
Factors Associated with SARS-CoV-2 Infection in Fully Vaccinated Nursing Home Residents and Workers
 , , , , , , , , , , and
, , , , , , , , , , and
Abstract
:1. Introduction
2. Methods
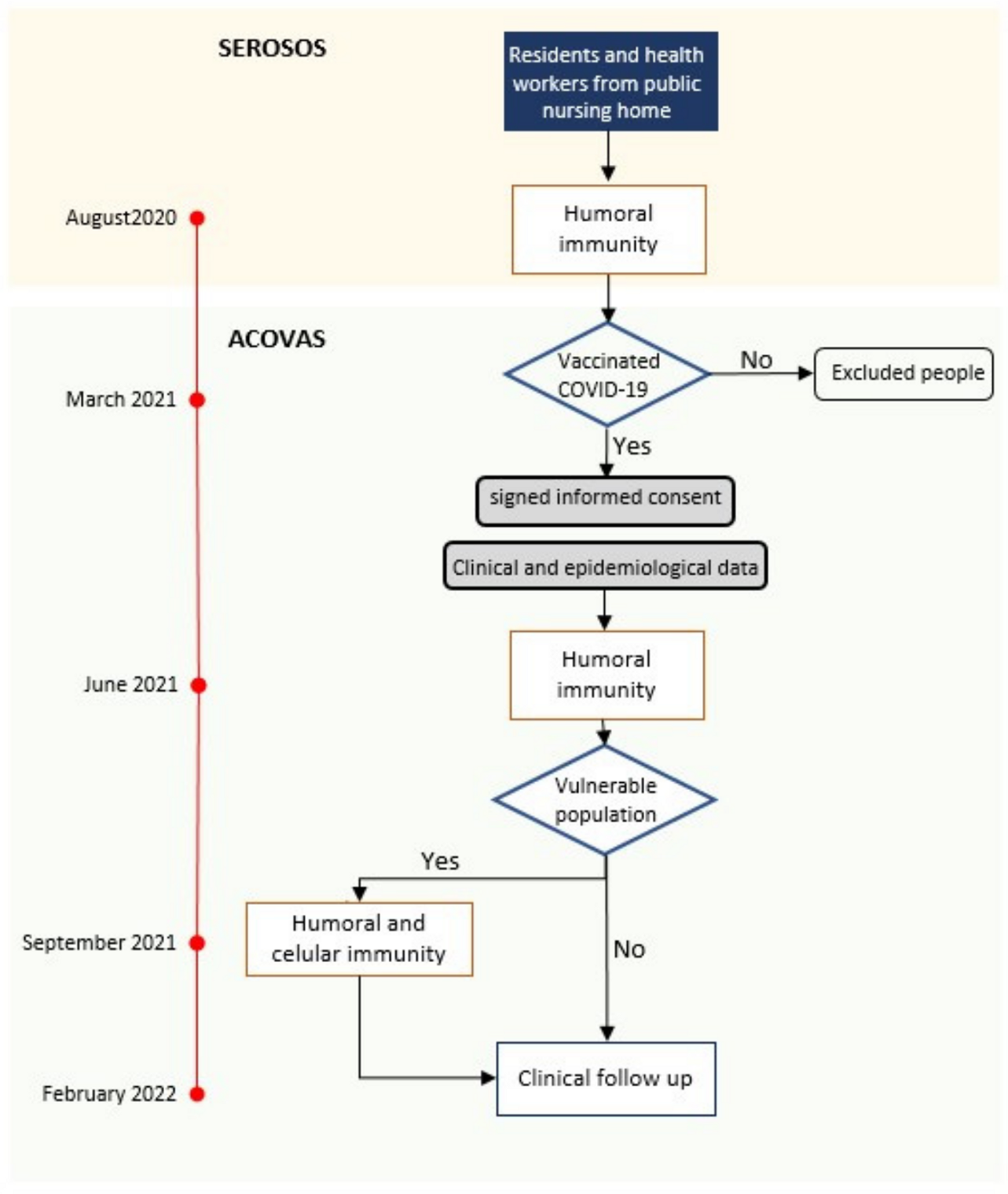
2.1. Study Design
2.2. Population
2.3. Laboratory Analysis
2.4. Statistical Analysis
3. Results
3.1. Clinical Parameters
3.2. Immunological Parameters

{kind=link}
| Residents (267) | Staff (302) | p | |||
| August 2020 | Concentration of anti-spike antibodies (mean [SD] AU/µL) | 1.5 [3.2] | 0.4 [1.8] | <0.01 | |
| Proportion of positive serologies (%) | 203 (76.0) | 106 (35.1 | <0.01 | ||
| June 2021 | Concentration of anti-spike IgG antibodies (mean [SD] AU/µL) | 15.7 [17.9] | 7.7 [12.7] | <0.01 | |
| Positive serologies (%) | 267 (100) | 301 (99.7) | 0.4 | ||
| September 2021 | Concentration of anti-spike IgG antibodies (mean [SD] AU/µL) | 9.4 [12.7] | 2.3 [9.4] | <0.01 | |
| Positive serologies (%) | 189 (100) | 58 (100) | 1 | ||
| Proportion of neutralizing antibodies (mean % [SD]) | 63.3 [34.1] | 17.7 [17.2] | <0.01 | ||
| Celullar immunity (IGRA positivity) | CD4+ (%) | 117 (62.2) | 24 (39.3) | <0.01 | |
| CD8+ (%) | 71 (37.8) | 7 (11.5) | <0.01 | ||
| CD4+/CD8+ (%) | 123 (65.4) | 24 (39.3) | <0.01 | ||
| History of COVID-19 | |||||||
|---|---|---|---|---|---|---|---|
| Residents | Staff | ||||||
| Yes | No | p | Yes | No | p | ||
| No. of participants | 206 | 59 | 122 | 164 | |||
| August 2020 | Concentration of anti-spike IgG antibodies (mean [SD] AU/µL) | 1.76 [3.48] | 0.69 [1.30] | <0.01 | 0.94 [2.68] | 0.07 [0.36] | <0.01 |
| Proportion of positive serologies (%) | 83.5 | 52.5 | <0.01 | 63.9 | 14.0 | <0.01 | |
| June 2021 | Concentration of anti-spike IgG antibodies (mean [SD] AU/µL) | 20.65 [25.23] | 8.83 [12.57] | <0.01 | 16.63 [22.32] | 3.13 [6.81] | <0.01 |
| Proportion of positive serologies (%) | 100 | 100 | 1 | 100 | 100 | 1 | |
| Elevation in the concentration of anti-spike IgG antibodies from August 2020 | 18.89 [23.79] | 8.14 [12.07] | <0.01 | 15.67 [21.21] | 3.06 [6.75] | <0.01 | |
3.3. The Omicron Epidemic
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Candel, F.J.; Barreiro, P.; San Román, J.; Carretero, M.d.M.; Sanz, J.C.; Pérez-Abeledo, M.; Ramos, B.; Viñuela-Prieto, J.M.; Canora, J.; Martínez-Peromingo, F.J.; et al. The demography and characteristics of SARS-CoV-2 seropositive residents and staff of nursing homes for older adults in the Community of Madrid: The SeroSOS study. Age Ageing 2021, 50, 1038–1047. [Google Scholar] [CrossRef]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; Fernández de Larrea, N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Moreno-Torres, V.; de la Fuente, S.; Mills, P.; Muñoz, A.; Muñez, E.; Ramos, A.; Fernández-Cruz, A.; Arias, A.; Pintos, I.; Vargas, J.A.; et al. Major determinants of death in patients hospitalized with COVID-19 during the first epidemic wave in Madrid, Spain. Medicine 2021, 100, e25634. [Google Scholar] [CrossRef]
- San Román, J.; Candel, F.J.; Carretero, M.d.M.; Sanz, J.C.; Pérez-Abeledo, M.; Barreiro, P.; Viñuela-Prieto, J.M.; Ramos, B.; Canora, J.; Barba, R.; et al. Cross-sectional analysis of risk factors for outbreak of COVID-19 in nursing homes for older adults in the Community of Madrid. Gerontology 2023, 69, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Menéndez Colino, R.; Merello de Miguel, A.; Argentina, F.; Barcons Marques, M.; Chaparro Jiménez, B.; López Hernández, P.; Jiménez Bueno, S.; Montero Vega, M.D.; García Rodríguez, J.; Ferrer Simo, B.; et al. Evolución de la COVID-19 en las residencias de personas mayores desde la según ola hasta la vacunación. Descripción de un programa de coordinación entre atención primaria, geriatría y salud pública. Rev. Esp. Salud Pública 2021, 95, e1–e11. [Google Scholar]
- Mateos-Nozal, J.; Galán Montemayor, J.C.; Lores Torres, S.; Barreiro, P.; Paños Zamora, A.; Martín Martínez, F.; García Castelo, D.; Rodríguez-Domínguez, M.; Martínez Peromingo, F.J.; Cruz-Jentoft, A.J. SARS-CoV-2 B1.1.7 Variant outbreak in a fully vaccinated nursing home—Madrid, June 2021. J. Am. Med. Dir. Assoc. 2021, 22, 2266–2268. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef] [PubMed]
- Mlcochova, P.; Kemp, S.A.; Dhar, M.S.; Papa, G.; Meng, B.; Ferreira, I.A.T.M.; Datir, R.; Collier, D.A.; Albecka, A.; Singh, S.; et al. SARS-CoV-2 B.1.617.2 Delta variant replication and immune evasion. Nature 2021, 599, 114–119. [Google Scholar] [CrossRef]
- Tian, D.; Sun, Y.; Xu, H.; Ye, Q. The emergence and epidemic characteristics of the highly mutated SARS-CoV-2 Omicron variant. J. Med. Virol. 2022, 94, 2376–2383. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. SARS-CoV-2 Variants of Concern as of 27 July 2023. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 26 July 2023).
- Nemet, I.; Kliker, L.; Lustig, Y.; Zuckerman, N.; Erster, O.; Cohen, C.; Kreiss, Y.; Alroy-Preis, S.; Regev-Yochay, G.; Mendelson, E.; et al. Third BNT162b2 Vaccination Neutralization of SARS-CoV-2 Omicron Infection. N. Engl. J. Med. 2022, 386, 492–494. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a Fourth Dose of Covid-19 mRNA Vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef]
- Suzuki, R.; Yamasoba, D.; Kimura, I.; Wang, L.; Kishimoto, M.; Ito, J.; Morioka, Y.; Nao, N.; Nasser, H.; Uriu, K.; et al. Attenuated fusogenicity and pathogenicity of SARS-CoV-2 Omicron variant. Nature 2022, 603, 700–705. [Google Scholar] [CrossRef]
- Shuai, H.; Chan, J.F.; Hu, B.; Chai, Y.; Yuen, T.T.; Yin, F.; Huang, X.; Yoon, C.; Hu, J.C.; Liu, H.; et al. Attenuated replication and pathogenicity of SARS-CoV-2 B.1.1.529 Omicron. Nature 2022, 603, 693–699. [Google Scholar] [CrossRef]
- Shao, J.; Fan, R.; Hu, J.; Zhang, T.; Lee, C.; Huang, X.; Wang, F.; Liang, H.; Jin, Y.; Jiang, Y.; et al. Clinical Progression and Outcome of Hospitalized Patients Infected with SARS-CoV-2 Omicron Variant in Shanghai, China. Vaccines 2022, 10, 1409. [Google Scholar] [CrossRef]
- Maslo, C.; Friedland, R.; Toubkin, M.; Laubscher, A.; Akaloo, T.; Kama, B. Characteristics and Outcomes of Hospitalized Patients in South Africa During the COVID-19 Omicron Wave Compared with Previous Waves. JAMA 2022, 327, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirseborn, F.; Toffa, S.; Rickeard, T.; Gallagher, E. COVID-19 vaccine effectiveness against the Omicron (B.1.1.529) variant. N. Engl. J. Med. 2022, 386, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Pajon, R.; Doria-Rose, N.A.; Shen, X.; Schmidt, S.D.; O’Dell, S.; McDanal, C.; Feng, W.; Tong, J.; Eaton, A.; Maglinao, M.; et al. SARS-CoV-2 Omicron Variant Neutralization after mRNA-1273 Booster Vaccination. N. Engl. J. Med. 2022, 386, 1088–1091. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Beltran, W.F.; St Denis, K.J.; Hoelzemer, A.; Lam, E.C.; Nitido, A.D.; Sheehan, M.L.; Berrios, C.; Ofoman, O.; Chang, C.C.; Hauser, B.M.; et al. mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell 2022, 185, 457–466. [Google Scholar] [CrossRef] [PubMed]
- UK Health Security Agency. SARS-CoV-2 Variants of Concern and Variants under Investigation in England Technical Briefing: Update on Hospitalization and Vaccine Effectiveness for Omicron VOC-21 NOV01 (B.1.1.529). Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1044481/Technical-Briefing-31-Dec-2021-Omicron_severity_update.pdf (accessed on 30 July 2023).
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef] [PubMed]
- Mateos-Nozal, J.; Pérez Panizo, N.; Zárate-Sáez, C.M.; Vaquero-Pinto, M.N.; Roldán-Plaza, C.; Mejía Ramírez-Arellano, M.V.; Sánchez García, E.; Garza-Martínez, A.J.; Cruz-Jentoft, A.J. Proactive geriatric comanagement of nursing home patients by a new hospital-based Liaison Geriatric Unit: A new model for the future. J. Am. Med. Dir. Assoc. 2022, 23, 308–310. [Google Scholar] [CrossRef]
- Wang, E.; Liu, A.; Wang, Z.; Shang, X.; Zhang, L.; Jin, Y.; Ma, Y.; Zhang, L.; Bai, T.; Song, J.; et al. The prognostic value of the Barthel Index for mortality in patients with COVID-19: A cross-sectional study. Front. Public Health 2023, 10, 978237. [Google Scholar] [CrossRef] [PubMed]
- Vinyoles, E.; Vila, J.; Argimon, J.M.; Espinàs, J.; Abos, T.; Limón, E. Concordance among Mini-Examen Cognoscitivo and Mini-Mental State Examination in cognitive impairment screening. Aten Primaria 2002, 30, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.; Shin, S.; Nam, M.; Hong, Y.J.; Roh, E.Y.; Park, K.U.; Song, E.Y. Performance evaluation of three automated quantitative immunoassays and their correlation with a surrogate virus neutralization test in coronavirus disease 19 patients and pre-pandemic controls. J. Clin. Lab. Anal. 2021, 35, e23921. [Google Scholar] [CrossRef] [PubMed]
- Barreiro, P.; Sanz, J.C.; San Román, J.; Pérez-Abeledo, M.; Carretero, M.; Megías, G.; Viñuela-Prieto, J.M.; Ramos, B.; Canora, J.; Martínez-Peromingo, F.J.; et al. A Pilot Study for the Evaluation of an Interferon Gamma Release Assay (IGRA) To Measure T-Cell Immune Responses after SARS-CoV-2 Infection or Vaccination in a Unique Cloistered Cohort. J. Clin. Microbiol. 2022, 60, e0219921. [Google Scholar] [CrossRef]
- Red de Vigilancia Epidemiológica. Informe Epidemiológico Semanal Comunidad de Madrid. Semana 32. 16 August 2023. Available online: https://www.comunidad.madrid/sites/default/files/doc/sanidad/epid/informe_epidemiologico_semanal.pdf (accessed on 18 August 2023).
- Kaufman, H.W.; Letovsky, S.; Meyer, W.A., 3rd; Gillim, L.; Assimon, M.M.; Kabelac, C.A.; Kroner, J.W.; Reynolds, S.L.; Eisenberg, M. SARS-CoV-2 spike-protein targeted serology test results and their association with subsequent COVID-19-related outcomes. Front. Public Health 2023, 11, 1193246. [Google Scholar] [CrossRef] [PubMed]
- Aalto, U.L.; Pitkälä, K.H.; Andersen-Ranberg, K.; Bonin-Guillaume, S.; Cruz-Jentoft, A.J.; Eriksdotter, M.; Gordon, A.L.; Gosch, M.; Holmerova, I.; Kautiainen, H.; et al. COVID-19 pandemic and mortality in nursing homes across USA and Europe up to October 2021. Eur. Geriatr. Med. 2022, 13, 705–709. [Google Scholar] [CrossRef]
- Hernandez-Suarez, C.; Murillo-Zamora, E. Waning immunity to SARS-CoV-2 following vaccination or infection. Front. Med. 2022, 9, 972083. [Google Scholar] [CrossRef]
- Blain, H.; Tuaillon, E.; Gamon, L.; Pisoni, A.; Miot, S.; Rolland, Y.; Picot, M.; Bousquet, J. Antibody response after one and two jabs of the BNT162b2 vaccine in nursing home residents: The CONsort-19 study. Allergy 2021, 77, 271–281. [Google Scholar] [CrossRef]
- Primorac, D.; Brlek, P.; Matišić, V.; Molnar, V.; Vrdoljak, K.; Zadro, R.; Parčina, M. Cellular Immunity-The Key to Long-Term Protection in Individuals Recovered from SARS-CoV-2 and after Vaccination. Vaccines 2022, 10, 442. [Google Scholar] [CrossRef]
- Van Praet, J.T.; Vandecasteele, S.; De Roo, A.; Vynck, M.; De Vriese, A.S.; Reynders, M. Dynamics of the cellular and humoral immune response after BNT162b2 messenger ribonucleic acid coronavirus disease2019 (COVID-19) vaccination in COVID-19 naïve nursing home residents. J. Infect. Dis. 2021, 224, 1690–1693. [Google Scholar]
- Achiron, A.; Gurevich, M.; Falb, R.; Dreyer-Alster, S.; Sonis, P.; Mandel, M. SARS-CoV-2 antibody dynamics and B-cell memory response over time in COVID-19 convalescent subjects. Clin. Microbiol. Infect. 2021, 27, 1349.e1–1349.e6. [Google Scholar] [CrossRef]
- IMSERSO. Actualización nº 101. Enfermedad por Coronavirus (COVID-19) en Centros Residenciales. 29 January 2023. Available online: https://imserso.es/documents/20123/117116/Inf_resid_20230129.pdf/a7dfa113-f148-a028-88ad-23fa85009e60 (accessed on 1 October 2023).
- Pierobon, S.; Braggion, M.; Fedeli, U.; Nordio, M.; Basso, C.; Zorzi, M. Impact of vaccination on the spread of SARS-CoV-2 infection in north-east Italy nursing homes. A propensity score and risk analysis. Age Ageing 2022, 51, afab224. [Google Scholar] [CrossRef]
- Zeng, C.; Evans, J.P.; King, T.; Zheng, Y.M.; Oltz, E.M.; Whelan, S.P.J.; Saif, L.J.; Peeples, M.E.; Liu, S.L. SARS-CoV-2 spreads through cell-to-cell transmission. Proc. Natl. Acad. Sci. USA 2022, 119, e2111400119. [Google Scholar] [CrossRef]
- Sekine, T.; Perez-Potti, A.; Rivera-Ballesteros, O.; Strålin, K.; Gorin, J.B.; Olsson, A.; Llewellyn-Lacey, S.; Kamal, H.; Bogdanovic, G.; Muschiol, S.; et al. Robust T Cell Immunity in Convalescent Individuals with Asymptomatic or Mild COVID-19. Cell 2020, 183, 158–168. [Google Scholar] [CrossRef]
- Koyama, T.; Miyakawa, K.; Tokumasu, R.; Jeremiah, S.S.; Kudo, M.; Ryo, A. Evasion of vaccine-induced humoral immunity by emerging sub-variants of SARS-CoV-2. Future Microbiol. 2022, 17, 417–424. [Google Scholar] [CrossRef]
- Dos Santos, L.A.; Adrielle Dos Santos, L.; Filho, P.G.G.; Silva, A.M.F.; Santos, J.V.G.; Santos, D.S.; Aquino, M.M.; de Jesus, R.M.; Almeida, M.L.D.; da Silva, J.S.; et al. Recurrent COVID-19 including evidence of reinfection and enhanced severity in thirty Brazilian healthcare workers. J. Infect. 2021, 82, 399–406. [Google Scholar] [CrossRef]
- Guo, L.; Zhang, Q.; Gu, X.; Ren, L.; Huang, T.; Li, Y.; Zhang, H.; Liu, Y.; Zhong, J.; Wang, X.; et al. Durability and cross-reactive immune memory to SARS-CoV-2 in individuals 2 years after recovery from COVID-19: A longitudinal cohort study. Lancet Microbe 2023, 5, e24–e33. [Google Scholar] [CrossRef] [PubMed]
- Candel, F.J.; Barreiro, P.; San Román, J.; Abanades, J.C.; Barba, R.; Barberán, J.; Bibiano, C.; Canora, J.; Cantón, R.; Calvo, C.; et al. Recommendations for use of antigenic tests in the diagnosis of acute SARS-CoV-2 infection in the second pandemic wave: Attitude in different clinical settings. Rev. Esp. Quimioter. 2020, 33, 466–484. [Google Scholar] [CrossRef] [PubMed]
- Chrysostomou, A.C.; Vrancken, B.; Haralambous, C.; Alexandrou, M.; Gregoriou, I.; Ioannides, M.; Ioannou, C.; Kalakouta, O.; Karagiannis, C.; Marcou, M.; et al. Unraveling the dynamics of Omicron (BA.1, BA.2, and BA.5) waves and emergence of the Deltacton variant: Genomic epidemiology of the SARS-CoV-2 epidemic in Cyprus (Oct 2021–Oct 2022). Viruses 2023, 15, 1933. [Google Scholar] [CrossRef] [PubMed]

| Residents | Staff | p | |
|---|---|---|---|
| No | 267 | 302 | |
| Age (mean [SD] years) | 87.6 [7.7] | 50.7 [10.3] | <0.01 |
| Females (%) | 217 (81.3) | 248 (82.1) | 0.6 |
| Low weight (%) | 65 (24.5) | 4 (1.4) | <0.01 |
| Obesity (%) | 68 (25.7) | 39 (13.9) | <0.01 |
| Hypertension (%) | 180 (67.7) | 55 (19.2) | <0.01 |
| Diabetes mellitus (%) | 64 (24.0) | 8 (2.8) | <0.01 |
| Dyslipidemia (%) | 69 (25.9) | 54 (18.9) | <0.05 |
| COPD (%) | 26 (9.8) | 10 (3.5) | <0.05 |
| Heart disease (%) | 121 (45.7) | 10 (3.5) | <0.01 |
| Active malignancy (%) | 18 (6.8) | 2 (0.7) | <0.01 |
| Immunodepression (%) | 8 (3.0) | 9 (3.1) | 0.9 |
| Barthel score (mean [SD] points) | 39.0 [40.0] | -- | -- |
| Lobo-MMT score (mean [SD] points) | 12.6 [10.9] | -- | -- |
| No of comorbidities (mean [SD]) | 3.0 [1.3] | 0.7 [0.9] | <0.01 |
| COVID-19 before June 2021 (%) | 206 (77.7) | 122 (42.7) | <0.01 |
| COVID-19 before September 2021 (%) | 206 (77.7) | 125 (43.0) | <0.01 |
| OR (95% CI), p | |
|---|---|
| Age (per year) | 1.00 (0.98–1.03), 0.7 |
| Sex (male vs. female) | 0.53 (0.25–1.12), 0.1 |
| History of COVID-19 | 1.35 (0.70–2.61), 0.4 |
| Concentration of anti-spike antibodies (per AU/mL) | 1.02 (0.99–1.06), 0.2 |
| Proportion of neutralizing anti-spike antibodies (per point) | 1.02 (1.01–1.03), <0.001 |
| All (%) | Residents (%) | Staff (%) | p | Vulnerable (%) | Not-Vulnerable (%) | p | |
|---|---|---|---|---|---|---|---|
| SARS-CoV-2 infection | 82 (14.4) | 32 (11.9) | 50 (16.6) | 0.1 | 32 (13.0) | 50 (15.5) | 0.4 |
| Any cause death | 37 (6.5) | 37 (13.9) | 0 (0) | <0.001 | 26 (10.5) | 11 (3.4) | 0.001 |
| SARS-CoV2 Infection | Any Cause Death | |||||
|---|---|---|---|---|---|---|
| Yes | No | p | Yes | No | p | |
| No. (%) | 32 (11.9) | 235 (88.1) | - | 37 (13.9) | 229 (86.1) | - |
| Females (%) | 28 (87.5) | 189 (80.4) | 0.3 | 26 (70.3) | 191 (83.0) | 0.06 |
| Low weight (%) | 6 (18.8) | 59 (25.3) | 0.4 | 16 (44.4) | 49 (21.4) | 0.003 |
| Obesity (%) | 6 (18.8) | 62 (26.6) | 0.3 | 6 (16.7) | 62 (27.1) | 0.2 |
| Hypertension (%) | 21 (65.6) | 159 (67.9) | 0.8 | 24 (64.9) | 156 (68.1) | 0.7 |
| Diabetes mellitus (%) | 12 (37.5) | 52 (22.1) | 0.06 | 7 (18.9) | 57 (24.8) | 0.4 |
| Dyslipidemia (%) | 12 (37.5) | 57 (24.4) | 0.1 | 6 (16.2) | 63 (27.5) | 0.1 |
| COPD (%) | 0 (0) | 26 (11.1) | 0.05 | 2 (5.4) | 24 (10.5) | 0.3 |
| Heart disease (%) | 7 (21.9) | 114 (48.9) | 0.004 | 19 (52.8) | 102 (44.5) | 0.4 |
| Active malignancy (%) | 2 (6.3) | 16 (6.9) | 0.9 | 6 (16.7) | 12 (5.2) | 0.01 |
| Immunodepression (%) | 0 (0) | 8 (3.4) | 0.3 | 0 (0.0) | 8 (3.5) | 0.3 |
| Barthel score (mean [SD] points) | 38.9 (32.1) | 39.0 (30.7) | 0.9 | 25.6 (27.6) | 41.1 (30.7) | 0.1 |
| Dementia (%) | 25 (78.1) | 162 (69.2) | 0.3 | 29 (80.6) | 158 (68.7) | 0.1 |
| Lobo-MMT score (mean [SD] points) | 9.2 (11.2) | 13.1 (10.8) | 0.1 | 9.8 (9.8) | 13.1 (11.0) | 0.2 |
| No. of comorbidities (mean [SD]) | 2.8 (1.2) | 3.1 (1.3) | 0.4 | 3.1 (1.3) | 3.0 (1.3) | 0.9 |
| COVID-19 before June 2021 (%) | 24 (75.0) | 182 (78.1) | 0.7 | 27 (75.0) | 179 (78.2) | 0.7 |
| COVID-19 before September 2021 (%) | 24 (75.0) | 182 (78.1) | 0.7 | 27 (75.0) | 179 (78.2) | 0. 7 |
| SARS-CoV2 Infection | Any Cause Death | |||||||
|---|---|---|---|---|---|---|---|---|
| Yes | No | p | Yes | No | p | |||
| No (%) | 32 (12) | 235 (88) | - | 37 (13.9) | 230 (86.1) | - | ||
| August 2020 | IgG anti-spike antibodies (mean [SD] AU/µL) | 1.9 [4.6] | 1.4 [2.9] | 0.4 | 1.5 [4.0] | 1.5 [3.0] | 0.5 | |
| Positive serologies (%) | 26 (81.3) | 177 (75.3) | 0.5 | 28 (75.7) | 175 (76.1) | 1 | ||
| June 2021 | IgG anti-spike antibodies (mean [SD] AU/µL) | 13.7 [16.7] | 16.0 [18.0] | 0.5 | 14.2 [19.2] | 18.5 [24.1] | 0.5 | |
| Positive serologies (%) | 32 (100) | 235 (100) | 1 | 37 (100) | 230 (100) | 1 | ||
| September 2021 | IgG anti-spike antibodies (mean [SD] AU/µL) | 8.4 [3.4] | 9.5 [12.7] | 0.7 | 7.1 [7.0] | 10.3 [16.2] | 0.5 | |
| Positive serologies (%) | 21 (100) | 168 (100) | 1 | 20 (100) | 169 (100) | 1 | ||
| Proportion ofneutralizing antibodies (mean % [SD]) | 62.4 [33.0] | 63.4 [34.3] | 0.9 | 63.7 [38.3] | 63.2 [33.7] | 0.9 | ||
| Cellular immunity (positivity): | CD4+ (%) | 14 (66.7) | 103 (61.7) | 0.7 | 13 (65.0) | 104 (61.9) | 0.8 | |
| CD8+ (%) | 9 (42.9) | 62 (37.1) | 0.6 | 3 (15.0) | 68 (40.5) | 0.03 | ||
| CD4+/CD8+ (%) | 14 (66.7) | 109 (65.3) | 0.9 | 13 (65.0) | 123 (65.4) | 1 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mateos-Nozal, J.; Rodríguez-Domínguez, M.; San Román, J.; Candel, F.J.; Villarrubia, N.; Pérez-Panizo, N.; Segura, E.; Cuñarro, J.M.; Ramírez-Arellano, M.V.M.; Rodríguez-Ramos, R.; et al. Factors Associated with SARS-CoV-2 Infection in Fully Vaccinated Nursing Home Residents and Workers. Viruses 2024, 16, 186. https://doi.org/10.3390/v16020186
Mateos-Nozal J, Rodríguez-Domínguez M, San Román J, Candel FJ, Villarrubia N, Pérez-Panizo N, Segura E, Cuñarro JM, Ramírez-Arellano MVM, Rodríguez-Ramos R, et al. Factors Associated with SARS-CoV-2 Infection in Fully Vaccinated Nursing Home Residents and Workers. Viruses. 2024; 16(2):186. https://doi.org/10.3390/v16020186
Chicago/Turabian StyleMateos-Nozal, Jesús, Mario Rodríguez-Domínguez, Jesús San Román, Francisco Javier Candel, Noelia Villarrubia, Nuria Pérez-Panizo, Esther Segura, Juan Manuel Cuñarro, Manuel V. Mejía Ramírez-Arellano, Rafael Rodríguez-Ramos, and et al. 2024. "Factors Associated with SARS-CoV-2 Infection in Fully Vaccinated Nursing Home Residents and Workers" Viruses 16, no. 2: 186. https://doi.org/10.3390/v16020186