


Association of Maternal Inactivated COVID-19 Vaccination within 3 Months before Conception with Neonatal Outcomes

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Primary Outcomes
2.3. Secondary Outcomes
2.4. Statistical Analysis
3. Results
3.1. Demographic and Baseline Characteristics
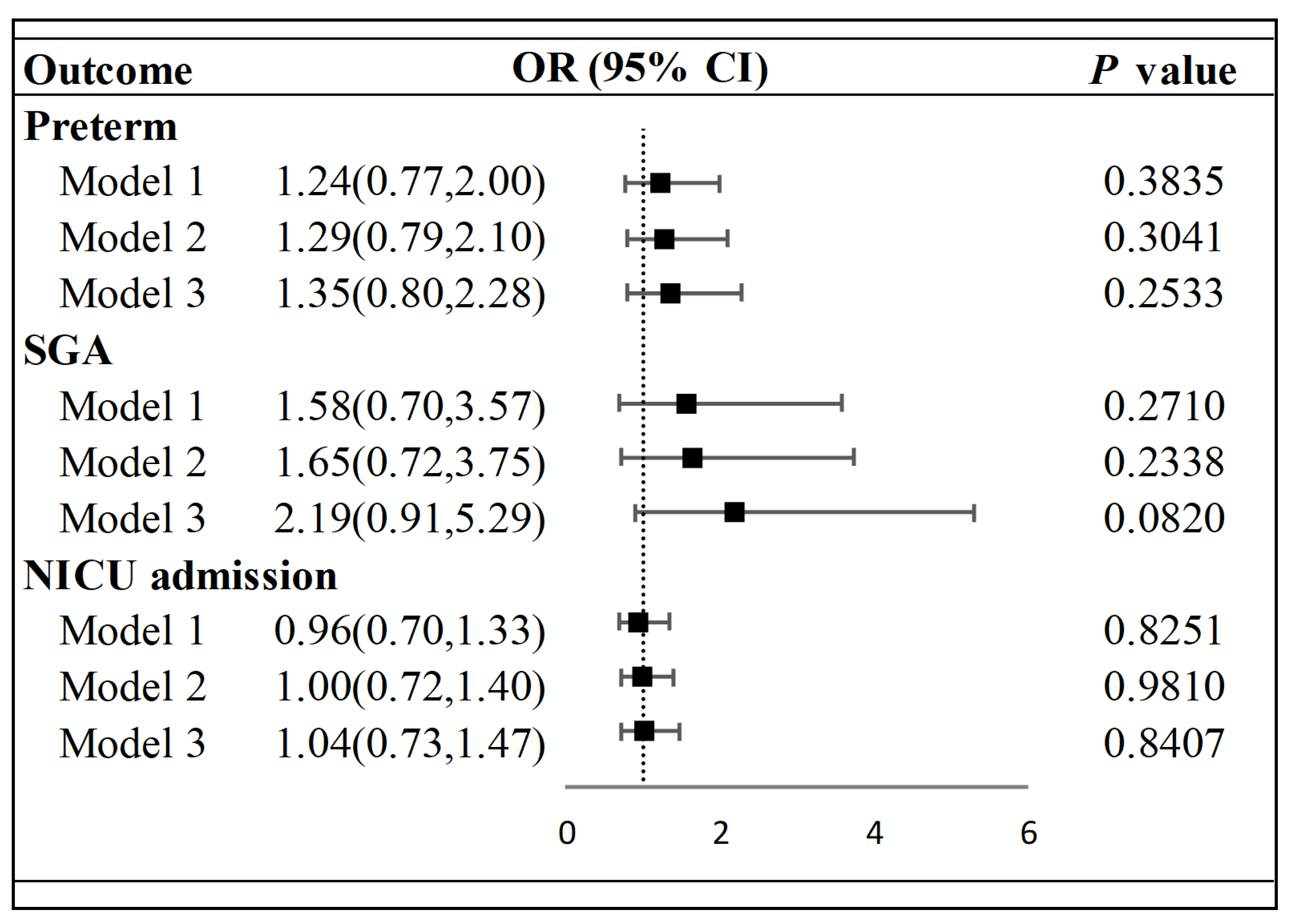
3.2. Primary Outcomes
3.3. Secondary Outcomes
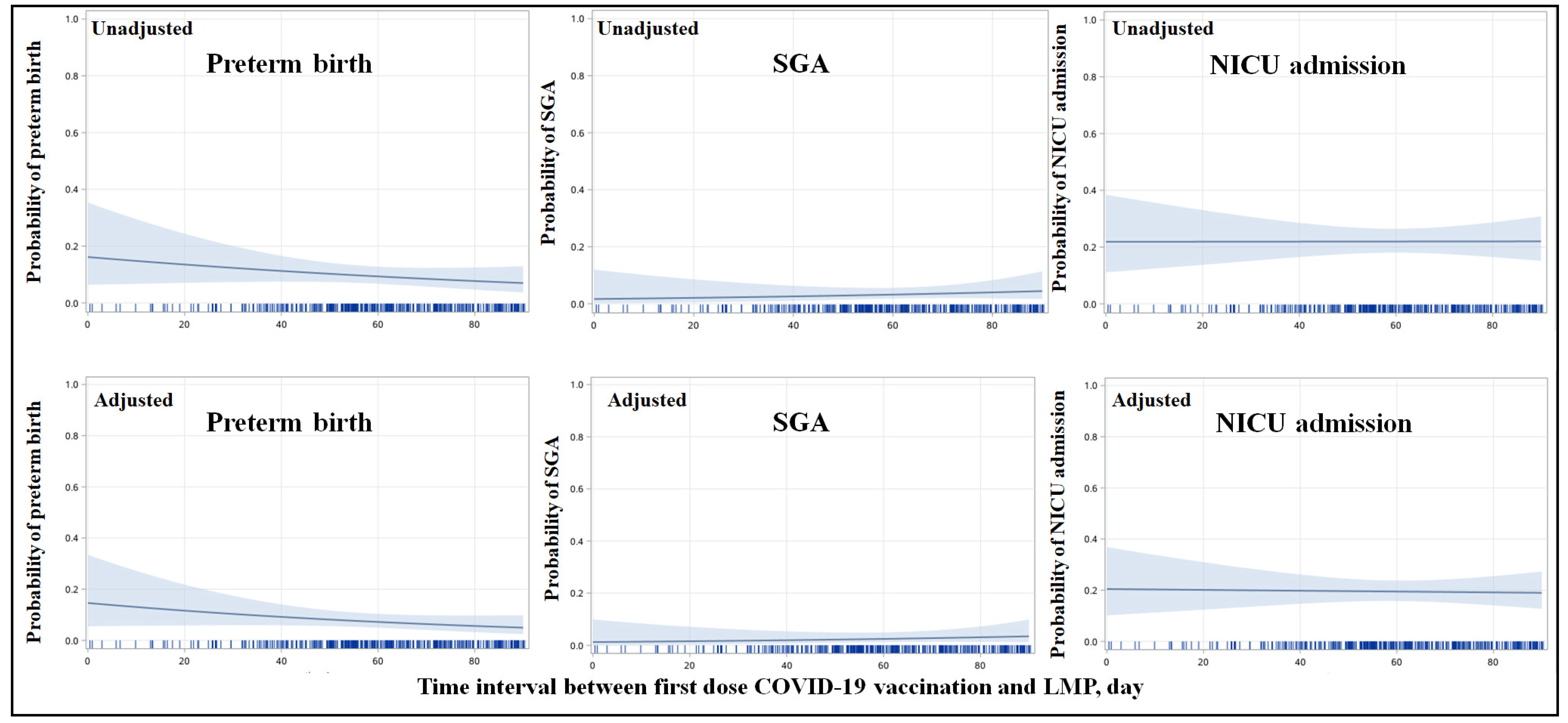
3.4. Subgroup Analysis According to the Timing of COVID-19 Vaccination
3.5. Subgroup Analysis According to Different Vaccine Types
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 30 July 2023).
- World Health Organization. Weekly Epidemiological Update on COVID-19—27 July 2023. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---27-july-2023 (accessed on 30 July 2023).
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J.; et al. Safety and Efficacy of Nvx-Cov2373 Covid-19 Vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and Efficacy of the Chadox1 Ncov-19 Vaccine (Azd1222) against SARS-CoV-2: An Interim Analysis of Four Randomised Controlled Trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the Bnt162b2 Mrna COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.; Kalafat, E.; Blakeway, H.; Townsend, R.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; Le Doare, K.; Ladhani, S.; et al. Systematic Review and Meta-Analysis of the Effectiveness and Perinatal Outcomes of COVID-19 Vaccination in Pregnancy. Nat. Commun. 2022, 13, 2414. [Google Scholar] [CrossRef] [PubMed]
- Goldshtein, I.; Steinberg, D.M.; Kuint, J.; Chodick, G.; Segal, Y.; Ben David, S.S.; Ben-Tov, A. Association of Bnt162b2 COVID-19 Vaccination During Pregnancy with Neonatal and Early Infant Outcomes. JAMA Pediatr. 2022, 176, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Huang, T.; Chen, Z.; Zhang, L.; Gao, Q.; Liu, G.; Zheng, J.; Ding, F. Systematic Review and Meta-Analysis of Neonatal Outcomes of COVID-19 Vaccination in Pregnancy. Pediatr. Res. 2023, 94, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Ibroci, E.; Liu, X.; Lieb, W.; Jessel, R.; Gigase, F.A.; Chung, K.; Graziani, M.; Lieber, M.; Ohrn, S.; Lynch, J.; et al. Impact of Prenatal Covid-19 Vaccination on Delivery and Neonatal Outcomes: Results from a New York City Cohort. Vaccine 2023, 41, 649–656. [Google Scholar] [CrossRef]
- Ma, Y.; Shan, Z.; Gu, Y.; Huang, Y. Safety and Efficacy of Inactivated Covid-19 Vaccines in Women Vaccinated During the First Trimester of Pregnancy. Int. J. Infect. Dis. 2023, 130, 196–202. [Google Scholar] [CrossRef]
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; Vale, M.S.D.; Cardona-Perez, J.A.; et al. Maternal and Neonatal Morbidity and Mortality among Pregnant Women with and without COVID-19 Infection: The Intercovid Multinational Cohort Study. AMA Pediatr. 2021, 175, 817–826. [Google Scholar] [CrossRef]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical Manifestations, Risk Factors, and Maternal and Perinatal Outcomes of Coronavirus Disease 2019 in Pregnancy: Living Systematic Review and Meta-Analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef]
- Leung, C.; Selle, L.; de Paiva, K.M.; Haas, P. Neonates Are More Vulnerable to Symptomatic SARS-CoV-2 Infection Than Children: A Matched Cohort Study in Brazil. World J. Pediatr. 2022, 18, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Cascant-Vilaplana, M.M.; Lara-Cantón, I.; Ramos-Garcia, V.; Pinilla-González, A.; Solaz-García, Á.; Quintás, G.; Marín-Reina, P.; Aguar, M.; Torrejón-Rodríguez, L.; Vento, M.; et al. Metabolic Dysregulation in Term Infants from SARS-CoV-2-Infected Mothers. World J. Pediatr. 2023, 19, 912–917. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.G.; Grinceviciene, S.; Haldre, K.; Lonnee-Hoffmann, R.; Donders, F.; Tsiakalos, A.; Adriaanse, A.; de Oliveira, J.M.; Ault, K.; Mendling, W.; et al. Isidog Consensus Guidelines on COVID-19 Vaccination for Women before, During and after Pregnancy. J. Clin. Med. 2021, 10, 2902. [Google Scholar] [CrossRef] [PubMed]
- Chinese Medical Association. Expert opinions on COVID-19 vaccination before conception, in pregnancy and lactation. Chin. J. Perinat. Med. 2022, 25, 13–17. [Google Scholar]
- World Health Organization. WHO COVID-19 Vaccines. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines (accessed on 30 July 2023).
- Centers for Disease Control and Prevention. COVID-19 Vaccines for People Who Would Like to Have a Baby. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/planning-for-pregnancy.html (accessed on 30 July 2023).
- Zhao, Y.; Zhao, Y.; Su, X.; Zhou, Y.; Zhang, Z.; Zhang, Y.; Li, M.; Jin, L. No Association of Vaccination with Inactivated Covid-19 Vaccines before Conception with Pregnancy Complications and Adverse Birth Outcomes: A Cohort Study of 5457 Chinese Pregnant Women. J. Med. Virol. 2023, 95, e28735. [Google Scholar] [CrossRef]
- National Health Commission of People’s Republic of China. National Vaccination of COVID-19. Available online: http://www.nhc.gov.cn/xcs/xxgzbd/gzbd_index.shtml (accessed on 30 July 2023).
- World Health Organization. The Sinopharm COVID-19 vaccine: What you Need to Know. Available online: https://www.who.int/news-room/feature-stories/detail/the-sinopharm-covid-19-vaccine-what-you-need-to-know (accessed on 30 July 2023).
- World Health Organization. The Moderna COVID-19 (mRNA-1273) Vaccine: What You Need to Know. Available online: https://www.who.int/news-room/feature-stories/detail/the-moderna-covid-19-mrna-1273-vaccine-what-you-need-to-know (accessed on 30 July 2023).
- Li, M.; Hao, J.; Jiang, T.; Deng, W.; Lu, H.; Wang, S.; Wan, G.; Xie, Y.; Yi, W. Maternal and Neonatal Safety of COVID-19 Vaccination During the Peri-Pregnancy Period: A Prospective Study. J. Med. Virol. 2023, 95, e28378. [Google Scholar] [CrossRef]
- Saito, S.; Nakashima, A.; Shima, T.; Ito, M. Th1/Th2/Th17 and Regulatory T-Cell Paradigm in Pregnancy. Am. J. Reprod. Immunol. 2010, 63, 601–610. [Google Scholar] [CrossRef]
- European Society of Human Reproduction and Embryology COVID-19Working Group. COVID-19 Vaccination and Assisted Reproduction. (Publication Date 08 June 2021). Available online: https://www.eshre.eu/Home/COVID19WG (accessed on 30 July 2023).
- Aharon, D.; Lederman, M.; Ghofranian, A.; Hernandez-Nieto, C.; Canon, C.; Hanley, W.B.; Gounko, D.M.; Lee, J.A.B.; Stein, D.; Buyuk, E.; et al. In Vitro Fertilization and Early Pregnancy Outcomes after Coronavirus Disease 2019 (COVID-19) Vaccination. Obstet.Gynecol. 2022, 139, 490–497. [Google Scholar] [CrossRef]
- Odeh-Natour, R.; Shapira, M.; Estrada, D.; Freimann, S.; Tal, Y.; Atzmon, Y.; Bilgory, A.; Aslih, N.; Abu-Raya, Y.S.; Shalom-Paz, E. Does Mrna SARS-CoV-2 Vaccine in the Follicular Fluid Impact Follicle and Oocyte Performance in Ivf Treatments? Am. J. Reprod. Immunol. 2022, 87, e13530. [Google Scholar] [CrossRef]
- Huang, J.; Xia, L.; Lin, J.; Liu, B.; Zhao, Y.; Xin, C.; Ai, X.; Cao, W.; Zhang, X.; Tian, L.; et al. No Effect of Inactivated SARS-CoV-2 Vaccination on in Vitro Fertilization Outcomes: A Propensity Score-Matched Study. J. Inflamm. Res. 2022, 15, 839–849. [Google Scholar] [CrossRef]
- Shi, W.; Wang, M.; Xue, X.; Li, N.; Chen, L.; Shi, J. Association between Time Interval from COVID-19 Vaccination to in Vitro Fertilization and Pregnancy Rate after Fresh Embryo Transfer. JAMA Netw. Open 2022, 5, e2236609. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Unvaccinated | Vaccinated | p Value | |
|---|---|---|---|
| Demographic characteristics | N = 487 | N = 369 | |
| Maternal age, years | 31.49 ± 4.27 | 31.50 ± 4.26 | 0.9669 |
| Ethic Han, n (%) | 473 (97.13) | 362 (98.10) | 0.3598 |
| Education, n (%) | 0.0485 | ||
| Senior high or below | 143 (29.36) | 83 (22.49) | |
| College or higher | 344 (70.64) | 286 (77.51) | |
| Per capita annual disposable income, n (%) | 0.1545 | ||
| <4380 USD | 94 (19.30) | 86 (23.31) | |
| ≥4380 USD | 393 (80.70) | 283 (76.69) | |
| Vaccination Information | |||
| Types of inactivated, n (%) | <0.0001 | ||
| Sinopharm-BIBP | 0 (0.00) | 231 (62.6) | |
| Sinovac-Coronavac | 0 (0.00) | 138 (37.4) | |
| Dose of maternal vaccination, n (%) | <0.0001 | ||
| 0 | 487 (100.00) | 0 (0.00) | |
| 1 | 0 (0.00) | 42 (11.38) | |
| 2 | 0 (0.00) | 327 (88.62) | |
| Preexisting maternal comorbidities | |||
| DM, n (%) | 2 (0.41) | 3 (0.81) | 1.0000 |
| HTN, n (%) | 1 (0.21) | 0 (0.00) | 0.6568 |
| CVD, n (%) | 0 (0.00) | 1 (0.27) | 0.4311 |
| DM/HTN/CVD, n (%) | 3 (0.62) | 4 (1.08) | 0.4722 |
| History of gestation | |||
| History of abnormal pregnancy, n (%) a | 68 (13.96) | 33 (8.94) | 0.0242 |
| History of preterm delivery, n (%) | 1 (0.21) | 1 (0.27) | 1.0000 |
| Unplanned pregnancy, n (%) | 32 (6.57) | 92 (24.93) | <0.0001 |
| Ways of getting pregnancy, n (%) | <0.0001 | ||
| Natural | 391 (80.29) | 350 (94.85) | |
| ART | 96 (19.71) | 19 (5.15) | |
| GDM, n (%) | 112 (23.00) | 82 (22.22) | 0.7883 |
| HDCP, n (%) | 27 (5.54) | 27 (7.32) | 0.2907 |
| PE, n (%) | 20 (4.11) | 15 (4.07) | 0.9756 |
| Hypothyroidism during pregnancy, n (%) | 29 (5.95) | 23 (6.23) | 0.8660 |
| Abnormality of placenta, n (%) b | 42 (8.62) | 29 (7.86) | 0.6877 |
| Unvaccinated | Vaccinated | p Value | |
|---|---|---|---|
| N = 487 | N = 369 | ||
| Female, n (%) | 245 (50.31) | 179 (48.51) | 0.6022 |
| Cesarean delivery, n (%) | 224 (46.00) | 156 (42.28) | 0.2781 |
| SGA, n (%) | 11 (2.26) | 12 (3.25) | 0.3734 |
| Preterm birth (<37 weeks), n (%) | 38 (7.80) | 35 (9.49) | 0.3828 |
| Very preterm birth (<32 weeks), n (%) | 7 (1.44) | 4 (1.08) | 0.7653 |
| LBW (<2500 g), n (%) | 35 (7.19) | 27 (7.32) | 0.9420 |
| VLBW (<1500 g), n (%) | 6 (1.23) | 3 (0.81) | 0.7393 |
| NICU admission, n (%) | 110 (22.59) | 81 (21.95) | 0.8248 |
| Neonatal bacterial infection, n (%) | 33 (6.78) | 22 (5.96) | 0.6305 |
| Mortality, n (%) | 0 | 0 | 1.0000 |
| Unvaccinated | Within 2 Month | Between 2~3 Month | |
|---|---|---|---|
| N = 487 | N = 184 | N = 185 | |
| Preterm | OR (95%CI) | OR (95%CI) | OR (95%CI) |
| Model 1 | 1.00 (Reference) | 1.52 (0.87, 2.67) | 0.97 (0.51, 1.83) |
| Model 2 | 1.00 (Reference) | 1.62 (0.92, 2.88) | 0.99 (0.52, 1.88) |
| Model 3 | 1.00 (Reference) | 1.72 (0.94, 3.13) | 1.03 (0.53, 2.01) |
| SGA | |||
| Model 1 | 1.00 (Reference) | 1.21 (0.41, 3.53) | 1.70 (0.65, 4.46) |
| Model 2 | 1.00 (Reference) | 1.28 (0.44, 3.75) | 1.75 (0.66, 4.63) |
| Model 3 | 1.00 (Reference) | 1.68 (0.54, 5.17) | 2.35 (0.84, 6.60) |
| NICU admission | |||
| Model 1 | 1.00 (Reference) | 0.95 (0.63, 1.43) | 0.98 (0.65, 1.47) |
| Model 2 | 1.00 (Reference) | 1.01 (0.66, 1.53) | 1.00 (0.66, 1.52) |
| Model 3 | 1.00 (Reference) | 1.04 (0.68, 1.60) | 1.03 (0.67, 1.59) |
| Unvaccinated | Sinopharm-BIBP | Sinovac-Coronavac | |
|---|---|---|---|
| N = 487 | N = 231 | N = 138 | |
| Preterm | |||
| Model 1 | 1.00 (Reference) | 1.50 (0.89, 2.53) | 0.82 (0.39, 1.75) |
| Model 2 | 1.00 (Reference) | 1.55 (0.91, 2.64) | 0.87 (0.41, 1.87) |
| Model 3 | 1.00 (Reference) | 1.64 (0.93, 2.88) | 0.89 (0.41, 1.96) |
| SGA | |||
| Model 1 | 1.00 (Reference) | 2.16 (0.92, 5.07) | 0.64 (0.14, 2.91) |
| Model 2 | 1.00 (Reference) | 2.24 (0.95, 5.28) | 0.67 (0.15, 3.09) |
| Model 3 | 1.00 (Reference) | 3.02 (1.20, 7.63) | 0.87 (0.18, 4.15) |
| NICU admission | |||
| Model 1 | 1.00 (Reference) | 1.02 (0.70, 1.48) | 0.87 (0.55, 1.39) |
| Model 2 | 1.00 (Reference) | 1.05 (0.72, 1.54) | 0.92 (0.57, 1.48) |
| Model 3 | 1.00 (Reference) | 1.09 (0.73, 1.61) | 0.95 (0.58, 1.55) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Mu, X.; Wang, X.; Zhang, L.; Liu, G.; Zheng, J.; Ding, F. Association of Maternal Inactivated COVID-19 Vaccination within 3 Months before Conception with Neonatal Outcomes. Vaccines 2023, 11, 1710. https://doi.org/10.3390/vaccines11111710
Chen Z, Mu X, Wang X, Zhang L, Liu G, Zheng J, Ding F. Association of Maternal Inactivated COVID-19 Vaccination within 3 Months before Conception with Neonatal Outcomes. Vaccines. 2023; 11(11):1710. https://doi.org/10.3390/vaccines11111710
Chicago/Turabian StyleChen, Zhihui, Xingbo Mu, Xinyan Wang, Lulu Zhang, Ge Liu, Jun Zheng, and Fangrui Ding. 2023. "Association of Maternal Inactivated COVID-19 Vaccination within 3 Months before Conception with Neonatal Outcomes" Vaccines 11, no. 11: 1710. https://doi.org/10.3390/vaccines11111710