
Neutralizing Antibody Response following a Third Dose of the mRNA-1273 Vaccine among Cancer Patients
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Procedures and Data Collection
2.2. SARS-CoV-2 Antibody Detection and Quantification Assay
2.3. SARS-CoV-2 Neutralizing Antibody Detection and Quantification Assay
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
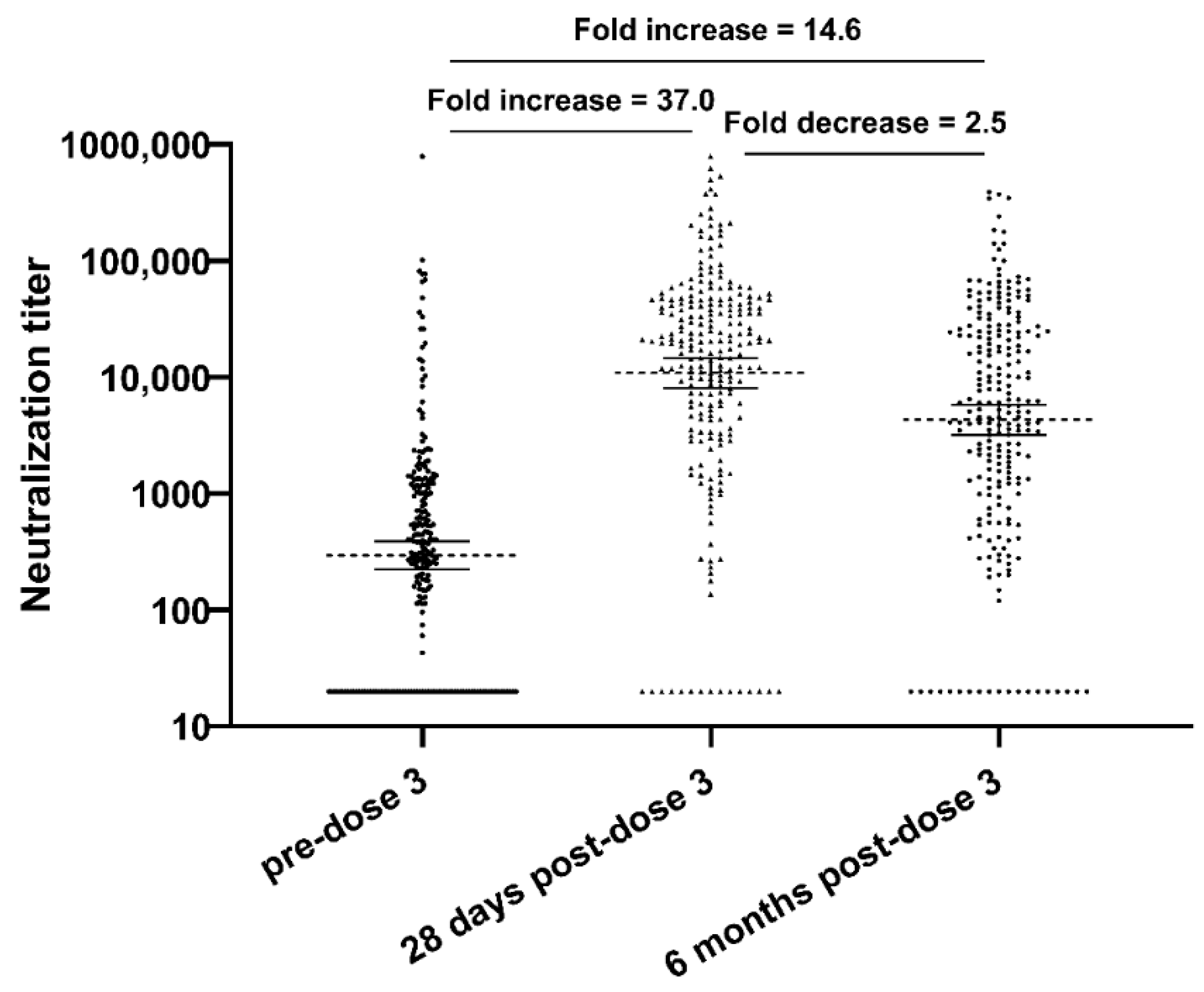
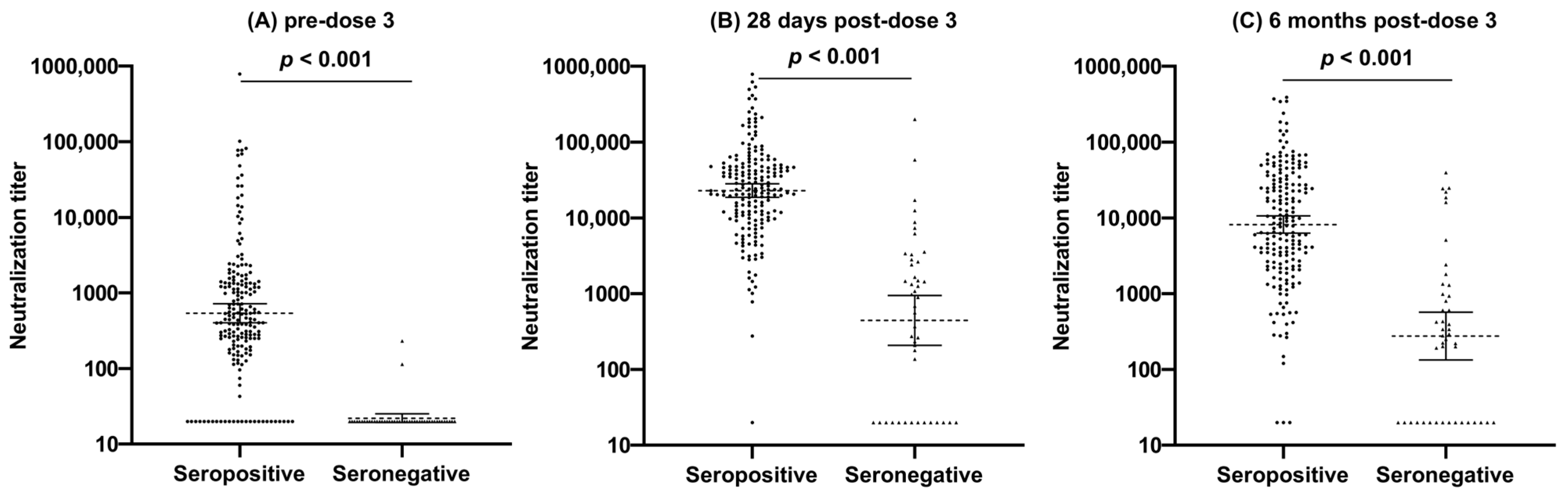
3.2. Neutralization Response
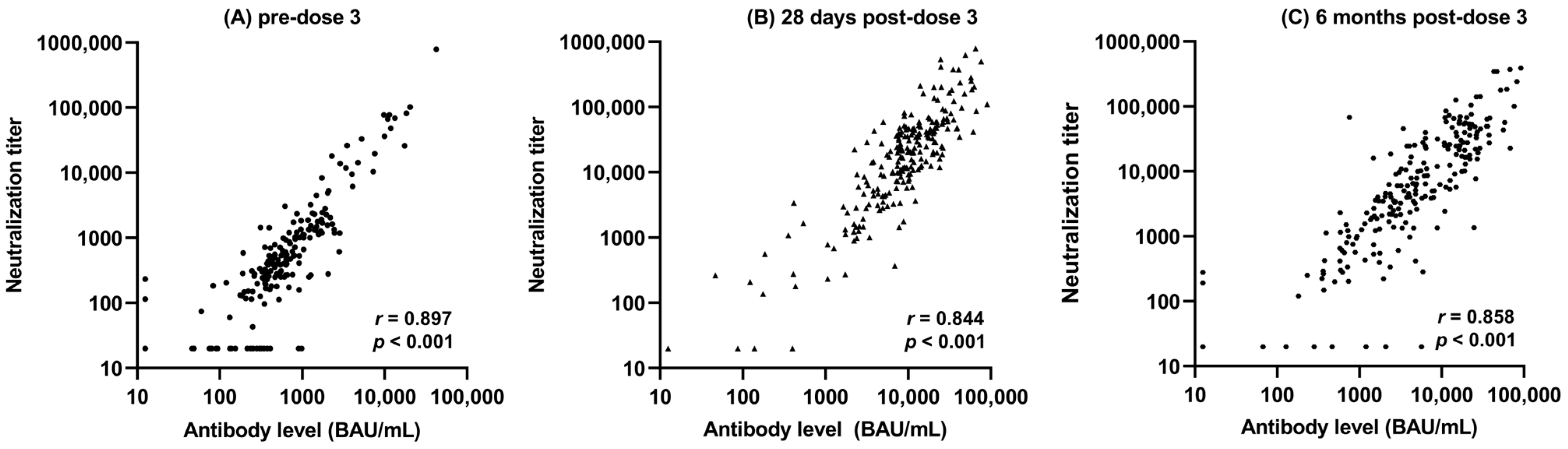
3.3. Correlation between Total Antibody and Neutralization Titers
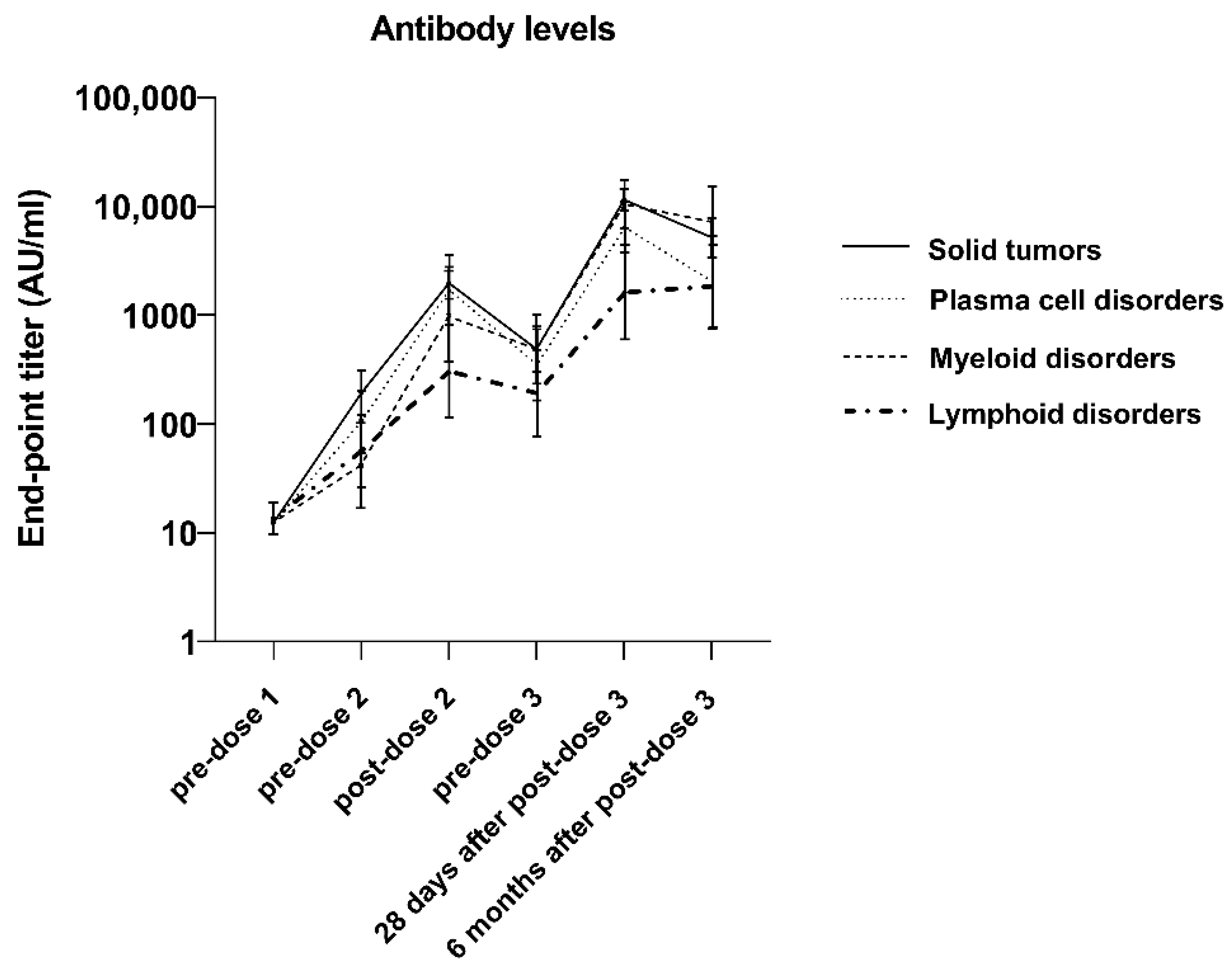
3.4. Antibody Response Duration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chavez-MacGregor, M.; Lei, X.; Zhao, H.; Scheet, P.; Giordano, S.H. Evaluation of COVID-19 Mortality and Adverse Outcomes in US Patients with or Without Cancer. JAMA Oncol. 2022, 8, 69–78. [Google Scholar] [CrossRef]
- Giuliano, A.R.; Lancet, J.E.; Pilon-Thomas, S.; Dong, N.; Jain, A.G.; Tan, E.; Ball, S.; Tworoger, S.S.; Siegel, E.M.; Whiting, J.; et al. Evaluation of Antibody Response to SARS-CoV-2 mRNA-1273 Vaccination in Patients with Cancer in Florida. JAMA Oncol. 2022, 8, 748–754. [Google Scholar] [CrossRef]
- Greenberger, L.M.; Saltzman, L.A.; Senefeld, J.W.; Johnson, P.W.; DeGennaro, L.J.; Nichols, G.L. Antibody response to SARS-CoV-2 vaccines in patients with hematologic malignancies. Cancer Cell 2021, 39, 1031–1033. [Google Scholar] [CrossRef]
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bronstein, Y.; Morales, M.; Ziv, T.; Arbel, Y.S.; Scarfò, L.; et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with chronic lymphocytic leukemia. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef]
- Massarweh, A.; Eliakim-Raz, N.; Stemmer, A.; Levy-Barda, A.; Yust-Katz, S.; Zer, A.; Benouaich-Amiel, A.; Ben-Zvi, H.; Moskovits, N.; Brenner, B.; et al. Evaluation of Seropositivity Following BNT162b2 Messenger RNA Vaccination for SARS-CoV-2 in Patients Undergoing Treatment for Cancer. JAMA Oncol. 2021, 7, 1133–1140. [Google Scholar] [CrossRef]
- Monin, L.; Laing, A.G.; Muñoz-Ruiz, M.; McKenzie, D.R.; del Molino del Barrio, I.; Alaguthurai, T.; Domingo-Vila, C.; Hayday, T.S.; Graham, C.; Seow, J.; et al. Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: Interim analysis of a prospective observational study. Lancet Oncol. 2021, 22, 765–778. [Google Scholar] [CrossRef]
- Shapiro, L.C.; Thakkar, A.; Campbell, S.T.; Forest, S.K.; Pradhan, K.; Gonzalez-Lugo, J.D.; Quinn, R.; Bhagat, T.D.; Choudhary, G.S.; McCort, M.; et al. Efficacy of booster doses in augmenting waning immune responses to COVID-19 vaccine in patients with cancer. Cancer Cell 2022, 40, 3–5. [Google Scholar] [CrossRef]
- Terpos, E.; Trougakos, I.P.; Gavriatopoulou, M.; Papassotiriou, I.; Sklirou, A.D.; Ntanasis-Stathopoulos, I.; Papanagnou, E.-D.D.; Fotiou, D.; Kastritis, E.; Dimopoulos, M.A. Low neutralizing antibody responses against SARS-CoV-2 in older patients with myeloma after the first BNT162b2 vaccine dose. Blood 2021, 137, 3674–3676. [Google Scholar] [CrossRef]
- Thakkar, A.; Gonzalez-Lugo, J.D.; Goradia, N.; Gali, R.; Shapiro, L.C.; Pradhan, K.; Rahman, S.; Kim, S.Y.; Ko, B.; Sica, R.A.; et al. Seroconversion rates following COVID-19 vaccination among patients with cancer. Cancer Cell 2021, 39, 1081–1090.e2. [Google Scholar] [CrossRef]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Franzese, M.; Coppola, L.; Silva, R.; Santini, S.A.; Cinquanta, L.; Ottomano, C.; Salvatore, M.; Incoronato, M. SARS-CoV-2 antibody responses before and after a third dose of the BNT162b2 vaccine in Italian healthcare workers aged ≤60 years: One year of surveillance. Front Immunol. 2022, 13, 947187. [Google Scholar] [CrossRef] [PubMed]
- Lake, D.F.; Roeder, A.J.; Gonzalez-Moa, M.J.; Koehler, M.; Kaleta, E.; Jasbi, P.; Vanderhoof, J.; McKechnie, D.; Forman, J.; Edwards, B.A.; et al. Third COVID-19 vaccine dose boosts neutralizing antibodies in poor responders. Commun. Med. 2022, 2, 85. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.-M.; Xu, Q.-Y.; Jia, Z.-J.; Wu, M.-J.; Liu, Y.-Y.; Lin, L.-R.; Liu, L.-L.; Yang, T.-C. A Third Dose of an Inactivated Vaccine Dramatically Increased the Levels and Decay Times of Anti-SARS-CoV-2 Antibodies, but Disappointingly Declined Again: A Prospective, Longitudinal, Cohort Study at 18 Serial Time Points Over 368 Days. Front. Immunol. 2022, 13, 876037. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Guo, Q.; Dai, Y.; Jiang, J.; Liu, M.; Ji, T.; Zhou, P.; Gong, F. Neutralizing activity of a third dose of CoronaVac against Omicron subvariants within a 20-month follow-up study. Hum. Vaccin. Immunother. 2023, 19, 2242217. [Google Scholar] [CrossRef] [PubMed]
- Malin, J.J.; Suárez, I.; Biehl, L.M.; Schommers, P.; Knops, E.; Di Cristanziano, V.; Heger, E.; Pflieger, E.; Wyen, C.; Bettin, D.; et al. Immune response to mRNA-based COVID-19 booster vaccination in people living with HIV. HIV Med. 2023, 24, 785–793. [Google Scholar] [CrossRef]
- Baek, Y.J.; Lee, Y.-J.; Park, S.R.; Kim, K.H.; Beom, S.-H.; Lee, C.-K.; Shin, S.J.; Rha, S.Y.; Kim, S.; Lee, K.H.; et al. Immunogenicity and Safety of Vaccines against Coronavirus Disease in Actively Treated Patients with Solid Tumors: A Prospective Cohort Study. Cancer Res. Treat. 2023, 55, 746–757. [Google Scholar] [CrossRef]
- Ligumsky, H.; Dor, H.; Etan, T.; Golomb, I.; Nikolaevski-Berlin, A.; Greenberg, I.; Halperin, T.; Angel, Y.; Henig, O.; Spitzer, A.; et al. COVI3 study investigators. Immunogenicity and safety of BNT162b2 mRNA vaccine booster in actively treated patients with cancer. Lancet Oncol. 2022, 23, 193–195. [Google Scholar] [CrossRef]
- Giuliano, A.; Kuter, B.; Pilon-Thomas, S.; Whiting, J.; Mo, Q.; Leav, B.; Sirak, B.; Cubitt, C.; Dukes, C.; Isaacs-Soriano, K.; et al. Safety and immunogenicity of a third dose of mRNA-1273 vaccine among cancer patients. Cancer Commun. 2023, 43, 749–764. [Google Scholar] [CrossRef]
- Dukes, C.W.; Rossetti, R.A.; Hensel, J.A.; Snedal, S.; Cubitt, C.L.; Schell, M.J.; Abrahamsen, M.; Isaacs-Soriano, K.; Kennedy, K.; Mangual, L.N.; et al. SARS-CoV-2 antibody response duration and neutralization following natural infection. J. Clin. Virol. Plus. 2023, 3, 100158. [Google Scholar] [CrossRef]
- Huang, Y.; Borisov, O.; Kee, J.J.; Carpp, L.N.; Wrin, T.; Cai, S.; Sarzotti-Kelsoe, M.; McDanal, C.; Eaton, A.; Pajon, R.; et al. Calibration of two validated SARS-CoV-2 pseudovirus neutralization assays for COVID-19 vaccine evaluation. Sci. Rep. 2021, 11, 23921. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.; Garner-Spitzer, E.; Jasinska, J.; Kollaritsch, H.; Stiasny, K.; Kundi, M.; Wiedermann, U. Age-related differences in humoral and cellular immune responses after primary immunisation: Indications for stratified vaccination schedules. Sci. Rep. 2018, 8, 9825. [Google Scholar] [CrossRef]
- Agha, M.E.; Blake, M.; Chilleo, C.; Wells, A.; Haidar, G. Suboptimal Response to Coronavirus Disease 2019 Messenger RNA Vaccines in Patients with Hematologic Malignancies: A Need for Vigilance in the Postmasking Era. Open Forum Infect Dis. 2021, 8, ofab353. [Google Scholar] [CrossRef]
- Pleyer, C.; Ali, M.A.; Cohen, J.I.; Tian, X.; Soto, S.; Ahn, I.E.; Gaglione, E.M.; Nierman, P.; Marti, G.E.; Hesdorffer, C.; et al. Effect of Bruton tyrosine kinase inhibitor on efficacy of adjuvanted recombinant hepatitis B and zoster vaccines. Blood 2021, 137, 185–189. [Google Scholar] [CrossRef]
- Janzic, U.; Bidovec-Stojkovic, U.; Korosec, P.; Mohorcic, K.; Mrak, L.; Caks, M.; Ravnik, M.; Skof, E.; Rijavec, M. A Three-Dose mRNA COVID-19 Vaccine Regime Produces Both Suitable Immunogenicity and Satisfactory Efficacy in Patients with Solid Cancers. Vaccines 2023, 11, 1017. [Google Scholar] [CrossRef]
- Overheu, O.; Lendowski, S.; Quast, D.R.; Kühn, D.; Blanco, E.V.; Kraeft, A.-L.; Steinmann, E.; Kourti, E.; Lugnier, C.; Steinmann, J.; et al. Longitudinal data on humoral response and neutralizing antibodies against SARS-CoV-2 Omicron BA.1 and subvariants BA.4/5 and BQ.1.1 after COVID-19 vaccination in cancer patients. J. Cancer Res. Clin. Oncol. 2023, 149, 10633–10644. [Google Scholar] [CrossRef]
- Felip, E.; Pradenas, E.; Romeo, M.; Marfil, S.; Trinité, B.; Urrea, V.; Hernández, A.; Ballana, E.; Cucurull, M.; Mateu, L.; et al. Impact of chemotherapy and/or immunotherapy on neutralizing antibody response to SARS-CoV-2 mRNA-1237 vaccine in patients with solid tumors. Mol. Oncol. 2023, 17, 686–694. [Google Scholar] [CrossRef]
- Zeng, C.; Evans, J.P.; Reisinger, S.; Woyach, J.; Liscynesky, C.; El Boghdadly, Z.; Rubinstein, M.P.; Chakravarthy, K.; Saif, L.; Oltz, E.M.; et al. Impaired neutralizing antibody response to COVID-19 mRNA vaccines in cancer patients. Cell Biosci. 2021, 11, 197. [Google Scholar] [CrossRef]
- Fendler, A.; Shepherd, S.T.C.; Au, L.; Wilkinson, K.A.; Wu, M.; Byrne, F.; Cerrone, M.; Schmitt, A.M.; Joharatnam-Hogan, N.; Shum, B.; et al. Adaptive immunity and neutralizing antibodies against SARS-CoV-2 variants of concern following vaccination in patients with cancer: The CAPTURE study. Nat. Cancer. 2021, 2, 1305–1320. [Google Scholar] [CrossRef]
- Higashimoto, Y.; Kozawa, K.; Miura, H.; Kawamura, Y.; Ihira, M.; Hiramatsu, H.; Suzuki, R.; Haga, K.; Takai-Todaka, R.; Sawada, A.; et al. Correlation between anti-S IgG and neutralizing antibody titers against three live SARS-CoV-2 variants in BNT162b2 vaccine recipients. Hum. Vaccin. Immunother. 2022, 18, 2105611. [Google Scholar] [CrossRef]
- Heftdal, L.D.; Hamm, S.R.; Pérez-Alós, L.; Madsen, J.R.; Armenteros, J.J.A.; Fogh, K.; Kronborg, C.C.; Vallentin, A.P.; Hasselbalch, R.B.; Møller, D.L.; et al. Humoral and cellular immune responses after three or four doses of BNT162b2 in patients with hematological malignancies. Eur. J. Haematol. 2023, 111, 229–239. [Google Scholar] [CrossRef]
- Thakkar, A.; Pradhan, K.; Duva, B.; Carreno, J.M.; Sahu, S.; Thiruthuvanathan, V.; Campbell, S.; Gallego, S.; Bhagat, T.D.; Rivera, J.; et al. Study of efficacy and longevity of immune response to third and fourth doses of COVID-19 vaccines in patients with cancer: A single arm clinical trial. eLife 2023, 12, e83694. [Google Scholar] [CrossRef] [PubMed]
- Lasagna, A.; Bergami, F.; Lilleri, D.; Percivalle, E.; Quaccini, M.; Serra, F.; Comolli, G.; Sarasini, A.; Sammartino, J.C.; Ferrari, A.; et al. Six-month humoral and cellular immune response to the third dose of BNT162b2 anti-SARS-CoV-2 vaccine in patients with solid tumors: A longitudinal cohort study with a focus on the variants of concern. ESMO Open 2022, 7, 100574. [Google Scholar] [CrossRef] [PubMed]
- Fendler, A.; Shepherd, S.T.; Au, L.; Wilkinson, K.A.; Wu, M.; Schmitt, A.M.; Tippu, Z.; Farag, S.; Rogiers, A.; Harvey, R.; et al. Immune responses following third COVID-19 vaccination are reduced in patients with hematological malignancies compared to patients with solid cancer. Cancer Cell 2022, 40, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention. COVID-19 Vaccines for People Who Are Moderately or Severely Immunocompromised: Centers for Disease Control and Prevention. 2023. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/immuno.html?s_cid=11710:immunocompromised%20covid%20booster%20dose:sem.ga:p:RG:GM:gen:PTN.Grants:FY22 (accessed on 30 July 2023).
- Center for Disease Control and Prevention. Stay Up to Date with COVID-19 Vaccines: Centers for Disease Control and Prevention. 2023. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/stay-up-to-date.html (accessed on 30 July 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Cancer Patients (N = 238) | |
|---|---|
| n (%) | |
| Age group (median age 67 years) | |
| ≤67 years | 124 (52.1) |
| >67 years | 114 (47.9) |
| Gender | |
| Male | 131 (55) |
| Female | 107 (45) |
| Ethnicity | |
| Hispanic | 17 (7.1) |
| Non-Hispanic | 221 (92.9) |
| Race | |
| African American | 9 (3.8) |
| Asian | 3 (1.3) |
| White | 219 (92) |
| Other # | 7 (2.9) |
| Primary patient category | |
| Hematologic malignancies | 134 (56.3) |
| Myeloid | 33 (24.6) |
| Lymphoid | 54 (40.3) |
| Plasma cell disorders | 47 (35.1) |
| Solid tumors | 104 (43.7) |
| Disease status | |
| Previously untreated | 21 (8.8) |
| Remission | 143 (60.1) |
| Relapse/refractory/stable disease | 74 (31.1) |
| Lymphocyte count a | |
| >1 × 109/L | 129 (64.2) |
| ≤1 × 109/L | 72 (35.8) |
| Among plasma cell disorders (n = 47) | |
| IgG level a | |
| <700 mg/dL | 26 (56.5) |
| ≥700 mg/dL | 20 (43.5) |
| IgA level a | |
| <70 mg/dL | 24 (52.2) |
| ≥70 mg/dL | 22 (47.8) |
| IgM level a | |
| <40 mg/dL | 36 (78.3) |
| ≥40 mg/dL | 10 (21.7) |
| Received anticancer therapy within 3 months b | |
| No | 130 (54.6) |
| Yes | 108 (45.4) |
| Small molecules c | |
| No | 186 (78.2) |
| Yes | 52 (21.8) |
| Anti-CD20 antibodies within 6 months | |
| No | 228 (95.8) |
| Yes | 10 (4.2) |
| Anti-CD38 antibodies within 6 months | |
| No | 224 (94.1) |
| Yes | 14 (5.9) |
| Patients treated with cellular therapy | |
| No | 200 (84) |
| Yes | 38 (16) |
| Patients treated with cellular therapy type | |
| Allo-HSCT at any time prior to vaccination | 19 (50) |
| Auto-HSCT within the past 24 months | 13 (34.2) |
| CD19 CAR-T at any time prior to vaccination | 5 (13.2) |
| BCMA CAR-T at any time prior to vaccination | 1 (2.6) |
| BTK inhibitors | |
| No | 233 (97.9) |
| Yes | 5 (2.1) |
| Line of systemic therapy to date | |
| 0 | 56 (23.5) |
| 1 | 97 (40.8) |
| ≥2 | 85 (35.7) |
| n | Pre-Dose 3 | p-Value * | 28 Days Post-Dose 3 | p-Value ** | 6 Months Post-Dose 3 | p-Value *** | |
|---|---|---|---|---|---|---|---|
| Overall | 238 | 294.3 (221.5–391) | 10,876.7 (8118.6–14,571.7) | 4311 (3187.7–5830.2) | |||
| Age group (median age 67 years) | <0.001 | 0.049 | 0.006 | ||||
| ≤67 | 124 | 445.8 (308.7–643.8) | 13,765 (9433.5–20,085.4) | 5946.1 (3854–9173.8) | |||
| >67 | 114 | 187.3 (122–287.6) | 8418.7 (5352.8–13,240.6) | 3038.6 (2006.1–4602.6) | |||
| Gender | 0.074 | 0.416 | 0.196 | ||||
| Male | 131 | 232.9 (160.6–337.7) | 10,238.7 (6952.1–15,078.9) | 3742.6 (2527.1–5542.8) | |||
| Female | 107 | 392 (252.7–608.1) | 11,712.2 (7451.7–18,408.6) | 5125.7 (3191.6–8232) | |||
| Ethnicity | 0.684 | 0.582 | 0.679 | ||||
| Hispanic | 17 | 253.4 (95–675.6) | 9121.3 (2731.6–30,458.4) | 4904 (1164.2–20,657.7) | |||
| Non-Hispanic | 221 | 297.7 (220.9–401.2) | 11,024.9 (8137.3–14,937.3) | 4268.5 (3132.3–5816.8) | |||
| Race | 0.707 | 0.319 | 0.079 | ||||
| African American | 9 | 186.3 (64.8–536.1) | 9756.2 (1497.2–63,574.3) | 3596.2 (593.4–21,795.3) | |||
| Asian | 3 | 315.8 (0.8–119,688.4) | 37,742.6 (4145.2–343,651.3) | 1652.5 (0–353,348,110.9) | |||
| White | 219 | 291.1 (215.2–393.7) | 10,275.8 (7561.4–13,964.5) | 4106.5 (3011.5–5599.6) | |||
| Other # | 7 | 726.7 (143.6–3677) | 43,432.2 (8454.6–223,116.2) | 37,547.5 (9493.9–148,496.6) | |||
| Primary patient category a | 0.186 | 0.002 | 0.184 | ||||
| Hematologic malignancies b | 134 | 251.4 (168.3–375.6) | 0.608 | 6593.8 (4176.4–10,410.6) | 0.029 | 3330.9 (2130.9–5206.6) | 0.165 |
| Myeloid | 33 | 319.5 (146–699.1) | 13,485.4 (5804.7–31,328.9) | 7010.9 (3089–15,912.4) | |||
| Lymphoid | 54 | 212.2 (105.5–426.8) | 2966.6 (1263.0–6967.8) | 2174.4 (1023.5–4619.5) | |||
| Plasma cell disorders | 47 | 258.2 (134.5–495.7) | 9988.9 (5490.6–18,172.6) | 3224.3 (1512.2–6874.6) | |||
| Solid tumors | 104 | 360.5 (242.1–537) | 20,727.9 (15,638–27,474.4) | 6010.5 (4106.6–8797) | |||
| Disease status | 0.160 | 0.913 | 0.753 | ||||
| Previously untreated | 21 | 361.6 (116.1–1126.2) | 15,220.6 (6170.9–37,542.0) | 3736.5 (1326.6–10,524) | |||
| Remission | 143 | 341.4 (238.3–489.1) | 11,226.4 (7805.7–16,146.1) | 4214.7 (2848.6–6235.9) | |||
| Relapse/refractory/stable disease | 74 | 208.4 (124.2–349.6) | 9300.8 (5154.2–16,783.4) | 4690 (2686–8188.9) | |||
| Lymphocyte count c | 0.003 | <0.001 | 0.006 | ||||
| >1 × 109/L | 129 | 398.9 (269.5–590.5) | 18,435.1 (13,000.9–26,140.9) | 6158.8 (4320.7–8778.8) | |||
| ≤1 × 109/L | 72 | 158 (93.2–267.8) | 3299.5 (1745.7–6236.2) | 1806.9 (930.9–3507.2) | |||
| Among plasma cell disorders (n = 47) | |||||||
| IgG level c | 0.289 | 0.012 | 0.506 | ||||
| <700 mg/dL | 26 | 181.3 (77.8–422.5) | 5359.3 (2377.0–12,083.7) | 2683.3 (946.0–7611.3) | |||
| ≥700 mg/dL | 20 | 374.4 (122.4–1145) | 21,475.2 (8904.1–51,795.1) | 3915.7 (1114.9–13,752.7) | |||
| IgA level c | 0.165 | 0.014 | 0.230 | ||||
| <70 mg/dL | 24 | 171.8 (58.6–503.9) | 4491.7 (1731.0–11,655.3) | 1953.3 (627.8–6077.9) | |||
| ≥70 mg/dL | 22 | 371.7 (167.6–824.7) | 22,951.3 (12,215.8–43,121.3) | 5349.7 (1796.4–15,931.3) | |||
| IgM level c | 0.290 | 0.107 | 0.957 | ||||
| <40 mg/dL | 36 | 216.3 (103.7–451.4) | 8591.7 (4635.3–15,924.9) | 3258.7 (1436.8–7391) | |||
| ≥40 mg/dL | 10 | 409.6 (69.6–2412.6) | 15,735.4 (2109.4–11,7382.5) | 2839.2 (261.9–30,777.6) | |||
| Received anticancer therapy within 3 months d | <0.001 | <0.001 | 0.051 | ||||
| No | 130 | 480.1 (328.2–702.2) | 17,528.3 (12,547.1–24,487.1) | 6116.3 (4224.8–8854.7) | |||
| Yes | 108 | 163.3 (108.8–245.2) | 6124.0 (3760.9–9972.1) | 2829.6 (1735.3–4613.9) | |||
| Small molecules e | 0.008 | 0.001 | 0.140 | ||||
| No | 186 | 366.6 (265.6–505.8) | 13,381.5 (9655.7–18,545) | 4946.4 (3549.5–6893.0) | |||
| Yes | 52 | 134.2 (75.7–237.9) | 5182.5 (2747.0–9777.5) | 2636.3 (1291.8–5380.1) | |||
| Anti-CD20 antibodies | 0.081 | 0.002 | 0.862 | ||||
| No | 228 | 309.3 (232.2–411.9) | 12,511.5 (9458.2–16,550.5) | 4380.0 (3224.2–5950.1) | |||
| Yes | 10 | 94.9 (13.6–660.8) | 446.7 (44.6–4476.8) | 3001.1 (396.3–22,723.4) | |||
| Anti-CD38 antibodies | 0.023 | 0.030 | 0.275 | ||||
| No | 224 | 315.3 (236.6–420.2) | 11,356.0 (8359.2–15,427.3) | 4527.3 (3325.1–6164.1) | |||
| Yes | 14 | 97.7 (20.7–460.3) | 5455.1 (2316.3–12,847.4) | 1969.7 (429.9–9024.1) | |||
| Patients treated with cellular therapy | 0.379 | 0.554 | 0.147 | ||||
| No | 200 | 282.7 (208.9–382.5) | 11,397.5 (8452.1–15,369.3) | 4024.2 (2918.6–5548.6) | |||
| Yes | 38 | 363.9 (158.7–834.5) | 8503.1 (3207.5–22,542.2) | 6193.6 (2580.5–14,865.6) | |||
| Patients treated with cellular therapy type | |||||||
| Allo-HSCT at any time prior to vaccination | 19 | 479.1 (153.4–1496.1) | 13,973 (3385.5–57,669.7) | 17,795.9 (6538.5–48,435.1) | |||
| Auto-HSCT within the past 24 months | 13 | 402.4 (83.5–1939.9) | 19,059.3 (7203.1–50,430.6) | 6203.8 (1915.5–20,093) | |||
| CD19 CAR-T at any time prior to vaccination | 5 | 83.9 (1.6–4491.1) | 128.8 (3–5542.8) | 245.9 (3–20,446.3) | |||
| BCMA CAR-T at any time prior to vaccination | 1 | 816 (.) | 23,603 (.) | 120 (.) | |||
| BTK inhibitors | 0.145 | 0.007 | 0.032 | ||||
| No | 233 | 303.7 (227.8–404.9) | 11,467.8 (8548.4–15,384.2) | 4514.3 (3332.5–6115.4) | |||
| Yes | 5 | 68.0 (8.5–544.1) | 923.6 (128.3–6649.2) | 503.3 (36.5–6941.0) | |||
| Line of systemic therapy to date | 0.205 | 0.907 | 0.232 | ||||
| 0 | 56 | 428.5 (230.8–795.6) | 14,685.2 (8390.2–25,703.1) | 4029.5 (2198.9–7384.2) | |||
| 1 | 97 | 310.4 (204.3–471.7) | 10,684.9 (6897.9–16,551.2) | 6056.9 (3974.6–9230.1) | |||
| ≥2 | 85 | 216.2 (131.2–356.2) | 9107.8 (5264.5–15,756.7) | 3057.6 (1716.1–5447.6) |
| Neutralization Titer at Different Timepoints | ||||||
|---|---|---|---|---|---|---|
| Pre-Dose 3 | 28 Days Post-Dose 3 | 6 Months Post-Dose 3 | ||||
| Antibody Level | Spearman Correlation Coefficients (95% CI) | p Value | Spearman Correlation Coefficients (95% CI) | p Value | Spearman Correlation Coefficients (95% CI) | p Value |
| Pre-dose 3 (n = 238) | 0.897 (0.868–0.919) | <0.001 | 0.662 (0.583–0.727) | <0.001 | 0.494 (0.390–0.583) | <0.001 |
| 28 days post-dose 3 (n = 238) | 0.515 (0.414–0.602) | <0.001 | 0.844 (0.802–0.876) | <0.001 | 0.555 (0.459–0.636) | <0.001 |
| 6 months post-dose 3 (n = 234) | 0.424 (0.312–0.523) | <0.001 | 0.613 (0.525–0.687) | <0.001 | 0.858 (0.819–0.888) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dukes, C.W.; Potez, M.; Lancet, J.; Kuter, B.J.; Whiting, J.; Mo, Q.; Leav, B.; Wang, H.; Vanas, J.S.; Cubitt, C.L.; et al. Neutralizing Antibody Response following a Third Dose of the mRNA-1273 Vaccine among Cancer Patients. Vaccines 2024, 12, 13. https://doi.org/10.3390/vaccines12010013
Dukes CW, Potez M, Lancet J, Kuter BJ, Whiting J, Mo Q, Leav B, Wang H, Vanas JS, Cubitt CL, et al. Neutralizing Antibody Response following a Third Dose of the mRNA-1273 Vaccine among Cancer Patients. Vaccines. 2024; 12(1):13. https://doi.org/10.3390/vaccines12010013
Chicago/Turabian StyleDukes, Christopher W., Marine Potez, Jeffrey Lancet, Barbara J. Kuter, Junmin Whiting, Qianxing Mo, Brett Leav, Haixing Wang, Julie S. Vanas, Christopher L. Cubitt, and et al. 2024. "Neutralizing Antibody Response following a Third Dose of the mRNA-1273 Vaccine among Cancer Patients" Vaccines 12, no. 1: 13. https://doi.org/10.3390/vaccines12010013