
The Validity of the ROX Index and APACHE II in Predicting Early, Late, and Non-Responses to Non-Invasive Ventilation in Patients with COVID-19 in a Low-Resource Setting
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Settings for HFNO
2.2. Settings for NIV
2.3. Criteria for Failure of Response to HFNO [10]
- Oxygenation criteria: SpO2 < 88% for more than 6 h while receiving HFNO with a flow of 60 L/min and partial pressure of arterial oxygen/fraction of inspired oxygen (P/F) ratio < 100.
- Ventilation criteria: presence of respiratory acidosis with a pH < 7.25.
- Work of breathing criteria: tachypnoea with RR > 30 and the use of accessory muscles of respiration.
- Others: need for invasive mechanical ventilation due to hemodynamic instability despite fluid resuscitation (systolic blood pressure < 90 mm of Hg and/or mean arterial pressure less than 65 mm of Hg), altered sensorium (GCS < 12), need for airway protection, and dysrhythmias causing hemodynamic instability and cardiopulmonary arrest.
2.4. Criteria for Failure of Response to NIV [11]
- Oxygenation criteria: SpO2 < 88% for more than 6 h while receiving NIV with a P/F ratio < 100, and a minimum PEEP of 5 cm of water and minimum pressure support of 5 cm of water.
- Ventilation criteria: presence of respiratory acidosis with a pH < 7.25.
- Work of breathing criteria: tachypnoea with RR > 30 and the use of accessory muscles of respiration.
- Others: need for invasive mechanical ventilation due to hemodynamic instability despite fluid resuscitation (systolic blood pressure < 90 mm of Hg and/or mean arterial pressure less than 65 mm of Hg), altered sensorium (GCS < 9), need for airway protection, dysrhythmias causing hemodynamic instability, and cardiopulmonary arrest.
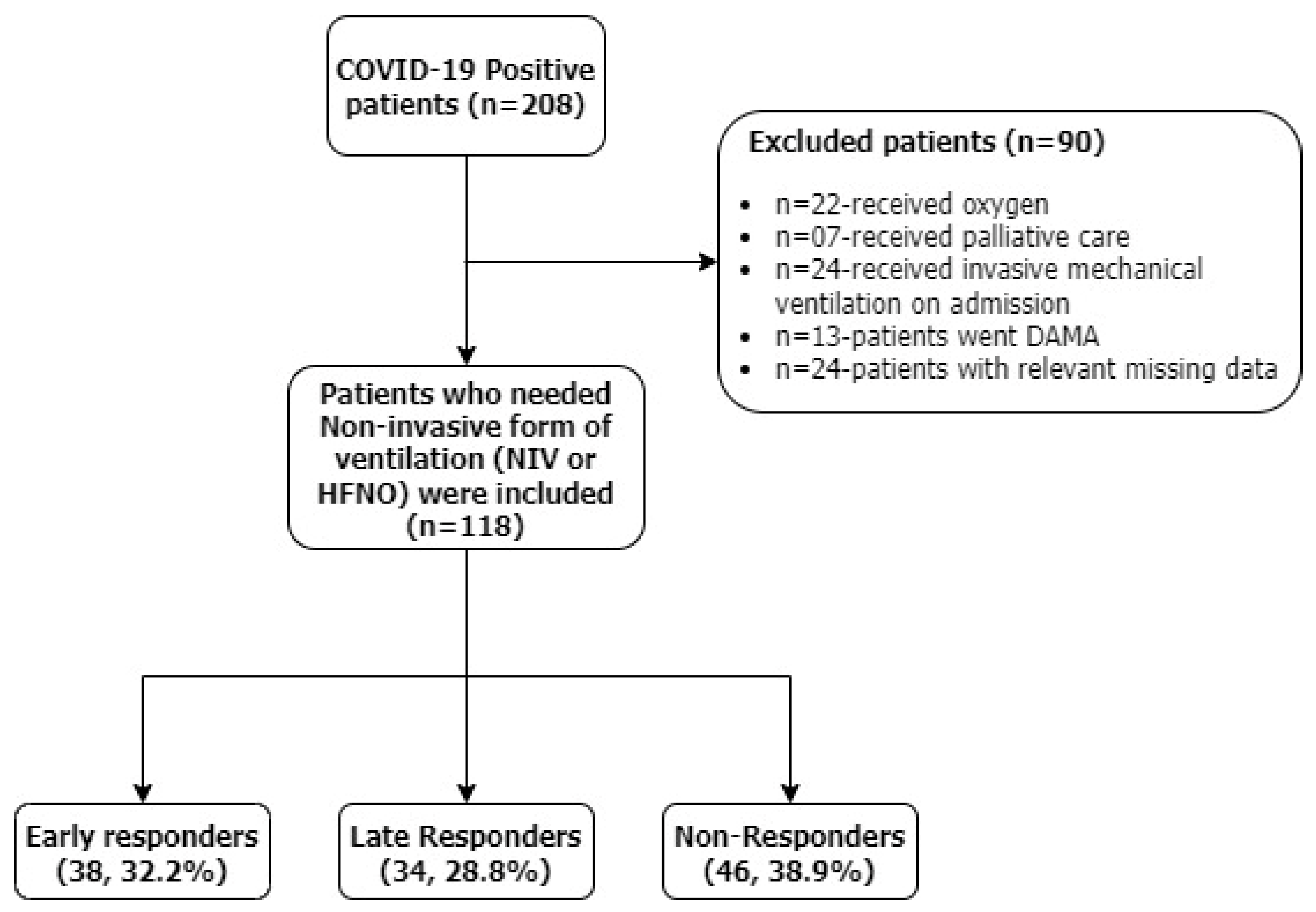
- Early responders—responded well within 5 days and weaned off HFNO/NIV, discharged after complete recovery.
- Late responders—response time more than 5 days and weaned off HFNO/NIV, shifted to general wards after completing ICU stay.
- Non-responders—patients who failed NIV and/or HFNO and required invasive mechanical ventilation at any time after hospital admission or patients who succumbed to illness.
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation/Acronym | Definition/Full-Form |
| AKI | Acute Kidney Injury |
| ALT | Alanine Aminotransferase |
| APACHE II | Acute Physiology and Chronic Health Evaluation |
| ARDS | Acute Respiratory Distress |
| AST | Aspartate Transaminase |
| AUC | Area Under the Curve |
| CI | Confidence Interval |
| COVID-19 | Coronavirus Disease 2019 |
| CPAP | Continuous Positive Airway Pressure |
| ECMO | Extracorporeal Membrane Oxygenation |
| HFNO | High-Flow Nasal Oxygenation |
| HR | Hazard Ratio |
| ICU | Intensive Care Unit |
| ISCCM | Indian Society of Critical Care Medicine |
| LMIC | Low- and Middle-Income Countries |
| MODS | Multi-Organ Dysfunction Syndrome |
| MOHFW | Ministry Of Health and Family Welfare |
| NIV | Non-Invasive Ventilation |
| NLR | Neutrophil-to-Lymphocyte Ratio |
| NPV | Negative Predictive Values |
| OR | Odds Ratio |
| PaO2 | Partial Pressure of Oxygen |
| PaO2/FiO2 | Ratio of Partial Pressure of Arterial Oxygen and Fraction of Inspired Oxygen |
| PCO2 | Partial Pressure of Carbon Dioxide |
| PH | Acidity/Alkalinity |
| PPV | Positive Predictive Values |
| ROC | Receiver Operating Characteristic |
| ROX | Ratio of Oxygen Saturation |
| RTPCR | Reverse Transcription Polymerase Chain Reaction |
| RR | Respiratory Rate |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| SEN | Sensitivity |
| SOFA | Sequential Organ Failure Assessment |
| SAPS | Simplified Acute Physiology Score |
| SPE | Specificity |
| SPO2/FIO2 | Ratio of Oxygen Saturation to The Fraction of Inspired Oxygen |
| WBC | White Blood Count |
References
- Haniffa, R.; Isaam, I.; De Silva, A.P.; Dondorp, A.M.; De Keizer, N.F. Performance of Critical Care Prognostic Scoring Systems in Low and Middle-Income Countries: A Systematic Review. Crit. Care 2018, 22, 18. [Google Scholar] [CrossRef] [PubMed]
- Siow, W.T.; Liew, M.F.; Shrestha, B.R.; Muchtar, F.; See, K.C. Managing COVID-19 in Resource-Limited Settings: Critical Care Considerations. Crit. Care 2020, 24, 167. [Google Scholar] [CrossRef] [PubMed]
- Gianstefani, A.; Farina, G.; Salvatore, V.; Alvau, F.; Artesiani, M.L.; Bonfatti, S.; Campinoti, F.; Caramella, I.; Ciordinik, M.; Lorusso, A.; et al. Role of ROX Index in the First Assessment of COVID-19 Patients in the Emergency Department. Intern. Emerg. Med. 2021, 16, 1959–1965. [Google Scholar] [CrossRef] [PubMed]
- Prower, E.; Grant, D.; Bisquera, A.; Breen, C.P.; Camporota, L.; Gavrilovski, M.; Pontin, M.; Douiri, A.; Glover, G.W. The ROX Index Has Greater Predictive Validity than NEWS2 for Deterioration in COVID-19. EClinicalMedicine 2021, 35, 100828. [Google Scholar] [CrossRef]
- Alberdi-Iglesias, A.; Martín-Rodríguez, F.; Ortega Rabbione, G.; Rubio-Babiano, A.I.; Núñez-Toste, M.G.; Sanz-García, A.; del Pozo Vegas, C.; Castro Villamor, M.A.; Martín-Conty, J.L.; Jorge-Soto, C.; et al. Role of SpO2/FiO2 Ratio and ROX Index in Predicting Early Invasive Mechanical Ventilation in COVID-19. A Pragmatic, Retrospective, Multi-Center Study. Biomedicines 2021, 9, 1036. [Google Scholar] [CrossRef] [PubMed]
- Privitera, D.; Capsoni, N.; Mazzone, A.; Airoldi, C.; Angaroni, L.; Pierotti, F.; Rocca, E.; Dal Molin, A.; Bellone, A. Nursing Evaluation during Treatment with Helmet Continuous Positive Airway Pressure in Patients with Respiratory Failure Due to COVID-19 Pneumonia: A Case Series. Aust. Crit. Care 2022, 35, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Privitera, D.; Angaroni, L.; Capsoni, N.; Forni, E.; Pierotti, F.; Vincenti, F.; Bellone, A. Flowchart for Non-Invasive Ventilation Support in COVID-19 Patients from a Northern Italy Emergency Department. Intern. Emerg. Med. 2020, 15, 767–771. [Google Scholar] [CrossRef]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M., Jr.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America; American Thoracic Society. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44 (Suppl. S2), S27–S72. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 27 October 2023).
- Management of Critical COVID-19 Advanced Non-Invasive Respiratory Support: High-Flow Nasal Oxygen and Non-Invasive Ventilation—Part 2. Available online: https://www.who.int/publications/m/item/management-of-critical-covid-19-advanced-non-invasive-respiratory-support--high-flow-nasal-oxygen-and-non-invasive-ventilation-part-2 (accessed on 27 October 2023).
- Irwin, R.S.; Lilly, C.M.; Mayo, P.H.; Rippe, J.M. Irwin and Rippe’s Intensive Care Medicine, 8th ed.; Wolters Kluwer Health: Waltham, MA, USA, 2017; ISBN 978-1-975102-22-7. [Google Scholar]
- Gallardo, A.; Zamarrón-López, E.; Deloya-Tomas, E.; Pérez-Nieto, O.R. Advantages and Limitations of the ROX Index. Pulmonology 2022, 28, 320–321. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.; Singh, A.; Khanna, P. ROX Index in COVID-19 Patients—Is It the Answer? Adv. Respir. Med. 2021, 89, 615–617. [Google Scholar] [CrossRef] [PubMed]
- Basoulis, D.; Avramopoulos, P.; Aggelara, M.; Karamanakos, G.; Voutsinas, P.-M.; Karapanou, A.; Psichogiou, M.; Samarkos, M.; Ntziora, F.; Sipsas, N.V. Validation of Sequential ROX-Index Score Beyond 12 Hours in Predicting Treatment Failure and Mortality in COVID-19 Patients Receiving Oxygen via High-Flow Nasal Cannula. Can. Respir. J. 2023, 2023, 7474564. [Google Scholar] [CrossRef]
- Leszek, A.; Wozniak, H.; Giudicelli-Bailly, A.; Suh, N.; Boroli, F.; Pugin, J.; Grosgurin, O.; Marti, C.; Le Terrier, C.; Quintard, H. Early Measurement of ROX Index in Intermediary Care Unit Is Associated with Mortality in Intubated COVID-19 Patients: A Retrospective Study. J. Clin. Med. 2022, 11, 365. [Google Scholar] [CrossRef]
- Blasi, F.; Ostermann, H.; Racketa, J.; Medina, J.; McBride, K.; Garau, J.; on behalf of the REACH study group. Early versus Later Response to Treatment in Patients with Community-Acquired Pneumonia: Analysis of the REACH Study. Respir. Res. 2014, 15, 6. [Google Scholar] [CrossRef]
- Fair Allocation of Intensive Care Unit Resources. Am. J. Respir. Crit. Care Med. 1997, 156, 1282–1301. [CrossRef]
- Rapsang, A.G.; Shyam, D.C. Scoring Systems in the Intensive Care Unit: A Compendium. Indian J. Crit. Care Med. Peer-Rev. Off. Publ. Indian Soc. Crit. Care Med. 2014, 18, 220. [Google Scholar] [CrossRef]
- Tian, Y.; Yao, Y.; Zhou, J.; Diao, X.; Chen, H.; Cai, K.; Ma, X.; Wang, S. Dynamic APACHE II Score to Predict the Outcome of Intensive Care Unit Patients. Front. Med. 2022, 8, 744907. [Google Scholar] [CrossRef]
- Parthasarathi, A.; Padukudru, S.; Arunachal, S.; Basavaraj, C.K.; Krishna, M.T.; Ganguly, K.; Upadhyay, S.; Anand, M.P. The Role of Neutrophil-to-Lymphocyte Ratio in Risk Stratification and Prognostication of COVID-19: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1233. [Google Scholar] [CrossRef] [PubMed]
- Blez, D.; Soulier, A.; Bonnet, F.; Gayat, E.; Garnier, M. Monitoring of High-Flow Nasal Cannula for SARS-CoV-2 Severe Pneumonia: Less Is More, Better Look at Respiratory Rate. Intensive Care Med. 2020, 46, 2094–2095. [Google Scholar] [CrossRef]
- Calligaro, G.L.; Lalla, U.; Audley, G.; Gina, P.; Miller, M.G.; Mendelson, M.; Dlamini, S.; Wasserman, S.; Meintjes, G.; Peter, J.; et al. The Utility of High-Flow Nasal Oxygen for Severe COVID-19 Pneumonia in a Resource-Constrained Setting: A Multi-Centre Prospective Observational Study. EClinicalMedicine 2020, 28, 100570. [Google Scholar] [CrossRef] [PubMed]
- Chandel, A.; Patolia, S.; Brown, A.W.; Collins, A.C.; Sahjwani, D.; Khangoora, V.; Cameron, P.C.; Desai, M.; Kasarabada, A.; Kilcullen, J.K.; et al. High-Flow Nasal Cannula Therapy in COVID-19: Using the ROX Index to Predict Success. Respir. Care 2021, 66, 909–919. [Google Scholar] [CrossRef]
- Panadero, C.; Abad-Fernández, A.; Rio-Ramirez, M.T.; Acosta Gutierrez, C.M.; Calderon-Alcala, M.; Lopez-Riolobos, C.; Matesanz-Lopez, C.; Garcia-Prieto, F.; Diaz-Garcia, J.M.; Raboso-Moreno, B.; et al. High-Flow Nasal Cannula for Acute Respiratory Distress Syndrome (ARDS) Due to COVID-19. Multidiscip. Respir. Med. 2020, 15, 693. [Google Scholar] [CrossRef]
- Colaianni-Alfonso, N.; Montiel, G.; Castro-Sayat, M.; Siroti, C.; Laura Vega, M.; Toledo, A.; Haedo, S.; Previgliano, I.; Mazzinari, G.; Miguel Alonso-Íñigo, J. Combined Noninvasive Respiratory Support Therapies to Treat COVID-19. Respir. Care 2021, 66, 1831–1839. [Google Scholar] [CrossRef]
- Prakash, J.; Bhattacharya, P.K.; Yadav, A.K.; Kumar, A.; Tudu, L.C.; Prasad, K. ROX Index as a Good Predictor of High Flow Nasal Cannula Failure in COVID-19 Patients with Acute Hypoxemic Respiratory Failure: A Systematic Review and Meta-Analysis. J. Crit. Care 2021, 66, 102–108. [Google Scholar] [CrossRef]
- Ahlström, B.; Frithiof, R.; Hultström, M.; Larsson, I.-M.; Strandberg, G.; Lipcsey, M. The Swedish COVID-19 Intensive Care Cohort: Risk Factors of ICU Admission and ICU Mortality. Acta Anaesthesiol. Scand. 2021, 65, 525–533. [Google Scholar] [CrossRef]
- Ayed, M.; Borahmah, A.A.; Yazdani, A.; Sultan, A.; Mossad, A.; Rawdhan, H. Assessment of Clinical Characteristics and Mortality-Associated Factors in COVID-19 Critical Cases in Kuwait. Med. Princ. Pract. 2021, 30, 185–192. [Google Scholar] [CrossRef]
- Patient Characteristics, Clinical Course and Factors Associated to ICU Mortality in Critically Ill Patients Infected with SARS-CoV-2 in Spain: A Prospective, Cohort, Multicentre Study|Elsevier Enhanced Reader. Available online: https://reader.elsevier.com/reader/sd/pii/S2341192920300986?token=20F68360940F50E715DBCF2544032E595793179C0C680F67036DBD34B57B22943A8F4A52FAEEBBF067D35D48BCB4F99E&originRegion=eu-west-1&originCreation=20230317052537 (accessed on 17 March 2023).
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated with Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Abate, S.M.; Ali, Y.; Mantedafro, B.; Basu, B. Prevalence and Risk Factors of Mortality among Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. Bull. World Health Organ. 2020. [Google Scholar] [CrossRef]
- Wendel Garcia, P.D.; Fumeaux, T.; Guerci, P.; Heuberger, D.M.; Montomoli, J.; Roche-Campo, F.; Schuepbach, R.A.; Hilty, M.P.; Alfaro Farias, M.; Margarit, A.; et al. Prognostic Factors Associated with Mortality Risk and Disease Progression in 639 Critically Ill Patients with COVID-19 in Europe: Initial Report of the International RISC-19-ICU Prospective Observational Cohort. EClinicalMedicine 2020, 25, 100449. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Early Responders (N = 38) | Late Responders (N = 34) | Non-Responders (N = 46) | p-Value | |
|---|---|---|---|---|
| Age (years) | 59.0 (45.0–67.0) | 58.0 (50.9–66.2) | 62.0 (52.0–70.1) | 0.17 * |
| Male % | 27 (71.1) | 29 (85.3) | 37 (80.4) | 0.32 † |
| Female % | 11 (28.9) | 5 (14.7) | 9 (19.6%) | |
| Duration of ICU stay (days) | 7.5 (6.0–9.0) | 10.0 (8.0–11.6) | 10.0 (8.7–16.0) | 0.01 * |
| Mode of Intervention | 22 (57.9) | 17 (50.0) | 33 (71.1) | 0.13 † |
| Vitals | ||||
| Heart Rate (beats/minute) | 108.0 (94.3–116.0) | 100.0 (97.0–117.3) | 98.0 (88.2–112.0) | 0.28 * |
| Respiratory Rate | 28.0 (26.0–31.7) | 32.0 (28.0–40.0) | 34.0 (28.0–39.0) | 0.01 * |
| Systolic blood pressure | 130.0 (120.0–140.0) | 140.0 (120.0–150.0) | 140.0 (130.0–148.3) | 0.22 * |
| Diastolic blood pressure | 70.0 (70.0–80.0) | 80.0 (70.0–80.0) | 80.0 (70.0–88.3) | 0.24 * |
| PH | 7.5 (7.4–7.5) | 7.4 (7.4–7.4) | 7.4 (7.4–7.5) | 0.10 * |
| PCO2 | 30.7 (28.9–34.2) | 33.8 (27.4–37.4) | 30.6 (28.2–34.6) | 0.87 * |
| PaO2 | 78.3 (63.7–89.8) | 65.1 (54.0–96.1) | 72.7 (57.8–83.9) | 0.22 * |
| P/F ratio | 156.6 (122.8–193.6) | 98.0 (77.8–169.3) | 104.6 (73.0–144.9) | <0.01* |
| Hematological investigations | ||||
| Hemoglobin (g/dL) | 13.5 (11.7–14.6) | 13.8 (12.8–14.6) | 13.3 (11.6–13.9) | 0.42 * |
| WBC count (X1000 cells/cu. mm) | 7290.0 (4826.7–9595.0) | 8980.0 (7405.0–10,853.3) | 11,590.0 (8038.3–13,136.7) | <0.01 * |
| Absolute Neutrophil count | 6699.6 (4204.8–9742.7) | 8037.8 (6422.6–9611.6) | 10,167.2 (7067.1–11,928.4) | 0.01 * |
| Absolute Lymphocyte count | 800.9 (588.4–1208.3) | 930.0 (572.1–1182.0) | 745.0 (574.9–1111.3) | 0.42 * |
| Platelet count | 2.2 (1.9–2.9) | 2.2 (1.7–2.8) | 2.6 (1.7–3.2) | 0.71 * |
| Procalcitonin | 0.3 (0.1–0.7) | 0.2 (0.1–0.4) | 0.7 (0.2–1.7) | 0.03 * |
| C-Reactive Peptide | 108.1 (52.5–172.3) | 89.0 (41.0–203.0) | 88.8 (41.3–168.7) | 0.49 * |
| Serum Albumin | 3.3(2.9–3.6) | 3.3 (3.1–3.5) | 3.3 (3.1–3.6) | 0.72 * |
| Serum AST | 32.0 (26.0–45.8) | 33.0 (24.2–53.8) | 59.0 (43.3–81.3) | <0.01 * |
| Serum ALT | 28.0 (21.0–36.8) | 30.0 (22.2–57.7) | 41.0 (23.0–63.5) | 0.13 * |
| Urea | 28.0 (20.2–37.8) | 38.0 (31.0–49.0) | 40.0 (31.3–62.8) | <0.01 * |
| Creatinine | 0.8 (0.7–1.0) | 0.9 (0.7–0.9) | 1.1 (0.8–1.4) | 0.01 * |
| Blood Urea Nitrogen | 13.1 (9.4–17.7) | 17.7 (14.5–22.9) | 18.7 (14.6–29.3) | <0.01 * |
| Sodium | 135.0 (132.0–138.0) | 135.0 (131.2–138.8) | 135.0 (131.0–139.0) | 0.63 * |
| Potassium | 4.4 (4.0–4.9) | 4.3 (3.7–4.4) | 4.4 (4.0–4.8) | 0.79 * |
| Comorbidities | ||||
| Diabetes Mellitus | 23 (60.5) | 21 (61.8) | 23 (50.0) | 0.49 † |
| Hypertension | 20 (52.6) | 20 (58.8) | 25 (54.3) | 0.86 † |
| Chronic Cardiac disease | 4 (10.5) | 3 (8.8) | 12 (26.1) | 0.06 † |
| Chronic Kidney disease | 4 (10.5) | 3 (8.8) | 2 (4.3) | 0.54 † |
| Chronic respiratory disease | 1 (2.6) | 2 (5.9) | 3 (6.5) | 0.70 † |
| Complications | ||||
| Sepsis | 2 (5.3) | 2 (5.9) | 23 (50.0) | <0.01 † |
| MODS | 3 (7.9) | 6 (17.6) | 31 (67.4) | <0.01 † |
| Acute Kidney Injury | 2 (5.3) | 7 (20.6) | 23 (50.0) | <0.01 † |
| Intubation | 0 (0) | 0 (0) | 46 (100) | <0.01 † |
| Mortality | 0 (0) | 0 (0) | 37 (80) | <0.01 † |
| Scores | ||||
| APACHE II | 9.0 (5.4–11.6) | 11.0 (8.4–14.6) | 15.0 (10.0–18.3) | <0.01 * |
| ROX on admission | 6.4 (5.5–7.7) | 4.3 (3.5–5.8) | 4.1 (3.7–5.0) | <0.01 * |
| ROX on day 2 | 7.4 (5.3–9.2) | 4.9 (4.1–5.8) | 4.4 (3.6–5.7) | <0.01 * |
| ROX on day 3 | 7.8 (6.2–9.9) | 5.6 (4.2–7.1) | 4.2 (3.3–5.8) | <0.01 * |
| Predictor | Estimate | SE | Z | p | Odds Ratio | 95% Confidence Interval | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Late vs. Early | Intercept | 4.07379 | 2.0088 | 2.028 | 0.043 | 58.779 | 1.1463 | 3013.9 |
| Age | −0.00743 | 0.0301 | −0.247 | 0.805 | 0.993 | 0.9357 | 1.053 | |
| Sex: Female–Male | −1.35952 | 0.9257 | −1.469 | 0.142 | 0.257 | 0.0418 | 1.576 | |
| Mode of Intervention | −0.09002 | 0.7008 | −0.128 | 0.898 | 0.914 | 0.2314 | 3.609 | |
| ROX on admission | −0.75948 | 0.2373 | −3.2 | 0.001 | 0.468 | 0.2939 | 0.745 | |
| ROX on day 2 | −0.512 | 0.191 | −2.67 | 0.008 | 0.599 | 0.412 | 0.872 | |
| ROX on day 3 | −0.594 | 0.221 | −2.69 | 0.007 | 0.552 | 0.358 | 0.851 | |
| APACHE II | 0.08962 | 0.0899 | 0.997 | 0.319 | 1.094 | 0.9171 | 1.304 | |
| Sepsis | 0.0719 | 1.109 | 0.0648 | 0.948 | 1.075 | 0.1222 | 9.452 | |
| MODS | −0.3049 | 1.167 | −0.261 | 0.794 | 0.737 | 0.0749 | 7.258 | |
| Acute Kidney Injury | 1.7603 | 1.197 | 1.471 | 0.141 | 5.814 | 0.5569 | 60.70 | |
| Diabetes Mellitus | −0.00741 | 0.532 | −0.0139 | 0.989 | 0.993 | 0.3496 | 2.82 | |
| Hypertension | 0.30225 | 0.531 | 0.5691 | 0.569 | 1.353 | 0.4777 | 3.83 | |
| Chronic Cardiac disease | −0.22465 | 0.829 | −0.271 | 0.786 | 0.799 | 0.1574 | 4.05 | |
| Chronic Kidney disease | −0.22582 | 0.836 | −0.270 | 0.787 | 0.798 | 0.155 | 4.11 | |
| Chronic respiratory disease | 0.79948 | 1.258 | 0.6355 | 0.525 | 2.224 | 0.189 | 26.18 | |
| Non- vs. Early | Intercept | 2.26483 | 2.1752 | 1.041 | 0.298 | 9.629 | 0.1355 | 684.11 |
| Age | 0.01381 | 0.0328 | 0.422 | 0.673 | 1.014 | 0.9508 | 1.081 | |
| Sex: Female–Male | −1.96438 | 1.0491 | −1.872 | 0.061 | 0.14 | 0.0179 | 1.096 | |
| Mode of Intervention | 0.71202 | 0.7939 | 0.897 | 0.37 | 2.038 | 0.43 | 9.661 | |
| ROX on admission | −0.94045 | 0.2701 | −3.482 | <0.001 | 0.39 | 0.23 | 0.663 | |
| ROX on day 2 | −0.751 | 0.222 | −3.39 | <0.001 | 0.472 | 0.306 | 0.729 | |
| ROX on day 3 | −0.69 | 0.251 | −2.75 | 0.006 | 0.502 | 0.307 | 0.82 | |
| APACHE II | 0.195 | 0.0498 | 3.92 | <0.001 | 1.216 | 1.1024 | 1.34 | |
| Sepsis | 2.1241 | 0.914 | 2.3248 | 0.02 | 8.365 | 1.3956 | 50.14 | |
| MODS | 1.3667 | 1.009 | 1.3543 | 0.176 | 3.922 | 0.5427 | 28.35 | |
| Acute Kidney Injury | 1.7162 | 1.113 | 1.5421 | 0.123 | 5.563 | 0.6281 | 49.28 | |
| Diabetes Mellitus | −0.62774 | 0.51 | −1.2319 | 0.218 | 0.534 | 0.1966 | 1.45 | |
| Hypertension | 0.27071 | 0.51 | 0.5311 | 0.595 | 1.311 | 0.4827 | 3.56 | |
| Chronic Cardiac disease | 1.34248 | 0.672 | 1.997 | 0.046 | 3.829 | 1.0252 | 14.3 | |
| Chronic Kidney disease | −1.22034 | 0.956 | −1.2765 | 0.202 | 0.295 | 0.0453 | 1.92 | |
| Chronic respiratory disease | 0.73604 | 1.206 | 0.6101 | 0.542 | 2.088 | 0.1962 | 22.21 | |
| Cut Point | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | AUC | |
|---|---|---|---|---|---|---|
| APACHE II on admission | 14 | 84.62% | 68.35% | 56.90% | 90% | 0.847 |
| ROX on admission | 5.2 | 79.49% | 74.68% | 60.78% | 88.06% | 0.843 |
| ROX on day 2 | 5.8 | 89.66% | 67.31% | 60.47% | 92.11% | 0.836 |
| ROX on day 3 | 5.3 | 75.76% | 73.53% | 58.14% | 86.21% | 0.798 |
| Cut Point | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Youden’s Index | AUC | |
|---|---|---|---|---|---|---|---|
| APACHE II on admission | 14 | 65.28% | 76.09% | 81.03% | 58.33% | 0.414 | 0.751 |
| ROX on admission | 4 | 73.21% | 72% | 85.42% | 54.55% | 0.452 | 0.759 |
| ROX on day 2 | 4.6 | 61.11% | 73.91% | 78.57% | 54.84% | 0.35 | 0.734 |
| ROX on day 3 | 5.3 | 74.60% | 65.79% | 78.33% | 60.98% | 0.404 | 0.745 |
| HR (Univariable) | HR (Multivariable) | |
|---|---|---|
| Age | 1.02 (0.99–1.05) | 0.95 (0.84–1.06) |
| Sex (ref: Male) | 0.55 (0.22–1.38) | 0.28 (0.02–2.67) |
| ROX on admission | 0.45 (0.32–0.60) *** | 0.29 (0.13–0.52) *** |
| ROX on day 2 | 0.66 (0.47–0.92) * | 0.55 (0.34–0.89) * |
| ROX on day 3 | 0.85 (0.61–0.92) * | 0.83 (0.68–1.02) |
| APACHE II on admission | 1.11 (1.03–1.19) ** | 1.12 (1.03–1.21) * |
| Hypertension | 1.01 (1.00–1.03) | 1.01 (0.98–1.04) |
| Chronic Cardiac disease | 1.03 (1.01–1.06) ** | 1.09 (1.02–1.21) * |
| Chronic Kidney disease | 1.16 (0.93–1.64) | 1.83 (0.75–43.16) |
| Chronic respiratory disease | 1.14 (0.51–2.48) | 0.90 (0.13–6.16) |
| Complications | ||
| Sepsis | 8.56 (2.35–55.26) ** | 5.87 (1.27–45.18,) * |
| MODS | 10.57 (3.44–46.37) *** | 7.89 (2.12–40.58) ** |
| Acute Kidney Injury | 6.96 (2.25–30.63) ** | 5.80 (1.63–28.22) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arunachala, S.; Parthasarathi, A.; Basavaraj, C.K.; Kaleem Ullah, M.; Chandran, S.; Venkataraman, H.; Vishwanath, P.; Ganguly, K.; Upadhyay, S.; Mahesh, P.A. The Validity of the ROX Index and APACHE II in Predicting Early, Late, and Non-Responses to Non-Invasive Ventilation in Patients with COVID-19 in a Low-Resource Setting. Viruses 2023, 15, 2231. https://doi.org/10.3390/v15112231
Arunachala S, Parthasarathi A, Basavaraj CK, Kaleem Ullah M, Chandran S, Venkataraman H, Vishwanath P, Ganguly K, Upadhyay S, Mahesh PA. The Validity of the ROX Index and APACHE II in Predicting Early, Late, and Non-Responses to Non-Invasive Ventilation in Patients with COVID-19 in a Low-Resource Setting. Viruses. 2023; 15(11):2231. https://doi.org/10.3390/v15112231
Chicago/Turabian StyleArunachala, Sumalatha, Ashwaghosha Parthasarathi, Chetak Kadabasal Basavaraj, Mohammed Kaleem Ullah, Shreya Chandran, Hariharan Venkataraman, Prashant Vishwanath, Koustav Ganguly, Swapna Upadhyay, and Padukudru Anand Mahesh. 2023. "The Validity of the ROX Index and APACHE II in Predicting Early, Late, and Non-Responses to Non-Invasive Ventilation in Patients with COVID-19 in a Low-Resource Setting" Viruses 15, no. 11: 2231. https://doi.org/10.3390/v15112231