
Effectiveness of COVID-19 Vaccination with mRNA Vaccines for Patients with Cirrhosis in Hungary: Multicentre Matched Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
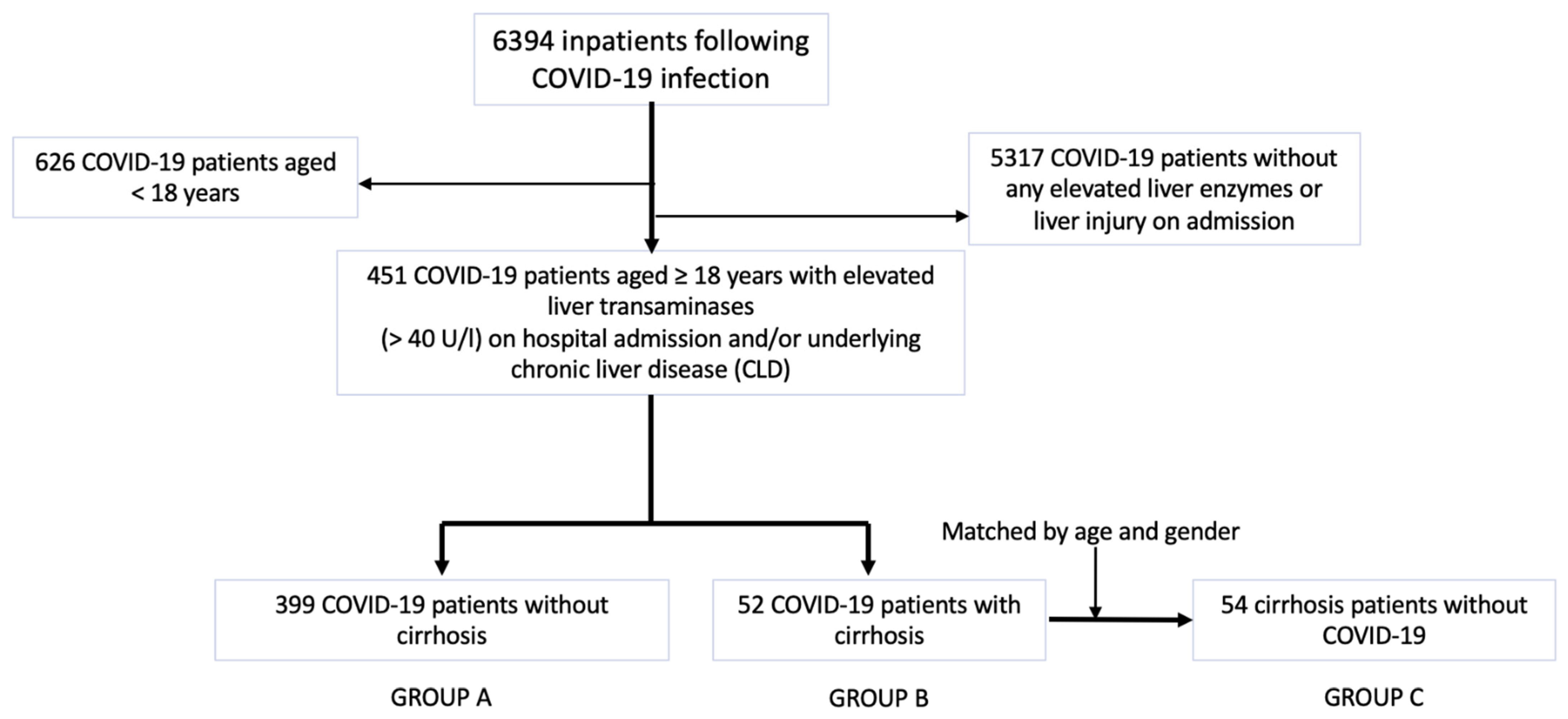
2.1. Patient Cohorts
2.2. Data Collection
2.3. Liver Cirrhosis Severity
2.4. COVID-19 Vaccines
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
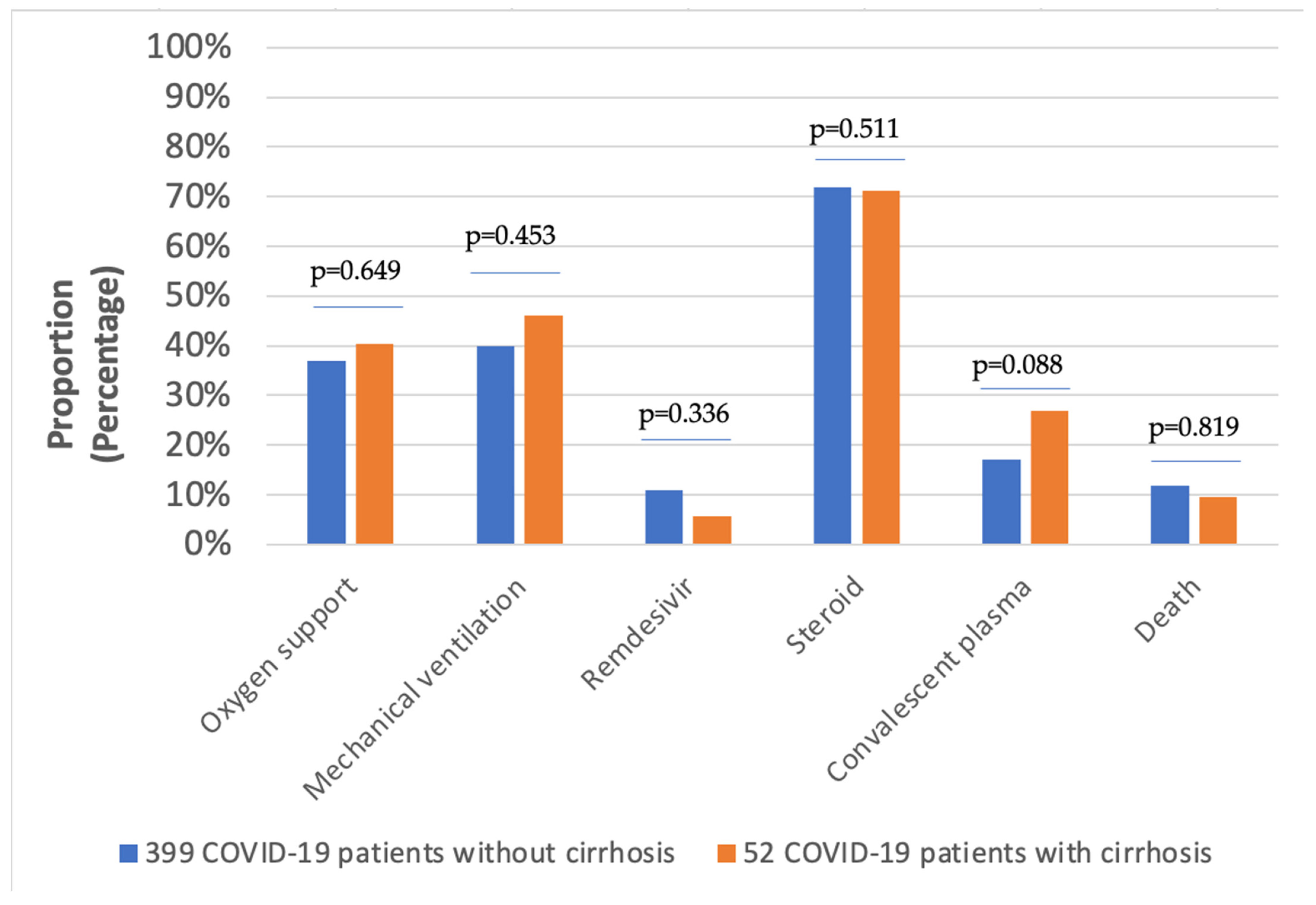
3.2. Hospital Outcomes
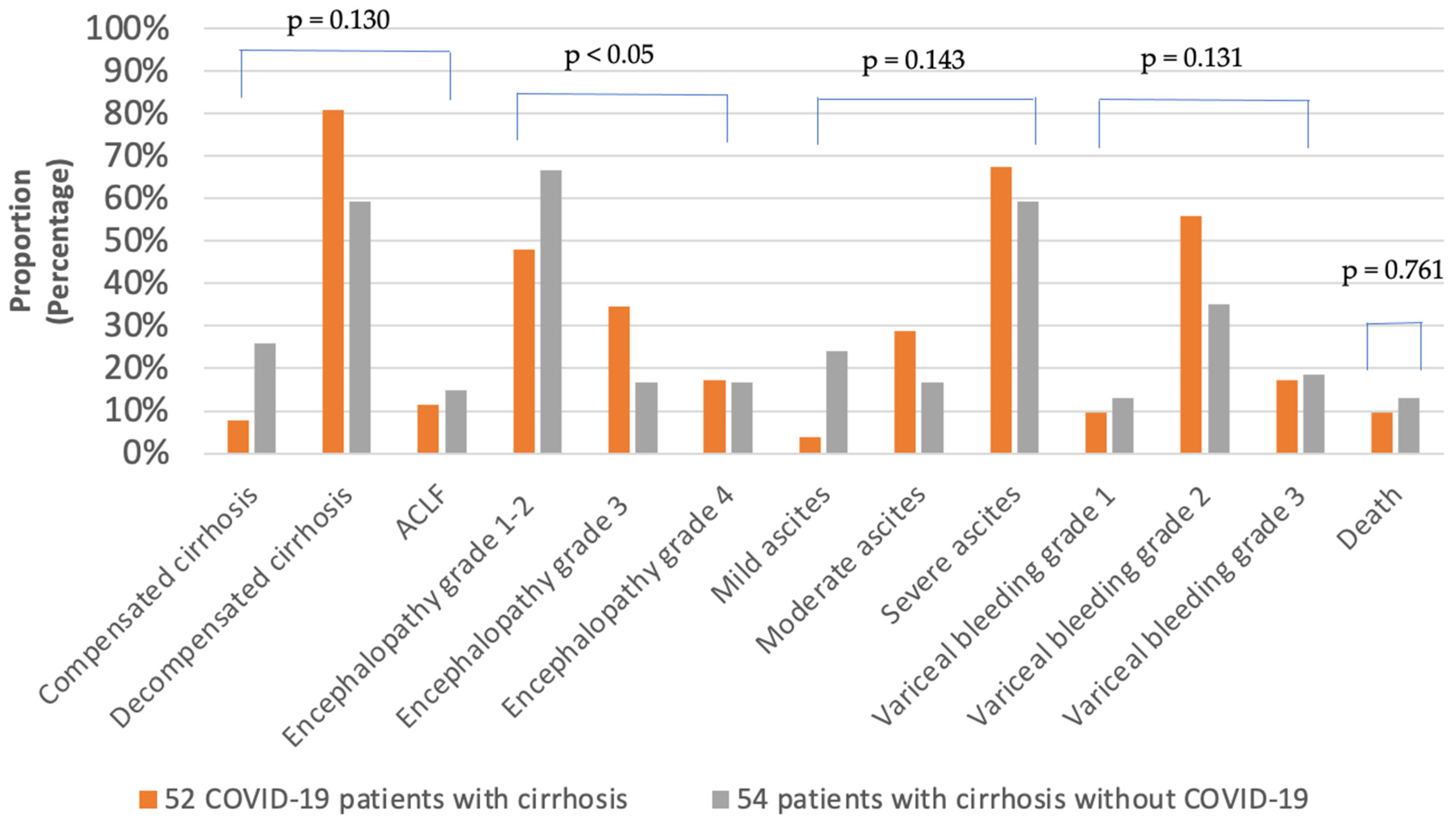
3.3. Clinical Characteristics of Patients with Cirrhosis
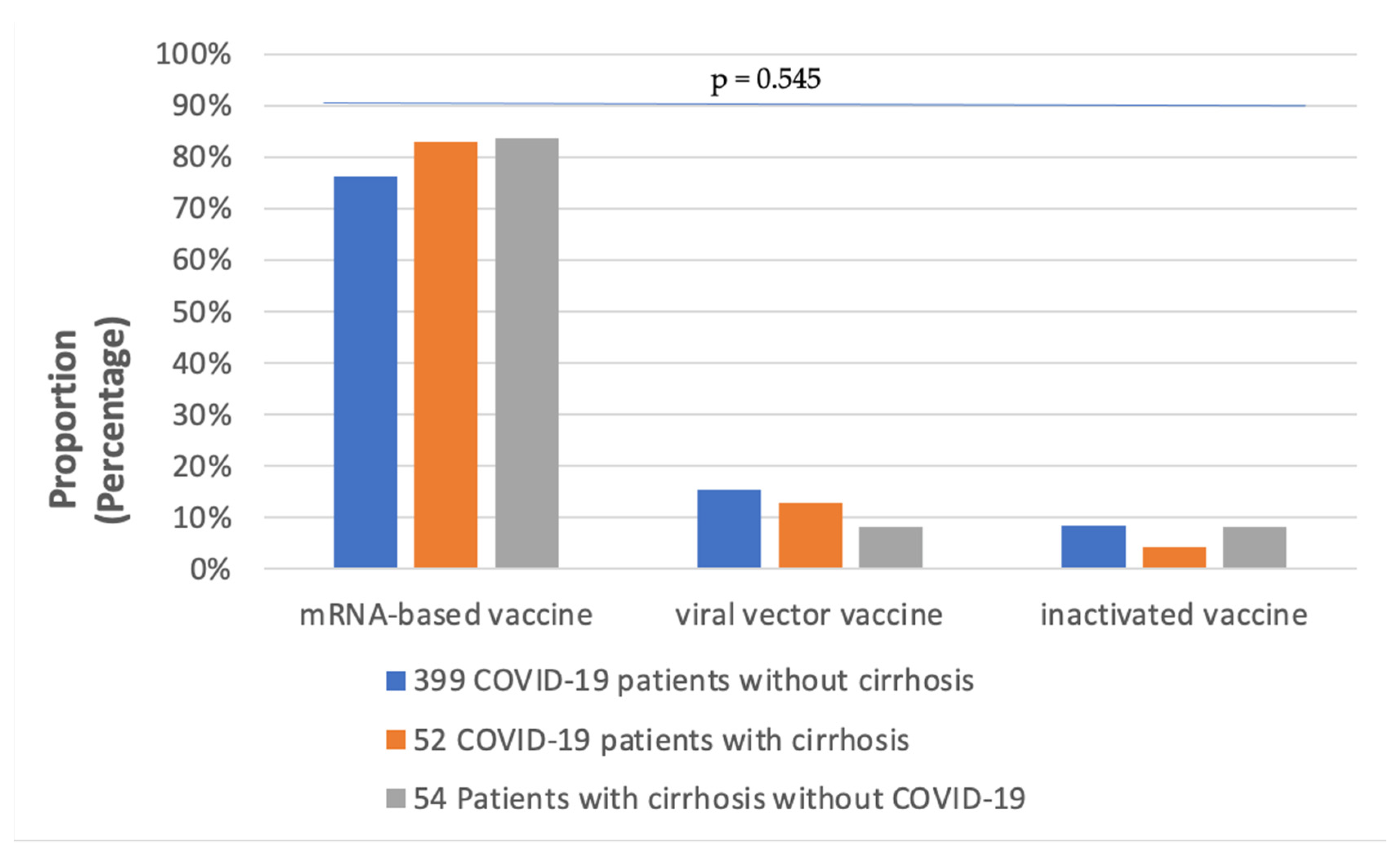
3.4. COVID-19 Vaccination
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Coronavirus disease 2019 | (COVID-19) |
| interquartile range | (IQR) |
| acute-on-chronic liver failure | (ACLF) |
| cirrhosis-associated immune dysfunction | (CAID) |
| high-resolution computer tomography | (HRCT) |
References
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Marjot, T.; Moon, A.M.; Cook, J.A.; Abd-Elsalam, S.; Aloman, C.; Armstrong, M.J.; Pose, E.; Brenner, E.J.; Cargill, T.; Catana, M.A.; et al. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: An international registry study. J. Hepatol. 2021, 74, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Marjot, T.; Eberhardt, C.S.; Boettler, T.; Belli, L.S.; Berenguer, M.; Buti, M.; Jalan, R.; Mondelli, M.U.; Moreau, R.; Shouval, D.; et al. Impact of COVID-19 on the liver and on the care of patients with chronic liver disease, hepatobiliary cancer, and liver transplantation: An updated EASL position paper. J. Hepatol. 2022, 77, 1161–1197. [Google Scholar] [CrossRef]
- Sarin, S.K.; Choudhury, A.; Lau, G.K.; Zheng, M.H.; Ji, D.; Abd-Elsalam, S.; Hwang, J.; Qi, X.; Cua, I.H.; Suh, J.I.; et al. Pre-existing liver disease is associated with poor outcome in patients with SARS-CoV2 infection; The APCOLIS Study (APASL COVID-19 Liver Injury Spectrum Study). Hepatol. Int. 2020, 14, 690–700. [Google Scholar] [CrossRef]
- Iavarone, M.; D’Ambrosio, R.; Soria, A.; Triolo, M.; Pugliese, N.; Del Poggio, P.; Perricone, G.; Massironi, S.; Spinetti, A.; Buscarini, E.; et al. High rates of 30-day mortality in patients with cirrhosis and COVID-19. J. Hepatol. 2020, 73, 1063–1071. [Google Scholar] [CrossRef]
- Kim, D.; Adeniji, N.; Latt, N.; Kumar, S.; Bloom, P.P.; Aby, E.S.; Perumalswami, P.; Roytman, M.; Li, M.; Vogel, A.S.; et al. Predictors of Outcomes of COVID-19 in Patients With Chronic Liver Disease: US Multi-center Study. Clin. Gastroenterol. Hepatol. 2021, 19, 1469–1479.e19. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Garcia-Tsao, G.; Biggins, S.W.; Kamath, P.S.; Wong, F.; McGeorge, S.; Shaw, J.; Pearson, M.; Chew, M.; Fagan, A.; et al. Comparison of mortality risk in patients with cirrhosis and COVID-19 compared with patients with cirrhosis alone and COVID-19 alone: Multicentre matched cohort. Gut 2021, 70, 531–536. [Google Scholar] [CrossRef]
- Marjot, T.; Webb, G.J.; Barritt, A.S.; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: Mechanistic and clinical perspectives. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Patel, M.M.; Ginde, A.A.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; Gaglani, M.; McNeal, T.; et al. Effectiveness of SARS-CoV-2 mRNA Vaccines for Preventing COVID-19 Hospitalizations in the United States. medRxiv 2021. [Google Scholar] [CrossRef]
- John, B.V.; Deng, Y.; Schwartz, K.B.; Taddei, T.H.; Kaplan, D.E.; Martin, P.; Chao, H.H.; Dahman, B. Postvaccination COVID-19 infection is associated with reduced mortality in patients with cirrhosis. Hepatology 2022, 76, 126–138. [Google Scholar] [CrossRef]
- Müller, V.; Polivka, L.; Valyi-Nagy, I.; Nagy, A.; Szekanecz, Z.; Bogos, K.; Vago, H.; Kamondi, A.; Fekete, F.; Szlavik, J.; et al. Booster Vaccination Decreases 28-Day All-Cause Mortality of the Elderly Hospitalized Due to SARS-CoV-2 Delta Variant. Vaccines 2022, 10, 986. [Google Scholar] [CrossRef] [PubMed]
- Bakasis, A.D.; Bitzogli, K.; Mouziouras, D.; Pouliakis, A.; Roumpoutsou, M.; Goules, A.V.; Androutsakos, T. Antibody Responses after SARS-CoV-2 Vaccination in Patients with Liver Diseases. Viruses 2022, 14, 207. [Google Scholar] [CrossRef] [PubMed]
- Willuweit, K.; Frey, A.; Passenberg, M.; Korth, J.; Saka, N.; Anastasiou, O.E.; Möhlendick, B.; Schütte, A.; Schmidt, H.; Rashidi-Alavijeh, J. Patients with Liver Cirrhosis Show High Immunogenicity upon COVID-19 Vaccination but Develop Premature Deterioration of Antibody Titers. Vaccines 2022, 10, 377. [Google Scholar] [CrossRef] [PubMed]
- Vokó, Z.; Kiss, Z.; Surján, G.; Surján, O.; Barcza, Z.; Pályi, B.; Formanek-Balku, E.; Molnár, G.A.; Herczeg, R.; Gyenesei, A.; et al. Nationwide effectiveness of five SARS-CoV-2 vaccines in Hungary-the HUN-VE study. Clin. Microbiol. Infect. 2022, 28, 398–404. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Laboratory Testing for Coronavirus Disease (COVID-19) in Suspected Human Cases: Interim Guidance, 19 March 2020. World Health Organization. 2020. Available online: https://apps.who.int/iris/handle/10665/331501 (accessed on 1 November 2022).
- Polivka, L.; Gajdacsi, J.; Fazekas, L.; Sebok, S.; Barczi, E.; Hidvegi, E.; Sutto, Z.; Dinya, E.; Maurovich-Horvat, P.; Szabo, A.J.; et al. Long-term survival benefit of male and multimorbid COVID-19 patients with 5-day remdesivir treatment. J. Glob. Health 2022, 12, 05031. [Google Scholar] [CrossRef] [PubMed]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Theodorakopoulos, T.; Kalafateli, M.; Kalambokis, G.N.; Samonakis, D.N.; Aggeletopoulou, I.; Tsolias, C.; Mantaka, A.; Tselekouni, P.; Vourli, G.; Assimakopoulos, S.F.; et al. Natural history of grade 1 ascites in patients with liver cirrhosis. Ann. Gastroenterol. 2021, 34, 93–103. [Google Scholar] [CrossRef]
- Weissenborn, K. Hepatic Encephalopathy: Definition, Clinical Grading and Diagnostic Principles. Drugs 2019, 79, 5–9. [Google Scholar] [CrossRef] [Green Version]
- Jalan, R.; Pavesi, M.; Saliba, F.; Amorós, A.; Fernandez, J.; Holland-Fischer, P.; Sawhney, R.; Mookerjee, R.; Caraceni, P.; Moreau, R.; et al. The CLIF Consortium Acute Decompensation score (CLIF-C ADs) for prognosis of hospitalised cirrhotic patients without acute-on-chronic liver failure. J. Hepatol. 2015, 62, 831–840. [Google Scholar] [CrossRef] [Green Version]
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013, 144, 1426–1437.e21–29. [Google Scholar] [CrossRef]
- O’Leary, J.G.; Reddy, K.R.; Garcia-Tsao, G.; Biggins, S.W.; Wong, F.; Fallon, M.B.; Subramanian, R.M.; Kamath, P.S.; Thuluvath, P.; Vargas, H.E.; et al. NACSELD acute-on-chronic liver failure (NACSELD-ACLF) score predicts 30-day survival in hospitalized patients with cirrhosis. Hepatology 2018, 67, 2367–2374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, A.M.; Webb, G.J.; García-Juárez, I.; Kulkarni, A.V.; Adali, G.; Wong, D.K.; Lusina, B.; Dalekos, G.N.; Masson, S.; Shore, B.M.; et al. SARS-CoV-2 Infections Among Patients With Liver Disease and Liver Transplantation Who Received COVID-19 Vaccination. Hepatol. Commun. 2022, 6, 889–897. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Khan, A. Clinical Characteristics and Outcomes of Coronavirus Disease 2019 Among Patients With Preexisting Liver Disease in the United States: A Multicenter Research Network Study. Gastroenterology 2020, 159, 768–771.e3. [Google Scholar] [CrossRef] [PubMed]
- Ge, J.; Pletcher, M.J.; Lai, J.C. Outcomes of SARS-CoV-2 Infection in Patients With Chronic Liver Disease and Cirrhosis: A National COVID Cohort Collaborative Study. Gastroenterology 2021, 161, 1487–1501.e5. [Google Scholar] [CrossRef]
- Zampino, R.; Mele, F.; Florio, L.L.; Bertolino, L.; Andini, R.; Galdo, M.; De Rosa, R.; Corcione, A.; Durante-Mangoni, E. Liver injury in remdesivir-treated COVID-19 patients. Hepatol. Int. 2020, 14, 881–883. [Google Scholar] [CrossRef]
- Teschke, R.; Méndez-Sánchez, N.; Eickhoff, A. Liver Injury in COVID-19 Patients with Drugs as Causatives: A Systematic Review of 996 DILI Cases Published 2020/2021 Based on RUCAM as Causality Assessment Method. Int. J. Mol. Sci. 2022, 23, 4828. [Google Scholar] [CrossRef]
- Sharma, P.; Kumar, A.; Anikhindi, S.; Bansal, N.; Singla, V.; Shivam, K.; Arora, A. Effect of COVID-19 on Pre-existing Liver disease: What Hepatologist Should Know? J. Clin. Exp. Hepatol. 2021, 11, 484–493. [Google Scholar] [CrossRef]
- Gao, S.; Yang, Q.; Wang, X.; Hu, W.; Lu, Y.; Yang, K.; Jiang, Q.; Li, W.; Song, H.; Sun, F.; et al. Association Between Drug Treatments and the Incidence of Liver Injury in Hospitalized Patients With COVID-19. Front. Pharmacol. 2022, 13, 799338. [Google Scholar] [CrossRef]
- Tobian, A.A.R.; Cohn, C.S.; Shaz, B.H. COVID-19 convalescent plasma. Blood 2022, 140, 196–207. [Google Scholar] [CrossRef] [PubMed]
- Drácz, B.; Czompa, D.; Müllner, K.; Hagymási, K.; Miheller, P.; Székely, H.; Papp, V.; Horváth, M.; Hritz, I.; Szijártó, A.; et al. The Elevated De Ritis Ratio on Admission Is Independently Associated with Mortality in COVID-19 Patients. Viruses 2022, 14, 2360. [Google Scholar] [CrossRef]
- Deutsch-Link, S.; Curtis, B.; Singal, A.K. COVID-19 and alcohol associated liver disease. Dig. Liver Dis. 2022, 54, 1459–1468. [Google Scholar] [CrossRef] [PubMed]
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.P.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schütte, A.; Ciesek, S.; Wedemeyer, H.; Lange, C.M. Influenza virus infection as precipitating event of acute-on-chronic liver failure. J. Hepatol. 2019, 70, 797–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, T.; Li, J.; Shao, L.; Xin, J.; Jiang, L.; Zhou, Q.; Shi, D.; Jiang, J.; Sun, S.; Jin, L.; et al. Development of diagnostic criteria and a prognostic score for hepatitis B virus-related acute-on-chronic liver failure. Gut 2018, 67, 2181–2191. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Garcia-Tsao, G.; Wong, F.; Biggins, S.W.; Kamath, P.S.; McGeorge, S.; Chew, M.; Pearson, M.; Shaw, J.; Kalluri, A.; et al. Cirrhosis Is Associated With High Mortality and Readmissions Over 90 Days Regardless of COVID-19: A Multicenter Cohort. Liver Transpl. 2021, 27, 1343–1347. [Google Scholar] [CrossRef]
- Rotshild, V.; Hirsh-Raccah, B.; Miskin, I.; Muszkat, M.; Matok, I. Comparing the clinical efficacy of COVID-19 vaccines: A systematic review and network meta-analysis. Sci. Rep. 2021, 11, 22777. [Google Scholar] [CrossRef]
- Plumb, I.D.; Feldstein, L.R.; Barkley, E.; Posner, A.B.; Bregman, H.S.; Hagen, M.B.; Gerhart, J.L. Effectiveness of COVID-19 mRNA Vaccination in Preventing COVID-19-Associated Hospitalization Among Adults with Previous SARS-CoV-2 Infection-United States, June 2021-February 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 549–555. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Fix, O.K.; Blumberg, E.A.; Chang, K.M.; Chu, J.; Chung, R.T.; Goacher, E.K.; Hameed, B.; Kaul, D.R.; Kulik, L.M.; Kwok, R.M.; et al. American Association for the Study of Liver Diseases Expert Panel Consensus Statement: Vaccines to Prevent Coronavirus Disease 2019 Infection in Patients With Liver Disease. Hepatology 2021, 74, 1049–1064. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Group | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| GROUP A and GROUP B | Laboratory-confirmed SARS-CoV-2 infection Age ≥ 18 years Elevated liver transaminases (>40 U/L) on hospital admission and/or underlying chronic liver disease (CLD) in the medical history | Rapid Antigen Test-confirmed SARS-CoV-2 infection without PCR-positivity Age < 18 years |
| GROUP A | Absence of liver cirrhosis diagnosis | Patients receiving one dose of COVID-19 vaccine including single-dose Janssen vaccine |
| GROUP B | Clinicopathologically confirmed liver cirrhosis | |
| GROUP C | Clinicopathologically confirmed liver cirrhosis; at least 2 days of hospitalisation in hepatology units; matched with GROUP B for equivalent severity grades and clinical course | |
| Laboratory-confirmed SARS-CoV-2 negativity | SARS-CoV-2 positivity on admission | |
| Age ≥ 18 years | Age < 18 years |
| Variables | GROUP A (n = 399) | GROUP B (n = 52) | GROUP C (n = 54) | p* | p- | p; |
|---|---|---|---|---|---|---|
| Gender (male/female) | 219/180 | 36/16 | 33/21 | 0.121 | 0.054 | 0.420 |
| Fatal outcome | 47 (11.8) | 5 (9.6) | 7 (13.0) | 0.880 | 0.819 | 0.761 |
| Liver disease | 46 (11.5) | 52 (100) | 54 (100) | <0.001 | <0.001 | - |
| Stage of cirrhosis Compensated Decompensated ACLF | - | 4 (7.7) 42 (80.8) 6 (11.5) | 14 (25.9) 32 (59.3) 8 (14.8) | <0.001 | <0.001 | 0.130 |
| Cirrhosis etiology Alcohol PBC PSC AIH HBV HCV Cryptogen NASH Budd-Chiari Wilson’s disease Haemochromatosis Cystic fibrosis | 3 (0.8) 1 (0.3) 5 (1.3) 0 (0) 1 (0.3) 2 (0.6) 0 (0) 0 (0) 0 (0) 1 (0.3) 1 (0.3) 0 (0) | 27 (51.9) 2 (3.8) 6 (11.5) 5 (9.6) 2 (3.8) 8 (15.4) 3 (5.8) 0 (0) 1 (1.9) 0 (0) 0 (0) 0 (0) | 22 (40.7) 0 (0) 5 (9.3) 3 (5.6) 4 (7.4) 10 (18.6) 8 (14.8) 1 (1.9) 0 (0) 1 (1.9) 1 (1.9) 1 (1.9) | <0.001 <0.05 <0.001 <0.001 <0.001 <0.001 <0.001 <0.05 0.103 <0.05 <0.05 <0.05 | <0.001 <0.05 <0.001 <0.001 <0.05 <0.001 <0.05 0.692 0.115 0.885 0.885 - | 0.330 0.238 0.759 0.484 0.679 0.797 0.202 0.509 0.491 0.509 0.509 0.509 |
| Ascites grades Mild Moderate Severe | 0 (0) 0 (0) 0 (0) | 2 (3.8) 15 (28.8) 35 (67.4) | 13 (24) 9 (16.7) 32 (59.3) | <0.001 | <0.001 | 0.143 |
| Encephalopathy stages 1-2 3 4 | 398 (99.7) 1 (0.3) 0 (0) | 25 (48.0) 18 (34.5) 9 (17.3) | 36 (66.7) 9 (16.7) 9 (16.7) | <0.001 | <0.001 | <0.05 |
| Erosive oesophagitis | 93 (23.3) | 31 (59.6) | 41 (75.9) | <0.001 | <0.001 | 0.096 |
| Esophageal varices Grade 1 Grade 2 Grade 3 | 2 (0.6) 1 (0.3) 0 (0) | 5 (9.6) 29 (55.8) 9 (17.3) | 7 (13.0) 19 (35.2) 10 (18.5) | <0.001 | <0.001 | 0.131 |
| Hypertension | 239 (59.9) | 29 (55.8) | 32 (59.3) | 0.882 | 0.653 | 0.844 |
| Cardiovascular disease | 172 (43.1) | 22 (42.3) | 29 (53.7) | 0.337 | 0.518 | 0.251 |
| Diabetes mellitus | 133 (33.3) | 20 (38.5) | 20 (37.0) | 0.700 | 0.534 | 0.519 |
| Renal disease | 60 (15.0) | 6 (11.5) | 8 (14.8) | 0.810 | 0.544 | 0.776 |
| Cancer HCC CRC Pancreas Klatskin | 29 (7.3) 18 (4.5) 5 (1.3) 3 (0.8) 1 (0.3) | 9 (17.3) 6 (11.5) 2 (3.8) 0 (0) 1 (1.9) | 9 (16.7) 9 (16.7) 0 (0) 0 (0) 0 (0) | <0.05 | <0.05 | 0.795 |
| Smoking | 202 (50.6) | 25 (48.0) | 17 (31.5) | <0.05 | 0.769 | 0.112 |
| COVID-19 Treatment Remdesivir Steroid use Convalescent Plasma | 44 (11) 287 (71.9) 68 (17.0) | 3 (5.8) 37 (71.2) 14 (26.9) | 0 (0) 0 (0) 0 (0) | <0.05 <0.001 <0.001 | 0.336 0.511 0.088 | 0.115 <0.001 <0.001 |
| Oxygen supply | 147 (41) | 21 (40.4) | 3 (5.6) | <0.001 | 0.649 | <0.001 |
| Mechanical ventilation | 159 (39.8) | 24 (46.2) | 6 (11.1) | <0.001 | 0.453 | <0.001 |
| COVID-19 vaccination | 357 (89.5) | 47 (90.4) | 49 (90.7) | 0.966 | 0.535 | 0.605 |
| COVID-19 vaccines mRNA viral vector inactivated | 272 (68.2) 55 (13.8) 30 (7.5) | 39 (75.0) 6 (11.5) 2 (3.8) | 41 (75.9) 4 (7.4) 4 (7.4) | 0.545 | 0.818 | 0.171 |
| Variable | GROUP B (n = 52) | GROUP A (n = 399) | GROUP C (n = 54) | p* | p- | p; | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pfizer-BioNTech (n = 27) | Moderna (n = 12) | Pfizer-BioNTech (n = 199) | Moderna (n = 73) | Pfizer-BioNTech (n = 36) | Moderna (n = 5) | Pfizer-BioNTech | Moderna | Pfizer-BioNTech | Moderna | Pfizer-BioNTech | Moderna | |
| Encephalopathy stage | <0.001 | <0.001 | <0.001 | <0.001 | <0.05 | 0.082 | ||||||
| Stage 1-2 | 11 (21.2 | 6 (11.5) | 199 (49.9) | 72 (18) | 25 (46.3) | 1 (1.9) | ||||||
| Stage 3 | 8 (15.4) | 6 (11.5) | 0 (0) | 1 (0.3) | 7 (13) | 2 (3.7) | ||||||
| Stage 4 | 8 (15.4) | 0 (0) | 0 (0) | 0 (0) | 4 (7.4) | 2 (3.7) | ||||||
| Ascites grade | <0.001 | <0.001 | <0.001 | <0.001 | 0.094 | 0.503 | ||||||
| Mild | 0 (0) | 0 (0) | 199 (49.9) | 72 (18) | 10 (18.5) | 0 (0) | ||||||
| Moderate | 6 (11.5) | 5 (9.6) | 0 (0) | 1 (0.3) | 3 (5.6) | 3 (5.6) | ||||||
| Severe | 21 (40.4) | 7 (13.5) | 0 (0) | 0 (0) | 23 (42.6) | 2 (3.7) | ||||||
| Esophageal varices | <0.001 | <0.001 | <0.001 | <0.001 | 0.162 | 0.412 | ||||||
| Grade 1 | 3 (5.8) | 0 (0) | 1 (0.3) | 1 (0.3) | 4 (7.4) | 0 (0) | ||||||
| Grade 2 | 15 (28.8) | 8 (15.4) | 1 (0.3) | 0 (0) | 14 (25.9) | 1 (1.9) | ||||||
| Grade 3 | 6 (11.5) | 1 (1.9) | 0 (0) | 0 (0) | 7 (13) | 1 (1.9) | ||||||
| Oxygen support | 9 (17.3) | 6 (11.5) | 65 (16.3) | 29 (7.3) | 1 (1.9) | 1 (1.9) | <0.05 | 0.517 | 0.945 | 0.505 | <0.05 | 0.267 |
| Mechanical ventilation | 16 (30.8) | 4 (7.7) | 89 (22.3) | 22 (5.5) | 5 (9.3) | 1 (1.9) | <0.001 | 0.861 | 0.156 | 0.825 | <0.001 | 0.594 |
| Fatal outcome | 4 (7.7) | 0 (0) | 25 (6.3) | 6 (1.5) | 3 (5.6) | 2 (3.7) | 0.706 | <0.05 | 0.743 | 0.306 | 0.422 | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drácz, B.; Müller, V.; Takács, I.; Hagymási, K.; Dinya, E.; Miheller, P.; Szijártó, A.; Werling, K. Effectiveness of COVID-19 Vaccination with mRNA Vaccines for Patients with Cirrhosis in Hungary: Multicentre Matched Cohort Study. Vaccines 2023, 11, 50. https://doi.org/10.3390/vaccines11010050
Drácz B, Müller V, Takács I, Hagymási K, Dinya E, Miheller P, Szijártó A, Werling K. Effectiveness of COVID-19 Vaccination with mRNA Vaccines for Patients with Cirrhosis in Hungary: Multicentre Matched Cohort Study. Vaccines. 2023; 11(1):50. https://doi.org/10.3390/vaccines11010050
Chicago/Turabian StyleDrácz, Bálint, Veronika Müller, István Takács, Krisztina Hagymási, Elek Dinya, Pál Miheller, Attila Szijártó, and Klára Werling. 2023. "Effectiveness of COVID-19 Vaccination with mRNA Vaccines for Patients with Cirrhosis in Hungary: Multicentre Matched Cohort Study" Vaccines 11, no. 1: 50. https://doi.org/10.3390/vaccines11010050