
Parental Acceptance, Parental Hesitancy, and Uptake of Seasonal Influenza Vaccination among Children Aged 6–59 Months: A Systematic Review and Meta-Analysis
 , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
- (1)
- willing* OR accept* OR refus* OR hesitan* OR inten* OR reject* OR declin* OR uptake* OR factor* OR determinant* OR reason* OR facilitator* OR barrier* OR attitude* OR perception* OR view* OR predict* OR enabl* OR knowledge OR perspective*;
- (2)
- parent* OR guardian* OR caregiver*;
- (3)
- influenza OR flu;
- (4)
- vaccin* OR immuni*;
- (5)
- child* OR infant* OR toddler* OR pediatr* OR preschool* OR kindergart*;
- (6)
- 1 AND 2 AND 3 AND 4 AND 5.
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
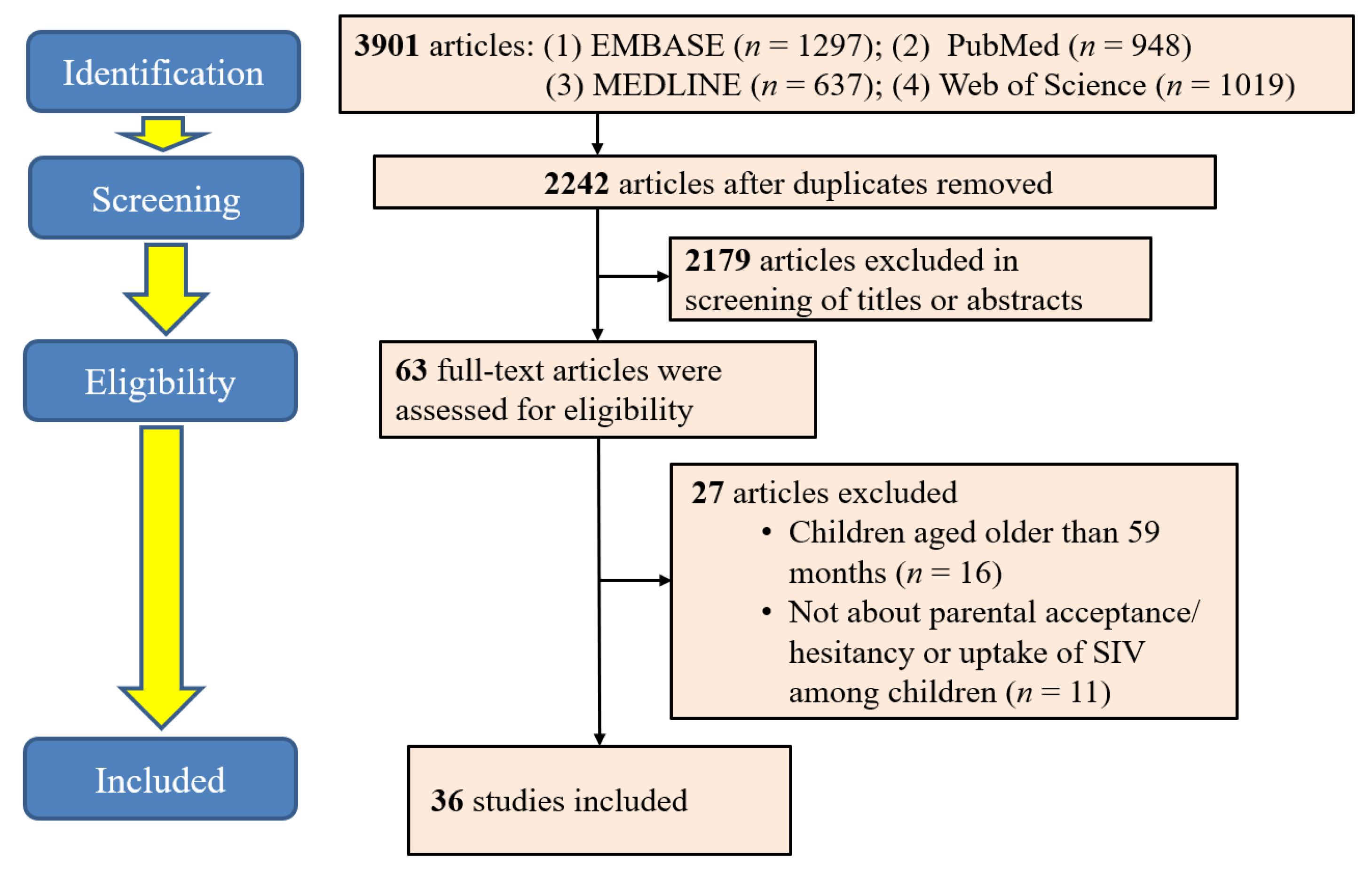
3.1. Identification of Studies
3.2. Overview of Included Studies
3.3. Primary Findings
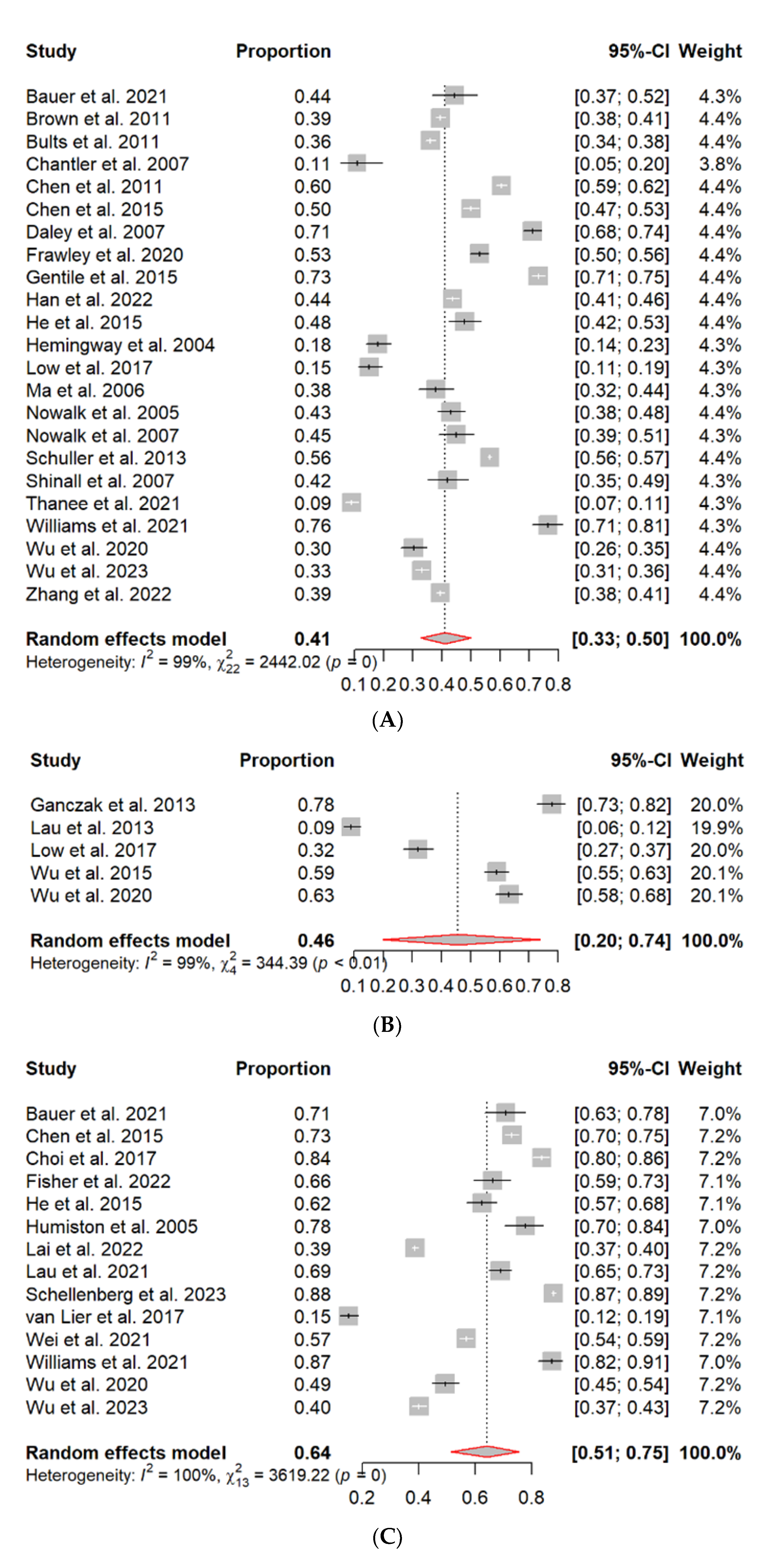
3.3.1. SIV Uptake in the Last Flu Season among Children Aged 6–59 Months
3.3.2. SIV Uptake in Lifetime among Children Aged 6–59 Months
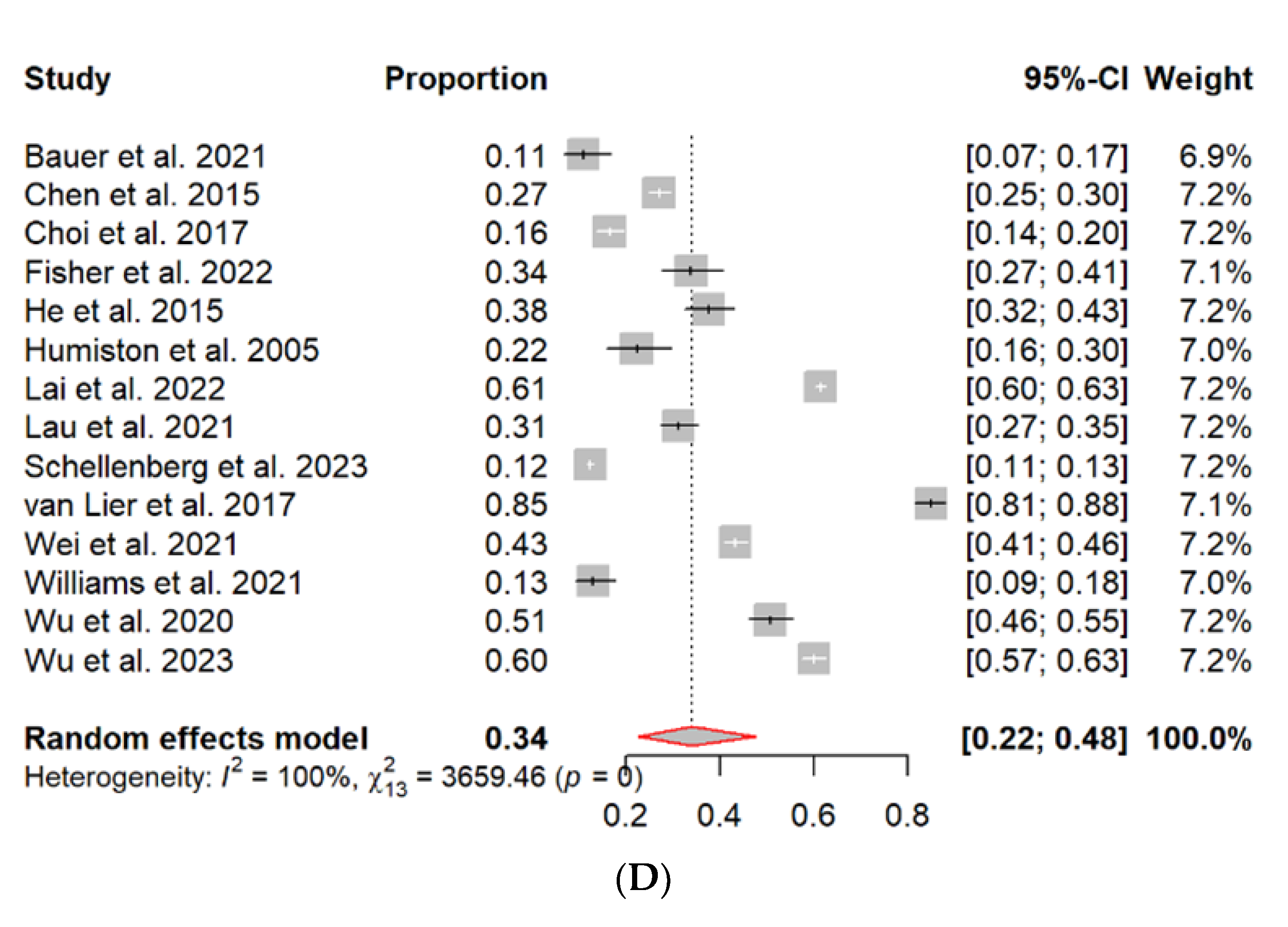
3.3.3. Parental Acceptance and Hesitancy of SIV
3.3.4. Factors Associated with Parental Acceptance/Hesitancy of SIV, and SIV Uptake in Children Aged 6–59 Months
3.3.5. Parental Attitudes and Perceptions of SIV
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Influenza vaccines: Vaccins antigrippaux. Wkly. Epidemiol. Rec. 2005, 33, 279–287. [Google Scholar]
- Willis, G.A.; Preen, D.B.; Richmond, P.C.; Jacoby, P.; Effler, P.V.; Smith, D.W.; Robins, C.; Borland, M.L.; Levy, A.; Keil, A.D.; et al. The impact of influenza infection on young children, their family and the health care system. Influ. Other Respir. Viruses 2018, 13, 18–27. [Google Scholar] [CrossRef] [Green Version]
- Lafond, K.E.; Nair, H.; Rasooly, M.H.; Valente, F.; Booy, R.; Rahman, M.; Kitsutani, P.; Yu, H.; Guzman, G.; Coulibaly, D.; et al. Global Role and Burden of Influenza in Pediatric Respiratory Hospitalizations, 1982–2012: A Systematic Analysis. PLoS Med. 2016, 13, e1002060. [Google Scholar] [CrossRef] [Green Version]
- Nair, H.; Brooks, W.A.; Katz, M.; Roca, A.; Berkley, J.A.; Madhi, S.A.; Simmerman, J.M.; Gordon, A.; Sato, M.; Howie, S.; et al. Global burden of respiratory infections due to seasonal influenza in young children: A systematic review and meta-analysis. Lancet 2011, 378, 1917–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brotherton, J.; Wang, H.; Schaffer, A.; Quinn, H.; Menzies, R.; Hull, B.; Lawrence, G.; Wood, J.; Wood, N.; Rosewell, A.; et al. Vaccine preventable disease and vaccination coverage in Australia 2003 to 2005. Commuity Dis. Intellance 2007, 31 (Suppl. S1), S1–S152. [Google Scholar]
- Centers for Disease Control and Prevention. Update: Influenza activity—United States, 2009–10 season. Morb. Mortal. Wkly. Rep. 2010, 59, 901–908. [Google Scholar]
- Mantel, C.; Chu, S.Y.; Hyde, T.B.; Lambach, P. Seasonal influenza vaccination in middle-income countries: Assessment of immunization practices in Belarus, Morocco, and Thailand. Vaccine 2019, 38, 212–219. [Google Scholar] [CrossRef]
- Harper, S.A.; Bradley, J.S.; Englund, J.A.; File, T.M.; Gravenstein, S.; Hayden, F.G.; McGeer, A.J.; Neuzil, K.M.; Pavia, A.T.; Tapper, M.L.; et al. Seasonal Influenza in Adults and Children-Diagnosis, Treatment, Chemoprophylaxis, and Institutional Outbreak Management: Clinical Practice Guidelines of the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 48, 1003–1032. [Google Scholar] [CrossRef]
- Hurwitz, E.S.; Haber, M.; Chang, A.; Shope, T.; Teo, S.; Ginsberg, M.; Waecker, N.; Nancy, J.C. Effectiveness of influenza vaccination of day care children in reducing influenza-related morbidity among household contacts. JAMA J. Am. Med. Assoc. 2000, 284, 1677–1682. [Google Scholar] [CrossRef] [Green Version]
- Moreno, J.; De Hoz, F.; Rico, A.; Cotes, K.; Porras, A. Vaccine effectiveness against influenza: Meta analysis literature. Biomédica 2009, 29, 87–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shono, A.; Kondo, M. Factors associated with seasonal influenza vaccine uptake among children in Japan. BMC Infect. Dis. 2015, 15, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Vaccines against influenza WHO position paper. Wkly. Epidemiol. Rec. 2012, 87, 461–476. [Google Scholar]
- Fisher, W.A.; Gilca, V.; Murti, M.; Orth, A.; Garfield, H.; Roumeliotis, P.; Rampakakis, E.; Brown, V.; Yaremko, J.; Buynder, B.V.; et al. Parental Attitudes and Perceptions of Support after Brief Clinician Intervention Predict Intentions to Accept the Adjuvanted Seasonal Influenza Vaccination: Findings from the Pediatric Influenza Vaccination Optimization Trial (PIVOT)-I. Vaccines 2022, 10, 1957. [Google Scholar] [CrossRef]
- Zhang, H.; Ren, X.; Tian, K.; Yu, J.; Zhu, A.; Zhang, L.; Gao, G.; Li, Z. The Impact and Vaccination Coverage of Seasonal Influenza among Children Aged 6–59 Months in China in 2017–2018: An Internet Panel Survey. Vaccines 2022, 10, 630. [Google Scholar] [CrossRef]
- Frawley, J.E.; McManus, K.; McIntyre, E.; Seale, H.; Sullivan, E. Uptake of funded influenza vaccines in young Australian children in 2018; parental characteristics, information seeking and attitudes. Vaccine 2020, 38, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Sun, X.; Yang, Y.; Zhan, S.; Fu, C. Seasonal influenza vaccine hesitancy profiles and determinants among Chinese children’s guardians and the elderly. Expert Rev. Vaccines 2021, 20, 601–610. [Google Scholar] [CrossRef]
- van Lier, A.; Ferreira, J.A.; Mollema, L.; Sanders, E.A.; de Melker, H.E. Intention to vaccinate universally against varicella, rotavirus gastroenteritis, meningococcal B disease and seasonal influenza among parents in the Netherlands: An internet survey. BMC Res. Notes 2017, 10, 672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Wei, Z.; Yang, Y.; Sun, X.; Zhan, S.; Jiang, Q.; Fu, C. Gap between cognitions and behaviors among children’s guardians of influenza vaccination: The role of social influence and vaccine-related knowledge. Hum. Vaccines Immunother. 2023, 19, 2166285. [Google Scholar] [CrossRef] [PubMed]
- Thanee, C.; Kittikraisak, W.; Sinthuwattanawibool, C.; Roekworachai, K.; Klinklom, A.; Kornsitthikul, K.; Jirasakpisarn, S.; Srirompotong, U.; Chittaganpitch, M.; Dawood, F.S.; et al. Knowledge, attitude/perception, and practice related to seasonal influenza vaccination among caregivers of young Thai children: A cross-sectional study. PLoS ONE 2021, 16, e0253561. [Google Scholar] [CrossRef]
- Nowalk, M.P.; Lin, C.J.; Zimmerman, R.K.; Ko, F.S.; Hoberman, A.; Raymund, M.; Kearney, D.H.; Greenberg, D.P. Changes in parents’ perceptions of infant influenza vaccination over two years. J. Natl. Med. Assoc. 2007, 99, 636–641. [Google Scholar] [PubMed]
- Imburgia, T.M.; Hendrix, K.S.; Donahue, K.L.; Sturm, L.A.; Zimet, G.D. Predictors of influenza vaccination in the U.S. among children 9–13 years of age. Vaccine 2017, 35, 2338–2342. [Google Scholar] [CrossRef]
- Lau, J.T.F.; Mo, P.K.H.; Cai, Y.S.; Tsui, H.Y.; Choi, K.C. Coverage and parental perceptions of influenza vaccination among parents of children aged 6 to 23 months in Hong Kong. BMC Public Health 2013, 13, 1026. [Google Scholar] [CrossRef] [Green Version]
- Wu, A.M.S.; Lau, J.T.F.; Ma, Y.L.; Lau, M.M.C. Prevalence and associated factors of seasonal influenza vaccination among 24-to 59-month-old children in Hong Kong. Vaccine 2015, 33, 3556–3561. [Google Scholar] [CrossRef]
- Wu, A.M.S.; Lau, J.T.F.; Ma, Y.L.; Cheng, K.M.; Lau, M.M.C. A longitudinal study using parental cognitions based on the theory of planned behavior to predict childhood influenza vaccination. J. Infect. Public Health 2020, 13, 970–979. [Google Scholar] [CrossRef]
- Bauer, K.E.; Agruss, J.C.; Mayefsky, J.H. Partnering with parents to remove barriers and improve influenza immunization rates for young children. J. Am. Assoc. Nurse Pract. 2021, 33, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Biezen, R.; Grando, D.; Mazza, D.; Brijnath, B. Why do we not want to recommend influenza vaccination to young children? A qualitative study of Australian parents and primary care providers. Vaccine 2018, 36, 859–865. [Google Scholar] [CrossRef]
- Daley, M.F.; Crane, L.A.; Chandramouli, V.; Beaty, B.L.; Barrow, J.; Allred, N.; Berman, S.; Kempe, A. Misperceptions about influenza vaccination among parents of healthy young children. Clin. Pediatr. 2007, 46, 408–417. [Google Scholar] [CrossRef]
- Smith, L.E.; Amlot, R.; Weinman, J.; Yiend, J.; Rubin, G.J. A systematic review of factors affecting vaccine uptake in young children. Vaccine 2017, 35, 6059–6069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.S. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Rev. Esp. Nutr. Hum. Die. 2016, 20, 148–160. [Google Scholar] [CrossRef] [Green Version]
- Pace, R.; Pluye, P.; Bartlett, G.; Macaulay, A.C.; Salsberg, J.; Jagosh, J.; Seller, R. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int. J. Nurs. Stud. 2012, 49, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.; Clayton-Boswell, H.; Chaves, S.S.; Prill, M.M.; Iwane, M.K.; Szilagyi, P.G.; Edwards, K.M.; Staat, M.A.; Weinberg, G.A.; Fairbrother, G.; et al. Validity of parental report of influenza vaccination in young children seeking medical care. Vaccine 2011, 29, 9488–9492. [Google Scholar] [CrossRef]
- Bults, M.; Beaujean, D.J.M.A.; Richardus, J.H.; van Steenbergen, J.E.; Voeten, H.A.C.M. Pandemic influenza A (H1N1) vaccination in The Netherlands: Parental reasoning underlying child vaccination choices. Vaccine 2011, 29, 6226–6235. [Google Scholar] [CrossRef] [PubMed]
- Chantler, T.; Pace, D.; Wright, A.; Pollard, A.J.; Yu, L.M.; Nguyen-Van-Tam, J.S.; MacDonald, N. Uptake and acceptability of influenza vaccination in day nursery children. Community Pract. 2007, 80, 32–36. [Google Scholar]
- Chen, M.F.; Wang, R.H.; Schneider, J.K.; Tsai, C.T.; Jiang, D.D.S.; Hung, M.N.; Lin, L.J. Using the Health Belief Model to Understand Caregiver Factors Influencing Childhood Influenza Vaccinations. J. Community Health Nurs. 2011, 28, 29–40. [Google Scholar] [CrossRef]
- Chen, C.H.; Chiu, P.J.; Chih, Y.C.; Yeh, G.L. Determinants of influenza vaccination among young Taiwanese children. Vaccine 2015, 33, 1993–1998. [Google Scholar] [CrossRef]
- Choi, A.; Kim, D.H.; Kim, Y.K.; Eun, B.W.; Jo, D.S. The impact of an educational intervention on parents’ decisions to vaccinate their <60-monthold children against influenza. Korean J. Pediatr. 2017, 60, 254–260. [Google Scholar]
- Ganczak, M.; Dmytrzyk-Daniłów, G.; Karakiewicz, B.; Korzeń, M.; Szych, Z. Determinants influencing self-paid vaccination coverage, in 0-5 years old Polish children. Vaccine 2013, 31, 5687–5692. [Google Scholar] [CrossRef]
- Gentile, A.; Juárez, M.; Hernandez, S.; Moya, A.; Bakir, J.; Lucion, M. Influenza vaccine: Delayed vaccination schedules and missed opportunities in children under 2 years old. Vaccine 2015, 33, 3913–3917. [Google Scholar] [CrossRef]
- Han, K.; Hou, Z.; Tu, S.; Wang, Q.; Hu, S.; Xing, Y.; Du, J.; Zang, S.; Chantler, T.; Larson, H. Childhood Influenza Vaccination and Its Determinants during 2020-2021 Flu Seasons in China: A Cross-Sectional Survey. Vaccines 2022, 10, 1994. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Liao, Q.Y.; Huang, Y.Q.; Feng, S.; Zhuang, X.M. Parents’ Perception and their Decision on their Children’s Vaccination Against Seasonal Influenza in Guangzhou. Chin. Med. J. 2015, 128, 327–341. [Google Scholar] [CrossRef] [PubMed]
- Hemingway, C.O.; Poehling, K.A. Change in recommendation affects influenza vaccinations among children 6 to 59 months of age. Pediatrics 2004, 114, 948–952. [Google Scholar] [CrossRef]
- Humiston, S.G.; Lerner, E.; Hepworth, E.; Blythe, T.; Goepp, J.G. Parent opinions about universal influenza vaccination for infants and toddlers. Arch. Pediatr. Adolesc. Med. 2005, 159, 108–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, X.; Li, M.; Hou, Z.; Guo, J.; Zhang, H.; Wang, J.; Fang, H. Factors associated with caregivers’ hesitancy to vaccinate children against influenza: A cross-sectional survey in China. Vaccine 2022, 40, 3975–3983. [Google Scholar] [CrossRef]
- Lau, J.T.; Wu, A.M.; Ma, Y.L.; Lau, M.M. Associated Factors of Behavioral Intention Regarding Childhood Influenza Vaccination Among Parents of Ever-Vaccinated and Never-Vaccinated 24-to 59-Month-Old Children in Hong Kong. Asia Pac. J. Public Health 2021, 33, 262–272. [Google Scholar] [CrossRef]
- Low, M.S.; Tan, H.; Hartman, M.; Tam, C.C.; Hoo, C.; Lim, J.; Chiow, S.; Lee, S.; Thing, R.; Cai, M.; et al. Parental perceptions of childhood seasonal influenza vaccination in Singapore: A cross-sectional survey. Vaccine 2017, 35, 6096–6102. [Google Scholar] [CrossRef]
- Ma, K.K.; Schaffner, W.; Colmenares, C.; Howser, J.; Jones, J.; Poehling, K.A. Influenza vaccinations of young children increased with media coverage in 2003. Pediatrics 2006, 117, E157–E163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowalk, M.P.; Zimmerman, R.K.; Lin, C.J.; Ko, F.S.; Raymund, M.; Hoberman, A.; Kearney, D.H.; Greenberg, D.P. Parental perspectives on influenza immunization of children aged 6 to 23 months. Am. J. Prev. Med. 2005, 29, 210–214. [Google Scholar] [CrossRef]
- Price, T.; McColl, E.; Visram, S. Barriers and facilitators of childhood flu vaccination: The views of parents in North East England. J. Public Health 2022, 30, 2619–2626. [Google Scholar] [CrossRef]
- Schuller, K.A.; Probst, J.C. Factors associated with influenza vaccination among US children in 2008. J. Infect. Public Health 2013, 6, 80–88. [Google Scholar] [CrossRef] [Green Version]
- Schellenberg, N.; Petrucka, P.; Dietrich Leurer, M.; Crizzle, A.M. Determinants of vaccine refusal, delay and reluctance in parents of 2-year-old children in Canada: Findings from the 2017 Childhood National Immunization Coverage Survey (cNICS). Travel Med. Infect. Dis. 2023, 53, 102584. [Google Scholar] [CrossRef]
- Shinall, M.C.; Plosa, E.J.; Poehling, K.A. Validity of parental report of influenza vaccination in children 6 to 59 months of age. Pediatrics 2007, 120, e783–e787. [Google Scholar] [CrossRef]
- Williams, J.T.; Rice, J.D.; Lou, Y.; Soderborg, T.K.; Bayliss, E.A.; Federico, S.G.; Hambidge, S.J.; O’Leary, S.T. Parental Vaccine Hesitancy and Risk of Pediatric Influenza Under-Vaccination in a Safety-Net Health Care System. Acad Pediatr. 2021, 21, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.E.; Webster, R.K.; Weinman, J.; Amlot, R.; Yiend, J.; Rubin, G.J. Psychological factors associated with uptake of the childhood influenza vaccine and perception of post-vaccination side-effects: A cross-sectional survey in England. Vaccine 2017, 35, 1936–1945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, Y.; Santibanez, T.A.; Kahn, K.E.; Srivastav, A. Parental-Reported Full Influenza Vaccination Coverage of Children in the US. Am. J. Prev. Med. 2017, 52, e103–e113. [Google Scholar] [CrossRef] [Green Version]
- Grohskopf, L.A.; Blanton, L.H.; Ferdinands, J.M.; Chung, J.R.; Broder, K.R.; Talbot, H.K.; Morgan, R.L.; Fry, A.M. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022–23 Influenza Season. Mmwr-Morb. Mortal. W. 2022, 71, 1–32. [Google Scholar] [CrossRef]
- Government of Canada. Public Funding for Influenza Vaccination by Province/Territory (as of June 2023). Available online: https://www.canada.ca/en/public-health/services/provincial-territorial-immunization-information/public-funding-influenza-vaccination-province-territory.html (accessed on 15 May 2023).
- Mcleroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An Ecological Perspective on Health Promotion Programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Wang, Z.; Fang, Y.; Chan, P.S.F.; Chidgey, A.; Fong, F.; Ip, M.; Lau, J.T. Effectiveness of a Community-Based Organization-Private Clinic Service Model in Promoting Human Papillomavirus Vaccination among Chinese Men Who Have Sex with Men. Vaccines 2021, 9, 1218. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.S.F.; Fang, Y.; Chidgey, A.; Fong, F.; Ip, M.; Wang, Z. Would Chinese Men Who Have Sex With Men Take Up Human Papillomavirus (HPV) Screening as an Alternative Prevention Strategy to HPV Vaccination? Front. Med. 2022, 9, 904873. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; Sharma, M.; Lee, R.C. Designing and Evaluating a Health Belief Model-Based Intervention to Increase Intent of Hpv Vaccination among College Males. Int. Q. Community Health Educ. 2014, 34, 101–117. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.H.; Tang, J.; Zhang, J.J.; Wu, Q.S. Impact of the coronavirus disease 2019 epidemic and a free influenza vaccine strategy on the willingness of residents to receive influenza vaccines in Shanghai, China. Hum. Vaccines Immunother. 2021, 17, 2289–2292. [Google Scholar] [CrossRef] [PubMed]
- Seiler, M.; Goldman, R.D.; Staubli, G.; Hoeffe, J.; Gualco, G.; Manzano, S. Parents’ intent to vaccinate against influenza during the COVID-19 pandemic in two regions in Switzerland. Swiss Med. Wkly. 2021, 151, w20508. [Google Scholar] [CrossRef] [PubMed]
- Salawati, E.; Alwafi, H.; Samannodi, M.; Minshawi, F.; Gari, A.; Abualnaja, S.; Almatrafi, M.A. Parents’ Willingness to Vaccinate Their Children Against Seasonal Influenza After the COVID-19 Pandemic in Saudi Arabia: A Retrospective Cross-Sectional Survey. Patient Prefer. Adherence 2021, 15, 2821–2835. [Google Scholar] [CrossRef]
- Pandolfi, E.; Marino, M.G.; Carloni, E.; Romano, M.; Gesualdo, F.; Borgia Pcarloni, R.; Guarino, A.; Giannattasio, A.; Tozzi, A.E. The effect of physician’s recommendation on seasonal influenza immunization in children with chronic diseases. BMC Public Health 2012, 12, 984. [Google Scholar] [CrossRef] [Green Version]
- Norman, D.A.; Barnes, R.; Pavlos, R.; Bhuiyan, M.; Alene, K.A.; Danchin, M.; Seale, H.; Moore, H.C.; Blyth, C.C. Improving Influenza Vaccination in Children With Comorbidities: A Systematic Review. Pediatrics 2021, 147, e20201433. [Google Scholar] [CrossRef]
- Ryan, G. Challenges to Adolescent HPV Vaccination and Implementation of Evidence-Based Interventions to Promote Vaccine Uptake During the COVID-19 Pandemic: “HPV Is Probably Not at the Top of Our List”. Prev. Chronic Dis. 2022, 19, E15. [Google Scholar] [CrossRef] [PubMed]
- Balogun, M.; Banke-Thomas, A.; Gwacham-Anisiobi, U.; Yesufu, V.; Ubani, O.; Afolabi, B.B. Actions and Adaptations Implemented for Maternal, Newborn and Child Health Service Provision During the Early Phase of the COVID-19 Pandemic in Lagos, Nigeria: Qualitative Study of Health Facility Leaders. Ann. Glob. Health 2022, 88, 1–14. [Google Scholar] [CrossRef]
- Kazi, A.M.; Ahsan, N.; Mughis, W.; Jamal, S.; Allana, R.; Raza, M.; Muneer, S.; Mughal, M.A.; Kaleemuddin, H.; Sameen, F.; et al. Usability and Acceptability of a Mobile App for Behavior Change and to Improve Immunization Coverage among Children in Pakistan: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 9527. [Google Scholar] [CrossRef]
- Murthy, S.; Sawant, M.; Doreswamy, S.S.; Pothula, S.C.; Yan, S.D.; Pathani, T.S.; Thakur, D.; Rajarama Sastry Vemuri, S.; Upadhyaya, S.; Alam, S.; et al. Supporting Immunization Uptake during a Pandemic, Using Remote Phone Call Intervention among Babies Discharged from a Special Neonatal Care Unit (SNCU) in South India. Vaccines 2022, 10, 507. [Google Scholar] [CrossRef]
- Kovar, C.L.; Pestaner, M.; Corbett, R.W.; Rose, C.L. HPV vaccine promotion: Snapshot of two health departments during the COVID-19 pandemic. Public Health Nurs. 2021, 38, 715–719. [Google Scholar] [CrossRef]
- Khader, Y.S.; Maalouf, W.; Khdair, M.A.; Al-Nsour, M.; Aga, E.; Khalifa, A.; Kassasbeh, M.; El-Halabi, S.; Alfven, T.; El-Khatib, Z. Scaling the Children Immunization App (CIMA) to Support Child Refugees and Parents in the Time of the COVID-19 Pandemic: A Social Capital Approach to Scale a Smartphone Application in Zaatari Camp, Jordan. J. Epidemiol. Glob. Health 2022, 12, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.J.; Piao, M.; Kim, J.; Lee, J.H. Development and Evaluation of a Child Vaccination Chatbot Real-Time Consultation Messenger Service during the COVID-19 Pandemic. Appl. Sci. 2021, 11, 12142. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Study Year | Country/ Region | Study Design | Sample Size | Age of the Children | Uptake in the Last Flu Season/Uptake in Lifetime/Acceptance/Hesitancy | Key Findings |
|---|---|---|---|---|---|---|---|
| Bauer et al., 2021 [26] | 2018 | USA | Quantitative: cross-sectional survey | 165 | 6–24 months | Uptake in the last flu season: 44% Acceptance: 71% Hesitancy: 11% | Uptake in the last flu season
|
| Biezen et al., 2018 [27] | 2015 | Australia | Qualitative: focus group | 50 | 6–59 months | NA |
|
| Brown et al., 2011 [32] | 2007 | USA | Quantitative: cross-sectional survey | 3072 | 6–59 months | Uptake in the last flu season: 39.5% | Uptake in the last flu season
|
| Bults et al., 2011 [33] | 2009 | The Netherlands | Quantitative: cross-sectional survey | 3127 | 6–59 months | Uptake in the last flu season: 36% | Uptake in the last flu season
|
| Chantler et al., 2007 [34] | 2005 | UK | Mixed-method: Semi-structured interview and cross-sectional survey | Semi-structured interview: 10 Survey: 83 | 6–23 months | Uptake in the last flu season: 11% | Uptake in the last flu season
|
| Chen et al., 2011 [35] | 2009 | Taiwan | Quantitative: cross-sectional survey | 2778 | 6–36 months | Uptake in the last flu season: 60.4% | Uptake in the last flu season
|
| Chen et al., 2015 [36] | 2011 | Taiwan | Quantitative: cross-sectional survey | 1300 | 6–36 months | Uptake in the last flu season: 50% Acceptance: 73% Hesitancy: 27% | Acceptance
|
| Choi et al., 2017 [37] | 2015 | Republic of Korea | Quantitative: cross-sectional survey | 639 | <60 months | Acceptance: 83.6% Hesitancy: 16.4% | Acceptance:
|
| Daley et al., 2007 [28] | 2004 | USA | Quantitative: cross-sectional survey | 839 | 6–21 months | Uptake in the last flu season: 71% | Uptake in the last flu season
|
| Fisher et al., 2022 [14] | 2016 | Canada | Quantitative: cross-sectional survey | 207 | 6–23 months | Acceptance: 66% Hesitancy: 34% | Acceptance
|
| Frawley et al., 2020 [16] | 2018 | Australia | Quantitative: cross-sectional survey | 1002 | 6–59 months | Uptake in the last flu season: 52.9% | Uptake in the last flu season
|
| Ganczak et al., 2013 [38] | 2010 | Poland | Quantitative: cross-sectional survey | 308 | 6–59 months | Uptake in lifetime: 77.9% | Uptake in lifetime
|
| Gentile et al., 2015 [39] | 2013 | Argentina | Quantitative: cross-sectional survey | 1350 | 6–24 months | Uptake in the last flu season: 73.1% | Uptake in the last flu season
|
| Han et al., 2022 [40] | 2021 | China | Quantitative: cross-sectional survey | 2081 | <5 years | Uptake in the last flu season: 43.63% | Uptake in the last flu season
|
| He et al., 2015 [41] | 2013 | China | Quantitative: cross-sectional survey | 335 | 6–36 months | Uptake in the last flu season: 47.7% Acceptance: 62.4% Hesitancy: 37.6% | Uptake in the last flu season
|
| Hemingway et al., 2004 [42] | 2003 | USA | Quantitative: cross-sectional survey | 329 | 6–59 months | Uptake in the last flu season: 18% | Uptake in the last flu season
|
| Humiston et al., 2005 [43] | 2004 | USA | Quantitative: cross-sectional survey | 153 | 6–23 months | Acceptance: 78% Hesitancy: 22% | Acceptance
|
| Lai et al., 2022 [44] | 2019 | China | Quantitative: cross-sectional survey | 6668 | 6–59 months | Acceptance: 38.6% Hesitancy: 61.4% | Hesitancy
|
| Lau et al., 2021 [45] | 2011 | Hong Kong | Quantitative: cross-sectional survey | 540 | 24–59 months | Acceptance: 68.9% Hesitancy: 31.1% | Acceptance
|
| Lau et al., 2013 [23] | 2006 | Hong Kong | Quantitative: cross-sectional survey | 401 | 6–23 months | Uptake in lifetime: 9% | Uptake in lifetime
|
| Low et al., 2017 [46] | 2016 | Singapore | Quantitative: cross-sectional survey | 332 | 6 months–5 years | Uptake in the last flu season: 15% Uptake in lifetime: 32% | Uptake in the last flu season
|
| Ma et al., 2006 [47] | 2004 | USA | Quantitative: cross-sectional survey | 256 | 6–59 months | Uptake in the last flu season: 38% | Uptake in the last flu season
|
| Nowalk et al., 2005 [48] | 2003 | USA | Quantitative: cross-sectional survey | 436 | 6–23 months | Uptake in the last flu season: 43.2% | Uptake in the last flu season
|
| Nowalk et al., 2007 [21] | 2004 | USA | Quantitative: cross-sectional survey | 274 | 6–23 months. | Uptake in the last flu season: 45% | Uptake in the last flu season
|
| Price et al.,, 2022 [49] | 2020 | UK | Qualitative: semi-structured interview | 12 | 2–3 years | NA |
|
| Schuller et al., 2013 [50] | 2008 | USA | Quantitative: cross-sectional survey | 25,256 | 19–35 months | Uptake in the last flu season: 56.4% | Uptake in the last flu season
|
| Schellenberg et al., 2023 [51] | 2018 | Canada | Quantitative: cross-sectional survey | 6125 | 24 months | Acceptance: 87.7% Hesitancy: 12.3% | Hesitancy
|
| Shinall et al., 2007 [52] | 2005 | USA | Quantitative: cross-sectional survey | 198 | 6–59 months | Uptake in the last flu season: 42% | Uptake in the last flu season
|
| Thanee et al., 2021 [20] | 2019 | Thailand | Quantitative: cross-sectional survey | 700 | 6–36 months | Uptake in the last flu season: 9% | Uptake in the last flu season
|
| van Lier et al., 2017 [18] | 2012 | The Netherlands | Quantitative: cross-sectional survey | 491 | 0–48 months | Acceptance: 15% Hesitancy: 85% | Acceptance
|
| Wei et al., 2021 [17] | China | Quantitative: cross-sectional survey | 1564 | 0–59 months | Acceptance: 56.8% Hesitancy: 43.2% | Hesitancy
| |
| Williams et al., 2021 [53] | 2020 | USA | Quantitative: cross-sectional survey | 263 | 2 years | Uptake in the last flu season: 76.5% Acceptance: 87% Hesitancy: 13% | Hesitancy
|
| Wu et al., 2015 [24] | 2011 | Hong Kong | Quantitative: cross-sectional survey | 540 | 24–59 months | Uptake in lifetime: 58.9% | Uptake in lifetime
|
| Wu et al., 2020 [25] | 2011 | Hong Kong | Quantitative: cross-sectional survey | 440 | 24–59 months | Uptake in the last flu season: 30.22% Uptake in lifetime: 63.2% Acceptance: 49.3% Hesitancy: 50.7% | Uptake in the last flu season
|
| Wu et al., 2023 [19] | 2019 | China | Quantitative: cross-sectional survey | 1404 | 0–59 months | Uptake in the last flu season: 33.1% Hesitancy: 40% Hesitancy: 60% | Uptake in the last flu season
|
| Zhang et al., 2022 [15] | 2018 | China | Quantitative: cross-sectional survey | 4719 | 6–59 months | Uptake in the last flu season: 39.4% | Uptake in the last flu season
|
| Author, Year | Country/Region | Sample Size | Uptake in the Last Flu Season | Uptake in Lifetime | Acceptance | Hesitancy | Associated Factors |
|---|---|---|---|---|---|---|---|
| Bauer et al., 2021 [26] | USA | 165 | 44% | - | 71% | 11% | - |
| Brown et al., 2011 [32] | USA | 3072 | 39.5% | - | - | - | - |
| Bults et al., 2011 [33] | The Netherlands | 3127 | 36% | - | - | - | Uptake in the last flu season: experienced feelings of doubt about the vaccination decision (−); information-seeking behaviour (−); social influence on their vaccination decision (+) |
| Chantler et al., 2007 [34] | UK | 83 | 11% | - | - | - | - |
| Chen et al., 2011 [35] | Taiwan | 2778 | 60.4% | - | - | - | Uptake in the last flu season: age of the caregiver (−); unemployed (+); living in rural areas (+); chronic disease (−); hospitalisation history (−); influenza histories of the child (+); perceived susceptibility (+)/perceived benefits of vaccinations (+); perceived barriers (−); cues to action (+) |
| Chen et al., 2015 [36] | Taiwan | 1300 | 50% | - | 73% | 27% | Uptake in the last flu season: age of the caregiver (+); female gender (−); average household income (−); being mother compared to father(−); being grandfather compared to father (+); influenza vaccination of the children in the last year (+); children’s average frequency of cold per year (+); perceived benefits of the vaccination (+); cues to action (+); self-efficacy of childhood vaccination (+) |
| Choi et al., 2017 [37] | Republic of Korea | 639 | - | - | 83.6% | 16.4% | Uptake in the last flu season: household income (+); parental education level (+) |
| Daley et al., 2007 [28] | USA | 839 | 71% | - | - | - | Uptake in the past year: belief that IV is the social norm (+); perceived barriers (−) |
| Fisher et al., 2022 [14] | Canada | 207 | - | - | 66% | 34% | Acceptance: household income (+); perceived vaccine safety (+); perceived benefit (+); cues to action (+); perceived support from significant others (+) |
| Frawley et al., 2020 [16] | Australia | 1002 | 52.9% | - | - | - | Uptake in the last flu season: being mother (−); having a health care card (+); know the influenza vaccine was free for the child (+); a recommendation from a health professional (+) |
| Ganczak et al., 2013 [38] | Poland | 308 | - | 77.9% | - | - | Uptake in lifetime: age of the parent (+); socio-economic status (+); having only one child (+); health system factor, i.e., practice location (+); cost of a vaccine (−) |
| Gentile et al., 2015 [39] | Argentina | 1350 | 73.1% | - | - | - | Uptake in the last flu season: perceived importance of IV (+) |
| Han et al., 2022 [40] | China | 2081 | 43.6% | - | - | - | Uptake in the last flu season: parental education level (+); household income (−); confidence in the importance, safety, and effectiveness of influenza vaccine (+); knowing other caregivers were vaccinating their children (+); receiving positive influence from healthcare workers and family members (+); poor access, including conflicts between caregivers’ availability and vaccination service schedules and inconvenient transportation to the vaccination site (−) |
| He et al., 2015 [41] | China | 335 | 47.7% | - | 62.4% | 37.6% | Uptake in the last flu season: household income (+); age of the child (+); social norm (+); perceived control (+); perceived vaccine safety (+) Acceptance: household income (+); children with a history of taking SIV (+); perceived children’s health status (+); worry/anxious about their children influenza infection (+); perceived control (+); perceived vaccine safety (+); perceived benefit (+); social norm (+); perceived severity (+) |
| Hemingway et al., 2004 [42] | USA | 329 | 18% | - | - | - | Uptake in the last flu season: a physician’s recommendation (+); family members vaccinated (+) |
| Humiston et al., 2005 [43] | USA | 153 | - | - | 78% | 22% | Acceptance: perceived severity (+); perceived vaccine safety (+); perceived importance to vaccinate the child (+); parental education level (+) |
| Lai et al., 2022 [44] | China | 6668 | - | - | 38.6% | 61.4% | Hesitancy: perceiving importance to vaccinate the child (−); perceived vaccine safety (−); perceived vaccine efficacy (−); know children as a priority group (−); trusting vaccination advice from medical staff (−); perceived barriers (+); age of the child (−); the number of children in the family (−); caregivers’ age (−); parental education level (−); household income (+) |
| Lau et al., 2021 [45] | Hong Kong | 540 | - | - | 68.9% | 31.1% | Acceptance: being a mother (−); age of the child (−); positive influenza vaccination experience in family members (+); age of the parents (−); parental education level (+); perceived susceptibility (+); perceived benefit (+); perceived barrier (−); cue to action (+); subjective norm (+); having family members vaccinated (+) |
| Lau et al., 2013 [23] | Hong Kong | 401 | - | 9% | - | - | Uptake in lifetime: a physician’s recommendations (+); parental perceptions of the side effects of IV (−) |
| Low et al., 2017 [46] | Singapore | 332 | 15% | 32% | - | - | Uptake in the last flu season: a physician’s recommendation (+); the child was vaccinated before (+); willingness to vaccinate (+); feeling well-informed about influenza vaccine (+); receiving influenza vaccine information from television (−) |
| Ma et al., 2006 [47] | USA | 256 | 38% | - | - | - | Uptake in the last flu season: a physician’s recommendation (+); having a family member vaccinated (+); having a continuity clinic visit (+); having a high-risk medical condition (+) |
| Nowalk et al., 2005 [48] | USA | 436 | 43.2% | - | - | - | Uptake in the last flu season: a physician’s recommendation (+); relatives and friends think that child should have flu shot (+); the belief that a child with asthma should receive a flu shot (+); the belief that receiving an influenza shot is a smart idea (+); the belief that unvaccinated child will get flu (+); belief that flu shot prevents flu (+); worrying that child will get the flu from flu shot (−); belief that the flu shot is more trouble than it is worth (−) |
| Nowalk et al., 2007 [21] | USA | 274 | 45% | - | - | - | Uptake in the last flu season: a physician’s recommendation (+); receiving a reminder (+); the parental belief that the child should be vaccinated (+) |
| Schuller et al., 2013 [50] | USA | 25,256 | 56.4% | - | - | - | Uptake in the last flu season: age of the parent (+); married (+); parental education level (+); a child with private insurance (+); age of the child (+); first-born child (+); ethnicity: black (+); household income level (+) |
| Schellenberg et al., 2023 [51] | Canada | 6125 | - | - | 87.7% | 12.3% | Hesitancy: female parents (−); child had health issues (−); age of the child (−); knowledge, attitudes and belief (−) |
| Shinall et al., 2007 [52] | USA | 198 | 42% | - | - | - | Uptake in the last flu season: age of the child (−); child with chronic medical conditions (+) |
| Thanee et al., 2021 [20] | Thailand | 700 | 9% | - | - | - | Uptake in the last flu season: parental education level (+); knowledge about influenza illness (+); healthcare providers as a primary source of information about influenza illness for parents (+); parents’ strongly agreeing with the national recommendation for influenza vaccination in young children (+); using health insurance provided by the government or parent’s employer for children’s doctor visits (+); the children’s history of receiving influenza vaccination (+) |
| van Lier et al., 2017 [18] | The Netherlands | 491 | - | - | 15% | 85% | Acceptance: perceived importance of vaccination against the particular disease (+); the perception of whether or not the disease is severe enough to justify vaccination (+) |
| Wei et al., 2021 [17] | China | 1564 | - | - | 56.8% | 43.2% | Hesitancy: living in a rural area (+); do not know the government recommendation for flu vaccination (+); do not know the flu vaccine is vaccinated annually (+); family members, friends and neighbours had a positive attitude toward flu vaccine (−) |
| Williams et al., 2021 [53] | USA | 263 | 76.5% | - | 87% | 13% | Hesitancy: English-speaking (+); non-Latino race/ethnicity (+); non-publicly insured (+); born in the United States (+) |
| Wu et al., 2015 [24] | Hong Kong | 540 | - | 58.9% | - | - | Uptake in lifetime: family members vaccinated (+); perceived susceptibility of seasonal influenza (+); perceived benefits of IV (+); perceived barriers of IV (−); cue to action (+); supportive subjective norm (+) |
| Wu et al., 2020 [25] | Hong Kong | 440 | 30.2% | 63.2% | 49.3% | 50.7% | Uptake in the last flu season: caregivers being female (+); parental positive attitude (+); subjective norm (+); behavioral intention (+) Uptake in a lifetime: positive attitudes (e.g., belief that IV is effective) (+); perceived norm (+); negative attitudes (−) Acceptance: visiting doctor before (+); positive attitudes (+); perceived norm (+); parttime/unemployed (−); child’s uptake in the past year (+) |
| Wu et al., 2023 [19] | China | 1404 | 33.1% | - | 40.0% | 60.0% | Uptake in the last flu season: caregiver being male (+); the age of the parent (+); parental education level (+); perceived benefit (+); knowing that government recommends influenza vaccination (+); knowing that the influenza vaccine is recommended to be taken annually (+); those who reported that their communities promote influenza vaccination (+); with support of their family members, friends and neighbours, and HCWs (+); hesitancy (−) Hesitancy: relative knowledge (−); social influence (−) |
| Zhang et al., 2022 [15] | China | 4719 | 39.4% | - | - | - | Uptake in the last flu season: age of the child (+); living in Southern China (+) |
| Moderator | Number of Studies | Proportion of Outcome (95% CI) | Heterogeneity | Moderator Effect (Meta-Regression) | ||
|---|---|---|---|---|---|---|
| Univariate | ||||||
| I2 Within | p-Value | Coefficient | p-Value | |||
| Uptake in the last flu season | ||||||
| Study year | 0.01 | 0.87 | ||||
| 2010 or before | 11 | 0.41 (0.30–0.53) | 99% | <0.01 | ||
| 2011–2015 | 4 | 0.51 (0.33–0.68) | 99% | <0.01 | ||
| 2016–2019 | 6 | 0.29 (0.16–0.47) | 99% | <0.01 | ||
| 2020 or after | 2 | 0.61 (0.28–0.96) | 99% | <0.01 | ||
| Region | 0.03 | 0.61 | ||||
| Asia | 9 | 0.34 (0.23–0.48) | 99% | <0.01 | ||
| Americas | 11 | 0.50 (0.38–0.61) | 99% | <0.01 | ||
| Europe | 2 | 0.21 (0.06–0.55) | 95% | <0.01 | ||
| Oceania | 1 | 0.53 (0.50–0.56) | - | - | ||
| Sample size | 0.11 | 0.17 | ||||
| ≤1000 | 13 | 0.35 (0.23–0.49) | 99% | <0.01 | ||
| >1000 | 10 | 0.48 (0.40–0.57) | 99% | <0.01 | ||
| Uptake in lifetime | ||||||
| Study year | −0.02 | 0.91 | ||||
| 2010 or before | 2 | 0.37 (0.02–0.95) | 100% | <0.01 | ||
| 2011–2015 | 2 | 0.61 (0.57–0.65) | 47% | 0.17 | ||
| 2016–2019 | 1 | 0.32 (0.27–0.37) | - | - | ||
| Region | 0.19 | 0.28 | ||||
| Asia | 4 | 0.37 (0.14–0.68) | 99% | <0.01 | ||
| Americas | 0 | - | - | - | ||
| Europe | 1 | 0.78 (0.73–0.82) | - | - | ||
| Oceania | 0 | - | - | - | ||
| Sample size | - | - | ||||
| ≤1000 | 5 | 0.46 (0.20–0.74) | 99% | <0.01 | ||
| >1000 | 0 | - | - | - | ||
| Parental acceptance | ||||||
| Study year | 0.02 | 0.77 | ||||
| 2010 or before | 1 | 0.78 (0.70–0.84) | - | - | ||
| 2011–2015 | 6 | 0.59 (0.36–0.78) | 99% | <0.01 | ||
| 2016–2019 | 6 | 0.62 (0.44–0.77) | 100% | <0.01 | ||
| 2020 or after | 1 | 0.87 (0.82–0.91) | - | - | ||
| Region | 0.19 | 0.04 | ||||
| Asia | 8 | 0.60 (0.48–0.71) | 99% | <0.01 | ||
| Americas | 5 | 0.79 (0.70–0.87) | 96% | <0.01 | ||
| Europe | 1 | 0.15 (0.12–0.19) | - | - | ||
| Oceania | 0 | - | - | - | ||
| Sample size | −0.05 | 0.66 | ||||
| ≤1000 | 9 | 0.66 (0.49–0.79) | 99% | <0.01 | ||
| >1000 | 5 | 0.62 (0.40–0.80) | 100% | <0.01 | ||
| Parental hesitancy | ||||||
| Study year | −0.04 | 0.68 | ||||
| 2010 or before | 1 | 0.22 (0.16–0.30) | - | - | ||
| 2011–2015 | 6 | 0.41 (0.22–0.64) | 93% | <0.01 | ||
| 2016–2019 | 6 | 0.34 (0.17–0.55) | 100% | <0.01 | ||
| 2020 or after | 1 | 0.13 (0.09–0.18) | - | - | ||
| Region | 0.22 | 0.02 | ||||
| Asia | 8 | 0.40 (0.29–0.52) | 99% | <0.01 | ||
| Americas | 5 | 0.17 (0.11–0.26) | 95% | <0.01 | ||
| Europe | 1 | 0.85 (0.81–0.88) | - | - | ||
| Oceania | 0 | - | - | |||
| Sample size | 0.07 | 0.57 | ||||
| ≤1000 | 9 | 0.31 (0.18–0.50) | 99% | <0.01 | ||
| >1000 | 5 | 0.38 (0.20–0.60) | 100% | <0.01 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, P.S.-f.; Fang, Y.; Kawuki, J.; Chen, S.; Liang, X.; Mo, P.K.-h.; Wang, Z. Parental Acceptance, Parental Hesitancy, and Uptake of Seasonal Influenza Vaccination among Children Aged 6–59 Months: A Systematic Review and Meta-Analysis. Vaccines 2023, 11, 1360. https://doi.org/10.3390/vaccines11081360
Chan PS-f, Fang Y, Kawuki J, Chen S, Liang X, Mo PK-h, Wang Z. Parental Acceptance, Parental Hesitancy, and Uptake of Seasonal Influenza Vaccination among Children Aged 6–59 Months: A Systematic Review and Meta-Analysis. Vaccines. 2023; 11(8):1360. https://doi.org/10.3390/vaccines11081360
Chicago/Turabian StyleChan, Paul Shing-fong, Yuan Fang, Joseph Kawuki, Siyu Chen, Xue Liang, Phoenix Kit-han Mo, and Zixin Wang. 2023. "Parental Acceptance, Parental Hesitancy, and Uptake of Seasonal Influenza Vaccination among Children Aged 6–59 Months: A Systematic Review and Meta-Analysis" Vaccines 11, no. 8: 1360. https://doi.org/10.3390/vaccines11081360