
Predictors of SARS-CoV-2 Infection and Severe and Lethal COVID-19 after Three Years of Follow-Up: A Population-Wide Study
 , ,
, ,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
- -
- Demographic data (Italian “Anagrafica”), which contained all death records;
- -
- SARS-CoV-2 laboratory or pharmacy tests, containing the information on all positive nasopharyngeal swabs detected through RT-PCR by the regional accredited laboratories (throughout the follow-up) or through rapid antigen test by local pharmacies (since January 2021), from the start of the pandemic;
- -
- COVID-19 vaccinations (from 1 January 2021, the start of the vaccination campaign, to 31 December 2022);
- -
- COVID-19 database, which includes all data on officially recorded COVID-19 cases, hospitalized or not;
- -
- Co-pay exemption dataset (Italian “Esenzioni Ticket”);
- -
- Administrative discharge abstracts of the last ten years.
- (a)
- SARS-CoV-2 infection—asymptomatic infection or mild disease, defined as fever or malaise plus at least one of the followings: sore throat, muscle pain, shortness of breath, dry cough, headache, conjunctivitis and diarrhea [21], with no hospital admission;
- (b)
- Severe COVID-19 disease—virologically confirmed COVID-19 syndrome, diagnosed by a specialist physician and requiring hospital admission;
- (c)
- COVID-19-related death—severe COVID-19 disease causing death within 60 days [22].
3. Results
3.1. Predictors of SARS-CoV-2 Infection
3.2. Predictors of Severe COVID-19 and COVID-19-Related Death
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Reyna-Villasmil, E.; Caponcello, M.G.; Maldonado, N.; Olivares, P.; Caroccia, N.; Bonazzetti, C.; Tazza, B.; Carrara, E.; Giannella, M.; Tacconelli, E.; et al. Association of Patients’ Epidemiological Characteristics and Comorbidities with Severity and Related Mortality Risk of SARS-CoV-2 Infection: Results of an Umbrella Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 2437. [Google Scholar] [CrossRef] [PubMed]
- Bravi, F.; Flacco, M.E.; Carradori, T.; Volta, C.A.; Cosenza, G.; De Togni, A.; Acuti Martellucci, C.; Parruti, G.; Mantovani, L.; Manzoli, L. Predictors of severe or lethal COVID-19, including Angiotensin Converting Enzyme inhibitors and Angiotensin II Receptor Blockers, in a sample of infected Italian citizens. PLoS ONE 2020, 15, e0235248. [Google Scholar] [CrossRef] [PubMed]
- Corrao, G.; Franchi, M.; Cereda, D.; Bortolan, F.; Leoni, O.; Jara, J.; Valenti, G.; Pavesi, G. Factors associated with severe or fatal clinical manifestations of SARS-CoV-2 infection after receiving the third dose of vaccine. J. Intern. Med. 2022, 292, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Moscatt, V.; Marino, A.; Pampaloni, A.; Scuderi, D.; Ceccarelli, M.; Benanti, F.; Gussio, M.; Larocca, L.; Boscia, V.; et al. Clinical characteristics and predictors of death among hospitalized patients infected with SARS-CoV-2 in Sicily, Italy: A retrospective observational study. Biomed. Rep. 2022, 16, 34. [Google Scholar] [CrossRef] [PubMed]
- Monari, C.; Pisaturo, M.; Maggi, P.; Macera, M.; Di Caprio, G.; Pisapia, R.; Gentile, V.; Fordellone, M.; Chiodini, P.; Coppola, N. Early predictors of clinical deterioration in a cohort of outpatients with COVID-19 in southern Italy: A multicenter observational study. J. Med. Virol. 2022, 94, 5336–5344. [Google Scholar] [CrossRef]
- Izcovich, A.; Ragusa, M.A.; Tortosa, F.; Lavena Marzio, M.A.; Agnoletti, C.; Bengolea, A.; Ceirano, A.; Espinosa, F.; Saavedra, E.; Sanguine, V.; et al. Prognostic factors for severity and mortality in patients infected with COVID-19: A systematic review. PLoS ONE 2020, 15, e0241955. [Google Scholar] [CrossRef]
- Min, K.; Cheng, Z.; Liu, J.; Fang, Y.; Wang, W.; Yang, Y.; Geldsetzer, P.; Barnighausen, T.; Yang, J.; Liu, D.; et al. Early-stage predictors of deterioration among 3145 nonsevere SARS-CoV-2-infected people community-isolated in Wuhan, China: A combination of machine learning algorithms and competing risk survival analyses. J. Evid. Based Med. 2023, 16, 166–177. [Google Scholar] [CrossRef]
- Italian Institute of Health. Characteristics of COVID-19 Patients Dying in Italy Report Based on Available Data on 10 January 2022. Available online: https://www.epicentro.iss.it/en/coronavirus/sars-cov-2-analysis-of-deaths-10-2-2022 (accessed on 5 July 2023).
- DeSantis, S.M.; Yaseen, A.; Hao, T.; Leon-Novelo, L.; Talebi, Y.; Valerio-Shewmaker, M.A.; Pinzon Gomez, C.L.; Messiah, S.E.; Kohl, H.W.; Kelder, S.H.; et al. Incidence and Predictors of Breakthrough and Severe Breakthrough Infections of SARS-CoV-2 After Primary Series Vaccination in Adults: A Population-Based Survey of 22 575 Participants. J. Infect. Dis. 2023, 227, 1164–1172. [Google Scholar] [CrossRef]
- Grima, P.; Guido, M.; Zizza, A. Clinical characteristics and risk factors associated with COVID-19 mortality in a non-Intensive Care Unit. J. Prev. Med. Hyg. 2023, 64, E3–E8. [Google Scholar] [CrossRef]
- Vardavas, C.I.; Mathioudakis, A.G.; Nikitara, K.; Stamatelopoulos, K.; Georgiopoulos, G.; Phalkey, R.; Leonardi-Bee, J.; Fernandez, E.; Carnicer-Pont, D.; Vestbo, J.; et al. Prognostic factors for mortality, intensive care unit and hospital admission due to SARS-CoV-2: A systematic review and meta-analysis of cohort studies in Europe. Eur. Respir. Rev. 2022, 31, 220098. [Google Scholar] [CrossRef] [PubMed]
- Acuti Martellucci, C.; Flacco, M.E.; Soldato, G.; Di Martino, G.; Carota, R.; Caponetti, A.; Manzoli, L. Effectiveness of COVID-19 Vaccines in the General Population of an Italian Region before and during the Omicron Wave. Vaccines 2022, 10, 662. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Cho, K.; Song, J.; Rahmati, M.; Koyanagi, A.; Lee, S.W.; Yon, D.K.; Il Shin, J.; Smith, L. The case fatality rate of COVID-19 during the Delta and the Omicron epidemic phase: A meta-analysis. J. Med. Virol. 2023, 95, e28522. [Google Scholar] [CrossRef] [PubMed]
- Flacco, M.E.; Acuti Martellucci, C.; Soldato, G.; Carota, R.; Fazii, P.; Caponetti, A.; Manzoli, L. Rate of reinfections after SARS-CoV-2 primary infection in the population of an Italian province: A cohort study. J. Public Health 2021, 44, e475–e478. [Google Scholar] [CrossRef] [PubMed]
- Flacco, M.E.; Soldato, G.; Acuti Martellucci, C.; Di Martino, G.; Carota, R.; Caponetti, A.; Manzoli, L. Risk of SARS-CoV-2 Reinfection 18 Months After Primary Infection: Population-Level Observational Study. Front. Public Health 2022, 10, 884121. [Google Scholar] [CrossRef]
- Flacco, M.E.; Martellucci, C.A.; Soldato, G.; Di Martino, G.; Carota, R.; De Benedictis, M.; Di Marco, G.; Parruti, G.; Di Luzio, R.; Caponetti, A.; et al. COVID-19 Vaccination Did Not Increase the Risk of Potentially Related Serious Adverse Events: 18-Month Cohort Study in an Italian Province. Vaccines 2022, 11, 31. [Google Scholar] [CrossRef]
- Flacco, M.E.; Soldato, G.; Acuti Martellucci, C.; Carota, R.; Di Luzio, R.; Caponetti, A.; Manzoli, L. Interim Estimates of COVID-19 Vaccine Effectiveness in a Mass Vaccination Setting: Data from an Italian Province. Vaccines 2021, 9, 628. [Google Scholar] [CrossRef]
- Riccardo, F.; Andrianou, X.; Bella, A.; Del Manso, M.; Urdiales, A.M.; Fabiani, M.; Bellino, S.; Boros, S.; D’Ancona, F.; Rota, M.C.; et al. COVID-19 Integrated Surveillance System. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-sorveglianza (accessed on 7 January 2022).
- Cascella, M.; Rajnik, M.; Cuomo, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation and Treatment Coronavirus (COVID-19). In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- UK Health Security Agency. UKHSA Reporting of COVID-19 Deaths: Technical Summary—1 February 2022; GOV-11236; UK Health Security Agency: London, UK, 2022. [Google Scholar]
- Rosenberg, E.S.; Dorabawila, V.; Easton, D.; Bauer, U.E.; Kumar, J.; Hoen, R.; Hoefer, D.; Wu, M.; Lutterloh, E.; Conroy, M.B.; et al. Covid-19 Vaccine Effectiveness in New York State. N. Engl. J. Med. 2021, 386, 116–127. [Google Scholar] [CrossRef]
- Italian Government. Raccomandazioni Ad Interim Sui Gruppi Target Della Vaccinazione Anti SARS-CoV-2/COVID-19. Available online: https://www.gazzettaufficiale.it/do/gazzetta/serie_generale/3/pdfPaginato?dataPubblicazioneGazzetta=20210324&numeroGazzetta=72&tipoSerie=SG&tipoSupplemento=GU&numeroSupplemento=0&progressivo=0&numPagina=1&edizione=0&rangeAnni= (accessed on 3 July 2023).
- Rosso, A.; Flacco, M.E.; Soldato, G.; Di Martino, G.; Acuti Martellucci, C.; Carota, R.; De Benedictis, M.; Di Marco, G.; Di Luzio, R.; Fiore, M.; et al. Effectiveness of COVID-19 Vaccines in the General Population of an Italian Province: Two years of follow-up. Vaccines 2023, 10, 662. [Google Scholar]
- Sharma, J.; Rajput, R.; Bhatia, M.; Arora, P.; Sood, V. Clinical Predictors of COVID-19 Severity and Mortality: A Perspective. Front. Cell Infect. Microbiol. 2021, 11, 674277. [Google Scholar] [CrossRef]
- Starke, K.R.; Reissig, D.; Petereit-Haack, G.; Schmauder, S.; Nienhaus, A.; Seidler, A. The isolated effect of age on the risk of COVID-19 severe outcomes: A systematic review with meta-analysis. BMJ Glob. Health 2021, 6, e006434. [Google Scholar] [CrossRef] [PubMed]
- Michels, E.H.; Appelman, B.; de Brabander, J.; van Amstel, R.B.; Chouchane, O.; van Linge, C.C.A.; Schuurman, A.R.; Reijnders, T.D.; Sulzer, T.A.; Klarenbeek, A.M.; et al. Age-related changes in plasma biomarkers and their association with mortality in COVID-19. Eur. Respir. J. 2023, 62, 2300011. [Google Scholar] [CrossRef] [PubMed]
- Veiga, V.C.; Cavalcanti, A.B. Age, host response, and mortality in COVID-19. Eur. Respir. J. 2023, 62, 2300796. [Google Scholar] [CrossRef]
- Goldstein, E.; Lipsitch, M.; Cevik, M. On the Effect of Age on the Transmission of SARS-CoV-2 in Households, Schools, and the Community. J. Infect. Dis. 2021, 223, 362–369. [Google Scholar] [CrossRef]
- Viner, R.M.; Mytton, O.T.; Bonell, C.; Melendez-Torres, G.J.; Ward, J.; Hudson, L.; Waddington, C.; Thomas, J.; Russell, S.; van der Klis, F.; et al. Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared With Adults: A Systematic Review and Meta-analysis. JAMA Pediatr. 2021, 175, 143–156. [Google Scholar] [CrossRef]
- Sama, I.E.; Ravera, A.; Santema, B.T.; van Goor, H.; Ter Maaten, J.M.; Cleland, J.G.F.; Rienstra, M.; Friedrich, A.W.; Samani, N.J.; Ng, L.L.; et al. Circulating plasma concentrations of angiotensin-converting enzyme 2 in men and women with heart failure and effects of renin-angiotensin-aldosterone inhibitors. Eur. Heart J. 2020, 41, 1810–1817. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.-C.; Uhl, S.; Hoagland, D.; Møller, R.; Jordan, T.X.; Oishi, K.; Panis, M.; Sachs, D.; et al. Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 2020, 181, 1036–1045. [Google Scholar] [CrossRef] [PubMed]
- Flacco, M.E.; Acuti Martellucci, C.; Baccolini, V.; De Vito, C.; Renzi, E.; Villari, P.; Manzoli, L. COVID-19 vaccines reduce the risk of SARS-CoV-2 reinfection and hospitalization: Meta-analysis. Front. Med. (Lausanne) 2022, 9, 1023507. [Google Scholar] [CrossRef]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef]
- Italian Government. Decree-Law no. 105 of 23 July 2021. Urgent Measures to Deal with the Epidemiological Emergency from COVID-19 and for the Safe Exercise of Social and Economic Activities [Misure Urgenti per Fronteggiare l’emergenza Epidemiologica da COVID-19 e per l’esercizio in Sicurezza di Attivita’ Sociali ed Economiche]; Italian Government: Rome, Italy, 2021.
- Calabrò, G.E.; Pappalardo, C.; D’ambrosio, F.; Vece, M.; Lupi, C.; Lontano, A.; Di Russo, M.; Ricciardi, R.; de Waure, C. The Impact of Vaccination on COVID-19 Burden of Disease in the Adult and Elderly Population: A Systematic Review of Italian Evidence. Vaccines 2023, 11, 1011. [Google Scholar] [CrossRef] [PubMed]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. J. Med. Virol. 2022, 94, 2969–2976. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Luciani, A.; Borgonovo, K.; Ghilardi, M.; Parati, M.C.; Petro, D.; Lonati, V.; Pesenti, A.; Cabiddu, M. Third dose of SARS-CoV-2 vaccine: A systematic review of 30 published studies. J. Med. Virol. 2022, 94, 2837–2844. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Lan, X.; Zhang, L.; Zhang, X.; Zhang, J.; Song, M.; Liu, J. The effectiveness of the first dose COVID-19 booster vs. full vaccination to prevent SARS-CoV-2 infection and severe COVID-19 clinical event: A meta-analysis and systematic review of longitudinal studies. Front. Public Health 2023, 11, 1165611. [Google Scholar] [CrossRef]
- Italian Government. Misure Urgenti per Fronteggiare L’emergenza COVID-19, in Particolare nei Luoghi di Lavoro, Nelle Scuole e Negli Istituti della Formazione Superiore. (22G00002); Italian Government: Rome, Italy, 2021; Volume 56.
- Italian Ministry of Health. Circular Letter n.9498 of 4 April 2022. Update on Quarantine and Self-Surveillance Measures for Close (High-Risk) Contacts of SARS-CoV-2 Infection Cases [Aggiornamento Sulle Misure di Quarantena e Autosorveglianza per i Contatti Stretti (ad Alto Rischio) di Casi di Infezione da SARS-Cov-2]; Italian Ministry of Health: Rome, Italy, 2022.
- de Meijere, G.; Valdano, E.; Castellano, C.; Debin, M.; Kengne-Kuetche, C.; Turbelin, C.; Noel, H.; Weitz, J.S.; Paolotti, D.; Hermans, L.; et al. Attitudes towards booster, testing and isolation, and their impact on COVID-19 response in winter 2022/2023 in France, Belgium, and Italy: A cross-sectional survey and modelling study. Lancet Reg. Health Eur. 2023, 28, 100614. [Google Scholar] [CrossRef]
- Flacco, M.E.; Acuti Martellucci, C.; Baccolini, V.; De Vito, C.; Renzi, E.; Villari, P.; Manzoli, L. Risk of reinfection and disease after SARS-CoV-2 primary infection: Meta-analysis. Eur. J. Clin. Investig. 2022, 52, e13845. [Google Scholar] [CrossRef]
- Vancsa, S.; Dembrovszky, F.; Farkas, N.; Szako, L.; Teutsch, B.; Bunduc, S.; Nagy, R.; Parniczky, A.; Eross, B.; Peterfi, Z.; et al. Repeated SARS-CoV-2 Positivity: Analysis of 123 Cases. Viruses 2021, 13, 512. [Google Scholar] [CrossRef] [PubMed]
- Axfors, C.; Ioannidis, J.P.A. Infection fatality rate of COVID-19 in community-dwelling elderly populations. Eur. J. Epidemiol. 2022, 37, 235–249. [Google Scholar] [CrossRef]


{kind=link}
| Overall Sample | |
|---|---|
| (n = 300,079) | |
| Male gender, % (n) | 48.8 (146,435) |
| Mean age in years (SD) | 49.1 (20.9) |
| Age class in years, % (n) | |
| 21.5 (64,614) |
| 46.8 (140,460) |
| 31.7 (95,005) |
| Risk factors and comorbidities, % (n) A | |
| Hypertension | 14.1 (42,420) |
| Diabetes | 5.6 (16,674) |
| CVD | 8.5 (25,557) |
| COPD | 4.0 (11,912) |
| Kidney disease | 2.1 (6297) |
| Cancer | 5.9 (17,668) |
| Vaccination status, % (n) | |
| 16.7 (49,994) |
| 5.1 (15,409) |
| 16.0 (47,974) |
| 62.2 (186,702) |
| SARS-CoV-2 infection, % (n) | 41.5 (124,622) |
| Severe COVID-19, % (n) (among the infected) | 3.67 (4574) |
| COVID-19-related death, % (n) (among the infected) | 1.76 (2190) |
| Mean follow-up in days (SD) E | 932 (225) |
| SARS-CoV-2 Infection | Severe COVID-19 Ʊ | COVID-19-Related Death Ʊ | |
|---|---|---|---|
| (n = 124,622) | (n = 4574) | (n = 2190) | |
| Gender | %, * | %, * | %, * |
| Females | 43.7 | 3.11 | 1.67 |
| Males | 39.2 | 4.33 | 1.86 |
| Mean age in years (SD) | 46.6 (20.0) | 68.7 (16.7) | 79.1 (12.4) |
| Age class in years | %, * | %, * | %,* |
| 10–29 | 44.8 | 0.30 | 0.03 |
| 30–59 | 44.9 | 2.04 | 0.25 |
| 60 or more | 34.3 | 9.82 | 6.20 |
| Risk factors and comorbidities A | * | * | * |
| No hypertension | 42.2 | 2.01 | 0.79 |
| Hypertension | 37.4 | 15.04 | 8.41 |
| * | * | * | |
| No diabetes | 41.7 | 2.96 | 1.32 |
| Diabetes | 38.4 | 16.84 | 9.78 |
| * | * | * | |
| No CVD | 41.2 | 2.30 | 0.87 |
| CVD | 44.9 | 17.20 | 10.46 |
| * | * | * | |
| No COPD | 41.3 | 3.12 | 1.41 |
| COPD | 46.8 | 15.39 | 9.26 |
| * | * | * | |
| No kidney disease | 41.6 | 3.10 | 1.32 |
| Kidney disease | 39.3 | 31.86 | 23.45 |
| * | * | * | |
| No cancer | 41.7 | 3.21 | 1.36 |
| Cancer | 38.7 | 11.52 | 8.59 |
| Vaccination status B | |||
| 27,346/61,458 | 2963/27,346 | 1202/15,882 |
| % | 44.5 | 10.84 | 7.57 |
| 2181/6341 | 68/2181 | 100/11.249 |
| % | 34.4 | 3.12 | 0.89 |
| 30,221/50,359 | 483/30,221 | 230/27,836 |
| % | 60.0 | 1.60 | 0.83 |
| 64,874/181,921 | 1060/64,874 | 658/69,655 |
| % | 35.7 | 1.63 | 0.94 |
| Mean follow-up in days (SD) F | 749 (203) | 493 (280) | 616 (315) |
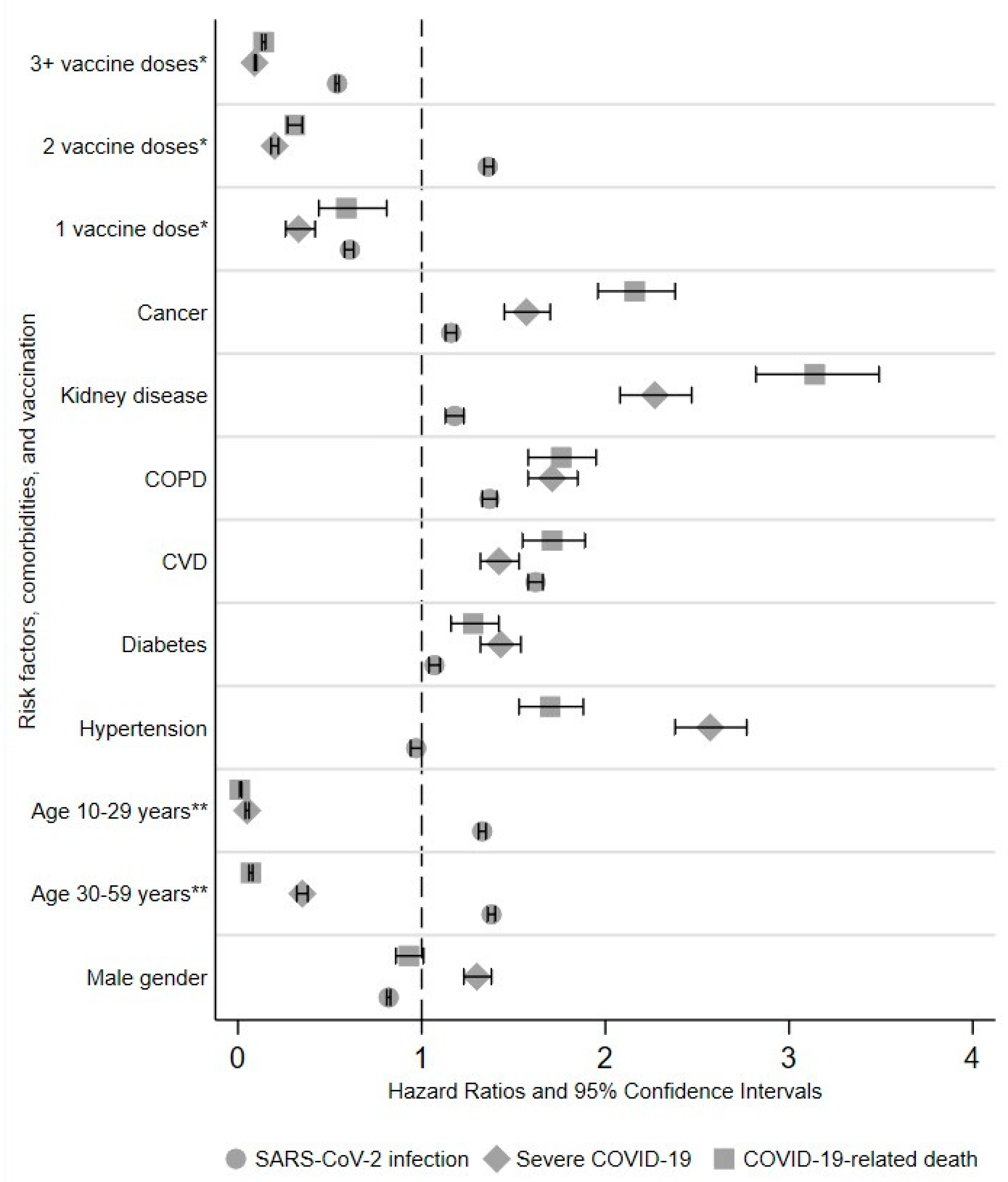
| Outcomes | SARS-CoV-2 Infection | Severe COVID-19 B | COVID-19-Related Death B |
|---|---|---|---|
| HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| Male gender | 0.82 (0.81–0.83) * | 1.30 (1.23–1.38) * | 0.93 (0.86–1.01) |
| Age class in years | |||
| 60 or more | 1 (Ref. cat.) | 1 (Ref. cat.) | 1 (Ref. cat.) |
| 30–59 | 1.38 (1.36–1.40) * | 0.35 (0.32–0.38) * | 0.07 (0.06–0.08) * |
| 10–29 | 1.33 (1.31–1.35) * | 0.05 (0.04–0.06) * | 0.01 (0.01–0.02) * |
| Risk factors and comorbidities | |||
| Hypertension | 0.97 (0.94–1.00) | 2.57 (2.38–2.77) * | 1.70 (1.53–1.88) * |
| Diabetes | 1.07 (1.04–1.10) * | 1.43 (1.32–1.54) * | 1.28 (1.16–1.42) * |
| CVD | 1.62 (1.58–1.66) * | 1.42 (1.32–1.53) * | 1.71 (1.55–1.89) * |
| COPD | 1.37 (1.33–1.41) * | 1.71 (1.58–1.85) * | 1.76 (1.58–1.95) * |
| Kidney disease | 1.18 (1.13–1.23) * | 2.27 (2.08–2.47) * | 3.14 (2.82–3.49) * |
| Cancer | 1.16 (1.13–1.19) * | 1.57 (1.45–1.70) * | 2.16 (1.96–2.38) * |
| Vaccination status | |||
| 1 (Ref. cat.) | 1 (Ref. cat.) | 1 (Ref. cat.) |
| 0.61 (0.58–0.63) * | 0.33 (0.26–0.42) * | 0.59 (0.44–0.81) * |
| 1.36 (1.34–1.39) * | 0.20 (0.18–0.22) * | 0.31 (0.27–0.35) * |
| 0.54 (0.53–0.55) * | 0.09 (0.09–0.10) * | 0.14 (0.13–0.15) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flacco, M.E.; Acuti Martellucci, C.; Soldato, G.; Di Martino, G.; Rosso, A.; Carota, R.; De Benedictis, M.; Di Marco, G.; Di Luzio, R.; Ricci, M.; et al. Predictors of SARS-CoV-2 Infection and Severe and Lethal COVID-19 after Three Years of Follow-Up: A Population-Wide Study. Viruses 2023, 15, 1794. https://doi.org/10.3390/v15091794
Flacco ME, Acuti Martellucci C, Soldato G, Di Martino G, Rosso A, Carota R, De Benedictis M, Di Marco G, Di Luzio R, Ricci M, et al. Predictors of SARS-CoV-2 Infection and Severe and Lethal COVID-19 after Three Years of Follow-Up: A Population-Wide Study. Viruses. 2023; 15(9):1794. https://doi.org/10.3390/v15091794
Chicago/Turabian StyleFlacco, Maria Elena, Cecilia Acuti Martellucci, Graziella Soldato, Giuseppe Di Martino, Annalisa Rosso, Roberto Carota, Marco De Benedictis, Graziano Di Marco, Rossano Di Luzio, Matteo Ricci, and et al. 2023. "Predictors of SARS-CoV-2 Infection and Severe and Lethal COVID-19 after Three Years of Follow-Up: A Population-Wide Study" Viruses 15, no. 9: 1794. https://doi.org/10.3390/v15091794