
A Systematic Review on the Safety and Efficacy of COVID-19 Vaccines Approved in Saudi Arabia
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
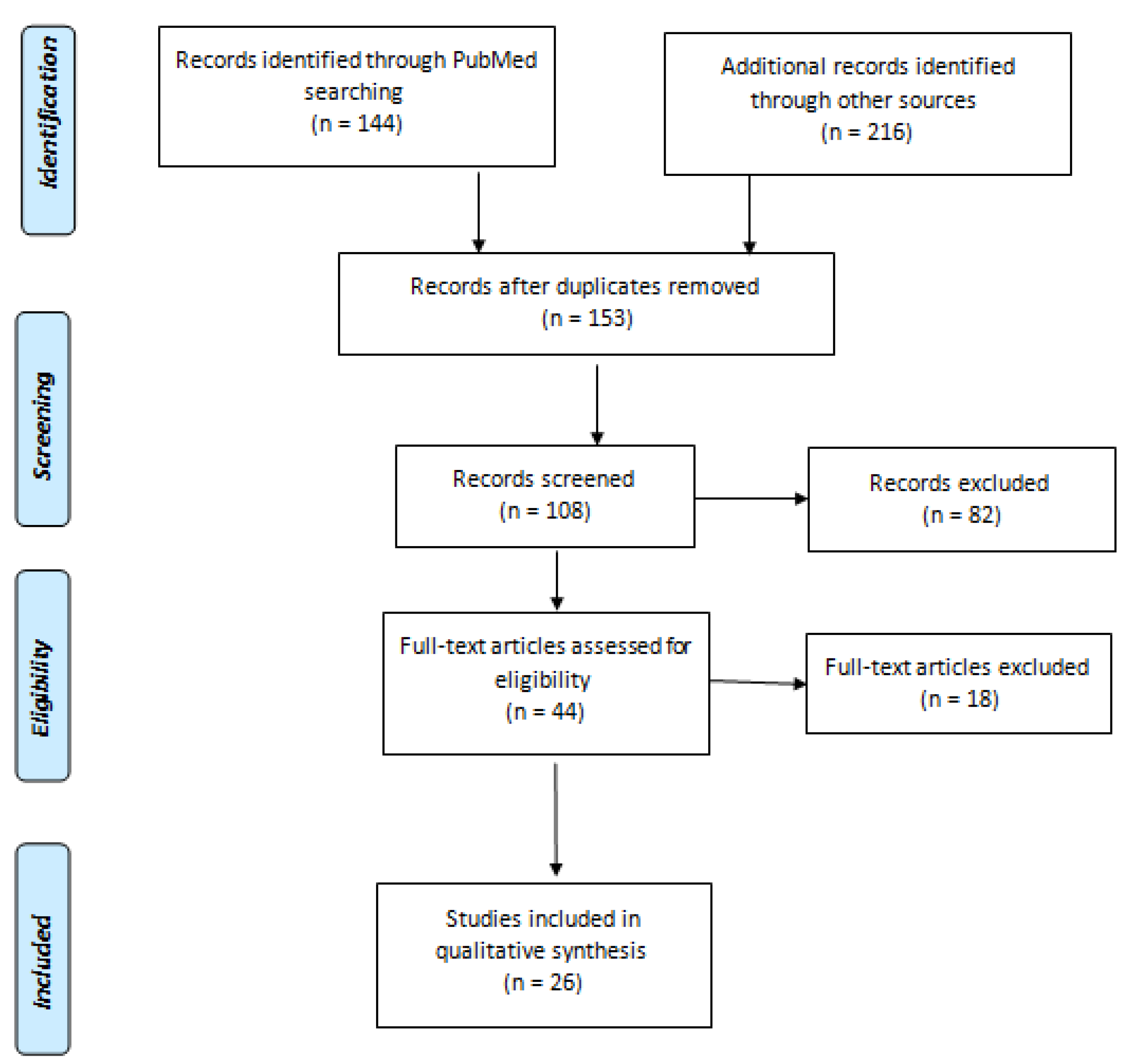
2.1. Literature Search Strategy
2.2. Study Selection
2.3. Eligibility Criteria
- Articles are written in the English language containing detailed information about the type of COVID-19 vaccines and the number of volunteers with their consent.
- Cross-sectional studies that were published in the last three years (2019–2022).
- Studies in which human volunteers were used for COVID-19 vaccine testing.
- Studies evaluating the safety and efficacy of the COVID-19 vaccine, including the dose, duration, presence of adverse reactions, and a clear procedure to determine the effectiveness.
- Published articles in reputed journals giving comprehensive information about statistics and their significance.
2.4. Data Extraction
2.5. Quality Assessment
3. Results
3.1. Extraction of the Scientific Data for the Approved COVID-19 Vaccines
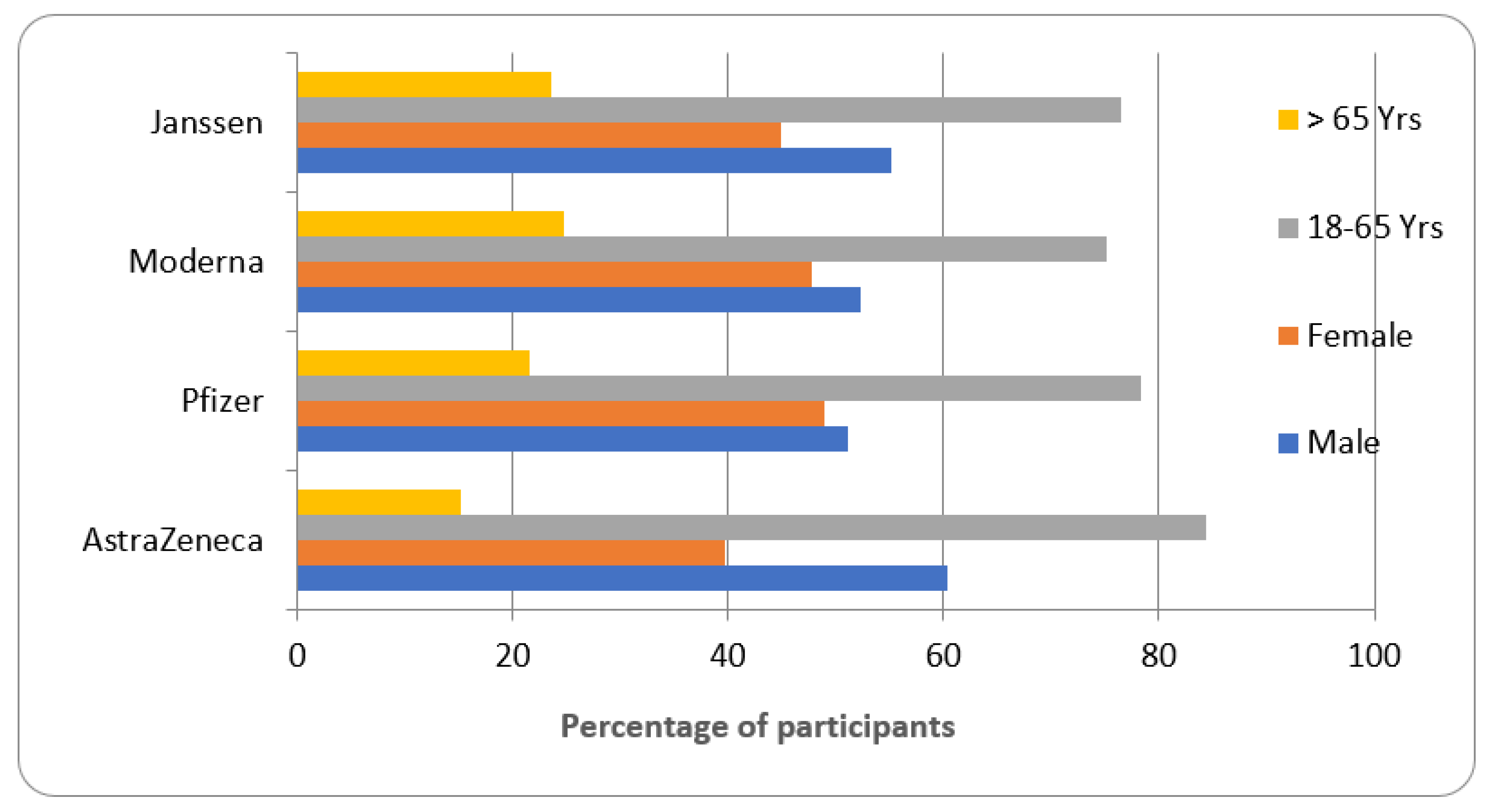
3.2. Characteristics of Participants Enrolled for COVID-19 Vaccines Testing [22,23,24,25]
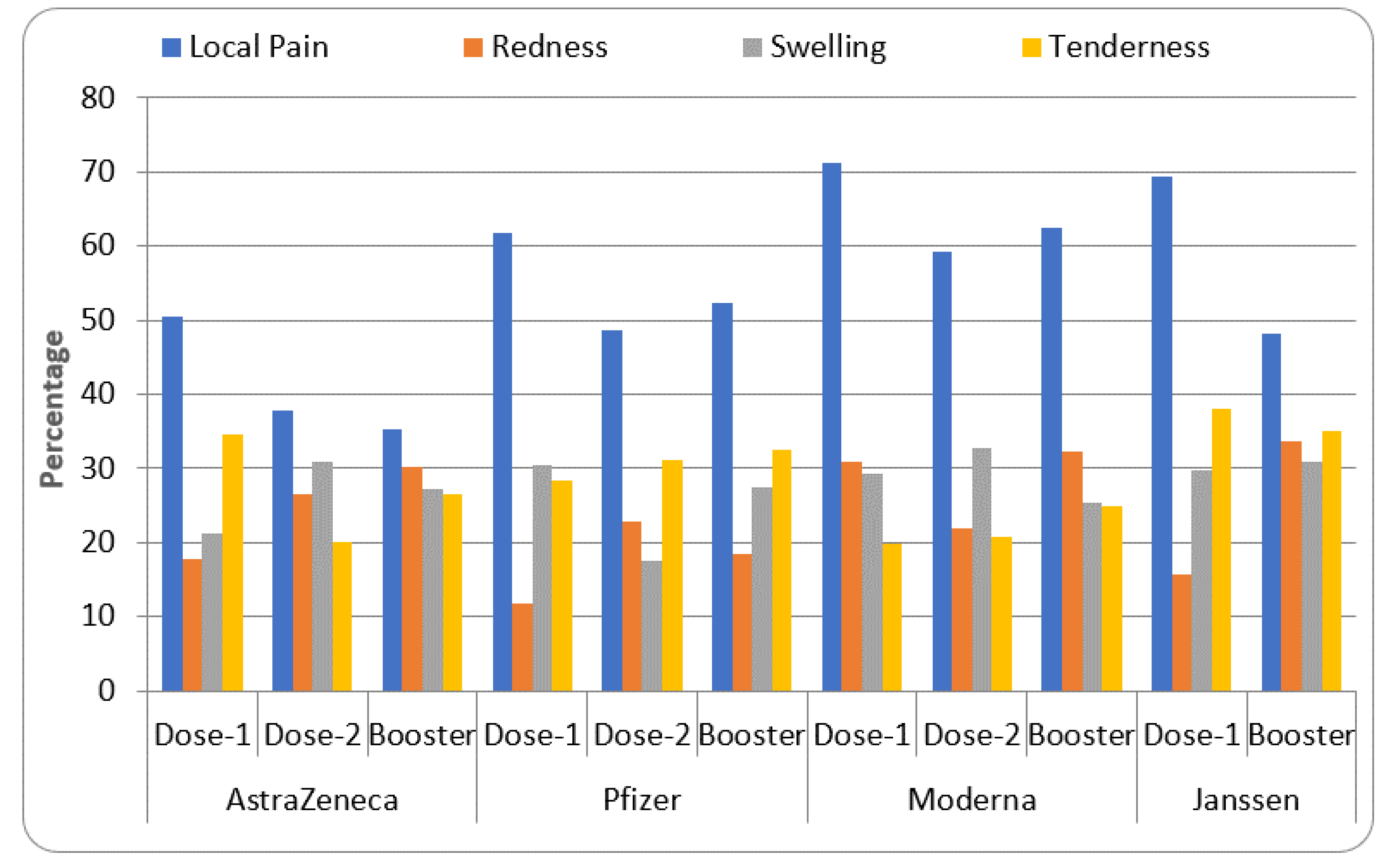
3.3. Common Local Reactions after COVID-19 Vaccination [26,27,28,29,30,31,32,33]
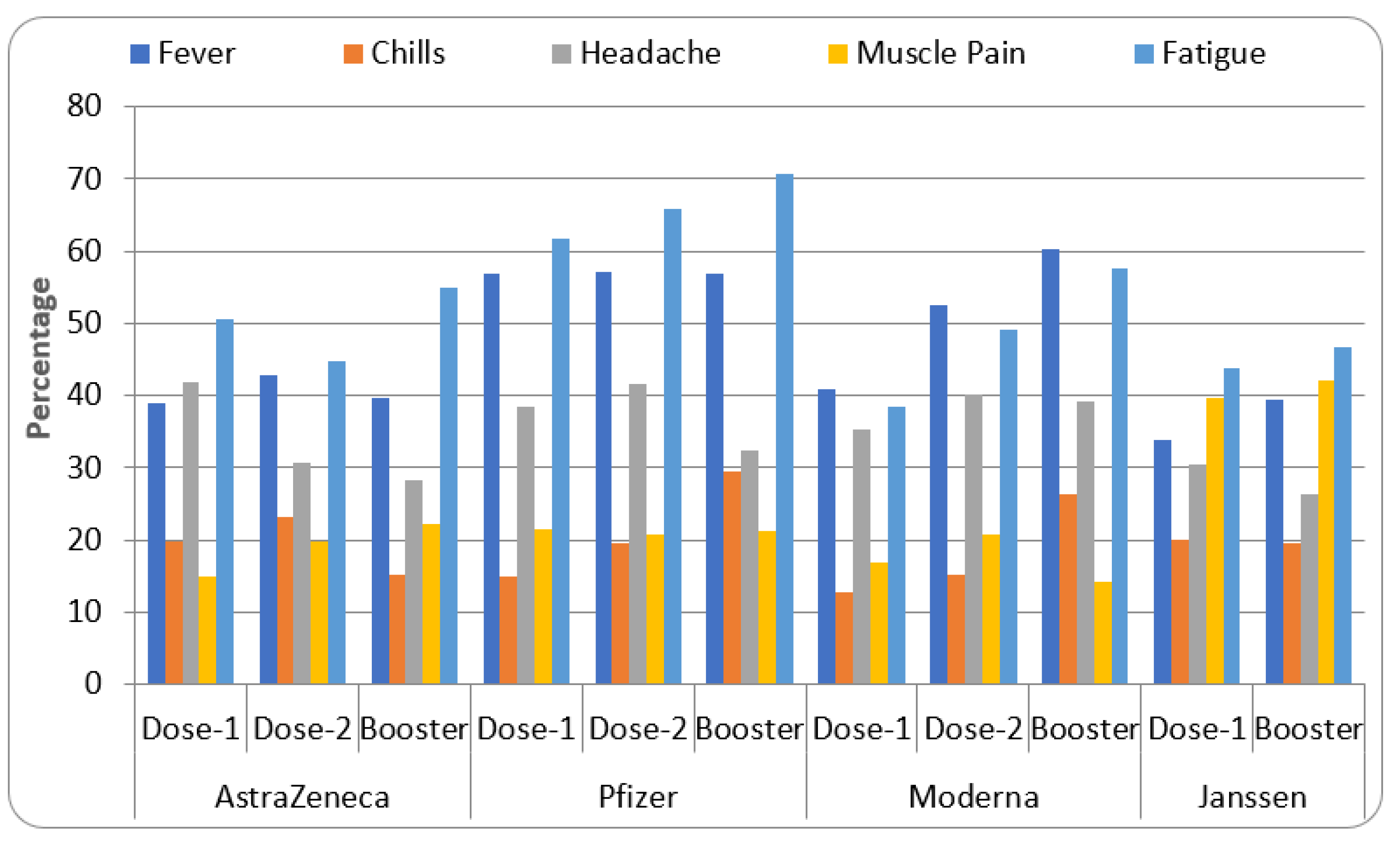
3.4. Common System Reactions after COVID-19 Vaccination [27,29,32,34,35,36]
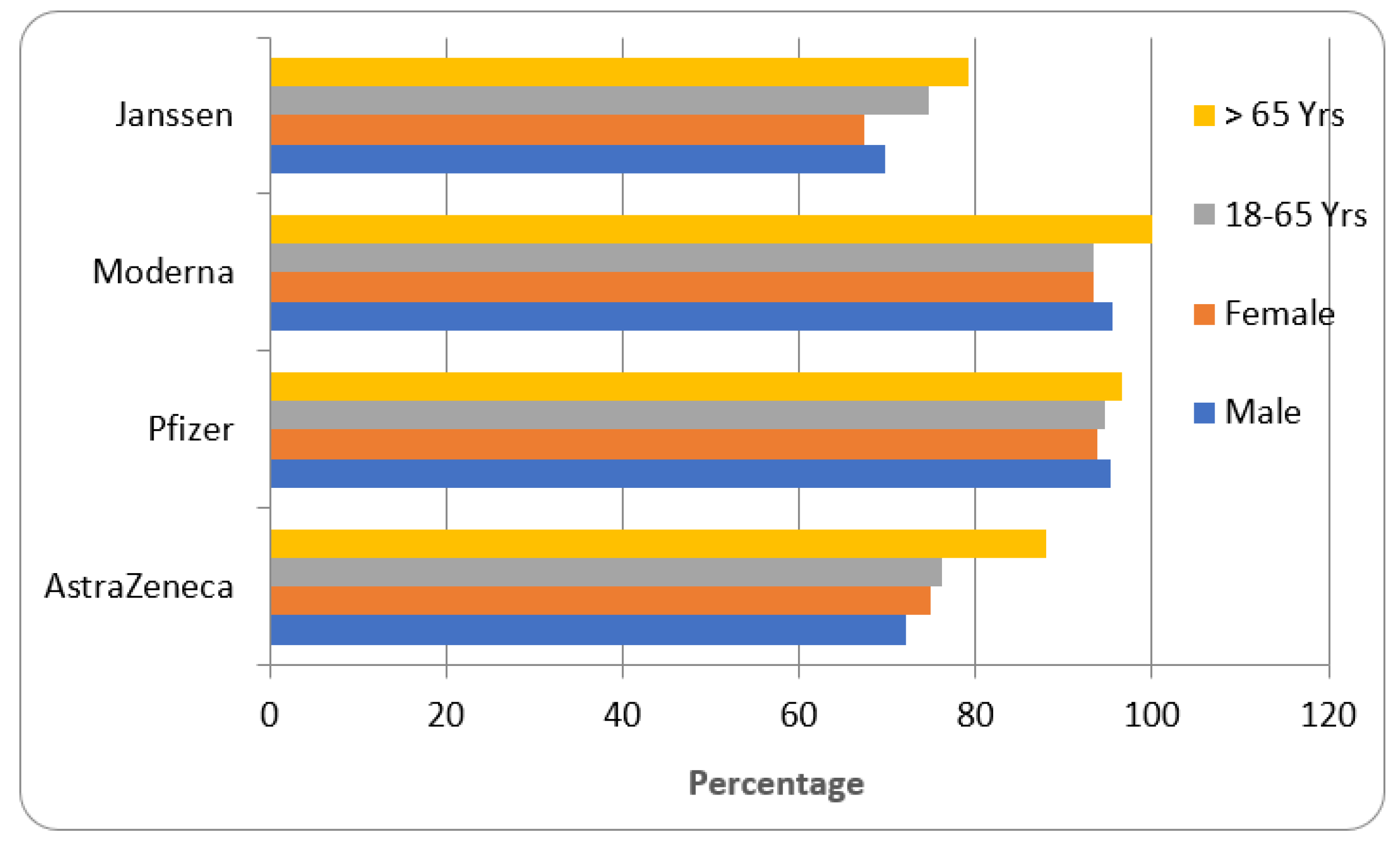
3.5. Efficacy of COVID-19 Vaccine in Different Groups of Participants [26,28,30,33,37,38,39]
4. Discussion
5. Conclusions
6. Future Implication and Limitation of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiat. 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Sanders, J.; Monogue, M.; Jodlowski, T.; Cutrell, J. Pharmacologic Treatments for Coronavirus Disease 2019 (COVID-19). JAMA 2020, 18, 1824–1837. [Google Scholar] [CrossRef]
- Pandey, A.; Belbase, P.; Parajuli, A. COVID-19, Vaccine Development to Vaccination. J. Nepal Health Res. Council. 2021, 18, 807–809. [Google Scholar] [CrossRef]
- Conklin, L.; Hviid, A.; Orenstein, W.A.; Pollard, A.J.; Wharton, M.; Zuber, P. Vaccine safety issues at the turn of the 21st century. BMJ Glob. Health 2021, 6, e004898. [Google Scholar] [CrossRef]
- Brüssow, H.; Zuber, S. Can a combination of vaccination and face mask wearing contain the COVID-19 pandemic? Microb. Biotechnol. 2022, 15, 721–737. [Google Scholar] [CrossRef]
- Asdaq, S.M.B.; Rabbani, S.I.; Alshammari, M.K.; Alshammari, R.S.; Kamal, M.; Imran, M.; AlShammari, N.A.; Al Twallah, M.F.; Alshahrani, A.H. Burden of COVID-19: A preliminary analysis in the population of Saudi Arabia. PeerJ 2022, 10, e13219. [Google Scholar] [CrossRef]
- Shukla, V.V.; Shah, R.C. Vaccinations in Primary Care. Indian J. Pediatr. 2018, 85, 1118–1127. [Google Scholar] [CrossRef]
- Yu, Y.B.; Taraban, M.B.; Wang, W.; Briggs, K.T. Improving Biopharmaceutical Safety through Verification-Based Quality Control. Trends Biotechnol. 2017, 5, 1140–1155. [Google Scholar] [CrossRef]
- Prüβ, B.M. Current State of the First COVID-19 Vaccines. Vaccines 2021, 9, 30. [Google Scholar] [CrossRef]
- Food And Drug Administration. Ensuring the Safety of Vaccines in the United States. 2011. Available online: https://www.fda.gov/files/vaccinesEnsuring-the-Safety-of-Vaccines-in-the-United-States.pdf (accessed on 28 March 2022).
- Food and Drug Administration. FDA NEWS RELEASE FDA Takes Key Action in Fight Against COVID-19 by Issuing Emergency Use Authorization for First COVID-19 Vaccine Action Follows Thorough Evaluation of Available Safety, Effectiveness, and Manufacturing Quality Information by FDA Career Scientists, Input from Independent Experts. US FDA. 2020. Available online: https://www.fda.gov/news-events/press-announcements/fda-takes-key-action-fight-against-COVID-19-issuing-emergency-use-authorization-first-COVID-19 (accessed on 26 January 2022).
- Gallagher, J. COVID-19: Seven UK Blood Clot Deaths after AstraZeneca Vaccine. BBC News. 2021. Available online: https://www.bbc.com/news/health-56620646 (accessed on 30 April 2022).
- Hayes, P. Blood-clot Death “Likely” Linked to AstraZeneca COVID Vaccine. Reuters News. 2021. Available online: https://www.reuters.com/business/healthcare-pharmaceuticals/australia-reports-first-death-blood-clots-likely-linked-astrazeneca-vaccine-2021-04-16/ (accessed on 30 March 2022).
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A.A. Global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef]
- Hernández, A.; Calina, D.; Poulas, K.; Docea, A.; Tsatsakis, A. Safety of COVID-19 vaccines administered in the EU: Should we be concerned? Toxicol. Rep. 2021, 8, 871–879. [Google Scholar] [CrossRef] [PubMed]
- Tam, W.W.S.; Tang, A.; Woo, B.; Goh, S.Y.S. Perception of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement of authors publishing reviews in nursing journals: A cross-sectional online survey. BMJ Open. 2019, 9, 026271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, K.S.; Kunz, R.; Kleijnen, J.; Antes, G. Five steps to conducting a systematic review. J. R. Soc. Med. 2003, 96, 118–121. [Google Scholar] [CrossRef]
- Ministry of Health, Saudi Arabia. Approved COVID-19 Vaccines in Saudi Arabia. Available online: https://www.moh.gov.sa/awarenessplateform/VariousTopics/Documents/COVID-19Vaccine-English.pdf (accessed on 20 February 2022).
- Ahn, E.J.; Kang, H. Introduction to systematic review and meta-analysis. Korean J. Anesthesiol. 2018, 71, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 5, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Cirillo, N. Reported orofacial adverse effects of COVID-19 vaccines: The knowns and the unknowns. J. Oral Pathol. Med. 2021, 50, 424–427. [Google Scholar] [CrossRef]
- Ebrahimi, N.; Aslani, S.; Babaie, F.; Hemmatzadeh, M.; Hosseinzadeh, R. Recent findings on the Coronavirus disease 2019 (COVID-19); immunopathogenesis and immunotherapeutics. Int. Immunopharmacol. 2020, 89, 107082. [Google Scholar] [CrossRef]
- Tande, A.J.; Pollock, B.D.; Shah, N.D.; Farrugia, G.; Virk, A.; Melanie, S.; Laura, B.; Matthew, B.; Elie, F.B. Impact of the COVID-19 Vaccine on Asymptomatic Infection Among Patients Undergoing Pre-Procedural COVID-19 Molecular Screening. Clin. Infect. Dis. 2021, 42, 388–391. [Google Scholar]
- Aliabadi, F.; Ajami, M.; Pazoki–Toroudi, H. Why does COVID-19 pathology have several clinical forms? BioEssays 2020, 42, 2000198. [Google Scholar] [CrossRef]
- Akira, S.; Hemmi, H. Recognition of pathogen-associated molecular patterns by TLR family. Immunol. Lett. 2003, 85, 85–95. [Google Scholar] [CrossRef] [PubMed]
- AlAnoud, T.R.; Alshamsan, A.; Al-jedai, A. Current COVID-19 vaccine candidates: Implications in the Saudi population. Saudi Pharm. J. 2020, 28, 1743–1748. [Google Scholar]
- Tanaka, K. In Connection with the Evaluation of mRNA Vaccine against COVID-19. Three Proposals to Prevent New Coronavirus Infections (Project report) 2021. Available online: www.publication/In_connection_with_the_evaluation_of_mRNA_vaccine_against_COVID-19 (accessed on 25 April 2022).
- Walsh, E.E.; Frenck Jr, R.W.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. NEJM 2020, 14, 1–13. [Google Scholar] [CrossRef]
- Hassine, H.I. Covid-19 vaccines and variants of concern: A review. Rev. Med. Virol. 2022, 32, e2313. [Google Scholar] [CrossRef]
- Francis, A.I.; Ghany, S.; Gilkes, T.; Umakanthan, S. Review of COVID-19 vaccine subtypes, efficacy and geographical distributions. Postgrad. Med. J. 2022, 98, 389–394. [Google Scholar] [CrossRef]
- Rashedi, R.; Samieefar, N.; Masoumi, N.; Mohseni, S.; Rezaei, N. COVID-19 vaccines mix-and-match: The concept, the efficacy and the doubts. J. Med. Virol. 2022, 94, 1294–1299. [Google Scholar] [CrossRef]
- Altmann, D.M.; Boyton, R.J. COVID-19 vaccination: The road ahead. Science 2022, 375, 1127–1132. [Google Scholar] [CrossRef]
- Mejren, A.; Sørensen, C.M.; Gormsen, L.C.; Tougaard, R.S.; Nielsen, B.D. Large-vessel giant cell arteritis after COVID-19 vaccine. Scand. J. Rheumatol. 2022, 51, 154–155. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Kamiya, H.; Inoshima, I.; Hirasawa, Y.; Tago, O.; Arai, M. COVID-19 mRNA Vaccine-induced Pneumonitis. Intern. Med. 2022, 61, 81–86. [Google Scholar] [CrossRef]
- Lee, A.C.K.; Morling, J.R. COVID-19 vaccine dilemmas. Public Health 2022, 202, 10–11. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines. 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Shao, W.; Chen, X.; Zhang, B.; Wang, G.; Zhang, W. Real-world effectiveness of COVID-19 vaccines: A literature review and meta-analysis. Int. J. Infect. Dis. 2022, 114, 252–260. [Google Scholar] [CrossRef]
- Lombardi, A.; Bozzi, G.; Ungaro, R.; Villa, S.; Castelli, V.; Mangioni, D.; Muscatello, A.; Gori, A.; Bandera, A. Mini Review Immunological Consequences of Immunization With COVID-19 mRNA Vaccines: Preliminary Results. Front. Immunol. 2021, 12, 1–11. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention (CDC). Information on Pfizer COVID-19 Vaccines. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/Pfizer-BioNTech.html (accessed on 30 March 2022).
- Center for Disease Control and Prevention (CDC). Information on Moderna COVID-19 Vaccines. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/Moderna.html (accessed on 30 March 2022).
- Center for Disease Control and Prevention (CDC). Information on Janssen COVID-19 Vaccines. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/janssen.html (accessed on 30 March 2022).
- Guidelines for Taking Booster Dose in Saudi Arabia. Available online: https://covid19.cdc.gov.sa/professionals-health-workers/interim-guidelines-for-the-use-of-sars-cov-2-vaccine/ (accessed on 26 January 2023).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | AstraZeneca [12,25,34] | Pfizer [15,22,30,32] | Moderna [11,21,32,35] | Janssen [8,36,39] |
|---|---|---|---|---|
| Vaccine type | Vector-based | RNA-based | RNA-based | Vector-based |
| Manufacturing country | UK | US | US | The Netherlands/US |
| Dose | 0.5 mL | 0.3 mL | 0.5 mL | 0.5 mL |
| Number of dose and suggested duration between them * | 2 (28 days) | 2 (21 days) | 2 (28 days) | Single dose |
| Route of administration | Intra-muscular (Preferably deltoid muscle) | Intra-muscular (Preferably deltoid muscle) | Intra-muscular (Preferably deltoid muscle) | Intra-muscular (Preferably deltoid muscle) |
| Mechanism of action | Adenovirus is used as a vector to carry the genetic code for making viral spike protein by host cells, triggering antibody production. | m-RNA induces the host cell to produce spike proteins, triggering the production of immune cells. | m-RNA induces the host cell to produce spike proteins, triggering the production of immune cells. | Adenovirus is used as a vector to carry the genetic code for making viral spike protein by host cells, triggering antibody production. |
| Protection post-vaccination | Significant antibody levels can be seen after 14 days | Significant antibody level in blood after 14 days | Significant antibody level in blood after 14 days | Significant antibody level in blood after 14 days |
| High risk participants | Patients suffering from cardiovascular, respiratory, metabolic, hepatic, renal, haematological and immunocompromised conditions | |||
| Storage temperature | 2 to 8 °C | −20 to −70 °C | 2 to 8 °C | 2 to 8 °C |
| Specific adverse events | Thrombosis, Anaphylaxis | Lymphadenopathy, Myocarditis | Cholecystitis, Myocardial infarction | Hypersensitivity, Appendicitis |
| Precautions | Pregnancy, lactation, less than 18 years, severe illness and allergic to vaccine components | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhandod, T.A.; Rabbani, S.I.; Almuqbil, M.; Alshehri, S.; Hussain, S.A.; Alomar, N.F.; Mir, M.A.; Asdaq, S.M.B. A Systematic Review on the Safety and Efficacy of COVID-19 Vaccines Approved in Saudi Arabia. Vaccines 2023, 11, 281. https://doi.org/10.3390/vaccines11020281
Alhandod TA, Rabbani SI, Almuqbil M, Alshehri S, Hussain SA, Alomar NF, Mir MA, Asdaq SMB. A Systematic Review on the Safety and Efficacy of COVID-19 Vaccines Approved in Saudi Arabia. Vaccines. 2023; 11(2):281. https://doi.org/10.3390/vaccines11020281
Chicago/Turabian StyleAlhandod, Thekra Ali, Syed Imam Rabbani, Mansour Almuqbil, Sultan Alshehri, Syed Arif Hussain, Nasser Fawzan Alomar, Manzoor Ahmad Mir, and Syed Mohammed Basheeruddin Asdaq. 2023. "A Systematic Review on the Safety and Efficacy of COVID-19 Vaccines Approved in Saudi Arabia" Vaccines 11, no. 2: 281. https://doi.org/10.3390/vaccines11020281