
Burden of Chikungunya Virus Infection during an Outbreak in Myanmar

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment and Study Areas
2.2. Molecular Detection of the CHIKV Genome Using Quantitative Reverse Transcription Polymerase Chain Reaction (qRT-PCR)
2.3. Detection of Anti-CHIKV IgM and IgG Antibodies
2.4. Neutralization Assay for the CHIKV Virus
2.5. Statistical Analysis
3. Results
3.1. Demographic Data of the Participants
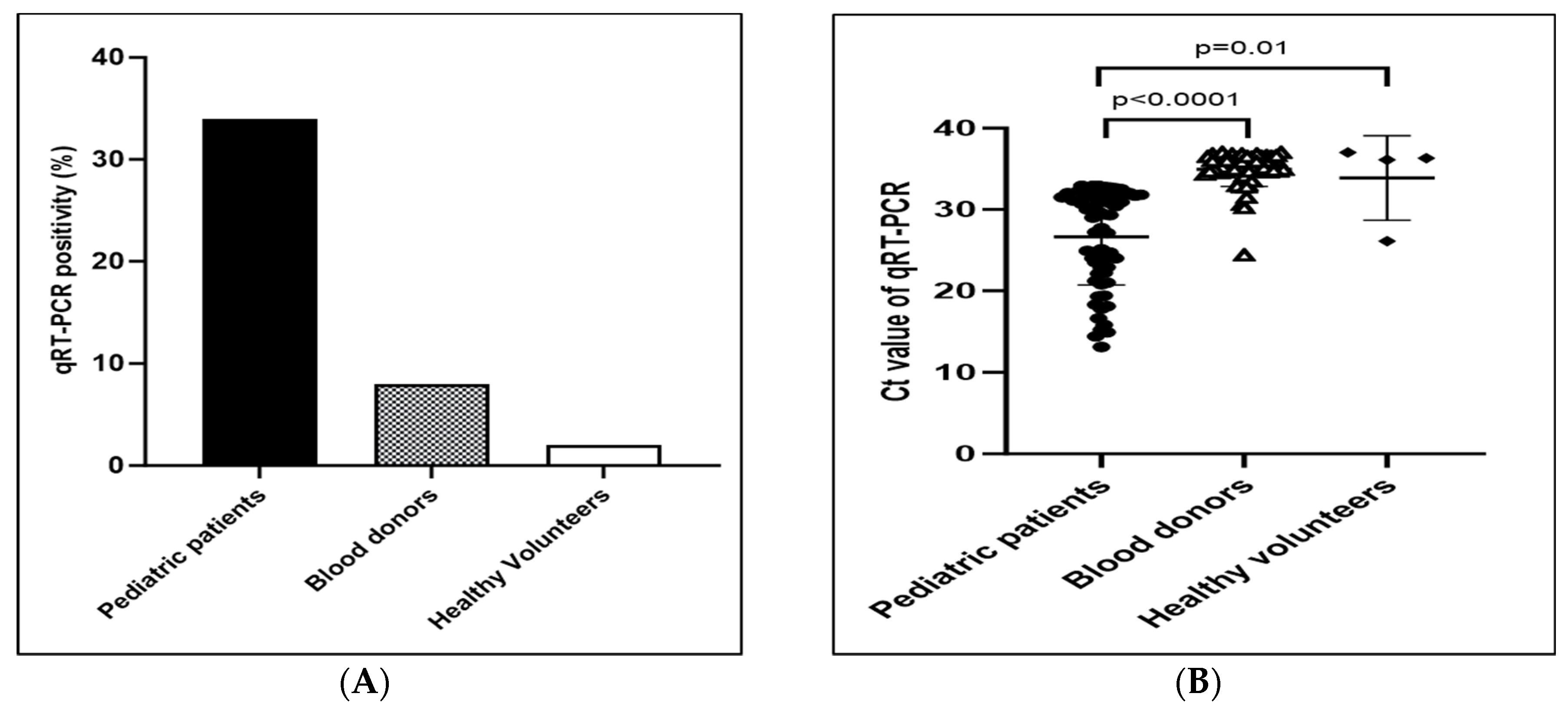
3.2. Proportion of Positive Molecular Tests among Study Population
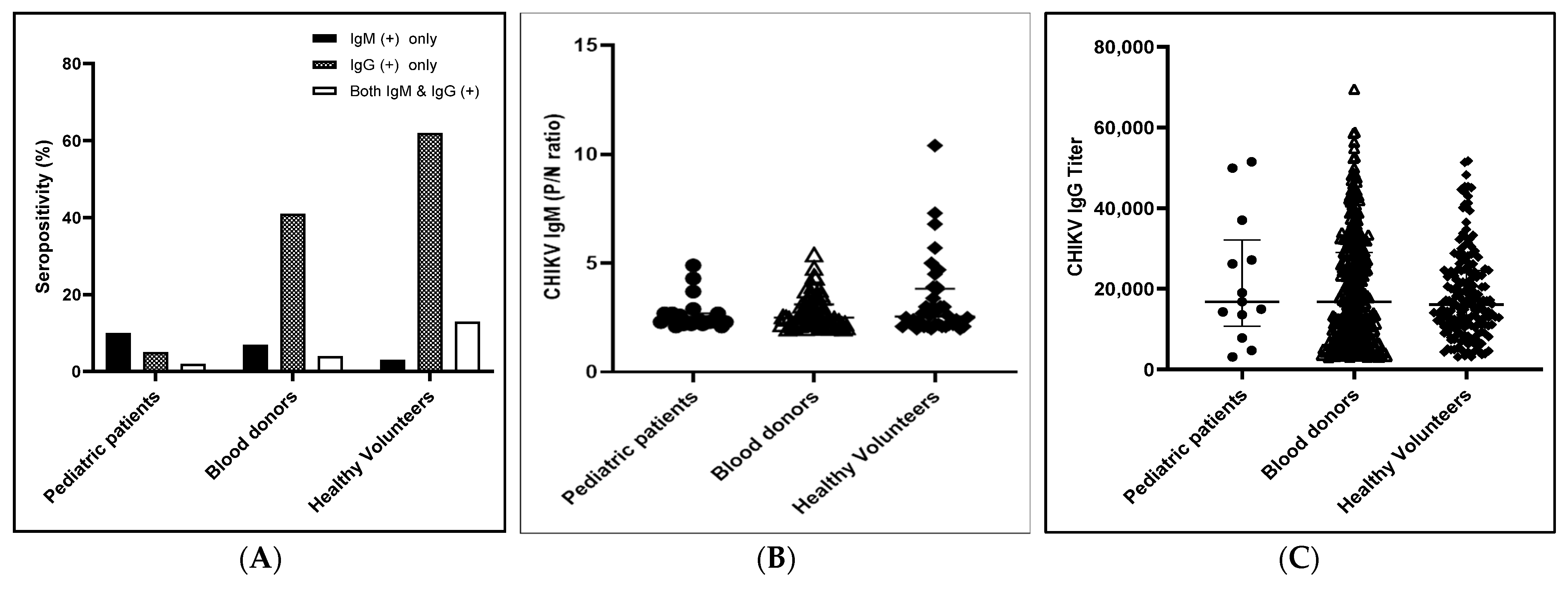
3.3. Immune Status (Anti-CHIKV IgM and Anti-CHIKV IgG Abs Positivity) against CHIKV among Study Population
3.4. CHIKV Neutralizing Antibody Levels among the Different Populations
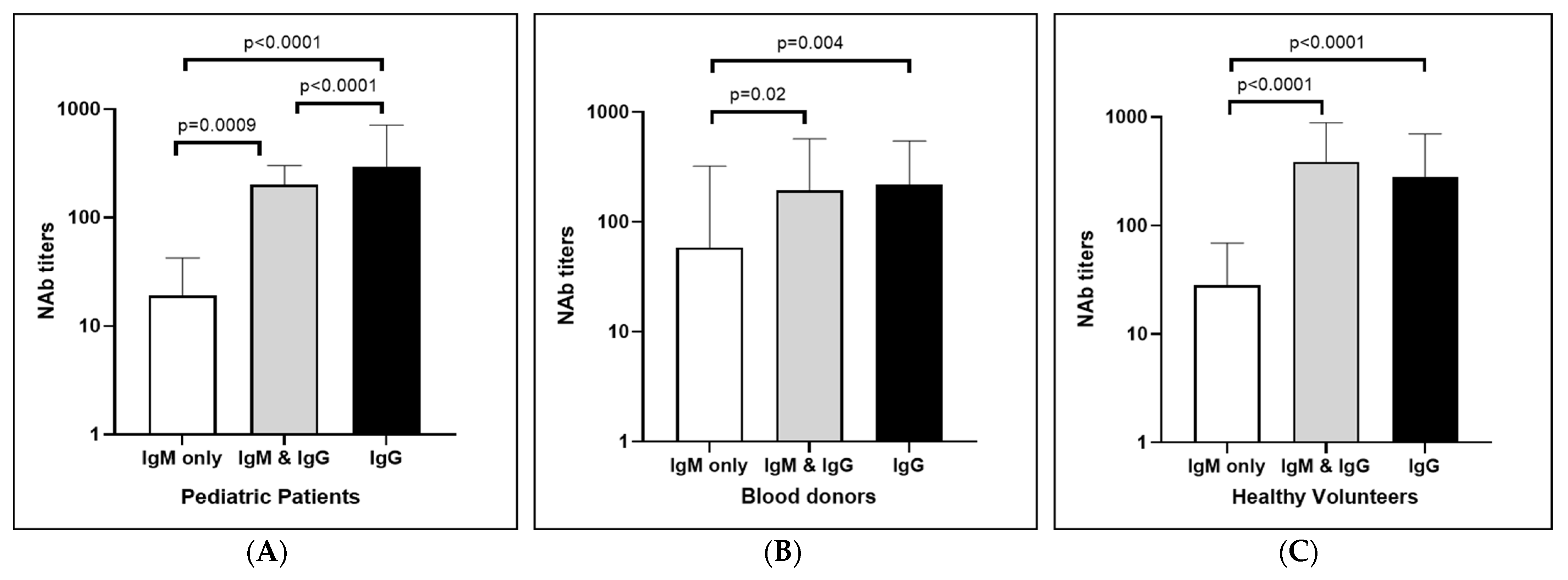
3.5. Comparison of Neutralizing Antibody Levels between Anti-CHIKV IgM Only, Anti-CHIKV IgG Only, and Both Positive Cases
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burrell, C.J.; Howard, C.R.; Murphy, F.A. Togaviruses. In Fenner and White’s Medical Virology; Academic Press: Cambridge, MA, USA, 2017. [Google Scholar]
- Vazeille, M.; Moutailler, S.; Coudrier, D.; Rousseaux, C.; Khun, H.; Huerre, M.; Thiria, J.; Dehecq, J.S.; Fontenille, D.; Schuffenecker, I.; et al. Two Chikungunya Isolates from the Outbreak of La Reunion (Indian Ocean) Exhibit Different Patterns of Infection in the Mosquito, Aedes albopictus. PLoS ONE 2007, 2, e1168. [Google Scholar] [CrossRef]
- Mourad, O.; Makhani, L.; Chen, L.H. Chikungunya: An Emerging Public Health Concern. Curr. Infect. Dis. Rep. 2022, 24, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Rueda, J.C.; Santos, A.M.; Angarita, J.I.; Giraldo, R.B.; Saldarriaga, E.L.; Ballesteros Muñoz, J.G.; Forero, E.; Valencia, H.; Somoza, F.; Martin-Arsanios, D.; et al. Demographic and Clinical Characteristics of Chikungunya Patients from Six Colombian Cities, 2014–2015. Emerg. Microbes Infect. 2019, 8, 1490–1500. [Google Scholar] [CrossRef] [PubMed]
- Thaung, U.; Ming, C.K.; Swe, T.; Thein, S. Epidemiological Features of Dengue and Chikungunya Infections in Burma. Southeast Asian J. Trop. Med. Public Health 1975, 6, 276–283. [Google Scholar]
- Luvai, E.A.C.; Kyaw, A.K.; Sabin, N.S.; Yu, F.; Hmone, S.W.; Thant, K.Z.; Inoue, S.; Morita, K.; Tun, M.M.N. Evidence of Chikungunya Virus Seroprevalence in Myanmar among Denguesuspected Patients and Healthy Volunteers in 2013, 2015, and 2018. PLoS Negl. Trop. Dis. 2021, 15, e0009961. [Google Scholar] [CrossRef] [PubMed]
- Kyaw, A.K.; Ngwe Tun, M.M.; Nabeshima, T.; Soe, A.M.; Thida; Aung, T.H.; Htwe, T.T.; Myaing, S.S.; Mar, T.T.; Aung, T.; et al. Chikungunya Virus Infection in Blood Donors and Patients during Outbreak, Mandalay, Myanmar, 2019. Emerg. Infect. Dis. 2020, 26, 2741–2745. [Google Scholar] [CrossRef]
- Ngwe Tun, M.M.; Kyaw, A.K.; Nabeshima, T.; Dumre, S.P.; Soe, A.M.; Nwe, K.M.; Myaing, S.S.; Lwin, E.P.; Win, Y.T.; Inoue, S.; et al. Coinfection and Circulation of Chikungunya Virus and Dengue Virus in Pediatric Patients in Myanmar, 2019. Microbes Infect. 2023, 25, 105129. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.E.; Lenschow, D.J.; Miner, J.J. Chikungunya Fever: Epidemiology, Clinical Manifestations and Diagnosis. UpToDate. January 2021. Available online: https://medilib.ir/uptodate/show/3024 (accessed on 7 June 2023).
- Piantadosi, A.; Kanjilal, S. Diagnostic Approach for Arboviral Infections in the United States. J. Clin. Microbiol. 2020, 58, e01926-19. [Google Scholar] [CrossRef]
- Mehta, R.; Gerardin, P.; de Brito, C.A.A.; Soares, C.N.; Ferreira, M.L.B.; Solomon, T. The Neurological Complications of Chikungunya Virus: A Systematic Review. Rev. Med. Virol. 2018, 28, e1978. [Google Scholar] [CrossRef] [Green Version]
- Haselbeck, A.H.; Im, J.; Prifti, K.; Marks, F.; Holm, M.; Zellweger, R.M. Serology as a Tool to Assess Infectious Disease Landscapes and Guide Public Health Policy. Pathogens 2022, 11, 732. [Google Scholar] [CrossRef]
- Alexander, N.; Carabali, M.; Lim, J.K. Estimating Force of Infection from Serologic Surveys with Imperfect Tests. PLoS ONE 2021, 16, e0247255. [Google Scholar] [CrossRef]
- Chelluboina, S.; Robin, S.; Aswathyraj, S.; Arunkumar, G. Persistence of Antibody Response in Chikungunya. Virusdisease 2019, 30, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Do Nascimento Costa, D.M.; Coêlho, M.R.C.D.; Da Cruz Gouveia, P.A.; Bezerra, L.A.; Marques, C.D.L.; Duarte, A.L.B.P.; Valente, L.M.; Da Silveira, V.M. Long-Term Persistence of Serum-Specific Anti-Chikungunya IgM Antibody—A Case Series of Brazilian Patients. Rev. Soc. Bras. Med. Trop. 2021, 54, e0855-2020. [Google Scholar] [CrossRef]
- Pierro, A.; Rossini, G.; Gaibani, P.; Finarelli, A.C.; Moro, M.L.; Landini, M.P.; Sambri, V. Persistence of Anti-Chikungunya Virus-Specific Antibodies in a Cohort of Patients Followed Fromthe Acute Phase of Infectionafter the 2007 Outbreak in Italy. New Microbes New Infect. 2015, 7, 23–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erasmus, J.H.; Rossi, S.L.; Weaver, S.C. Development of Vaccines for Chikungunya Fever. J. Infect. Dis. 2016, 214, S488–S496. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. New Vaccine Introduction. Checklist for Planning, Communication and Advocacy; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2017. [Google Scholar]
- Ho, P.S.; Ng, M.M.L.; Chu, J.J.H. Establishment of One-Step SYBR Green-Based Real Time-PCR Assay for Rapid Detection and Quantification of Chikungunya Virus Infection. Virol. J. 2010, 7, 13. [Google Scholar] [CrossRef] [Green Version]
- Tun, M.M.N.; Inoue, S.; Thant, K.Z.; Talemaitoga, N.; Aryati, A.; Dimaano, E.M.; Matias, R.R.; Buerano, C.C.; Natividad, F.F.; Abeyewickreme, W.; et al. Retrospective Seroepidemiological Study of Chikungunya Infection in South Asia, Southeast Asia and the Pacific Region. Epidemiol. Infect. 2016, 144, 2268–2275. [Google Scholar] [CrossRef] [Green Version]
- Ngwe Tun, M.M.; Thant, K.Z.; Inoue, S.; Nabeshima, T.; Aoki, K.; Kyaw, A.K.; Myint, T.; Tar, T.; Maung, K.T.T.; Hayasaka, D.; et al. Detection of East/Central/South African Genotype of Chikungunya Virus in Myanmar, 2010. Emerg. Infect. Dis. 2014, 20, 1378–1381. [Google Scholar] [CrossRef] [Green Version]
- Pandey, B.D.; Neupane, B.; Pandey, K.; Tun, M.M.N.; Morita, K. Detection of Chikungunya Virus in Nepal. Am. J. Trop. Med. Hyg. 2015, 93, 697–700. [Google Scholar] [CrossRef] [Green Version]
- Verma, A.; Nayak, K.; Chandele, A.; Singla, M.; Ratageri, V.H.; Lodha, R.; Kabra, S.K.; Murali-Krishna, K.; Ray, P. Chikungunya-Specific IgG and Neutralizing Antibody Responses in Natural Infection of Chikungunya Virus in Children from India. Arch. Virol. 2021, 166, 1913–1920. [Google Scholar] [CrossRef]
- Huits, R.; De Kort, J.; Van Den Berg, R.; Chong, L.; Tsoumanis, A.; Eggermont, K.; Bartholomeeusen, K.; Ariën, K.K.; Jacobs, J.; Van Esbroeck, M.; et al. Chikungunya Virus Infection in Aruba: Diagnosis, Clinical Features and Predictors of Post-Chikungunya Chronic Polyarthralgia. PLoS ONE 2018, 13, e0196630. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Fu, S.; Zhang, H.; Li, M.; Zhou, T.; Wang, J.; Zhang, Y.; Wang, H.; Tang, Q.; Liang, G. Distribution of Mosquitoes and Mosquito-Borne Viruses along the China-Myanmar Border in Yunnan Province. Jpn. J. Infect. Dis. 2012, 65, 215–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waggoner, J.J.; Ballesteros, G.; Gresh, L.; Mohamed-Hadley, A.; Tellez, Y.; Sahoo, M.K.; Abeynayake, J.; Balmaseda, A.; Harris, E.; Pinsky, B.A. Clinical Evaluation of a Single-Reaction Real-Time RT-PCR for Pan-Dengue and Chikungunya Virus Detection. J. Clin. Virol. 2016, 78, 57–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galán-Huerta, K.A.; Rivas-Estilla, A.M.; Fernández-Salas, I.; Farfan-Ale, J.A.; Ramos-Jiménez, J. Chikungunya Virus: A General Overview. Med. Univ. 2015, 17, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Nabli, B.; Chippaux-Hyppolite, C.; Chippaux, A.; Tamalet, J. Enquête Sérologique En Tunisie Sur Les Arbovirus. Bull. World Health Organ. 1970, 42, 297–303. [Google Scholar]
- Aubry, M.; Teissier, A.; Huart, M.; Merceron, S.; Vanhomwegen, J.; Mapotoeke, M.; Mariteragi-Helle, T.; Roche, C.; Vial, A.L.; Teururai, S.; et al. Seroprevalence of Dengue and Chikungunya Virus Antibodies, French Polynesia, 2014–2015. Emerg. Infect. Dis. 2018, 24, 558–561. [Google Scholar] [CrossRef] [Green Version]
- Bowen, E.T.W.; Simpson, D.I.H.; Platt, G.S.; Way, H.; Bright, W.F.; Day, J.; Achapa, S.; Roberts, J.M.D. Large Scale Irrigation and Arbovirus Epidemiology, Kano Plain, Kenya II. Preliminary Serological Survey. Trans. R. Soc. Trop. Med. Hyg. 1973, 67, 702–709. [Google Scholar] [CrossRef]
- Kama, M.; Aubry, M.; Naivalu, T.; Vanhomwegen, J.; Mariteragi-Helle, T.; Teissier, A.; Paoaafaite, T.; Hué, S.; Hibberd, M.L.; Manuguerra, J.C.; et al. Sustained Low-Level Transmission of Zika and Chikungunya Viruses after Emergence in the Fiji Islands. Emerg. Infect. Dis. 2019, 25, 1535–1538. [Google Scholar] [CrossRef] [Green Version]
- Somlor, S.; Vongpayloth, K.; Diancourt, L.; Buchy, P.; Duong, V.; Phonekeo, D.; Ketmayoon, P.; Vongphrachanh, P.; Brey, P.T.; Caro, V.; et al. Chikungunya Virus Emergence in the Lao PDR, 2012–2013. PLoS ONE 2017, 12, e0189879. [Google Scholar] [CrossRef] [Green Version]
- Skalinski, L.M.; Santos, A.E.S.; Paixão, E.; Itaparica, M.; Barreto, F.; da Conceição Nascimento Costa, M.; Teixeira, M.G. Chikungunya Seroprevalence in Population-Based Studies: A Systematic Review and Meta-Analysis. Arch. Public Health 2023, 81, 80. [Google Scholar] [CrossRef]
- Vongpunsawad, S.; Intharasongkroh, D.; Thongmee, T.; Poovorawan, Y. Seroprevalence of Antibodies to Dengue and Chikungunya Viruses in Thailand. PLoS ONE 2017, 12, e0180560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chua, C.L.; Sam, I.C.; Chiam, C.W.; Chan, Y.F. The Neutralizing Role of IgM during Early Chikungunya Virus Infection. PLoS ONE 2017, 12, e0171989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.A.; Hyde, T.B.; Mounier-Jack, S.; Brenzel, L.; Favin, M.; Gordon, W.S.; Shearer, J.C.; Mantel, C.F.; Arora, N.; Durrheim, D. New Vaccine Introductions: Assessing the Impact and the Opportunities for Immunization and Health Systems Strengthening. Vaccine 2013, 31, B122–B128. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall Number (%) | Male (%) | Female (%) |
|---|---|---|---|
| Age(years) | |||
| ≤5 | 70 (6.2) | 43 (61.4) | 27 (38.6) |
| 5–15 | 126 (11.2) | 63 (50.0) | 63 (50.0) |
| 16–45 | 872 (77.6) | 635 (73.0) | 237 (27.0) |
| ≥46 | 56 (5.0) | 39 (69.6) | 17 (30.3) |
| Total | 1124 (100) | 780 (69.4) | 344 (30.6) |
| Healthy Status | |||
| Dengue suspected patients | 196 (17.4) | 106 (54.1) | 90 (45.9) |
| Blood donors | 691(61.5) | 508 (73.5) | 183 (26.5) |
| Healthy volunteers | 237 (21.1) | 166 (70.0) | 71 (30.0) |
| Total | 1124 (100) | 780 (69.4) | 344 (30.6) |
| Region | |||
| Mandalay | 887 (78.9) | 614 (69.2) | 273 (30.8) |
| Yangon | 237 (21.1) | 166 (70.0) | 71 (30.0) |
| Total | 1124 (100) | 780 (69.4) | 344 (30.6) |
| IgM Ab Only (+) (n) | Confirmation Test (n, %) * | IgG Ab Only (+) (n) | Confirmation Test (n, %) * | IgM and IgG Ab (+) (n) | Confirmation Test (n, %) * | |
|---|---|---|---|---|---|---|
| Dengue suspected patients | 19 | 17/19 (89.5%) | 10 | 10/10 (100%) | 3 | 3/3 (100%) |
| Blood donors | 49 | 39/48 ** (81.2%) | 281 | 270/281 (96.1%) | 30 | 30/30 (100%) |
| Healthy volunteers | 8 | 4/8 (50%) | 146 | 146/146 (100%) | 30 | 30/30 (100%) |
| Total | 76 | 60/75 (80%) | 437 | 426/437 (96.3%) | 63 | 63/63 (100%) |
| Age (Years) | Neutralization Titer (FRNT50) | Positive/Tested (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 10 | 20 | 40 | 80 | 160 | 320 | 640 | 1280 | 2560 | ||
| Patients | ||||||||||
| 1–3 | 2 | 3 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 8/49 (16.3) |
| 4–6 | 4 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 7/60 (11.6) |
| 7–9 | 3 | 2 | 0 | 1 | 0 | 2 | 0 | 0 | 0 | 8/66 (12.1) |
| 10–12 | 1 | 0 | 0 | 2 | 4 | 1 | 0 | 0 | 0 | 8/21 (38.0) |
| Blood donors | ||||||||||
| 18–25 | 3 | 2 | 4 | 8 | 15 | 46 | 21 | 3 | 0 | 102/277 (36.8) |
| 26–35 | 3 | 1 | 5 | 14 | 33 | 32 | 14 | 2 | 0 | 104/234 (44.4) |
| 36–45 | 1 | 2 | 7 | 13 | 17 | 19 | 5 | 6 | 0 | 70/133 (52.6) |
| 46–55 | 0 | 0 | 4 | 5 | 7 | 10 | 6 | 1 | 0 | 33/47 (70.2) |
| Healthy volunteers | ||||||||||
| 18–25 | 1 | 0 | 1 | 8 | 21 | 21 | 19 | 11 | 0 | 82/96 (85.4) |
| 26–35 | 0 | 1 | 1 | 5 | 16 | 20 | 14 | 6 | 1 | 64/94 (68.0) |
| 36–45 | 0 | 0 | 4 | 7 | 2 | 6 | 4 | 2 | 0 | 25/38 (65.7) |
| 46–55 | 0 | 0 | 1 | 1 | 2 | 3 | 2 | 0 | 0 | 9/9 (100) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngwe Tun, M.M.; Kyaw, A.K.; Nwe, K.M.; Myaing, S.S.; Win, Y.T.; Inoue, S.; Takamatsu, Y.; Urano, T.; Thu, H.M.; Hmone, S.W.; et al. Burden of Chikungunya Virus Infection during an Outbreak in Myanmar. Viruses 2023, 15, 1734. https://doi.org/10.3390/v15081734
Ngwe Tun MM, Kyaw AK, Nwe KM, Myaing SS, Win YT, Inoue S, Takamatsu Y, Urano T, Thu HM, Hmone SW, et al. Burden of Chikungunya Virus Infection during an Outbreak in Myanmar. Viruses. 2023; 15(8):1734. https://doi.org/10.3390/v15081734
Chicago/Turabian StyleNgwe Tun, Mya Myat, Aung Kyaw Kyaw, Khine Mya Nwe, Su Su Myaing, Ye Thu Win, Shingo Inoue, Yuki Takamatsu, Takeshi Urano, Hlaing Myat Thu, Saw Wutt Hmone, and et al. 2023. "Burden of Chikungunya Virus Infection during an Outbreak in Myanmar" Viruses 15, no. 8: 1734. https://doi.org/10.3390/v15081734