
Revision of Cytomegalovirus Immunoglobulin M Antibody Titer Cutoff in a Maternal Antibody Screening Program in Japan: A Cohort Comparison Involving a Total of 32,000 Pregnant Women
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Antibody and DNA Tests
2.2. Maternal Screening Program and Neurological Tests in cCMV Infants
2.3. Comparison of Maternal Screening with the Original and Revised Cutoffs of CMV IgM Antibody Titer
3. Results
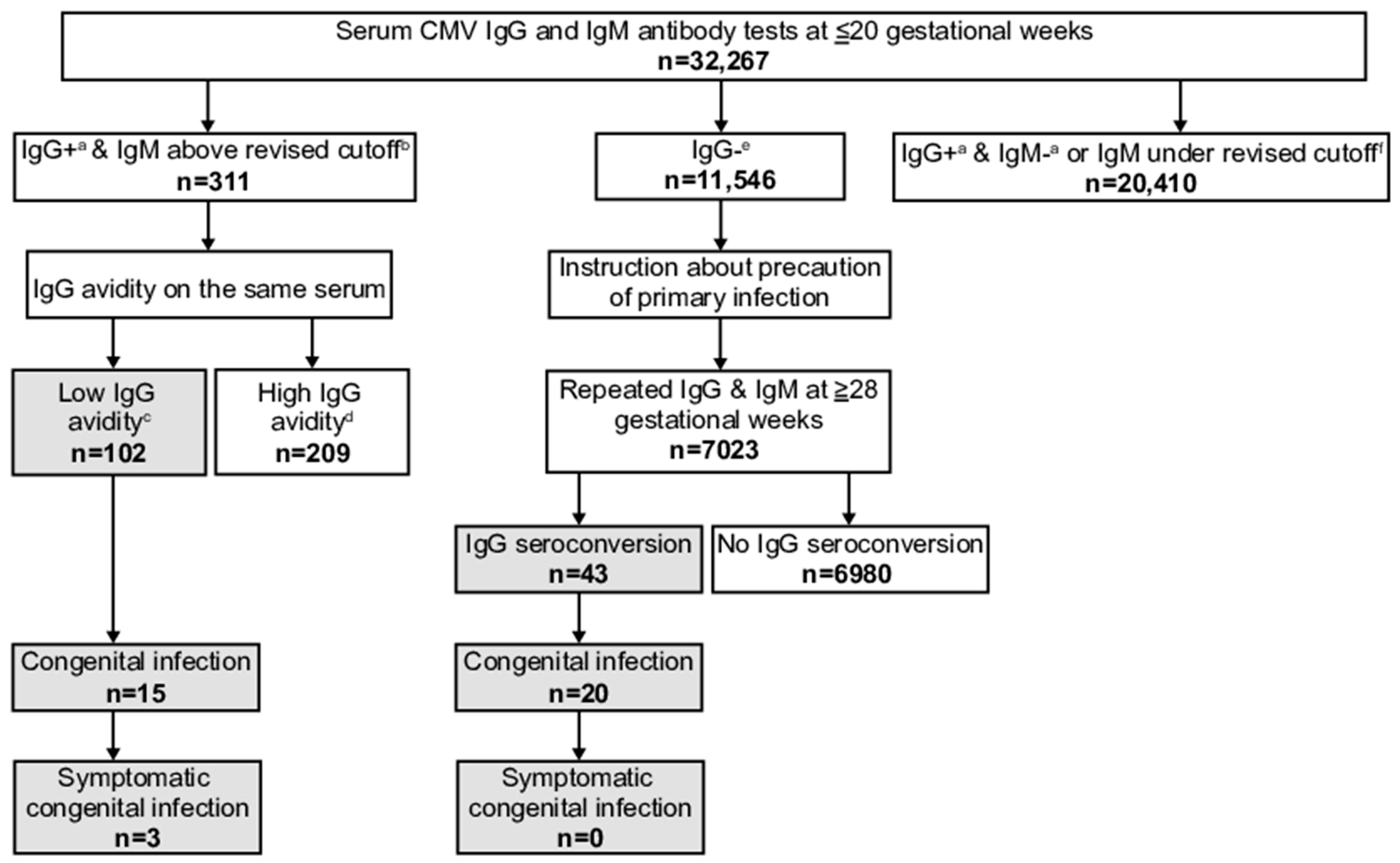
3.1. Maternal Screening with Revised Cutoff of CMV IgM Antibody Titer and Infant cCMV
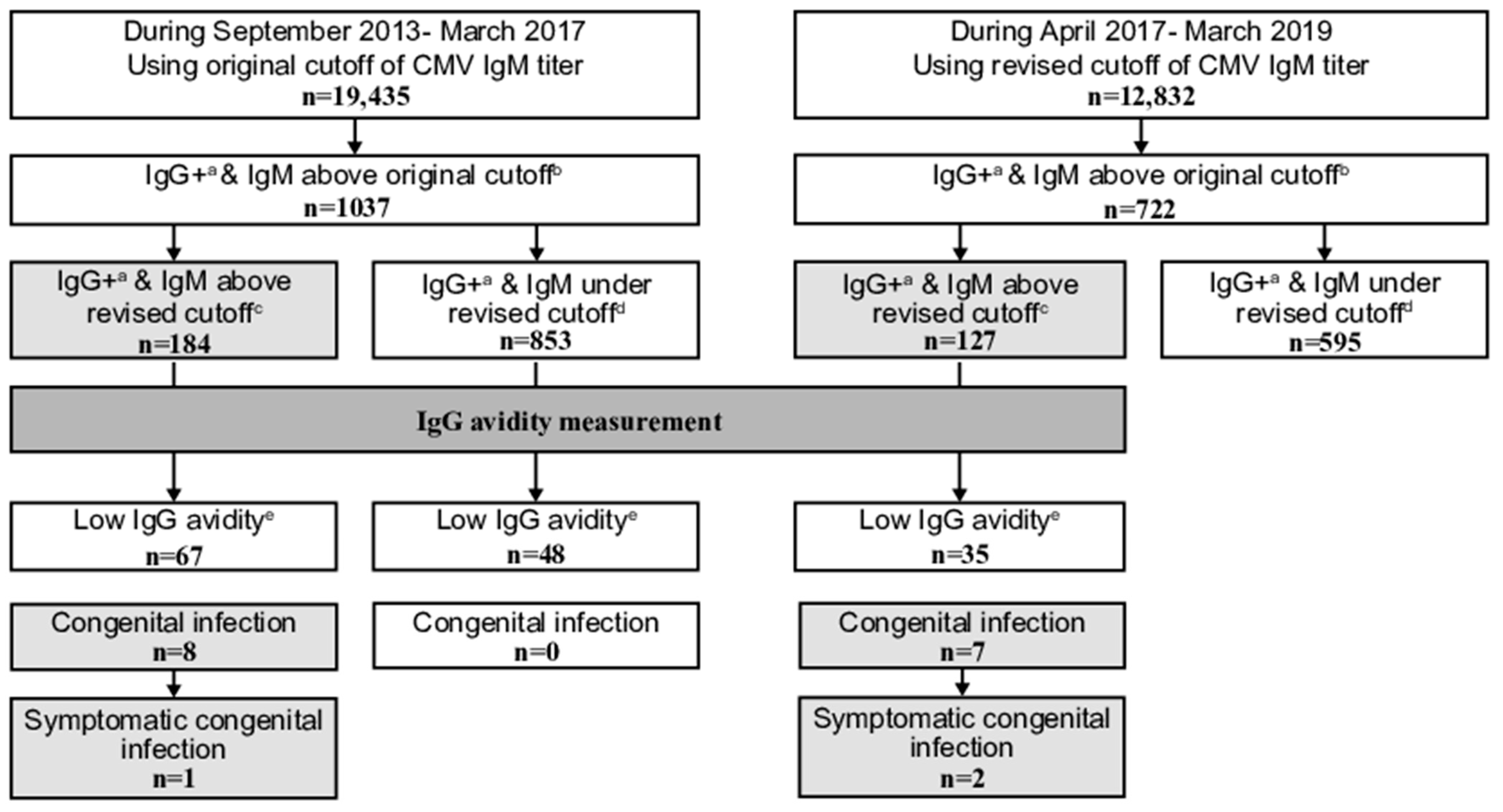
3.2. Revised Versus Original Cutoff of CMV IgM Antibody Titer
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ssentongo, P.; Hehnly, C.; Birungi, P.; Roach, M.A.; Spady, J.; Fronterre, C.; Wang, M.; Murray-Kolb, L.E.; Al-Shaar, L.; Chinchilli, V.M.; et al. Congenital Cytomegalovirus Infection Burden and Epidemiologic Risk Factors in Countries With Universal Screening: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e2120736. [Google Scholar] [CrossRef]
- Zenebe, M.H.; Mekonnen, Z.; Loha, E.; Padalko, E. Congenital cytomegalovirus infections mother-newborn pair study in Southern Ethiopia. Can. J. Infect. Dis. Microbiol. 2021, 2021, 4646743:1–4646743:7. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, G.; Garofoli, F.; Stronati, M. Congenital cytomegalovirus infection: Treatment, sequelae and follow-up. J. Matern. Fetal Neonatal Med. 2010, 23 (Suppl. 3), 45–48. [Google Scholar] [CrossRef] [PubMed]
- Berth, M.; Grangeot-Keros, L.; Heskia, F.; Dugua, J.M.; Vauloup-Fellous, C. Analytical issues possibly affecting the performance of commercial human cytomegalovirus IgG avidity assays. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1579–1584. [Google Scholar] [CrossRef] [PubMed]
- Leruez-Ville, M.; Foulon, I.; Pass, R.; Ville, Y. Cytomegalovirus infection during pregnancy: State of the science. Am. J. Obstet. Gynecol. 2020, 223, 330–349. [Google Scholar] [CrossRef]
- Toriyabe, K.; Morikawa, F.; Minematsu, T.; Ikejiri, M.; Suga, S.; Ikeda, T. Anti-cytomegalovirus immunoglobulin M titer for congenital infection in first-trimester pregnancy with primary infection: A multicenter prospective cohort study. J. Perinatol. 2017, 37, 1272–1277. [Google Scholar] [CrossRef]
- Torii, Y.; Yoshida, S.; Yanase, Y.; Mitsui, T.; Horiba, K.; Okumura, T.; Takeuchi, S.; Suzuki, T.; Kawada, J.I.; Kotani, T.; et al. Serological screening of immunoglobulin M and immunoglobulin G during pregnancy for predicting congenital cytomegalovirus infection. BMC Pregnancy Childbirth. 2019, 19, 205. [Google Scholar] [CrossRef] [Green Version]
- Ikuta, K.; Koshizuka, T.; Kanno, R.; Inoue, N.; Kubo, T.; Koyano, S.; Suzutani, T. Evaluation of the indirect and IgM-capture anti-human cytomegalovirus IgM ELISA methods as confirmed by cytomegalovirus IgG avidity. Microbiol. Immunol. 2019, 63, 172–178. [Google Scholar] [CrossRef]
- Shimada, K.; Toriyabe, K.; Kitamura, A.; Morikawa, F.; Minematsu, T.; Ikejiri, M.; Suga, S.; Toyoda, H.; Amano, K.; Kitano, M.; et al. Primary cytomegalovirus infection during pregnancy and congenital infection: A population-based, mother-child, prospective cohort study. J. Perinatol. 2021, 41, 2474–2481. [Google Scholar] [CrossRef]
- Shimada, K.; Toriyabe, K.; Kitamura, A.; Morikawa, F.; Ikejiri, M.; Minematsu, T.; Nakamura, H.; Suga, S.; Ikeda, T. Characteristics and serology of pregnant women with cytomegalovirus immunoglobulin G seroconversion during pregnancy in Japan. Taiwan J. Obstet. Gynecol. 2021, 60, 621–627. [Google Scholar] [CrossRef]
- Voordouw, B.; Rockx, B.; Jaenisch, T.; Fraaij, P.; Mayaud, P.; Vossen, A.; Koopmans, M. Performance of Zika assays in the context of Toxoplasma gondii, Parvovirus B19, rubella virus, and cytomegalovirus (TORCH) diagnostic assays. Clin. Microbiol. Rev. 2019, 33, e00130-18:1–e00130-18:23. [Google Scholar] [CrossRef] [PubMed]
- Lagrou, K.; Bodeus, M.; Van Ranst, M.; Goubau, P. Evaluation of the new architect cytomegalovirus immunoglobulin M (IgM), IgG, and IgG avidity assays. J. Clin. Microbiol. 2009, 47, 1695–1699. [Google Scholar] [CrossRef] [Green Version]
- Carlier, P.; Harika, N.; Bailly, R.; Vranken, G. Laboratory evaluation of the new Access® cytomegalovirus immunoglobulin IgM and IgG assays. J. Clin. Virol. 2010, 49, 192–197. [Google Scholar] [CrossRef]
- Revello, M.G.; Vauloup-Fellous, C.; Grangeot-Keros, L.; van Helden, J.; Dickstein, Y.; Lipkin, I.; Mühlbacher, A.; Lazzarotto, T. Clinical evaluation of new automated cytomegalovirus IgM and IgG assays for the Elecsys® analyser platform. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 3331–3339. [Google Scholar] [CrossRef] [PubMed]
- Delforge, M.L.; Desomberg, L.; Montesinos, I. Evaluation of the new LIAISON® CMV IgG, IgM and IgG Avidity II assays. J. Clin. Virol. 2015, 72, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Chiereghin, A.; Pavia, C.; Gabrielli, L.; Piccirilli, G.; Squarzoni, D.; Turello, G.; Gibertoni, D.; Simonazzi, G.; Capretti, M.G.; Lanari, M.; et al. Clinical evaluation of the new Roche platform of serological and molecular cytomegalovirus-specific assays in the diagnosis and prognosis of congenital cytomegalovirus infection. J. Virol. Methods 2017, 248, 250–254. [Google Scholar] [CrossRef]
- Maine, G.T.; Stricker, R.; Schuler, M.; Spesard, J.; Brojanac, S.; Iriarte, B.; Herwig, K.; Gramins, T.; Combs, B.; Wise, J.; et al. Development and clinical evaluation of a recombinant-antigen-based cytomegalovirus immunoglobulin M automated immunoassay using the Abbott AxSYM analyzer. J. Clin. Microbiol. 2000, 38, 1476–1481. [Google Scholar] [CrossRef] [Green Version]
- Prince, H.E.; Lapé-Nixon, M. Role of cytomegalovirus (CMV) IgG avidity testing in diagnosing primary CMV infection during pregnancy. Clin. Vaccine Immunol. 2014, 21, 1377–1384. [Google Scholar] [CrossRef] [Green Version]
- Lazzarotto, T.; Galli, C.; Pulvirenti, R.; Rescaldani, R.; Vezzo, R.; La Gioia, A.; Martinelli, C.; La Rocca, S.; Agresti, G.; Grillner, L.; et al. Evaluation of the Abbott AxSYM cytomegalovirus (CMV) immunoglobulin M (IgM) assay in conjunction with other CMV IgM tests and a CMV IgG avidity assay. Clin. Diagn. Lab. Immunol. 2001, 8, 196–198. [Google Scholar] [CrossRef] [Green Version]
- Genser, B.; Truschnig-Wilders, M.; Stünzner, D.; Landini, M.P.; Halwachs-Baumann, G. Evaluation of five commercial enzyme immunoassays for the detection of human cytomegalovirus-specific IgM antibodies in the absence of a commercially available gold standard. Clin. Chem. Lab. Med. 2001, 39, 62–70. [Google Scholar] [CrossRef]
- Gentile, M.; Galli, C.; Pagnotti, P.; Di Marco, P.; Tzantzoglou, S.; Bellomi, F.; Ferreri, M.L.; Selvaggi, C.; Antonelli, G. Measurement of the sensitivity of different commercial assays in the diagnosis of CMV infection in pregnancy. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 28, 977–981. [Google Scholar] [CrossRef] [PubMed]
- Baalawi, F.; Robertson, P.W.; Lahra, M.; Rawlinson, W.D. Comparison of five CMV IgM immunoassays with CMV IgG avidity for diagnosis of primary CMV infection. Pathology 2012, 44, 381–383. [Google Scholar] [CrossRef]
- Weber, B.; Berger, A.; Rabenau, H. Human cytomegalovirus infection: Diagnostic potential of recombinant antigens for cytomegalovirus antibody detection. J. Virol. Methods 2001, 96, 157–170. [Google Scholar] [CrossRef]
- Binnicker, M.J.; Jespersen, D.J.; Harring, J.A. Multiplex detection of IgM and IgG class antibodies to Toxoplasma gondii, rubella virus, and cytomegalovirus using a novel multiplex flow immunoassay. Clin. Vaccine Immunol. 2010, 17, 1734–1738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajasekariah, H.; Scott, G.; Robertson, P.W.; Rawlinson, W.D. Improving diagnosis of primary cytomegalovirus infection in pregnant women using immunoblots. J. Med. Virol. 2013, 85, 315–319. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No. | Maternal Age (Year) | Maternal Parity (Para) | Result of Maternal Antibody Screening | Titer of IgM at Early Pregnancy (Index) | Avidity Index of IgG at Early Pregnancy (%) | GW of Maternal Antibody Tests in Early/Late Pregnancy (Week) | GW of Delivery (Week) | Delivery Mode | Infant Sex | Infant Body Weight at Birth (g) | Infant Height at Birth (cm) | Infant HC at Birth (cm) | Infant Apgar Scores at 1, 5 min | UA pH | Universal Newborn Hearing Screening | Amount of CMV DNA in Neonatal Urine (log10) (Copy/mL) | Viral Isolation of Neonatal Urine | Subunit of gB | Infant Abnormal Neurological Tests |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 24 | 2 | Low IgG avidity | 12.00 | 2.2 | 10/- | 38 + 6 | Vaginal | Male | 2930 | 50.0 | 32.0 | 9, 10 | 7.309 | Pass | 6 | + | 1 | - |
| 2 | 30 | 1 | Low IgG avidity | 8.49 | 11.4 | 10/- | 39 + 6 | Vaginal | Male | 3102 | 50.0 | 33.4 | 9, 10 | 7.349 | Pass | 4 | + | 3 | - |
| 3 | 30 | 0 | Low IgG avidity | 7.74 | 31.9 | 11/- | 37 + 5 | Vacuum | Male | 3090 | 51.0 | 33.5 | 3, 9 | 7.068 | Left refer | 4 | + | 3 | MRI + ABR |
| 4 | 26 | 0 | Low IgG avidity | 9.72 | 0.0 | 7/- | 41 + 3 | Vaginal | Male | 2930 | 48.0 | 32.0 | 10, 10 | 7.360 | Pass | 7 | + | 3 | - |
| 5 | 22 | 1 | Low IgG avidity | 12.00 | 2.5 | 13/- | 39 + 3 | Vaginal | Female | 2816 | 48.3 | 32.0 | 9, 10 | 7.284 | Pass | 6 | + | 1 | - |
| 6 | 24 | 0 | Low IgG avidity | 12.00 | 2.5 | 10/- | 40 + 2 | Vaginal | Male | 3482 | 49.5 | 32.0 | 8, 10 | 7.236 | Bilateral refer | 4 | - | 1 | ABR |
| 7 | 32 | 1 | Low IgG avidity | 12.00 | 4.5 | 11/- | 39 + 4 | Vaginal | Female | 3008 | 48.0 | 33.0 | 10, 10 | 7.367 | Pass | 5 | + | 1 | - |
| 8 | 20 | 1 | IgG seroconversion | - | - | 12/34 | 39 + 1 | Vaginal | Male | 3496 | 50.3 | 34.0 | 10, 10 | 7.340 | Pass | 6 | + | 1 | - |
| 9 | 27 | 1 | IgG seroconversion | - | - | 11/43 * | 38 + 1 | Vaginal | Female | 2458 | 49.0 | 30.0 | 10, 10 | 7.460 | Right refer | 3 | + | 1 | ABR ** |
| 10 | 30 | 1 | IgG seroconversion | - | - | 8/36 | 39 + 5 | Vaginal | Male | 3512 | 50.5 | 33.3 | 9, 10 | 7.462 | Pass | 4 | + | 3 | - |
| 11 | 22 | 0 | IgG seroconversion | - | - | 12/34 | 41 + 0 | Vaginal | Male | 4006 | 51.0 | 36.0 | 9, 10 | 7.276 | Pass | 6 | - | 3 | - |
| 12 | 35 | 1 | IgG seroconversion | - | - | 16/36 | 39 + 5 | Vaginal | Female | 3428 | 49.0 | 35.5 | 8, 9 | 7.273 | Pass | 6 | + | 1 | - |
| 13 | 26 | 1 | High IgG avidity | 3.68 | 76.6 | 14/- | 22 + 1 | Abortion | Male | 476 | 25.0 | 18.0 | - | - | - | 5 (Ascites) | -(Ascites) | - | - |
| 14 | 27 | 2 | High IgG avidity | 2.17 | 77.3 | 9/- | 40 + 1 | Vaginal | Female | 3134 | 50.0 | 33.0 | 10, 10 | 7.297 | Pass | 4 | + | 1 | ABR |
| Results of Maternal CMV Antibody Screening | Number of Pregnant Women | Number of Neonatal Urine CMV DNA Tests | Number of cCMV Cases Including Symptomatic cCMV | Number of Symptomatic cCMV Cases |
|---|---|---|---|---|
| Positive * IgG, IgM above the revised cutoff, and high IgG avidity | 209 | 71 | 0 | 0 |
| Positive * IgG, IgM under the revised cutoff, and high IgG avidity | 805 | 48 | 2 | 2 |
| Positive * IgG, IgM under the revised cutoff, and unknown IgG avidity | 595 | 126 | 0 | 0 |
| Positive * IgG and negative * IgM | 18,962 | 146 | 0 | 0 |
| Study Period | April 2017–March 2019 | September 2013–March 2017 | p Value |
|---|---|---|---|
| Cutoff of CMV IgM titer to measure IgG avidity as a reflex test in maternal antibody screening program | The revised cutoff (≥4.00 index) of CMV IgM titer | The original cutoff (≥1.21 index) of CMV IgM titer | |
| Total number of participating pregnant women | 12,832 | 19,435 | |
| Number of pregnant women with positive CMV IgG * and IgM above the original cutoff (≥1.21 index of IgM titer) | 722 (5.6%) | 1037 (5.3%) | 0.26 |
| Number of pregnant women with positive CMV IgG * and IgM above the revised cutoff (≥4.00 index of IgM titer) | 127 (1.0%) | 184 (1.0%) | 0.73 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitamura, A.; Toriyabe, K.; Hagimoto-Akasaka, M.; Hamasaki-Shimada, K.; Ikejiri, M.; Minematsu, T.; Suga, S.; Kondo, E.; Kihira, M.; Morikawa, F.; et al. Revision of Cytomegalovirus Immunoglobulin M Antibody Titer Cutoff in a Maternal Antibody Screening Program in Japan: A Cohort Comparison Involving a Total of 32,000 Pregnant Women. Viruses 2023, 15, 962. https://doi.org/10.3390/v15040962
Kitamura A, Toriyabe K, Hagimoto-Akasaka M, Hamasaki-Shimada K, Ikejiri M, Minematsu T, Suga S, Kondo E, Kihira M, Morikawa F, et al. Revision of Cytomegalovirus Immunoglobulin M Antibody Titer Cutoff in a Maternal Antibody Screening Program in Japan: A Cohort Comparison Involving a Total of 32,000 Pregnant Women. Viruses. 2023; 15(4):962. https://doi.org/10.3390/v15040962
Chicago/Turabian StyleKitamura, Asa, Kuniaki Toriyabe, Miki Hagimoto-Akasaka, Kyoko Hamasaki-Shimada, Makoto Ikejiri, Toshio Minematsu, Shigeru Suga, Eiji Kondo, Masamichi Kihira, Fumihiro Morikawa, and et al. 2023. "Revision of Cytomegalovirus Immunoglobulin M Antibody Titer Cutoff in a Maternal Antibody Screening Program in Japan: A Cohort Comparison Involving a Total of 32,000 Pregnant Women" Viruses 15, no. 4: 962. https://doi.org/10.3390/v15040962