
A Bibliometric Analysis of Melanoma Treated with Vaccinations Research from 2013 to 2023: A Comprehensive Review of the Literature

Abstract
:1. Introduction
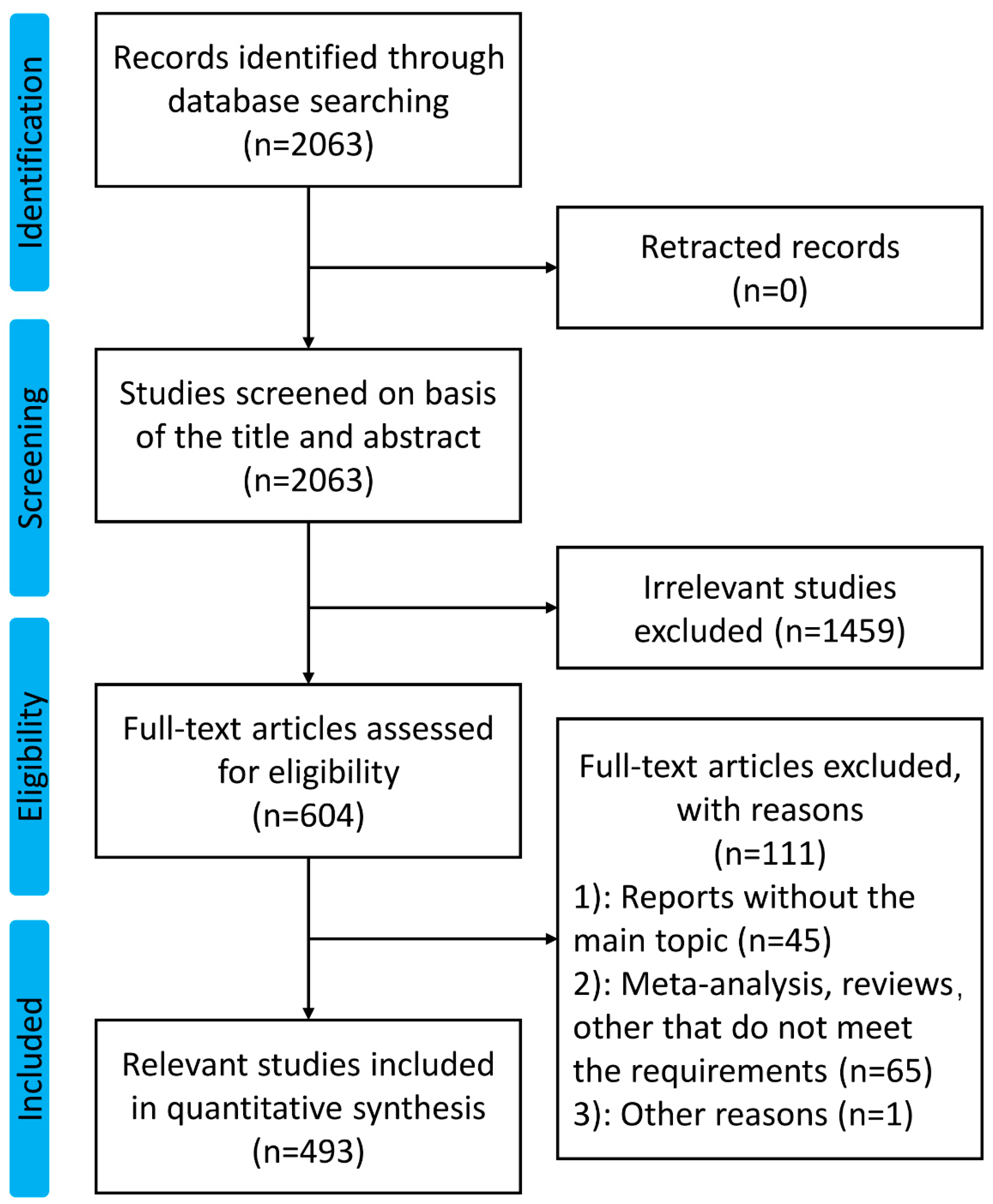
2. Methods
2.1. Data Collection and Data Extraction
2.2. Data Analysis and Visualization
3. Results
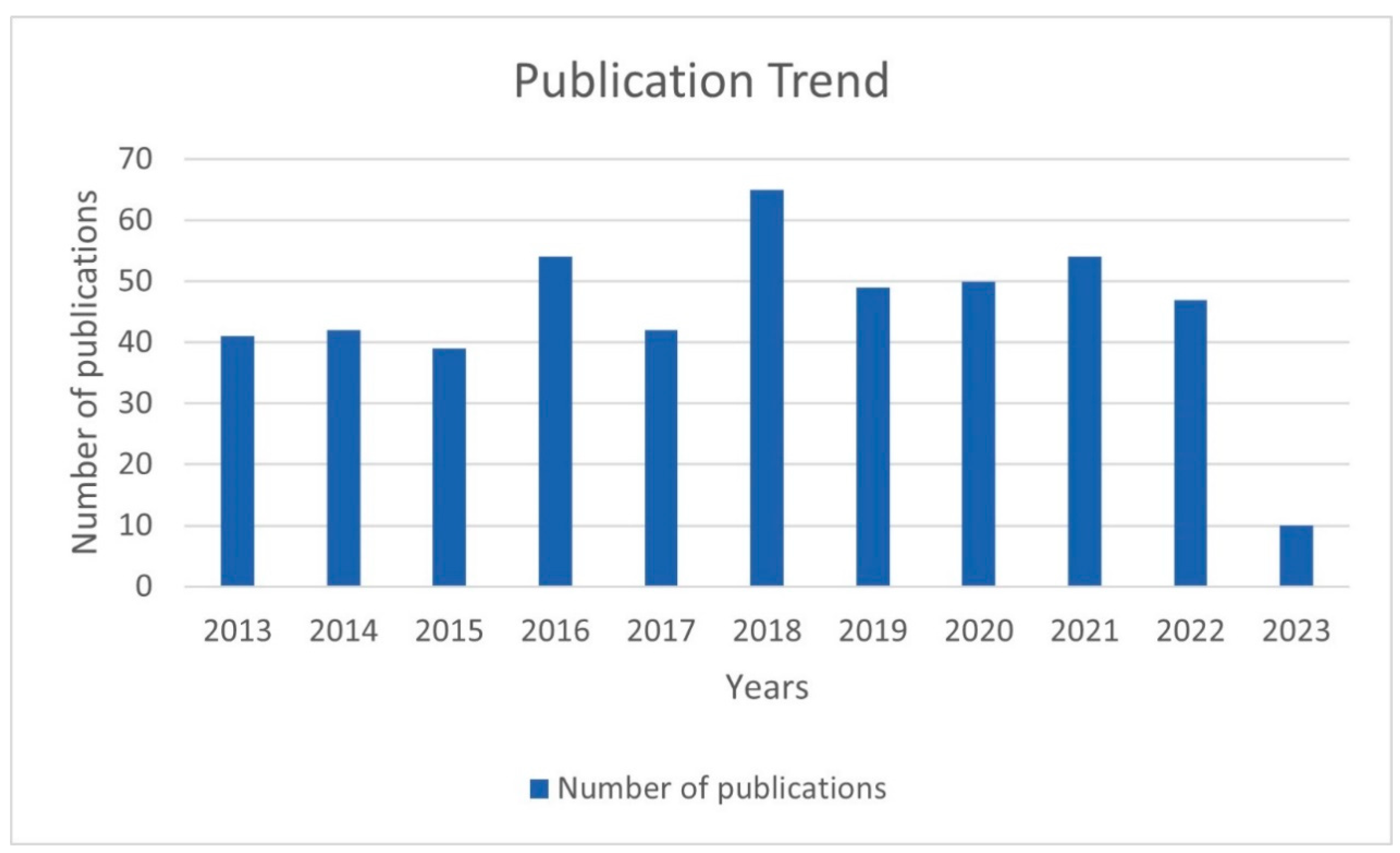
3.1. Publication Trend
3.2. Journals of Publication
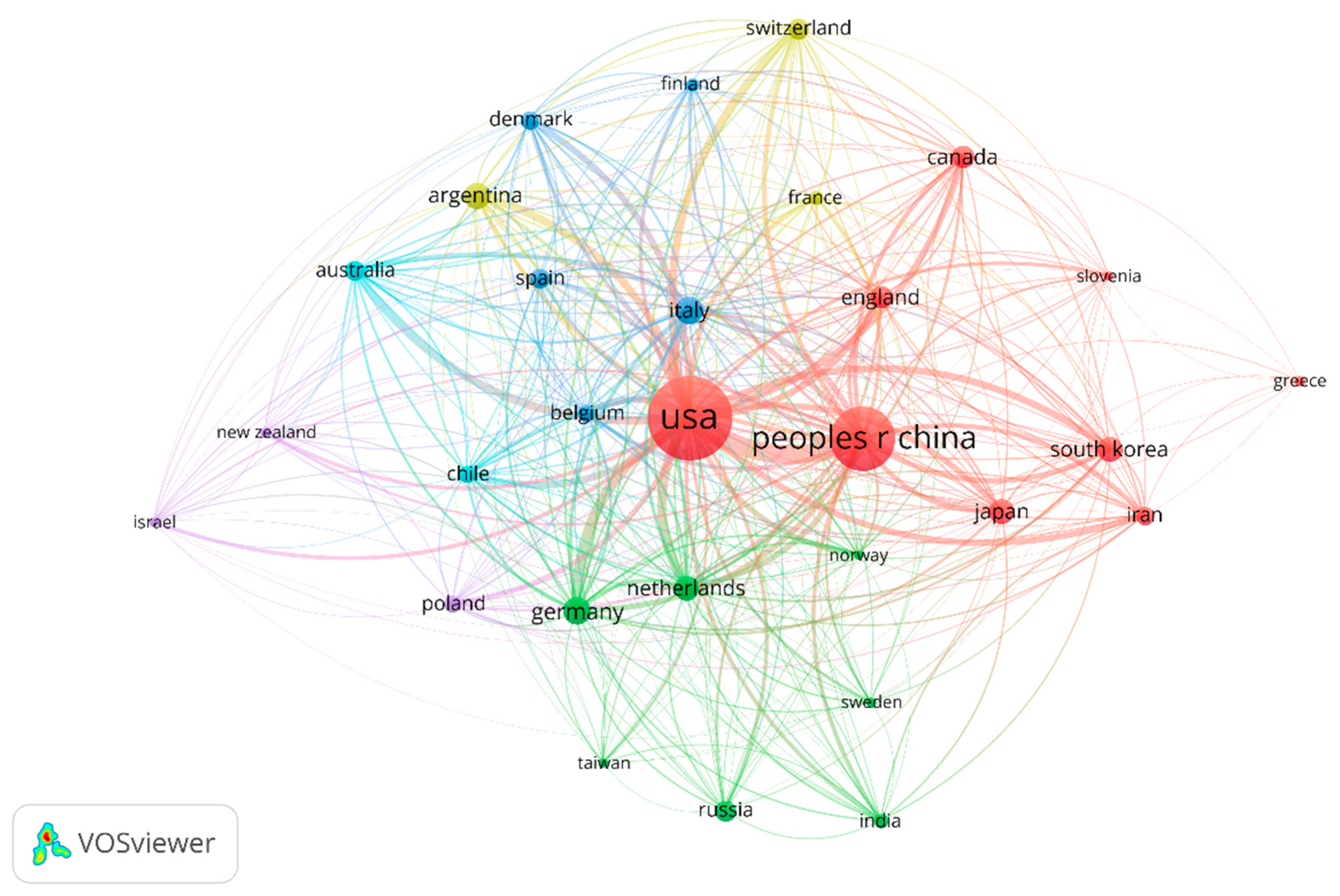
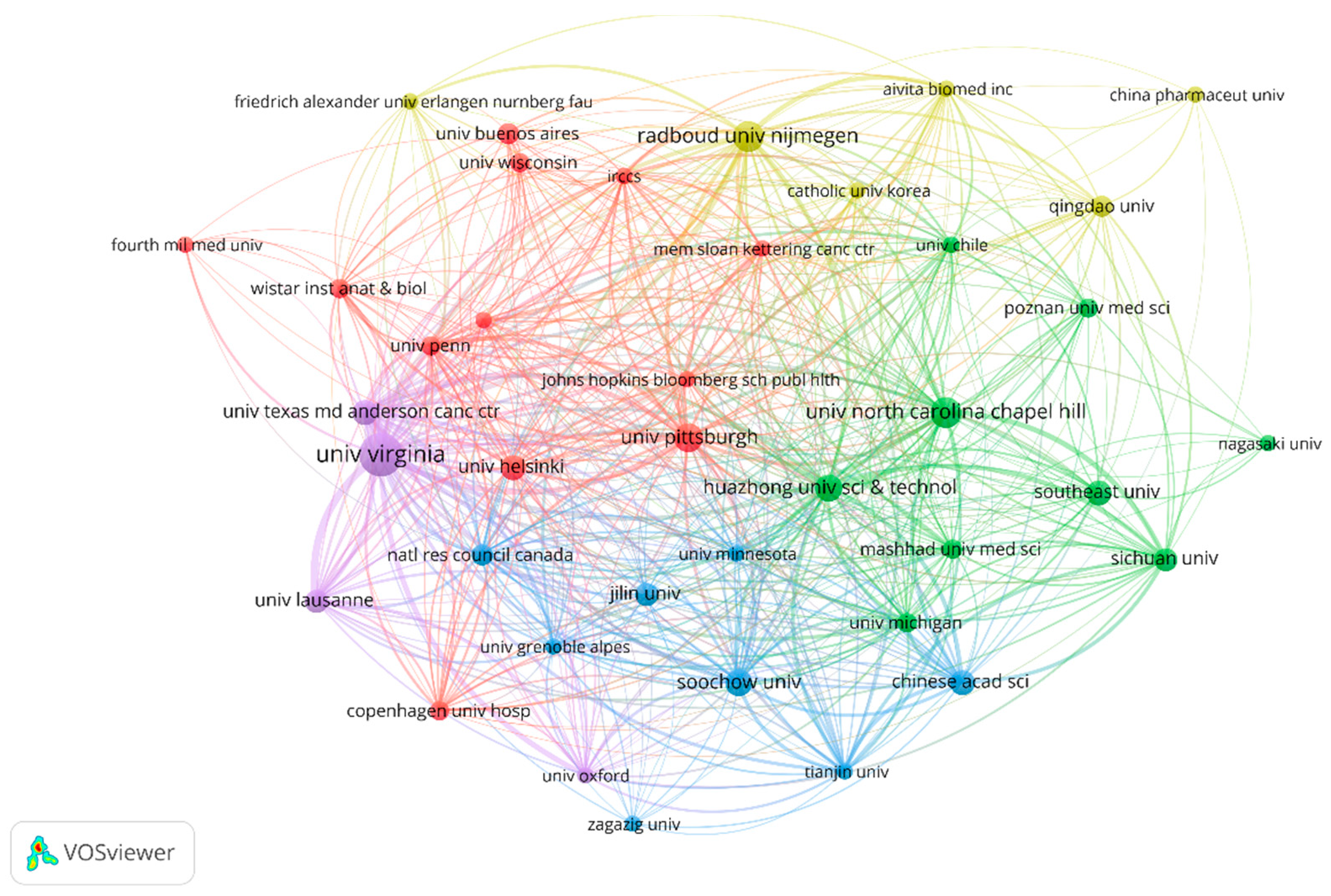
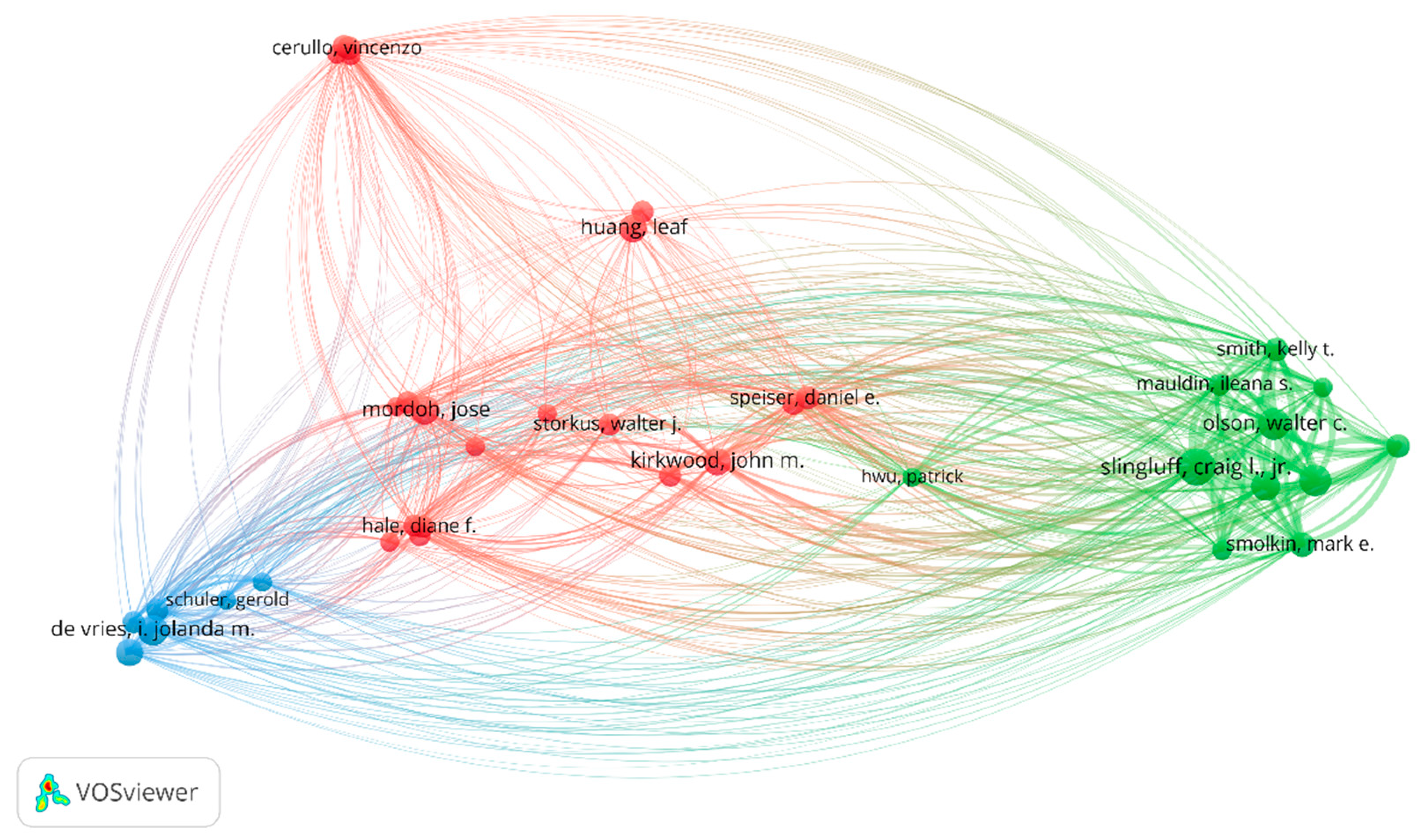
3.3. Analysis of Countries/Regions, Organizations, and Authors
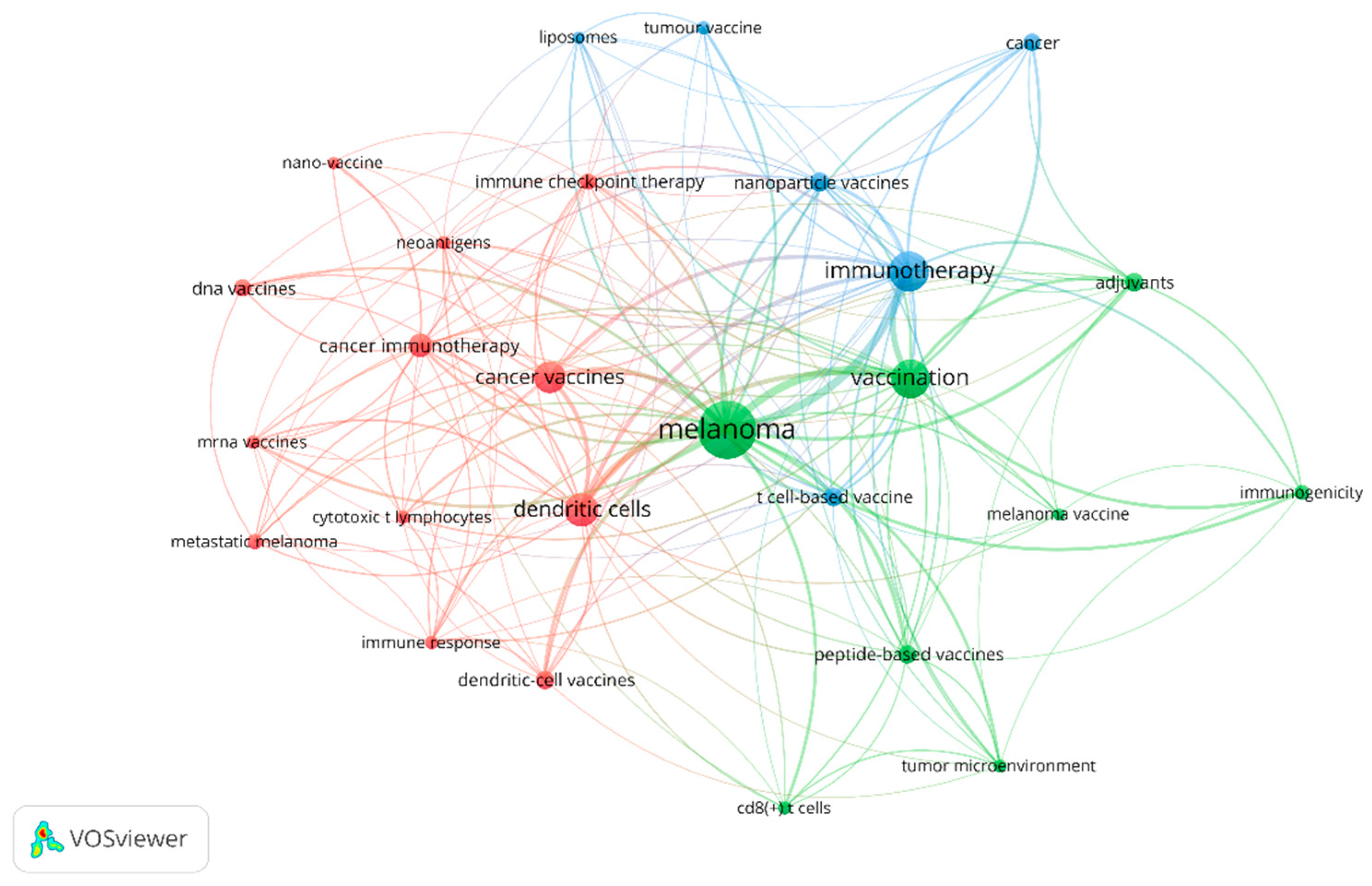
3.4. Co-Occurrence Analysis of Keywords
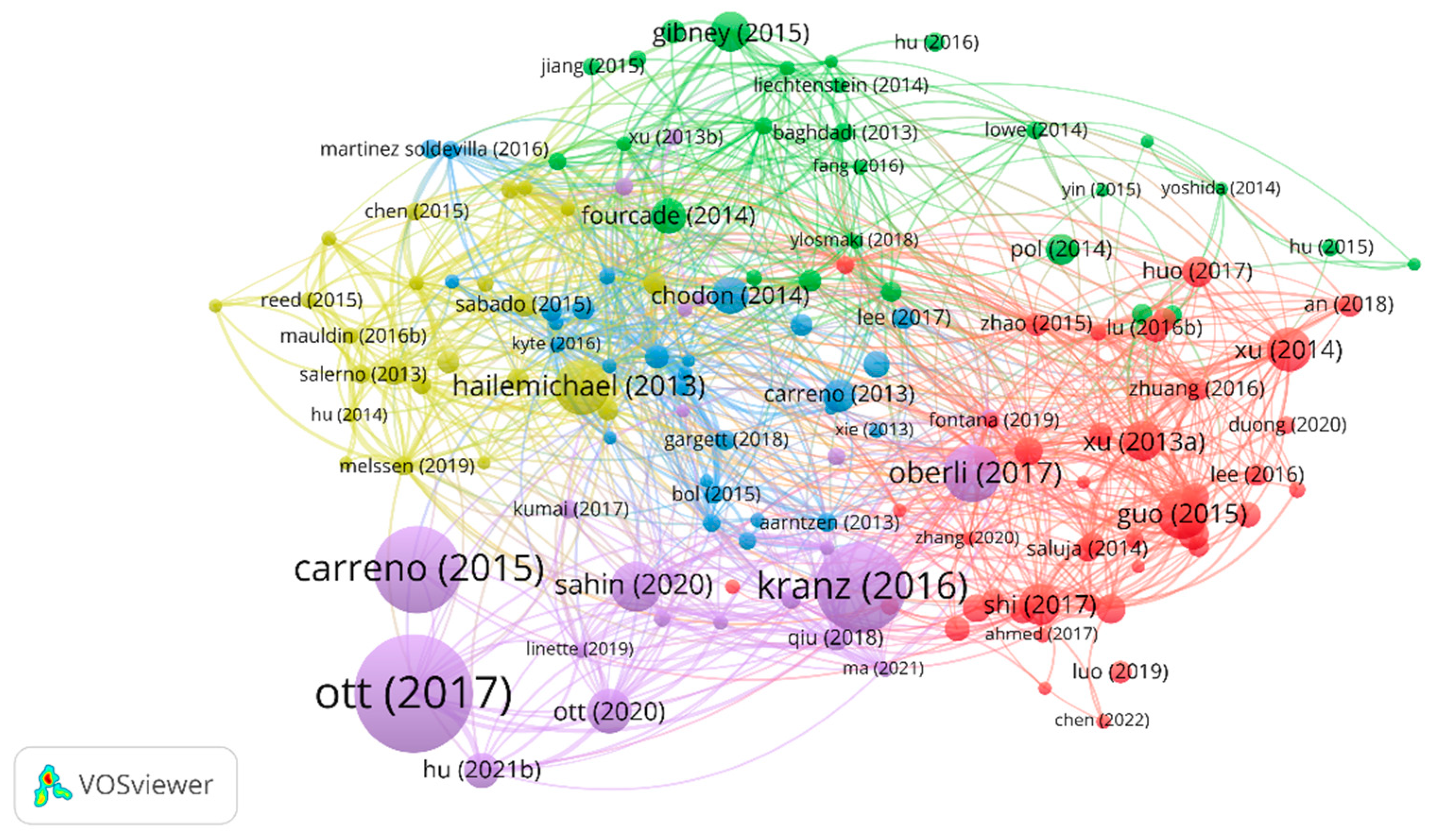
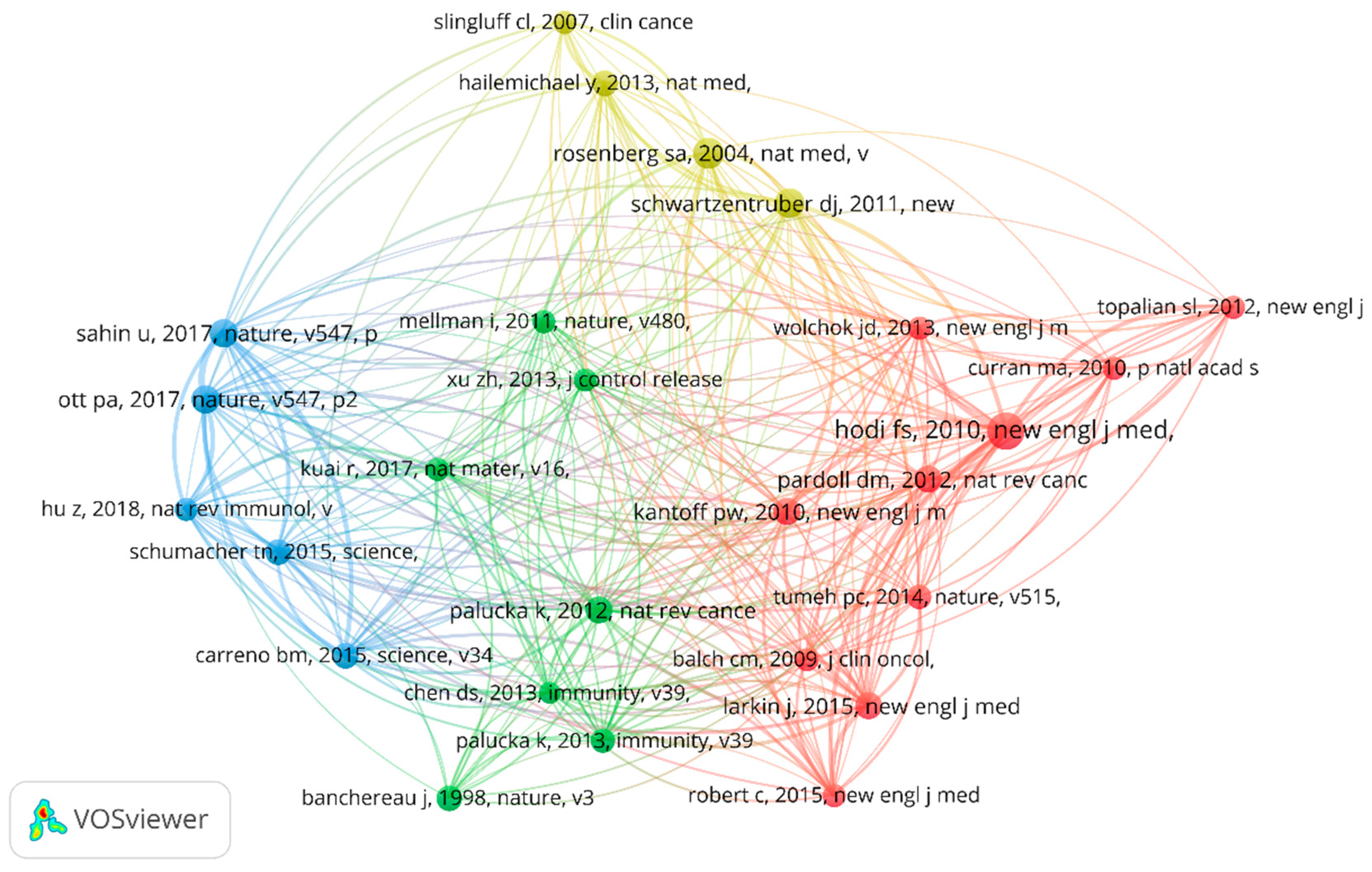
3.5. Reference Citations and Co-Citations
4. Discussions
5. Future Recommendations and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davis, L.E.; Shalin, S.C.; Tackett, A.J. Current state of melanoma diagnosis and treatment. Cancer Biol. Ther. 2019, 20, 1366–1379. [Google Scholar] [CrossRef] [Green Version]
- Seedor, R.S.; Orloff, M. Treatment of Metastatic Melanoma in the Elderly. Curr. Oncol. Rep. 2022, 24, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Switzer, B.; Puzanov, I.; Skitzki, J.J.; Hamad, L.; Ernstoff, M.S. Managing Metastatic Melanoma in 2022: A Clinical Review. JCO Oncol. Pract. 2022, 18, 335–351. [Google Scholar] [CrossRef]
- Saxena, M.; van der Burg, S.H.; Melief, C.; Bhardwaj, N. Therapeutic cancer vaccines. Nat. Rev. Cancer 2021, 21, 360–378. [Google Scholar] [CrossRef] [PubMed]
- Morse, M.A.; Gwin, W.R.; Mitchell, D.A. Vaccine Therapies for Cancer: Then and Now. Target. Oncol. 2021, 16, 121–152. [Google Scholar] [CrossRef]
- Ott, P.A.; Fritsch, E.F.; Wu, C.J.; Dranoff, G. Vaccines and melanoma. Hematol. Oncol. Clin. N. Am. 2014, 28, 559–569. [Google Scholar] [CrossRef] [PubMed]
- Lau, P.; Shen, M.; Ma, F.; Chen, Y.; Zhang, J.; Su, J.; Chen, X.; Liu, H. A Bayesian network meta-analysis of comparison of cancer therapeutic vaccines for melanoma. J. Eur. Acad. Dermatol. 2021, 35, 1976–1986. [Google Scholar] [CrossRef]
- Maurer, D.M.; Butterfield, L.H.; Vujanovic, L. Melanoma vaccines: Clinical status and immune endpoints. Melanoma Res. 2019, 29, 109–118. [Google Scholar] [CrossRef]
- Bianchi, V.; Bulek, A.; Fuller, A.; Lloyd, A.; Attaf, M.; Rizkallah, P.J.; Dolton, G.; Sewell, A.K.; Cole, D.K. A Molecular Switch Abrogates Glycoprotein 100 (gp100) T-cell Receptor (TCR) Targeting of a Human Melanoma Antigen. J. Biol. Chem. 2016, 291, 8951–8959. [Google Scholar] [CrossRef] [Green Version]
- Ge, Y.; Chao, T.; Sun, J.; Liu, W.; Chen, Y.; Wang, C. Frontiers and Hotspots Evolution in Psycho-cardiology: A Bibliometric Analysis From 2004 to 2022. Curr. Prob. Cardiol. 2022, 47, 101361. [Google Scholar] [CrossRef]
- Ott, P.A.; Hu, Z.; Keskin, D.B.; Shukla, S.A.; Sun, J.; Bozym, D.J.; Zhang, W.; Luoma, A.; Giobbie-Hurder, A.; Peter, L.; et al. An immunogenic personal neoantigen vaccine for patients with melanoma. Nature 2017, 547, 217–221. [Google Scholar] [CrossRef] [Green Version]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Da, S.N.L.J.; Georgieva, M.; Haaland, B.; de Lima, L.G. A systematic review and network meta-analysis of immunotherapy and targeted therapy for advanced melanoma. Cancer Med. 2017, 6, 1143–1153. [Google Scholar] [CrossRef]
- Villani, A.; Potestio, L.; Fabbrocini, G.; Troncone, G.; Malapelle, U.; Scalvenzi, M. The Treatment of Advanced Melanoma: Therapeutic Update. Int. J. Mol. Sci. 2022, 23, 6388. [Google Scholar] [CrossRef]
- Wollina, U. Melanoma surgery-An update. Dermatol. Ther. 2022, 35, e15966. [Google Scholar] [CrossRef]
- Adamik, J.; Butterfield, L.H. What’s next for cancer vaccines. Sci. Transl. Med. 2022, 14, eabo4632. [Google Scholar] [CrossRef]
- Igarashi, Y.; Sasada, T. Cancer Vaccines: Toward the Next Breakthrough in Cancer Immunotherapy. J. Immunol. Res. 2020, 2020, 5825401. [Google Scholar] [CrossRef]
- Paston, S.J.; Brentville, V.A.; Symonds, P.; Durrant, L.G. Cancer Vaccines, Adjuvants, and Delivery Systems. Front. Immunol. 2021, 12, 627932. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.; Vandermeulen, G.; Préat, V. Cancer DNA vaccines: Current preclinical and clinical developments and future perspectives. J. Exp. Clin. Cancer Res. 2019, 38, 146. [Google Scholar] [CrossRef] [PubMed]
- Sahin, U.; Türeci, Ö. Personalized vaccines for cancer immunotherapy. Science 2018, 359, 1355–1360. [Google Scholar] [CrossRef] [Green Version]
- Kerr, M.D.; McBride, D.A.; Chumber, A.K.; Shah, N.J. Combining therapeutic vaccines with chemo- and immunotherapies in the treatment of cancer. Expert Opin. Drug Dis. 2021, 16, 89–99. [Google Scholar] [CrossRef]
- Hu, Z.; Leet, D.E.; Allesøe, R.L.; Oliveira, G.; Li, S.; Luoma, A.M.; Liu, J.; Forman, J.; Huang, T.; Iorgulescu, J.B.; et al. Personal neoantigen vaccines induce persistent memory T cell responses and epitope spreading in patients with melanoma. Nat. Med. 2021, 27, 515–525. [Google Scholar] [CrossRef]
- Sahin, U.; Oehm, P.; Derhovanessian, E.; Jabulowsky, R.A.; Vormehr, M.; Gold, M.; Maurus, D.; Schwarck-Kokarakis, D.; Kuhn, A.N.; Omokoko, T.; et al. An RNA vaccine drives immunity in checkpoint-inhibitor-treated melanoma. Nature 2020, 585, 107–112. [Google Scholar] [CrossRef]
- Gardner, A.; de Mingo, P.Á.; Ruffell, B. Dendritic Cells and Their Role in Immunotherapy. Front. Immunol. 2020, 11, 924. [Google Scholar] [CrossRef]
- Peng, M.; Mo, Y.; Wang, Y.; Wu, P.; Zhang, Y.; Xiong, F.; Guo, C.; Wu, X.; Li, Y.; Li, X.; et al. Neoantigen vaccine: An emerging tumor immunotherapy. Mol. Cancer 2019, 18, 128. [Google Scholar] [CrossRef] [Green Version]
- Dillman, R.O.; Cornforth, A.N.; Nistor, G. Cancer stem cell antigen-based vaccines: The preferred strategy for active specific immunotherapy of metastatic melanoma? Expert Opin. Biol. Ther. 2013, 13, 643–656. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Fan, J.; Wu, Y.; Ma, Z.; Huang, J.; Zhang, Y.; Zhou, Z.; Mo, F.; Liu, X.; Yuan, H.; et al. Synthetic multiepitope neoantigen DNA vaccine for personalized cancer immunotherapy. Nanomed. Nanotechnol. Biol. Med. 2021, 37, 102443. [Google Scholar] [CrossRef] [PubMed]
- Bezeljak, U. Cancer gene therapy goes viral: Viral vector platforms come of age. Radiol. Oncol. 2022, 56, 1–13. [Google Scholar] [CrossRef]
- Hu, Z.; Ott, P.A.; Wu, C.J. Towards personalized, tumour-specific, therapeutic vaccines for cancer. Nat. Rev. Immunol. 2018, 18, 168–182. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Lv, J.; Dang, Q.; Liu, L.; Weng, S.; Wang, L.; Zhou, Z.; Kong, Y.; Li, H.; Han, Y.; et al. Engineering neoantigen vaccines to improve cancer personalized immunotherapy. Int. J. Biol. Sci. 2022, 18, 5607–5623. [Google Scholar] [CrossRef]
- Sahin, U.; Derhovanessian, E.; Miller, M.; Kloke, B.P.; Simon, P.; Löwer, M.; Bukur, V.; Tadmor, A.D.; Luxemburger, U.; Schrörs, B.; et al. Personalized RNA mutanome vaccines mobilize poly-specific therapeutic immunity against cancer. Nature 2017, 547, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Roudko, V.; Cimen, B.C.; Greenbaum, B.; Lucas, A.; Samstein, R.; Bhardwaj, N. Lynch Syndrome and MSI-H Cancers: From Mechanisms to “Off-The-Shelf” Cancer Vaccines. Front. Immunol. 2021, 12, 757804. [Google Scholar] [CrossRef]
- Azimi, C.S.; Tang, Q.; Roybal, K.T.; Bluestone, J.A. NextGen cell-based immunotherapies in cancer and other immune disorders. Curr. Opin. Immunol. 2019, 59, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Oberli, M.A.; Reichmuth, A.M.; Dorkin, J.R.; Mitchell, M.J.; Fenton, O.S.; Jaklenec, A.; Anderson, D.G.; Langer, R.; Blankschtein, D. Lipid Nanoparticle Assisted mRNA Delivery for Potent Cancer Immunotherapy. Nano Lett. 2017, 17, 1326–1335. [Google Scholar] [CrossRef]
- Liu, S.; Jiang, Q.; Zhao, X.; Zhao, R.; Wang, Y.; Wang, Y.; Liu, J.; Shang, Y.; Zhao, S.; Wu, T.; et al. A DNA nanodevice-based vaccine for cancer immunotherapy. Nat. Mater. 2021, 20, 421–430. [Google Scholar] [CrossRef]
- Yang, R.; Xu, J.; Xu, L.; Sun, X.; Chen, Q.; Zhao, Y.; Peng, R.; Liu, Z. Cancer Cell Membrane-Coated Adjuvant Nanoparticles with Mannose Modification for Effective Anticancer Vaccination. ACS Nano 2018, 12, 5121–5129. [Google Scholar] [CrossRef]
- Sun, H.; Hu, W.; Yan, Y.; Zhang, Z.; Chen, Y.; Yao, X.; Teng, L.; Wang, X.; Chai, D.; Zheng, J.; et al. Using PAMPs and DAMPs as adjuvants in cancer vaccines. Hum. Vacc. Immunother. 2021, 17, 5546–5557. [Google Scholar] [CrossRef]
- Wen, R.; Umeano, A.C.; Kou, Y.; Xu, J.; Farooqi, A.A. Nanoparticle systems for cancer vaccine. Nanomed. Nanotechnol. Biol. Med. 2019, 14, 627–648. [Google Scholar] [CrossRef]
- Fucikova, J.; Hensler, M.; Kasikova, L.; Lanickova, T.; Pasulka, J.; Rakova, J.; Drozenova, J.; Fredriksen, T.; Hraska, M.; Hrnciarova, T.; et al. An Autologous Dendritic Cell Vaccine Promotes Anticancer Immunity in Patients with Ovarian Cancer with Low Mutational Burden and Cold Tumors. Clin. Cancer Res. 2022, 28, 3053–3065. [Google Scholar] [CrossRef]
- Jia, W.; Zhang, T.; Huang, H.; Feng, H.; Wang, S.; Guo, Z.; Luo, Z.; Ji, X.; Cheng, X.; Zhao, R. Colorectal cancer vaccines: The current scenario and future prospects. Front. Immunol. 2022, 13, 942235. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, Z. The history and advances in cancer immunotherapy: Understanding the characteristics of tumor-infiltrating immune cells and their therapeutic implications. Cell. Mol. Immunol. 2020, 17, 807–821. [Google Scholar] [CrossRef]
- Waldman, A.D.; Fritz, J.M.; Lenardo, M.J. A guide to cancer immunotherapy: From T cell basic science to clinical practice. Nat. Rev. Immunol. 2020, 20, 651–668. [Google Scholar] [CrossRef]
- Fan, A.; Wang, B.; Wang, X.; Nie, Y.; Fan, D.; Zhao, X.; Lu, Y. Immunotherapy in colorectal cancer: Current achievements and future perspective. Int. J. Biol. Sci. 2021, 17, 3837–3849. [Google Scholar] [CrossRef] [PubMed]
- Calmeiro, J.; Carrascal, M.A.; Tavares, A.R.; Ferreira, D.A.; Gomes, C.; Cruz, M.T.; Falcão, A.; Neves, B.M. Pharmacological combination of nivolumab with dendritic cell vaccines in cancer immunotherapy: An overview. Pharmacol. Res. 2021, 164, 105309. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Xia, B.R.; Zhang, Z.C.; Zhang, Y.J.; Lou, G.; Jin, W.L. Immunotherapy for Ovarian Cancer: Adjuvant, Combination, and Neoadjuvant. Front. Immunol. 2020, 11, 577869. [Google Scholar] [CrossRef]
- Duraiswamy, J.; Kaluza, K.M.; Freeman, G.J.; Coukos, G. Dual blockade of PD-1 and CTLA-4 combined with tumor vaccine effectively restores T-cell rejection function in tumors. Cancer Res. 2013, 73, 3591–3603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Wang, Y.; Miao, L.; Liu, Q.; Musetti, S.; Li, J.; Huang, L. Combination Immunotherapy of MUC1 mRNA Nano-vaccine and CTLA-4 Blockade Effectively Inhibits Growth of Triple Negative Breast Cancer. Mol. Ther. 2018, 26, 45–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kranz, L.M.; Diken, M.; Haas, H.; Kreiter, S.; Loquai, C.; Reuter, K.C.; Meng, M.; Fritz, D.; Vascotto, F.; Hefesha, H.; et al. Systemic RNA delivery to dendritic cells exploits antiviral defence for cancer immunotherapy. Nature 2016, 534, 396–401. [Google Scholar] [CrossRef]
- Carreno, B.M.; Magrini, V.; Becker-Hapak, M.; Kaabinejadian, S.; Hundal, J.; Petti, A.A.; Ly, A.; Lie, W.R.; Hildebrand, W.H.; Mardis, E.R.; et al. A dendritic cell vaccine increases the breadth and diversity of melanoma neoantigen-specific T cells. Science 2015, 348, 803–808. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Platforms | Characteristics | |
|---|---|---|
| Peptide-Based Vaccines | Strengths | 1. Relatively safe and well-tolerated. 2. Have a well-defined antigenic target, can focus on specific tumor-associated antigens (TAAs). 3. Can be synthesized easily and at low cost. 4. Can induce both CD4+ and CD8+ T-cell responses. |
| Limitations | 1. Often exhibit limited immunogenicity, resulting in modest clinical efficacy. 2. Require patient-specific HLA matching, which can be challenging in large-scale applications. 3. May induce immune tolerance due to self-antigen presentation. | |
| Targeted Population | Suitable for patients with a well-characterized tumor antigen profile and a high likelihood of having HLA types matching the vaccine peptides. | |
| Future Developments | 1. Incorporate adjuvants or immune checkpoint inhibitors to enhance immunogenicity. 2. Explore personalized neoantigens to target tumor heterogeneity. 3. Investigate novel delivery systems to improve peptide stability and uptake. | |
| DNA-Based Vaccines | Strengths | 1. Can induce both humoral and cellular immune responses. 2. Have the potential for broad antigen coverage due to the expression of full-length TAAs. 3. Relatively easy to manufacture and can be modified rapidly. 4. Can be tailored to incorporate personalized neoantigens. |
| Limitations | 1. Low transfection efficiency limits the immune response generated. 2. The risk of integration into the host genome is a concern, although it is rare. 3. The need for electroporation or viral vectors for efficient delivery poses logistical challenges. | |
| Targeted Population | Have the potential to benefit a wide range of patients, especially those with solid tumors expressing well-characterized antigens and those who can receive efficient delivery methods. | |
| Future Developments | 1. Improve transfection efficiency through advanced delivery techniques. 2. Enhance antigen expression levels to optimize immune responses. 3. Combine DNA vaccines with other immunotherapies to enhance clinical outcomes. | |
| Viral Vector-Based Vaccines | Strengths | 1. Can efficiently deliver TAAs to target cells, enhancing antigen presentation. 2. Have the potential to induce robust immune responses. 3. Can be modified to express multiple antigens simultaneously. 4. Can amplify the vaccine effect through viral replication. |
| Limitations | 1. Safety concerns. 2. Pre-existing immunity to the vector may limit vaccine effectiveness. 3. Immune evasion mechanisms employed by the virus may hinder vaccine efficacy. | |
| Targeted Population | Can benefit patients with advanced melanoma who have intact immune systems and limited pre-existing immunity against the vector. | |
| Future Developments | 1. Improve vector design to enhance tumor targeting and antigen expression. 2. Overcome pre-existing immunity through the development of novel vectors. 3. Investigate combination therapies for synergistic effects. | |
| Dendritic Cell-Based Vaccines | Strengths | 1. Offer the possibility of targeting multiple antigens simultaneously. 2. Can be modified ex vivo to enhance their immunogenicity. 3. Can be personalized based on patient-specific antigens. |
| Limitations | 1. The complex and expensive process of dendritic cell isolation and activation limits scalability. 2. The limited lifespan of dendritic cells after infusion hinders long-term immune responses. 3. The immunosuppressive tumor microenvironment may hinder dendritic cell function. | |
| Targeted Population | May benefit patients with advanced melanoma who have intact immune systems and accessible tumor tissues for dendritic cell isolation. | |
| Future Developments | 1. Explore artificial antigen-presenting cells (aAPCs) as a substitute to streamline the process. 2. Use of genetic engineering to enhance their antigen presentation and T-cell activation capabilities. 3. Investigate combination therapies to overcome immune suppression. | |
| Whole Cell-Based Vaccines | Strengths | 1. Can provide a broad range of antigens. 2. Can induce both humoral and cellular immune responses. 3. Can address tumor heterogeneity and immune escape mechanisms. 4. The process of whole cell-based vaccine production is relatively straightforward. |
| Limitations | 1. Quality control and standardization can be challenging. 2. The immune response may not be specific to tumor antigens. 3. The potential for immune tolerance to self-antigens exists. | |
| Targeted Population | May benefit patients with advanced melanoma, particularly those with a high tumor mutational burden or tumor heterogeneity. | |
| Future Developments | 1. Identify optimal antigen combinations to maximize immune responses. 2. Incorporate other immunotherapies to enhance vaccine efficacy. 3. Develop personalized vaccine formulations based on individual tumor neoantigen profiles. | |
| Titles | Year | Journals | Databases | Topics |
|---|---|---|---|---|
| 1. Characterization of the T cell receptor repertoire and melanoma tumor microenvironment upon combined treatment with ipilimumab and hTERT vaccination. | 2022 | J Transl Med | PubMed | Tumor microenvironment Cancer vaccine |
| 2. Phase I/II clinical trial of a helper peptide vaccine plus PD-1 blockade in PD-1 antibody-naïve and PD-1 antibody-experienced patients with melanoma (MEL64). | 2022 | J Immunother Cancer | PubMed | PD-1 Cancer vaccine |
| 3. Dendritic cell vaccines targeting tumor blood vessel antigens in combination with dasatinib induce therapeutic immune responses in patients with checkpoint-refractory advanced melanoma. | 2021 | J Immunother Cancer | PubMed | Dendritic cells Neoplasm antigens |
| 4. Melanoma stem cell vaccine induces effective tumor immunity against melanoma. | 2023 | Hum Vaccin Immunother | Embase | CD8-Positive T-cell Cancer vaccine |
| 5. Targeting the tumor microenvironment by liposomal Epacadostat in combination with liposomal gp100 vaccine. | 2023 | Sci Rep | Embase | Tissue distribution Tumor microenvironment |
| 6. A randomized controlled trial of long NY-ESO-1 peptide-pulsed autologous dendritic cells with or without alpha-galactosylceramide in high-risk melanoma. | 2023 | Cancer Immunol Immunother | Cochrane | Dendritic cell NY-ESO-1 |
| 7. An update of cutaneous melanoma patients treated in adjuvancy with the allogeneic melanoma vaccine vaccimel and presentation of a selected case report with in-transit metastases. | 2022 | Front Immunol | Cochrane | Immunologic adjuvants Cancer vaccine |
| 8. Engineered antibody cytokine chimera synergizes with DNA-launched nanoparticle vaccines to potentiate melanoma suppression. | 2023 | Front Immunol | Cochrane | DNA vaccines Nanoparticles |
| 9. Liposomal celecoxib combined with dendritic cell therapy enhances antitumor efficacy in melanoma. | 2023 | J Control Release | WOS | Combination therapy Dendritic Cells |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Jia, Q.-N.; Wu, M.; Liu, M.; Li, J. A Bibliometric Analysis of Melanoma Treated with Vaccinations Research from 2013 to 2023: A Comprehensive Review of the Literature. Vaccines 2023, 11, 1113. https://doi.org/10.3390/vaccines11061113
Wang X, Jia Q-N, Wu M, Liu M, Li J. A Bibliometric Analysis of Melanoma Treated with Vaccinations Research from 2013 to 2023: A Comprehensive Review of the Literature. Vaccines. 2023; 11(6):1113. https://doi.org/10.3390/vaccines11061113
Chicago/Turabian StyleWang, Xinyu, Qian-Nan Jia, Mengyin Wu, Mingjuan Liu, and Jun Li. 2023. "A Bibliometric Analysis of Melanoma Treated with Vaccinations Research from 2013 to 2023: A Comprehensive Review of the Literature" Vaccines 11, no. 6: 1113. https://doi.org/10.3390/vaccines11061113