
Review of Vaccination Recommendations in Guidelines for Non-Communicable Diseases with Highest Global Disease Burden among Adults 75 Years Old and Above


{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
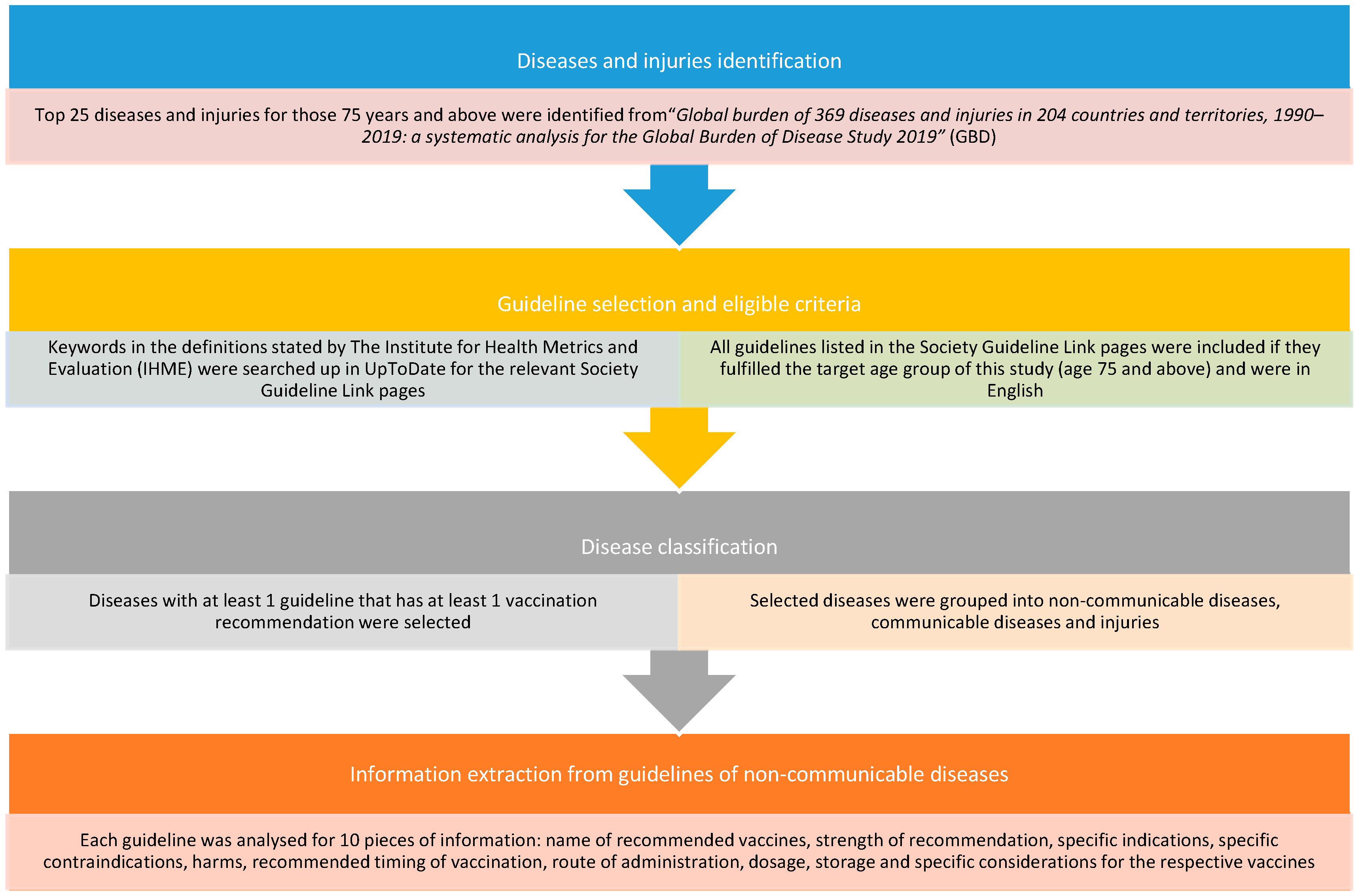
2.1. Diseases and Injuries Identification
2.2. Guideline Selection and Eligible Criteria
2.3. Disease Classification
2.4. Information Extraction
3. Results
3.1. IHD
3.2. Hypertensive Heart Disease
3.3. Atrial Fibrillation and Flutter
3.4. COPD
3.5. Asthma
3.6. Cirrhosis and Other Chronic Liver Diseases
3.7. Colon and Rectal Cancer
3.8. Stomach Cancer
3.9. Diabetes
3.10. CKD
3.11. Stroke
4. Discussion
4.1. Discussion for Each Recommended Vaccine
4.1.1. Influenza Vaccine
Cardiac-Related Diseases
Respiratory-Related Diseases
Gastrointestinal-Related Diseases
Other Diseases
Vaccine Administration Details
4.1.2. Pneumococcal Vaccine
Cardiac-Related Diseases
Respiratory-Related Diseases
Gastrointestinal-Related Diseases
Other Diseases
Vaccine Administration Details
4.1.3. Hepatitis Vaccine
Gastrointestinal-Related Diseases
Cardiac-Related Diseases
Respiratory-Related Diseases and Other Diseases
Vaccine Administration Details
4.1.4. COVID-19 Vaccine
4.1.5. Varicella Zoster Vaccine
4.1.6. Tdap Vaccine
4.1.7. MMR and Varicella Vaccine
4.1.8. HPV Vaccine
4.1.9. Meningococcal Vaccine
4.1.10. Poliovirus Vaccine
4.1.11. Yellow Fever Vaccine
4.2. Strengths and Limitations
4.3. Clinical Implications and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Vaccine Action Plan. Decade of vaccine collaboration. Vaccine 2013, 31 (Suppl. 2), B5–B31. [Google Scholar] [CrossRef] [PubMed]
- Berg, R.L.; Cassells, J.S. The Second Fifty Years: Promoting Health and Preventing Disability. In The Second Fifty Years: Promoting Health and Preventing Disability; National Academies Press: Washington, DC, USA, 1992. [Google Scholar] [CrossRef]
- Mouton, C.P.; Bazaldua, O.V.; Pierce, B.; Espino, D.V. Common infections in older adults. Am. Fam. Physician 2001, 63, 257–268. [Google Scholar] [PubMed]
- Pan American Health Organization. Noncommunicable Diseases. Available online: https://www.paho.org/en/topics/noncommunicable-diseases#:~:text=The%20term%20NCDs%20refers%20to,diabetes%20and%20chronic%20lung%20illnesses (accessed on 28 May 2023).
- World Health Organization. Noncommunicable Diseases: Mortality. Available online: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/ncd-mortality (accessed on 28 May 2023).
- World Health Organization. Vaccines and Immunization. Available online: https://www.who.int/health-topics/vaccines-and-immunization#tab=tab_1 (accessed on 15 December 2022).
- World Health Organization, Strategic Advisory Group of Experts (SAGE). WHO Vaccine Position Papers; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Abbafati, C.; Machado, D.B.; Cislaghi, B.; Salman, O.M.; Karanikolos, M.; McKee, M.; Abbas, K.M.; Brady, O.J.; Larson, H.J.; Trias-Llimós, S.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Edson, R.S.; Beckman, T.J.; West, C.P.; Aronowitz, P.B.; Badgett, R.G.; Feldstein, D.A.; Henderson, M.C.; Kolars, J.C.; McDonald, F.S. A multi-institutional survey of internal medicine residents’ learning habits. Med. Teach. 2010, 32, 773–775. [Google Scholar] [CrossRef]
- Phua, J.; See, K.C.; Khalizah, H.J.; Low, S.P.; Lim, T.K. Utility of the electronic information resource UpToDate for clinical decision-making at bedside rounds. Singap. Med. J. 2012, 53, 116–120. [Google Scholar]
- World Health Organization. World Health Statistics 2023: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2023; p. 88.
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, E.; Greenfield, S.; Wolman, D.M.; Mancher, M.; Graham, R. (Eds.) Clinical Practice Guidelines We Can Trust; The National Academies Press: Washington, DC, USA, 2011; p. 290. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Lewandowsky, S.; Antfolk, J. The association between vaccination confidence, vaccination behavior, and willingness to recommend vaccines among Finnish healthcare workers. PLoS ONE 2019, 14, e0224330. [Google Scholar] [CrossRef] [Green Version]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention (CDC). Vaccine Label Examples. Available online: https://www.cdc.gov/vaccines/hcp/admin/storage/guide/vaccine-storage-labels.pdf (accessed on 3 September 2022).
- Australian Government Department of Health and Aged Care. Australian Immunisation Handbook; Australian Government Department of Health and Aged Care: Canberra, Australia, 2022. Available online: https://immunisationhandbook.health.gov.au/contents/about-the-handbook#citation (accessed on 19 December 2022).
- Hannoun, C. The evolving history of influenza viruses and influenza vaccines. Expert Rev. Vaccines 2013, 12, 1085–1094. [Google Scholar] [CrossRef]
- Nichol, K.L.; Wuorenma, J.; von Sternberg, T. Benefits of influenza vaccination for low-, intermediate-, and high-risk senior citizens. Arch. Intern. Med. 1998, 158, 1769–1776. [Google Scholar] [CrossRef] [Green Version]
- Darvishian, M.; Gefenaite, G.; Turner, R.M.; Pechlivanoglou, P.; Van der Hoek, W.; Van den Heuvel, E.R.; Hak, E. After adjusting for bias in meta-analysis seasonal influenza vaccine remains effective in community-dwelling elderly. J. Clin. Epidemiol. 2014, 67, 734–744. [Google Scholar] [CrossRef] [Green Version]
- Jaiswal, V.; Ang, S.P.; Yaqoob, S.; Ishak, A.; Chia, J.E.; Nasir, Y.M.; Anjum, Z.; Alraies, M.C.; Jaiswal, A.; Biswas, M. Cardioprotective effects of influenza vaccination among patients with established cardiovascular disease or at high cardiovascular risk: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2022, 29, 1881–1892. [Google Scholar] [CrossRef]
- Liu, I.F.; Huang, C.C.; Chan, W.L.; Huang, P.H.; Chung, C.M.; Lin, S.J.; Chen, J.W.; Leu, H.B. Effects of annual influenza vaccination on mortality and hospitalization in elderly patients with ischemic heart disease: A nationwide population-based study. Prev. Med. 2012, 54, 431–433. [Google Scholar] [CrossRef]
- Vardeny, O.; Claggett, B.; Udell, J.A.; Packer, M.; Zile, M.; Rouleau, J.; Swedberg, K.; Desai, A.S.; Lefkowitz, M.; Shi, V.; et al. Influenza Vaccination in Patients With Chronic Heart Failure: The PARADIGM-HF Trial. JACC Heart Fail. 2016, 4, 152–158. [Google Scholar] [CrossRef]
- Rodrigues, B.S.; David, C.; Costa, J.; Ferreira, J.J.; Pinto, F.J.; Caldeira, D. Influenza vaccination in patients with heart failure: A systematic review and meta-analysis of observational studies. Heart 2020, 106, 350–357. [Google Scholar] [CrossRef]
- Bolton, A.; Thyagaturu, H.; Ashraf, M.; Carnahan, R.; Hodgson-Zingman, D. Effects of atrial fibrillation on outcomes of influenza hospitalization. Int. J. Cardiol. Heart Vasc. 2022, 42, 101106. [Google Scholar] [CrossRef]
- Liu, J.C.; Wang, T.J.; Sung, L.C.; Kao, P.F.; Yang, T.Y.; Hao, W.R.; Chen, C.C.; Hsu, Y.P.; Wu, S.Y. Influenza vaccination reduces hemorrhagic stroke risk in patients with atrial fibrillation: A population-based cohort study. Int. J. Cardiol. 2017, 232, 315–323. [Google Scholar] [CrossRef]
- Kao, P.F.; Liu, J.C.; Hsu, Y.P.; Sung, L.C.; Yang, T.Y.; Hao, W.R.; Lin, Y.C.; Wu, S.Y. Influenza vaccination might reduce the risk of ischemic stroke in patients with atrial fibrillation: A population-based cohort study. Oncotarget 2017, 8, 112697–112711. [Google Scholar] [CrossRef] [Green Version]
- Liao, K.M.; Chen, Y.J.; Shen, C.W.; Ou, S.K.; Chen, C.Y. The Influence of Influenza Virus Infections in Patients with Chronic Obstructive Pulmonary Disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2022, 17, 2253–2261. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, P.; An, Z.; Yue, C.; Wang, Y.; Liu, Y.; Yuan, X.; Ma, Y.; Li, K.; Yin, Z.; et al. Effectiveness of influenza and pneumococcal vaccines on chronic obstructive pulmonary disease exacerbations. Respirology 2022, 27, 844–853. [Google Scholar] [CrossRef]
- Vasileiou, E.; Sheikh, A.; Butler, C.; El Ferkh, K.; von Wissmann, B.; McMenamin, J.; Ritchie, L.; Schwarze, J.; Papadopoulos, N.G.; Johnston, S.L.; et al. Effectiveness of Influenza Vaccines in Asthma: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2017, 65, 1388–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suarez-Varela, M.M.; Llopis, A.; Fernandez-Fabrellas, E.; Sanz, F.; Perez-Lozano, M.J.; Martin, V.; Astray, J.; Castilla, J.; Egurrola, M.; Force, L.; et al. Asthma and influenza vaccination in elderly hospitalized patients: Matched case-control study in Spain. J. Asthma 2018, 55, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Alukal, J.J.; Naqvi, H.A.; Thuluvath, P.J. Vaccination in Chronic Liver Disease: An Update. J. Clin. Exp. Hepatol. 2022, 12, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Harmala, S.; Parisinos, C.A.; Shallcross, L.; O’Brien, A.; Hayward, A. Effectiveness of influenza vaccines in adults with chronic liver disease: A systematic review and meta-analysis. BMJ Open 2019, 9, e031070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, B.; Yeo, Y.H.; Jeong, D.; Sheen, E.; Park, H.; Nguyen, P.; Hsu, Y.C.; Garcia, G.; Nguyen, M.H. Higher mortality and hospital charges in patients with cirrhosis and acute respiratory illness: A population-based study. Sci. Rep. 2018, 8, 9969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobotka, L.A.; Mumtaz, K.; Hinton, A.; Conteh, L.F. The time to advocate for influenza vaccines in patients with cirrhosis is now. Clin. Res. Hepatol. Gastroenterol. 2022, 46, 101838. [Google Scholar] [CrossRef]
- Taha, A.; Vinograd, I.; Sakhnini, A.; Eliakim-Raz, N.; Farbman, L.; Baslo, R.; Stemmer, S.M.; Gafter-Gvili, A.; Leibovici, L.; Paul, M. The association between infections and chemotherapy interruptions among cancer patients: Prospective cohort study. J. Infect. 2015, 70, 223–229. [Google Scholar] [CrossRef]
- Kunisaki, K.M.; Janoff, E.N. Influenza in immunosuppressed populations: A review of infection frequency, morbidity, mortality, and vaccine responses. Lancet Infect. Dis. 2009, 9, 493–504. [Google Scholar] [CrossRef] [Green Version]
- Vinograd, I.; Eliakim-Raz, N.; Farbman, L.; Baslo, R.; Taha, A.; Sakhnini, A.; Lador, A.; Stemmer, S.M.; Gafter-Gvili, A.; Leibovici, L.; et al. Clinical effectiveness of seasonal influenza vaccine among adult cancer patients. Cancer 2013, 119, 4028–4035. [Google Scholar] [CrossRef] [Green Version]
- Wang, I.K.; Lin, C.L.; Chang, Y.C.; Lin, P.C.; Liang, C.C.; Liu, Y.L.; Chang, C.T.; Yen, T.H.; Huang, C.C.; Sung, F.C. Effectiveness of influenza vaccination in elderly diabetic patients: A retrospective cohort study. Vaccine 2013, 31, 718–724. [Google Scholar] [CrossRef]
- Vamos, E.P.; Pape, U.J.; Curcin, V.; Harris, M.J.; Valabhji, J.; Majeed, A.; Millett, C. Effectiveness of the influenza vaccine in preventing admission to hospital and death in people with type 2 diabetes. CMAJ 2016, 188, E342–E351. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.I.; Kao, P.F.; Wu, M.Y.; Fang, Y.A.; Miser, J.S.; Liu, J.C.; Sung, L.C. Influenza Vaccination is Associated with Lower Risk of Acute Coronary Syndrome in Elderly Patients with Chronic Kidney Disease. Medicine 2016, 95, e2588. [Google Scholar] [CrossRef]
- Fang, Y.A.; Chen, C.I.; Liu, J.C.; Sung, L.C. Influenza Vaccination Reduces Hospitalization for Heart Failure in Elderly Patients with Chronic Kidney Disease: A Population-Based Cohort Study. Acta Cardiol. Sin. 2016, 32, 290–298. [Google Scholar] [CrossRef]
- Liu, J.C.; Hsu, Y.P.; Kao, P.F.; Hao, W.R.; Liu, S.H.; Lin, C.F.; Sung, L.C.; Wu, S.Y. Influenza Vaccination Reduces Dementia Risk in Chronic Kidney Disease Patients: A Population-Based Cohort Study. Medicine 2016, 95, e2868. [Google Scholar] [CrossRef]
- Chen, C.C.; Wu, C.H.; Lin, C.H.; Chiu, C.C.; Yang, T.Y.; Lei, M.H.; Yeh, H.T.; Jian, W.; Fang, Y.A.; Hao, W.R.; et al. Influenza Vaccination and Risk of Lung Cancer in Patients with Chronic Kidney Disease: A Nationwide, Population-Based Cohort Study. Cancers 2022, 14, 2926. [Google Scholar] [CrossRef]
- Holodinsky, J.K.; Zerna, C.; Malo, S. Association between influenza vaccination and risk of stroke in Alberta, Canada: A population-based study. Lancet Public Health 2022, 7, e914–e922. [Google Scholar] [CrossRef]
- Siriwardena, A.N. Increasing evidence that influenza is a trigger for cardiovascular disease. J. Infect. Dis. 2012, 206, 1636–1638. [Google Scholar] [CrossRef]
- De Boer, P.T.; Crepey, P.; Pitman, R.J.; Macabeo, B.; Chit, A.; Postma, M.J. Cost-Effectiveness of Quadrivalent versus Trivalent Influenza Vaccine in the United States. Value Health 2016, 19, 964–975. [Google Scholar] [CrossRef] [Green Version]
- Thommes, E.W.; Ismaila, A.; Chit, A.; Meier, G.; Bauch, C.T. Cost-effectiveness evaluation of quadrivalent influenza vaccines for seasonal influenza prevention: A dynamic modeling study of Canada and the United Kingdom. BMC Infect. Dis. 2015, 15, 465. [Google Scholar] [CrossRef] [Green Version]
- Reichert, T.A.; Simonsen, L.; Sharma, A.; Pardo, S.A.; Fedson, D.S.; Miller, M.A. Influenza and the winter increase in mortality in the United States, 1959℃1999. Am. J. Epidemiol. 2004, 160, 492–502. [Google Scholar] [CrossRef]
- Vollaard, A.; Schreuder, I.; Slok-Raijmakers, L.; Opstelten, W.; Rimmelzwaan, G.; Gelderblom, H. Influenza vaccination in adult patients with solid tumours treated with chemotherapy. Eur. J. Cancer 2017, 76, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Berical, A.C.; Harris, D.; Dela Cruz, C.S.; Possick, J.D. Pneumococcal Vaccination Strategies. An Update and Perspective. Ann. Am. Thorac. Soc. 2016, 13, 933–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tackling, G.; Borhade, M.B. Hypertensive Heart Disease; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Odutayo, A.; Wong, C.X.; Hsiao, A.J.; Hopewell, S.; Altman, D.G.; Emdin, C.A. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: Systematic review and meta-analysis. BMJ 2016, 354, i4482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Froes, F.; Roche, N.; Blasi, F. Pneumococcal vaccination and chronic respiratory diseases. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 3457–3468. [Google Scholar] [CrossRef] [Green Version]
- Czaicki, N.; Bigaj, J.; Zielonka, T.M. Pneumococcal Vaccine in Adult Asthma Patients. Adv. Exp. Med. Biol. 2021, 1289, 55–62. [Google Scholar] [CrossRef]
- Laratta, C.R.; Williams, K.; Vethanayagam, D.; Ulanova, M.; Vliagoftis, H. A case series evaluating the serological response of adult asthma patients to the 23-valent pneumococcal polysaccharide vaccine. Allergy Asthma Clin. Immunol. 2017, 13, 27. [Google Scholar] [CrossRef] [Green Version]
- McCashland, T.M.; Preheim, L.C.; Gentry-Nielsen, M.J. Pneumococcal Vaccine Response in Cirrhosis and Liver Transplantation. J. Infect. Dis. 2000, 181, 757–760. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.J.; Huang, Y.-T.; Kim, S.J.; Kerpelev, M.; Gonzalez, V.; Kaltsas, A.; Papanicolaou, G. Trends in Invasive Pneumococcal Disease in Cancer Patients After the Introduction of 7-valent Pneumococcal Conjugate Vaccine: A 20-year Longitudinal Study at a Major Urban Cancer Center. Clin. Infect. Dis. 2017, 66, 244–253. [Google Scholar] [CrossRef] [Green Version]
- Chiou, W.Y.; Hung, S.K.; Lin, H.Y.; Chen, L.C.; Hsu, F.C.; Tsai, S.J.; Yu, B.H.; Lee, M.S.; Li, C.Y. Effectiveness of 23-valent pneumococcal polysaccharide vaccine on elderly patients with colorectal cancer: A population-based propensity score-matched cohort study. Medicine 2019, 98, e18380. [Google Scholar] [CrossRef] [Green Version]
- American Association of Diabetes Educators. Vaccination Practices for Adults with Diabetes; American Association of Diabetes Educators: Chicago, IL, USA, 2019. [Google Scholar]
- Haddiya, I. Current Knowledge of Vaccinations in Chronic Kidney Disease Patients. Int. J. Nephrol. Renovasc. Dis. 2020, 13, 179–185. [Google Scholar] [CrossRef]
- Tseng, H.F.; Slezak, J.M.; Quinn, V.P.; Sy, L.S.; Van den Eeden, S.K.; Jacobsen, S.J. Pneumococcal vaccination and risk of acute myocardial infarction and stroke in men. JAMA 2010, 303, 1699–1706. [Google Scholar] [CrossRef] [Green Version]
- Siriwardena, A.N.; Asghar, Z.; Coupland, C.C. Influenza and pneumococcal vaccination and risk of stroke or transient ischaemic attack-matched case control study. Vaccine 2014, 32, 1354–1361. [Google Scholar] [CrossRef]
- Masuda, T.; Nakatani, E.; Shirai, T.; Akamatsu, T.; Tamura, K.; Takahashi, S.; Tanaka, Y.; Watanabe, H.; Endo, Y.; Suzuki, T.; et al. Effectiveness of a 23-valent pneumococcal polysaccharide vaccine for the prevention of pneumococcal pneumonia in the elderly with chronic respiratory diseases: A case–control study of a single center. BMC Pulm. Med. 2021, 21, 123. [Google Scholar] [CrossRef]
- Jackson, L.A.; Gurtman, A.; Rice, K.; Pauksens, K.; Greenberg, R.N.; Jones, T.R.; Scott, D.A.; Emini, E.A.; Gruber, W.C.; Schmoele-Thoma, B. Immunogenicity and safety of a 13-valent pneumococcal conjugate vaccine in adults 70 years of age and older previously vaccinated with 23-valent pneumococcal polysaccharide vaccine. Vaccine 2013, 31, 3585–3593. [Google Scholar] [CrossRef] [Green Version]
- Portoles-Perez, J.; Marques-Vidas, M.; Picazo, J.J.; Gonzalez-Romo, F.; Garcia-Rojas, A.; Perez-Trallero, E.; Gil-Gregorio, P.; de la Camara, R.; Morato, M.L.; Rodriguez, A.; et al. Recommendations for vaccination against pneumococcus in kidney patients in Spain. Nefrologia 2014, 34, 545–551. [Google Scholar] [CrossRef]
- Choi, W.; Kim, J.G.; Beom, S.H.; Hwang, J.E.; Shim, H.J.; Cho, S.H.; Shin, M.H.; Jung, S.H.; Chung, I.J.; Song, J.Y.; et al. Immunogenicity and Optimal Timing of 13-Valent Pneumococcal Conjugate Vaccination during Adjuvant Chemotherapy in Gastric and Colorectal Cancer: A Randomized Controlled Trial. Cancer Res. Treat. 2020, 52, 246–253. [Google Scholar] [CrossRef]
- Singh, K.K.; Panda, S.K.; Shalimar; Acharya, S.K. Patients with Diabetes Mellitus are Prone to Develop Severe Hepatitis and Liver Failure due to Hepatitis Virus Infection. J. Clin. Exp. Hepatol. 2013, 3, 275–280. [Google Scholar] [CrossRef] [Green Version]
- Noble, J.; Jouve, T.; Malvezzi, P.; Rostaing, L. Renal complications of liver diseases. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 1135–1142. [Google Scholar] [CrossRef]
- Tung, J.; Carlisle, E.; Smieja, M.; Kim, P.T.; Lee, C.H. A randomized clinical trial of immunization with combined hepatitis A and B versus hepatitis B alone for hepatitis B seroprotection in hemodialysis patients. Am. J. Kidney Dis. 2010, 56, 713–719. [Google Scholar] [CrossRef]
- Keeffe, E.B. Hepatitis A and B superimposed on chronic liver disease: Vaccine-preventable diseases. Trans. Am. Clin. Climatol. Assoc. 2006, 117, 227–237; discussion 237–238. [Google Scholar]
- Abraham, P. Viral hepatitis in India. Clin. Lab. Med. 2012, 32, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.; Song, Y.M.; Choi, Y.H.; Ebrahim, S.; Davey Smith, G. Hepatitis B virus seropositivity and the risk of stroke and myocardial infarction. Stroke 2007, 38, 1436–1441. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Xiong, J.; Chen, X.; Niu, M.; Chen, X.; Guan, Y.; Zheng, K.; Xu, K. Hepatitis B virus infection and decreased risk of stroke: A meta-analysis. Oncotarget 2017, 8, 59658–59665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marjot, T.; Webb, G.J.; Barritt, A.S.t.; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: Mechanistic and clinical perspectives. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.Z.; Chen, Z.; Sidell, M.A.; Eckel, S.P.; Martinez, M.P.; Lurmann, F.; Thomas, D.C.; Gilliland, F.D.; Xiang, A.H. Asthma Disease Status, COPD, and COVID-19 Severity in a Large Multiethnic Population. J. Allergy Clin. Immunol. Pract. 2021, 9, 3621–3628.e2. [Google Scholar] [CrossRef]
- Orioli, L.; Hermans, M.P.; Thissen, J.P.; Maiter, D.; Vandeleene, B.; Yombi, J.C. COVID-19 in diabetic patients: Related risks and specifics of management. Ann. Endocrinol. 2020, 81, 101–109. [Google Scholar] [CrossRef]
- Kawai, K.; Yawn, B.P. Risk Factors for Herpes Zoster: A Systematic Review and Meta-analysis. Mayo Clin. Proc. 2017, 92, 1806–1821. [Google Scholar] [CrossRef] [Green Version]
- Hata, A.; Kuniyoshi, M.; Ohkusa, Y. Risk of Herpes zoster in patients with underlying diseases: A retrospective hospital-based cohort study. Infection 2011, 39, 537–544. [Google Scholar] [CrossRef] [Green Version]
- Hudson, D.; Khanna, R.; Brahmania, M.; Qumosani, K.; Teriaky, A. A225 Vaccine-Preventable Diseases in Hospitalized Patients with End-Stage Liver Disease/Cirrhosis: A Nationwide Cohort Analysis. J. Can. Assoc. Gastroenterol. 2022, 5, 115–116. [Google Scholar] [CrossRef]
- Vink, P.; Delgado Mingorance, I.; Maximiano Alonso, C.; Rubio-Viqueira, B.; Jung, K.H.; Rodriguez Moreno, J.F.; Grande, E.; Marrupe Gonzalez, D.; Lowndes, S.; Puente, J.; et al. Immunogenicity and safety of the adjuvanted recombinant zoster vaccine in patients with solid tumors, vaccinated before or during chemotherapy: A randomized trial. Cancer 2019, 125, 1301–1312. [Google Scholar] [CrossRef] [Green Version]
- Tanriover, M.D.; Soyler, C.; Ascioglu, S.; Cankurtaran, M.; Unal, S. Low seroprevalance of diphtheria, tetanus and pertussis in ambulatory adult patients: The need for lifelong vaccination. Eur. J. Intern. Med. 2014, 25, 528–532. [Google Scholar] [CrossRef]
- Mbayei, S.A.; Faulkner, A.; Miner, C.; Edge, K.; Cruz, V.; Pena, S.A.; Kudish, K.; Coleman, J.; Pradhan, E.; Thomas, S.; et al. Severe Pertussis Infections in the United States, 2011–2015. Clin. Infect. Dis. 2019, 69, 218–226. [Google Scholar] [CrossRef] [Green Version]
- Macina, D.; Evans, K.E. Pertussis in Individuals with Co-morbidities: A Systematic Review. Infect. Dis. Ther. 2021, 10, 1141–1170. [Google Scholar] [CrossRef]
- Grasse, M.; Meryk, A.; Schirmer, M.; Grubeck-Loebenstein, B.; Weinberger, B. Booster vaccination against tetanus and diphtheria: Insufficient protection against diphtheria in young and elderly adults. Immun. Ageing 2016, 13, 26. [Google Scholar] [CrossRef] [Green Version]
- Weinberger, B. Adult vaccination against tetanus and diphtheria: The European perspective. Clin. Exp. Immunol. 2017, 187, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Weinberger, B.; Schirmer, M.; Matteucci Gothe, R.; Siebert, U.; Fuchs, D.; Grubeck-Loebenstein, B. Recall responses to tetanus and diphtheria vaccination are frequently insufficient in elderly persons. PLoS ONE 2013, 8, e82967. [Google Scholar] [CrossRef] [Green Version]
- He, Q.; Gao, H.; Gao, M.; Qi, S.; Zhang, Y.; Wang, J. Anti-Gastrins Antiserum Combined with Lowered Dosage Cytotoxic Drugs to Inhibit the Growth of Human Gastric Cancer SGC7901 Cells in Nude Mice. J. Cancer 2015, 6, 448–456. [Google Scholar] [CrossRef] [Green Version]
- Wong, L.P.; Wong, P.F.; AbuBakar, S. Vaccine hesitancy and the resurgence of vaccine preventable diseases: The way forward for Malaysia, a Southeast Asian country. Hum. Vaccines Immunother. 2020, 16, 1511–1520. [Google Scholar] [CrossRef]
- Siani, A. Measles outbreaks in Italy: A paradigm of the re-emergence of vaccine-preventable diseases in developed countries. Prev. Med. 2019, 121, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Marquis, S.R.; Logue, J.K.; Chu, H.Y.; Loeffelholz, T.; Quinn, Z.Z.; Liu, C.; Stewart, F.M.; Carpenter, P.A.; Pergam, S.A.; Krantz, E.M. Seroprevalence of Measles and Mumps Antibodies Among Individuals With Cancer. JAMA Netw. Open 2021, 4, e2118508. [Google Scholar] [CrossRef]
- Yong, M.; Parkinson, K.; Goenka, N.; O’Mahony, C. Diabetes and genital warts: An unhappy coalition. Int. J. STD AIDS 2010, 21, 457–459. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Illana, E.; Lopez-Lacort, M.; Navarro-Illana, P.; Vilata, J.J.; Diez-Domingo, J. Effectiveness of HPV vaccines against genital warts in women from Valencia, Spain. Vaccine 2017, 35, 3342–3346. [Google Scholar] [CrossRef] [PubMed]
- Rhee, Y.; Sha, B.E.; Santos, C.A.Q. Optimizing Vaccination in Adult Patients With Liver Disease and Liver Transplantation. Clin. Liver Dis. 2020, 15, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammerquist, R.J.; Messerschmidt, K.A.; Pottebaum, A.A.; Hellwig, T.R. Vaccinations in asplenic adults. Am. J. Health Syst. Pharm. 2016, 73, e220–e228. [Google Scholar] [CrossRef]
- Tsang, V. Vaccination recommendations for the hematology and oncology and post-stem cell transplant populations. J. Adv. Pract. Oncol. 2012, 3, 71–83. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishak, A.R.; Hsieh, Y.C.; Srinivasan, H.; See, K.C. Review of Vaccination Recommendations in Guidelines for Non-Communicable Diseases with Highest Global Disease Burden among Adults 75 Years Old and Above. Vaccines 2023, 11, 1076. https://doi.org/10.3390/vaccines11061076
Ishak AR, Hsieh YC, Srinivasan H, See KC. Review of Vaccination Recommendations in Guidelines for Non-Communicable Diseases with Highest Global Disease Burden among Adults 75 Years Old and Above. Vaccines. 2023; 11(6):1076. https://doi.org/10.3390/vaccines11061076
Chicago/Turabian StyleIshak, Abdul Rahman, Yu Chun Hsieh, Harshitha Srinivasan, and Kay Choong See. 2023. "Review of Vaccination Recommendations in Guidelines for Non-Communicable Diseases with Highest Global Disease Burden among Adults 75 Years Old and Above" Vaccines 11, no. 6: 1076. https://doi.org/10.3390/vaccines11061076