
Prevalence of Human Papillomavirus Types 16/18 and Effect of Vaccination among Japanese Female General Citizens in the Vaccine Crisis Era
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Material Collection
2.2. HPV Detection and Genotyping Procedures
2.3. Statistical Methods
3. Results
3.1. Study Participants
3.2. Status of HPV Vaccination and Participant Characteristics
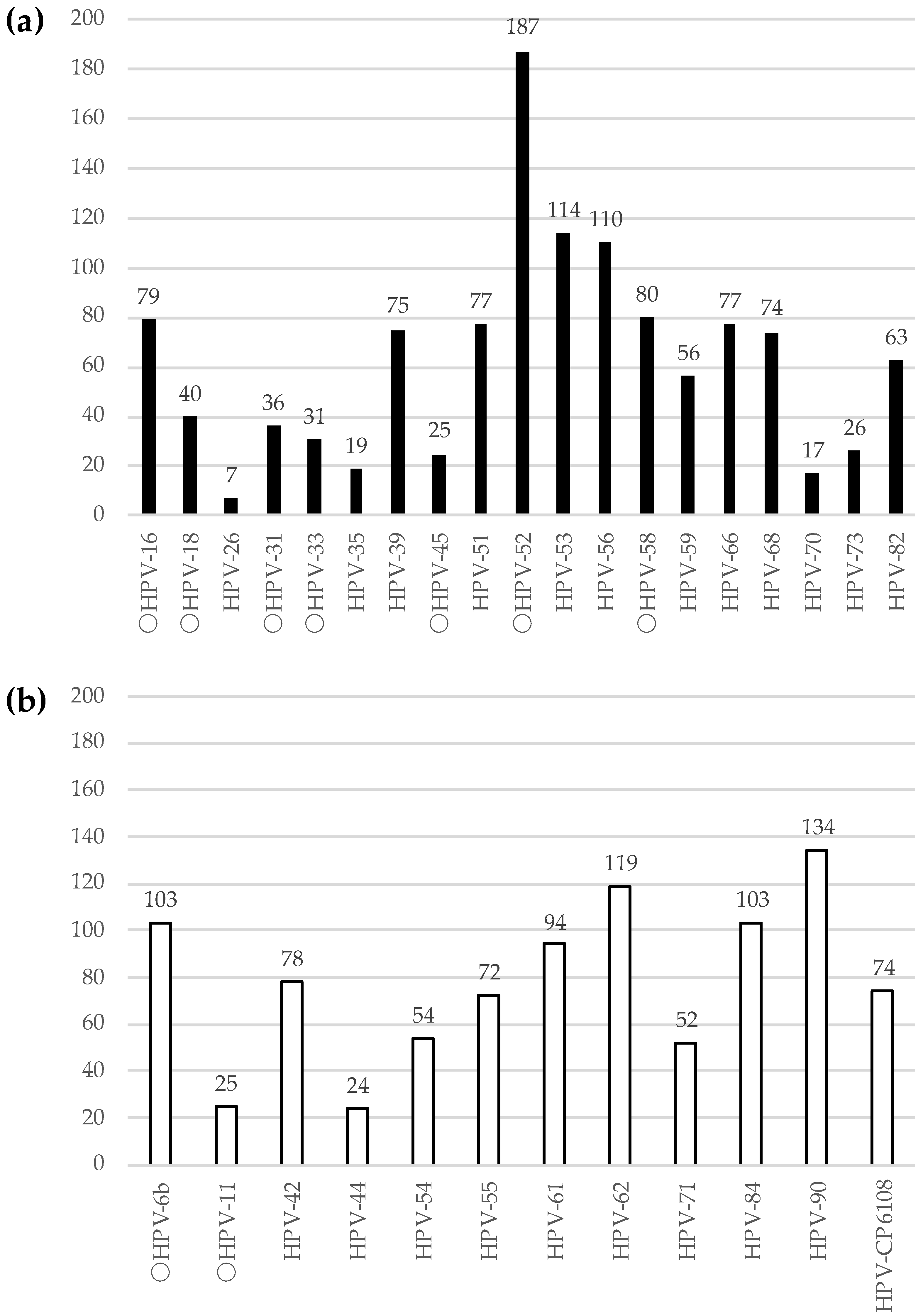
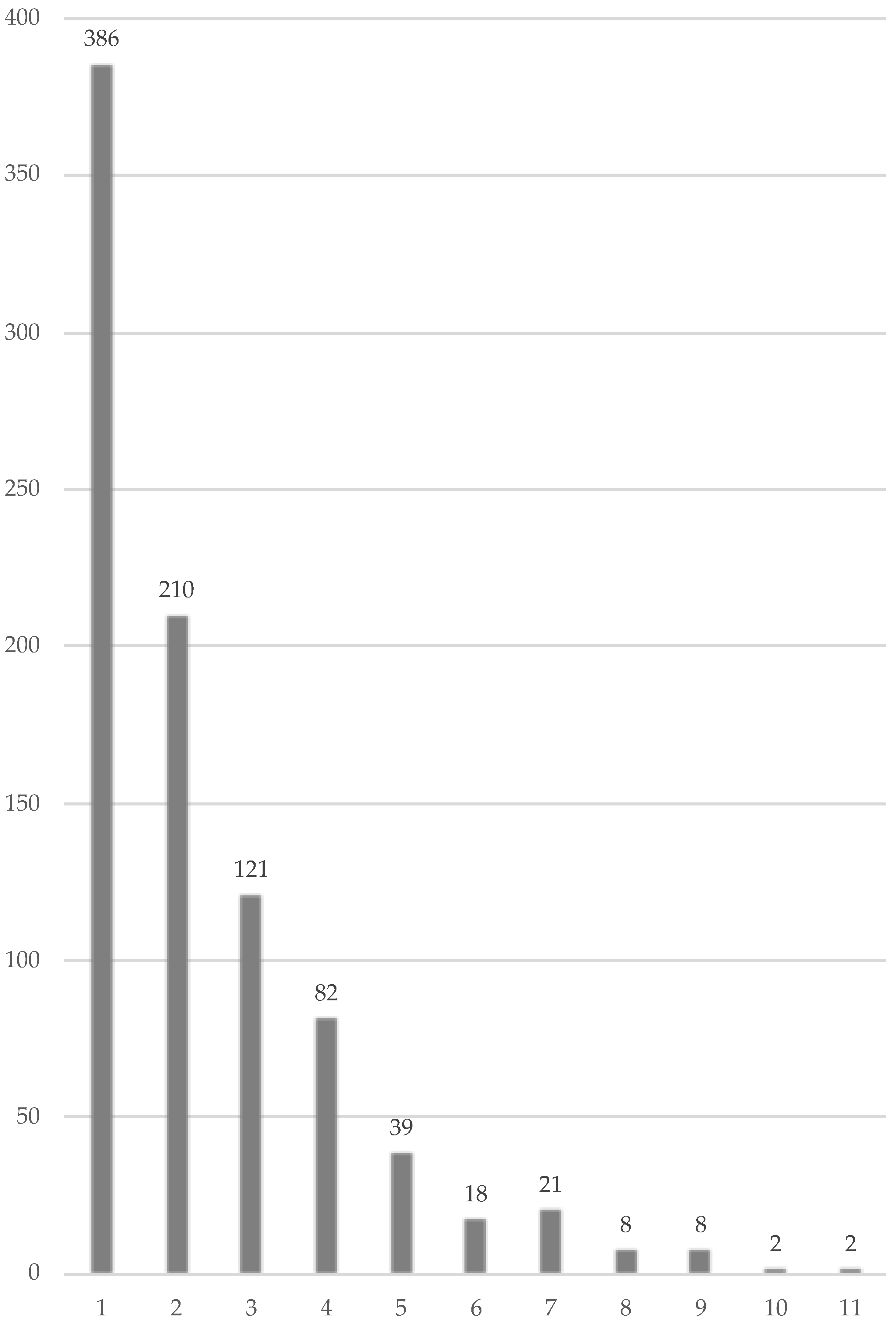
3.3. Distribution of HPV Genotypes and Coverage of HPV Vaccination by Age Groups
3.4. Association between Characteristics of the Participants and Risk of HPV Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GLOBOCAN 2020. Available online: https://gco.iarc.fr/today/data/factsheets/populations/900-world-fact-sheets.pdf (accessed on 10 October 2022).
- CANCER STATISTICS IN JAPAN. Available online: https://ganjoho.jp/reg_stat/statistics/stat/cancer/17_cervix_uteri.html (accessed on 10 October 2022).
- Katanoda, K.; Shibata, A.; Matsuda, T.; Hori, M.; Nakata, K.; Narita, Y.; Ogawa, C.; Munakata, W.; Kawai, A.; Nishimoto, H. Childhood, adolescent and young adult cancer incidence in Japan in 2009–2011. Jpn. J. Clin. Oncol. 2017, 47, 762–771. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization, Immunization, Vaccines and Biologicals. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/diseases/human-papillomavirus-vaccines-(HPV) (accessed on 31 December 2022).
- World Health Organization, Cervical Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer (accessed on 31 December 2022).
- Kunitoki, K.; Funato, M.; Mitsunami, M.; Kinoshita, T.; Reich, M.R. Access to HPV vaccination in Japan: Increasing social trust to regain vaccine confidence. Vaccine 2021, 39, 6104–6110. [Google Scholar] [CrossRef] [PubMed]
- Hanley, S.J.B.; Yoshioka, E.; Ito, Y.; Kishi, R. HPV vaccination crisis in Japan. Lancet 2015, 385, 2571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simms, K.T.; Hanley, S.J.B.; Smith, M.A.; Keane, A.; Canfell, K. Impact of HPV vaccine hesitancy on cervical cancer in Japan: A modeling study. Lancet Public Health 2020, 5, e223–e234. [Google Scholar] [CrossRef] [PubMed]
- Karube, A.; Saito, F.; Nakamura, E.; Shitara, A.; Ono, N.; Konno, M.; Tamura, D.; Nagao, D. Reduction in HPV 16/18 prevalence among young women following HPV vaccine introduction in a highly vaccinated district, Japan, 2008-2017. J. Rural. Med. 2019, 14, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, K.; Yaegashi, N.; Iwata, T.; Yamamoto, K.; Aoki, Y.; Okadome, M.; Ushijima, K.; Kamiura, S.; Takehara, K.; MINT Study Group; et al. Reduction in HPV16/18 prevalence among young women with high-grade cervical lesions following the Japanese HPV vaccination program. Cancer Sci. 2019, 110, 3811–3820. [Google Scholar] [CrossRef]
- Onuki, M.; Yamamoto, K.; Yahata, H.; Kanao, H.; Horie, K.; Konnai, K.; Nio, A.; Takehara, K.; Kamiura, S.; For The Mint Study Group; et al. Changes in HPV16/18 Prevalence among Unvaccinated Women with Cervical Intraepithelial Neoplasia in Japan: Assessment of Herd Effects following the HPV Vaccination Program. Vaccines 2022, 10, 188. [Google Scholar] [CrossRef]
- Kitamura, T.; Suzuki, M.; Shigehara, K.; Fukuda, K. Prevalence and Risk Factors of Human Papillomavirus Infection among Japanese Female People: A Nationwide Epidemiological Survey by Self-Sampling. Asian Pac. J. Cancer Prev. 2021, 22, 1843–1849. [Google Scholar] [CrossRef]
- Imai, H.; Nakao, H.; Shinohara, H.; Watarai, M.; Matsumoto, N.; Yamagishi, T.; Saito, M.; Kitamura, T. Prevalence, Potential Predictors, and Genotype-Specific Prevalence of Human Papillomavirus Infection among Sexually Active Students in Japan. PLoS ONE 2015, 10, e0132462. [Google Scholar] [CrossRef] [Green Version]
- Bouvard, V.; Baan, R.; Straif, K.; Grosse, Y.; Secretan, B.; El Ghissassi, F.; Benbrahim-Tallaa, L.; Guha, N.; Freeman, C.; WHO International Agency for Research on Cancer Monograph Working Group; et al. A review of human carcinogens--Part B: Biological agents. Lancet Oncol. 2009, 10, 321–322. [Google Scholar] [CrossRef]
- Onuki, M.; Matsumoto, K.; Satoh, T.; Oki, A.; Okada, S.; Minaguchi, T.; Ochi, H.; Nakao, S.; Someya, K.; Yamada, N.; et al. Human papillomavirus infections among Japanese women: Age-related prevalence and type-specific risk for cervical cancer. Cancer Sci. 2009, 100, 1312–1316. [Google Scholar] [CrossRef] [PubMed]
- Azuma, Y.; Kusumoto-Matsuo, R.; Takeuchi, F.; Uenoyama, A.; Kondo, K.; Tsunoda, H.; Nagasaka, K.; Kawana, K.; Morisada, T.; Iwata, T.; et al. Human papillomavirus genotype distribution in cervical intraepithelial neoplasia grade 2/3 and invasive cervical cancer in Japanese women. Jpn. J. Clin. Oncol. 2014, 44, 910–917. [Google Scholar] [CrossRef]
- Nicolet, L.; Viviano, M.; Dickson, C.; Jeannot, E. Factors influencing the decision to vaccinate against HPV amongst a population of female health students. Vaccines 2022, 10, 680. [Google Scholar] [CrossRef]
- Konno, R.; Dobbelaere, K.O.; Godeaux, O.O.; Tamura, S.; Yoshikawa, H. Immunogenicity, reactogenicity, and safety of human papillomavirus 16/18 AS04-adjuvanted vaccine in Japanese women: Interim analysis of a phase II, double-blind, randomized controlled trial at month 7. Int. J. Gynecol. Cancer 2009, 19, 905–911. [Google Scholar] [CrossRef]
- Kurokawa, T.; Onuma, T.; Shinagawa, A.; Chino, Y.; Kobayashi, M.; Yoshida, Y. The ideal strategy for cervical cancer screening in Japan: Result from the Fukui Cervical Cancer Screening Study. Cytopathology 2018, 29, 361–367. [Google Scholar] [CrossRef]
- Newsletter from the Ministry of Health, Labour and Welfare in Japan. Available online: https://www.mhlw.go.jp/stf/houdou_kouhou/kouhou_shuppan/magazine/202205_00001.html (accessed on 23 October 2022).
- Matsuzawa, Y.; Kitamura, T.; Suzuki, M.; Koyama, Y.; Shigehara, K. Prevalence, Genotype Distribution, and Predictors against HPV Infections Targeted by 2-, 4-, 9-Valent HPV Vaccines among Japanese Males. Vaccines 2020, 8, 221. [Google Scholar] [CrossRef]
- de Sanjosé, S.; Diaz, M.; Castellsagué, X.; Clifford, G.; Bruni, L.; Muñoz, N.; Bosch, F.X. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: A meta-analysis. Lancet Infect. Dis. 2007, 7, 453–459. [Google Scholar] [CrossRef] [PubMed]
- News/HPV Self-Sampling in Sweden Leading to Faster Elimination of Cervical Cancer. Available online: https://www.who.int/europe/news/item/08-09-2022-hpv-self-sampling-in-sweden-leading-to-faster-elimination-of-cervical-cancer (accessed on 23 October 2022).
- Serrano, B.; Ibáñez, R.; Robles, C.; Peremiquel-Trillas, P.; de Sanjosé, S.; Bruni, L. Worldwide use of HPV self-sampling for cervical cancer screening. Prev. Med. 2022, 154, 106900. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Center Japan/Updated Cervical Cancer Screening Guidelines based on Efficacy Assessment. Available online: https://www.ncc.go.jp/jp/information/pr_release/2020/0729/20200729.pdf (accessed on 23 October 2022).
- Kudo, R.; Yamaguchi, M.; Sekine, M.; Adachi, S.; Ueda, Y.; Miyagi, E.; Hara, M.; Hanley, S.; Enomoto, T. Bivalent Human Papillomavirus Vaccine Effectiveness in a Japanese Population: High Vaccine-Type-Specific Effectiveness and Evidence of Cross-Protection. J. Infect. Dis. 2019, 219, 382–390. [Google Scholar] [CrossRef] [Green Version]
- Kreimer, A.R.; Sampson, J.N.; Porras, C.; Schiller, J.T.; Kemp, T.; Herrero, R.; Wagner, S.; Boland, J.; Schussler, J.; Costa Rica HPV Vaccine Trial (CVT) Group; et al. Evaluation of Durability of a Single Dose of the Bivalent HPV Vaccine: The CVT Trial. J. Natl. Cancer Inst. 2020, 112, 1038–1046. [Google Scholar] [CrossRef]
- Tsang, S.H.; Sampson, J.N.; Schussler, J.; Porras, C.; Wagner, S.; Boland, J.; Cortes, B.; Lowy, D.R.; Schiller, J.T.; Costa Rica HPV Vaccine Trial (CVT) Group; et al. Durability of Cross-Protection by Different Schedules of the Bivalent HPV Vaccine: The CVT Trial. J. Natl. Cancer Inst. 2020, 112, 1030–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaguchi, M.; Sekine, M.; Kudo, R.; Adachi, S.; Ueda, Y.; Miyagi, E.; Hara, M.; Hanley, S.; Enomoto, T. Differential misclassification between self-reported status and official HPV vaccination records in Japan: Implications for evaluating vaccine safety and effectiveness. Papillomavirus Res. 2018, 6, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.; Ploner, A.; Elfström, K.M.; Wang, J.; Roth, A.; Fang, F.; Sundström, K.; Dillner, J.; Sparén, P. HPV Vaccination and the Risk of Invasive Cervical Cancer. N. Engl. J. Med. 2020, 383, 1340–1348. [Google Scholar] [CrossRef] [PubMed]
- Falcaro, M.; Castañon, A.; Ndlela, B.; Checchi, M.; Soldan, K.; Lopez-Bernal, J.; Elliss-Brookes, L.; Sasieni, P. The effects of the national HPV vaccination programme in England, UK, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: A register-based observational study. Lancet 2021, 398, 2084–2092. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | Number of Participants | |
|---|---|---|
| (Total, n = 2044) | ||
| Age, year-old | Median (range) | 30 (16–75) |
| Age group, n (%) | 16–19 years | 33 (1.6%) |
| 20–24 years | 423 (20.7%) | |
| 25–29 years | 531 (26.0%) | |
| 30–34 years | 398 (19.5%) | |
| 35–39 years | 270 (13.2%) | |
| 40–44 years | 193 (9.4%) | |
| 45–49 years | 109 (5.3%) | |
| ≥50 years | 87 (4.3%) | |
| Educational status, n (%) | ≤12 years | 294 (14.6%) |
| >12 years | 1726 (85.4%) | |
| Missing | 24 | |
| Smoking status, n (%) | Never | 1533 (75.7%) |
| Former | 326 (16.1%) | |
| Current | 165 (8.2%) | |
| Missing | 20 | |
| Number of lifetime sex partners, n (%) | 1–5 | 994 (50.5%) |
| 6–10 | 424 (21.6%) | |
| 11–20 | 284 (14.4%) | |
| ≥21 | 265 (13.5%) | |
| Missing | 77 | |
| Age of coitarche, n (%) | <20 years | 1158 (59.9%) |
| ≥20 years | 775 (40.1%) | |
| Missing | 111 | |
| Marital status, n (%) | Married | 742 (36.7%) |
| Unmarried | 1282 (63.3%) | |
| Missing | 20 | |
| Divorce, n (%) | Never | 1862 (92.3%) |
| Once | 144 (7.1%) | |
| Twice | 11 (0.5%) | |
| Missing | 27 | |
| Number of children, n (%) | 0 | 1434 (70.6%) |
| 1 | 247 (12.2%) | |
| 2 | 263 (12.9%) | |
| ≥3 | 87 (4.3%) | |
| Missing | 13 | |
| Experience of commercial sex work, n (%) | No | 1852 (91.5%) |
| Yes | 171 (8.5%) | |
| Missing | 21 | |
| Current STI, n (%) | No | 1892 (93.6%) |
| Yes | 130 (6.4%) | |
| Missing | 22 | |
| Past history of STI, n (%) | No | 1401 (69.5%) |
| Yes | 615 (30.5%) | |
| Missing | 28 | |
| Status of HPV vaccination, n (%) | No | 1579 (77.7%) |
| Yes | 454 (22.3%) | |
| Missing | 11 | |
| Parameters | Unvaccinated | Vaccinated | p-Value | |
|---|---|---|---|---|
| (n = 1579) | (n = 454) | |||
| Age, years, median (range) | 32 (16–75) | 24 (18–46) | <0.001 | |
| Age group, n (%) | 16–19 | 26 (1.6%) | 5 (1.1%) | <0.001 |
| 20–24 | 165 (10.4%) | 254 (55.9%) | ||
| 25–29 | 405 (25.6%) | 123 (27.1%) | ||
| 30–34 | 359 (22.7%) | 38 (8.4%) | ||
| 35–39 | 248 (15.7%) | 22 (4.8%) | ||
| 40–44 | 184 (11.7%) | 8 (1.8%) | ||
| 45–49 | 105 (6.6%) | 4 (0.9%) | ||
| ≥50 | 87 (5.5%) | 0 (0.0%) | ||
| Educational status, n (%) | ≤12 years | 252 (16.1%) | 42 (9.4%) | <0.001 |
| >12 years | 1316 (83.9%) | 407 (90.6%) | ||
| Missing | 11 | 5 | ||
| Smoking status, n (%) | Never | 1158 (74.0%) | 371 (81.7%) | <0.001 |
| Former | 277 (17.7%) | 49 (10.8%) | ||
| Current | 130 (8.3%) | 34 (7.5%) | ||
| Missing | 14 | 0 | ||
| Number of lifetime sex partners, n (%) | 1–5 | 766 (50.2%) | 226 (51.7%) | 0.703 |
| 6–10 | 325 (21.3%) | 97 (22.2%) | ||
| 11–20 | 222 (14.5%) | 62 (14.2%) | ||
| ≥21 | 213 (14.0%) | 52 (11.9%) | ||
| Missing | 53 | 17 | ||
| Age of coitarche, n (%) | <20 years | 863 (57.7%) | 293 (67.5%) | <0.001 |
| ≥20 years | 632 (42.3%) | 141 (32.5%) | ||
| Missing | 84 | 20 | ||
| Marital status, n (%) | Married | 671 (42.8%) | 71 (15.7%) | <0.001 |
| Unmarried | 897 (57.2%) | 380 (84.3%) | ||
| Missing | 11 | 3 | ||
| Divorce, n (%) | Never | 1416 (90.7%) | 441 (97.8%) | <0.001 |
| Once | 135 (8.6%) | 9 (2.0%) | ||
| Twice | 10 (0.6%) | 1 (0.2%) | ||
| Missing | 18 | 3 | ||
| Number of children, n (%) | 0 | 1017 (64.7%) | 412 (90.7%) | <0.001 |
| 1 | 224 (14.2%) | 23 (5.1%) | ||
| 2 | 251 (16.0%) | 12 (2.6%) | ||
| 3 | 80 (5.1%) | 7 (1.5%) | ||
| Missing | 7 | 0 | ||
| Experience of commercial sex work, n (%) | No | 1434 (91.5%) | 414 (91.8%) | 0.818 |
| Yes | 134 (8.5%) | 37 (8.2%) | ||
| Missing | 11 | 3 | ||
| Current STI, n (%) | No | 1475 (94.2%) | 413 (91.2%) | 0.023 |
| Yes | 90 (5.8%) | 40 (8.8%) | ||
| Missing | 14 | 1 | ||
| Past history of STI, n (%) | No | 1085 (69.6%) | 313 (69.2%) | 0.902 |
| Yes | 475 (30.4%) | 139 (30.8%) | ||
| Missing | 19 | 2 | ||
| Characteristics of the Participants | Crude OR (95% CI) | Adjusted OR * (95%CI) | |
|---|---|---|---|
| Age group | 16–19 | Reference | Reference |
| 20–24 | 1.153 (0.553–2.406) | 0.991 (0.399–2.457) | |
| 25–29 | 1.127 (0.543–2.339) | 0.897 (0.364–2.208) | |
| 30–34 | 0.764 (0.364–1.603) | 0.671 (0.267–1.686) | |
| 35–39 | 0.673 (0.316–1.436) | 0.586 (0.226–1.517) | |
| 40–44 | 0.517 (0.236–1.133) | 0.445 (0.164–1.210) | |
| 45–49 | 0.468 (0.201–1.090) | 0.395 (0.132–1.183) | |
| ≥50 | 0.394 (0.161–0.963) | 0.872 (0.282–2.701) | |
| Educational status | ≤12 years | Reference | Reference |
| >12 years | 0.765 (0.592–0.989) | 1.134 (0.815–1.578) | |
| Smoking status | Never | Reference | Reference |
| Former | 1.459 (1.137–1.872) | 1.294 (0.949–1.763) | |
| Current | 2.292 (1.657–3.170) | 1.289 (0.871–1.905) | |
| Number of lifetime sex partners | 1–5 | Reference | Reference |
| 6–10 | 2.941 (2.273–3.806) | 2.978 (2.215–4.004) | |
| 11–20 | 5.239 (3.936–6.974) | 5.471 (3.871–7.734) | |
| ≥21 | 8.718 (6.454–11.775) | 8.611 (5.755–12.885) | |
| Age of coitarche | <20 years | Reference | Reference |
| ≥20 years | 0.658 (0.540–0.802) | 1.318 (1.015–1.711) | |
| Marital status | Married | Reference | Reference |
| Unmarried | 2.433 (1.974–3.000) | 1.467 (1.046–2.058) | |
| Divorce | Never | Reference | Reference |
| Once | 1.240 (0.872–1.764) | 1.217 (0.773–1.918) | |
| Twice | 5.678 (1.501–21.481) | 5.397 (0.926–31.450) | |
| Number of children | 0 | Reference | Reference |
| 1 | 0.565 (0.416–0.768) | 0.849 (0.546–1.318) | |
| 2 | 0.405 (0.293–0.561) | 0.677 (0.415–1.103) | |
| ≥3 | 0.296 (0.163–0.539) | 0.590 (0.278–1.252) | |
| Commercial sex work experience | No | Reference | Reference |
| Yes | 3.089 (2.246–4.249) | 0.800 (0.529–1.209) | |
| Current STI | No | Reference | Reference |
| Yes | 4.193 (2.889–6.086) | 2.271 (1.455–3.547) | |
| Past history of STI | No | Reference | Reference |
| Yes | 3.047 (2.497–3.719) | 1.586 (1.225–2.054) | |
| Status of HPV vaccination | No | Reference | Reference |
| Yes | 1.295 (1.041–1.610) | 0.965 (0.717–1.299) | |
| Characteristics of the Participants | Crude OR (95% CI) | Adjusted OR * (95%CI) | |
|---|---|---|---|
| Age group | 16–19 | Reference | Reference |
| 20–24 | 0.419 (0.116–1.509) | 0.557 (0.135–2.291) | |
| 25–29 | 0.793 (0.232–2.714) | 0.485 (0.122–1.930) | |
| 30–34 | 0.670 (0.191–2.349) | 0.373 (0.091–1.532) | |
| 35–39 | 0.506 (0.136–1.877) | 0.276 (0.062–1.234) | |
| 40–44 | 0.604 (0.159–2.294) | 0.286 (0.059–1.375) | |
| 45–49 | 0.283 (0.054–1.475) | 0.083 (0.007–0.942) | |
| ≥50 | 0.482 (0.102–2.280) | 0.364 (0.055–2.420) | |
| Educational status | ≤12 years | Reference | Reference |
| >12 years | 0.960 (0.564–1.632) | 1.595 (0.843–3.016) | |
| Smoking status | Never | Reference | Reference |
| Former | 1.332 (0.817–2.171) | 1.083 (0.618–1.897) | |
| Current | 1.444 (0.769–2.710) | 0.787 (0.362–1.712) | |
| Number of lifetime sex partners | 1–5 | Reference | Reference |
| 6–10 | 3.039 (1.788–5.167) | 3.099 (1.694–5.669) | |
| 11–20 | 2.669 (1.455–4.898) | 3.035 (1.514–6.086) | |
| ≥21 | 5.113 (2.989–8.747) | 4.685 (2.282–9.619) | |
| Age of coitarche | <20 years | Reference | Reference |
| ≥20 years | 0.957 (0.645–1.419) | 1.560 (0.963–2.527) | |
| Marital status | Married | Reference | Reference |
| Unmarried | 1.167 (0.782–1.742) | 0.879 (0.477–1.619) | |
| Divorce | Never | Reference | Reference |
| Once | 0.864 (0.394–1.893) | 0.722 (0.285–1.827) | |
| Twice | 3.756 (0.801–17.608) | 3.452 (0.568–20.986) | |
| Number of children | 0 | Reference | Reference |
| 1 | 1.203 (0.701–2.065) | 1.205 (0.562–2.585) | |
| 2 | 0.643 (0.329–1.257) | 0.721 (0.282–1.842) | |
| ≥3 | 0.581 (0.180–1.878) | 0.886 (0.226–3.471) | |
| Commercial sex work experience | No | Reference | Reference |
| Yes | 2.477 (1.487–4.127) | 1.070 (0.557–2.053) | |
| Current STI | No | Reference | Reference |
| Yes | 3.478 (2.068–5.847) | 1.988 (1.045–3.783) | |
| Past history of STI | No | Reference | Reference |
| Yes | 2.909 (1.986–4.260) | 1.798 (1.112–2.908) | |
| Status of HPV vaccination | No | Reference | Reference |
| Yes | 0.087 (0.028–0.276) | 0.047 (0.011–0.196) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitamura, T.; Suzuki, M.; Shigehara, K.; Fukuda, K.; Matsuyama, T.; Kume, H. Prevalence of Human Papillomavirus Types 16/18 and Effect of Vaccination among Japanese Female General Citizens in the Vaccine Crisis Era. Viruses 2023, 15, 159. https://doi.org/10.3390/v15010159
Kitamura T, Suzuki M, Shigehara K, Fukuda K, Matsuyama T, Kume H. Prevalence of Human Papillomavirus Types 16/18 and Effect of Vaccination among Japanese Female General Citizens in the Vaccine Crisis Era. Viruses. 2023; 15(1):159. https://doi.org/10.3390/v15010159
Chicago/Turabian StyleKitamura, Tadaichi, Motofumi Suzuki, Kazuyoshi Shigehara, Kazuko Fukuda, Taeko Matsuyama, and Haruki Kume. 2023. "Prevalence of Human Papillomavirus Types 16/18 and Effect of Vaccination among Japanese Female General Citizens in the Vaccine Crisis Era" Viruses 15, no. 1: 159. https://doi.org/10.3390/v15010159