
Prevalence of Emergent Dolutegravir Resistance Mutations in People Living with HIV: A Rapid Scoping Review

 , , ,
, , ,
Abstract
:1. Introduction
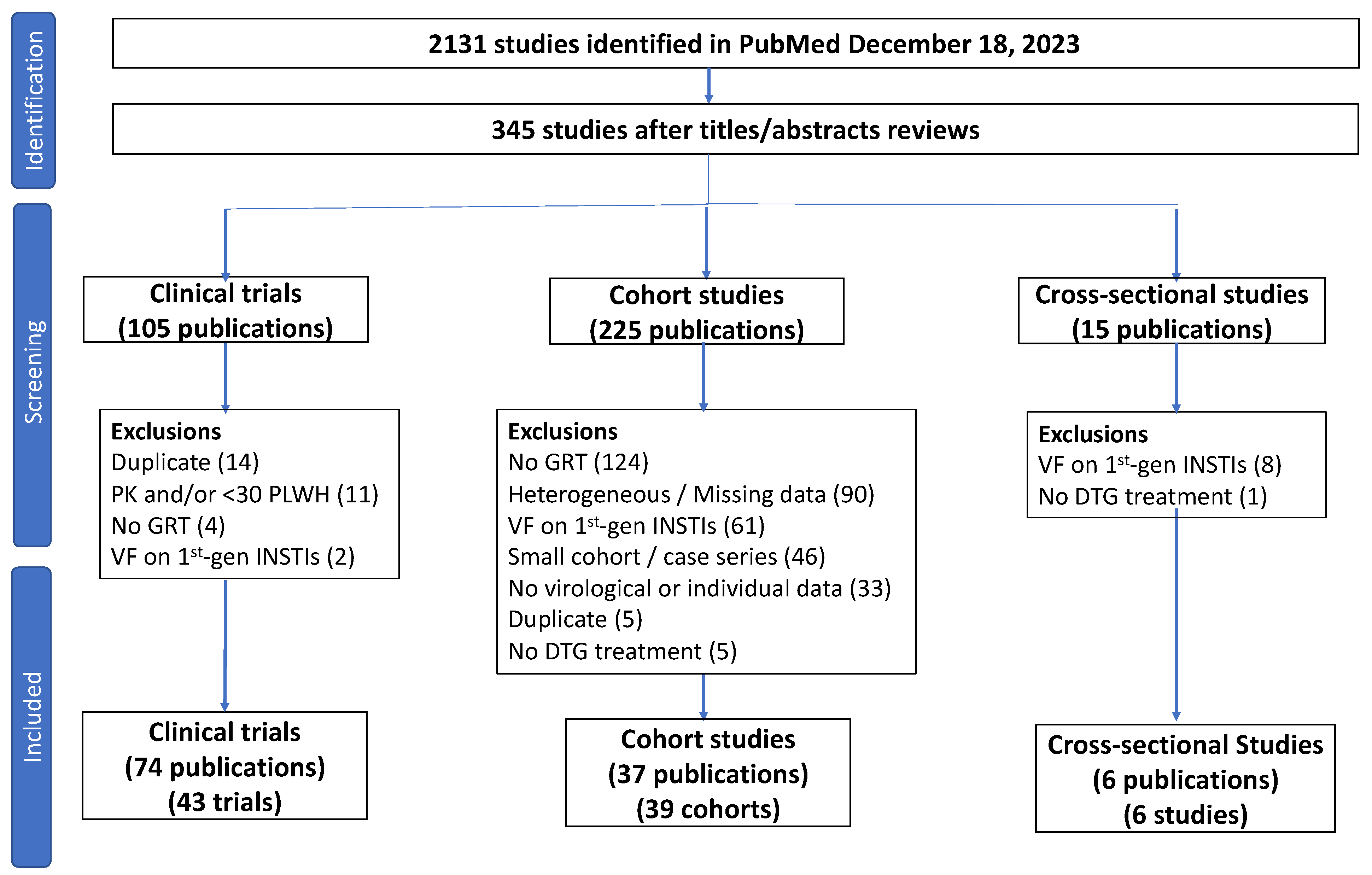
2. Materials and Methods
3. Results
3.1. ART-Naïve PLWH (Scenarios 1 and 2)

{kind=link}
| Trial | Regions | Population | DTG-Containing Regimen | # PLWH | Weeks | # (%) VF on DTG 1 | # (%) Undergoing GRT 2 | # (%) with INSTI DRMs 3 |
|---|---|---|---|---|---|---|---|---|
| DTG plus 2 NRTIs | ||||||||
| SPRING-1 2012–2013 [6,7] 4 | Europe, North America | Adults; without DRMs | DTG + 2 NRTIs | 51 | 96 | 2 (3.9%) | 0 (0%) | 0 (0%) |
| SPRING-2 2013 [8,9] | Europe, North America | Adults; without DRMs | DTG + 2 NRTIs | 411 | 96 | 22 (5.4%) | 22 (5.4%) | 0 (0%) |
| SINGLE 2013, 2015 [10,11] | Europe, North America | Adults; without DRMs | DTG + ABC/3TC | 414 | 144 | 43 (10.4%) | 39 (9.4%) | 0 (0%) |
| FLAMINGO 2014, 2015 [12,13] | Europe, North America | Adults; without DRMs | DTG + 2 NRTIs | 242 | 96 | 19 (7.9%) | 2 (0.8%) | 0 (0%) |
| ARIA 2017 [14] | Europe, North America, South America, Asia, Africa | Adult women; without DRMs | DTG + ABC/3TC | 248 | 48 | 16 (6.5%) | 6 (2.4%) | 0 (0%) |
| ADVANCE 2019, 2020 [15,16,17] 5 | South Africa | Adults/Adolescents | DTG + TXF/FTC | 702 | 96 | 25 (3.6%) | 28 (4.0%) | 0 (0%) |
| NAMSAL 2019, 2020 [18,19] 6 | Cameroon | Adults | DTG + TDF/FTC | 310 | 96 | 8 (2.6%) | 3 (1.0%) | 0 (0%) |
| GS-US-3801490 2017, 2019 [20,21,22] | Europe, North America | Adults | DTG + TAF/FTC | 325 | 96 | 9 (2.8%) | 6 (1.8%) | 0 (0%) |
| GS-US-3801489 2017, 2019 [23,24] | Europe, North America | Adults; without DRMs | DTG + ABC/3TC | 315 | 96 | 7 (2.2%) | 5 (1.6%) | 0 (0%) |
| SYMTRI 2022 [25] | Spain | Adults | DTG + ABC/3TC | 155 | 48 | 6 (3.9%) | Not reported | 0 (0%) |
| GEMINI-1/GEMINI-2 2019, 2020, 2022 [26,27,28] | Europe, North America, South America, Asia, Africa | Adults without known major DRMs | DTG + TDF/FTC | 717 | 96 | 14 (2.0%) | 7 (1.0%) | 0 (0%) |
| IMPAACT 2010/VESTED 2021, 2023 [29,30] | Sub-Saharan Africa, Thailand, Brazil, India, U.S. | Pregnant women (14–28 weeks) | DTG + TXF/FTC | 405 | 50 post-partum | 20 (4.9%) | 15 (3.7%) | 1 (0.2%) |
| OPTIMPRIM2 2022 [31] | France | Adults with primary HIV (1 had M184VI) | DTG + TDF/FTC | 49 | 48 | 3 (6.1%) | Not reported | 0 (0%) |
| ALLIANCE 2023 [32] | Europe, North America, Asia | Adults with HBV Infection | DTG + TDF/FTC | 122 | 48 | 7 (5.7%) | 6 (4.9%) | 0 (0%) |
| INSPIRING 2020 [33] | Europe, South America, Africa, Asia | Adults; Anti-TB therapy ≤ 8 weeks | DTG BID + 2 NRTIs | 69 | 48 | 2 (2.9%) | 2 (2.9%) | 0 (0%) |
| RADIANT-TB 2023 [34] 7 | South Africa | Adults; Anti-TB therapy ≤ 12 weeks | DTG + TDF/3TC | 52 | 48 | 3 (5.8%) | 3 (5.8%) | 0 (0%) |
| DTG BID + TDF/3TC | 49 | 48 | 3 (6.1%) | 3 (6.1%) | 0 (0%) | |||
| DTG plus 3TC | ||||||||
| GEMINI-1/GEMINI-2 2019, 2020, 2022 [26,27,28] | Europe, North America, South America, Asia, Africa | VL ≤ 500,000; no major DRMs | DTG/3TC | 716 | 96 | 22 (3.1%) | 10 (1.4%) | 0 (0%) |
| ACTG A5353 2018, 2019 [43,44] | United States | VL ≤ 500,000; no major DRMs | DTG/3TC | 120 | 48 | 6 (5.0%) | 4 (3.3%) | 1 (0.8) |
| STAT 2021, 2023 [45,46] 8 | United States | Newly diagnosed individuals | DTG/3TC | 131 | 48 | 19 (14.5%) | 2 (1.5%) | 0 (0%) |
| DOLAVI 2022 [47] 9 | Spain | Newly diagnosed individuals | DTG/3TC | 88 | 48 | 12 (13.7%) | 1 (1.1%) | 0 (0%) |
3.2. ART-Experienced PLWH with a History of VF on an NNRTI-Containing Regimen (Scenario 3)
3.3. ART-Experienced PLWH with VS (Scenarios 4, 5, and 6)
| Trial | Regions | Population | DTG-Containing Regimen | # PLWH | Weeks | # (%) VF 1 | # (%) Undergoing GRT 2 | # (%) INSTI DRMs |
|---|---|---|---|---|---|---|---|---|
| DTG plus 2 NRTIs | ||||||||
| NEAT022 2017, 2019 [75,76] 3 | Europe | <50 copies x ≥ 6 months on a boosted PI regimen; no h/o VF or NRTI DRMs | DTG + 2 NRTIs | 205 | 96 | 5 (2.4%) | 3 (1.5%) | 0 (0%) |
| STRIIVING 2017 [77] 3 | North America | <50 copies x ≥ 6M on an NNRTI-, boosted PI, or 1st-generation INSTI regimen; no h/o VF | DTG + ABC/3TC | 275 | 48 | 0 (0%) | 0 (0%) | 0 (0%) |
| 2SD 2023 [78] 4 | Kenya | <50 copies x ≥ 3M on a 2nd-line boosted PI regimen | DTG + 2 NRTIs | 397 | 48 | 20 (5.0%) | 0 (0%) | 0 (0%) |
| DTG plus a second ARV | ||||||||
| TANGO 2020, 2022 [82,83] | Europe, North America, Asia, Oceania | <50 copies/mL x ≥ 6 months on a TAF-containing regimen (78% on an INSTI); no h/o of VF or DRMs | DTG/3TC | 369 | 144 | 1 (0.3%) | 0 (0%) | 0 (0%) |
| SALSA 2023 [84] | Europe, North America, South America, Asia, Africa | <50 copies/mL x ≥ 6 months; 40% on an INSTI; no h/o of VF or DRMs | DTG/3TC | 246 | 48 | 1 (0.4%) | 0 (0%) | 0 (0%) |
| DOLAM–Phase B 2021 [85] 5 | Spain | <50 copies/mL x ≥ 12 months; 47% on an INSTI; no h/o of VF or DRMs on an XTC- or INSTI-containing regimen | DTG/3TC | 131 | 48 | 3 (2.3%) | 3 (2.3%) | 0 (0%) |
| LAMIDOL 2019 [86] | France | <50 copies/mL x ≥ 24 months; 21% on an INSTI; no h/o of VF or DRMs | DTG/3TC | 104 | 48 | 1 (1.0%) | 1 (1.0%) | 0 (0%) |
| ASPIRE 2018 [87] | United States | <50 copies/mL x ≥ 6 months; 37% on an INSTI; no h/o of VF or DRMs | DTG/3TC | 44 | 24 | 1 (2.3%) | 1 (2.3%) | 0 (0%) |
| ART-PRO 2020, 2021, 2022 [88,89,90] | Spain | <50 copies/mL x ≥ 12 months; 21 had a history of M184VI; single arm pilot trial. | DTG/3TC | 41 | 48 | 0 (0%) | 0 (0%) | 0 (0%) |
| SIMPL’HIV 2020 [91] | Switzerland | <50 copies/mL x ≥ 6 months; 63% on an INSTI; no h/o VF or DRMs; | DTG/FTC | 93 | 48 | 1 (1.1%) | 1 (1.1%) | 0 (0%) |
| SWORD-1 and 2 2018, 2019, 2020 [92,93,94] 5 | Europe, North America, Asia, Oceania | <50 copies/mL x ≥ 6 months on a 1st or 2nd ART regimen; 20% on an INSTI; no h/o of VF or DRMs | DTG/RPV | 513 | 144 | 14 (2.7%) | 7 (1.4%) | 0 (0%) |
| DUALIS 2020 [95,96] | Germany | <50 copies/mL x ≥ 6 months receiving boosted DRV + 2 NRTIs; 7% with prior INSTI use; no h/o DTG or DRV DRMs | DTG/DRV/r | 131 | 48 | 5 (3.8%) | Not reported | 0 (0%) |
| SMILE 2023 [97] 6 | Uganda, South Africa, Thailand, Europe, Latin America | Perinatally infected children/adolescents; <50 copies/mL x ≥ 12 months; no h/o DTG or DRV DRMs | DTG/DRV/r | 158 | 48 | 8 (5.1%) | 6 (3.8%) | 0 (0%) |
| DTG monotherapy | ||||||||
| DOMONO 2017, 2018, 2019 7 | Netherlands | VL < 50 x ≥ 6 months; plasma HIV-1 RNA zenith <105 copies/mL and CD4 count nadir > 200 cells/mm3; 15% INSTI experienced; no h/o VF. | DTG monotherapy | 99 | 48 | 10 (10.1%) | 8 (8.1%) | 4 (4.1%) |
| DOLAM 2018 [118] 8 | Spain | VL < 50 x ≥ 12 months; CD4 count nadir > 200 cells/mm3; 17% INSTI experienced; no h/o VF on an INSTI regimen. | DTG monotherapy | 31 | 24 | 2 (6.5%) | 2 (6.5%) | 2 (6.5%) |
| EARLY SIMPLIFIED 2019, 2023 [119,120] | Switzerland | VL < 50 x ≥ 12 months; ART began within 6 months of HIV infection; 60% INSTI experienced; no h/o VF. | DTG monotherapy | 68 | 96 | 0 (0%) | 0 (0%) | 0 (0%) |
| MONCAY 2019 [121] 9 | France | VL < 50 x ≥ 12 months and on DTG/ABC/3TC x ≥ 1 month; CD4 count nadir > 100 cells/mm3; no h/o VF on an INSTI regimen. | DTG monotherapy | 78 | 48 | 7 (9.0%) | 7 (9.0%) | 2 (2.6%) |
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- World Health Organization. Consolidated Guidelines on HIV Prevention, Testing, Treatment, Service Delivery and Monitoring: Recommendations for a Public Health Approach. Available online: https://www.who.int/publications-detail-redirect/9789240031593 (accessed on 17 August 2022).
- Clinton Health Access Initiative. The State of HIV Treatment, Testing, and Prevention in Low- and Middle-Income Countries; HIV Market Report 2023; Clinton Health Access Initiative: Boston, MA, USA, 2023. [Google Scholar]
- Tao, K.; Rhee, S.-Y.; Chu, C.; Avalos, A.; Ahluwalia, A.K.; Gupta, R.K.; Jordan, M.R.; Shafer, R.W. Treatment Emergent Dolutegravir Resistance Mutations in Individuals Naïve to HIV-1 Integrase Inhibitors: A Rapid Scoping Review. Viruses 2023, 15, 1932. [Google Scholar] [CrossRef] [PubMed]
- Tzou, P.L.; Rhee, S.-Y.; Descamps, D.; Clutter, D.S.; Hare, B.; Mor, O.; Grude, M.; Parkin, N.; Jordan, M.R.; Bertagnolio, S.; et al. Integrase Strand Transfer Inhibitor (INSTI)-Resistance Mutations for the Surveillance of Transmitted HIV-1 Drug Resistance. J. Antimicrob. Chemother. 2020, 75, 170–182. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- van Lunzen, J.; Maggiolo, F.; Arribas, J.R.; Rakhmanova, A.; Yeni, P.; Young, B.; Rockstroh, J.K.; Almond, S.; Song, I.; Brothers, C.; et al. Once Daily Dolutegravir (S/GSK1349572) in Combination Therapy in Antiretroviral-Naive Adults with HIV: Planned Interim 48 Week Results from SPRING-1, a Dose-Ranging, Randomised, Phase 2b Trial. Lancet Infect. Dis. 2012, 12, 111–118. [Google Scholar] [CrossRef]
- Stellbrink, H.-J.; Reynes, J.; Lazzarin, A.; Voronin, E.; Pulido, F.; Felizarta, F.; Almond, S.; St Clair, M.; Flack, N.; Min, S.; et al. Dolutegravir in Antiretroviral-Naive Adults with HIV-1: 96-Week Results from a Randomized Dose-Ranging Study. AIDS 2013, 27, 1771–1778. [Google Scholar] [CrossRef] [PubMed]
- Raffi, F.; Rachlis, A.; Stellbrink, H.-J.; Hardy, W.D.; Torti, C.; Orkin, C.; Bloch, M.; Podzamczer, D.; Pokrovsky, V.; Pulido, F.; et al. Once-Daily Dolutegravir versus Raltegravir in Antiretroviral-Naive Adults with HIV-1 Infection: 48 Week Results from the Randomised, Double-Blind, Non-Inferiority SPRING-2 Study. Lancet 2013, 381, 735–743. [Google Scholar] [CrossRef]
- Raffi, F.; Jaeger, H.; Quiros-Roldan, E.; Albrecht, H.; Belonosova, E.; Gatell, J.M.; Baril, J.-G.; Domingo, P.; Brennan, C.; Almond, S.; et al. Once-Daily Dolutegravir versus Twice-Daily Raltegravir in Antiretroviral-Naive Adults with HIV-1 Infection (SPRING-2 Study): 96 Week Results from a Randomised, Double-Blind, Non-Inferiority Trial. Lancet Infect. Dis. 2013, 13, 927–935. [Google Scholar] [CrossRef]
- Walmsley, S.L.; Antela, A.; Clumeck, N.; Duiculescu, D.; Eberhard, A.; Gutiérrez, F.; Hocqueloux, L.; Maggiolo, F.; Sandkovsky, U.; Granier, C.; et al. Dolutegravir plus Abacavir–Lamivudine for the Treatment of HIV-1 Infection. N. Engl. J. Med. 2013, 369, 1807–1818. [Google Scholar] [CrossRef]
- Walmsley, S.; Baumgarten, A.; Berenguer, J.; Felizarta, F.; Florence, E.; Khuong-Josses, M.-A.; Kilby, J.M.; Lutz, T.; Podzamczer, D.; Portilla, J.; et al. Brief Report: Dolutegravir Plus Abacavir/Lamivudine for the Treatment of HIV-1 Infection in Antiretroviral Therapy-Naive Patients: Week 96 and Week 144 Results From the SINGLE Randomized Clinical Trial. JAIDS J. Acquir. Immune Defic. Syndr. 2015, 70, 515–519. [Google Scholar] [CrossRef]
- Clotet, B.; Feinberg, J.; van Lunzen, J.; Khuong-Josses, M.-A.; Antinori, A.; Dumitru, I.; Pokrovskiy, V.; Fehr, J.; Ortiz, R.; Saag, M.; et al. Once-Daily Dolutegravir versus Darunavir plus Ritonavir in Antiretroviral-Naive Adults with HIV-1 Infection (FLAMINGO): 48 Week Results from the Randomised Open-Label Phase 3b Study. Lancet 2014, 383, 2222–2231. [Google Scholar] [CrossRef]
- Molina, J.-M.; Clotet, B.; van Lunzen, J.; Lazzarin, A.; Cavassini, M.; Henry, K.; Kulagin, V.; Givens, N.; de Oliveira, C.F.; Brennan, C. Once-Daily Dolutegravir versus Darunavir plus Ritonavir for Treatment-Naive Adults with HIV-1 Infection (FLAMINGO): 96 Week Results from a Randomised, Open-Label, Phase 3b Study. Lancet HIV 2015, 2, e127–e136. [Google Scholar] [CrossRef] [PubMed]
- Orrell, C.; Hagins, D.P.; Belonosova, E.; Porteiro, N.; Walmsley, S.; Falcó, V.; Man, C.Y.; Aylott, A.; Buchanan, A.M.; Wynne, B.; et al. Fixed-Dose Combination Dolutegravir, Abacavir, and Lamivudine versus Ritonavir-Boosted Atazanavir plus Tenofovir Disoproxil Fumarate and Emtricitabine in Previously Untreated Women with HIV-1 Infection (ARIA): Week 48 Results from a Randomised, Open-Label, Non-Inferiority, Phase 3b Study. Lancet HIV 2017, 4, e536–e546. [Google Scholar] [CrossRef] [PubMed]
- Venter, W.D.F.; Moorhouse, M.; Sokhela, S.; Fairlie, L.; Mashabane, N.; Masenya, M.; Serenata, C.; Akpomiemie, G.; Qavi, A.; Chandiwana, N.; et al. Dolutegravir plus Two Different Prodrugs of Tenofovir to Treat HIV. N. Engl. J. Med. 2019, 381, 803–815. [Google Scholar] [CrossRef] [PubMed]
- Venter, W.D.F.; Sokhela, S.; Simmons, B.; Moorhouse, M.; Fairlie, L.; Mashabane, N.; Serenata, C.; Akpomiemie, G.; Masenya, M.; Qavi, A.; et al. Dolutegravir with Emtricitabine and Tenofovir Alafenamide or Tenofovir Disoproxil Fumarate versus Efavirenz, Emtricitabine, and Tenofovir Disoproxil Fumarate for Initial Treatment of HIV-1 Infection (ADVANCE): Week 96 Results from a Randomised, Phase 3, Non-Inferiority Trial. Lancet HIV 2020, 7, e666–e676. [Google Scholar] [CrossRef] [PubMed]
- Pepperrell, T.; Venter, W.D.F.; McCann, K.; Bosch, B.; Tibbatts, M.; Woods, J.; Sokhela, S.; Serenata, C.; Moorhouse, M.; Qavi, A.; et al. Participants on Dolutegravir Resuppress Human Immunodeficiency Virus RNA After Virologic Failure: Updated Data from the ADVANCE Trial. Clin. Infect. Dis. 2021, 73, e1008–e1010. [Google Scholar] [CrossRef] [PubMed]
- Kouanfack, C.; The NAMSAL ANRS 12313 Study Group. Dolutegravir-Based or Low-Dose Efavirenz–Based Regimen for the Treatment of HIV-1. N. Engl. J. Med. 2019, 381, 816–826. [Google Scholar] [CrossRef] [PubMed]
- Calmy, A.; Tovar Sanchez, T.; Kouanfack, C.; Mpoudi-Etame, M.; Leroy, S.; Perrineau, S.; Lantche Wandji, M.; Tetsa Tata, D.; Omgba Bassega, P.; Abong Bwenda, T.; et al. Dolutegravir-Based and Low-Dose Efavirenz-Based Regimen for the Initial Treatment of HIV-1 Infection (NAMSAL): Week 96 Results from a Two-Group, Multicentre, Randomised, Open Label, Phase 3 Non-Inferiority Trial in Cameroon. Lancet HIV 2020, 7, e677–e687. [Google Scholar] [CrossRef]
- Sax, P.E.; Pozniak, A.; Montes, M.L.; Koenig, E.; DeJesus, E.; Stellbrink, H.-J.; Antinori, A.; Workowski, K.; Slim, J.; Reynes, J.; et al. Coformulated Bictegravir, Emtricitabine, and Tenofovir Alafenamide versus Dolutegravir with Emtricitabine and Tenofovir Alafenamide, for Initial Treatment of HIV-1 Infection (GS-US-380–1490): A Randomised, Double-Blind, Multicentre, Phase 3, Non-Inferiority Trial. Lancet 2017, 390, 2073–2082. [Google Scholar] [CrossRef]
- Sax, P.E.; DeJesus, E.; Crofoot, G.; Ward, D.; Benson, P.; Dretler, R.; Mills, A.; Brinson, C.; Peloquin, J.; Wei, X.; et al. Bictegravir versus Dolutegravir, Each with Emtricitabine and Tenofovir Alafenamide, for Initial Treatment of HIV-1 Infection: A Randomised, Double-Blind, Phase 2 Trial. Lancet HIV 2017, 4, e154–e160. [Google Scholar] [CrossRef]
- Stellbrink, H.-J.; Arribas, J.R.; Stephens, J.L.; Albrecht, H.; Sax, P.E.; Maggiolo, F.; Creticos, C.; Martorell, C.T.; Wei, X.; Acosta, R.; et al. Co-Formulated Bictegravir, Emtricitabine, and Tenofovir Alafenamide versus Dolutegravir with Emtricitabine and Tenofovir Alafenamide for Initial Treatment of HIV-1 Infection: Week 96 Results from a Randomised, Double-Blind, Multicentre, Phase 3, Non-Inferiority Trial. Lancet HIV 2019, 6, e364–e372. [Google Scholar] [CrossRef]
- Gallant, J.; Lazzarin, A.; Mills, A.; Orkin, C.; Podzamczer, D.; Tebas, P.; Girard, P.-M.; Brar, I.; Daar, E.S.; Wohl, D.; et al. Bictegravir, Emtricitabine, and Tenofovir Alafenamide versus Dolutegravir, Abacavir, and Lamivudine for Initial Treatment of HIV-1 Infection (GS-US-380-1489): A Double-Blind, Multicentre, Phase 3, Randomised Controlled Non-Inferiority Trial. Lancet 2017, 390, 2063–2072. [Google Scholar] [CrossRef]
- Wohl, D.A.; Yazdanpanah, Y.; Baumgarten, A.; Clarke, A.; Thompson, M.A.; Brinson, C.; Hagins, D.; Ramgopal, M.N.; Antinori, A.; Wei, X.; et al. Bictegravir Combined with Emtricitabine and Tenofovir Alafenamide versus Dolutegravir, Abacavir, and Lamivudine for Initial Treatment of HIV-1 Infection: Week 96 Results from a Randomised, Double-Blind, Multicentre, Phase 3, Non-Inferiority Trial. Lancet HIV 2019, 6, e355–e363. [Google Scholar] [CrossRef]
- Podzamczer, D.; Micán, R.; Tiraboschi, J.; Portilla, J.; Domingo, P.; Llibre, J.M.; Ribera, E.; Vivancos, M.J.; Morano, L.; Masiá, M.; et al. Darunavir/Cobicistat/Emtricitabine/Tenofovir Alafenamide Versus Dolutegravir/Abacavir/Lamivudine in Antiretroviral-Naive Adults (SYMTRI): A Multicenter Randomized Open-Label Study (PReEC/RIS-57). Open Forum Infect. Dis. 2022, 9, ofab595. [Google Scholar] [CrossRef]
- Cahn, P.; Madero, J.S.; Arribas, J.R.; Antinori, A.; Ortiz, R.; Clarke, A.E.; Hung, C.-C.; Rockstroh, J.K.; Girard, P.-M.; Sievers, J.; et al. Dolutegravir plus Lamivudine versus Dolutegravir plus Tenofovir Disoproxil Fumarate and Emtricitabine in Antiretroviral-Naive Adults with HIV-1 Infection (GEMINI-1 and GEMINI-2): Week 48 Results from Two Multicentre, Double-Blind, Randomised, Non-Inferiority, Phase 3 Trials. Lancet 2019, 393, 143–155. [Google Scholar] [CrossRef]
- Cahn, P.; Madero, J.S.; Arribas, J.R.; Antinori, A.; Ortiz, R.; Clarke, A.E.; Hung, C.-C.; Rockstroh, J.K.; Girard, P.-M.; Sievers, J.; et al. Durable Efficacy of Dolutegravir Plus Lamivudine in Antiretroviral Treatment–Naive Adults with HIV-1 Infection: 96-Week Results from the GEMINI-1 and GEMINI-2 Randomized Clinical Trials. JAIDS J. Acquir. Immune Defic. Syndr. 2020, 83, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Cahn, P.; Sierra Madero, J.; Arribas, J.R.; Antinori, A.; Ortiz, R.; Clarke, A.E.; Hung, C.-C.; Rockstroh, J.K.; Girard, P.-M.; Sievers, J.; et al. Three-Year Durable Efficacy of Dolutegravir plus Lamivudine in Antiretroviral Therapy—Naive Adults with HIV-1 Infection. AIDS 2022, 36, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Lockman, S.; Brummel, S.S.; Ziemba, L.; Stranix-Chibanda, L.; McCarthy, K.; Coletti, A.; Jean-Philippe, P.; Johnston, B.; Krotje, C.; Fairlie, L.; et al. Efficacy and Safety of Dolutegravir with Emtricitabine and Tenofovir Alafenamide Fumarate or Tenofovir Disoproxil Fumarate, and Efavirenz, Emtricitabine, and Tenofovir Disoproxil Fumarate HIV Antiretroviral Therapy Regimens Started in Pregnancy (IMPAACT 2010/VESTED): A Multicentre, Open-Label, Randomised, Controlled, Phase 3 Trial. Lancet 2021, 397, 1276–1292. [Google Scholar] [CrossRef] [PubMed]
- Chinula, L.; Ziemba, L.; Brummel, S.; McCarthy, K.; Coletti, A.; Krotje, C.; Johnston, B.; Knowles, K.; Moyo, S.; Stranix-Chibanda, L.; et al. Efficacy and Safety of Three Antiretroviral Therapy Regimens Started in Pregnancy up to 50 Weeks Post Partum: A Multicentre, Open-Label, Randomised, Controlled, Phase 3 Trial. Lancet HIV 2023, 10, e363–e374. [Google Scholar] [CrossRef] [PubMed]
- Chéret, A.; Bauer, R.; Meiffrédy, V.; Lopez, P.; Ajana, F.; Lacombe, K.; Morlat, P.; Lascoux, C.; Reynes, J.; Calin, R.; et al. Once-Daily Dolutegravir versus Darunavir plus Cobicistat in Adults at the Time of Primary HIV-1 Infection: The OPTIPRIM2-ANRS 169 Randomized, Open-Label, Phase 3 Trial. J. Antimicrob. Chemother. 2022, 77, 2506–2515. [Google Scholar] [CrossRef] [PubMed]
- Avihingsanon, A.; Lu, H.; Leong, C.L.; Hung, C.-C.; Koenig, E.; Kiertiburanakul, S.; Lee, M.-P.; Supparatpinyo, K.; Zhang, F.; Rahman, S.; et al. Bictegravir, Emtricitabine, and Tenofovir Alafenamide versus Dolutegravir, Emtricitabine, and Tenofovir Disoproxil Fumarate for Initial Treatment of HIV-1 and Hepatitis B Coinfection (ALLIANCE): A Double-Blind, Multicentre, Randomised Controlled, Phase 3 Non-Inferiority Trial. Lancet HIV 2023, 10, e640–e652. [Google Scholar] [CrossRef] [PubMed]
- Dooley, K.E.; Kaplan, R.; Mwelase, N.; Grinsztejn, B.; Ticona, E.; Lacerda, M.; Sued, O.; Belonosova, E.; Ait-Khaled, M.; Angelis, K.; et al. Dolutegravir-Based Antiretroviral Therapy for Patients Coinfected with Tuberculosis and Human Immunodeficiency Virus: A Multicenter, Noncomparative, Open-Label, Randomized Trial. Clin. Infect. Dis. 2020, 70, 549–556. [Google Scholar] [CrossRef]
- Griesel, R.; Zhao, Y.; Simmons, B.; Omar, Z.; Wiesner, L.; Keene, C.M.; Hill, A.M.; Meintjes, G.; Maartens, G. Standard-Dose versus Double-Dose Dolutegravir in HIV-Associated Tuberculosis in South Africa (RADIANT-TB): A Phase 2, Non-Comparative, Randomised Controlled Trial. Lancet HIV 2023, 10, e433–e441. [Google Scholar] [CrossRef]
- Grayhack, C.; Sheth, A.; Kirby, O.; Davis, J.; Sibliss, K.; Nkwihoreze, H.; Aaron, E.; Alleyne, G.; Laguerre, R.; Rana, A.; et al. Evaluating Outcomes of Mother–Infant Pairs Using Dolutegravir for HIV Treatment during Pregnancy. AIDS 2018, 32, 2017–2021. [Google Scholar] [CrossRef]
- Rhee, S.-Y.; Clutter, D.; Hare, C.B.; Tchakoute, C.T.; Sainani, K.; Fessel, W.J.; Hurley, L.; Slome, S.; Pinsky, B.A.; Silverberg, M.J.; et al. Virological Failure and Acquired Genotypic Resistance Associated with Contemporary Antiretroviral Treatment Regimens. Open Forum Infect. Dis. 2020, 7, ofaa316. [Google Scholar] [CrossRef]
- Mondi, A.; Cozzi-Lepri, A.; Tavelli, A.; Rusconi, S.; Vichi, F.; Ceccherini-Silberstein, F.; Calcagno, A.; De Luca, A.; Maggiolo, F.; Marchetti, G.; et al. Effectiveness of Dolutegravir-Based Regimens as Either First-Line or Switch Antiretroviral Therapy: Data from the Icona Cohort. J. Int. AIDS Soc. 2019, 22, e25227. [Google Scholar] [CrossRef]
- Armenia, D.; Bouba, Y.; Gagliardini, R.; Gori, C.; Bertoli, A.; Borghi, V.; Gennari, W.; Micheli, V.; Callegaro, A.P.; Gazzola, L.; et al. Evaluation of Virological Response and Resistance Profile in HIV-1 Infected Patients Starting a First-Line Integrase Inhibitor-Based Regimen in Clinical Settings. J. Clin. Virol. 2020, 130, 104534. [Google Scholar] [CrossRef] [PubMed]
- Suárez-García, I.; Alejos, B.; Hernando, V.; Viñuela, L.; Vera García, M.; Rial-Crestelo, D.; Pérez Elías, M.J.; Albendín Iglesias, H.; Peraire, J.; Tiraboschi, J.; et al. Effectiveness and Tolerability of Dolutegravir/Lamivudine for the Treatment of HIV-1 Infection in Clinical Practice. J. Antimicrob. Chemother. 2023, 78, 1423–1432. [Google Scholar] [CrossRef]
- Chin, B.S.; Lee, J.H.; Kim, G. Similar Durability of Two Single Tablet Regimens, Dolutegravir/Abacavir/Lamivudine and Elvitegravir/Cobicistat/Tenofovir/Emtricitabine: Single Center Experience. J. Korean Med. Sci. 2020, 35, e235. [Google Scholar] [CrossRef] [PubMed]
- Ntamatungiro, A.J.; Eichenberger, A.; Okuma, J.; Vanobberghen, F.; Ndege, R.; Kimera, N.; Francis, J.M.; Kagura, J.; Weisser, M.; for the Kilombero and Ulanga Antiretroviral Cohort (KIULARCO) Study Group. Transitioning to Dolutegravir in a Programmatic Setting: Virological Outcomes and Associated Factors Among Treatment-Naive Patients with HIV-1 in the Kilombero and Ulanga Antiretroviral Cohort in Rural Tanzania. Open Forum Infect. Dis. 2023, 10, ofad321. [Google Scholar] [CrossRef] [PubMed]
- Diaz, R.S.; Hunter, J.R.; Camargo, M.; Dias, D.; Galinskas, J.; Nassar, I.; De Lima, I.B.; Caldeira, D.B.; Sucupira, M.C.; Schechter, M. Dolutegravir-Associated Resistance Mutations after First-Line Treatment Failure in Brazil. BMC Infect. Dis. 2023, 23, 347. [Google Scholar] [CrossRef]
- Taiwo, B.O.; Zheng, L.; Stefanescu, A.; Nyaku, A.; Bezins, B.; Wallis, C.L.; Godfrey, C.; Sax, P.E.; Acosta, E.; Haas, D.; et al. ACTG A5353: A Pilot Study of Dolutegravir Plus Lamivudine for Initial Treatment of Human Immunodeficiency Virus-1 (HIV-1)–Infected Participants with HIV-1 RNA <500000 Copies/mL. Clin. Infect. Dis. 2018, 66, 1689–1697. [Google Scholar] [CrossRef]
- Nyaku, A.N.; Zheng, L.; Gulick, R.M.; Olefsky, M.; Berzins, B.; Wallis, C.L.; Godfrey, C.; Sax, P.E.; Acosta, E.P.; Haas, D.W.; et al. Dolutegravir plus Lamivudine for Initial Treatment of HIV-1-Infected Participants with HIV-1 RNA <500 000 Copies/mL: Week 48 Outcomes from ACTG 5353. J. Antimicrob. Chemother. 2019, 74, 1376–1380. [Google Scholar] [CrossRef] [PubMed]
- Rolle, C.-P.; Berhe, M.; Singh, T.; Ortiz, R.; Wurapa, A.; Ramgopal, M.; Leone, P.A.; Matthews, J.E.; Dalessandro, M.; Underwood, M.R.; et al. Dolutegravir/Lamivudine as a First-Line Regimen in a Test-and-Treat Setting for Newly Diagnosed People Living with HIV. AIDS 2021, 35, 1957–1965. [Google Scholar] [CrossRef] [PubMed]
- Rolle, C.-P.; Berhe, M.; Singh, T.; Ortiz, R.; Wurapa, A.; Ramgopal, M.; Jayaweera, D.T.; Leone, P.A.; Matthews, J.E.; Cupo, M.; et al. Sustained Virologic Suppression with Dolutegravir/Lamivudine in a Test-and-Treat Setting through 48 Weeks. Open Forum Infect. Dis. 2023, 10, ofad101. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo-Tenorio, C.; Pasquau, J.; Vinuesa, D.; Ferra, S.; Terrón, A.; SanJoaquín, I.; Payeras, A.; Martínez, O.J.; López-Ruz, M.Á.; Omar, M.; et al. DOLAVI Real-Life Study of Dolutegravir Plus Lamivudine in Naive HIV-1 Patients (48 Weeks). Viruses 2022, 14, 524. [Google Scholar] [CrossRef] [PubMed]
- Cahn, P.; Rolón, M.J.; Figueroa, M.I.; Gun, A.; Patterson, P.; Sued, O. Dolutegravir–Lamivudine as Initial Therapy in HIV-1 Infected, ARV-Naive Patients, 48-Week Results of the PADDLE (Pilot Antiretroviral Design with Dolutegravir LamivudinE) Study. J. Int. AIDS Soc. 2017, 20, 21678. [Google Scholar] [CrossRef]
- Cabello-Ubeda, A.; de Quirós, J.C.L.B.; Carbonero, L.M.; Sanz, J.; Vergas, J.; Mena, Á.; Torralba, M.; Segurado, M.H.; Pinto, A.; Tejerina, F.; et al. 48-Week Effectiveness and Tolerability of Dolutegravir (DTG) + Lamivudine (3TC) in Antiretroviral-Naïve Adults Living with HIV: A Multicenter Real-Life Cohort. PLoS ONE 2022, 17, e0277606. [Google Scholar] [CrossRef]
- Li, J.; Chen, D.; Wen, Z.; Du, Y.; Huang, Z.; Zhong, H.; Wang, Y.; Yin, S. Real-World Efficacy and Safety of Dolutegravir plus Lamivudine versus Tenofovir plus Lamivudine and Efavirenz in ART-Naïve HIV-1-Infected Adults. Medicine 2022, 101, e31100. [Google Scholar] [CrossRef]
- Cahn, P.; Pozniak, A.L.; Mingrone, H.; Shuldyakov, A.; Brites, C.; Andrade-Villanueva, J.F.; Richmond, G.; Buendia, C.B.; Fourie, J.; Ramgopal, M.; et al. Dolutegravir versus Raltegravir in Antiretroviral-Experienced, Integrase-Inhibitor-Naive Adults with HIV: Week 48 Results from the Randomised, Double-Blind, Non-Inferiority SAILING Study. Lancet 2013, 382, 700–708. [Google Scholar] [CrossRef]
- Underwood, M. Euro Resistance Wk: Resistance Post Week 48 in ART-Experienced, Integrase Inhibitor-Naive Subjects with Dolutegravir (DTG) vs. Raltegravir (RAL) in SAILING (ING111762). In Proceedings of the 13th European HIV & Hepatitis Workshop, Barcelona, Spain, 3–5 June 2015. [Google Scholar]
- Aboud, M.; Kaplan, R.; Lombaard, J.; Zhang, F.; Hidalgo, J.A.; Mamedova, E.; Losso, M.H.; Chetchotisakd, P.; Brites, C.; Sievers, J.; et al. Dolutegravir versus Ritonavir-Boosted Lopinavir Both with Dual Nucleoside Reverse Transcriptase Inhibitor Therapy in Adults with HIV-1 Infection in Whom First-Line Therapy Has Failed (DAWNING): An Open-Label, Non-Inferiority, Phase 3b Trial. Lancet Infect. Dis. 2019, 19, 253–264. [Google Scholar] [CrossRef]
- Underwood, M.; Horton, J.; Nangle, K.; Hopking, J.; Smith, K.; Aboud, M.; Wynne, B.; Sievers, J.; Stewart, E.L.; Wang, R. Integrase Inhibitor Resistance Mechanisms and Structural Characteristics in Antiretroviral Therapy-Experienced, Integrase Inhibitor-Naive Adults with HIV-1 Infection Treated with Dolutegravir plus Two Nucleoside Reverse Transcriptase Inhibitors in the DAWNING Study. Antimicrob. Agents Chemother. 2022, 66, e0164321. [Google Scholar] [CrossRef]
- Paton, N.I.; Musaazi, J.; Kityo, C.; Walimbwa, S.; Hoppe, A.; Balyegisawa, A.; Kaimal, A.; Mirembe, G.; Tukamushabe, P.; Ategeka, G.; et al. Dolutegravir or Darunavir in Combination with Zidovudine or Tenofovir to Treat HIV. N. Engl. J. Med. 2021, 385, 330–341. [Google Scholar] [CrossRef] [PubMed]
- Paton, N.I.; Musaazi, J.; Kityo, C.; Walimbwa, S.; Hoppe, A.; Balyegisawa, A.; Asienzo, J.; Kaimal, A.; Mirembe, G.; Lugemwa, A.; et al. Efficacy and Safety of Dolutegravir or Darunavir in Combination with Lamivudine plus Either Zidovudine or Tenofovir for Second-Line Treatment of HIV Infection (NADIA): Week 96 Results from a Prospective, Multicentre, Open-Label, Factorial, Randomised, Non-Inferiority Trial. Lancet HIV 2022, 9, e381–e393. [Google Scholar] [CrossRef] [PubMed]
- Keene, C.M.; Griesel, R.; Zhao, Y.; Gcwabe, Z.; Sayed, K.; Hill, A.; Cassidy, T.; Ngwenya, O.; Jackson, A.; van Zyl, G.; et al. Virologic Efficacy of Tenofovir, Lamivudine and Dolutegravir as Second-Line Antiretroviral Therapy in Adults Failing a Tenofovir-Based First-Line Regimen. AIDS 2021, 35, 1423–1432. [Google Scholar] [CrossRef] [PubMed]
- Keene, C.M.; Cassidy, T.; Zhao, Y.; Griesel, R.; Jackson, A.; Sayed, K.; Omar, Z.; Hill, A.; Ngwenya, O.; Van Zyl, G.; et al. Recycling Tenofovir in Second-Line Antiretroviral Treatment with Dolutegravir: Outcomes and Viral Load Trajectories to 72 Weeks. JAIDS J. Acquir. Immune Defic. Syndr. 2023, 92, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Griesel, R.; Omar, Z.; Simmons, B.; Hill, A.; van Zyl, G.; Keene, C.; Maartens, G.; Meintjes, G. Initial Supplementary Dose of Dolutegravir in Second-Line Antiretroviral Therapy: A Noncomparative, Double-Blind, Randomized Placebo-Controlled Trial. Clin. Infect. Dis. 2023, 76, 1832–1840. [Google Scholar] [CrossRef] [PubMed]
- Viani, R.M.; Alvero, C.; Fenton, T.; Acosta, E.P.; Hazra, R.; Townley, E.; Steimers, D.; Min, S.; Wiznia, A.; on Behalf of the P1093 Study Team. Safety, Pharmacokinetics and Efficacy of Dolutegravir in Treatment-Experienced HIV-1 Infected Adolescents: Forty-Eight-Week Results from IMPAACT P1093. Pediatr. Infect. Dis. J. 2015, 34, 1207–1213. [Google Scholar] [CrossRef]
- Viani, R.M.; Ruel, T.; Alvero, C.; Fenton, T.; Acosta, E.P.; Hazra, R.; Townley, E.; Palumbo, P.; Buchanan, A.M.; Vavro, C.; et al. Long-Term Safety and Efficacy of Dolutegravir in Treatment-Experienced Adolescents with Human Immunodeficiency Virus Infection: Results of the IMPAACT P1093 Study. J. Pediatr. Infect. Dis. Soc. 2020, 9, 159–165. [Google Scholar] [CrossRef]
- Vavro, C.; Ruel, T.; Wiznia, A.; Montañez, N.; Nangle, K.; Horton, J.; Buchanan, A.M.; Stewart, E.L.; Palumbo, P. Emergence of Resistance in HIV-1 Integrase with Dolutegravir Treatment in a Pediatric Population from the IMPAACT P1093 Study. Antimicrob. Agents Chemother. 2022, 66, e0164521. [Google Scholar] [CrossRef]
- Turkova, A.; White, E.; Mujuru, H.A.; Kekitiinwa, A.R.; Kityo, C.M.; Violari, A.; Lugemwa, A.; Cressey, T.R.; Musoke, P.; Variava, E.; et al. Dolutegravir as First- or Second-Line Treatment for HIV-1 Infection in Children. N. Engl. J. Med. 2021, 385, 2531–2543. [Google Scholar] [CrossRef] [PubMed]
- Amuge, P.; Lugemwa, A.; Wynne, B.; Mujuru, H.A.; Violari, A.; Kityo, C.M.; Archary, M.; Variava, E.; White, E.; Turner, R.M.; et al. Once-Daily Dolutegravir-Based Antiretroviral Therapy in Infants and Children Living with HIV from Age 4 Weeks: Results from the below 14 Kg Cohort in the Randomised ODYSSEY Trial. Lancet HIV 2022, 9, e638–e648. [Google Scholar] [CrossRef]
- Lepik, K.J.; Harrigan, P.R.; Yip, B.; Wang, L.; Robbins, M.A.; Zhang, W.W.; Toy, J.; Akagi, L.; Lima, V.D.; Guillemi, S.; et al. Emergent Drug Resistance with Integrase Strand Transfer Inhibitor-Based Regimens. AIDS 2017, 31, 1425–1434. [Google Scholar] [CrossRef]
- Sörstedt, E.; Carlander, C.; Flamholc, L.; Hejdeman, B.; Svedhem, V.; Sönnerborg, A.; Gisslén, M.; Yilmaz, A. Effect of Dolutegravir in Combination with Nucleoside Reverse Transcriptase Inhibitors (NRTIs) on People Living with HIV Who Have Pre-Existing NRTI Mutations. Int. J. Antimicrob. Agents 2018, 51, 733–738. [Google Scholar] [CrossRef]
- Schramm, B.; Temfack, E.; Descamps, D.; Nicholas, S.; Peytavin, G.; Bitilinyu-Bangoh, J.E.; Storto, A.; Lê, M.P.; Abdi, B.; Ousley, J.; et al. Viral Suppression and HIV-1 Drug Resistance 1 Year after Pragmatic Transitioning to Dolutegravir First-Line Therapy in Malawi: A Prospective Cohort Study. Lancet HIV 2022, 9, e544–e553. [Google Scholar] [CrossRef]
- Brown, J.A.; Nsakala, B.L.; Mokhele, K.; Rakuoane, I.; Muhairwe, J.; Urda, L.; Amstutz, A.; Tschumi, N.; Klimkait, T.; Labhardt, N.D. Viral Suppression after Transition from Nonnucleoside Reverse Transcriptase Inhibitor- to Dolutegravir-Based Antiretroviral Therapy: A Prospective Cohort Study in Lesotho (DO-REAL Study). HIV Med. 2022, 23, 287–293. [Google Scholar] [CrossRef]
- Semengue, E.N.J.; Fokam, J.; Etame, N.-K.; Molimbou, E.; Chenwi, C.A.; Takou, D.; Mossiang, L.; Meledie, A.P.; Yagai, B.; Nka, A.D.; et al. Dolutegravir-Based Regimen Ensures High Virological Success despite Prior Exposure to Efavirenz-Based First-LINE ART in Cameroon: An Evidence of a Successful Transition Model. Viruses 2023, 15, 18. [Google Scholar] [CrossRef]
- van Oosterhout, J.J.; Chipungu, C.; Nkhoma, L.; Kanise, H.; Hosseinipour, M.C.; Sagno, J.B.; Simon, K.; Cox, C.; Hoffman, R.; Steegen, K.; et al. Dolutegravir Resistance in Malawi’s National HIV Treatment Program. Open Forum Infect. Dis. 2022, 9, ofac148. [Google Scholar] [CrossRef]
- Abdullahi, A.; Kida, I.M.; Maina, U.A.; Ibrahim, A.H.; Mshelia, J.; Wisso, H.; Adamu, A.; Onyemata, J.E.; Edun, M.; Yusuph, H.; et al. Limited Emergence of Resistance to Integrase Strand Transfer Inhibitors (INSTIs) in ART-Experienced Participants Failing Dolutegravir-Based Antiretroviral Therapy: A Cross-Sectional Analysis of a Northeast Nigerian Cohort. J. Antimicrob. Chemother. 2023, 78, 2000–2007. [Google Scholar] [CrossRef] [PubMed]
- Kamori, D.; Barabona, G.; Rugemalila, J.; Maokola, W.; Masoud, S.S.; Mizinduko, M.; Sabasaba, A.; Ruhago, G.; Sambu, V.; Mushi, J.; et al. Emerging Integrase Strand Transfer Inhibitor Drug Resistance Mutations among Children and Adults on ART in Tanzania: Findings from a National Representative HIV Drug Resistance Survey. J. Antimicrob. Chemother. 2023, 78, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Khamadi, S.A.; Bahemana, E.; Dear, N.; Mavere, C.; George, F.; Kapene, R.; Papianus, G.; Willoughby, W.; Chambers, J.; Ganesan, K.; et al. Factors Associated with Viral Suppression and Drug Resistance in Children and Adolescents Living with HIV in Care and Treatment Programs in Southern Tanzania. J. Pediatr. Infect. Dis. Soc. 2023, 12, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Bwire, G.M.; Aiko, B.G.; Mosha, I.H.; Kilapilo, M.S.; Mangara, A.; Kazonda, P.; Swai, J.P.; Swalehe, O.; Jordan, M.R.; Vercauteren, J.; et al. High Viral Suppression and Detection of Dolutegravir-Resistance Associated Mutations in Treatment-Experienced Tanzanian Adults Living with HIV-1 in Dar Es Salaam. Sci. Rep. 2023, 13, 20493. [Google Scholar] [CrossRef]
- Gatell, J.M.; Assoumou, L.; Moyle, G.; Waters, L.; Johnson, M.; Domingo, P.; Fox, J.; Martinez, E.; Stellbrink, H.-J.; Guaraldi, G.; et al. Switching from a Ritonavir-Boosted Protease Inhibitor to a Dolutegravir-Based Regimen for Maintenance of HIV Viral Suppression in Patients with High Cardiovascular Risk. AIDS 2017, 31, 2503–2514. [Google Scholar] [CrossRef]
- Gatell, J.M.; Assoumou, L.; Moyle, G.; Waters, L.; Johnson, M.; Domingo, P.; Fox, J.; Martinez, E.; Stellbrink, H.-J.; Guaraldi, G.; et al. Immediate Versus Deferred Switching from a Boosted Protease Inhibitor–Based Regimen to a Dolutegravir-Based Regimen in Virologically Suppressed Patients with High Cardiovascular Risk or Age ≥50 Years: Final 96-Week Results of the NEAT022 Study. Clin. Infect. Dis. 2019, 68, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Trottier, B.; Lake, J.E.; Logue, K.; Brinson, C.; Santiago, L.; Brennan, C.; Koteff, J.A.; Wynne, B.; Hopking, J.; Granier, C.; et al. Dolutegravir/Abacavir/Lamivudine versus Current ART in Virally Suppressed Patients (STRIIVING): A 48-Week, Randomized, Non-Inferiority, Open-Label, Phase IIIb Study. Antivir. Ther. 2017, 22, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Ombajo, L.A.; Penner, J.; Nkuranga, J.; Mecha, J.; Mburu, M.; Odhiambo, C.; Ndinya, F.; Aksam, R.; Njenga, R.; Wahome, S.; et al. Second-Line Switch to Dolutegravir for Treatment of HIV Infection. N. Engl. J. Med. 2023, 388, 2349–2359. [Google Scholar] [CrossRef] [PubMed]
- Olearo, F.; Nguyen, H.; Bonnet, F.; Yerly, S.; Wandeler, G.; Stoeckle, M.; Cavassini, M.; Scherrer, A.; Costagiola, D.; Schmid, P.; et al. Impact of the M184V/I Mutation on the Efficacy of Abacavir/Lamivudine/Dolutegravir Therapy in HIV Treatment-Experienced Patients. Open Forum Infect. Dis. 2019, 6, ofz330. [Google Scholar] [CrossRef] [PubMed]
- Jary, A.; Marcelin, A.-G.; Charpentier, C.; Wirden, M.; Lê, M.P.; Peytavin, G.; Descamps, D.; Calvez, V. M184V/I Does Not Impact the Efficacy of Abacavir/Lamivudine/Dolutegravir Use as Switch Therapy in Virologically Suppressed Patients. J. Antimicrob. Chemother. 2020, 75, 1290–1293. [Google Scholar] [CrossRef] [PubMed]
- Borghetti, A.; Alkhatib, M.; Dusina, A.; Duca, L.; Borghi, V.; Zazzi, M.; Di Giambenedetto, S. Virological Outcomes with Dolutegravir plus Either Lamivudine or Two NRTIs as Switch Strategies: A Multi-Cohort Study. J. Antimicrob. Chemother. 2022, 77, 740–746. [Google Scholar] [CrossRef] [PubMed]
- van Wyk, J.; Ajana, F.; Bisshop, F.; De Wit, S.; Osiyemi, O.; Portilla Sogorb, J.; Routy, J.-P.; Wyen, C.; Ait-Khaled, M.; Nascimento, M.C.; et al. Efficacy and Safety of Switching to Dolutegravir/Lamivudine Fixed-Dose 2-Drug Regimen vs. Continuing a Tenofovir Alafenamide–Based 3- or 4-Drug Regimen for Maintenance of Virologic Suppression in Adults Living with Human Immunodeficiency Virus Type 1: Phase 3, Randomized, Noninferiority TANGO Study. Clin. Infect. Dis. 2020, 71, 1920–1929. [Google Scholar] [CrossRef]
- Osiyemi, O.; De Wit, S.; Ajana, F.; Bisshop, F.; Portilla, J.; Routy, J.P.; Wyen, C.; Ait-Khaled, M.; Leone, P.; Pappa, K.A.; et al. Efficacy and Safety of Switching to Dolutegravir/Lamivudine Versus Continuing a Tenofovir Alafenamide–Based 3- or 4-Drug Regimen for Maintenance of Virologic Suppression in Adults Living with Human Immunodeficiency Virus Type 1: Results through Week 144 From the Phase 3, Noninferiority TANGO Randomized Trial. Clin. Infect. Dis. 2022, 75, 975–986. [Google Scholar] [CrossRef]
- Llibre, J.M.; Brites, C.; Cheng, C.-Y.; Osiyemi, O.; Galera, C.; Hocqueloux, L.; Maggiolo, F.; Degen, O.; Taylor, S.; Blair, E.; et al. Efficacy and Safety of Switching to the 2-Drug Regimen Dolutegravir/Lamivudine Versus Continuing a 3- or 4-Drug Regimen for Maintaining Virologic Suppression in Adults Living with Human Immunodeficiency Virus 1 (HIV-1): Week 48 Results from the Phase 3, Noninferiority SALSA Randomized Trial. Clin. Infect. Dis. 2023, 76, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Rojas, J.; de Lazzari, E.; Negredo, E.; Domingo, P.; Tiraboschi, J.; Ribera, E.; Abdulghani, N.; Puig, J.; Mateo, M.G.; Podzamczer, D.; et al. Efficacy and Safety of Switching to Dolutegravir plus Lamivudine versus Continuing Triple Antiretroviral Therapy in Virologically Suppressed Adults with HIV at 48 Weeks (DOLAM): A Randomised Non-Inferiority Trial. Lancet HIV 2021, 8, e463–e473. [Google Scholar] [CrossRef] [PubMed]
- Joly, V.; Burdet, C.; Landman, R.; Vigan, M.; Charpentier, C.; Katlama, C.; Cabié, A.; Benalycherif, A.; Peytavin, G.; Yeni, P.; et al. Dolutegravir and Lamivudine Maintenance Therapy in HIV-1 Virologically Suppressed Patients: Results of the ANRS 167 Trial (LAMIDOL). J. Antimicrob. Chemother. 2019, 74, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Taiwo, B.O.; Marconi, V.C.; Berzins, B.; Moser, C.B.; Nyaku, A.N.; Fichtenbaum, C.J.; Benson, C.A.; Wilkin, T.; Koletar, S.L.; Colasanti, J.; et al. Dolutegravir Plus Lamivudine Maintains Human Immunodeficiency Virus-1 Suppression Through Week 48 in a Pilot Randomized Trial. Clin. Infect. Dis. 2018, 66, 1794–1797. [Google Scholar] [CrossRef] [PubMed]
- De Miguel Buckley, R.; Rial-Crestelo, D.; Montejano, R.; Pinto, A.; Jimenez-Gonzalez, M.; Lagarde, M.; Esteban-Cantos, A.; Aranguren-Rivas, P.; Cadiñanos, J.; Bisbal, O.; et al. Long-Term Evaluation of Residual Viremia in a Clinical Trial of Dolutegravir Plus Lamivudine as Maintenance Treatment for Participants with and without Prior Lamivudine Resistance. Open Forum Infect. Dis. 2022, 9, ofac610. [Google Scholar] [CrossRef] [PubMed]
- Rial-Crestelo, D.; de Miguel, R.; Montejano, R.; Dominguez-Dominguez, L.; Aranguren-Rivas, P.; Esteban-Cantos, A.; Bisbal, O.; Santacreu-Guerrero, M.; Garcia-Alvarez, M.; Alejos, B.; et al. Long-Term Efficacy of Dolutegravir plus Lamivudine for Maintenance of HIV Viral Suppression in Adults with and without Historical Resistance to Lamivudine: Week 96 Results of ART-PRO Pilot Study. J. Antimicrob. Chemother. 2021, 76, 738–742. [Google Scholar] [CrossRef] [PubMed]
- De Miguel, R.; Rial-Crestelo, D.; Dominguez-Dominguez, L.; Montejano, R.; Esteban-Cantos, A.; Aranguren-Rivas, P.; Stella-Ascariz, N.; Bisbal, O.; Bermejo-Plaza, L.; Garcia-Alvarez, M.; et al. Dolutegravir plus Lamivudine for Maintenance of HIV Viral Suppression in Adults with and without Historical Resistance to Lamivudine: 48-Week Results of a Non-Randomized, Pilot Clinical Trial (ART-PRO). EBioMedicine 2020, 55, 102779. [Google Scholar] [CrossRef]
- Sculier, D.; Wandeler, G.; Yerly, S.; Marinosci, A.; Stoeckle, M.; Bernasconi, E.; Braun, D.L.; Vernazza, P.; Cavassini, M.; Buzzi, M.; et al. Efficacy and Safety of Dolutegravir plus Emtricitabine versus Standard ART for the Maintenance of HIV-1 Suppression: 48-Week Results of the Factorial, Randomized, Non-Inferiority SIMPL’HIV Trial. PLoS Med. 2020, 17, e1003421. [Google Scholar] [CrossRef]
- Llibre, J.M.; Hung, C.-C.; Brinson, C.; Castelli, F.; Girard, P.-M.; Kahl, L.P.; Blair, E.A.; Angelis, K.; Wynne, B.; Vandermeulen, K.; et al. Efficacy, Safety, and Tolerability of Dolutegravir-Rilpivirine for the Maintenance of Virological Suppression in Adults with HIV-1: Phase 3, Randomised, Non-Inferiority SWORD-1 and SWORD-2 Studies. Lancet 2018, 391, 839–849. [Google Scholar] [CrossRef]
- Aboud, M.; Orkin, C.; Podzamczer, D.; Bogner, J.R.; Baker, D.; Khuong-Josses, M.-A.; Parks, D.; Angelis, K.; Kahl, L.P.; Blair, E.A.; et al. Efficacy and Safety of Dolutegravir–Rilpivirine for Maintenance of Virological Suppression in Adults with HIV-1: 100-Week Data from the Randomised, Open-Label, Phase 3 SWORD-1 and SWORD-2 Studies. Lancet HIV 2019, 6, e576–e587. [Google Scholar] [CrossRef]
- van Wyk, J.; Orkin, C.; Rubio, R.; Bogner, J.; Baker, D.; Khuong-Josses, M.-A.; Parks, D.; Angelis, K.; Kahl, L.P.; Matthews, J.; et al. Brief Report: Durable Suppression and Low Rate of Virologic Failure 3 Years After Switch to Dolutegravir + Rilpivirine 2-Drug Regimen: 148-Week Results From the SWORD-1 and SWORD-2 Randomized Clinical Trials. J. Acquir. Immune Defic. Syndr. 2020, 85, 325–330. [Google Scholar] [CrossRef]
- Spinner, C.D.; Kümmerle, T.; Schneider, J.; Cordes, C.; Heiken, H.; Stellbrink, H.-J.; Krznaric, I.; Scholten, S.; Jensen, B.; Wyen, C.; et al. Efficacy and Safety of Switching to Dolutegravir with Boosted Darunavir in Virologically Suppressed Adults with HIV-1: A Randomized, Open-Label, Multicenter, Phase 3, Noninferiority Trial: The DUALIS Study. Open Forum Infect. Dis. 2020, 7, ofaa356. [Google Scholar] [CrossRef]
- Wolf, E.; Boesecke, C.; Balogh, A.; Bidner, H.; Cordes, C.; Heiken, H.; Krznaric, I.; Kümmerle, T.; Stellbrink, H.-J.; Schneider, J.; et al. Virologic Outcomes of Switching to Boosted Darunavir plus Dolutegravir with Respect to History of Drug Resistance. AIDS Res. Ther. 2021, 18, 58. [Google Scholar] [CrossRef]
- Compagnucci, A.; Chan, M.K.; Saïdi, Y.; Cressey, T.R.; Bamford, A.; Riault, Y.; Coelho, A.; Nolan, A.; Chalermpantmetagul, S.; Morkunaite, G.; et al. Nucleoside/Nucleotide Reverse Transcriptase Inhibitor Sparing Regimen with Once Daily Integrase Inhibitor plus Boosted Darunavir Is Non-Inferior to Standard of Care in Virologically-Suppressed Children and Adolescents Living with HIV—Week 48 Results of the Randomised SMILE Penta-17-ANRS 152 Clinical Trial. EClinicalMedicine 2023, 60, 102025. [Google Scholar] [CrossRef]
- Gantner, P.; Cuzin, L.; Allavena, C.; Cabie, A.; Pugliese, P.; Valantin, M.-A.; Bani-Sadr, F.; Joly, V.; Ferry, T.; Poizot-Martin, I.; et al. Efficacy and Safety of Dolutegravir and Rilpivirine Dual Therapy as a Simplification Strategy: A Cohort Study. HIV Med. 2017, 18, 704–708. [Google Scholar] [CrossRef]
- Baldin, G.; Ciccullo, A.; Borghetti, A.; Di Giambenedetto, S. Virological Efficacy of Dual Therapy with Lamivudine and Dolutegravir in HIV-1-Infected Virologically Suppressed Patients: Long-Term Data from Clinical Practice. J. Antimicrob. Chemother. 2019, 74, 1461–1463. [Google Scholar] [CrossRef]
- Casado, J.L.; Monsalvo, M.; Fontecha, M.; Vizcarra, P.; Rodriguez, M.A.; Vivancos, M.J.; Moreno, S. Dolutegravir plus Rilpivirine as Dual Regimen in Virologically Suppressed HIV-1 Infected Patients in a Clinical Setting. HIV Res. Clin. Pract. 2019, 20, 64–72. [Google Scholar] [CrossRef]
- Castagna, A.; Rusconi, S.; Gulminetti, R.; Bonora, S.; Mazzola, G.; Quiros-Roldan, M.E.; De Socio, G.V.; Ladisa, N.; Carosella, S.; Cattelan, A.; et al. Switch to Dolutegravir and Unboosted Atazanavir in HIV-1 Infected Patients with Undetectable Viral Load and Long Exposure to Antiretroviral Therapy. AIDS 2019, 33, 1256–1260. [Google Scholar] [CrossRef] [PubMed]
- Calza, L.; Colangeli, V.; Borderi, M.; Testi, D.; Granozzi, B.; Bon, I.; Re, M.C.; Viale, P. Simplification to Dual Therapy Containing Lamivudine and Raltegravir or Dolutegravir in HIV-Infected Patients on Virologically Suppressive Antiretroviral Therapy. J. Antimicrob. Chemother. 2020, 75, 3327–3333. [Google Scholar] [CrossRef] [PubMed]
- Ciccullo, A.; Borghi, V.; Giacomelli, A.; Cossu, M.V.; Sterrantino, G.; Latini, A.; Giacometti, A.; De Vito, A.; Gennari, W.; Madeddu, G.; et al. Five Years with Dolutegravir Plus Lamivudine as a Switch Strategy: Much More Than a Positive Finding. JAIDS J. Acquir. Immune Defic. Syndr. 2021, 88, 234. [Google Scholar] [CrossRef] [PubMed]
- Ciccullo, A.; Baldin, G.; Borghi, V.; Cossu, M.V.; Giacomelli, A.; Lagi, F.; Farinacci, D.; Iannone, V.; Passerotto, R.A.; Capetti, A.; et al. Analysing the Efficacy and Tolerability of Dolutegravir plus Either Rilpivirine or Lamivudine in a Multicentre Cohort of Virologically Suppressed PLWHIV. J. Antimicrob. Chemother. 2023, 78, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Ergen, P.; Bektas, B.; Aydın, Ö.; Keskin, H.; Üçışık, A.C.; Karadağ, F.Y.; Cağ, Y. Evaluation of Treatment Efficacy after Switching to Dolutegravir-Lamivudine Dual Therapy in People Living with HIV. Afr. Health Sci. 2022, 22, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Kim, J.; Lee, J.A.; Kim, C.H.; Ahn, J.Y.; Jeong, S.J.; Ku, N.S.; Choi, J.Y.; Yeom, J.-S.; Song, Y.G.; et al. Real-World Effectiveness, Tolerability, and Safety of Dolutegravir/Lamivudine in Korea. Viruses 2022, 14, 2558. [Google Scholar] [CrossRef]
- Maggiolo, F.; Gulminetti, R.; Pagnucco, L.; Digaetano, M.; Cervo, A.; Valenti, D.; Callegaro, A.; Mussini, C. Long-Term Outcome of Lamivudine/Dolutegravir Dual Therapy in HIV-Infected, Virologically Suppressed Patients. BMC Infect. Dis. 2022, 22, 782. [Google Scholar] [CrossRef] [PubMed]
- Troya, J.; Dueñas, C.; Irazola, I.; de los Santos, I.; de la Fuente, S.; Gil, D.; Hernández, C.; Galindo, M.J.; Gómez, J.; Delgado, E.; et al. Dolutegravir plus Rilpivirine: Benefits beyond Viral Suppression: DORIPEX Retrospective Study. Medicine 2022, 101, e29252. [Google Scholar] [CrossRef]
- Bowman, C.; Ambrose, A.; Kanitkar, T.; Flores, K.; Simoes, P.; Hart, J.; Hunter, A.; Akodu, J.; Barber, T.J. Real World Use of Dolutegravir Two Drug Regimens. AIDS 2023, 37, 785–788. [Google Scholar] [CrossRef]
- Buzón, L.; Dueñas, C.; Pedrero, R.; Iribarren, J.A.; de los Santos, I.; Díaz de Santiago, A.; Morán, M.Á.; Pousada, G.; Moreno, E.; Ferreira, E.; et al. Dolutegravir Plus 3TC in Virologically Suppressed PLWHIV: Immunological Outcomes in a Multicenter Retrospective Cohort in Spain during the COVID-19 Pandemic. Viruses 2023, 15, 322. [Google Scholar] [CrossRef]
- Palmier, E.; De Miguel, R.; Montejano, R.; Busca, C.; Micán, R.; Ramos, L.; Cadiñanos, J.; Serrano, L.; Bernardino, J.I.; Pérez-Valero, I.; et al. Three-Year Efficacy of Switching to Dolutegravir plus Lamivudine: A Real-World Study. HIV Med. 2023, 24, 1013–1019. [Google Scholar] [CrossRef]
- Calza, L.; Colangeli, V.; Legnani, G.; Cretella, S.; Bon, I.; Viale, P. Efficacy and Safety of Switching to Dolutegravir/Lamivudine in Virologically Suppressed People Living with HIV-1 Aged over 65 Years. AIDS Res. Hum. Retroviruses 2023, 40, 73–79. [Google Scholar] [CrossRef]
- Knobel, H.; Cañas-Ruano, E.; Guelar, A.; Knobel, P.; Villar-García, J.; González-Mena, A.; Canepa, C.; Arrieta-Aldea, I.; Marcos, A.; Abalat-Torrres, A.; et al. Switching to Dolutegravir/Lamivudine or Bictegravir/Emtricitabine/Tenofovir Alafenamide. A Comparative Real-World Study. HIV Res. Clin. Pract. 2023, 24, 2239564. [Google Scholar]
- Poliseno, M.; Mazzitelli, M.; Narducci, A.; Ferrara, S.M.; Resnati, C.; Gervasoni, C.; Cattelan, A.M.; Lo Caputo, S. Doravirine Plus Integrase Strand Transfer Inhibitors as a 2-Drug Treatment–Switch Strategy in People Living with HIV: The Real-Life DORINI Multicentric Cohort Study. JAIDS J. Acquir. Immune Defic. Syndr. 2023, 94, 235–243. [Google Scholar] [CrossRef]
- Wijting, I.; Rokx, C.; Boucher, C.; van Kampen, J.; Pas, S.; de Vries-Sluijs, T.; Schurink, C.; Bax, H.; Derksen, M.; Andrinopoulou, E.-R.; et al. Dolutegravir as Maintenance Monotherapy for HIV (DOMONO): A Phase 2, Randomised Non-Inferiority Trial. Lancet HIV 2017, 4, e547–e554. [Google Scholar] [CrossRef]
- Wijting, I.E.A.; Lungu, C.; Rijnders, B.J.A.; van der Ende, M.E.; Pham, H.T.; Mesplede, T.; Pas, S.D.; Voermans, J.J.C.; Schuurman, R.; van de Vijver, D.A.M.C.; et al. HIV-1 Resistance Dynamics in Patients with Virologic Failure to Dolutegravir Maintenance Monotherapy. J. Infect. Dis. 2018, 218, 688–697. [Google Scholar] [CrossRef]
- Wijting, I.; Rutsaert, S.; Rokx, C.; Burger, D.; Verbon, A.; van Kampen, J.; Boucher, C.; Rijnders, B.; Vandekerckhove, L. Predictors of Virological Failure in HIV-1-Infected Patients Switching to Dolutegravir Maintenance Monotherapy. HIV Med. 2019, 20, 63–68. [Google Scholar] [CrossRef]
- Blanco, J.L.; Rojas, J.; Paredes, R.; Negredo, E.; Mallolas, J.; Casadella, M.; Clotet, B.; Gatell, J.M.; de Lazzari, E.; Martinez, E.; et al. Dolutegravir-Based Maintenance Monotherapy versus Dual Therapy with Lamivudine: A Planned 24 Week Analysis of the DOLAM Randomized Clinical Trial. J. Antimicrob. Chemother. 2018, 73, 1965–1971. [Google Scholar] [CrossRef]
- Braun, D.L.; Turk, T.; Tschumi, F.; Grube, C.; Hampel, B.; Depmeier, C.; Schreiber, P.W.; Brugger, S.D.; Greiner, M.; Steffens, D.; et al. Noninferiority of Simplified Dolutegravir Monotherapy Compared to Continued Combination Antiretroviral Therapy That Was Initiated During Primary Human Immunodeficiency Virus Infection: A Randomized, Controlled, Multisite, Open-Label, Noninferiority Trial. Clin. Infect. Dis. 2019, 69, 1489–1497. [Google Scholar] [CrossRef]
- West, E.; Zeeb, M.; Grube, C.; Kuster, H.; Wanner, K.; Scheier, T.; Neumann, K.; Jörimann, L.; Hampel, B.; Metzner, K.J.; et al. Sustained Viral Suppression with Dolutegravir Monotherapy over 192 Weeks in Patients Starting Combination Antiretroviral Therapy during Primary HIV Infection (EARLY-SIMPLIFIED): A Randomized, Controlled, Multi-Site, Non-Inferiority Trial. Clin. Infect. Dis. 2023, 77, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Hocqueloux, L.; Raffi, F.; Prazuck, T.; Bernard, L.; Sunder, S.; Esnault, J.-L.; Rey, D.; Le Moal, G.; Roncato-Saberan, M.; André, M.; et al. Dolutegravir Monotherapy Versus Dolutegravir/Abacavir/Lamivudine for Virologically Suppressed People Living with Chronic Human Immunodeficiency Virus Infection: The Randomized Noninferiority MONotherapy of TiviCAY Trial. Clin. Infect. Dis. 2019, 69, 1498–1505. [Google Scholar] [CrossRef] [PubMed]
- Rojas, J.; Blanco, J.L.; Marcos, M.A.; Lonca, M.; Tricas, A.; Moreno, L.; Gonzalez-Cordon, A.; Torres, B.; Mallolas, J.; Garcia, F.; et al. Dolutegravir Monotherapy in HIV-Infected Patients with Sustained Viral Suppression. J. Antimicrob. Chemother. 2016, 71, 1975–1981. [Google Scholar] [CrossRef] [PubMed]
- Oldenbuettel, C.; Wolf, E.; Ritter, A.; Noe, S.; Heldwein, S.; Pascucci, R.; Wiese, C.; Krosigk, A.V.; Jaegel-Guedes, E.; Jaeger, H.; et al. Dolutegravir Monotherapy as Treatment De-Escalation in HIV-Infected Adults with Virological Control: DoluMono Cohort Results. Antivir. Ther. 2017, 22, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Tebano, G.; Soulié, C.; Schneider, L.; Blanc, C.; Agher, R.; Seang, S.; Valantin, M.A.; Palich, R.; Tubiana, R.; Peytavin, G.; et al. Long-Term Follow-up of HIV-Infected Patients on Dolutegravir Monotherapy. J. Antimicrob. Chemother. 2020, 75, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Gregson, J.; Kaleebu, P.; Marconi, V.C.; Van Vuuren, C.; Ndembi, N.; Hamers, R.L.; Kanki, P.; Hoffmann, C.J.; Lockman, S.; Pillay, D.; et al. Occult HIV-1 Drug Resistance to Thymidine Analogues Following Failure of First-Line Tenofovir Combined with a Cytosine Analogue and Nevirapine or Efavirenz in Sub Saharan Africa: A Retrospective Multi-Centre Cohort Study. Lancet Infect. Dis. 2017, 17, 296–304. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. HIV Drug Resistance Report 2021; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Benade, M.; Maskew, M.; Juntunen, A.; Flynn, D.B.; Rosen, S. Prior Exposure to Antiretroviral Therapy among Adult Patients Presenting for HIV Treatment Initiation or Reinitiation in Sub-Saharan Africa: A Systematic Review. BMJ Open 2023, 13, e071283. [Google Scholar] [CrossRef] [PubMed]
- Mulenga, L.B.; Fwoloshi, S.; Mweemba, A.; Siwingwa, M.; Sivile, S.; Kampamba, D.; Engamba, D.C.; Mbewe, N.; Phiri, H.; Shibemba, A.; et al. Dolutegravir with Recycled Nrtis Is Noninferior to Pi-Based Art: Visend Trial. In Proceedings of the 29th Conference on Retroviruses and Opportunistic Infections, Virtual, 12–16 February 2022. [Google Scholar]
- Matthews, G.; Borok, M.; Eriobou, N.; Kaplan, R.; Kumarasamy, N.; Avihingsanon, A.; Losso, M.H.; Azwa, I.S.; Karyana, M.; Dao, S.; et al. D2EFT: Dolutegravir and Darunavir Evaluation in Adults Failing First-Line Hiv Therapy. In Proceedings of the 30th Conference on Retroviruses and Opportunistic Infections, Seattle, WA, USA, 19–22 February 2023. [Google Scholar]
- World Health Organization. Sentinel Surveys of Acquired HIV Resistance to Dolutegravir among People Receiving Dolutegravir Containing Antiviral Therapy; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- da Silva, J.; Pals, S.; Chang, J.; Hackett, S.; Godfrey, C.; Raizes, E. Monitoring Emerging Human Immunodeficiency Virus Drug Resistance in Sub-Saharan Africa in the Era of Dolutegravir. J. Infect. Dis. 2022, 225, 364–366. [Google Scholar] [CrossRef]
- Bhatt, N.; Ismail, N.; Magule, C.; Hussein, C.; Meque, I.; Couto, A.; Nhangave, A.; Muteerwa, A.; Bonou, A.; Ramos, A.; et al. HIV Drug Resistance Profile in Clients Experiencing Treatment Failure after the Transition Fo a Dolutegravir-Based First-Line Antiretroviral Treatment Regimen in Mozambique [Abstract 51]. In Proceedings of the International Workshop on HIV Drug Resistance and Treatment Strategies, Cape Town, South Africa, 20–22 September 2023. [Google Scholar]
- Kalata, N.; Pals, S.; Bighignoli, B.; Kabaghe, A.; Mkungudza, J.; Panja, L.; Raizes, E.; Chitenje, M.; Kampira, E.; Maida, A.; et al. HIV Drug Resistance to Dolutegravir Is Uncommon among Adults Investigated for Treatment Failure in Malawi [Abstract 53]. In Proceedings of the International Workshop on HIV Drug Resistance and Treatment Strategies, Cape Town, South Africa, 20–22 September 2023. [Google Scholar]
- Namayanja, G.; Watera, C.; Pais, S.; Asio, J.; Ssemwanga, D.; Sanyu, G.; Zheng, D.; Zeh, C.; Hackett, S.; Ntali, J.; et al. Cyclic Acquired HIV Drug Resistance to Dolutegravir among People Living with HIV in Uganda. National Remnant Samples Surveillance 2022 [Abstract 50]. In Proceedings of the International Workshop on HIV Drug Resistance and Treatment Strategies, Cape Town, South Africa, 20–22 September 2023. [Google Scholar]
- Parikh, A.; Ochleng, C.; Almas, S.; Habib, P.; Towett, J.; Daud, I.; Maswal, J.; Owuoth, J.; Singoel, V.; Bahamena, E.; et al. HIV Drug Resistance in the Dolutegravir Era: Preliminary Results from East Africa [Abstract 56]. In Proceedings of the International Workshop on HIV Drug Resistance and Treatment Strategies, Cape Town, South Africa, 20–22 September 2023. [Google Scholar]

| Clinical Scenario | ART History | Viral Load Prior to DTG | DTG-Containing ART | Clinical Trials (Number Trials) | Clinical Trials (Number PLWH) | Cohort Studies (Number Studies) | Cohort Studies (Number PLWH) | Cross-Sectional Studies (Number Studies) | Cross-Sectional Studies (Number PLWH) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Naïve | Viremic | DTG + 2 NRTIs | 16 | 4585 | 7 | 2698 | 1 | 113 |
| 2 | Naïve | Viremic | DTG + 3TC | 4 | 1075 | 3 | 581 | 0 | 0 |
| 3 | Experienced | Viremic | DTG + 2 NRTIs | 6 | 1428 | 5 | 3630 | 4 | 218 |
| 4 | Experienced | Suppressed | DTG + 2 NRTIs | 3 | 877 | 3 | 2204 | 0 | 0 |
| 5 | Experienced | Suppressed | DTG + 2nd ARV | 10 | 1894 | 18 | 5930 | 0 | 0 |
| 6 | Experienced | Suppressed | DTG monotherapy | 4 | 276 | 3 | 123 | 0 | 0 |
| Trial | Regions | Population 1 | DTG-Containing Regimen 2 | # PLWH | Weeks | # (%) VF 3 | # (%) Undergoing GRT | # (%) with INSTI DRMs 4 |
|---|---|---|---|---|---|---|---|---|
| SAILING 2013, 2015 [51,52] | Europe, North America, South America, Asia, Oceania, Africa | Adults; VL ≥ 400; INSTI-naïve, ≥2-class resistance | DTG + OBR | 354 | 48 | 21 (5.9%) | 9 (2.5%) | 2 (0.6%) |
| DAWNING 2019, 2022 [53,54] | Europe, South America, Asia, Africa | Adults; VL ≥ 400 on a first-line NNRTI-containing regimen | DTG + 2 NRTIs (≥1 fully active) | 312 | 48 | 11 (3.5%) | 11 (3.5%) | 3 (1.0%) |
| NADIA 2021, 2022 [55,56] 5 | Uganda, Kenya, Zimbabwe | Adults/Adolescents; VL ≥ 1000 on a first-line NNRTI-containing regimen | DTG + TDF/3TC or AZT/3TC | 235 | 96 | 24 (10.2%) | 21 (8.9%) | 9 (3.8%) |
| ARTIST 2021, 2023 [57,58,59] | South Africa | Adults; VL ≥ 400 while on a first-line NNRTI-containing regimen | DTG + TDF/3TC | 135 | 24 | 21 (15.6%) | 4 (3.0%) | 0 (0%) |
| DTG BID + TDF/3TC | 64 | 24 | 9 (14.1%) | 3 (4.7%) | 0 (0%) | |||
| IMPAACT P1093 2015, 2020, 2022 [60,61,62] | North America, South America, Asia, Africa | Infants/children/adolescents with VL ≥ 1000; most ART-experienced | DTG + 2 NRTIs | 142 | 48 | 36 (25.3%) | 36 (25.3%) | 5 (3.5%) |
| ODYSSEY 2021, 2022 [63,64] | Europe, Asia, Africa | Children and adolescents with V ≥ 500 on a 1st- or 2nd-line ART regimen | DTG + 2 NRTIs | 196 | 96 | 31 (15.8%) | 29 (14.7%) | 4 (2.0%) |
| Clinical Scenario | ART History | Viral Load Prior to DTG | DTG-Containing ART | # Clinical Trials | Median (IQR) # Participants | Median (IQR) % with VF 1 | Median (IQR) % with GRT 2 | Median (IQR) % with INSTI-DRMs |
|---|---|---|---|---|---|---|---|---|
| 1 | Naïve | Viremic | DTG + 2 NRTIs | 16 | 279 (106–410) | 4.4 (2.8–6.1) | 2.7 (1.0–5.0) | 0 (0–0) |
| 2 | Naïve | Viremic | DTG + 3TC | 4 | 126 (96–570) | 9.4 (3.6–14.3) | 1.5 (1.2–2.9) | 0 (0–0.6) |
| 3 | Experienced | Viremic | DTG + 2 NRTIs | 6 | 217 (183–323) | 12.7 (5.3–18.2) | 6.6 (3.3–17.4) | 1.5 (0.5–3.6) |
| 4 | Experienced | Suppressed | DTG + 2 NRTIs | 3 | 275 (205–397) | 2.4 (0–5.0) | 0 (0–1.5) | 0 (0–0) |
| 5 | Experienced | Suppressed | DTG + 2nd ARV | 10 | 131 (81–277) | 1.7 (0.4–3.0) | 1.1 (0–2.3) | 0 (0–0) |
| 6 | Experienced | Suppressed | DTG monotherapy | 4 | 73 (40–93) | 7.8 (1.6–9.8) | 7.3 (1.6–8.8) | 3.4 (0.7–5.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, C.; Tao, K.; Kouamou, V.; Avalos, A.; Scott, J.; Grant, P.M.; Rhee, S.-Y.; McCluskey, S.M.; Jordan, M.R.; Morgan, R.L.; et al. Prevalence of Emergent Dolutegravir Resistance Mutations in People Living with HIV: A Rapid Scoping Review. Viruses 2024, 16, 399. https://doi.org/10.3390/v16030399
Chu C, Tao K, Kouamou V, Avalos A, Scott J, Grant PM, Rhee S-Y, McCluskey SM, Jordan MR, Morgan RL, et al. Prevalence of Emergent Dolutegravir Resistance Mutations in People Living with HIV: A Rapid Scoping Review. Viruses. 2024; 16(3):399. https://doi.org/10.3390/v16030399
Chicago/Turabian StyleChu, Carolyn, Kaiming Tao, Vinie Kouamou, Ava Avalos, Jake Scott, Philip M. Grant, Soo-Yon Rhee, Suzanne M. McCluskey, Michael R. Jordan, Rebecca L. Morgan, and et al. 2024. "Prevalence of Emergent Dolutegravir Resistance Mutations in People Living with HIV: A Rapid Scoping Review" Viruses 16, no. 3: 399. https://doi.org/10.3390/v16030399