validation of T-Track(R) CMV to assess the functionality of cytomegalovirus-reactive cell-mediated immunity in hemodialysis patients. BMC Immunol. 2017, 18, 15. [Google Scholar] [CrossRef] [Green Version]
- Barshes, N.R.; Goodpastor, S.E.; Goss, J.A. Pharmacologic immunosuppression. Front. Biosci. 2004, 9, 411–420. [Google Scholar] [CrossRef] [Green Version]
- Sood, S.; Haifer, C.; Yu, L.; Pavlovic, J.; Gow, P.J.; Jones, R.M.; Visvanathan, K.; Angus, P.W.; Testro, A.G. Targeted individual prophylaxis offers superior risk stratification for cytomegalovirus reactivation after liver transplantation. Liver Transpl. 2015, 21, 1478–1485. [Google Scholar] [CrossRef]
- Villacres, M.C.; Longmate, J.; Auge, C.; Diamond, D.J. Predominant type 1 CMV-specific memory T-helper response in humans: Evidence for gender differences in cytokine secretion. Hum. Immunol. 2004, 65, 476–485. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Recipient sex (no., %) | Male | 40 (71) |
| Female | 16 (29) | |
| Age, years (median, range) | 55 (20–68) | |
| Disease leading to transplantation (no.) | HCV | 11 |
| HBV | 9 | |
| Ethyltoxic Cirrhosis | 16 | |
| Autoimmune 1 | 10 | |
| Other | 10 | |
| Immunosuppressive regimens (no.) 2 | CNI, MMF | 44 |
| CNI, mTOR | 2 | |
| CNI | 4 | |
| CNI, MMF, steroids | 4 | |
| CNI, mTOR, steroids | 1 | |
| CNI, steroids | 1 | |
| CMV serostatus (no.,%) | D+/R− | 14 (25) |
| D−/R+ | 17 (30) | |
| D+/R+ | 25 (45) | |
| Patients with CMV-DNAemia post-transplant | D+/R− | 8/14 (67) |
| (no., % of the respective group) 3 | D−/R+ | 4/17 (24) |
| D+/R+ | 10/25 (40) | |
| Patients who received antiviral treatment for | D+/R− | 6/14 (43) |
| CMV-DNAemia (no.,% of the respective group) 3 | D−/R+ | 3/17 (18) |
| D+/R+ | 9/25 (36) | |
| Allograft rejection (no.) | 12 |
| (a) Two Different ELISpot Assays | ||||
|---|---|---|---|---|
| Parameter 1 | Parameter 2 | r | p | n |
| IE-1 Lo (Algo) | IE OI | 0.608 | <0.0001 | 100 |
| IE-1 Lo (Median) | IE OI | 0.606 | <0.0001 | 100 |
| IE-1 Lo (Algo) | IE-1 Lo (Median) | 0.987 | <0.0001 | 103 |
| pp65 Lo (Algo) | pp65 OI | 0.740 | <0.0001 | 99 |
| pp65 Lo (Median) | pp65 OI | 0.617 | <0.0001 | 99 |
| pp65 Lo (Algo) | pp65 Lo (Median) | 0.996 | <0.0001 | 103 |
| IE-1 Lo (Algo) | pp65 Lo (Algo) | 0.620 | <0.0001 | 103 |
| IE-1 Lo (Median) | pp65 Lo (Median) | 0.609 | <0.0001 | 103 |
| IE OI | pp65 OI | 0.706 | <0.0001 | 99 |
| (b) ELISpot Assays and QuantiFERON-CMV Assay | ||||
| Parameter | r | p | n | |
| IE-1 Lo (Algo) | 0.217 | 0.03 | 102 | |
| IE-1 Lo (Median) | 0.217 | 0.03 | 102 | |
| IE OI | 0.387 | <0.0001 | 99 | |
| pp65 Lo (Algo) | 0.565 | <0.0001 | 102 | |
| pp65 Lo (Median) | 0.551 | <0.0001 | 102 | |
| pp65 OI | 0.647 | <0.0001 | 98 | |
| ID | Age | Sex | IE-1 | pp65 | IE-1 | pp65 | IE-1 | pp65 | IE-1 | pp65 | QuantiFERON | CMV | Start 1 | End 1 | VL | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lo | Lo | OI | OI | Lo | Lo | OI | OI | Repli- | Max. | ||||||||||||
| M0 | M0 | M0 | M0 | M1 | M1 | M1 | M1 | M0 | M1 | M2 | M3 | M4 | M5 | M6 | cation | ||||||
| 1 | 57 | F | 0 | 0 | 1 | 0 | 14 | 19 | 12 | 105 | 0 | 0.3 | 0 | Y | M1 | M2 | 11,172 | ||||
| 2 | 39 | M | 0 | 0 | 0 | 0 | n.t. | n.t. | n.t. | n.t. | 0 | 0.7 | Y | M2 | M2 | 6696 | |||||
| 3 | 54 | F | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 100 | 2 | Y | M3 | M4 | 2007 | |||
| 4 | 55 | M | 2 | 0 | 4 | 8 | 0 | 0 | 0 | 0 | 0 | 0 | 17 | 5 | 3 | 7 | 5 | Y | M2 | M3 | 1006 |
| 5 | 47 | M | 0 | 0 | 0 | 0 | 1 | 7 | 20 | 40 | 0 | 0 | 7 | 4 | 100 | Y | M1 | M1 | 381 | ||
| 6 | 58 | F | 6 | 5 | 3 | 0 | 3 | 57 | 17 | 274 | 0 | 100 | 82 | 78 | 84 | 100 | 100 | Y | M3 | M5 | 321 |
| 7 | 66 | M | 0 | 1 | 0 | 2 | 1 | 100 | 4 | 76 | 0 | 38 | 4 | 4 | 0 | 8 | 7 | Y | M2 | M3 | 259 |
| 8 | 52 | M | 0 | 43 | 7 | 51 | 1 | 21 | 13 | 75 | 26 | 39 | 27 | 36 | 27 | Y | M1 | M1 | 258 | ||
| 9 | 43 | F | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | N | |||
| 10 | 51 | M | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | N | ||||
| 11 | 55 | M | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | N | |||
| 12 | 26 | M | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 7 | 0 | 0 | 0 | 0 | 0 | 0 | N | ||||
| 13 | 33 | M | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | N | ||||||
| 14 | 55 | M | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | N | |||||
| Test | AUC | Cohort | Time Point | Cut-Off | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| pp65 OI | 0.744 | All | M0 | 142 | 100% | 46% |
| IE-1 Lo | 0.762 | All | M1 | 3.5 | 100% | 59% |
| QuantiFERON | 0.605 | All | M1 | 32 | 100% | 23% |
| pp65 Lo | 0.700 | D+/R- | M0 | 0.5 | 100% | 40% |
| pp65 Lo | 0.722 | D+/R- | M1 | 0.5 | 100% | 44% |
| pp65 OI | 0.722 | D+/R- | M1 | 3.5 | 100% | 44% |
| QuantiFERON | 0.667 | D+/R- | M1 | 19 | 100% | 33% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gliga, S.; Fiedler, M.; Dornieden, T.; Achterfeld, A.; Paul, A.; Horn, P.A.; Herzer, K.; Lindemann, M. Comparison of Three Cellular Assays to Predict the Course of CMV Infection in Liver Transplant Recipients. Vaccines 2021, 9, 88. https://doi.org/10.3390/vaccines9020088
Gliga S, Fiedler M, Dornieden T, Achterfeld A, Paul A, Horn PA, Herzer K, Lindemann M. Comparison of Three Cellular Assays to Predict the Course of CMV Infection in Liver Transplant Recipients. Vaccines. 2021; 9(2):88. https://doi.org/10.3390/vaccines9020088
Chicago/Turabian StyleGliga, Smaranda, Melanie Fiedler, Theresa Dornieden, Anne Achterfeld, Andreas Paul, Peter A. Horn, Kerstin Herzer, and Monika Lindemann. 2021. "Comparison of Three Cellular Assays to Predict the Course of CMV Infection in Liver Transplant Recipients" Vaccines 9, no. 2: 88. https://doi.org/10.3390/vaccines9020088